")
Back to Journals » Patient Preference and Adherence » Volume 8
Managing treatment fatigue in patients with multiple sclerosis on long-term therapy: the role of multiple sclerosis nurses
Authors Crawford A, Jewell S, Mara H, McCatty L, Pelfrey R, Ristuccia R
Received 7 May 2014
Accepted for publication 4 July 2014
Published 19 August 2014 Volume 2014:8 Pages 1093—1099
DOI https://doi.org/10.2147/PPA.S67334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Ann Crawford, Sally Jewell,* Holly Mara, Laura McCatty, Regina Pelfrey
The Lash Group; Frisco, TX, USA
*Sally Jewell is now retired
Abstract: This article discusses the many ways that nurses can address the factors that lead to treatment fatigue in patients with multiple sclerosis (MS) on long-term disease-modifying therapy, ultimately helping to preserve the patient’s health and quality of life. Patients with MS on long-term therapy may suffer from treatment fatigue and poor adherence due to a variety of different factors, including difficulties with injections, anxiety/depression, financial problems, and inaccurate beliefs about the MS disease process. Because MS nurses have regular interactions with patients, they are ideally situated to help patients cope with these and other factors that may limit adherence.
Keywords: multiple sclerosis, disease-modifying therapy, injection, nurse
Introduction
Multiple sclerosis (MS) is a chronic disease requiring long-term treatment to slow its progression.1 Disease-modifying therapies (DMTs) are available for patients with MS; however, until recently, treatment options were mainly limited to injectable and intravenous medications. With the recent introduction of oral therapies (fingolimod in 2010, teriflunomide in 2012, and dimethyl fumarate in 2013), patients are now presented with more therapy choices, including the chance to switch from an injectable to an oral DMT. While for some long-term patients the opportunity to avoid an injection by moving to one of the newer oral medications is very appealing, an injectable therapy may continue to be recommended as an efficacious treatment for many patients. In addition, patients may also be reluctant to switch to an oral treatment because of the lack of long-term safety data on the oral MS therapies to date. As such, physicians and nurses who treat long-term patients need to be aware of the factors that may contribute to their dissatisfaction with an injectable DMT.
Although the concept of treatment fatigue for long-term patients has been discussed in the literature (eg, Pyatak et al),2 no universal definition for this condition could be found. For the purposes of this paper, treatment fatigue for patients with MS is defined as a waning commitment to continue with the prescribed treatment. The loss of commitment can be due to many different sources, and each can require a unique approach to helping patients overcome the barrier to adherence.
It is important to distinguish between compliance and adherence. The World Health Organization defines adherence to long-term therapy as, “the extent to which a person’s behavior – taking medications, following a diet, and/or executing life style changes – corresponds with agreed recommendations from a health care provider”.3 In contrast, the term adherence connotes an active patient role in the medication regime.3 Compliance and adherence may be perceived as synonymous; however, the key difference between adherence and compliance is that adherence requires agreement from the patient as an active participant.3
Maintaining a commitment to long-term therapy can be extremely difficult, even for the most motivated patients. For example, a recent review of 24 studies that assessed adherence in patients with MS reported that adherence rates with injectable DMTs were as low as 49% in some cases.4 Although poor adherence rates are commonly reported in the literature, there is no universally accepted minimum rate of adherence that is considered desirable for chronic treatment. A low rate of adherence could have a significant impact on a patient’s disease course, as good adherence has been correlated with lower relapse rates and lower risk of hospital admission,5 further highlighting the need to develop techniques to prevent treatment fatigue and maintain adherence over the long-term.
Role of multiple sclerosis nurses
Most manufacturers of injectable MS DMTs offer support programs with uniquely trained nurses who provide in-home training and on-going support for patients prescribed a DMT (Table 1). These programs are generally staffed by registered nurses (RNs) who have earned the Multiple Sclerosis Certified Nurse (MSCN) certification through the International Organization of MS Nurses. Follow-up in-home patient training and education by nurses as well as a series of follow-up phone calls are usually scheduled to monitor adherence and treatment fatigue. This follow-up contact is also helpful to assist in adverse event management, to monitor proper injection technique, and to assess for indications of treatment fatigue.
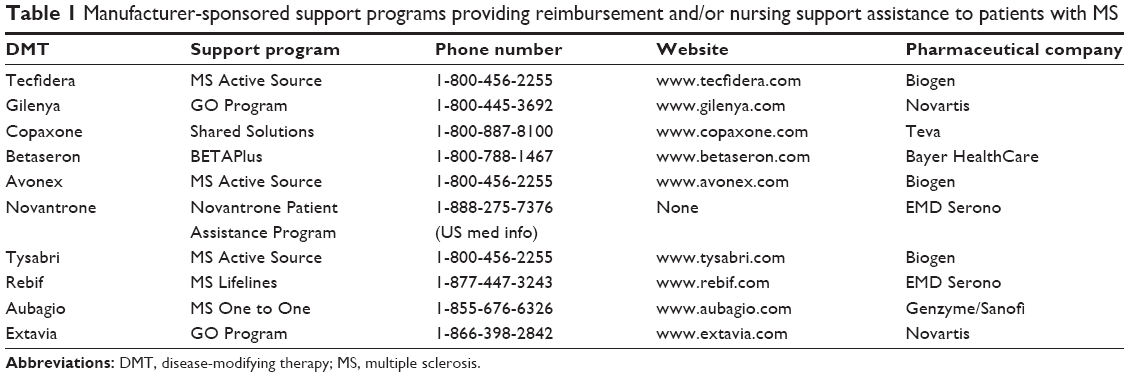 | Table 1 Manufacturer-sponsored support programs providing reimbursement and/or nursing support assistance to patients with MS |
MS nurses intervene with patients at diagnosis, providing ongoing support and education. At the initiation of treatment, nurses provide injection training along with education about realistic expectations of the effects of DMTs and tips for managing side effects. In the early phase of treatment, when side effects may be at their worst, the early support and intervention of nurses can be effective in assisting patients to remain adherent to therapy. It is important for nurses to maintain contact with patients over the long-term, as, later in treatment, the patients may show signs of treatment fatigue and feelings that they may not need to continue taking their medication as prescribed. In these cases, nurses can reinforce and educate as to the importance of remaining on therapy long-term. Patient-assistance programs that include nurse support are vital for imparting knowledge about self-injection and management of adverse events.6 Regularly reinforcing these key points can help patients adhere to complex medication administration protocols.6
MS nurses are often the main point of contact between patients and their care team on a day-to-day basis and therefore they play a pivotal role in producing positive outcomes in MS.6 The success of the pharmaceutical industry-sponsored patient support programs is indicative of the impact that properly trained nurses can have on patient education and skill development, all of which have an impact on patient adherence.6
Establishing a trusting relationship between patients and their treatment teams is critical when treating patients with MS, both at the start of therapy and over the long-term.7 Properly trained MS nurses can aid this process by instilling hope and a sense of empowerment that will help patients to achieve acceptance of their diagnosis and treatment.
Adherence to injectable therapies tends to decline over time,8 perhaps due to a loss of motivation and commitment relative to the period immediately following diagnosis. As symptoms begin to diminish and patients realize that long-term therapy is necessary, treatment fatigue may set in and adherence may falter. Most patients who discontinue therapy do so within 2 years of initiating treatment.9 For example, one observational study of patients on DMTs (n=632) found that 17% discontinued treatment over the course of 8 years and that 49% of those 17% stopped within the first 2 years.10 This decline in adherence after the 2-year mark may have occurred as treatment fatigue eroded the patients’ willingness to continue regular injections.
MS nurses can play a key role in educating, supporting, and encouraging patients with MS and their families to combat treatment fatigue. Ideally, the nurses should be part of an integrated health care team that is knowledgeable about MS and educates patients during each contact. The MS nurse also fulfills a primary role of teaching patients about their disease, symptom management, injection techniques, and health maintenance throughout the course of therapy. As such, MS nurses are positioned within the care team to directly work with patients to overcome treatment fatigue.
Factors that contribute to treatment fatigue
Treatment fatigue in patients on long-term therapy can be derived from multiple sources, and it is important for patients to understand that they may experience physical, cognitive, or psychosocial factors that can result in missed doses or therapy gaps. Adverse events associated with treatment are a common source of nonadherence. One observational study of patients on long-term therapy found that 50% of the sample had stopped taking medication due to clinical side effects.11 Common side effects leading to discontinuation by new patients on DMTs include influenza-like symptoms, depression, fatigue, and injection-site reactions (ISRs).12 Long-term patients typically discontinue treatment for perceived or clinical lack of efficacy.12 However, a resurgence of side effects, caused by a break or pause in therapy can cause the long-term patient to look for other treatment options.12
In addition to adverse events, psychosocial factors can precipitate treatment fatigue. Anxiety, fear, or ‘needle phobia’ may result in an inability to inject medication as prescribed.8,9 Depression, which affects approximately 50% of patients with MS,13 can also impact a patient’s motivation to maintain therapy.8,9,11,12 In addition to these psychological factors, financial burdens may cause patients to skip injections to make their medication last longer.4,8,9 Uninsured patients or patients unable to afford their medication copays may be forced to stop therapy for short periods of time or, in some cases, indefinitely.
In the USA, most pharmaceutical companies providing medication for the treatment of MS have programs that assist patients with affording their medications. When DMTs are prescribed for a patient, an insurance verification process is completed, and assistance is provided if needed and/or allowed. For uninsured or underinsured patients, a referral is made to various organizations or foundations that can assist in obtaining the medication.
The MS disease process itself may also lead to a decline in the patient’s willingness to comply with therapy. Cognitive issues that develope as part of the MS disease process may lead to nonadherence as patients forget to take their medication as prescribed. The multicenter observational Global Adherence Project found forgetting to take medication to be the most common reason for nonadherence.8 Sensory or motor deficits may also make self-injection difficult and sometimes impossible. DMT injections can be demanding and disruptive for patients who have cognitive deficits that increase the likelihood of forgetting to take their medication or motor impairments that reduce their manual dexterity.14,15
Multidisciplinary management of treatment fatigue
The team approach to care of patients with MS involves nurses working with others to identify sources of treatment fatigue and provide solutions to overcome these barriers (Figure 1). Using a multidisciplinary approach to patient care, MS nurses can work directly with patients through clinical practice, education, and advocacy. There are several areas in which MS nurses can directly intervene with patients who are facing treatment fatigue, including management of adverse events and overcoming psychosocial factors. Positive support and the encouragement to be self-empowered can set the stage for improved commitment to DMTs over the long-term.
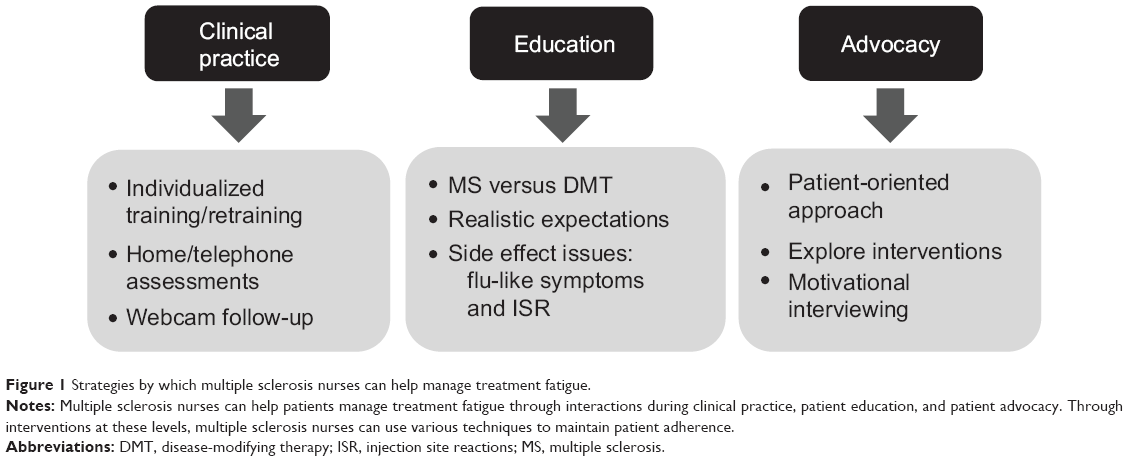 | Figure 1 Strategies by which multiple sclerosis nurses can help manage treatment fatigue. |
Using a patient-centered dialogue with active listening and open-ended questions can help MS nurses assess a patient’s commitment to sustaining treatment over the long-term. Although self-assessment questionnaires have been used to identify patients with medication adherence issues in the outpatient setting,16–18 and may predict risks for treatment fatigue, such as belief in their DMT, side effects, and depression, there is no one gold standard test to measure adherence. As an alternative, patients can be rated on a scale of 1–10, with a score of 10 showing the highest level of commitment. When interviewing patients, it is important to ask about potentially waning commitment levels in a nonthreatening manner. For example, nurses can ask, “How many doses have you missed in the past 2 weeks?” instead of “Are you taking your medication (injections) as prescribed?” Probing questions may be helpful to ascertain information about reasons for missed doses. Once high-risk patients have been identified, MS nurses can help patients address possible barriers and provide additional support and education. Consistent education and re-education should empower patients to maintain control of their treatment, potentially improving their long-term adherence.19
Managing adverse events
Continued contact between patients and MS nurses may help to prevent or resolve some potential adverse effects of treatment. Nurses have the opportunity to proactively educate patients on the techniques to mitigate or avoid possible side effects. In addition, when adverse events arise, MS nurses may be the first part of the care team to be involved. Consistent follow-up by MS nurses is essential for managing adverse events. Follow-up phone calls at key intervals can help the treatment team identify patients who are facing side effects that may limit their willingness to adhere to treatment. As demonstrated in the Success of Titration, Analgesics, and BETA Nurse Support on Acceptance rates in MS Treatment (START) study for new patients, follow-up at key intervals improved patient adherence.20 Accordingly, long-term patients can also benefit from consistent follow-up intervention from an MS nurse.
Patients can then be educated on ways to manage side effects, such as premedication with nonsteroidal anti-inflammatory drugs, dose titration, and alteration of the time of the injection.21 In addition, patients can be counseled on the importance of proper injection techniques, rotation of injection sites, and meticulous skin care, as these techniques have been shown to reduce adverse reactions at the site of the injection.21 Patients should also be educated on when to contact their health care professionals (HCPs) (ie, physicians, nurse practitioners, nurses) if they continue to have difficulties with adverse events despite using these techniques.
The START study measured the effectiveness of the combined effects of adverse event management techniques and nurse support on adherence to therapy in 96 patients with early-onset MS.20 The results showed that 78.1% of participants who received nurse support combined with dose titration and analgesics were adherent to therapy (ie, they completed >75% of scheduled injections) over the course of 12 months.20 The mean compliance rate was 84.4%.20 The authors concluded that the training and support provided by the nurses in the study provided the patients with encouragement, comfort, and confidence in the self-injection procedure, which may have contributed to the improvements in adherence that were seen.20
For patients who are still struggling with self-injections, we recommend in-person reinstruction with a nurse to improve the patient’s injection technique followed by additional phone contact. We have found that many of these patients have not retained all of the teaching points from the initial lessons and, therefore, retraining with the help of an MS nurse can improve injection technique. In our experience, often a small change in injection technique is all that is needed to successfully resolve the issues that are preventing the patient from successfully completing the injection.
Use of an autoinjector has also been shown to reduce adverse events, such as injection pain, when compared with standard syringes.22 When properly used, autoinjectors ensure that needles remain sterile and allow patients to independently inject in difficult-to-reach areas. Autoinjectors that disguise the needle so that the patient does not see it during the injection process can also be useful tools for patients with a dislike of needles or an outright needle phobia, potentially increasing the patient’s confidence that he or she can successfully complete the injection.
Some information from new patients can be transferred to manage long-term patients. Follow-up contact with most patients validates this theory. Use of an autoinjector is a strong predictor of adherence and further validated from follow-up contacts. A study of 294 patients from 82 sites in France evaluated patients who were starting their first month of therapy with interferon beta-1b using manual injections who were then switched to an autoinjector after 1 month. The percentage of patients reporting ISRs decreased significantly when autoinjectors were used (24% versus 36% using the standard injection technique [P<0.0001]).23 Another study assessed quality of life (QoL) and depression in 700 patients on long-term DMT (median disease duration 83.6 months) who were offered nurse support and the use of an autoinjector. The results showed that patients who used the autoinjector reported higher QoL and lower scores on a depression inventory than those who did not use the autoinjector (P<0.05).24 This study also found that use of an autoinjector was a strong predictor of medication adherence.25
Research has also indicated that use of a dry needle or injecting the needle deeper into the subcutaneous tissue may reduce side effects from injections, including ISRs.26 When using a dry needle, the patient includes an air bubble in the syringe prior to manual injection to minimize the leakage of medication into the skin after subcutaneous injection. One study found that ISRs were significantly reduced when patients were trained by nurses to include a 0.1 mL bubble in the syringe prior to injection.26 Although no autoinjectors were used in the study, patients anecdotally reported using the air bubble method with their autoinjectors after the study was completed.26 Some DMT-prepared syringes already have a small air bubble so that patients can take advantage of this technique.
In addition to dealing with ISRs, some patients using injectable DMTs will have skin care needs that require the care team to look beyond basic skin care methods. For example, it may be helpful for nurses to make a thorough assessment of all injection areas and inquire about daily skin care practice, including a discussion of the need for additional skin interventions. Patients administering injectable therapy on a routine basis may benefit from applying daily warm compresses, fragrance-free moisturizer, and massage to all injected areas.27 In addition, it may be necessary to use physical therapy or massage to prevent long-term complications from occurring or to restore skin to a more healthy state once these effects have already occurred.
The Graston Technique® (Graston Technique, LLC, Indianapolis, IN, USA), a patented form of instrument-assisted soft-tissue mobilization originally used for treatment of injury, surgical scarring, and chronic pain syndromes, enables specially trained providers to effectively break down scar tissue and fascial restrictions and therefore may be helpful for patients suffering from side effects of long-term needle use (Figure 2).28 This technique utilizes specially designed stainless steel instruments (GT Instruments; Indianapolis, IN) to specifically detect and treat areas exhibiting soft-tissue fibrosis or chronic inflammation.28 This therapy can be effective in a relatively short time frame, with patients usually receiving two treatments per week over 4–5 weeks.28 Further studies need be done to evaluate this technique for those with injection area issues.
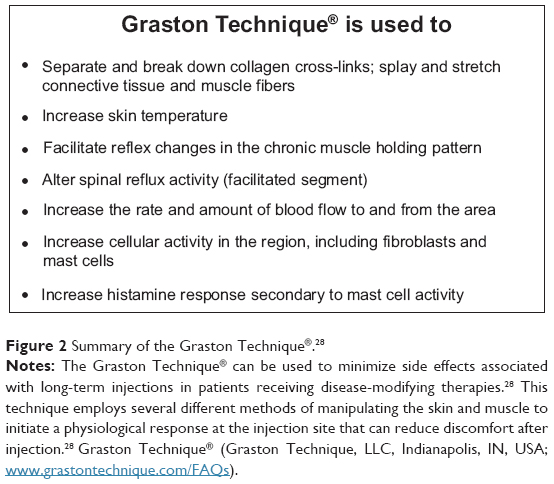 | Figure 2 Summary of the Graston Technique®.28 |
Other techniques for overcoming treatment fatigue
Motivational interviewing helps HCPs and patients explore the causes of diminishing commitment levels and to re-establish goals of treatment, empowering patients to take ownership of their health.29 When they do not feel in control, patient commitment can wane, leading to treatment fatigue. Motivational interviewing techniques provide a framework for conversing with patients that is based on active listening and a non-confrontational approach to explore the potential disconnect between a patient’s beliefs and behavior.30 Through this technique, HCPs can actively support patients who express a willingness to change their behavior, which has been shown to improve care for patients with chronic diseases.30 This approach allows for patient autonomy and demonstrates respect more so than a one-way conversation on why the patient must change his or her behavior. Like anything new, this technique improves with practice. For further information, see http://www.motivationalinterview.org for instructional videos and training opportunities.
For patients who have been on treatment for many years, a misunderstanding of the chronic nature of MS and the need for continual, long-term therapy or a belief that medication is no longer needed may precipitate treatment fatigue. A patient who states, “I’m symptom free, I haven’t had a relapse in …” may have unrealistic beliefs about the disease course and/or the treatment of MS. In other instances, patients may perceive a lack of efficacy when disease activity is still present despite long-term DMT and therefore have difficulty committing to a prescribed injection regime. Consequently, at diagnosis and periodically during the course of treatment, nurses should help patients with MS understand that DMTs will not cure the disease and that the onset of new symptoms or lesions may not be indicative of treatment failure.
Access to modern media can have a significant impact on a patient’s health beliefs and positively or negatively affect his or her ability to sustain long-term therapy. Patients often turn to the Internet, blogs, online support communities, and other media outlets for information or advice. Alternative therapies (diet, herbal, alternative medicine) may also appeal to some patients, as a claim of immediate improvement of symptoms or feelings of well-being can feel like a panacea for patients with MS who are struggling with injectable therapy. MS nurses should help patients explore these options by directing them to reliable sources that will provide medically accurate and evidence-based information.
For patients dealing with psychosocial factors, MS nurses can help patients recognize that feelings of depression or anxiety may occur and refer patients to their physicians when intervention is required. The occurrence of depression in patients with MS should be managed similarly to that of other patients (ie, through medication and/or therapy).21 Cognitive behavioral therapy has also been demonstrated to be effective for reducing symptoms of distress in patients with MS.31
In our experience, meditation, music, and guided imagery are some strategies that can be explored with patients experiencing needle anxiety/phobia. Helping patients to pair rewarding personal activities with the injection process may make the experience less aversive. For example, pairing a soothing stimulus during injection, such as a favorite piece of music; a warm, relaxing shower; or a favorite cup of tea, may help to relieve some of the anxiety that surrounds the injection process.
Disease-related cognitive issues can also be addressed with the involvement of the comprehensive treatment team as well as the family, as loved ones are often the first to recognize cognitive changes. Cognitive testing may identify subsequent strategies to overcome deficits in memory and executive functioning. To avoid missed doses, MS nurses may encourage patients to use medication reminders. Calendars, emails, electronic reminders, and smartphone applications are all tools that help patients with cognitive impairments track medication administration. Although there may also be electronic devices under development that include a reminder function, at the time of this writing none of these devices are currently available in the USA.
In many cases, nurse contact with patients will identify financial difficulties that may limit access to medication. Nurses can therefore make the necessary referrals to connect patients with available support resources. It is important to remind patients to call their HCPs or support programs if affordability issues arise, because most pharmaceutical companies, as well as many nonprofit foundations, offer financial assistance.
While many patients develop treatment fatigue and ask for drug holidays, breaks from DMT can cause a worsening of the disease process. In one study, gaps in treatment were correlated with the incidence of severe MS relapse.32 Patients who were off DMT for >90 days were twice as likely to have a severe relapse as patients with shorter periods of no medication for MS.32
Summary
Treatment fatigue can affect adherence to long-term therapy and impact disease outcomes and QoL for patients with MS. MS nurses should assist patients in recognizing and combating the sources of treatment fatigue. The ideas presented in this paper are intended to provide techniques that nurses can use to work with their patients to resolve potential barriers to maintaining long-term adherence. As has been said by C Everett Koop, the former Surgeon General of the USA, “Drugs don’t work in patients who don’t take them.”
Acknowledgments
The authors thank Robert C Ristuccia, PhD (Precept Medical Communications, Warren, NJ, USA) for editorial assistance, funded by Bayer HealthCare Pharmaceuticals, in preparation of this manuscript.
Disclosure
A Crawford, L McCatty, and R Pelfrey are employees of the Lash Group assigned to a Bayer HealthCare contract. S Jewell is a paid consultant for Bayer HealthCare Pharmaceuticals. H Mara is a former Lash Group employee.
References
Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372(9648): 1502–1517. | ||
Pyatak EA, Florindez D, Weigensberg MJ. Adherence decision making in the everyday lives of emerging adults with type 1 diabetes. Patient Prefer Adherence. 2013;7:709–718. | ||
Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. | ||
Menzin J, Caon C, Nichols C, White LA, Friedman M, Pill MW. Narrative review of the literature on adherence to disease-modifying therapies among patients with multiple sclerosis. J Manag Care Pharm. 2013;19(1 Suppl A):S24–S40. | ||
Steinberg SC, Faris RJ, Chang CF, Chan A, Tankersley MA. Impact of adherence to interferons in the treatment of multiple sclerosis: a non-experimental, retrospective, cohort study. Clin Drug Investig. 2010; 30(2):89–100. | ||
Halper J. The evolving role of the nurse in the treatment of multiple sclerosis. J Neurosci Nursing. 2009;41(4):E1–E13. | ||
Koudriavtseva T, Onesti E, Pestalozza IF, Sperduti I, Jandolo B. The importance of physician-patient relationship for improvement of adherence to long-term therapy: data of survey in a cohort of multiple sclerosis patients with mild and moderate disability. Neurol Sci. 2012;33(3): 575–584. | ||
Devonshire V, Lapierre Y, Macdonell R, et al; GAP Study Group. The Global Adherence Project (GAP): a multicenter observational study on adherence to disease-modifying therapies in patients with relapsing-remitting multiple sclerosis. Eur J Neurol. 2011;18(1):69–77. | ||
Costello K, Kennedy P, Scanzillo J. Recognizing nonadherence in patients with multiple sclerosis and maintaining treatment adherence in the long term. Medscape J Med. 2008;10(9):225. | ||
Rio J, Porcel J, Téllez N, et al. Factors related with treatment adherence to interferon beta and glatiramer acetate therapy in multiple sclerosis. Mult Scler. 2005;11(3):306–309. | ||
Ruggieri RM, Settipani N, Viviano L, et al. Long-term interferon-beta treatment for multiple sclerosis. Neurol Sci. 2003;24(5):361–364. | ||
O’Rourke KE, Hutchinson M. Stopping beta-interferon therapy in multiple sclerosis: an analysis of stopping patterns. Mult Scler. 2005; 11(1):46–50. | ||
Patten SB. Antidepressant treatment for major depression in multiple sclerosis: the evolving efficacy literature. Int J MS Care. 2009;11(4): 174–179. | ||
Deleu D, Alsharoqi I, Al Jumah MA, et al. Will new injection devices for interferon β-1a s.c. affect treatment adherence in patients with multiple sclerosis? An expert opinion in the Middle East. Int J Neurosci. 2011; 121(4):171–175. | ||
Mohr DC, Boudewyn AC, Likosky W, Levine E, Goodkin DE. Injectable medication for the treatment of multiple sclerosis: the influence of self-efficacy expectations and injection anxiety on adherence and ability to self-inject. Ann Behav Med. 2001;23(2):125–132. | ||
Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). 2008;10(5):348–354. | ||
Morisky DE, Malotte CK, Choi P, et al. A patient education program to improve adherence rates with antituberculosis drug regimens. Health Educ Q. 1990;17(3):253–267. | ||
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986; 24(1):67–74. | ||
Brandes DW, Callender T, Lathi E, O’Leary S. A review of disease-modifying therapies for MS: maximizing adherence and minimizing adverse events. Curr Med Res Opin. 2009;25(1):77–92. | ||
Dhib-Jalbut S, Markowitz C, Patel P, Boateng F, Rametta M; START Study Group. The combined effect of nursing support and adverse event mitigation on adherence to interferon beta-1b therapy in early multiple sclerosis: the START study. Int J MS Care. 2012;14(4): 198–208. | ||
Langer-Gould A, Moses HH, Murray TJ. Strategies for managing the side effects of treatments for multiple sclerosis. Neurology. 2004;63(11 Suppl 5):S35–S41. | ||
Phillips JT, Fox E, Grainger W, Tuccillo D, Liu S, Deykin A. An open-label, multicenter study to evaluate the safe and effective use of the single-use autoinjector with an Avonex® prefilled syringe in multiple sclerosis subjects. BMC Neurol. 2011;11:126. | ||
Brochet B, Lemaire G, Beddiaf A; l’Epicure study group. [Reduction of injection site reactions in multiple sclerosis (MS) patients newly started on interferon beta 1b therapy with two different devices]. Rev Neurol (Paris). 2006;162(6–7):735–740. French [with English abstract]. | ||
Pozzilli C, Schweikert B, Ecari U, Oentrich W, Bugge JP. Quality of life and depression in multiple sclerosis patients: longitudinal results of the BetaPlus study. J Neurol. 2012;259(11):2319–2328. | ||
Pozzilli C, Schweikert B, Ecari U, Oentrich W; BetaPlus Study Group. Supportive strategies to improve adherence to IFN β-1b in multiple sclerosis – results of the βPlus observational cohort study. J Neurol Sci. 2011;307(1–2):120–126. | ||
Moore LA, Kaufman MD, Algozzine R, Irish N, Martin M, Posey CR. Adherence to therapy: using an evidence-based protocol. Rehabil Nurs. 2007;32(6):227–232. | ||
Jolly H, Simpson K, Bishop B, et al. Impact of warm compresses on local injection-site reactions with self-administered glatiramer acetate. J Neurosci Nurs. 2008;40(4):232–239. | ||
Hammer WI. Graston technique®: a contemporary instrument assisted mobilization method for the evaluation and treatment of soft tissue lesions. In: Schliep R, Findley TW, Chaitow L, Huijing P, editors. Fascia: the Tensional Network of the Human Body: the Science and Clinical Applications in Manual and Movement Therapy. 1st ed. Philadelphia, PA: Elsevier Ltd; 2012:391–396. | ||
Miller NH. Motivational interviewing as a prelude to coaching in healthcare settings. J Cardiovasc Nurs. 2010;25(3):247–251. | ||
Duff AJ, Latchford GJ. Motivational interviewing for adherence problems in cystic fibrosis; evaluation of training healthcare professionals. J Clin Med Res. 2013;5(6):475–480. | ||
Moss-Morris R, Dennison L, Landau S, Yardley L, Silber E, Chalder T. A randomized controlled trial of cognitive behavioral therapy (CBT) for adjusting to multiple sclerosis (the saMS trial): does CBT work and for whom does it work? J Consult Clin Psychol. 2013;81(2): 251–262. | ||
Fox RJ, Salter AR, Tyry T, et al. Treatment discontinuation and disease progression with injectable disease-modifying therapies: findings from the north american research committee on multiple sclerosis database. Int J MS Care. 2013;15(4):194–201. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.