")
Back to Journals » International Journal of Women's Health » Volume 13
Maternal and Neonatal Outcomes of Placenta Previa with and without Coverage of a Uterine Scar: A Retrospective Cohort Study in a Tertiary Hospital
Authors Rao J , Fan D , Zhou Z, Luo X, Ma H , Wan Y, Shen X, Lin D , Zhang H, Liu Y, Liu Z
Received 12 March 2021
Accepted for publication 8 June 2021
Published 6 July 2021 Volume 2021:13 Pages 671—681
DOI https://doi.org/10.2147/IJWH.S310097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Everett Magann
Jiaming Rao,1 Dazhi Fan,1 Zixing Zhou,1 Xin Luo,1 Huiting Ma,1 Yingchun Wan,1 Xiuyin Shen,1 Dongxin Lin,1 Huishan Zhang,1 Yan Liu,2 Zhengping Liu1,2
1Foshan Fetal Medicine Institute, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University (Foshan Maternity & Child Healthcare Hospital), Foshan, Guangdong, 528000, People’s Republic of China; 2Department of Obstetrics, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University (Foshan Maternity & Child Healthcare Hospital), Foshan, Guangdong, 528000, People’s Republic of China
Correspondence: Zhengping Liu; Yan Liu
Foshan Fetal Medicine Institute and Department of Obstetrics, Affiliated Foshan Maternity & Child Healthcare Hospital, Southern Medical University (Foshan Maternity & Child Healthcare Hospital), Renminxi Road 11, Foshan, Guangdong, 528000, People’s Republic of China
Tel +86 757 82969878
Fax +86 757 82969772
Email [email protected]; [email protected]
Background: To compare the maternal and neonatal outcomes of placenta previa (PP) with and without coverage of a uterine scar in Foshan, China.
Methods: A retrospective cohort study comparing all singleton pregnancies with PP was conducted at a tertiary, university-affiliated medical center from 1 January 2012 to 31 April 2017 in Foshan, China. Demographic, clinical and laboratory data were extracted from electronic medical records (EMRs). Maternal and neonatal outcomes of PP with and without coverage of a uterine scar were compared by statistical method.
Results: There were 58,062 deliveries during the study period, of which 726 (1.25%) were complicated PP in singleton pregnancies and were further classified into two groups: the PP with coverage of a uterine scar group (PPCS, n=154) and the PP without coverage of a uterine scar group (Non-PPCS, n=572). Overall, premature birth (< 37 weeks, 67.5% vs 54.8%; P=0.019), cesarean section (100% vs 97.6%; P=0.050), intraoperative blood loss > 1000 mL (77.9% vs 16.0%; P< 0.001) or > 3000mL (29.9% vs 3.0%; P< 0.001), bleeding within 2-24 hours after delivery (168.2± 370.1 ml vs 49.9± 58.4 ml; P< 0.001), postpartum hemorrhage (48.7% vs 15.7%; P< 0.001), transfusion (34.6% vs 16.1%; P< 0.001), hemorrhage shock (7.8% vs 1.9%; P< 0.001), hysterectomy (2.6% vs 0.5%; P=0.019), fetal distress (35.7% vs 12.1%; P< 0.001) and APGAR score at 1 min (15.2% vs 7.1%; P=0.002) had a significant difference between PPCS group and Non-PPCS group. After grouping by whether complicated with placenta accreta spectrum disorders (PASD), we found that PPCS was significant associated with more intraoperative blood loss > 1000mL, intraoperative blood loss > 3000mL, bleeding within 2– 24 hours after delivery and fetal distress than the Non-PPCS group.
Conclusion: The PPCS group had poorer maternal and neonatal outcomes than the Non-PPCS group after grouping by whether pregnancies complicated with PASD or with different placental positions.
Keywords: placenta previa, placenta accreta spectrum disorders, pregnancy outcomes, uterine scar, hysterectomy, cesarean section
Plain Language Summary
Placenta previa is particularly dangerous when covering a uterine scar (PPCS). PPCS, also called pernicious placenta previa (PPP), one of the most dangerous types of PP and defined as when the placenta overlies a uterine scar that may or may not with accreta. The incidence of PPCS has increased correspondingly with the increase of cesarean section in China and often leads to unexpected bleeding during delivery and increased risk for peripartum hysterectomy.
This study investigated risk factors and maternal and neonatal outcomes in women with PPCS and Non-PPCS in a Chinese cohort. As the rate of CS increases with China’s universal two children policy, the rate of PP, especially PPCS, will most likely increase as well. Women with PPCS were more likely to have some poorer maternal and neonatal outcomes than the Non-PPCS group even after grouping by whether pregnancies complicated with PASD or with different placental positions. Health care providers should be aware of possible complications of PPCS to provide proper counseling to their patients.
Introduction
Placenta previa (PP) is defined as implantation of the placenta in the lower uterine segment overlying the endocervical os, and it is known as an important cause of serious fetal and maternal morbidity and mortality.1,2 PP is associated with an increased risk of bleeding, blood transfusion, postpartum anemia, hysterectomy, septicemia, thrombophlebitis and maternal death.3–5 A population-based study6 noted that 44.4% of patients with PP delivered before 37 weeks of gestation, 16.9% of these delivered before 34 weeks of gestation, and neonatal mortality rates were increased by threefold to fourfold.
The reported incidence for PP was higher in Asia (1.2%) and lower in Europe (0.36%), North America (0.29%) and sub-Saharan Africa (0.27%).7 Our previous research8 showed that the incidence of PP was between 0.93% and 2.01% in mainland China. Several factors2,5,8–10 increase the risk for PP, including prior cesarean delivery, prior surgical abortion, advancing maternal age, multiparity, multiple pregnancy, and assistive reproductive technology. Although the etiology of placenta previa remains indeterminate, there appears to be a link between endometrial damage and uterine scarring and subsequent placenta previa, which is an important and common cause of the occurrence of the PP. Certainly, Women who have undergone one or more cesarean section are at greater risk for subsequent placenta disorders, and there is a dose–response relationship between the number of prior cesarean sections and subsequent PP and PASD.
In general, PP is subdivided into three categories according to the position of the placenta and the cervix: complete previa, marginal previa, and partial previa. However, PP is particularly dangerous when covering a uterine scar (PPCS). PPCS, also called pernicious placenta previa (PPP), one of the most dangerous types of PP, was proposed by Chattopadhyay et al11 and defined as when the placenta overlies a uterine scar that may or may not with accreta. The incidence of PPCS has increased correspondingly with the increase of cesarean section in China and often leads to unexpected bleeding during delivery and increased risk for peripartum hysterectomy.9,12,13
A large number of previous studies have reported the clinical outcomes and associated risk factors of PP,5,10,11,14–17 and only a few reports have focused on comparing PPCS and Non-PPCS.9,12,13 Information about these conditions is important so that women with a specific type of PP can be appropriately counseled regarding their outcomes and clinical care providers can be appropriately prepared for their deliveries. Thus, the specific objective of this study was to investigate the maternal and neonatal outcomes of women with PPCS and Non-PPCS in a Chinese cohort.
Materials and Methods
Study Design and Population
A retrospective cohort study comparing pregnancies with PP with and without coverage of a uterine scar was conducted over 24 weeks. This hospital was a tertiary university-affiliated medical center with a stable number of approximately 13,000 deliveries per year, which accounted for approximately 10% of the city’s deliveries and provided care for the region’s obstetrical population, especially those with complicated pregnancies. There were 58,062 pregnancies who delivered a liveborn or a stillborn infant of at least 24 gestational weeks at our hospital during the period of January 2012 to March 2017, and 726 women who had complicated PP with a singleton pregnancy were included for further study (Figure 1). All data were retrospectively analyzed from the electronic medical records, surgical records and anesthetic records. Exclusion criteria included multiple pregnancies, misdiagnosis or fetal malformation; not delivering in the study hospital and no archive in the hospital electronic system; or loss of information regarding placental position.
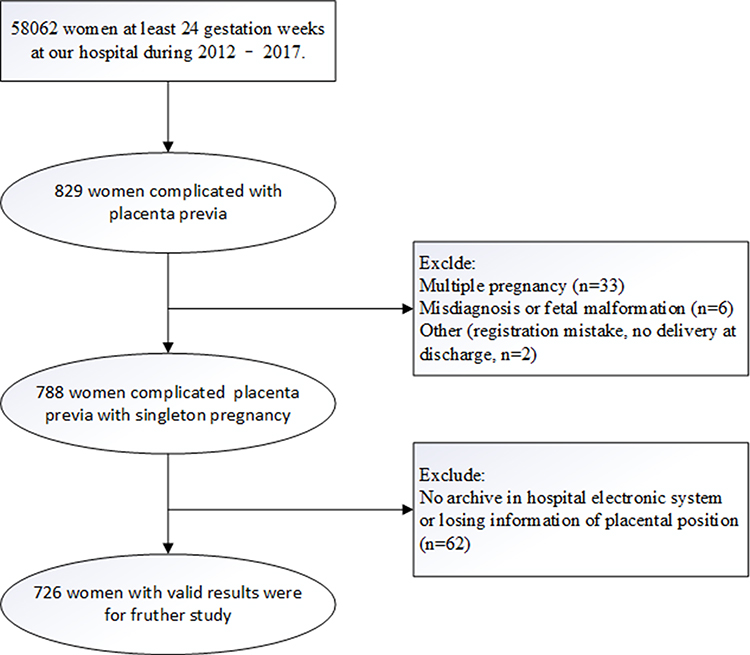 |
Figure 1 Flow chart of the study population. |
PP is defined as implantation of the placenta in the lower uterine segment in advance of the fetus, including complete placenta previa, partial placenta previa and marginal placenta previa. Low-lying placenta previa was excluded in our study because of its different clinical management.18 In this study, the patients with PP were divided into two groups: the placenta previa with coverage of a uterine scar group (PPCS group, n=154 cases) and the placenta previa without coverage of a uterine group (Non-PPCS group, n=572 cases). PPCS was defined as PP where the placenta covered a uterine scar in the lower uterine segment. Non-PPCS was defined as PP where placenta did not cover a uterine scar in the lower uterine segment. The placental position was divided into 3 groups: anterior, posterior, and ante-posterior or laterally positioned. The placental position was evaluated in a transverse cross-section by ultrasound or MRI, in which the maximum placental area was depicted. Anterior placenta is a placenta dominantly attached to the anterior wall of the uterus, and a posterior placenta is a placenta dominantly attached to the posterior wall of the uterus. The other placentas were defined as ante-posterior or laterally positioned.
All types of PP or AIP were diagnosed by experienced obstetricians, based on serial transvaginal or transabdominal ultrasonographic scans or MRI, and confirmed at the time of delivery and pathological results. Detailed diagnostic criteria have been reported in our previous studies.19
Definitions
Clinical and laboratory data were extracted from electronic medical records. The following clinical characteristics were evaluated in all patients: maternal age, BMI, gestational weeks, race/ethnicity, parity, prior CS, mode of delivery, in vitro fertilization and embryo transfer (IVF-ET) or not, diseases associated with pregnancy (gestational diabetes mellitus, hypertension disorder complicating pregnancy). To compare maternal and neonatal outcomes, gestational weeks, mode of delivery (vaginal, CS), postpartum hemorrhage, postpartum anemia, hysterectomy, infant weight, intrauterine death, fetal distress, Umbilical cord blood pH, Apgar score at 1 min, and Apgar score at 5 min were compared in the groups. We calculated gestational age on the basis of the actual delivery date in the medical record. PPH was diagnosed according to blood loss of more than 500 mL for vaginal deliveries and more than 1000 mL for cesarean delivery by the American College of Obstetricians and Gynecologists (ACOG).20 Postpartum anemia was defined as a hemoglobin concentration of <110 g/L (6.8 mmol/L) according to WHO.21 HDCP (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥ 90 mmHg, with or without proteinuria) can be classified into five groups: (1) gestational hypertension, (2) preeclampsia, (3) eclampsia, (4) superimposed preeclampsia on chronic hypertension and (5) chronic hypertension in pregnancy preeclampsia.22 GDM was diagnosed when one of the following conditions was met: (1) fasting plasma glucose ≥ 5.1 mmol /L two or more times; (2) two or more test results equal to or above the following values after a 75 g-load OGTT: fasting, 5.1 mmol/L; 1-hour, 10.0 mmol/L; 2-hour, 8.5 mmol/L. The prediction and diagnosis of fetal distress lacks a single indicator during the prenatal and delivery stages, and we are able to make a diagnosis based on a comprehensive assessment of the following observations:: (1) early stage tachycardia >160 bpm; during severe hypoxia <120bpm; CST shows late deceleration, variable deceleration; fetal heart rate <100 bpm, with frequent late decelerations indicating severe fetal hypoxia, may lie intrauterine any moment; (2)And/or meconium stained amniotic fluid; (3)And/or reduced or absent fetal movement; (4) And/or umbilical cord blood pH < 7.2.
Statistical Analysis
Categorical data were reported as numbers and percentages (%), and descriptive data were expressed as the means ± standard deviations (SD). Boxplots describe the amount of bleeding between groups by using the median, the upper quartile, and the lower quartile. The 95% confidence intervals or interquartile range were calculated and presented. Statistical significance was calculated using the χ2 test or Fisher’s exact test for differences in qualitative variables and the Mann–Whitney U-test or t-test for differences in continuous variables. Statistical analyses were performed with the Statistical Package for Social Science Version 22.0 (SPSS Inc, Chicago, IL, USA) and R (3.4.1). Two-tailed P values <0.05 were considered statistically significant.
Ethics Approval and Informed Consent
The study was approved by the Human Subjects Committee of the Southern Medical University Affiliated Maternal & Child Health Hospital of Foshan. To ensure patient privacy, our data did not include the patient’s name, phone number, home address, or other sensitive information. Informed consent is waived because research is based on EMRs and all information is processed anonymously. This study was conducted in accordance with the Declaration of Helsinki.
Results
There were 58,062 pregnant women who delivered a liveborn or a stillborn infant of at least 24 gestational weeks at our hospital during the period of January 2012 to March 2017, and 726 women had complicated PP with a singleton pregnancy and were identified for further data review (Figure 1). Of these 726 women, 152 (20.9%) had PPCS and 574 (79.1%) had Non-PPCS.
The clinical characteristics of the groups are shown in Table 1. The mean age of individuals with pregnancies complicated with PP was 31.71 ± 5.25 years old, the mean BMI was 26.06 ± 3.11, and the mean number of gestational weeks was 35.70 ± 2.46 weeks. Most of the women were Han Chinese (98.6%), 31.5% were primipara and 8.3% had a pregnancy with IVF-ET. PPCS was significantly associated with advanced maternal age, higher than average BMI, greater parity and prior CS compared with Non-PPCS. There were no significant differences in gestational weeks, IVF-ET, HDCP and GDM between the two groups.
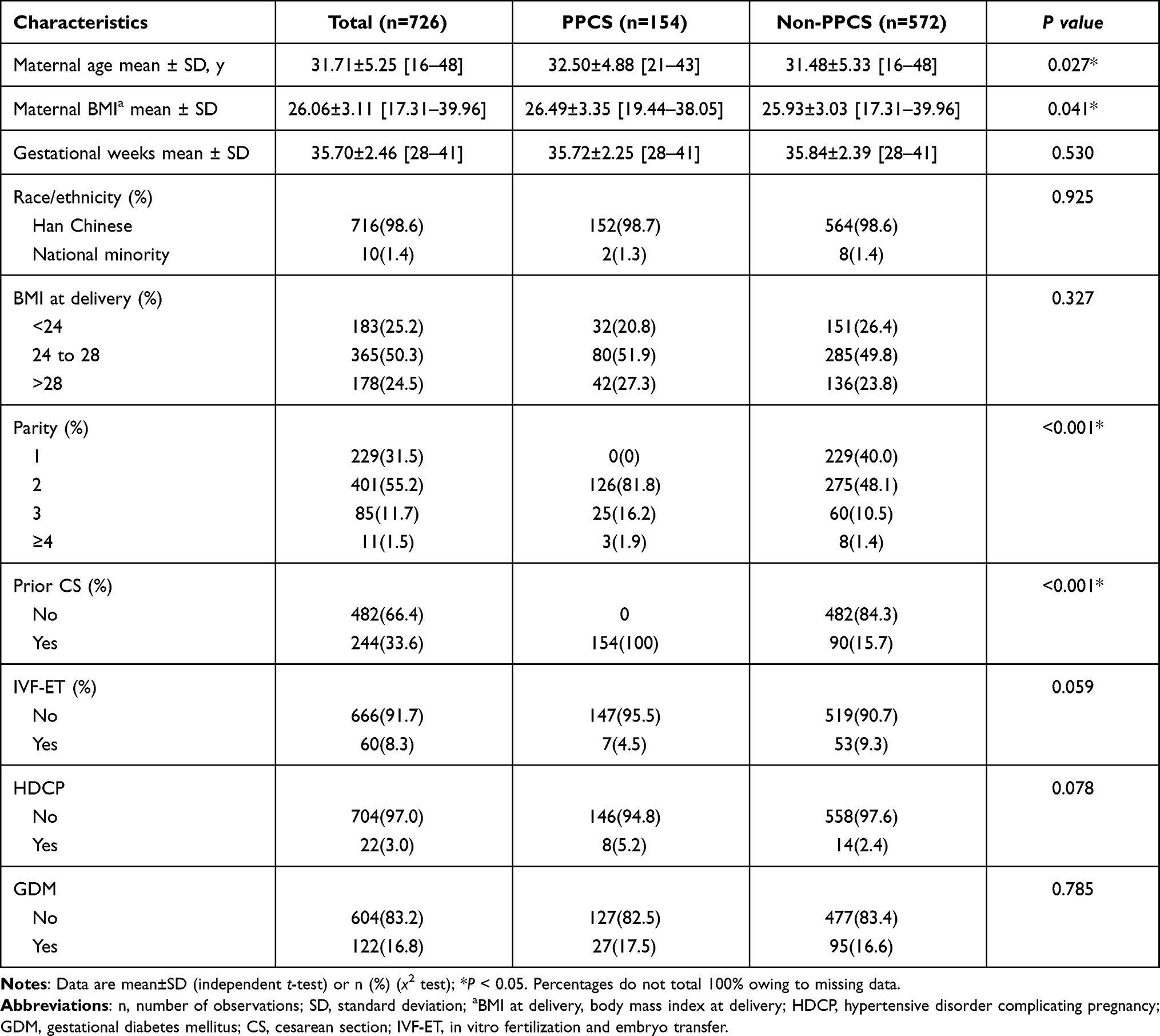 |
Table 1 Comparison of Baseline Characteristics of Patients with PPCS and Non-PPCS |
PPCS was significantly associated with a higher proportion of total PASD (46.8% vs 12.6%, P< 0.001) and placenta increta or percreta (37.7% vs 5.6%) compared to Non-PPCS. The PPCS group was dominated by anterior placentas (46.8%), followed by ante-posterior or laterally positioned (33.8%) and posterior placentas (19.5%), while the Non-PPCS group was dominated by posterior placentas (56.3%), followed by ante-posterior or laterally positioned (21.9%) and anterior placentas (21.9%) (Table 2).
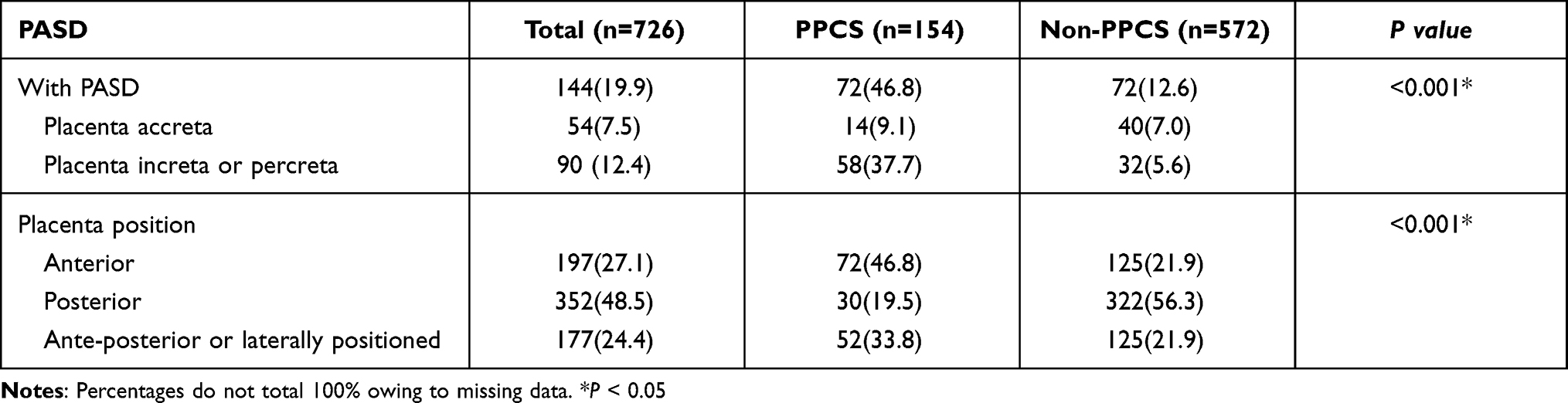 |
Table 2 Comparison of PASD and Placenta Position in Patients in the PPCS and Non-PPCS Groups |
In pregnancies complicated with PASD (n=144, Table 3), the PPCS group was associated with poor maternal outcomes for intraoperative blood loss (3000 [1500, 4500] mL vs 700[400, 1500] mL, P<0.001, Figure 2) and bleeding within 2–24 hours after delivery (220.1 ± 436.4mL vs 65.5±114.2 mL, P=0.008) than the Non-PPCS group. The PPCS group was associated with a higher incidence of intraoperative blood loss> 1000 mL (90.3% vs 40.8%, P<0.001), intraoperative blood loss> 3000 mL (52.8% vs 16.9%, P<0.001) and higher fetal distress (36.1% vs 18.1%, P=0.015) than the Non-PPCS group. There was no significant association between the PPCS group and the Non-PPCS group in the rates of gestational weeks, mode of delivery, postpartum hemorrhage, hemorrhagic shock, postpartum anemia, hysterectomy, intrauterine death, umbilical cord blood and APGAR score at 1 min and 5 min.
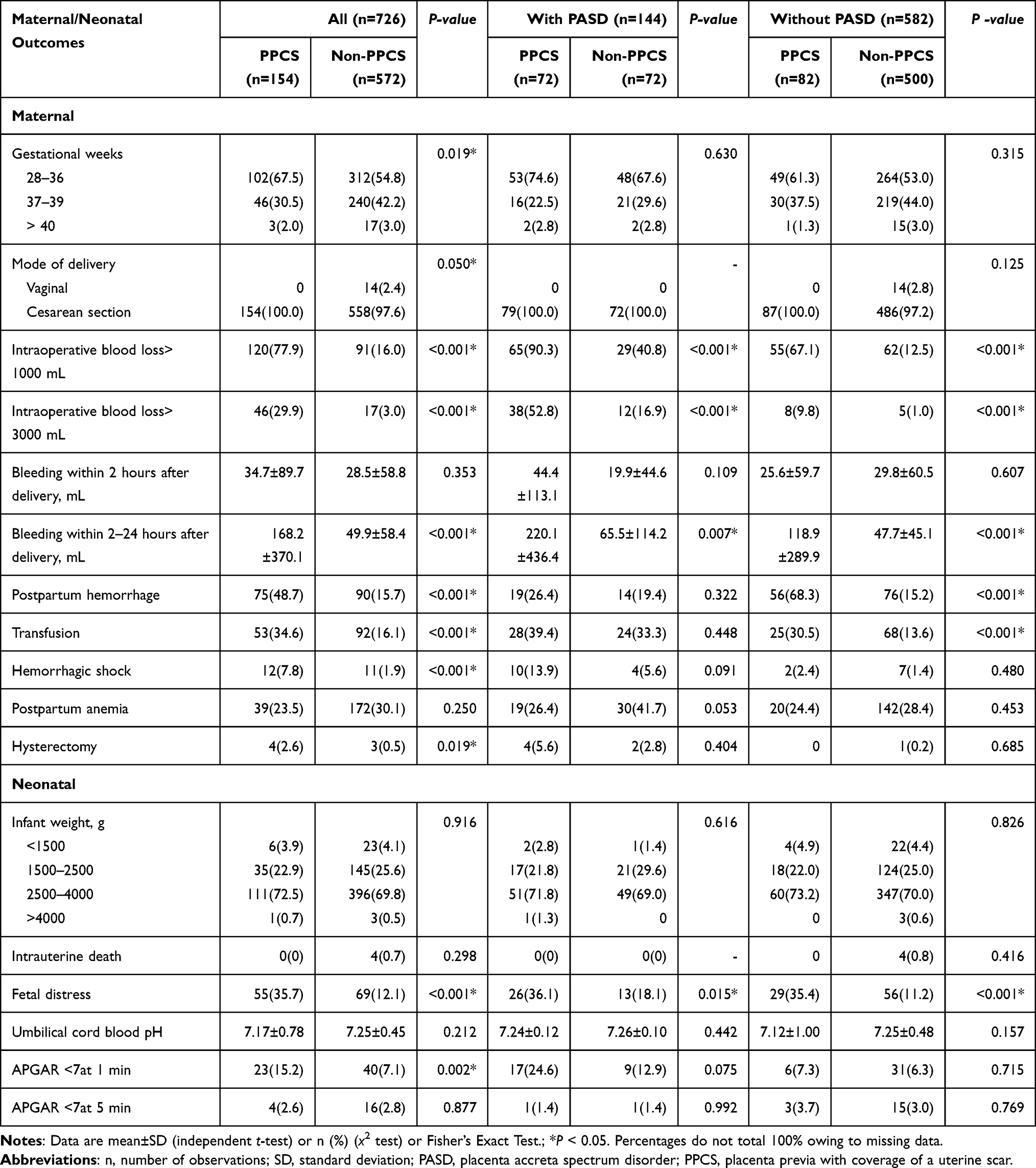 |
Table 3 Comparison of Pregnancy Outcomes with and without PASD in Patients with PPCS and Non-PPCS |
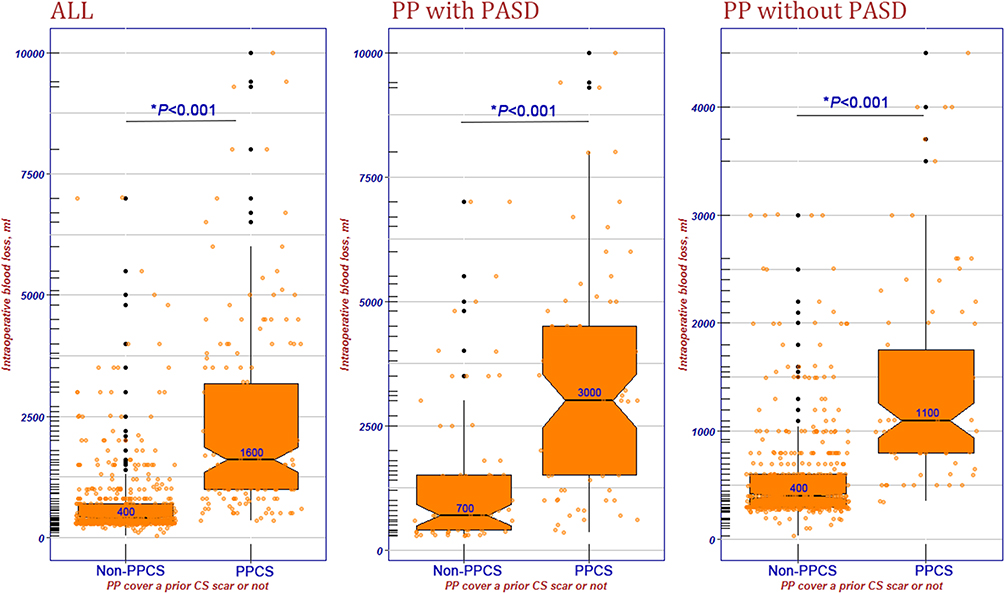 |
Figure 2 Box plots of intraoperative blood loss in the PPCS and Non-PPCS groups of women with and without PASD. *Using t-test for differences between Non-PPCS group and PPCS group. |
In pregnancies not complicated with PASD (n=582, Table 3), the PPCS group was associated with poor maternal outcomes for intraoperative blood loss (1100 [800, 1750] mL vs 400[300, 600] mL, P<0.001, Figure 2), bleeding within 2–24 hours after delivery (118.9±289.9 vs 47.7±45.1 mL, P<0.001). The PPCS group was associated with a higher incidence of intraoperative blood loss> 1000 mL (67.1% vs 12.5%, P<0.001), intraoperative blood loss> 3000 mL (9.8% vs 1.0%, P<0.001), postpartum hemorrhage (68.3% vs 15.2%, P<0.001), transfusion (30.5% vs 13.6%, P<0.001) and higher fetal distress (35.4% vs 11.2%, P<0.001) than the Non-PPCS group. There was no significant association between the PPCS group and Non-PPCS group in the rates of gestational weeks, mode of delivery, hemorrhagic shock, postpartum anemia, hysterectomy, intrauterine death, umbilical cord blood and Apgar score at 1 and 5 min.
In pregnancies complicated with PASD and different placenta position (Anterior, Posterior and Ante-posterior or laterally positioned, n=144, Table S1), the PPCS group was associated with higher intraoperative blood loss > 1000 mL (94.4% vs 57.1%, P=0.001), intraoperative blood loss > 3000 mL (55.6% vs 28.6%, P=0.048) than the Non-PPCS group in anterior placenta; the PPCS group was associated with higher intraoperative blood loss > 1000 mL (77.8% vs 23.1%, P=0.003), intraoperative blood loss > 3000 mL (44.4% vs 3.8%, P=0.003), bleeding within 2–24 hours after delivery (199.0±161.4 vs 58.41±72.04%, P=0.005) than the Non-PPCS group in posterior placenta; the PPCS group was associated with higher intraoperative blood loss > 1000 mL (88.9% vs 45.8%, P=0.001), intraoperative blood loss > 3000 mL (51.9% vs 20.8%, P=0.022) and APGAR <7 at 1 min (29.6% vs 0, P=0.004) than the Non-PPCS group in Ante-posterior or laterally positioned placenta.
In pregnancies not complicated with PASD and different placenta position (Anterior, Posterior and Ante-posterior or laterally positioned, n=582, Table S2), the PPCS group was associated with higher intraoperative blood loss > 1000 mL (66.7% vs 25.5%, P=0.001), intraoperative blood loss > 3000 mL (13.9% vs 3.9%, P=0.037), bleeding within 2–24 hours after delivery (69.5±82.6 vs 44.0±33.7, P=0.018) and postpartum hemorrhage (75.0% vs 29.1%, P<0.001) than the Non-PPCS group in anterior placenta; the PPCS group was associated with higher intraoperative blood loss > 1000 mL (71.4% vs 8.2%, P<0.001), bleeding within 2–24 hours after delivery (121.3±165.6 vs 49.4±51.6, P<0.001), postpartum hemorrhage (66.7% vs 9.5%, P<0.001), transfusion (23.8% vs 8.5%, P=0.021) than the Non-PPCS group in posterior placenta; the PPCS group was associated with higher intraoperative blood loss > 1000 mL (64.0% vs 12.0%, P<0.001), bleeding within 2–24 hours after delivery (196.6±510.5 vs 45.5±32.2, P=0.005) and postpartum hemorrhage (60.0% vs 17.8%, P<0.001) than the Non-PPCS group in Ante-posterior or laterally positioned placenta.
Discussion
Principal Findings of This Study
Prior studies have shown that PP was significantly associated with a range of adverse outcomes for both mothers and neonates; however, comparisons of PP with and without coverage of a uterine scar were rarely reported. Thus, the aim of our study was to investigate the maternal and neonatal outcomes of PPCS and Non-PPCS in a Chinese cohort. This large retrospective cohort study of 726 women with PP between January 2012 and March 2017 found that the PPCS group had poorer maternal and neonatal outcomes for intraoperative blood loss, postpartum hemorrhage, and higher hospitalization expenses than the Non-PPCS group, even after being grouped according to whether they were complicated with PASD and placenta position.
A survey of maternal and child health in Asia by the WHO showed that the rate of cesarean section in China was 46.2% in 2010, which is the three times (15%) of the WHO’s recommended upper limit.23 Another study24 recently found that the cesarean section rate rose from 28.8% in 2008 to 34.9% in 2014. However, this proportion varies widely in the 31 provinces of China from 4% to 62.5% in 2014. The high cesarean delivery rate is associated with an increased risk of placenta previa in subsequent pregnancies since the risk of PP rises as the number of prior cesarean sections increases. Besides, China’s family planning policy has been in place for more than three decades, and most couples have been restricted to only one child since 1980. Therefore, many pregnant women have had a primary cesarean section due to the popularity of caesarean sections and increased safety as well as social factors on account of only one child being allowed. Rising primary cesarean delivery rates strongly affect maternal mortality rates due to the increase of placenta previa and accreta after multiple cesareans. Placental accreta is a serious obstetrical complication and its management is challenging, with more difficult surgical operations and higher hysterectomy rates.25,26 With the rapid growth of the aging population, China relaxed its more than three-decade-old family planning policy and allowed a couple to have two children (Universal two-child policy) in 2016. Hence, it is conceivable that there will be more multipara with a scarred uterus and PPCS in the future in China, which will pose a huge challenge to health care providers.
PP diagnosed in early pregnancy may not persist in late pregnancy and near term. PP is suspected and diagnosed in approximately 5% of pregnancies between 15 and 16 weeks,27 and almost 90% of PP resolves to a normal position by term,28 which may be explained by the elongating of the uterus and the gradually rising position of the placenta away from the cervix with increasing gestational age. However, such a mechanism will be interfered with if the placenta is covered in uterine scarring from a prior CS such that the placenta cannot move normally. The effects of a previous cesarean section were obvious, and the placenta was unlikely to “migration” in the presence of a hysterectomy scar. Moreover, our data showed that nearly half (46.8%) of PPCS pregnancies combined with PASD, suggesting that we should do detailed prenatal examination, including ultrasound and MRI when we find this condition in clinical practice, to determine the likelihood of placenta implantation, location and depth of placenta accreta.
The correlation between gestational age and different types of placenta previa remains controversial. Some studies reported no differences in gestational age at delivery of infants born to mothers with different types of placenta previa.17,29 However, more studies agreed that premature delivery was more frequent in women with complete placenta previa,18,30 but the comparison of preterm birth rates between infants with mothers with PPCS and Non-PPCS is rarely reported. We found that there is no statistic significant difference between PPCS and Non-PPCS in mean gestational weeks, but the PPCS have the higher proportion of gestational weeks <37 the Non-PPCS (67.5% vs 54.8%).
Some studies have addressed whether types of placenta previa are associated with the severity of symptoms in mothers and neonates, but data aimed at understanding PPCS were insufficient. Our results show that women with PPCS had a higher rate of intraoperative blood loss, postpartum hemorrhage, transfusion, and hysterectomy and that the infants born to women with PPCS had lower Apgar scores at 1 min. Specifically, women in the PPCS group are at an approximately 3-fold (48.7% vs 15.7%) increased risk of postpartum hemorrhage, and 5-fold (2.6% vs 0.5%) increased risk of hysterectomy than women in the Non-PPCS group. Additionally, the presence of accreta is often the factor that determines a change in clinical management and outcome. We divided the subjects into an PASD group and non-PASD group and found that obstetric hysterectomy was performed in 5.6% and 0 of the women with PPCS and Non-PPCS, respectively, in the PASD group, while it was performed in 0% and 0.2% of the women with PPCS and Non-PPCS, respectively in the non-PASD group. Prior studies simply compared the hysterectomy rates between the two PASD groups but did not perform subgroup analysis based on the type of placenta implantation. Nevertheless, our results showed that the proportion of women with hysterectomy was lower than that reported in most other studies. Ling Li12 reported that the hysterectomy rate was 8.47% in women with PPCS and 0% in women with Non-PPCS. Another study13 in China reported hysterectomy rates were 11.9% (12/101) and 0.8% (3/369) in women with PPCS and Non-PPCS, respectively. However, there is also a report of a very low hysterectomy rate from Israel, which stated that only 1.2% of mothers with PP underwent a hysterectomy.31 One possible and important reason for the low hysterectomy rate in our study is that obstetricians in our hospital use a random placenta margin incision32 (also calledan Ar’s incision), and we have found it may be a potentially valuable surgical procedure to control intraoperative and postoperative bleeding in pregnancies with complete placenta previa. We believe that retaining the uterus is of great significance to young women who desire to preserve fertility, so it is acceptable to have an increased risk of postpartum hemorrhage and transfusion in women with PPCS if we can preserve the uterus.
There was no significant difference in IVF-ET between the PPCS and Non-PPCS groups in our study because IVF-ET is a potential confounding factor, both HDCP and diabetes or GMD of clinical outcomes. Studies have shown that women who conceived with assisted reproductive technology (ART) procedures had an increased incidence of placenta previa regardless of the type of ART procedure.33,34 The mechanism for the development of the relationship between IVF-ET and PP is uncertain. One explanation is that ART procedures, maternal factors associated with sterility or a combination of both may increase the risk of PP in ART pregnancies. Varying theories have been developed around the effects of hormones on the endometrium, the effects of embryo transfer and the effects of changes in uterine contraction wave patterns.35
Strengths and Limitations of the Study
This is one of the largest studies investigating risk factors and clinical outcomes for PPCS and Non-PPCS placenta previa from a single medical center. The largest strength of this study is that the large sample size allowed us to study the association of PPCS and Non-PPCS and maternal and neonatal outcomes. However, there are several potential limitations to this study. First, despite this hospital being the largest maternity and child health care hospital in Foshan, selection bias is likely because this is a single-center study and this is a retrospective review that relied on medical documentation and a database. Second, although we used ultrasound or MRI to distinguish between the front and back walls of the placenta, the division is not very precise since we did not measure the area of the anterior or posterior placenta walls. Larger studies are needed to determine the safety and efficacy of interventional radiology before this technique can be recommended for routine management of placenta implantation.36 Therefore, this study does not use the following procedures: intraoperative internal iliac artery and/or postoperative uterine artery embolization and internal iliac artery or abdominal balloon occlusion. It would be prudent to compare hospitals at different levels or in different regions due to the presence of different surgical instruments, surgical procedures, hemostasis procedures, surgical physician levels, and anesthetics. Finally, we only reported whether pregnant women had a previous cesarean section, and did not reported the specific number of previous cesarean sections, which may have lost some of information. All of these potential limitations should be considered when interpreting the results of this study.
Conclusion
In conclusion, we investigated risk factors and maternal and neonatal outcomes in women with PPCS and Non-PPCS in a Chinese cohort. As the rate of CS increases with China’s universal two children policy, the rate of PP, especially PPCS, will most likely increase as well. Women with PPCS were more likely to have some poorer maternal and neonatal outcomes than the Non-PPCS group even after grouping by whether pregnancies complicated with PASD or with different placental positions. Health care providers should be aware of possible complications of PPCS to provide proper counseling to their patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank Qili Yang and Xiaoli Li in data collection. The authors would like to thank all medical staff for their collaboration in clinical practice, particularly during data collection.
Author Contributions
JR designed and implemented the study, conducted data analysis and write the manuscript; FD, ZZ, LX, MH, WY, SX, LD and ZH designed the statistical analysis and help with data analysis; FD helped with analysis plan and result interpretation; LY and LZ designed the study and developed the manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the Science and the Foundation of Science and Technology Agency of Foshan City (Grant No: 2017AG100261, 2018AB000261).
Disclosure
The authors have no conflicts of interest relevant to this article.
References
1. Nyberg DA. Diagnostic Imaging of Fetal Anomalies. Lippincott Williams & Wilkins; 2003.
2. Silver RM. Abnormal placentation: placenta previa, vasa previa, and placenta accreta. Obstet Gynecol. 2015;126(3):654–668. doi:10.1097/AOG.0000000000001005
3. Crane JM, Van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol. 2000;17(2):101–105. doi:10.1055/s-2000-9269
4. Knight M. Peripartum hysterectomy in the UK: management and outcomes of the associated haemorrhage. BJOG. 2007;114(11):1380–1387. doi:10.1111/j.1471-0528.2007.01507.x
5. Grobman WA, Gersnoviez R, Landon MB, et al. Pregnancy outcomes for women with placenta previa in relation to the number of prior cesarean deliveries. Obstet Gynecol. 2007;110(6):1249–1255. doi:10.1097/01.AOG.0000292082.80566.cd
6. Ananth CV, Demissie K, Smulian JC, et al. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188(1):275–281. doi:10.1067/mob.2003.10
7. Cresswell J, Ronsmans C, Calvert C, et al. Prevalence of placenta praevia by world region: a systematic review and meta-analysis. Trop Med Int Health. 2013;18(6):712–724. doi:10.1111/tmi.12100
8. Fan D, Wu S, Wang W, et al. Prevalence of placenta previa among deliveries in Mainland China: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2016;95(40):e5107. doi:10.1097/md.0000000000005107
9. Yu L, Hu K, Yang H. [A retrospective analysis on the pernicious placenta previa from 2008 to 2014]. Zhonghua Fu Chan Ke Za Zhi. 2016;51(3):169–173. doi:10.3760/cma.j.issn.0529-567X.2016.03.002. Chinese.
10. Butler E, Dashe J, Ramus R. Association between maternal serum alpha-fetoprotein and adverse outcomes in pregnancies with placenta previa. Obstet Gynecol. 2001;97(1):35–38. doi:10.1016/s0029-7844(00)01095-4
11. Chattopadhyay SK, Kharif H, Sherbeeni MM. Placenta praevia and accreta after previous caesarean section. Eur J Obstet Gynecol Reprod Biol. 1993;52(3):151–156. doi:10.1016/0028-2243(93)90064-J
12. Li L, Liu Y, Yu N, et al. Analysis of risk factors for pernicious placenta praevia. Int J Clin Exp Med. 2017;10(2):3575–3581.
13. Zhu CK, Wang F, Zhou YM, et al. [Maternal outcomes in pregnant women with pernicious placenta previa]. Journal of Zhejiang University (Medical Sciences). 2015;44(3):253–257. doi:10.3785/j.issn.1008-9292.2015.05.03. Chinese.
14. Baldwin HJ, Patterson JA, Nippita TA, et al. Maternal and neonatal outcomes following abnormally invasive placenta: a population-based record linkage study. Acta Obstet Gynecol Scand. 2017;96:1373–1381. doi:10.1111/aogs.13201
15. Crane J, van den Hof M, Dodds L, et al. Neonatal outcomes with placenta previa. Obstet Gynecol. 1999;93(4):541–544. doi:10.1016/s0029-7844(98)00480-3
16. Rosenberg T, Pariente G, Sergienko R, et al. Critical analysis of risk factors and outcome of placenta previa. Arch Gynecol Obstet. 2011;284(1):47–51. doi:10.1007/s00404-010-1598-7
17. Daskalakis G, Simou M, Zacharakis D, et al. Impact of placenta previa on obstetric outcome. Int J Gynaecol Obstetr. 2011;114(3):238–241. doi:10.1016/j.ijgo.2011.03.012
18. Dola C, Garite T, Dowling D, et al. Placenta previa: does its type affect pregnancy outcome? Am J Perinatol. 2003;20(7):353–360.
19. Liu Y, Fan D, Fu Y, et al. Diagnostic accuracy of cystoscopy and ultrasonography in the prenatal diagnosis of abnormally invasive placenta. Medicine. 2018;97(15):e0438. doi:10.1097/MD.0000000000010438
20. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 76, october 2006: postpartum hemorrhage. Obstet Gynecol. 2006;108(4):1039. doi:10.1097/00006250-200610000-00046
21. World Health Organization. Iron Deficiency Anemia. Assessment, Prevention, and Control. World Health Organization; 2001.
22. Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181–192. doi:10.1016/s0029-7844(03)00475-7
23. Lumbiganon P, Laopaiboon M, Gülmezoglu A, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007–08. Lancet. 2010;375(9713):490–499. doi:10.1016/S0140-6736(09)61870-5
24. Li HT, Luo S, Trasande L, et al. Geographic variations and temporal trends in cesarean delivery rates in China, 2008–2014. JAMA. 2017;317(1):69–76. doi:10.1001/jama.2016.18663
25. Shazly SA, Hortu I, Shih JC, et al. Prediction of success of uterus-preserving management in women with placenta accreta spectrum (CON-PAS score): a multicenter international study. Int J Gynaecol Obstetr. 2020. doi:10.1002/ijgo.13518
26. Cirpan T, Akdemir A, Okmen F, et al. Effectiveness of segmental resection technique in the treatment of placenta accreta spectrum. J Maternal Fetal Neonat Med. 2019;1–7. doi:10.1080/14767058.2019.1702019.
27. Bowie JD, Rosenberg ER, Rosenberg ER, et al. The fallacy of placental migration: effect of sonographic techniques. AJR Am J Roentgenol. 1985;144(1):79. doi:10.2214/ajr.144.1.79
28. Khan AT, Stewart KS. Ultrasound placental localisation in early pregnancy. Scott Med J. 1987;32(1):19–21. doi:10.1177/003693308703200109
29. Tuzovic L. Complete versus incomplete placenta previa and obstetric outcome. Int J Gynaecol Obstetr. 2006;93(2):110–117. doi:10.1016/j.ijgo.2006.02.006
30. Sekiguchi A, Nakai A, Kawabata I, et al. Type and location of placenta previa affect preterm delivery risk related to antepartum hemorrhage. Int J Med Sci. 2013;10(12):1683–1688. doi:10.7150/ijms.6416
31. Walfisch A, Sheiner E. Placenta previa and immediate outcome of the term offspring. Arch Gynecol Obstet. 2016;294(4):739–744. doi:10.1007/s00404-016-4044-7
32. Fan D, Wu S, Ye S, et al. Random placenta margin incision for control hemorrhage during cesarean delivery complicated by complete placenta previa: a prospective cohort study. J Maternal Fetal Neonat Med. 2018;1–8. doi:10.1080/14767058.2018.1457638.
33. Pastore LM, Williams CD. Perinatal outcomes in singletons following in vitro fertilization: a meta-analysis. Obstet Gynecol. 2004;104(2):
34. Karami M, Jenabi E, Fereidooni B. The association of placenta previa and assisted reproductive techniques: a meta-analysis. J Maternal Fetal Neonat Med. 2018;31(14):1940–1947. doi:10.1080/14767058.2017.1332035
35. Rombauts L, Motteram C, Berkowitz E, et al. Risk of placenta praevia is linked to endometrial thickness in a retrospective cohort study of 4537 singleton assisted reproduction technology births. Human Reprod. 2014;29(12):2787–2793. doi:10.1093/humrep/deu240
36. Jauniaux E, Alfirevic Z, Bhide AG, et al. Placenta praevia and placenta accreta: diagnosis and management: green-top guideline no. 27a. BJOG. 2018. doi:10.1111/1471-0528.15306
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.