")
Back to Journals » OncoTargets and Therapy » Volume 9
Mast cells positive to tryptase, endothelial cells positive to protease-activated receptor-2, and microvascular density correlate among themselves in hepatocellular carcinoma patients who have undergone surgery
Authors Ammendola M , Sacco R, Sammarco G, Piardi T, Zuccalà V, Patruno R, Zullo A, Zizzo N, Nardo B, Marech I, Crovace A, Gadaleta CD, Pessaux P, Ranieri G
Received 29 January 2016
Accepted for publication 24 April 2016
Published 21 July 2016 Volume 2016:9 Pages 4465—4471
DOI https://doi.org/10.2147/OTT.S105368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Michele Ammendola,1 Rosario Sacco,1 Giuseppe Sammarco,1 Tullio Piardi,2 Valeria Zuccalà,3 Rosa Patruno,4 Alessandra Zullo,1 Nicola Zizzo,4 Bruno Nardo,5 Ilaria Marech,6 Alberto Crovace,7 Cosmo Damiano Gadaleta,6 Patrick Pessaux,8 Girolamo Ranieri6
1Department of Medical and Surgical Sciences, General Surgery Unit, University of Catanzaro “Magna Graecia” Medical School, Catanzaro, Italy; 2Department of General, Digestive and Endocrine Surgery, Hopital Robert Debre, Centre Hospitalier Universitaire de Reims, Universite de Reims Champagne-Ardenne, Reims, France; 3Department of Health Science, Pathology Unit, University of Catanzaro “Magna Graecia” Medical School, Catanzaro, 4Chair of Pathology, Veterinary Medical School, University “Aldo Moro”, Bari, 5Department of Medical and Surgery Sciences, S Orsola Hospital, University of Bologna, Bologna, 6Interventional Radiology Unit with Integrated Section of Translational Medical Oncology, National Cancer Research Centre, “Giovanni Paolo II”, 7Department of Emergency and Organ Transplantation (DETO), Veterinary Medical School, University “Aldo Moro”, Bari, Italy; 8Hepato-Biliary and Pancreatic Surgical Unit, General, Digestive and Endocrine Surgery, IRCAD, IHU Mix-Surg, Institute for Minimally Invasive Image-Guided Surgery, University of Strasbourg, Strasbourg, France
Background: Mast cells (MCs) can stimulate angiogenesis, releasing several proangiogenic cytokines stored in their cytoplasm. In particular MCs can release tryptase, a potent in vivo and in vitro proangiogenic factor via proteinase-activated receptor-2 (PAR-2) activation and mitogen-activated protein kinase phosphorylation. Nevertheless, no data are available concerning the relationship between MC density positive to tryptase (MCDPT), endothelial cells positive to PAR-2 forming microvascular density (PAR-2-MVD), and classical MVD (C-MVD) in hepatocellular carcinoma (HCC) angiogenesis. This study analyzed the correlation between MCDPT, PAR-2-MVD, and C-MVD, each correlated to the others and to the main clinicopathological features, in early HCC patients who underwent surgery.
Methods: A series of 53 HCC patients with early stage (stage 0 according to the Barcelona Clinic Liver Cancer Staging Classification) were selected and then underwent surgery. Tumor tissue samples were evaluated by means of immunohistochemistry and image analysis methods in terms of number of MCDPT, PAR-2-MVD, and C-MVD.
Results: A significant correlation between MCDPT, PAR-2-MVD, and C-MVD groups, each correlated to the others, was found by Pearson t-test analysis (r ranged from 0.67 to 0.81; P-value ranged from 0.01 to 0.03). No other significant correlation was found.
Conclusion: Our in vivo pilot data suggest that MCDPT and PAR-2-MVD may play a role in HCC angiogenesis and could be further evaluated as a target of antiangiogenic therapy.
Keywords: tumour angiogenesis, stromal cells, translational research
Introduction
Mast cells (MCs) can play a role in tumor angiogenesis, and their involvement has been demonstrated in several animal and human malignancies.1,2 MCs can secrete several classical proangiogenic factors, including vascular endothelial growth factor, fibroblast growth factor-2, thymidine phosphorylase, and interestingly a nonclassical proangiogenic factor named tryptase, stored in their secretory granules.3–7 With special reference to tryptase, it induces in vitro microvascular endothelial cells (EC) proliferation in the matrigel assay and displays in vivo capillary growth on the chick embryo chorioallantoic membrane, which is conversely suppressed by tryptase inhibitors.8 This proangiogenic stimulus induced by tryptase is mainly mediated via protease-activated receptor-2 (PAR-2), which belongs to the G-protein-coupled receptor family.9–12 Four forms of PARs have been reported (PAR-1 through PAR-4). In particular, PAR-2 can be activated by proteases such as trypsin and tryptase. These proteases cleave the N terminus to generate a tethered ligand, which interacts and activates the receptor.13–20 Signaling via PAR-2 expressed on ECs elicits activation of the major members of the mitogen-activated protein kinase phosphorylation family and induces EC proliferation. PAR-2 activation also leads to the production of other proangiogenic factors, such as vascular endothelial growth factor, interleukin-8 (IL-8), IL-6, granulocyte-macrophage colony-stimulating factor, and macrophage colony-stimulating factor.21–27
In literature, no data have been published on the relationship between MC density positive to tryptase (MCDPT), ECs positive to PAR-2 forming microvascular density (PAR-2-MVD), and classical MVD (C-MVD) in hepatocellular carcinoma (HCC) angiogenesis.28–30
In this pilot study, we analyzed the number of MCDPT, PAR-2-MVD, and C-MVD to correlate to each other in primary tumor tissue from HCC patients who underwent surgery.
Materials and methods
Study populations
A series of 53 HCC patients with early stage (stage 0 according to the Barcelona Clinic Liver Cancer staging classification) were selected and underwent curative liver resection: segmentectomies and left and right hepatectomies.31–34 The pretreatment evaluation included biochemical liver function, indocyanine green clearance test, complete blood count, coagulation profile, dose serum alpha-fetoprotein, chest X-ray, liver ultrasound with contrast medium (contrast-enhanced ultrasound), and a computed tomography scan of the abdomen. The diagnosis of HCC was histologically confirmed by echo-guided needle aspiration or, alternatively, by classic imaging findings for HCC associated with a pathological increase of alpha-fetoprotein levels higher than the cutoff of 200 ng/mL. In the global series, there were 53 HCCs.35,36 The clinicopathological features of the patients are summarized in Table 1. Full ethical approval and signed consent were obtained from individual patients. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the “Mater Domini” Hospital, “Magna Graecia” University, Catanzaro (2011.61; December 13, 2011).
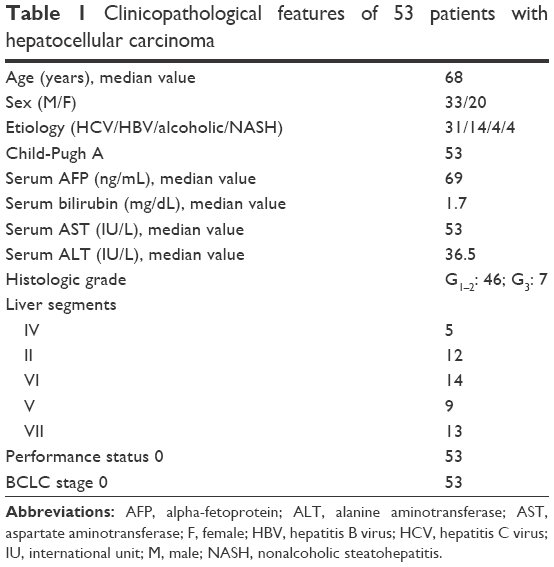 | Table 1 Clinicopathological features of 53 patients with hepatocellular carcinoma |
Immunohistochemistry
For the evaluation of MCDPT, PAR-2-MVD, and C-MVD, a three-layer biotin–avidin–peroxidase system was utilized.37 Briefly, 4 μm thick serial sections of formalin-fixed and paraffin-embedded tumor samples and adjacent normal liver tissue were cut. Sections were then microwaved at 500 W for 10 minutes, after which endogenous peroxidase activity was blocked with 3% hydrogen peroxide solution. Tumor sections were incubated with the following primary antibodies: antitryptase (clone AA1; Dako, Glostrup, Denmark) diluted 1:100 for 1 hour at room temperature, anti-PAR-2 (C-17, sc-8205; Santa Cruz Biotechnology, Dallas, TX, USA) diluted 1:50 for 1 hour at room temperature, and anti-CD34 antibody (QB-END 10; Bio-Optica, Milan, Italy) diluted 1:50 for 1 hour at room temperature as a pan-endothelial marker, respectively. The bound antibody was visualized using a biotinylated secondary antibody, an avidin–biotin peroxidase complex and liquid permanent red (LPS, K0640; Dako). Nuclear counterstaining was performed with Gill’s hematoxylin no 2 (Polysciences, Warrington, PA, USA). The primary antibody was omitted in negative controls.
Morphometrical assay
Light microscopy integrated with an image analysis system (Quantimet-500 Leica, Wetzlar, Germany) was utilized.37 In both tumor sections and adjacent normal liver sections, immunostained areas (hot spots) were selected at low magnification (×100), then MCDPT (Figures 1A and 2A, respectively), PAR-2-MVD (Figures 1B and 2B, respectively), and C-MVD (Figures 1C and 2C, respectively) were assessed at ×400 magnification (0.19 mm2 area).
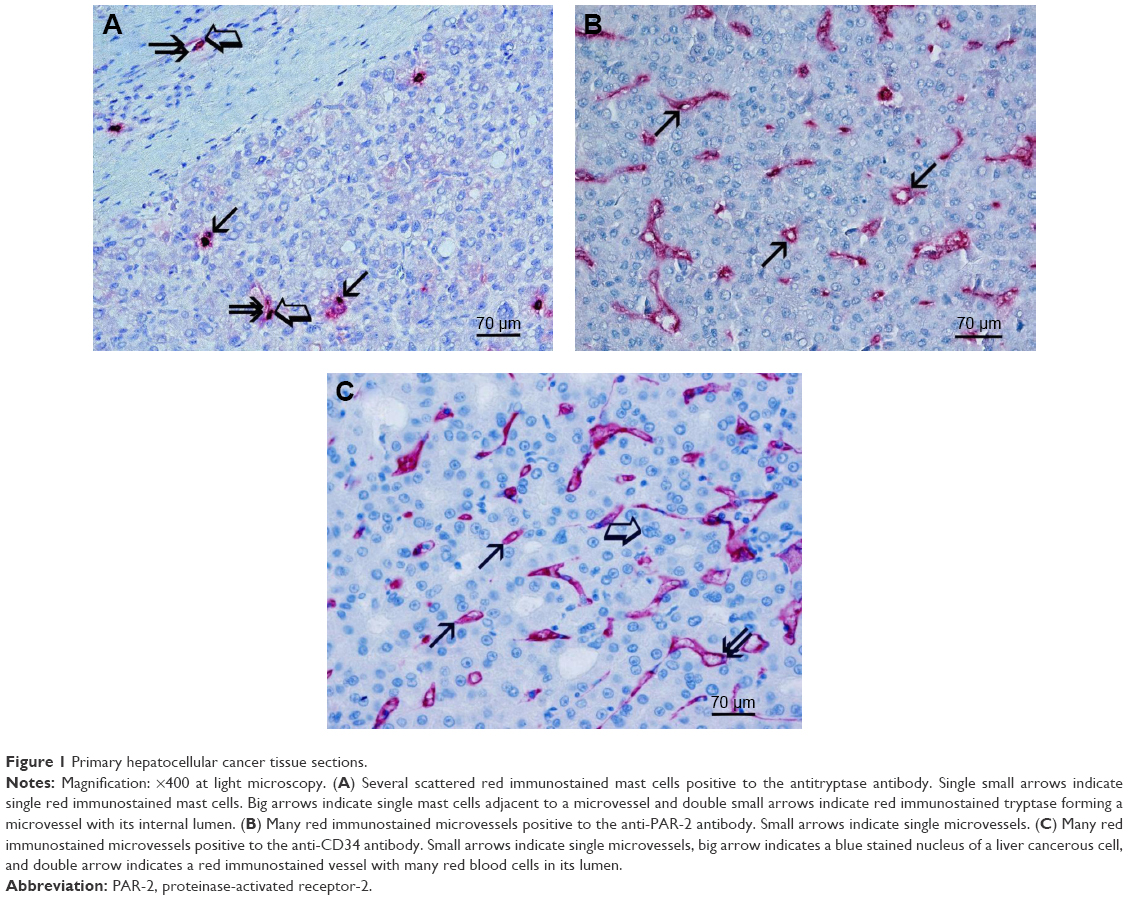 | Figure 1 Primary hepatocellular cancer tissue sections. |
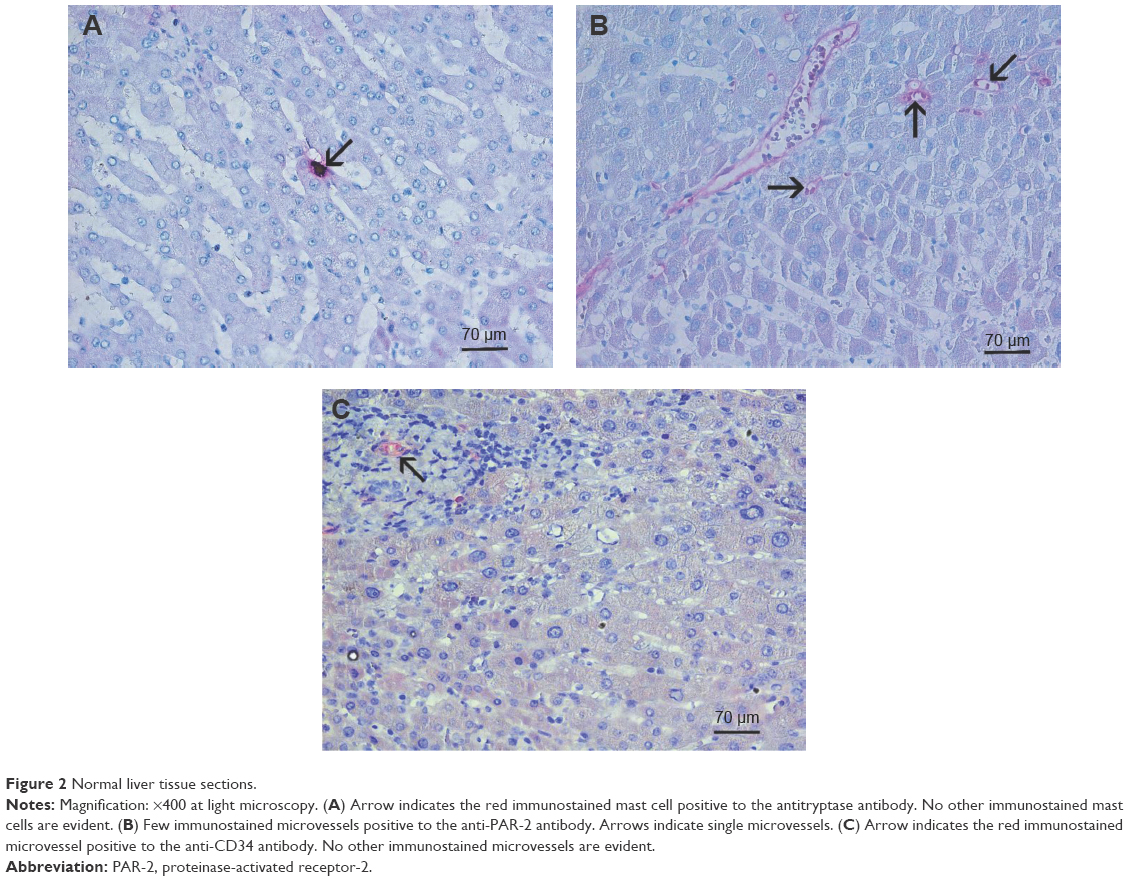 | Figure 2 Normal liver tissue sections. |
Statistical analysis
Mean values ±1 standard deviation (SD) of all the evaluated tissue parameters are reported in Table 2. Correlations between MCDPT, PAR-2-MVD, and C-MVD were calculated using Pearson’s (r) analysis. Correlations among all the analyzed parameters and the main clinicopathological features listed in Table 1 were performed by the chi-square test. P<0.05 was considered significant. All statistical analyses were performed with the SPSS statistical software package (SPSS, Inc., Chicago, IL, USA).
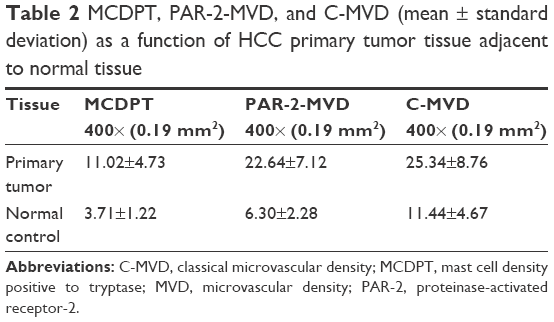 | Table 2 MCDPT, PAR-2-MVD, and C-MVD (mean ± standard deviation) as a function of HCC primary tumor tissue adjacent to normal tissue |
Results
The clinicopathological features of the patients with data expressed as median values are summarized in Table 1. In particular, a series of 53 HCC patients with early stage disease (stage 0 according to the Barcelona Clinic Liver Cancer staging classification) were studied.
In tumor tissue, mean values ±1 SD of MCDPT, PAR-2-MVD, and C-MVD were 11.02±4.73, 22.64±7.12, and 25.34±8.76, respectively. In adjacent normal liver tissue, mean values ±1 SD of MCDPT, PAR-2-MVD, and C-MVD were 3.71±1.22, 6.30±2.28, and 11.44±4.67, respectively. With special regard to tumor tissue, a significant correlation between MCDPT and C-MVD (r=0.77, P=0.02), between PAR-2-MVD and C-MVD (r=0.81, P=0.01), and between MCDPT and PAR-2-MVD (r=0.67, P=0.03) (Figure 3) was found. The results described above are summarized in Table 2. Furthermore, no correlation concerning MCDPT, PAR-2-MVD, and C-MVD and the main clinicopathological features was found.
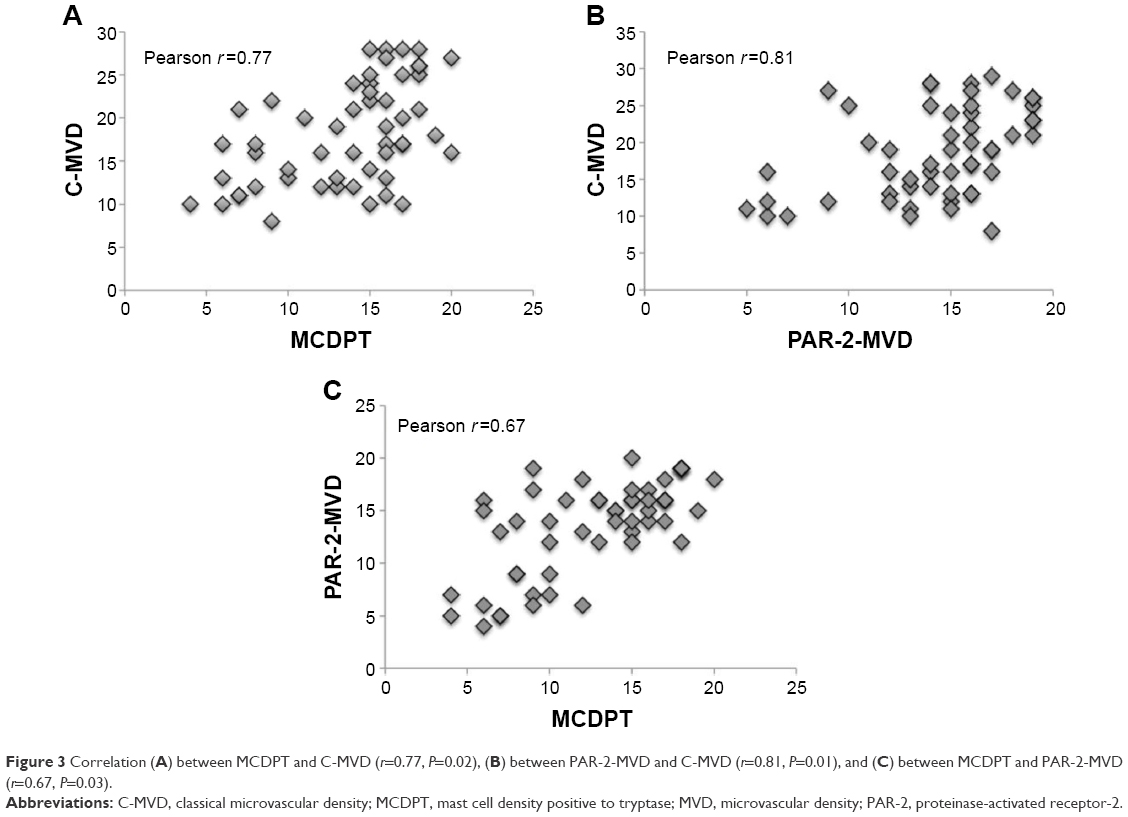 | Figure 3 Correlation (A) between MCDPT and C-MVD (r=0.77, P=0.02), (B) between PAR-2-MVD and C-MVD (r=0.81, P=0.01), and (C) between MCDPT and PAR-2-MVD (r=0.67, P=0.03). |
Discussion
HCC is the fifth leading cause of cancer mortality in the world. HCC is a well-established hypervascular tumor with a high rate of angiogenesis.38 In recent years, MCs have been revealed to be involved as important players in tumor angiogenesis by means of the release of proangiogenic factors stored in their secretory granules. However, the role of MCDPT in HCC angiogenesis has not been well investigated, and no data have been published regarding MVD in terms of PAR-2 endothelial expressing cells.39
In the tumor microenvironment, MCs can be activated in different ways such as: c-kit receptor activation and phosphorylation by stem cell factor, immunoglobulin E mechanism mediated by T lymphocyte–MC interaction, and other microenvironmental stimuli.40,41 After activation, intensive or piecemeal degranulation of secretory granules occurs depending on the MC activation mechanism, and MC-derived proangiogenic factors are released into the tumor microenvironment stimulating angiogenesis.42 Among them, tryptase has been characterized as a powerful nonclassical angiogenic factor in recent years.7,43–45
Tryptase is an agonist of PAR-2 in vascular ECs, which stimulates their proliferation. Signaling via PAR-2 on ECs elicits activation of the major members of the mitogen-activated protein kinase phosphorylation family and contributes to proliferation of ECs and then angiogenesis. Experimental data also suggest that PAR-2 activation leads to the production of other proangiogenic factors, such as vascular endothelial growth factor, interleukin-8, IL-6, granulocyte-macrophage colony-stimulating factor, and macrophage colony-stimulating factor.23–27,46–48
Among the few available data regarding the role of MC tryptase and angiogenesis in HCC patients, Grizzi et al49 have demonstrated that MC accumulation at the tumor site may lead to increased rates of tumor vascularity and, consequently, increased rates of tumor growth and metastasis. In this study, no immunohistochemical method was employed in that MC density was evaluated by a histochemical method using toluidine blue stain, and tumor vascularization was also evaluated by Direct-red 80.49
In order to analyze the role of MC tryptase, Goffredo et al suggested the potential biomarker role of tryptase in 30 HCC patients, and the study showed decreased serum tryptase levels after hepatic transarterial chemoembolization treatment, indicating that tryptase is concentrated in primary tumor tissue.28
Here, our pilot results demonstrate an association between MCDPT, PAR-2-MVD, and C-MVD, supporting the central role of tryptase as a main proangiogenic factor in primary HCC. Based on these data, it is possible to speculate that the inhibition of tryptase by means of gabexate mesilate or nafamostat mesilate could be a novel antiangiogenic strategy worthy of clinical investigation.50–53
Acknowledgment
The authors would like to thank Caroline Oakley for manuscript editing.
Author contribution
Michele Ammendola and Girolamo Ranieri conceived and designed the study; Rosario Sacco, Bruno Nardo, Giuseppe Sammarco, Michele Ammendola, and Alessandra Zullo performed the surgery: Cosmo Damiano Gadaleta, Ilaria Marech, Tullio Piardi, and Patrick Pessaux analyzed the data; Valeria Zuccalà, Rosa Patruno, Alberto Crovace, Nicola Zizzo, and Girolamo Ranieri contributed reagents/materials/analysis tools and immunohistochemistry. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Gulubova M, Vlaykova T. Prognostic significance of mast cell number and microvascular density for the survival of patients with primary colorectal cancer. J Gastroenterol Hepatol. 2009;24(7):265–275. | ||
Marech I, Ammendola M, Sacco R, et al. Serum tryptase, mast cells positive to tryptase and microvascular density evaluation in early breast cancer patients: possible translational significance. BMC Cancer. 2014;14:534. | ||
Marech I, Ammendola M, Gadaleta C, et al. Possible biological and translational significance of mast cells density in colorectal cancer. World J Gastroenterol. 2014;20(27):8910–8920. | ||
Ammendola M, Sacco R, Sammarco G, et al. Correlation between serum tryptase, mast cells positive to tryptase and microvascular density in colo-rectal cancer patients: possible biological-clinical significance. PLoS One. 2014;9(6):e99512. | ||
Ammendola M, Sacco R, Sammarco G, et al. Mast cells positive to tryptase and c-kit receptor expressing cells correlates with angiogenesis in gastric cancer patients surgically treated. Gastroenterol Res Pract. 2013;2013:703163. | ||
Ammendola M, Sacco R, Donato G, et al. Mast cell positivity to tryptase correlates with metastatic lymph nodes in gastrointestinal cancer patients treated surgically. Oncology. 2013;85(2):111–116. | ||
Marech I, Leporini C, Ammendola M, et al. Classical and non classical proangiogenic factors as a target of antiangiogenic therapy in tumor microenvironment. Cancer Lett. 2015;S0304–3835(15):00483–00488. | ||
Ribatti D, Ranieri G, Nico B, et al. Tryptase and chymase are angiogenic in vivo in the chorioallantoic membrane assay. Int J Dev Biol. 2011;55:99–102. | ||
Blair RJ, Meng H, Marchese MJ, et al. Human mast cells stimulate vascular tube formation. Tryptase is a novel, potent angiogenic factor. J Clin Invest. 1997;99:2691–2700. | ||
Stack MS, Johnson DA. Human mast cell tryptase activates single-chain urinary-type plasminogen activator (pro-urokinase). J Biol Chem. 1994;269:9416–9419. | ||
Fajardo I, Pejler G. Human mast cell beta-tryptase is a gelatinase. J Immunol. 2003;171:1493–1499. | ||
Itoh Y, Sendo T, Oishi R. Physiology and pathophysiology of proteinase-activated receptors (PARs): role of tryptase/PAR-2 in vascular endothelial barrier function. J Pharmacol Sci. 2005;97:14–19. | ||
Rickard A, Portell C, Kell PJ, et al. Protease-activated receptor stimulation activates a Ca2+-independent phospholipase A2 in bladder microvascular endothelial cells. Am J Physiol Renal Physiol. 2005;288:F714–F721. | ||
Matej R, Mandàkovà P, Netikovà I, et al. Proteinase-activated receptor-2 expression in breast cancer and the role of trypsin on growth and metabolism of breast cancer cell line MDA MB-231. Physiol Res. 2007;56:475–484. | ||
Morris DR, Ding Y, Ricks TK, et al. Protease-activated receptor-2 is essential for factor VIIa and Xa-induced signaling, migration, and invasion of breast cancer cells. Cancer Res. 2006;66:307–314. | ||
Ammendola M, Leporini C, Marech I, et al. Targeting mast cells tryptase in tumor microenvironment: a potential antiangiogenetic strategy. Biomed Int Res. 2014;2014:154702. | ||
Ammendola M, Sacco R, Sammarco G, et al. Mast cells density positive to tryptase correlates with angiogenesis in pancreatic ductal adenocarcinoma patients having undergone surgery. Gastroenterol Res Pract. 2014;2014:951957. | ||
Donato G, Conforti F, Camastra C, et al. The role of mast cell tryptases in cardiac myxoma: histogenesis and development of a challenging tumor. Oncol Lett. 2014;8(1):379–383. | ||
Ammendola M, Zuccalà V, Patruno R, et al. Tryptase-positive mast cells and angiogenesis in keloids: a new possible post-surgical target for prevention. Updates Surg. 2013;65(1):53–57. | ||
Ranieri G, Ammendola M, Patruno R, et al. Tryptase-positive mast cells correlate with angiogenesis in early breast cancer patients. Int J Oncol. 2009;35(1):115–120. | ||
Ammendola M, Marech I, Sammarco G, et al. Infiltrating mast cells correlate with angiogenesis in bone metastases from gastric cancer patients. Int J Mol Sci. 2015;16(2):3237–3250. | ||
Ribatti D, Ranieri G. Tryptase, a novel angiogenic factor stored in mast cell granules. Exp Cell Res. 2014;332(2):157–162. | ||
Malfettone A, Silvestris N, Saponaro C, et al. High density of tryptase-positive mast cells in human colorectal cancer: a poor prognostic factor related to protease-activated receptor 2 expression. J Cell Mol Med. 2013;17(8):1025–1037. | ||
Soreide K, Janssen EA, Körner H, et al. Trypsin in colorectal cancer: molecular biological mechanisms of proliferation, invasion, and metastasis. J Pathol. 2006;209(2):147–156. | ||
Darmoul D, Marie JC, Devaud H, et al. Initiation of human colon cancer cell proliferation by trypsin acting at protease-activated receptor-2. Br J Cancer. 2001;85(5):772–779. | ||
Uusitalo-Jarvinen H, Kurokawa T, Mueller BM, et al. Role of protease activated receptor 1 and 2 signaling in hypoxia-induced angiogenesis. Arterioscler Thromb Vasc Biol. 2007;27(6):1456–1462. | ||
Liu Y, Mueller BM. Protease-activated receptor-2 regulates vascular endothelial growth factor expression in MDA-MB-231 cells via MAPK pathways. Biochem Biophys Res Commun. 2006;344(4):1263–1270. | ||
Goffredo V, Gadaleta CD, Laterza A, et al. Tryptase serum levels in patients suffering from hepatocellular carcinoma undergoing intra-arterial chemoembolization: possible predictive role of response to treatment. Mol Clin Oncol. 2013;1(2):385–389. | ||
Terada T, Matsunaga Y. Increased mast cells in hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J Hepatol. 2000;33(6):961–966. | ||
Kaufmann R, Mussbach F, Henklein P, et al. Proteinase-activated receptor 2-mediated calcium signaling in hepatocellular carcinoma cells. J Cancer Res Clin Oncol. 2011;137(6):965–973. | ||
Forner A, Reig ME, de Lope CR, et al. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis. 2010;30(1):61–74. | ||
Masuzaki R, Yoshida H, Tateishi R, et al. Staging systems: is there a surgical staging and a medical one? hepatologist’s perspective. J Hepatobiliary Pancreat Sci. 2010;17(4):440–442. | ||
Maida M, Orlando E, Cammà C, et al. Staging systems of hepatocellular carcinoma: a review of literature. World J Gastroenterol. 2014;20(15):4141–4150. | ||
Graf D, Vallböhmer D, Knoefel WT, et al. Multimodal treatment of hepatocellular carcinoma. Eur J Intern Med. 2014;25(5):430–437. | ||
Mínguez B, Lachenmayer A. Diagnostic and prognostic molecular markers in hepatocellular carcinoma. Dis Markers. 2011;31(3):181–190. | ||
Rahbari NN, Mehrabi A, Mollberg NM, et al. Hepatocellular carcinoma: current management and perspectives for the future. Ann Surg. 2011;253(3):453–469. | ||
Ranieri G, Grammatica L, Patruno R, et al. A possible role of thymidine phosphorylase expression and 5-fluorouracil increased sensitivity in oropharyngeal cancer patients. J Cell Mol Med. 2007;11:362–368. | ||
Gadaleta CD, Ranieri G. Trans-arterial chemoembolization as a therapy for liver tumours: new clinical developments and suggestions for combination with angiogenesis inhibitors. Crit Rev Oncol Hematol. 2011;80(1):40–53. | ||
Theoharides TC, Conti P. Mast cells: the JEKYLL and HYDE of tumor growth. Trends Immunol. 2004;25:235–241. | ||
Bhattacharyya SP, Drucker I, Reshef T, et al. Activated T lymphocytes induce degranulation and cytokine production by human mast cells following cell-to-cell contact. J Leukoc Biol. 1998;63(3):337–341. | ||
Wasiuk A, de Vries VC, Hartmann K, et al. Mast cells as regulators of adaptive immunity to tumours. Clin Exp Immunol. 2009;155:140–146. | ||
Norrby K. Mast cells and angiogenesis. APMIS. 2002;110:355–371. | ||
Visciano C, Prevete N, Liotti F, et al. Tumor-associated mast cells in thyroid cancer. Int J Endocrinol. 2015;2015:705169. | ||
Marone G, Varricchi G, Loffredo S, Granata F. Mast cells and basophils in inflammatory and tumor angiogenesis and lymphangiogenesis. Eur J Pharmacol. 2016;778:146–151. | ||
Loffredo S, Staiano RI, Granata F, et al. Immune cells as a source and target of angiogenic and lymphangiogenic factors. Chem Immunol Allergy. 2014;99:15–36. | ||
Zhang X, Wang W, Mize GJ, et al. Protease-activated receptor 2 signaling up regulates angiogenic growth factors in renal cell carcinoma. Exp Mol Pathol. 2013;94(1):91–97. | ||
Rasmussen JG, Riis SE, Frobert O, et al. Activation of protease-activated receptor 2 induces VEGF independently of HIF-1. Plos One. 2012;7(9):e46087. | ||
Chang LH, Pan SL, Lai CY, et al. Activated PAR-2 regulates pancreatic cancer progression through ILK/HIF-α-induced TGF-α expression and MEK/VEGF-A-mediated angiogenesis. Am J Pathol. 2013;183(2):566–575. | ||
Grizzi F, Franceschini B, Chiriva-Internati M, et al. Mast cells and human hepatocellular carcinoma. World J Gastroenterol. 2003;9(7):1469–1473. | ||
Erba F, Fiorucci L, Pascarella S, et al. Selective inhibition of human mast cell tryptase by gabexate mesylate, an antiproteinase drug. Biochem Pharmacol. 2001;61(3):271–276. | ||
Mori S, Itoh Y, Shinohata R, et al. Nafamostat mesilate is an extremely potent inhibitor of human tryptase. J Pharmacol Sci. 2003;92(4):420–423. | ||
Humbert M, Castéran N, Letard S, et al. Masitinib combined with standard gemcitabine chemotherapy: in vitro and in vivo studies in human pancreatic tumour cell lines and ectopic mouse model. PLoS One. 2010;5(3):e9430. | ||
Marech I, Patruno R, Zizzo N, et al. Masitinib (AB1010), from canine tumour model to human clinical development: where we are? Crit Rev Oncol Hematol. 2014;91(1):98–111. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.