")
Back to Journals » Cancer Management and Research » Volume 10
Managing the cancer–work interface: the effect of cancer survivorship on unemployment
Authors Tracy JK , Falk D , Thompsom RJ, Scheindlin L, Adetunji F, Swanberg JE
Received 18 July 2018
Accepted for publication 24 October 2018
Published 28 November 2018 Volume 2018:10 Pages 6479—6487
DOI https://doi.org/10.2147/CMAR.S180649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Beicheng Sun
J Kathleen Tracy,1,2 Derek Falk,1,3 Rebecca J Thompson,4 Lily Scheindlin,1 Fiyinfolu Adetunji,1 Jennifer E Swanberg1–3,5
1Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, MD, USA; 2University of Maryland Greenebaum Comprehensive Cancer Center, University of Maryland Medical Center, Baltimore, MD, USA; 3University of Maryland School of Social Work, Baltimore, MD, USA; 4Management Department, Gettysburg College, Gettysburg, PA, USA; 5Department of Health Policy and Management, School of Professional Studies, Providence College, Providence, RI, USA
Objective: This study assessed differences in employment outcomes among cancer survivors using data from a nationally representative sample.
Methods: The 2011 Medical Expenditure Panel Survey (MEPS) data and the 2011 MEPS Experiences with Cancer Survivorship Supplement representing 3,360,465 people in the US population were analyzed to evaluate factors associated with unemployment among cancer survivors during the 5 years following diagnosis and treatment. The sample included adults 1) diagnosed with cancer within 5 years prior to survey completion and 2) engaged in paid employment since diagnosis. Individuals diagnosed with nonmelanoma skin cancer (n=33) were excluded from analyses.
Results: Data of 221 cancer survivors were used to identify factors associated with employment status at the time respondents were employed (n=155) vs unemployed (n=66). Results of bivariate analyses indicated that unemployed survivors were older, more likely to be women, more likely to be uninsured at the time of cancer diagnosis, and to report lower incomes than cancer survivors who continue to be employed. Unemployed survivors were more likely than employed survivors to have had anxiety about being forced to retire or quit early when they were employed because of cancer and to report cancer-related interference with physical and mental aspects of their job tasks; unemployed survivors also took less paid time off and were less likely to change to a flexible job schedule when they were employed. In multiple logistic regression analyses, worry about being forced to retire (protective), worry that cancer recurrence will interfere with home or work responsibilities (risk), and change to a flexible work schedule (risk) following cancer diagnosis were associated with unemployment after controlling for demographic differences between employed and unemployed cancer survivors.
Conclusion: Findings of this study highlight the extent to which the challenges of managing the cancer–work interface create challenges to employment among cancer survivors and may lead to long-term unemployment among cancer survivors. Future studies should evaluate the strategies that the survivors could use to manage the cancer–work interface during cancer treatment to attain medical, psychological, social, and employment outcomes.
Keywords: work, employment, cancer-work-management, survivor
Introduction
With improvements in cancer screening and early detection, cancer incidence rates in the last decade have stabilized.1 Furthermore, the 5-year survival across cancers is nearly 70%,1 increasing the number of cancer survivors. It is estimated that in 2014, ~14.5 million adults were cancer survivors; the number is expected to increase to 19 million by 2024.2 More than 70% of the incident cancers are diagnosed in adults between the age of 20 and 74 years, prime employment years. As a result, many cancer survivors are employed at the time of cancer diagnosis and are likely to continue to work or return to work (RTW) post treatment. Identifying factors associated with unemployment among cancer survivors is both a quality of life issue for cancer survivors and a public health issue.
Several factors have been linked to changes in employment following cancer diagnosis. These include type of cancer,3,4 type of treatment received5 with chemotherapy associated with greater disruption to employment,6 and type of work having more negative impacts on RTW.3 A meta-analysis by de Boer et al4 focused on comparison of cancer survivors and healthy controls with respect to employment. This systematic review noted that cancer survivorship is associated with higher rates of unemployment compared to healthy controls. Furthermore, US cancer survivors were nearly 1.5 times more likely to become unemployed than their European counterparts. More recently, a systematic review by Mehnert7 noted that 63.5% of the cancer survivors RTW following diagnosis and treatment. Factors associated with RTW or being employed included employer accommodations, flexible work arrangements, rehabilitation support services, younger age, higher education, male gender, fewer physical symptoms, and less time off. Similar to the results of the study by de Boer et al, Mehnert noted the increased risk of unemployment that cancer survivors experience compared to healthy controls.
Flexible and supportive work environments have been shown to enable success in the workplace throughout cancer treatment and survival.8 Existing research suggests that older age, being non-white, having lower education levels, living in a nonmetropolitan area, and working in a blue-collar job with public or no health insurance contribute to survivors not working or severely altering their employment.8–11
Much of the existing literature studies have compared employment issues of cancer survivors with those of noncancer survivors.11 A limited number of studies have examined the employment situations of people actively receiving treatment12 and workplace supports for those in treatment, but not for survivors years later.13 Few studies have focused on factors that determine which survivors remain employed compared with those who do not. The purpose of this study was to assess factors associated with unemployment 5 years postdiagnosis among cancer survivors using data from the national Medical Expenditure Panel survey (MEPS) and the Experiences with Cancer Supplement.
Methods
Data
Data from the 2011 MEPS and the 2011 MEPS Experiences with Cancer Survivorship Supplement were analyzed to identify factors associated with unemployment among cancer survivors. MEPS, conducted annually by the Agency for Healthcare Research and Quality (AHRQ), is a nationally representative survey that assesses healthcare costs and usage based on the data from families, individuals, medical providers, and employers. In 2011, AHRQ included the Experiences with Cancer Survivorship Supplement, which took the form of a self-administered questionnaire – the Cancer Self-Administered Questionnaire (CSAQ). The 2011 MEPS selection process oversampled household members who reported a previous cancer diagnosis, and each person who reported that he or she had a previous cancer diagnosis was asked to complete the CSAQ. Only adults aged 18+ were included in the supplement that queried topics including the burden of cancer, access to health care, employment patterns, job and workplace characteristics, and work productivity. MEPS and CSAQ data were accessed and downloaded directly from the AHRQ-MEPS website.14 The institutional review board of the University of Maryland, Baltimore, determined this secondary analysis to be nonhuman subject research.
Sample inclusion criteria consisted of adult (aged >18) respondents who 1) were diagnosed with cancer within 5 years prior to survey completion; 2) engaged in paid employment at some time since diagnosis; and 3) completed the CSAQ. Nonmelanoma skin cancer survivors were excluded to maintain consistency with other cancer survivorship studies. The final analytic sample (N=221) consisted of individuals who were employed (n=155) and unemployed (n=66) respondents at the time of the survey (Figure 1).
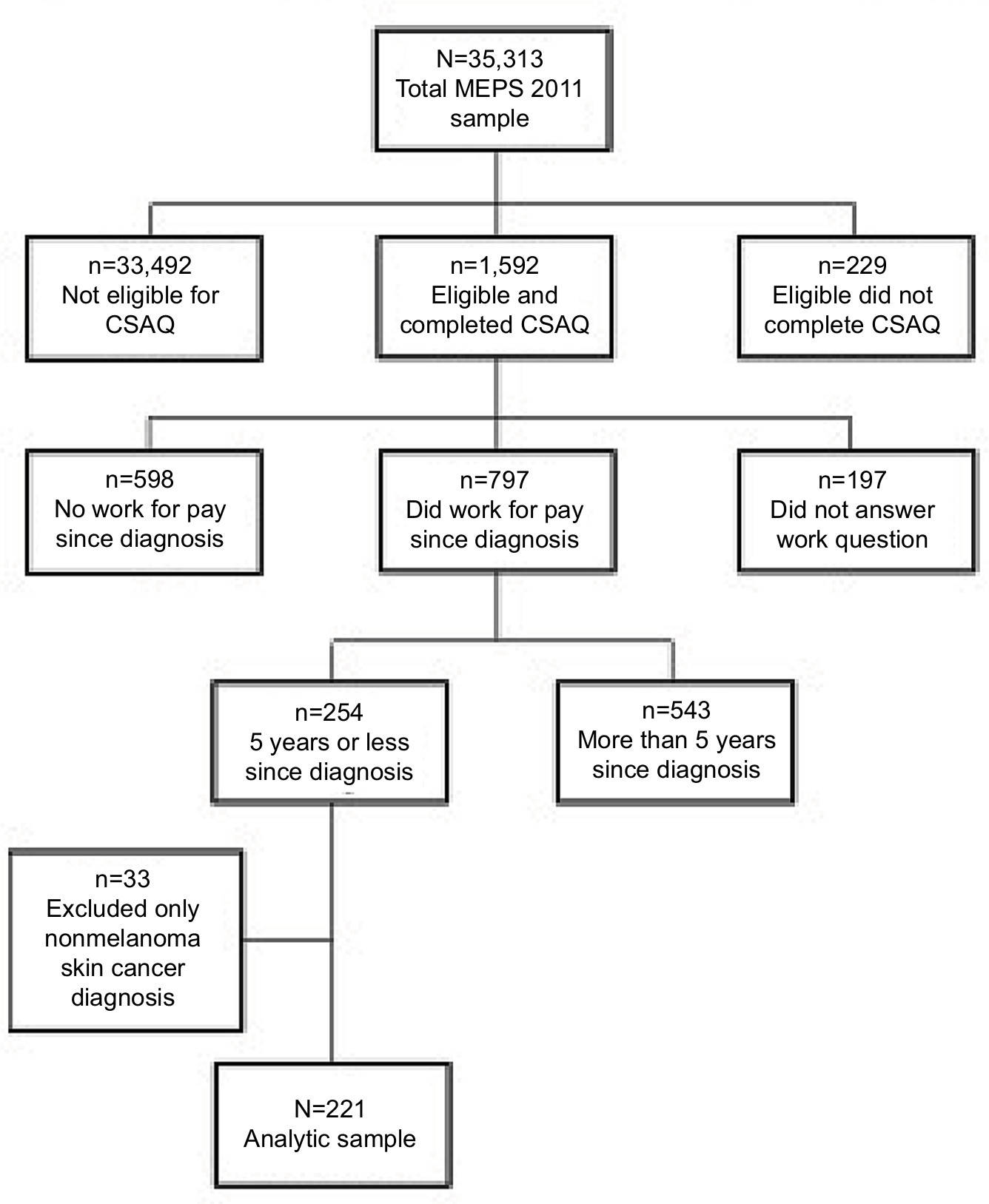 | Figure 1 Sampling flow chart of cancer survivor subsample generated from the 2011 MEPS of the CSAQ (N=221). Abbreviations: CSAQ, Cancer Self-Administered Questionnaire; MEPS, Medical Expenditure Panel Survey. |
Weighting
The 2011 MEPS data include sampling weights to account for survey nonresponse and to adjust the population control totals to the Current Population Survey for that year. The unweighted responses consisted of 35,313 household members across 2,052 variables with a response rate of 54.9%. The total 2011 MEPS survey included positive person-level weights for 33,622 respondents and positive family level weights for 13,449 families. The 1,419 CSAQ respondents also received separate sampling weights, which was used in the present analysis, totaling 20,105,356 with a pooled unweighted average response rate of 90.0%. This sum estimates the number of adults in the USA who reported a cancer diagnosis or cancer treatment during adulthood.
Measures
Demographic characteristics
Demographic variables included age, sex, educational attainment, race/ethnicity, marital status, and income. Total individual and family annual incomes were reported for all respondents, with missing data imputed using logical editing and weighted, sequential hot decks, as well as top coding to preserve confidentiality. Sources of income included the following: interest, business, dividends, refunds, retirement, alimony, sales, trust, social security, unemployment, workers’ compensation, veterans’ income, cash, child support, public assistance, and any other form. Family income as a percentage of the poverty line was categorized as either low income (1=199% of the federal poverty level or less) or middle and high income (0=200% of the federal poverty level or higher).
Insurance coverage
CSAQ respondents indicated if they were covered by insurance that paid for all or part of their medical care, tests, or cancer treatment at the time of diagnosis. These responses were dichotomized as either not insured (1= no) or insured (0= yes).
Cancer characteristics
Cancer characteristic variables included the type of cancer and current treatment status. Current treatment status was defined as those who were actively undergoing cancer treatment at the time of CSAQ administration (1=yes, 0=no). The three most common cancer diagnoses along with the respondents’ current treatment status were also extracted from the CSAQ.
Employment status
Employment status was based on a single item and was coded to reflect unemployed (1=yes, 0=no). Those who were employed at the time of survey or had a job to return to were coded as 0 (ie, not unemployed); those who were employed during the reference period but not employed at the time of survey or who were not employed with no job to return to at the time of the survey were coded as 1 (ie, unemployed). This allowed logistic regressions to estimate the odds of cancer survivors being unemployed at the time of the survey.
Cancer-related psychological job distress
Two items surveyed respondents’ anxiety related to the cancer–work interface. First, respondents were asked if they were worried about being forced to retire or quit early due to cancer-related effects on their health. Next, respondents were asked if they were worried about fulfilling home or job responsibilities if their cancer returned or got worse. Both items were coded dichotomously (1=yes, 0=no).
Cancer-related interference with job tasks
Two items assessed how a cancer diagnosis, its treatment, or the effects of the treatment interfered with job tasks. The first asked if cancer affected the respondent’s ability to perform any physical tasks required at work, whereas the second probed if cancer interfered with any mental tasks required at work. Responses were also coded dichotomously (1=yes, 0=no).
Employment characteristics
Employment characteristics referred to the job that respondents had since their cancer diagnosis and were described in two categories as follows: work leave and workplace supports. Two items assessed respondent’s leave from work due to their cancer diagnosis. Respondents indicated if they took extended paid time off from work (no, yes), and subsequently if they took extended unpaid time off from work (no, yes); to aid in interpretation of odds of unemployment, these items were recoded (1=no, 0=yes). The following three questions identified workplace supports: 1) changing to a flexible schedule; 2) to a less demanding job; or 3) from a full to part time job; these were coded dichotomously as either did not change (0=no) or changed (1=yes).
Statistical analyses
All analyses accounted for weighting using complex sample statistical design. Independent samples Student’s t-tests compared employed vs unemployed cancer survivors for age, whereas differences in sex, income level, health insurance status, major cancer diagnoses, current cancer treatment status, mental and physical work interference, paid and unpaid time off, and changes in work conditions were compared by employment status using Chi-square statistics. Logistic regression analyses were used to calculate the odds of being unemployed in the 5 years since the respondents’ cancer diagnosis using age, sex, income, and health insurance status as control variables. Cancer-related psychological job distress, cancer interference with job tasks (mental and physical), leave, and changes in schedules and job status were assessed in a series of stepwise logistic regression models. All analyses were conducted using SPSS software, version 24 (IBM Corporation, Armonk, NY, USA). Findings were considered statistically significant using two-tailed P-values of <0.05.
Results
The analytic sample for these analyses included 221 respondents from a nationally representative sample representing 3,360,465 people in the US population; 155 respondents were employed at the time of survey completion (representing 2,473,516 individuals or 73.6% of the population), whereas 66 respondents (representing 886,948 or 26.4% of the population) were unemployed at the time of survey completion. Table 1 illustrates the weighted sample characteristics and compares employed and unemployed cancer survivors using Student’s t-test and chi-square statistics. On average, cancer survivors were aged ~57 years. Unemployed survivors tended to be older than employed survivors with an average age of 62 years. A higher proportion of women were unemployed. Most respondents (93.3%) had insurance at the time of their diagnosis but those who were unemployed had a higher proportion of being uninsured (13% vs 1% of employed survivors). The most common cancer diagnoses and cancer treatment status were similar among employed and unemployed respondents with no significant differences observed between these groups.
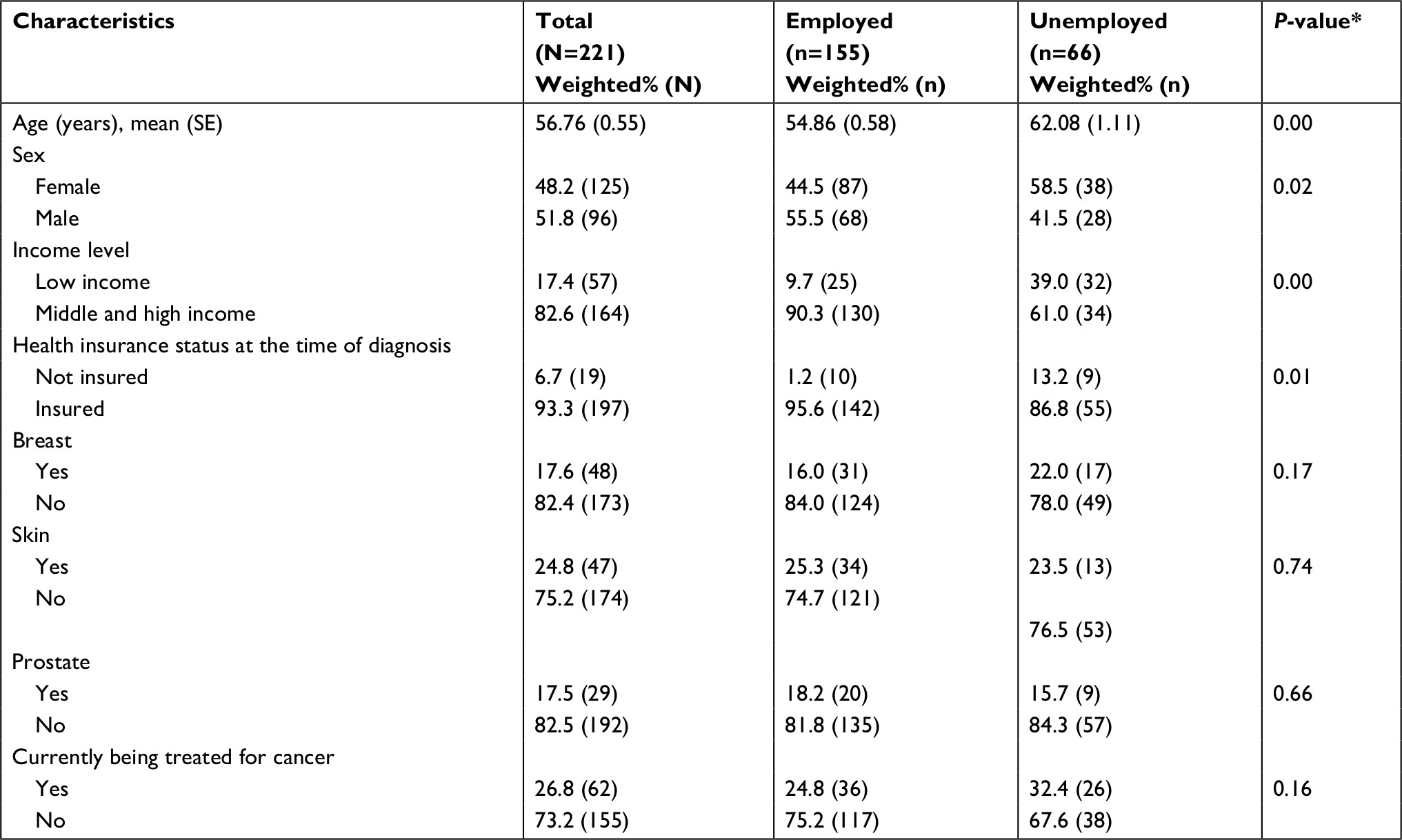 | Table 1 Demographic, financial, and cancer characteristics of employed and unemployed cancer survivors (N=221) Note: *Chi-square for all analyses except age where a Student’s t-test was used. |
Figure 2 presents results of bivariate comparisons between employed and unemployed for cancer- and work-related variables. A significantly greater proportion of unemployed cancer survivors worried about being forced to retire or quit early due to the effects of cancer. However, staying at their job due to health insurance and worrying about fulfilling home or job responsibilities if cancer returned or got worse were similar for employed and unemployed cancer survivors. Unemployed respondents reported higher rates of cancer-related interference with mental and physical job tasks compared to employed respondents. Unemployed cancer survivors were significantly less likely to have taken paid time off due to cancer diagnosis and treatment; no significant differences were noted between employed and unemployed with respect to unpaid time off. The majority of cancer survivors did not change to a flexible schedule; significantly fewer unemployed respondents changed their work schedule compared to employed respondents, 4% vs 16%, respectively. Few respondents changed to a less demanding job whether they remained employed or unemployed. Finally, unemployed cancer survivors changed from a full time to part time job at a slightly higher proportion than their employed counterparts.
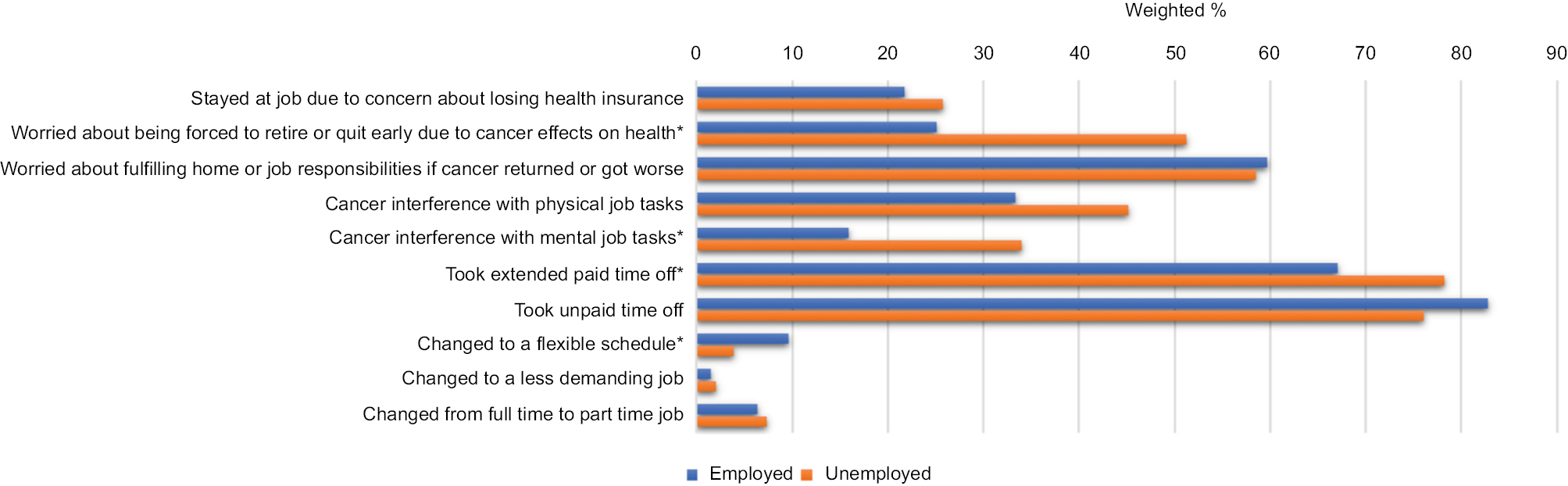 | Figure 2 Cancer- and work-related differences between employed and unemployed cancer survivors. Notes: *A significant difference of proportions using a chi-squared test. |
Table 2 presents data of a series of multiple logistic regression models. Significant variables identified from bivariate analyses were analyzed in separate models controlling for age, sex, income level, and health insurance status that were identified as significant correlates of employment status. Finally, a full model considered the significant independent variables from each of the previous regression models. Model 1 examined the association between employment status and cancer-related psychological distress. Those respondents who worried about being forced to retire or quit early due to their cancer had lower odds of being unemployed, and respondents who acknowledged anxiety about fulfilling home or work responsibilities if their cancer returned or got worse were nearly three times more likely to be unemployed. Model 2 evaluated the association between employment status and cancer-related interference with physical job tasks. Cancer interference with physical job tasks was not associated with employment status in Model 2 after controlling for demographics. Model 3 evaluated the association between employment and cancer-related interference with mental job tasks and revealed that, in contrast to Model 2, cancer interference with mental job tasks increased odds of unemployment by more than two times. Model 4 evaluated the correlation between employment status and employment characteristics. Those who changed to a flexible schedule were 4.46 times more likely to be unemployed. Model 5 collectively evaluated the associations between unemployment and Models 1–4 construct to determine the most parsimonious explanatory model of factors associated with unemployment among cancer survivors. Cancer-related psychological distress and employment characteristics remained significant in Model 5. Cancer interference with mental job tasks was no longer significant in the final model as the other variables accounted for a larger share of the variance in the model.
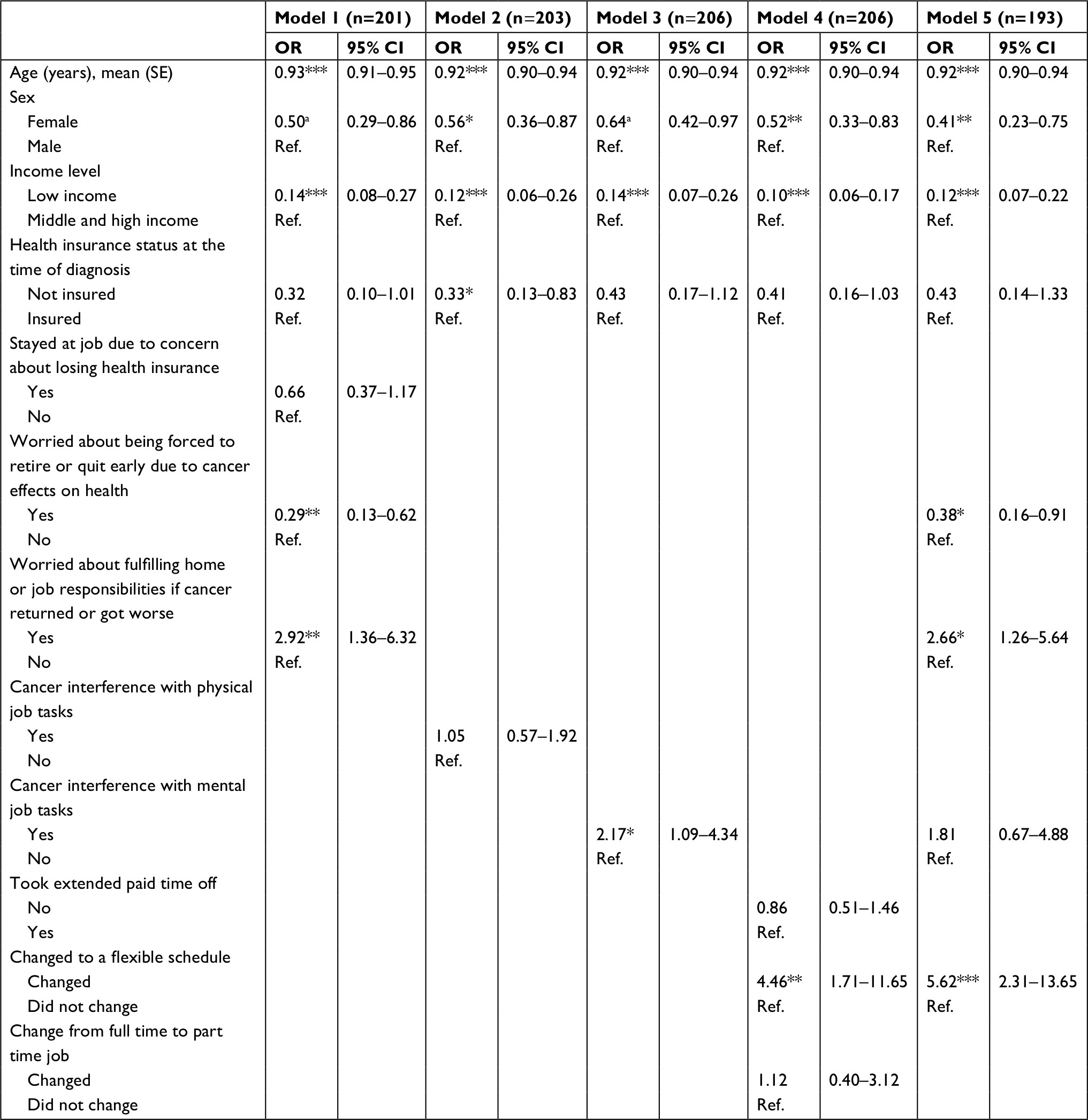 | Table 2 Odds of unemployment status for cancer survivors at 5 years postdiagnosis Notes: *P<0.05, **P<0.01, and ***P<0.001. Abbreviation: Ref., reference. |
Discussion
This study evaluated factors associated with unemployment among cancer survivors using data from the MEPS and associated CSAQ, a nationally representative US survey. The objective was to identify the factors that increase the risk of unemployment within a nationally representative sample of cancer survivors. Major findings from the analyses reported here suggest that cancer-related psychological job distress, cancer-related interference with mental job tasks, and lack of workplace resources and flexibility were related to long-term unemployment among cancer survivors. These findings highlight key psychosocial and employment factors that contribute to disparities in employment outcomes among cancer survivors. These results also provide support for the need to develop evidence-based interventions to address how these factors contribute to unemployment.
Reviews of the literature on cancer and work have previously indicated that sociodemographic factors influence cancer survivors’ ability to RTW.15 Results reported here suggest that not only do sociodemographic factors influence RTW but also survivors’ success at remaining employed following RTW. Our findings underscore the importance of supporting cancer survivors past the RTW milestone in order to maximize success for remaining employed. Furthermore, it is essential to identify the types of support that are most beneficial for remaining employed after RTW, and which stakeholders (oncology care team, social workers, employers, and family) are best positioned to provide additional supports for survivors’ employment success.
A greater proportion of unemployed survivors reported cancer-related psychological job distress. Specifically, unemployed survivors were more likely to worry about being forced to retire or quit early due to cancer while employed than their employed counterparts. Survivors who acknowledged anxiety about fulfilling home or work responsibilities if their cancer returned or got worse were nearly three times more likely to be unemployed. These data highlight the challenges of managing the impact of cancer on home and work quality of life and the negative effect this type of distress may have on employment among survivors. It is possible that employed cancer survivors those who experience physical or psychological effects of cancer may worry more about being forced to retire and fulfilling work and home responsibilities than cancer survivors with less adverse effects.7 Presence of job-related psychological job distress may be correlated with limitations of activities of daily living, work ability or psychological dysfunction and serve as a proxy measure for the said dysfunctions that result in unemployment.16–18 Additionally, following Mehnert’s model of factors related to employment outcomes among cancer survivors,7 the presence of psychological distress may mediate the relationship between cancer and work, such that those who experience job-related psychological distress may be more prone to unemployment.
Unemployed survivors reported cancer-related interference with both physical and mental aspects of their job tasks. Moskowitz et al19 noted that functional impairment among cancer survivors is a stronger predictor of work ability than health and well-being or residual symptoms. The current findings, however, indicate that only cancer-related interference with mental job tasks was related to unemployment after adjustment for demographic differences between employed and unemployed. This contrasts with previous studies that have shown that physically demanding jobs affect cancer survivors’ ability to work. Alternatively, it may also indicate that for survivors who RTW, challenges related to mental aspects of jobs are more difficult to overcome and manage. Cancer-related interference with mental job tasks may reflect a unique challenge for managing the cancer–work interface. Moskowitz et al noted previously that functional limitation – cognition being among the most important across all job types and categories, perhaps – is a stronger predictor of work ability than actual physical health.19,20 Our findings support the importance of cancer-related functional limitations, especially mental (ie, cognitive aspects) for positive employment outcomes.16
Unemployed cancer survivors were significantly less likely than employed survivors to have taken paid time off due to cancer diagnosis and were less likely to have switched to a flexible job schedule during or following cancer treatment. These findings raise the possibility that cancer survivors without access to paid time off or who have rigid schedules may eventually become unemployed due to the lack of workplace accommodations or available resources to help survivors manage the cancer–work interface during treatment or transition back to work after treatment.
Limitations
Despite the value of examining factors associated with unemployment in cancer survivors in a large nationally representative sample, this study had several limitations. First, the response rate to the MEPS Experiences with Cancer survey was 49.4%; therefore, the eligible sample might not be fully generalizable to the population of US cancer survivors. Our strategy for maximizing generalizability was to apply sample weights to all analyses, which included an adjustment for nonresponse. Second, the MEPS and CSAQ data are based on self-report and are therefore subject to recall bias. CSAQ items required respondents to recall feelings and decisions made over a 5-year period in the past. Respondents may or may not accurately recall these events and feelings. In an effort to limit recall bias, the current analyses were restricted to respondents who completed the CSAQ, had worked for pay since their cancer diagnosis, and were within 5 years of their diagnosis. This resulted in an analytic sample that was relatively small and may or may not adequately represent the full range of experiences of cancer survivors. Another limitation of the study is the reliance on a dichotomous measure of employment. Such a measure does not allow for a more nuanced understanding of the effects that cancer has on survivors’ employment experiences. For instance, a survivor may be employed but because of consequences associated with cancer may be underemployed or working fewer hours than prior to cancer diagnosis. This was a limitation that could not be addressed as it is a constraint of the original methodology of the MEPS and CSAQ. Finally, as with any secondary analyses, our analyses were limited by the variables available from the primary study, the completeness of these variables, and the content of questions used to derive variables. We were unable to include variables related to cancer stage, physical or psychological functional job limitations, or detailed information about employer accommodations (ie, supervisor support) – factors associated with employment outcomes.7
Summary and future directions
Unemployed cancer survivors experience more challenges managing the cancer–work interface than cancer survivors who RTW and remain employed as survivors. Our findings suggest that these challenges increase the risk of unemployment. Specifically, both work-related psychological distress and work-related changes were significantly associated with odds of being unemployed during the 5 years following cancer diagnosis after controlling for social and demographic factors. Taken together, our findings highlight a number of important themes regarding supports that cancer survivors may need in order to return to and maintain employment as survivors. Psychosocial supports (on and off the job) may be needed to allow cancer survivors to discuss and exchange information about how adverse treatment effects may influence work tasks. This information is essential for survivors’ ability to develop strategies for managing work life and optimize long-term employment. Periodic meetings with an oncology social worker or counselor post-treatment could provide added supports for employed cancer survivors, especially among survivors with functional limitations.
Likewise, workplace supports are needed for both cancer survivors and their employers. There is growing recognition among employers that supervisors and managers need education and strategies for how to support cancer survivors during treatment and upon RTW following treatment.21,22 Employers are in significant need of approaches that can be used to support the employee long after treatment is over, especially among cancer survivors who may have residual functional limitations. Cancer survivors may benefit, long-term, from work place supports that allow them to reduce work hours, alter work tasks, and/or offer greater flexibility in order to accommodate adverse effects of treatment and associated changes in functional ability.
Cancer care teams could also play an important role in reducing the risk of unemployment among cancer survivors. Although successful RTW or the ability to work during treatment or enhancing chances for long-term employment post treatment may seem beyond the scope of the cancer care team, the clinical care team is in a unique position to assess, advise, and assist cancer survivors in managing employment issues during and after treatment. Cancer survivorship care plans may be a useful tool in facilitating discussion of this important topic between patients and providers and may serve a valuable function in connecting patients with information, strategies, and resources to successfully navigate the cancer–work interface, meaningful employment, and by extension, quality of life.
Future research should examine the impact of managing the cancer–work interface on cancer treatment decision making, treatment outcomes, and patients’ quality of life. Furthermore, effort should be made to develop provider, employment, and policy strategies to minimize unemployment and to address occupational contributors to cancer disparities.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. | ||
Desantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64(4):252–271. | ||
Taskila T, Lindbohm ML. Factors affecting cancer survivors’ employment and work ability. Acta Oncol. 2007;46(4):446–451. | ||
de Boer AG, Taskila T, Ojajärvi A, van Dijk FJ, Verbeek JH. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA. 2009;301(7):753–762. | ||
Roelen CA, Koopmans PC, Schellart AJ, van der Beek AJ. Resuming work after cancer: a prospective study of occupational register data. J Occup Rehabil. 2011;21(3):431–440. | ||
Jagsi R, Abrahamse PH, Lee KL, et al. Treatment decisions and employment of breast cancer patients: results of a population-based survey. Cancer. 2017;123(24):4791–4799. | ||
Mehnert A. Employment and work-related issues in cancer survivors. Crit Rev Oncol Hematol. 2011;77(2):109–130. | ||
Cooper AF, Hankins M, Rixon L, Eaton E, Grunfeld EA. Distinct work-related, clinical and psychological factors predict return to work following treatment in four different cancer types. Psychooncology. 2013;22(3):659–667. | ||
Kolodziejczyk C, Heinesen E. Labour market participation after breast cancer for employees from the private and public sectors: educational and sector gradients in the effect of cancer. Econ Hum Biol. 2016;21:33–55. | ||
Whitney RL, Bell JF, Reed SC, et al. Predictors of financial difficulties and work modifications among cancer survivors in the United States. J Cancer Surviv. 2016;10(2):241–250. | ||
Keim-Malpass J, Levine B, Danhauer SC, Avis NE. Work-related perceptions and quality of life among breast cancer survivors. Psychooncology. 2016;25(7):873–876. | ||
Morrison T, Thomas R, Guitard P. Physicians’ perspectives on cancer survivors’ work integration issues. Can Fam Physician. 2015;61(1): e36–e42. | ||
Pryce J, Munir F, Haslam C. Cancer survivorship and work: symptoms, supervisor response, co-worker disclosure and work adjustment. J Occup Rehabil. 2007;17(1):83–92. | ||
MEPS [homepage on the Internet]. Medical expenditures panel survey: download data files, documentation and codebooks. https://meps.ahrq.gov/mepsweb/data_stats/download_data_files.jsp. Accessed August 31, 2018. | ||
Spelten ER, Sprangers MA, Verbeek JH. Factors reported to influence the return to work of cancer survivors: a literature review. Psychooncology. 2002;11(2):124–131. | ||
Hewitt M, Rowland JH, Yancik R. Cancer survivors in the United States: age, health, and disability. J Gerontol A Biol Sci Med Sci. 2003;58(1):M82–M91. | ||
National Research Council, Institute of Medicine. From Cancer Patient to Cancer Survivor: Lost in Transition. Washington, DC: The National Academies Press; 2006. | ||
Yabroff KR, Lawrence WF, Clauser S, Davis WW, Brown ML. Burden of illness in cancer survivors: findings from a population-based national sample. J Natl Cancer Inst. 2004;96(17):1322–1330. | ||
Moskowitz MC, Todd BL, Chen R, Feuerstein M. Function and friction at work: a multidimensional analysis of work outcomes in cancer survivors. J Cancer Surviv. 2014;8(2):173–182. | ||
Feuerstein M, Todd BL, Moskowitz MC, et al. Work in cancer survivors: a model for practice and research. J Cancer Surviv. 2010;4(4):415–437. | ||
Caron M, Durand MJ, Tremblay D. Perceptions of breast cancer survivors on the supporting practices of their supervisors in the return-to-work process: a qualitative descriptive study. J Occup Rehabil. 2018:28(1)89–96. | ||
Swanberg JE, Nichols HM, Ko J, Tracy JK, Vanderpool RC. Managing cancer and employment: decisions and strategies used by breast cancer survivors employed in low-wage jobs. J Psychosoc Oncol. 2017;35(2):180–201. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.