")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 11
Managing fatigue in patients with primary Sjögren’s syndrome: challenges and solutions
Authors Miyamoto ST , Lendrem DW , Ng WF , Hackett KL, Valim V
Received 11 December 2018
Accepted for publication 15 February 2019
Published 24 April 2019 Volume 2019:11 Pages 77—88
DOI https://doi.org/10.2147/OARRR.S167990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Samira Tatiyama Miyamoto,1 Dennis William Lendrem,2–4 Wan-Fai Ng,2–4 Katie Louise Hackett,2,4–5 Valéria Valim6,7
1Department of Integrated Education in Health, Universidade Federal do Espírito Santo, Vitória, Brazil; 2Musculoskeletal Research Group, Institute of Cellular Medicine, Newcastle University and NIHR Newcastle Biomedical Research Centre, Newcastle University, Newcastle upon Tyne, UK; 3NIHR Newcastle Biomedical Research Centre, Newcastle University, Newcastle upon Tyne, UK; 4Newcastle upon Tyne Hospitals NHS Trust, , Newcastle upon Tyne, UK; 5Department of Social Work, Education and Community Wellbeing, Northumbria University, Newcastle upon Tyne, UK; 6Department of Medical Clinic, Universidade Federal do Espírito Santo, Vitória, Brazil; 7Rheumatology Outpatient Clinic, Hospital Universitário Cassiano Antônio de Moraes (HUCAM), Vitória, Brazil
Abstract: Primary Sjögren’s syndrome (pSS) patients identify fatigue as their most important symptom and the one most difficult to cope with, but there are still many challenges and few solutions to manage this debilitating symptom. Promising pharmacological treatments, such as rituximab, have failed in more stringent tests including randomized controlled trials (RCTs) and meta-analysis. While non-pharmacological interventions may be safer, less costly, and address other common comorbidities, to date only aerobic exercise seems to be effective at reducing fatigue in pSS. All interventions, pharmacological or not, need to be tested in high-quality RCTs. The aim of this review is to provide an overview of fatigue management in pSS and discuss potential opportunities for future research.
Keywords: primary Sjögren’s syndrome, fatigue, treatment, review
Introduction
Fatigue is a hallmark of many rheumatologic conditions, including primary Sjögren’s syndrome (pSS). A systemic autoimmune disease characterized by lymphocytic infiltration and progressive destruction of exocrine glands, 20–40% of pSS patients present with severe systemic manifestations.1 Fatigue is reported in up to 70% of the pSS patients and most patients are also affected by dryness and pain.2
Fatigue is defined by Staud as “a subjective, unpleasant symptom that incorporates total body feelings ranging from tiredness to exhaustion, creating an unrelenting overall condition that interferes with individuals’ ability to function in their normal capacity”.3 PSS patients often complain that it is their greatest problem and the most difficult to cope with.4 They experience a heavy, resistant body and uncontrollable fluctuating fatigue.5 Fatigue in pSS is chronic, persistent, and intractable.6,7 In pSS its pathophysiology is unknown, and is likely to involve multiple factors.
Genetic factors have been postulated for the development of fatigue in pSS,8,9 but there is a paucity of studies to confirm this link. Fatigue in pSS may be linked to inflammatory mechanisms. Hartkamp et al did not find any association between the levels of fatigue and the serum levels of the inflammatory markers interleukin (IL)-1b, IL-2, IL-6, IL-10 and tumor necrosis factor alfa (TNF-α).10 However, Howard et al showed that lower levels of the pro-inflammatory cytokines inducible protein (IP)-10 and interferon-gamma (IFN-γ), together with pain and depression, were the most important predictors of fatigue.11 Nonetheless, the evidence for an association between fatigue and disease activity – or any other inflammatory markers – remains controversial.11–15
Fatigue is known to be associated with lower aerobic capacity16 and lower physical activity levels.17,18 Wouters et al have shown that pSS patients with lower physical activity, higher activity avoidance, and greater somatic focus have more severe symptoms of fatigue.19 Fatigue in pSS is associated with greater functional impairment.20 It is possible that interventions to increase aerobic capacity and levels of physical activity may improve the symptoms of fatigue.
PSS patients also present a range of other manifestations associated with fatigue. These include sleep disturbances,21–23 autonomic dysfunction,24,25 depression,11,13,15,26,27 dysfunctional or alexithymic psychological profile,28 neuroticism, and fibromyalgia.15 These complex associations and comorbidities require appropriate management in clinical practice based on a multi-disciplinary approach including rheumatologists and other health professionals.
A growing number of methods have been used to measure fatigue in pSS studies. Few of them used the specific instrument of the pSS, the Profile of Fatigue and Discomfort (PROFAD), whose fatigue component (Profile of Fatigue-ProF) measures the somatic (ProF-S) and mental (ProF-M) fatigue.29,30 Instead, most studies have used a single-item instrument, the 10-cm VAS, or non-disease specific multi-item questionnaires.
Despite VAS popularity, it does not capture the multi-dimensional nature of fatigue; neither it is able to identify patients with major fatigue. However, another recent and specific disease instrument, the EULAR Sjögren’s Syndrome Patients Reported Index (ESSPRI), also uses 0 to 10 numerical scales for the assessment of each of the three domains: dryness, fatigue and musculoskeletal pain.4,31
There are a range of multi-item questionnaires such as Multidimensional Fatigue Inventory (MFI),32 Fatigue Severity Scale (FSS),33 Functional Assessment of Cancer Therapy Scale-fatigue (FACIT-fatigue),34,35 Fatigue Impact Scale (FIS)36 and Chalder Fatigue Scale (CFS).37 Nevertheless, these instruments were designed initially to measure fatigue in other disorders and therefore may not necessarily be suitable for use in pSS.
Fatigue is inversely correlated with health-related quality of life27,38,39 and with both the physical,40,41 and the mental components of the SF-36.41 While treatment of this disabling symptom is likely to improve patients’ daily life, there is little evidence-based treatment of fatigue. This makes patient management a real challenge for rheumatologists and other health professionals. The aim of this review is to provide an overview on the management of fatigue in pSS and discuss potential targets for future research.
The main characteristics and outcomes of the selected studies are summarised in Table 1.
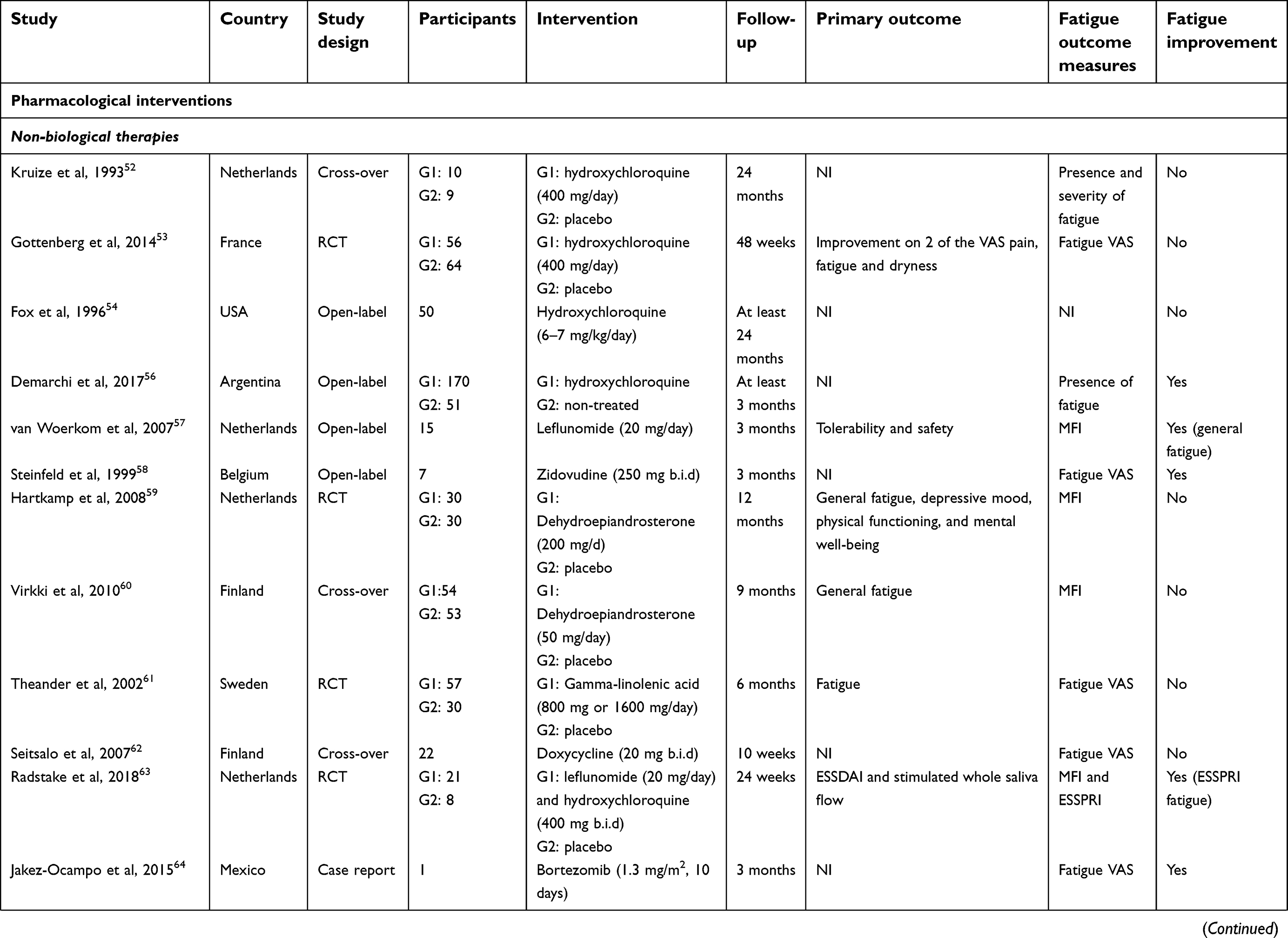  
| Table 1 Characteristics and outcomes of the studies |
Pharmacological treatment to treat fatigue in pSS: a real challenge
There is currently no evidence to support pharmacological treatment of fatigue in pSS. Both biological and non-biological treatments have been tried in pSS. Despite promising data from Phase II studies,42–44 two Phase III trials failed to demonstrate the efficacy of rituximab (RTX) in improving fatigue in pSS.45,46 It should be noted that for most of these clinical trials, fatigue is not the primary outcome. Instead, it is often part of a composite outcome. This may reflect the substantial costs, potential adverse events, and the diversity of instruments and lack of standard, objective and validated measurements of fatigue in pSS. For other biological therapies, results from Phase III trials are awaited. In addition, it is possible that biologic drugs potentially valuable to the treatment of pSS currently under investigation47 may be effective for fatigue.
Non-biological therapies
Hydroxychloroquine (HCQ) is an antimalarial drug with an immunomodulatory effect widely prescribed in patients with pSS reporting extraglandular manifestations, such as fatigue, arthralgia, arthritis or myalgia. However, evidence supporting its efficacy in treating such symptoms are weak, and its use is based largely on clinical experience and expert recommendations.48–51 A 2-year double-blind crossover trial with only 19 patients52 and a 2-year double-blind randomized controlled trial (RCT) with 120 patients53 did not demonstrate the efficacy of HCQ for fatigue measured by its severity and VAS, respectively. These studies and one retrospective study including 50 patients who were taking HCQ (6–7 mg/kg/day) for at least 2 years54 were included in a recent meta-analysis. This concluded that the effectiveness of HCQ was lower than placebo for fatigue and the most common adverse effects were gastrointestinal side effects.55 Conversely, another multicenter retrospective study including 221 patients with at least 1 year of follow-up, showed that fatigue was less frequent in those on HCQ therapy than those in the non-treated group (16.7% vs 83.3%, p<0.001).56 Thus whether HCQ is effective for fatigue in pSS remains unclear and further research is needed.
Small open-label studies have shown improvement in general fatigue measured by MFI using leflunomide (LEF) 20 mg daily in 15 patients after 24 weeks,57 and in fatigue VAS using zidovudine 250 mg twice daily in a study including only seven patients.58 In contrast, dehydroepiandrosterone,59,60 gamma-linolenic acid, an essential omega-6 fatty acid,61 and doxycycline62 have shown no efficacy in reducing fatigue in pSS RCTs. More recently, data from a Phase II clinical trials of a combination therapy using both HCQ and LEF with 42 patients (28 active arms, 14 placebos) showed improvement in ESSPRI fatigue.63
There is an interesting case report of a 44-year-old pSS patient refractory to conventional treatment (prednisone, azathioprine, and RTX), presenting with severe clinical manifestations including uncontrollable fatigue, headache, and hyperglobulinemic purpura, treated with bortezomib, a proteasome inhibitor licensed for the treatment of multiple myeloma. She showed a notable improvement of the general symptoms, particularly fatigue VAS, a decrease in serum globulin levels as well as in serum viscosity, and the return of the patient to her usual activities. More studies are needed to determine the safety and efficacy of this drug in patients with pSS.64
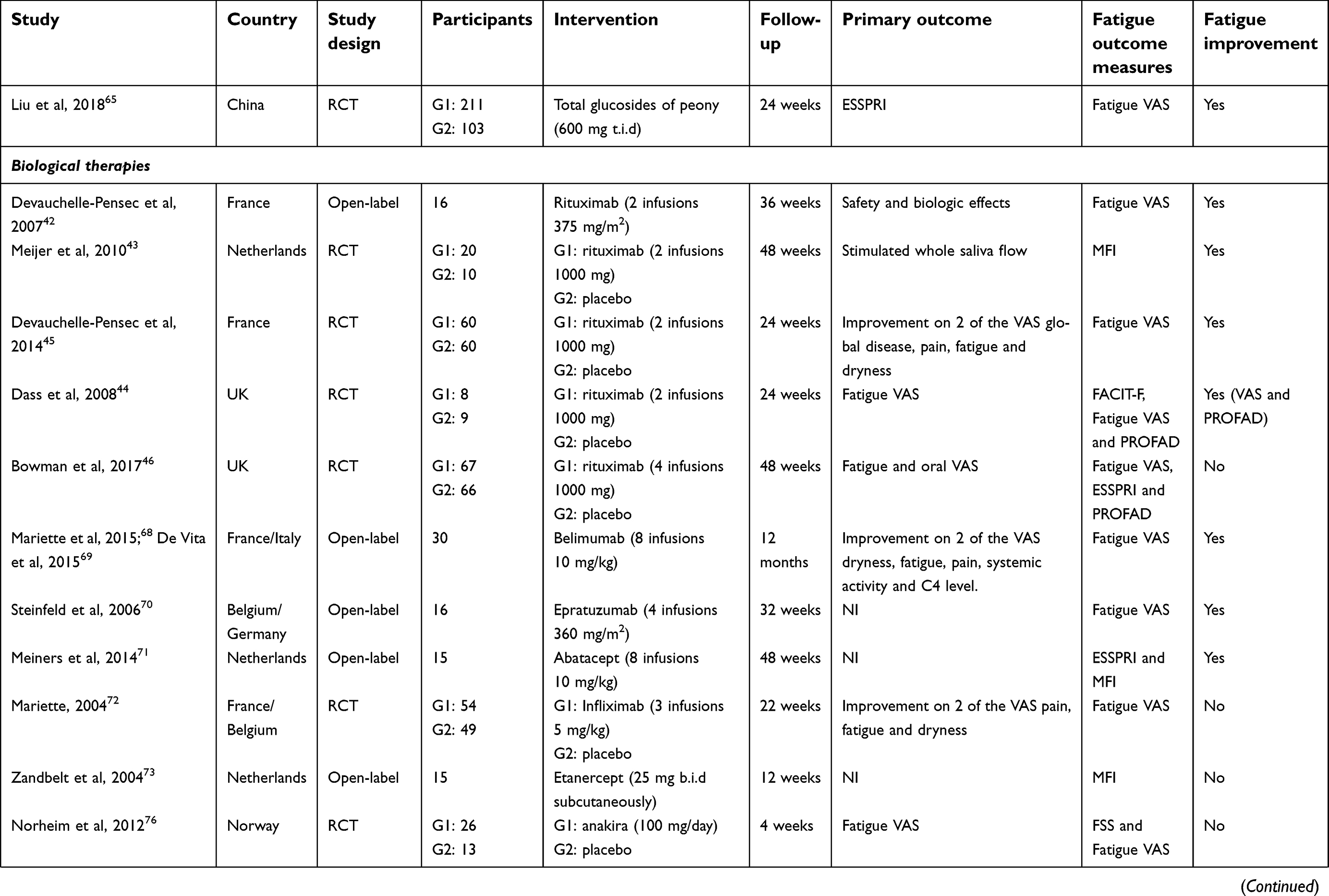
A recent Chinese multicenter RCT demonstrated the efficacy and safety of total glucosides of peony (TGP) in 320 patients with pSS who did not exhibit significant extra-glandular manifestations. TGP are extracted from the root of the Paeonia lactiflora pall and have been demonstrated to have immunomodulatory effects, such as inhibition of dendritic cell maturation and function. The results showed that ESSPRI scores improved dramatically, significantly alleviated some dryness symptoms, and improved fatigue VAS during the 24-week trial. The rate of adverse events in the TGP group was 10.9%; the main adverse event was diarrhea at a rate of 4.8%.65
Biological therapies
The increasing evidence that B cells play a leading role in the pSS pathogenesis indicates that RTX, a chimeric anti-CD20 monoclonal antibody which acts through depletion of B cells, may be an exciting therapy. A small prospective open-label study with 16 patients receiving two low-dose RTX infusions (375 mg/m2)42 and a RCT with 30 patients (2 infusions of 1000 mg)43 demonstrated an improvement in fatigue (VAS and MFI, respectively). However, a meta-analysis has shown that RTX is not able to reduce fatigue in pSS patients after 24 weeks.66
Improvement in fatigue is also observed in two other randomized controlled studies with two infusions (1000 mg) of RTX. In the study by Devauchelle-Pensec et al with 120 patients, reductions in fatigue VAS were observed at weeks 6 and 16.45 In the study by Dass et al with 17 patients, fatigue VAS and PROFAD improvement was significantly higher than the placebo group.44
However, Bowman et al in another larger RCT with 133 patients treated with two courses of RTX therapy (6 months apart), did not find significant differences in fatigue scores (VAS, ESSPRI, and PROFAD) between the RTX and the placebo arms (MD 5.0, 95% CI −3.37 to 13.37).46 Similarly, a more recent meta-analysis did not find significant differences between the RTX and placebo groups between baseline and week 24 in fatigue VAS (MD −3.24 95% CI −30.21 to 23.72).67
Belimumab, a monoclonal anti-BAFF antibody, is a promising biological drug to treat pSS, since 60% of the patients achieved the primary endpoint, including fatigue VAS and systemic activity, at week 28 in a prospective 1-year open-label study including 30 SS patients with systemic complications. Ten mg/kg of belimumab was administered at weeks 0, 2, and 4 and then every 4 weeks up to week 24.68,69
Another small, open-label study including 16 pSS patients with active disease investigated the use of epratuzumab, a humanized anti-CD22 monoclonal antibody, over 4 infusions of 360 mg/m2 once every 2 weeks, with 6 months of follow-up, showing efficacy in fatigue VAS.70
Similarly, abatacept, a selective modulator of costimulation of T cells, seemed to be effective in improving MFI, as well EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) and ESSPRI, in an open-label study including 15 patients. Eight intravenous abatacept infusions (10 mg/kg) were administered over 24 weeks of treatment with a follow-up at weeks 36 and 48.71
TNFα blockers, however, did not improve fatigue. Infliximab showed no efficacy, including fatigue VAS, in a double-blind, placebo-RCT including 103 patients receiving infusions of 5 mg/kg at weeks 0, 2, and 6 and followed up after 22 weeks.72
Similarly, just four of the 15 pSS patients included in a pilot study using etanercept subcutaneously twice per week for 12 weeks, with follow up visits at 18 and 24 weeks reported reduction in MFI.73
Animal studies support IL-1 receptors as potential targets. Dantzer et al report animal data demonstrating that sickness behavior is signaled through IL-1 receptors in the brain.74 In human studies, patients with pSS have higher levels of IL-1-RA in the cerebrospinal fluid with respect to controls, and its concentration correlated with fatigue.75 Norheim et al designed a double-blind RCT including 26 patients to test anakinra, a recombinant IL-1 receptor antagonist. However, while half of the patients in the active drug group reported a 50% reduction in fatigue VAS, compared to just one patient in the placebo group, there was no statistically significant reduction in the primary endpoint analysis using fatigue VAS. There were no significant changes in FSS scores between groups.76
May non-pharmacological interventions be potential treatments for fatigue in SSp?
Despite their potential, the only published non-pharmacological intervention that appears to be effective, is aerobic exercise. One problem is that complex interrelationships between physical activity, depression, sleep disturbances and pain in the pathophysiology of fatigue in pSS may make RCTs using fatigue as the primary outcome measure difficult to separate from confounding factors. However, in view of the possible adverse effects and substantial costs of biological therapies and the promising results of nonpharmacological studies from other rheumatic diseases, such interventions could be a great potential in the management of fatigue.
Exercise
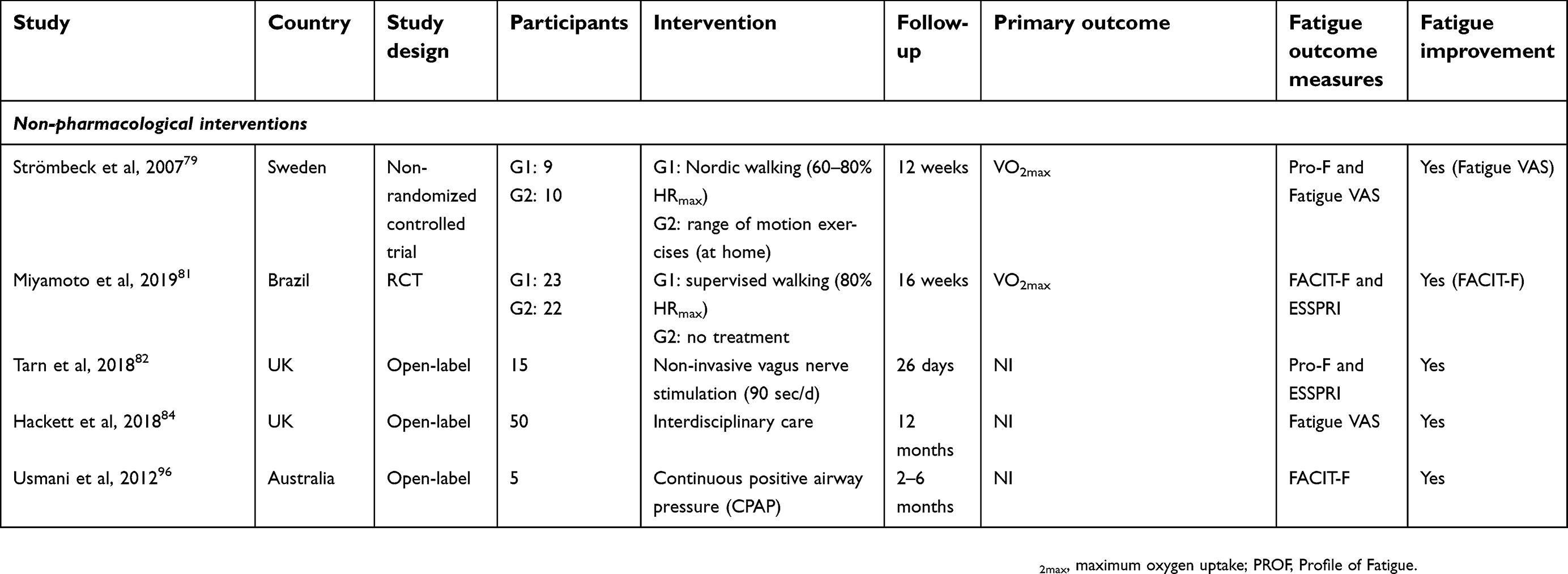
While exercise is recommended for the treatment of fatigue in pSS in recent guidelines48–51 and review studies,77,78 this is based largely on a single, relatively small (training group=9; control group=10) non-randomized control study of aerobic exercise in pSS. This study reported improvements in fatigue VAS (but not in Profile of fatigue, Pro-F), aerobic capacity, depression, and physical function. The training group performed a Nordic walking exercise three times a week for 12 weeks. The intensity of the prescribed exercise increased progressively over the training from 60–70% to a maximum of 70–80% of the age-predicted maximum heart rate (220 minus the age of the individual).79 However, this study was not included in the systematic review of Hackett et al on non-pharmacological treatment in pSS, as participants were not randomized.80 Miyamoto et al in a RCT with intention-to-treat analysis (training group=23; control group=22), demonstrated that a 16-week supervised walking program improves aerobic capacity, exercise tolerance, patient perception of improvement and fatigue measured by Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) without exacerbating disease activity in women with pSS. Fatigue ESSPRI domain did not show a significant reduction. The intensity of the exercise was based on the heart rate at 80% of the maximum heart rate reached in the treadmill test. Increasing the duration of exercise was made by time from 20 to 50 mins of effective walking.81
Other interventions
Other non-pharmacological interventions are the subject of recent studies. Tarn et al investigated the effect of a noninvasive vagus nerve stimulation device twice daily for a 26-day period in 15 female pSS patients finding a significant reduction in daytime sleepiness and Pro-F (but not in fatigue VAS). Authors suggest that the vagus nerve may play a role in the regulation of fatigue and immune responses in pSS. However, a RCT including a larger sample size is needed.82
Hackett et al argue for a personalized, holistic approach, delivered by a multidisciplinary care team. This empowers patients by taking their health concerns seriously. Patients may be supported to self-managing aspects of their condition, especially their key symptoms of dryness, fatigue, pain, and poor sleep.83 Data from 50 pSS patients attended at the Newcastle CRESTA Fatigue clinic, a UK National Health Service multidisciplinary clinic, showed an improvement in fatigue VAS scores and were maintained at 6–12 months follow-up. After the medical review of fatigue (including autonomic dysfunction, untreated comorbidities, and a medication review), therapy interventions are tailored according to the needs of the patient and may include occupational therapy (activity management), physiotherapy (core-strengthening exercises) and health psychology.84
One of the key interventions targeting self-management is patient education. This is defined as “planned organised learning experiences designed to support and enable people to manage life with their condition and optimise their health and well-being”.85 However, there is no study investigating the effect of a patient education program in pSS. In general chronic diseases, when compared to usual care, self-management programs have a small but statistically significant short-term improvement in fatigue, pain, disability, depression, health distress, self-rated health, and health-related quality of life, but not anxiety or depression.86
In addition to self-management and patient education, other psychosocial interventions have demonstrated a small benefit for managing fatigue in people with rheumatoid arthritis, such as cognitive behavioral therapy (CBT)87,88 and mindfulness.87 But there is no study performed in pSS. CBT is well recognized for psychological conditions such as depression or anxiety. However, CBT is weakly recommended in the guidelines for the management of fibromyalgia,89 and there is inconsistent to weak evidence to treat chronic fatigue syndrome.90
Mindfulness, a non-judgmental, present moment awareness meditation, has been shown to improve psychological well-being via improved cognitive and emotional reactivity.91 There is only limited evidence that this and other multi-modal approaches are effective for improving patient-reported outcomes and emotional disturbances related to rheumatoid arthritis.92
Sleep management may be important. Current recommendations include sleeping at a regular bedtime, avoid oversleeping and schedule breaks at work or during day at home for management of fatigue.93 Hackett et al report an increased prevalence of sleep disturbances in pSS patients compared with controls94 and suggest cognitive behavior therapy for insomnia (CBT-I) may be an appropriate treatment.23 This approach has not yet been tested in pSS, but there is evidence that it improves sleep, fatigue, and other quality-of-life outcomes in fibromyalgia patients.95 Usmani et al reported a higher frequency of obstructive apneas and hypopneas detected by polysomnography in pSS. These were doubled in the pSS group compared with controls. Five patients identified as having severe sleep apnoea were treated with continuous positive airway pressure (CPAP) resulting in significant improvements in both daytime sleepiness and fatigue, but not depression or anxiety.96
Possible solutions
There is still a long way to go to find solutions to manage fatigue in pSS. Certainly, the fragmented knowledge of the pathophysiological mechanisms of pSS, and especially of fatigue, is the main obstacle to find them. It is likely that basic research associated with therapeutic research may show more about the pathogenesis of pSS/fatigue and, consequently, define the most appropriate therapeutic approach. High-quality RCT for potential pharmacological and non-pharmacological interventions must be performed. However, the recommendation for the best patient-reported outcome measures for fatigue in pSS through a systemic review with meta-analysis is an urgent and essential need to standardize the evaluation methods in the RCTs and to guarantee valid and reliable results.
New knowledge about the pathogenesis of autoimmune diseases may lead to a new therapeutic approach in pSS. It is known that Janus kinase–Signal Transducers and Activators of Transcription (JAK–STAT) pathway play a central role in the pathogenesis of autoimmune diseases.97 Janus Kinases inhibitors (tofacitinib) have shown significant improvement in fatigue in rheumatoid arthritis,98 but have yet to be tested in pSS. Sphingosine-1-phosphate (S1P) enhances proliferation and IFN-γ production by CD4+T cells in pSS patients.99 Sphingosine-1-phosphate receptor (S1PR) modulators (fingolimod and siponimod) might provide potential treatment for several autoimmune diseases100 such as pSS.
Conclusion
Fatigue is a frequent and disabling symptom of pSS. The unknown pathophysiology of fatigue makes it difficult to determine a specific treatment for this symptom. Synthetic or biologic drugs have so far failed to show significant efficacy in improving fatigue. The role of HCQ remains unclear; RTX is questionable; LEF, zidovudine, bortezomib, TGP, belimumab, epratuzumab, abatacept, etanercept, and anakinra require further research. Other treatments such as dehydroepiandrosterone, gamma-linolenic acid, doxycycline, and infliximab are not effective based on available data.
Robust studies using non-pharmacological approaches are urgently needed. Non-pharmacological approaches are inherently attractive offering fewer adverse effects than drug treatments, and there are some data to support their use from other rheumatic diseases. Aerobic exercise seems to be effective and safe suggesting an important role for physical fitness in the pathogenesis of fatigue. Nonetheless, long-term RCTs are needed and other types of exercise should be explored too. CPAP is considered the most efficacious method to treat sleep apnea.101 However, the effect of CPAP or any other intervention for sleep disorders in pSS should be investigated by RCTs, as well as non-invasive vagus nerve stimulation, patient education programs or psychological techniques.
Much of the data comes from small trials, or the results of open-label studies that are not confirmed in RCTs, and there are few studies with long-term follow-up. One of the obstacles to trials in this area is the difficulties in measuring fatigue. Fatigue VAS scales may be of limited value. With the exception of PROFAD/ProF and ESSPRI fatigue domain, it is not possible to assume that the other instruments would have measures and practical properties of consistent measures in the population with pSS.
In addition, further studies exploring the pathogenesis of fatigue in pSS are crucial to guide therapeutic development. Certainly, in clinical practice, the multi-dimensional nature of fatigue suggests that effective management of pSS-associated fatigue may require a patient-centric, multidisciplinary approach.
Abbreviations
pSS, primary Sjögren’s syndrome; IL, interleukin; TNF-α, tumor necrosis factor alfa; IP, inducible protein; IFN-γ, interferon-gamma; PROFAD, Profile of Fatigue and Discomfort; VAS, visual analogue scale; ESSPRI, EULAR Sjögren’s Syndrome Patient Reported Index; MFI, Multidimensional Fatigue Inventory; FSS, Fatigue Severity Scale; FACIT-fatigue, Functional Assessment of Cancer Therapy Scale-fatigue; FIS, Fatigue Impact Scale; CFS, Chalder Fatigue Scale; RTX, rituximab; HCQ, hydroxychloroquine; RCT, randomized controlled trial; LEF, leflunomide; ESSDAI, EULAR Sjögren’s Syndrome Disease Activity Index; TGP, total glucosides of peony; CBT-I, cognitive behaviour therapy for insomnia; CPAP, continuous positive airway pressure; JAK–STAT, Janus kinase–Signal Transducers and Activators of Transcription; S1P, sphingosine-1-phosphate; S1PR, sphingosine-1-phosphate receptor.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seror R, Ravaud P, Bowman SJ, et al. EULAR Sjögren’s syndrome disease activity index: development of a consensus systemic disease activity index for primary Sjögren’s syndrome. Ann Rheum Dis. 2010;69(6):1103–1109. doi:10.1136/ard.2009.110619
2. Ng W-F, Bowman SJ. Primary Sjögren’s syndrome: too dry and too tired. Rheumatology (Oxford). 2010;49(5):844–853. doi:10.1093/rheumatology/keq009
3. Staud R. Peripheral and central mechanisms of fatigue in inflammatory and noninflammatory rheumatic diseases. Curr Rheumatol Rep. 2012;14(6):539–548. doi:10.1007/s11926-012-0277-z
4. Seror R, Ravaud P, Mariette X, et al. EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI): development of a consensus patient index for primary Sjogren’s syndrome. Ann Rheum Dis. 2011;70(6):968–972. doi:10.1136/ard.2010.143743
5. Mengshoel AM, Norheim KB, Omdal R. Primary Sjögren’s syndrome: fatigue is an ever-present, fluctuating, and uncontrollable lack of energy. Arthritis Care Res (Hoboken). 2014;66(8):1227–1232. doi:10.1002/acr.22263
6. Theander E, Andersson SI, Manthorpe R, Jacobsson LTH. Proposed core set of outcome measures in patients with primary Sjögren’s syndrome: 5 year follow up. J Rheumatol. 2005;32(8):1495–1502.
7. Haldorsen K, Bjelland I, Bolstad AI, Jonsson R, Brun JG. A five-year prospective study of fatigue in primary Sjögren’s syndrome. Arthritis Res Ther. 2011;13(5):R167. doi:10.1186/ar3487
8. Norheim KB, Le Hellard S, Nordmark G, et al. A possible genetic association with chronic fatigue in primary Sjögren’s syndrome: a candidate gene study. Rheumatol Int. 2014;34(2):191–197. doi:10.1007/s00296-013-2850-9
9. James K, Al-Ali S, Tarn J, et al. A transcriptional signature of fatigue derived from patients with primary Sjögren’s syndrome. PLoS One. 2015;10(12):e0143970. doi:10.1371/journal.pone.0143970
10. Hartkamp A, Geenen R, Bijl M, Kruize AA, Godaert GLR, Derksen RHWM. Serum cytokine levels related to multiple dimensions of fatigue in patients with primary Sjogren’s syndrome. Ann Rheum Dis. 2004;63(10):1335–1337. doi:10.1136/ard.2003.011825
11. Howard Tripp N, Tarn J, Natasari A, et al. Fatigue in primary Sjögren’s syndrome is associated with lower levels of proinflammatory cytokines. RMD Open. 2016;2(2):e000282. doi:10.1136/rmdopen-2016-000282
12. Barendregt PJ, Visser MRM, Smets EMA, Tulen JHM, Boomsma F, Markusse HM. Fatigue in primary Sjögren’s syndrome. Ann Rheum Dis. 1998;16:291–295. doi:10.1136/ard.57.5.291
13. Segal B, Thomas W, Rogers T, et al. Prevalence, severity, and predictors of fatigue in subjects with primary Sjögren’s syndrome. Arthritis Rheumatol. 2008;59(12):1780–1787. doi:10.1002/art.24311
14. Tensing EK, Solovieva SA, Tervahartiala T, et al. Fatigue and health profile in sicca syndrome of Sjögren’s and non-Sjögren’s syndrome origin. Clin Exp Rheumatol. 2001;19(3):313–316.
15. Karageorgas T, Fragioudaki S, Nezos A, Karaiskos D, Moutsopoulos HM, Mavragani CP. Fatigue in primary Sjögren’s syndrome: clinical, laboratory, psychometric, and biologic associations. Arthritis Care Res. 2016;68(1):123–131. doi:10.1002/acr.22720
16. Strömbeck B, Ekdahl C, Manthorpe R, Jacobsson LTH. Physical capacity in women with primary Sjögren’s syndrome: a controlled study. Arthritis Rheumatol. 2003;49(5):681–688. doi:10.1002/art.11384
17. Ng W-F, Miller A, Bowman JS, et al. Physical activity but not sedentary activity is reduced in primary Sjögren’s syndrome. Rheumatol Int. 2017;37(4):623–631. doi:10.1007/s00296-016-3637-6
18. Dassouki T, Benatti FB, Pinto AJ, et al. Objectively measured physical activity and its influence on physical capacity and clinical parameters in patients with primary Sjögren’s syndrome. Lupus. 2017;26(7):690–697. doi:10.1177/0961203316674819
19. Wouters EJM, van Leeuwen N, Bossema ER, et al. Physical activity and physical activity cognitions are potential factors maintaining fatigue in patients with primary Sjögren’s syndrome. Ann Rheum Dis. 2012;71(5):668–673. doi:10.1136/ard.2011.154245
20. Hackett KL, Newton JL, Frith J, et al. Impaired functional status in primary Sjögren’s syndrome. Arthritis Care Res. 2012;64(11):1760–1764. doi:10.1002/acr.21738
21. Theander L, Strömbeck B, Mandl T, Theander E. Sleepiness or fatigue? Can we detect treatable causes of tiredness in primary Sjögren’s syndrome? Rheumatology. 2010;49(6):1177–1183. doi:10.1093/rheumatology/keq023
22. Priori R, Minniti A, Antonazzo B, Fusconi M, Valesini G, Curcio G. Sleep quality in patients with primary Sjögren’s syndrome. Clin Exp Rheumatol. 2016;34(3):373–379.
23. Hackett KL, Deary V, Deane KHO, Newton JL, Ng W, Rapley T. Experience of sleep disruption in primary Sögren’s syndrome: A focus group study. Br J Occup Ther. 2018;81(4):218–226. doi:10.1177/0308022617745006
24. d’Elia HF, Rehnberg E, Kvist G, Ericsson A, Konttinen Y, Mannerkorpi K. Fatigue and blood pressure in primary Sjogren’s syndrome. Scand J Rheumatol. 2008;37(4):284–292. doi:10.1080/03009740801907995
25. Koh JH, Kwok SK, Lee J, Park SH. Autonomic dysfunction in primary Sjogren’s syndrome: A prospective cohort analysis of 154 Korean patients. Korean J Intern Med. 2017;32(1):165–173. doi:10.3904/kjim.2015.219
26. Westhoff G, Dörner T, Zink A. Fatigue and depression predict physician visits and work disability in women with primary Sjögren’s syndrome: results from a cohort study. Rheumatology. 2012;51(2):262–269. doi:10.1093/rheumatology/ker208
27. Lendrem D, Mitchell S, Mcmeekin P, et al. Health-related utility values of patients with primary Sjögren’s syndrome and its predictors. Ann Rheum Dis. 2014;73(7):1362–1368. doi:10.1136/annrheumdis-2012-202863
28. Van Leeuwen N, Bossema ER, Knoop H, et al. Psychological profiles in patients with Sjögren’s syndrome related to fatigue: A cluster analysis. Rheumatology. 2015;54(5):776–783. doi:10.1093/rheumatology/keu387
29. Bowman SJ, Booth DA, Platts RG. Measurement of fatigue and discomfort in primary Sjögren’s syndrome using a new questionnaire tool. Rheumatology. 2004;43(6):758–764. doi:10.1093/rheumatology/keh170
30. Bowman SJ, Hamburger J, Richards A, Barry RJ, Rauz S. Patient-reported outcomes in primary Sjogren’s syndrome: comparison of the long and short versions of the profile of fatigue and Discomfort-Sicca symptoms Inventory. Rheumatology. 2009;48(2):140–143. doi:10.1093/rheumatology/ken426
31. Seror R, Theander E, Brun JG, et al. Validation of EULAR primary Sjögren’s syndrome disease activity (ESSDAI) and patient indexes (ESSPRI). Ann Rheum Dis. 2015;74(5):859–866. doi:10.1136/annrheumdis-2013-204615
32. Smets E, Garssen B, Bonke B, De Haes J. The Multidimensional Fatigue Inventory (MFI): psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39:315–325.
33. Krupp L, LaRocca N, Muir-Nash J, Steinberg A. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121–1123.
34. Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. doi:10.1186/1477-7525-1-79
35. Webster K, Odom L, Peterman A, Lent L, Cella D. The Functional Assessment of Chronic Illness Therapy (FACIT) measurement system: validation of version 4 of the core questionnaire. Qual Life Res. 1999;8(7):604.
36. Fisk J, Ritvo P, Ross L, Haase D, Marrie T, Schlech W. Measuring the functional impact of fatigue: initial validation of the fatigue impact scale. Clin Infect Dis. 1994;18(Suppl. 1):S79–83.
37. Chalder T, Berelowitz G, Pawlikowska T, Al E. Development of a fatigue scale. J Psychosom Res. 1993;37:147–153.
38. Cornec D, Devauchelle-Pensec V, Mariette X, et al. Severe health-related quality of life impairment in active primary Sjögren’s Syndrome and patient-reported outcomes: data from a large therapeutic trial. Arthritis Care Res. 2017;69(4):528–535. doi:10.1002/acr.22974
39. Koh JH, Kwok SK, Lee J, et al. Pain, xerostomia, and younger age are major determinants of fatigue in Korean patients with primary Sjögren’s syndrome: a cohort study. Scand J Rheumatol. 2017;46(1):49–55. doi:10.3109/03009742.2016.1153142
40. Champey J, Corruble E, Gottenberg J-E, et al. Quality of life and psychological status in patients with primary Sjögren’s syndrome and sicca symptoms without autoimmune features. Arthritis Rheumatol. 2006;55(3):451–457. doi:10.1002/art.21990
41. Liu Z, Dong Z, Liang X, et al. Health-related quality of life and psychological status of women with primary Sjögren’s syndrome A cross-sectional study of 304 Chinese patients. Medicine (Baltimore). 2017;96(50):e9208. doi:10.1097/MD.0000000000009208
42. Devauchelle-Pensec V, Pennec Y, Morvan J, et al. Improvement of Sjögren’s syndrome after two infusions of rituximab (anti-CD20). Arthritis Care Res. 2007;57(2):310–317. doi:10.1002/art.22536
43. Meijer JM, Meiners PM, Vissink A, et al. Effectiveness of rituximab treatment in primary sjögren’s syndrome: A randomized, double-blind, placebo-controlled trial. Arthritis Rheumatol. 2010;62(4):960–968. doi:10.1002/art.27314
44. Dass S, Bowman SJ, Vital EM, et al. Reduction of fatigue in Sjögren syndrome with rituximab: results of a randomised, double-blind, placebo-controlled pilot study. Ann Rheum Dis. 2008;67(11):1541–1544. doi:10.1136/ard.2007.083865
45. Devauchelle-Pensec V, Mariette X, Jousse-Joulin S, et al. Treatment of primary Sjögren syndrome with rituximab: a randomized trial. Ann Intern Med. 2014;160(4):233–242. doi:10.7326/M13-1085
46. Bowman S, Colin C, O’Dwyer J, et al. Randomized controlled trial of Rituximab and cost- effectiveness analysis in treating fatigue and oral dryness in primary Sjogren’s Syndrome. Arthritis Rheumatol. 2017;69(7):1440–1450. doi:10.1002/art
47. Sambataro D, Sambataro G, Dal Bosco Y, Polosa R. Present and future of biologic drugs in primary Sjögren’s syndrome. Expert Opin Biol Ther. 2017;17(1):63–75. doi:10.1080/14712598.2017.1235698
48. Carsons SE, Vivino FB, Parke A, et al. Treatment guidelines for Rheumatologic Manifestations of Sjögren’s : use of biologics, management of Fatigue and Inflammatory Musculoskeletal pain. Arthritis Care Res (Hoboken). 2016:2–40. doi:10.1002/acr.
49. Valim V, Trevisani VFM, Pasoto SG, et al. Recommendations for the treatment of Sjögren’s syndrome. Rev Bras Reumatol. 2015;55(5):446–457. doi:10.1016/j.rbr.2015.07.004
50. Vivino FB, Carsons SE, Foulks G, et al. New treatment guidelines for Sjögren’s disease. Rheum Dis Clin N Am. 2016;42:531–551. doi:10.1016/j.rdc.2016.03.010
51. Price EJ, Rauz S, Tappuni AR, et al. The British Society for Rheumatology guideline for the management of adults with primary Sjögren’s Syndrome. Rheumatology. 2017;56(10):e24–e48. doi:10.1093/rheumatology/kex166
52. Kruize AA, René RJ, Kallenberg CGM, et al. Hydroxychloroquine treatment for primary Sjögren’s syndrome: a two year double blind crossover trial. Ann Rheum Dis. 1993;52:360–364.
53. Gottenberg J-E, Ravaud P, Puéchal X, et al. Effects of hydroxychloroquine on symptomatic improvement in primary Sjögren syndrome: the JOQUER randomized clinical trial. JAMA. 2014;312(3):249–258. doi:10.1001/jama.2014.7682
54. Fox RI, Dixon R, Guarrasi V, Krubel S. Treatment of primary Sjögren’s syndrome with hydroxychloroquine: a retrospective, open-label study. Lupus. 1996;5(Suppl 1):S31–6.
55. Wang SQ, Zhang LW, Wei P, Hua H. Is hydroxychloroquine effective in treating primary Sjogren’s syndrome: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2017;18(1):1–13. doi:10.1186/s12891-017-1543-z
56. Demarchi J, Papasidero S, Medina MA, et al. Primary Sjögren’s syndrome: extraglandular manifestations and hydroxychloroquine therapy. Clin Rheumatol. 2017;36(11):2455–2460. doi:10.1007/s10067-017-3822-3
57. van Woerkom JM, Kruize AA, Geenen R, et al. Safety and efficacy of leflunomide in primary Sjögren’s syndrome: a phase II pilot study. Ann Rheum Dis. 2007;66(8):1026–1032. doi:10.1136/ard.2006.060905
58. Steinfeld SD, Demols P, Van Vooren JP, Cogan E, Appelboom T. Zidovudine in primary Sjögren’s syndrome. Rheumatology. 1999;38(9):814–817.
59. Hartkamp A, Geenen R, Godaert GLR, Bootsma H, Kruize AA, Bijlsma JWJ. Effect of dehydroepiandrosterone administration on fatigue, well-being, and functioning in women with primary Sjögren syndrome: a randomised controlled trial. Ann Rheum Dis. 2008;67(1):91–97. doi:10.1136/ard.2007.071563
60. Virkki LM, Porola P, Forsblad-D’Elia H, Valtysdottir S, Solovieva SA, Konttinen YT. Dehydroepiandrosterone (DHEA) substitution treatment for severe fatigue in DHEA-deficient patients with primary Sjögren’s syndrome. Arthritis Care Res. 2010;62(1):118–124. doi:10.1002/acr.20022
61. Theander E, Horrobin DF, Jacobsson LTH, Manthorpe R. Gammalinolenic acid treatment of fatigue associated with primary Sjögren’s syndrome. Scand J Rheumatol. 2002;31(2):72–79.
62. Seitsalo H, Niemelä RK, Marinescu-Gava M, Vuotila T, Tjäderhane L, Salo T. Effectiveness of low-dose doxycycline (LDD) on clinical symptoms of Sjögren’s Syndrome: A randomized, double-blind, placebo controlled cross-over study. J Negat Results Biomed. 2007;6:1–6. doi:10.1186/1477-5751-6-11
63. Radstake TRDJ, Heijden EHM Van Der, Moret FM, Hillen MR. Clinical efficacy of leflunomide/hydroxychloroquine combination therapy in patients with primary Sjögren’s syndrome: results of a placebo-controlled double-blind randomized clinical trial (abstract). Arthritis Rheumatol. 2018;70(Suppl):10.
64. Jakez-Ocampo J, Atisha-Fregoso Y, Llorente L. Refractory primary Sjögren syndrome successfully treated with bortezomib. J Clin Rheumatol. 2015;21(1):31–32. doi:10.1097/RHU.0000000000000210
65. Liu X, Li X, Li X, et al. The efficacy and safety of total glucosides of peony in the treatment of primary Sjögren’s syndrome: a multi-center, randomized, double-blinded, placebo-controlled clinical trial. Clin Rheumatol. 2018. doi:10.1007/s10067-018-4315-8
66. Souza FBDV, Porfírio GJM, Andriolo BNG, Albuquerque JVD, Trevisani VFM. Rituximab effectiveness and safety for treating primary Sjögren’s syndrome (pSS): systematic review and meta-analysis. PLoS One. 2016;11(3):e0150749. doi:10.1371/journal.pone.0150749
67. Letaief H, Lukas C, Barnetche T, Gaujoux-Viala C, Combe B, Morel J. Efficacy and safety of biological DMARDs modulating B cells in primary Sjögren’s syndrome: systematic review and meta-analysis. Jt Bone Spine. 2018;85(1):15–22. doi:10.1016/j.jbspin.2017.06.004
68. Mariette X, Seror R, Quartuccio L, et al. Efficacy and safety of belimumab in primary Sjögren’s syndrome: results of the BELISS open-label phase II study. Ann Rheum Dis. 2015;74(3):526–531. doi:10.1136/annrheumdis-2013-203991
69. De VS, Quartuccio L, Seror R, et al. Efficacy and safety of belimumab given for 12 months in primary Sjögren’s syndrome: the BELISS open-label phase II study. Rheumatology. 2015;54(12):2249–2256. doi:10.1093/rheumatology/kev257
70. Steinfeld SD, Tant L, Burmester GR, et al. Epratuzumab (humanised anti-CD22 antibody) in primary Sjögren’s syndrome: an open-label phase I/II study. Arthritis Res Ther. 2006;8(4):R129. doi:10.1186/ar2018
71. Meiners PM, Vissink A, Kroese FGM, et al. Abatacept treatment reduces disease activity in early primary Sjögren’s syndrome (open-label proof of concept ASAP study). Ann Rheum Dis. 2014;73(7):1393–1396. doi:10.1136/annrheumdis-2013-204653
72. Mariette X, Ravaud P, Steinfeld S, et al. Inefficacy of Infliximab in primary Sjögren’s Syndrome: results of the randomized, controlled trial of remicade in primary Sjögren’s Syndrome (TRIPSS). Arthritis Rheum. 2004;50(4):1270–1276. doi:10.1002/art.20146
73. Zandbelt MM, de Wilde P, van Damme P, Hoyng CB, van de Putte L, van den Hoogen F. Etanercept in the treatment of patients with primary Sjögren’s syndrome: a pilot study. J Rheumatol. 2004;31(1):96–101.
74. Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56. doi:10.1038/nrn2297
75. Harboe E, Tjensvoll AB, Vefring HK, Gøransson LG, Kvaløy JT, Omdal R. Fatigue in primary Sjögren’s syndrome–a link to sickness behaviour in animals? Brain Behav Immun. 2009;23(8):1104–1108. doi:10.1016/j.bbi.2009.06.151
76. Norheim KB, Harboe E, Gøransson LG, Omdal R. Interleukin-1 inhibition and fatigue in primary Sjögren’s syndrome–a double blind, randomised clinical trial. PLoS One. 2012;7(1):e30123. doi:10.1371/journal.pone.0030123
77. Stefanski A, Tomiak C, Pleyer U, Dietrich T, Burmester GR, Dörner T. The diagnosis and treatment of Sjögren’s Syndrome. Dtsch Arztebl Int. 2017;114(20):354–361. doi:10.3238/arztebl.2017.0354
78. Saraux A, Pers JO, Devauchelle-Pensec V. Treatment of primary Sjögren syndrome. Nat Rev Rheumatol. 2016;12(8):456–471. doi:10.1038/nrrheum.2016.100
79. Strömbeck BE, Theander E, Jacobsson LTH. Effects of exercise on aerobic capacity and fatigue in women with primary Sjogren’s syndrome. Rheumatology. 2007;46(5):868–871. doi:10.1093/rheumatology/kem004
80. Hackett KL, Deane KHO, Strassheim V, et al. A systematic review of non-pharmacological interventions for primary Sjögren’s syndrome. Rheumatology. 2015;54(11):2025–2032. doi:10.1093/rheumatology/kev227
81. Miyamoto S, Valim V, Carletti L, et al. Supervised walking improves cardiorespiratory fitness, exercise tolerance, and fatigue in women with primary Sjögren’s syndrome: a randomized-controlled trial. Rheumatol Int. 2019;39(2):227–238. doi:10.1007/s00296-018-4213-z
82. Tarn J, Legg S, Mitchell S, Simon B, Ng W-F. The effects of noninvasive vagus nerve stimulation on fatigue and immune responses in patients with primary Sjögren’s Syndrome. Neuromodulation. 2018. doi:10.1111/ner.12879
83. Hackett KL, Deane KHO, Newton JL, et al. Mixed-methods study identifying key intervention targets to improve participation in daily living activities in primary Sjögren’s Syndrome patients. Arthritis Care Res. 2018;70(7):1064–1073. doi:10.1002/acr.23536
84. Hackett K, Davies K, Lendrem D, Hargreaves B, Ng W, Newton J. Improvement in fatigue following a multidisciplinary, biopsychosocial intervention: data from 50 primary Sjögren’s syndrome patients (abstract). Clin Exp Rheumatol. 2018;36(3):112.
85. Zangi HA, Ndosi M, Adams J, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015;74(6):954–962. doi:10.1136/annrheumdis-2014-206807
86. Franek J. Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ont Health Technol Assess Ser. 2013;13(9):1–60.
87. Cramp F, Hewlett S, Almeida C, et al. Non-pharmacological interventions for fatigue in rheumatoid arthritis: A cochrane review. Cochrane Database Syst Rev. 2013;8(CD008322). doi:10.1002/14651858.CD008322.pub2.www.cochranelibrary.com
88. Hewlett S, Ambler N, Almeida C, et al. OP0139-HPR Reducing arthritis fatigue - clinical teams (RAFT) using cognitive-behavioural approaches: an rct. Annals of the Rheumatic Diseases. 2017;76:110. doi:10.1136/annrheumdis-2017-eular.1877.
89. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76(2):318–328. doi:10.1136/annrheumdis-2016-209724
90. Geraghty KJ, Blease C. Cognitive behavioural therapy in the treatment of chronic fatigue syndrome: A narrative review on efficacy and informed consent. J Health Psychol. 2018;23(1):127–138. doi:10.1177/1359105316667798
91. Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin Psychol Rev. 2015;37:1–12. doi:10.1016/j.cpr.2015.01.006
92.
93. Grossman S, Tagliavini LB. Managing Sjögren’s Syndrome. Home Heal Now. 2015;33(9):487–492. doi:10.1097/NHH.0000000000000295
94. Hackett KL, Gotts ZM, Ellis J, et al. An investigation into the prevalence of sleep disturbances in primary Sjögren’s syndrome: a systematic review of the literature. Rheumatology. 2017;56(4):570–580. doi:10.1093/rheumatology/kew443
95. Martínez MP, Miró E, Sánchez AI, et al. Cognitive-behavioral therapy for insomnia and sleep hygiene in fibromyalgia: a randomized controlled trial. J Behav Med. 2014;37(4):683–697. doi:10.1007/s10865-013-9520-y
96. Usmani ZA, Hlavac M, Rischmueller M, et al. Sleep disordered breathing in patients with primary Sjögren’s syndrome: a group controlled study. Sleep Med. 2012;13(8):1066–1070. doi:10.1016/j.sleep.2012.06.010
97. Virtanen AT, Haikarainen T, Raivola J, Silvennoinen O. Selective JAKinibs : prospects in Inflammatory and autoimmune diseases. BioDrugs. 2019; epub ahead of print. doi:10.1007/s40259-019-00333-w.
98. Strand V, Kremer JM, Gruben D, Krishnaswami S, Zwillich SH, Wallenstein GV. Tofacitinib in combination with conventional disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis : patient-reported outcomes from a phase III randomized controlled trial. Arthritis Care Res. 2017;69(4):592–598. doi:10.1002/acr.23004
99. Sekiguchi M, Iwasaki T, Kitano M, et al. Role of Sphingosine 1-Phosphate in the Pathogenesis of Sjögren’s Syndrome. J Immunol. 2008;180:1921–1928. doi:10.4049/jimmunol.180.3.1921
100. Mao-Draayer Y, Sarazin J, Fox D, Schiopu E, Arbor A, States U. The sphingosine-1-phosphate receptor: A novel therapeutic target for multiple sclerosis and other autoimmune diseases. Clin Immunol. 2017;175:10–15. doi:10.1016/j.clim.2016.11.008
101. Iftikhar I, Bittencourt L, Youngstedt S, et al. Comparative efficacy of CPAP, MADs, exercise-training, and dietary weight loss for sleep apnea: a network meta-analysis. Sleep Med. 2017;30:7–14. doi:10.1016/j.sleep.2016.06.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.