")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Marked differences in core beliefs about self and others, between sociotropy and autonomy: personality vulnerabilities in the cognitive model of depression
Authors Otani K, Suzuki A, Matsumoto Y, Shirata T
Received 4 January 2018
Accepted for publication 23 February 2018
Published 27 March 2018 Volume 2018:14 Pages 863—866
DOI https://doi.org/10.2147/NDT.S161541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Koichi Otani, Akihito Suzuki, Yoshihiko Matsumoto, Toshinori Shirata
Department of Psychiatry, Yamagata University School of Medicine, Yamagata, Japan
Objective: The cognitive model of depression posits two distinctive personality vulnerabilities termed sociotropy and autonomy, each of which is composed of a cluster of maladaptive self-schemas. It is postulated that negative core beliefs about self underlie maladaptive self-schemas as a whole, whereas those about others may be implicated in the autonomous self-schemas. Therefore, the present study examined the relations of sociotropy and autonomy with core beliefs about self and others.
Methods: The sample of this study consisted of 321 healthy Japanese volunteers. Sociotropy and autonomy were evaluated by the corresponding subscales of the Sociotropy–Autonomy Scale. Core beliefs about self and others were assessed by the negative-self, positive-self, negative-other and positive-other subscales of the Brief Core Schema Scales.
Results: In the forced multiple regression analysis, sociotropy scores were correlated with negative-self scores (β = 0.389, P < 0.001). Meanwhile, autonomy scores were correlated with positive-self scores (β = 0.199, P < 0.01) and negative-other scores (β = 0.191, P < 0.01).
Conclusion: The present study suggests marked differences in core beliefs about self and others between sociotropy and autonomy, further contrasting the two personality vulnerabilities to depression.
Keywords: sociotropy, autonomy, core belief, self, other, personality, cognitive vulnerability
Introduction
Beck’s cognitive model posits that two personality vulnerabilities termed sociotropy and autonomy predispose to depression.1–3 Each of these personalities is composed of a cluster of maladaptive self-schemas, which are formed by negative experiences in early life. The sociotropic self-schemas concern self-evaluation in relation to interpersonal approval and acceptance. In contrast, the autonomous self-schemas concern self-evaluation in relation to independence, self-control and achievement. In each personality, life stressors congruent with the content of self-schemas lead to increased susceptibility to depression. This diathesis–stress scenario is one of the key concepts in cognitive theory of depression and is supported by systematic studies.2,4 The two personalities differ not only in mechanisms predisposing to depression but also in therapeutic techniques required when depressed. In particular, interpersonal techniques aimed at undercutting notions of total abandonment and deprivation of gratification are useful for sociotropic patients, whereas mastery techniques aimed at invalidating notions of helplessness and incompetence are useful for autonomous patients.1
On the other hand, the cognitive model postulates that negative core beliefs about self underlie maladaptive self-schemas.2,3 These core beliefs often refer to issues of survival and attachment and are expressed in brief and definite statements such as “I am helpless” and “I am unlovable”. Negative core beliefs about self form an important component of the self-concept because of their reference to basic aspects of human adaptation. These core beliefs give rise to maladaptive self-schemas in conditional, imperative and compensatory forms.
The discussion above suggests that negative core beliefs about self underlie the sociotropic and autonomous personalities and play an important role in their formation mechanisms. On the other hand, negative core beliefs about others may be implicated in the autonomous personality, as it concerns independence from others.1–3 Therefore, the present study examined the relations of sociotropy and autonomy with core beliefs about self and others. It was expected that both sociotropy and autonomy would be associated with negative core beliefs about self, and that autonomy would also be associated with those about others.
Methods
First, 332 Japanese volunteers without serious physical diseases were recruited among medical students at Yamagata University School of Medicine and medical staffs at Yamagata University Hospital and its affiliated hospitals. They were screened for psychiatric disorders by a brief interview and using a questionnaire. In the interview, six items of the Structured Clinical Interview for DSM-IV Axis I Disorders5 were used, that is, A1 for major depressive episode, A16 for manic episode, B1 for delusions, B6 for hallucinations, E2 for alcohol abuse and F68 for anxiety disorders. In the questionnaire, the volunteers were asked about the present or past history of psychiatric disorders. The subjects with psychiatric disorders (n = 9) and those with missing data (n = 2) were excluded, and the remaining 321 subjects were included for statistical analyses. Of them, 190 were males and 131 were females. Two hundred and thirty-five were medical students, and 86 were medical staffs. Their mean (SD) age was 27.5 (8.4) years, with an age range of 20–58 years. The present study was approved by the Ethics Committee of Yamagata University School of Medicine. All subjects provided written informed consent for the study.
Sociotropy and autonomy were evaluated by the Japanese version6 of the Sociotropy–Autonomy Scale (SAS; Beck et al, unpublished data). The SAS is widely used in studies to prove the diathesis–stress model of depression.2,4 Also, we have previously used this scale in studying various aspects of the two personalities, for example, their relations with the psychobiological model of personality7 and their developmental origins.8
The SAS has the sociotropy and autonomy subscales, each comprising 30 items. Representative items for the respective subscales were “It is important to be liked and approved by others” and “It is more important to be active and doing things than having close relations with other people”. Respondents indicate the percentage of the time each sentence describes them on a 4-point scale ranging from “0%” to “100%”. In the present sample, Cronbach’s alphas for the sociotropy and autonomy subscales were 0.89 and 0.84, respectively.
Core beliefs about self and others were assessed by the Japanese version9 of the Brief Core Schema Scales (BCSS).10 To date, the BCSS has been used in studies on the associations of these core beliefs with psychosis,10 prodromal psychosis,11 depression, anxiety, conduct problems and hyperactivity–inattention.12 The BCSS has the negative-self, positive-self, negative-other and positive-other subscales, each composed of six items. Representative items for the respective subscales were “I am unloved”, “I am successful”, “Other people are harsh” and “Other people are accepting”. First, respondents show whether they hold each belief, and if they hold it, they then show its strength on a 4-point scale ranging from 1 (believe it slightly) to 4 (believe it totally). In the present sample, Cronbach’s alphas for the negative-self, positive-self, negative-other and positive-other subscales were 0.83, 0.85, 0.76 and 0.88, respectively.
Statistical analyses were conducted by the linear regression analysis and the forced multiple regression analysis using SPSS Version 22 (IBM Japan, Tokyo, Japan). In the multiple regression analysis, dependent variables were subscale scores of the SAS, and independent variables were subscale scores of the BCSS, age and sex. Dummy variables were used for sex (0 = female, 1 = male). Statistical significance was set at P < 0.05.
Results
Table 1 shows the correlations among all the analyzed variables, and Table 2 shows the multiple regression analyses of subscale scores of the SAS. Sociotropy scores were correlated with negative-self scores (P < 0.001), whereas autonomy scores were correlated with positive-self scores (P < 0.01) and negative-other scores (P < 0.01).
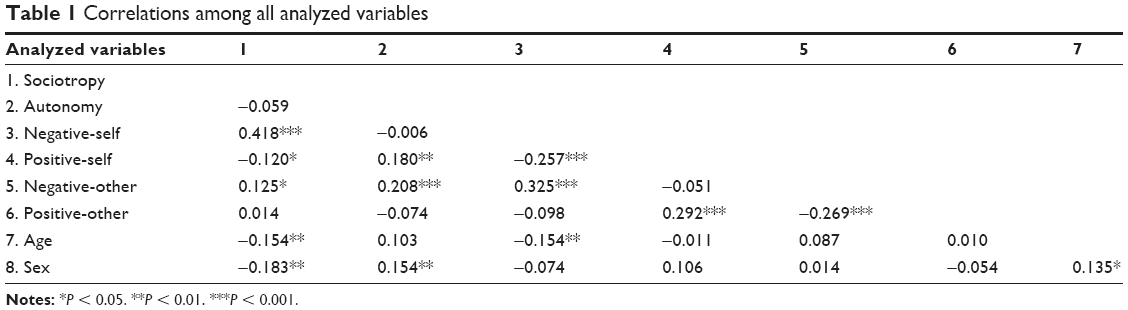 | Table 1 Correlations among all analyzed variables |
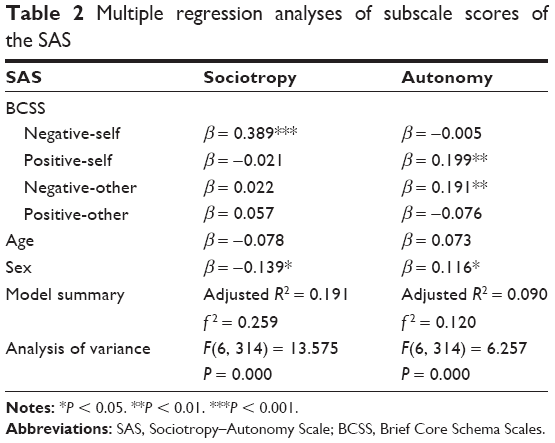 | Table 2 Multiple regression analyses of subscale scores of the SAS |
Discussion
As expected, the present study showed a significant correlation between sociotropy scores and negative-self scores. This result suggests that negative core beliefs about self underlie the sociotropic personality. Furthermore, it is suggested that these core beliefs are implicated in the formation mechanism of sociotropic self-schemas. For example, a core belief “I am unloved”10 may give rise to a self-schema “It is important to be liked and approved by others” (Beck et al, unpublished data). Therefore, our result on the sociotropic personality supports the pivotal role of negative core beliefs about self in cognitive vulnerability, one of the key concepts in the cognitive model of depression.2,3
Contrary to expectation, autonomy scores were correlated not with negative-self scores but with positive-self scores. Meanwhile, autonomous scores were correlated with negative-other scores as expected. Our hypothetical interpretation of these results in relation to the cognitive model of depression is as follows. Similar to the sociotropic person, the autonomous person originally has core beliefs of negative-self such as “I am weak”.10 These core beliefs together with core beliefs of negative-others such as “Other people are bad”10 lead to the compensatory formation of autonomous self-schemas such as “It is more important to be active and doing things than having close relations with other people” (Beck et al, unpublished data). The autonomous person attempts to obtain a positive self-regard by behaving according to these self-schemas and feeling one’s efficacy. Under no stressors or nonspecific stressors, this mechanism works, and a positive self-regard is maintained as reflected in the core beliefs of positive-self. However, under severe achievement-related stressors, this mechanism does not work anymore, and the apparently fragile positive self-concept turns into the original negative self-concept, leading to the onset of depression. Incidentally, our hypothesis is not contradictory to the description by Beck1 that the autonomous person has high levels of self-confidence and self-esteem when not depressed.
By revealing core beliefs about self and others underlying sociotropy and autonomy, this study makes some contribution to cognitive theory and therapy of depression. First of all, these core beliefs are considered to be implicated in the formation mechanisms of the two personalities. As a result, distinctive attitudes and behaviors of sociotropic and autonomous persons leading to increased susceptibility to depression are well understood by taking these core beliefs into account. This notion is also applicable to their characteristic styles in clinical settings; that is, a tendency to cling to the therapist in sociotropic patients1 is likely to be explained by core beliefs of negative-self and attempts to gain positive self-regard by external validation. Similarly, little interest in having a warm and empathetic relationship with the therapist in autonomous patients1 is likely to be ascribable to core beliefs of negative-others. Therefore, sociotropic patients may require the setting of limits or boundaries, whereas autonomous patients may require considerable efforts to form therapeutic alliance.
There are several limitations in the present study. First, our psychiatric screening might not be sufficient to exclude subjects with dysthymic disorder and minor depression, and their moods might influence the data on negative core beliefs. Second, the discussion on the autonomous personality is not supported by practical data and, therefore, may be too hypothetical. Third, the percentages explaining the variances in sociotropy and autonomy were relatively low, suggesting the necessity to search for other influencing factors such as genetic polymorphisms. Fourth, our subjects were all Japanese who may be fundamentally different from other ethnic groups, and therefore, the present results may not be directly applicable to populations with other ethnic backgrounds. Fifth, the majority of our subjects were young people who received higher education, and because of this specificity, our results should be cautiously extrapolated to general populations.
Conclusion
The present study suggests that sociotropy is correlated with core beliefs of negative-self, whereas autonomy is correlated with those of positive-self and negative-others. These marked differences in core beliefs about self and others further contrast the two personality vulnerabilities to depression.
Acknowledgments
The authors are grateful to Dr Yutaka Ono at the Ono Research Institute for kindly supplying the Japanese version of the Sociotropy–Autonomy Scale. This study was supported by funding from the Ministry of Education, Culture, Sports, Science and Technology of Japan. This had no effect on this study.
Author contributions
KO conceptualized and designed the study, collected, analyzed and interpreted the data, and drafted the manuscript. AS, YM and TS collected and analyzed the data, and modified the manuscript. All authors checked and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Beck AT. Cognitive therapy of depression: new perspectives. In: Clayton PJ, Barrett JE, editors. Treatment of Depression. Old Controversies and New Approaches. New York: Raven Press; 1983:265–290. | ||
Clark DA, Beck AT, Alford BA. Scientific Foundations of Cognitive Theory and Therapy of Depression. New York: John Wiley & Sons; 1999. | ||
Dozois DJA, Beck AT. Cognitive schemas, beliefs and assumptions. In: Dobson KS, Dozois DJA, editors. Risk Factors for Depression. Oxford: Elsevier; 2008:121–143. | ||
Mazure CM, Mciejewski PK, Jacobs SC, Bruce ML. Stressful life events interacting with cognitive/personality styles to predict late-onset major depression. Am J Geriatr Psychiatry. 2002;10:297–304. | ||
First MBH, Spitzer RL, Gibbon M, Williams JBM. Structured Clinical Interview for DSM-IV Axis I Disorders – Clinician Version. Washington: American Psychiatric Association; 1997. | ||
Izawa R. [An examination of two hypotheses for depression: personality style-stress interaction and personality style-life event congruence]. Jpn J Pers. 1997;6:1–14. Japanese [with English abstract]. | ||
Otani K, Suzuki A, Kamata M, Matsumoto Y, Shibuya N, Sadahiro R. Relationships of sociotropy and autonomy with dimensions of the Temperament and Character Inventory in healthy subjects. Compr Psychiatry. 2011;52:507–510. | ||
Otani K, Suzuki A, Kamata M, et al. Parental overprotection increases sociotropy with gender specificity in parents and recipients. J Affect Disord. 2014;136:824–827. | ||
Uchida T, Kawamura C, Mifune N, et al. [The Japanese version of the Brie Core Schema Scale for schemata concerning the self and others: identification of schema patterns and relationship with depression]. Jpn J Pers. 2012;20:143–154. Japanese [with English abstract]. | ||
Fowler D, Freeman D, Smith B, et al. The Brief Core Schema Scales (BCSS): psychometric properties and associations with paranoia and grandiosity in non-clinical and psychosis samples. Psychol Med. 2006;36:749–759. | ||
Addington J, Tran L. Using the Brief Core Schema Scales with individuals at clinical high risk of psychosis. Behav Cogn Psychother. 2009;37:227–231. | ||
Noone D, Ames C, Hassanali N, et al. A preliminary investigation of schematic beliefs and unusual experiences in children. Eur Psychiatry. 2015;30:569–575. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.