")
Back to Journals » Journal of Blood Medicine » Volume 13
Managing Fatigue in Patients with Paroxysmal Nocturnal Hemoglobinuria: A Patient-Focused Perspective
Authors Fattizzo B , Cavallaro F, Oliva EN , Barcellini W
Received 5 March 2022
Accepted for publication 23 May 2022
Published 17 June 2022 Volume 2022:13 Pages 327—335
DOI https://doi.org/10.2147/JBM.S339660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Bruno Fattizzo,1,2 Francesca Cavallaro,1,2 Esther Natalie Oliva,3 Wilma Barcellini1
1Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico - Haematology Unit, Milan, Italy; 2Università degli Studi di Milano - Department of Oncology and Hemato-Oncology, Milan, Italy; 3Grande Ospedale Metropolitano Bianchi Melacrino Morelli - Hematology Division, Reggio, Calabria, Italy
Correspondence: Bruno Fattizzo, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, via Francesco Sforza 35, Milan, 20100, Italy, Tel +39 3896873204, Email [email protected]
Abstract: The most frequently reported symptom in patients with paroxysmal nocturnal hemoglobinuria (PNH), a disease characterized by complement mediated hemolysis and chronic anemia, is “fatigue”. The latter seems the best word to communicate patient’ perception of personal health status and disease impact on daily living, namely quality of life (QoL). Objectivating QoL and grading patient’s fatigue is one of the most difficult medical tasks given the highly heterogeneous communication skills of patients and caregivers and the multitude of meanings that might be attributed to this term. Along with anemia, QoL in PNH is also affected by the emotional burden of a chronic life-long disease with heterogeneous treatment requirement, risk of hemolytic exacerbations (breakthrough hemolysis) and of thrombosis. In the last decade, structured surveys and scores have been adapted from cancer settings to evaluate fatigue and QoL in patients with PNH, and to assess the benefit of complement inhibitors in this setting. Eculizumab was the first drug utilized and was shown to improve QoL scores in the registrative trials. However, the intravenous fortnightly administration, the presence of residual anemia, and the risk of extravascular hemolysis are some of the unmet needs impacting QoL under eculizumab. Several novel drugs have been designed to improve patients’ convenience and alleviate anemia and fatigue. In this review, we focus on available studies that evaluated fatigue and QoL in PNH patients, and the effect of old and new therapeutic strategies.
Keywords: paroxysmal nocturnal hemoglobinuria, novel drugs, eculizumab, quality of life, fatigue
Introduction
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare condition characterized by chronic hemolysis resulting in anemia of various degree and fatigue, variably affecting quality of life (QoL). Additionally, PNH patients carry the emotional burden of a chronic life-long disease with heterogeneous treatment requirement, risk of hemolytic exacerbations (breakthrough hemolysis) and of thrombosis. A Patient-Reported Outcome (PRO) is any report of the status of a subject’s health condition (QoL and symptoms) that comes directly from the patient, without interpretation of the response by a clinician or anyone else.1 PROs are used as indicators for assessing health-related QoL (impacts of disease and its treatment and symptoms). Regarding therapy, the beneficial impact on survival and/or on a meaningful aspect of a patient’s life is fundamental, and health features affecting the way a patient feels or functions should be considered.2 Fatigue has been identified as a prevalent disturbance in PNH patients. There are many components of fatigue, one of which is anemia, as frequently shown in other diseases, particularly cancer. Objectivating and grading patient’s fatigue is one of the most difficult medical tasks given the highly heterogeneous communication skills of patients and caregivers and the multitude of meanings that might be attributed to this term. Clinicians usually evaluate patients’ QoL by simply asking them “how are you” during routine visits and the ability to elicit PROs varies between professionals. For this reason, there is a need for instruments to measure PROs. To aid the objective evaluation of QoL and the effect of treatment, the use of structured surveys has been implemented in the clinic. In this article, we will briefly address the unmet needs of PNH treatment and describe how novel therapies might fill the gap in patients’ management. Furthermore, we will focus on available reports that evaluate fatigue and QoL in PNH patients.
What is PNH?
PNH is a clonal disorder of the hematopoietic stem cell caused by acquired somatic mutations of PIGA gene. The latter encodes for a glycosyl-phosphatidylinositol (GPI) that anchors several molecules on the cellular membrane,3,4 including the complement inhibitory proteins CD55 (decay accelerating factor [DAF]) and CD59 (membrane inhibitor of reactive lysis [MIRL]). GPI deficiency results in complement-mediated intravascular hemolysis5–7 and thrombophilia, the main cause of morbidity and mortality in PNH. Chronic anemia mainly results in fatigue, shortness of breath on exertion, and reduction of physical activity, whilst dark urine are the typical symptom of intravascular hemolysis. Along with these, a variety of signs may be present including abdominal pain, bloating, back pain, headaches, esophageal spasms, erectile dysfunction, and fatigue, but also thrombosis of venous and arterial system, renal failure, pulmonary hypertension, so that PNH has been referred to as “the great impersonator”.3 Standard and high-sensitivity flow cytometric procedures for detecting PNH cells are the gold standard for disease diagnosis.8 Three different PNH cellular phenotypes have been recognized: type I with normal, PNH II with partial expression, and PNH III with absence of GPI-anchored proteins.9 The heterogeneity of PNH clone size (ie, the percentage of PNH+ cells), and the variable presence of complement activating conditions (infections, trauma, pregnancy, surgery) explain the different extent of hemolysis, and anemia, observed in the clinic. The degree of anemia is further affected by the characteristic association of PNH with bone marrow failure syndromes, namely aplastic anemia (AA), and with myelodysplastic syndromes (MDS), particularly hypoplastic ones that show several similarities with AA.10–12 Transfusion-dependent anemia along with thrombosis, PNH-related symptoms, and pregnancy (that increases thrombotic risk affecting maternal and fetal outcome), has been the main reason to start therapy with complement inhibitors. The latter revolutionized the natural history of the disease and re-drew the survival curve of PNH patients to that of the general population.
PNH Treatment and Its Limitations
Eculizumab (Soliris®, Alexion Pharmaceutics, Inc) has been the first complement inhibitor studied in PNH and was approved in 2007. It is a humanized monoclonal antibody that binds the C5 complement fraction, preventing its activation to C5b by the C5 convertase thus inhibiting the formation of the membrane attack complex.13 Treatment with eculizumab reduced transfusions, improved anemia and fatigue, and ameliorated PNH symptoms. Furthermore, it reduced thrombosis occurrence and improved survival.14–17 Additionally, eculizumab appeared safe during pregnancy, and ameliorated fetal-maternal outcomes, although formal toxicology studies in pregnancy are lacking.18 The recommended maintenance dose of eculizumab is fixed (900 mg every 2 weeks ± 2 days) intravenously. This implies a high level of medicalization of PNH patients with consequent interference with working and leisure activities. Further unmet needs include patients with residual anemia, the occurrence of hemolytic flares (breakthrough hemolysis, BTH), the presence of an underlying bone marrow failure on which eculizumab has no effect, and the increased risk of infections. All of these clinical issues further burden patients’ QoL. Regarding residual anemia,19 up to 25% of cases will still need blood transfusions. Along with concomitant conditions such as nutrients deficiencies and impaired erythropoiesis due to bone marrow failure, extravascular hemolysis of PNH erythrocytes as a consequence of C3 opsonization should be considered.3,19–21 This happens since the complement cascade upstream C5 is not blocked by eculizumab, and C3 continued to be produced and deposits on PNH-erythrocytes. C3 coated erythrocytes are then cleared by the monocyte/macrophage system, mainly in the liver. Clinically, extravascular hemolysis is evidenced by increased reticulocyte counts, indirect hyperbilirubinemia, and decreased haptoglobin in a patient with almost normal LDH values; additionally, the false positivity of direct antiglobulin test with anti-complement anti-sera provides a further demonstration. Moreover, patients of Asian ancestry (ie, Japanese, Han Chinese) may harbor a polymorphism of C5 (Arg885His) that impairs response to eculizumab.22 Homozygosity for the low-affinity allele L of the complement receptor gene CR1 has been associated with poor response to eculizumab.23,24 Regarding BTH, it may occur just before the subsequent infusion (pharmacokinetic PK BTH), or during complement activating conditions (pharmacodynamic PD BTH). The first situation may be managed by increasing eculizumab dose or frequency of administration (PK), and the second one requires a prompt control of the underlying trigger (PD). Concerning infectious risk, patients treated with eculizumab must be vaccinated prior to initiation of therapy to prevent the risk of Neisseria meningitidis13 A, B, C, W and Y serogroups and in some countries, additional life-long antibiotic prophylaxis is prescribed. Despite this, meningococcal sepsis may still occur, and even fatal episodes have been reported.25 Finally, eculizumab does not eliminate PNH clone but only prevents its complement mediated destruction. As a result, eculizumab needs to be administered lifelong in most cases further giving the patients the idea of a chronic “incurable” disease, with important impact on perceived QoL. Given these drawbacks, there is a need for new agents and approaches to optimally control PNH disease activity, as discussed thereafter.
Novel Therapies
Several novel complement inhibitors are under study. The new approaches aim at increasing the drug half-life or subcutaneous (sc) administration of C5 inhibitors (ie, ravulizumab iv, crovalimab sc), at producing small molecules that may be given orally, and at targeting the complement cascade upstream to C5 (including anti-C1, anti-C3 pegcetacoplan, and the alternative pathway factors B and D inhibitors iptacopan and danicopan).26,27 An innovative approach is the use of small interfering RNA (siRNA) molecules capable of inhibiting C5 synthesis, and very preliminary gene therapy.28 Preclinical and clinical trials showed that novel C5 inhibitors (ECU biosimilars, ECU with longer half-life such as ravulizumab IV or sc,29 small molecules,30,31 and siRNA32) are effective in inhibiting complement-mediated hemolysis and imply more manageable administration routes/schedules thus improving patient convenience. In particular, ravulizumab was not inferior to eculizumab and reduced the occurrence of BTH in two clinical trials,29,33 and some of the new agents proved effective in patients with C5 polymorphisms (ie, crovalimab).27 Importantly, proximal inhibitors (anti-C1 iv, anti-C3 sc, and oral anti-factor B and D) were effective both in naïve patients and in those with suboptimal response to eculizumab, significantly reducing C3 mediated extravascular hemolysis thus reducing residual anemia and fatigue. These agents appear very promising and are being developed both in combination with eculizumab and as single agents.27
Bone Marrow Transplant (BMT)
Except for anecdotal cases,34–36 PNH is a lifelong disease requiring long-term treatment (if indicated), and this represents one of the main factors affecting patient’ perception of severity and illness. The only curative therapy is allogeneic bone marrow transplant (BMT). BMT outcome significantly improved with the introduction of reduced intensity conditioning, and the addition of eculizumab has reduced morbidity and mortality linked to PNH;37 however, it remains a demanding, potentially life-threatening procedure that is limited to selected cases. As a matter of fact, a large European study comparing transplanted versus non-transplanted PNH patients, showed a worse survival after BMT if the indication was life-threatening thrombosis, whilst survival was not inferior if the indication was AA.38 On the whole, BMT is indicated in patients with PNH and severe AA (below 40 years and with available donor) or MDS (high-risk patients or low-risk MDS with life-threatening cytopenias) and has the potential to eradicate both AA/MDS and the PNH clone.
PNH Complications
Not only the occurrence but even the fear of PNH complications, further impact QoL and may lead to a feeling of “life limitation” and “frailty” in these patients. The disease is dominated by increased thrombotic risk, reported in as many as 40% of patients, possibly being the first sign at presentation.39 Thrombosis mainly affects the venous district and may also occur in atypical sites, including the cerebral, mesenteric, and renal vessels. Hepatic veins may also be involved in the so-called Budd–Chiari syndrome.40,41 Some studies have suggested that larger PNH clones correlate with increased thrombotic risk,42 however, many adjunctive congenital (eg, factor V Leiden or factor II mutations, protein C and S deficiencies, etc.) or acquired risk factors (eg, cigarette smoke, diabetes, obesity, estro-progestin compounds, pregnancy, surgery, prolonged immobilization, etc.) may contribute to thrombosis in this setting and deserve consideration. PNH can also be complicated by infectious events, either related to the coexistence of BMF and immunosuppression, or to complement inhibition. As stated before, anti-Neisseria meningitidis vaccinations are mandatory before eculizumab, and the addition of anti-Streptococcus pneumoniae and anti-Hemophilus influenzae vaccines have been required with novel agents in clinical trials. However, not all vaccinated subjects will get proper immunization and antibody titers are not routinely evaluated. Therefore, patient education remains pivotal for prompt recognition and treatment of infectious episodes. Additionally, infections may trigger PD BTH, further complicating the clinical picture. By a careful discussion of available strategies to prevent/promptly manage thrombotic and infectious risk, clinicians may aid PNH patients to get back to their daily lives.
PNH, QoL and Measures
Besides treating clinical manifestations and preventing major complications, the improvement of patients’ QoL is an emerging objective in the current management of PNH. QoL is defined by World Health Organisation (WHO) as
An individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.43
As stated above, QoL of PNH patients is usually reduced because of both PNH-related symptoms and complications, but also due to treatment-related issues that requires frequent hospital visits heavily interfering with working and leisure activities.44,45 As of today, there are no specific scores that have been fully validated to measure QoL in PNH so that questionnaires designed for cancer patients are usually administered in PNH clinical trials. The most frequent instruments are the Functional assessment of chronic illness (FACIT) Fatigue questionnaire (a 40-items score that determines fatigue’s impact on QoL)46 and the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30 Global Health Status/QOL (a questionnaire suitable for measuring cancer patients’ physical, psychological and social functions).47 FACIT-F scores range from 0 to 52, with lower scores indicating greater fatigue. EORTC-QLQ-C30 domain scales range from 0 to 100, with lower scores indicating worse QoL and higher scores for symptom scales indicating worse symptoms. Data from the International PNH Registry reveals an impaired QoL in PNH patients, with median scores for EORTC QLQ-C30 and FACIT-F score of 58.3 (41.7, 75.0) and 34.0 (27.0, 40.0), respectively.45 More recently, other scores have been developed to investigate in a better and more specific way PNH impact on QoL and the perceived benefit of treatment on QoL. The PNH-SQ (Symptom Questionnaire) is a novel questionnaire evaluating the presence and severity of 10 PNH-related symptoms over 24 hours.48 Moreover, a PNH/aplastic anemia (AA) specific QoL questionnaire has been created as a specific disease PRO measure, although psychometric evaluations are still undergoing.49 Lastly, PNH Patient Preference Questionnaire (PNH-PPQ), a 11-item questionnaire, has been validated to assess patients’ preferences in the context of the clinical trials comparing eculizumab with its long half-life analogue ravulizumab.50 As a matter of fact, the availability of several novel drugs will allow tailored therapy (ie, the choice of a specific compound for a specific patient) and defining patient’s preference also in regards to QoL and improvement of fatigue will be pivotal.
Assessment of QoL in PNH Clinical Trials
Tables 1 and 2 report the main findings regarding PNH therapies and QoL. Concerning eculizumab, in the Phase 3 TRIUMPH study,16,51 patients in the eculizumab arm had a mean increase in FACIT-F score of 6.4±1.2 points from baseline to week 26, significantly higher than the placebo arm. Eculizumab group also showed a significant improvement in EORTC QLQ-C30 score in various scales: global health, functioning (5 scales/5), symptom (2 scales/3) and single-item measures (3/6). Results from the phase 3 SHEPHERD study were concordant, with a mean increase in FACIT-F score of 12.1±1.01 from baseline to week 52, and EORTC QLQ-C30 improvement in global health, functioning (5 scales/5), symptoms (3 scales/3) and single-item measures (4/6).14,51 More recently, Ueda et al published data from the post-marketing surveillance of eculizumab in Japan:52 they showed a significant amelioration after 1 year of eculizumab therapy both in FACIT-F score, with a mean change from baseline of 9.4, and in EORTC QLQ-C30, with a mean change from baseline of 21.4 and 16.3 points for global health status and physical functioning, respectively. Furthermore, they noted that fatigue showed the highest improvement among symptoms (significant amelioration of 1/3 scales for symptoms), along with amelioration of dyspnea, insomnia and appetite loss (3 scales/6 single-item measures).
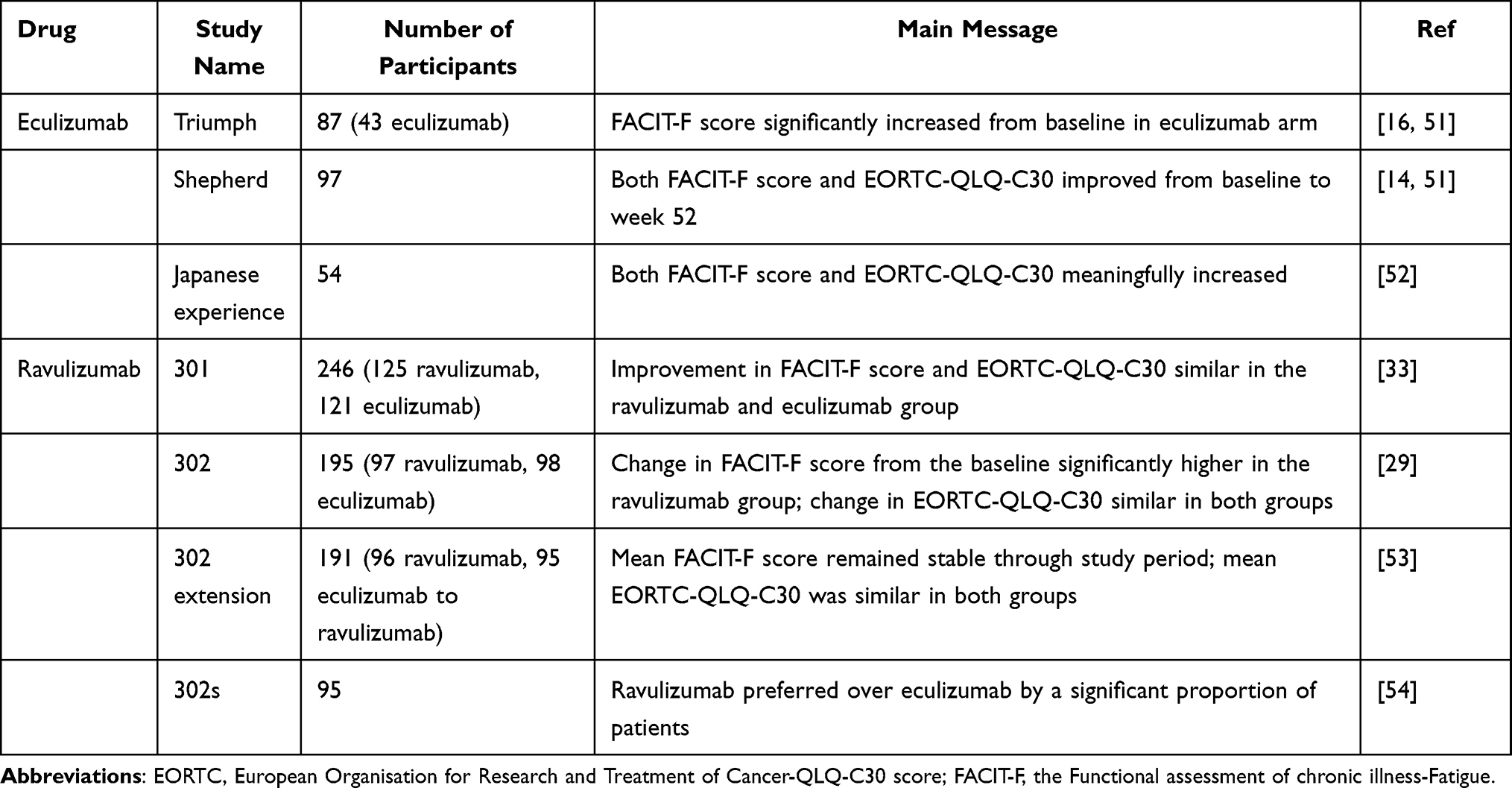 |
Table 1 Quality of Life (QoL) and Paroxysmal Nocturnal Hemoglobinuria (PNH) Therapy: Eculizumab and Ravulizumab |
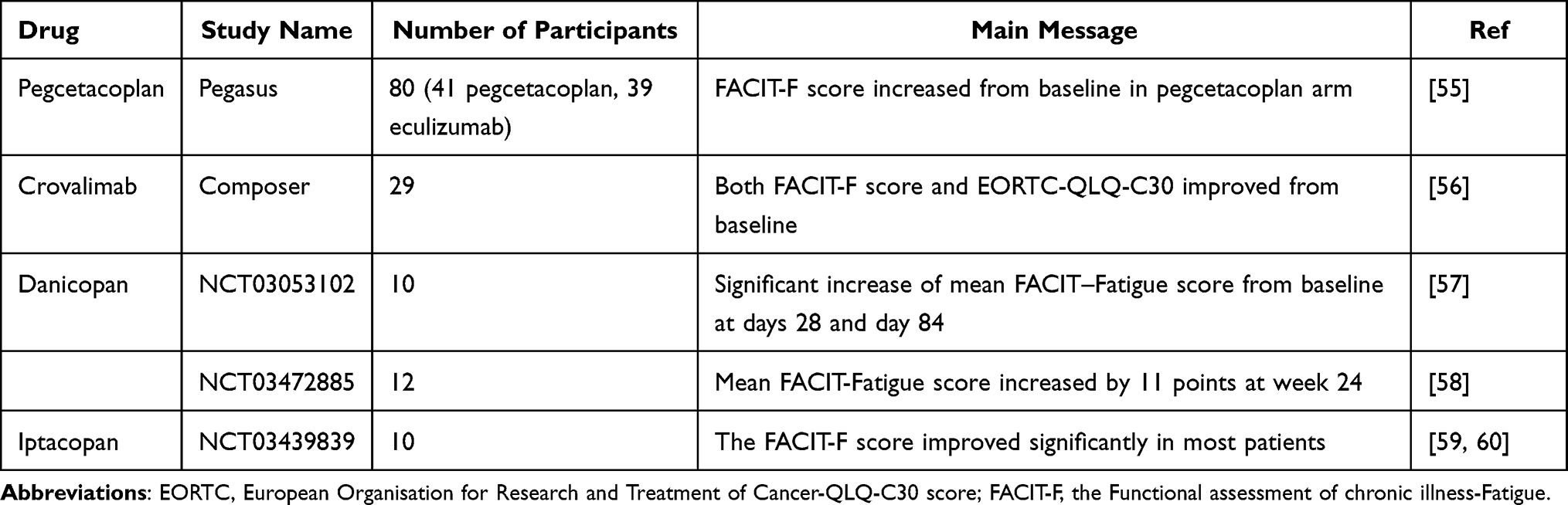 |
Table 2 Quality of Life (QoL) and Paroxysmal Nocturnal Hemoglobinuria (PNH) Therapy: New Drugs |
The long-lasting anti-C5 ravulizumab achieved an improvement in fatigue and QoL as well. The 301 study,33 assessing the non-inferiority of ravulizumab to eculizumab in patients naïve from complement inhibitors, demonstrated a similar increase in FACIT-F and EORTC-QLQ-C30 score both in the ravulizumab and eculizumab group. However, a higher percentage of patients in the ravulizumab arm obtained a ≥3-point improvement in FACIT-F score and a ≥ 10-point improvement in the EORTC QLQ-C30 score (global health status/QoL, physical functioning and fatigue). The subsequent 302 study,29 conducted in patients previously treated with eculizumab, showed a statistically significant change from the baseline in FACIT-F score in ravulizumab versus eculizumab group, while EORTC QLQ-C30 scores remained stable in both groups. In the 302 extension study,53 patients continued on ravulizumab or were switched from eculizumab to ravulizumab by week 26: mean FACIT-F and EORTC QLQ-C30 scores remained stable from week 26 to week 52, suggesting that the switch from eculizumab to ravulizumab did not affect fatigue or QoL. Finally, the 302s study54 included patients from the registrative trial with the aim of assessing the preference for ravulizumab or eculizumab using the PNH-PPQ survey: 93% of the patients preferred ravulizumab over eculizumab, 6% had no preferences and 1% preferred eculizumab. The main reasons for ravulizumab preference were the frequency of infusions (98%; this was selected as the most relevant factor determining treatment choice), the ability to plan activities (98%), the improvement in overall QoL (88%), the convenience of receiving treatment (85%) and the effectiveness of medication until the next infusion (78%). Regarding the latter, PK BTH seems to significantly impact QoL in a patient perspective analysis,50 particularly with eculizumab that is not adjusted on patient’s body weight or individual response. Conversely, ravulizumab decreased PNH-related symptoms for a longer duration, including those occurring pre-administration and consistent with the longer half-life and effective plasma concentrations of the drug.54
In the last few years, different therapies for PNH have been studied, all of them showing an improvement in terms of fatigue or QoL. Pegcetacoplan, a C3 inhibitor, obtained an increase of FACIT-F score of 9.2 points versus a decrease of 2.7 points with eculizumab, with 73% of patients in the pegcetacoplan arm achieving an increase of at least 3 points (versus 0% in the eculizumab arm).55 Data from the COMPOSER study showed that both FACIT-F score and EORTC QLQ-C30 scores improved at week 10 with crovalimab (of 8.8 and 21.1 points, respectively) a subcutaneous C5 inhibitor also active in patients with the Japanese polymorphism.56 Danicopan, an oral factor D inhibitor, achieved an increase of FACIT-F score both when used in patients naïve from complement inhibitors (34 points at baseline, increased by 9 and 13 points at days 28 and 85, p<0.05) and when added to eculizumab (mean FACIT-F increased by 11 points at week 24).57,58 Finally, latest data from trials evaluating iptacopan, an oral factor B inhibitor, showed a significant amelioration of FACIT-F score.59,60
Conclusions
PNH-related fatigue and symptoms are a puzzle of physical and psychological constraints to patients’ QoL. These include inability to perform working and leisure activities, but also a detrimental effect on daily living. To better assess these issues, clinicians may profit of several scores developed for chronic anemia due to cancer and other conditions, but also of the advent of novel PNH specific PRO measures that are being evaluated in clinical trials. The latter will allow to objectivate and measure QoL in PNH patients while also putting them and their expectations at the center when designing clinical trials. As a matter of fact, eculizumab revolutionized PNH management in the last 15 years, and also ameliorated QoL. However, recent studies with novel drugs clearly showed that the boundaries of QoL in PNH patients may be pushed far beyond those reached with eculizumab. Given the variety of novel compounds, including intravenous, subcutaneous, and oral drugs, with different half-lives, availability of auto-injection, and the potential to differently improve residual anemia in PNH, patients’ perspective and efficacy on QoL will become more and more crucial in treatment selection. Despite the advancement in disease treatment, the lifelong nature of PNH and the occurrence of BTH and thrombotic and infectious complications still burden the clinical course and affect individual health perception. Only education of clinicians and patients, along with maximization of preventive measures will improve the management of these unmet clinical needs.
Data Sharing Statement
All data are available within the manuscript and further may be available upon reasonable request to the corresponding author.
Consent for Publication
All Authors approved present submission.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding sources to declare.
Disclosure
Dr Bruno Fattizzo received consultancy honoraria and speaker bureau from Alexion, Amgegen, Annexon, Jannsen, and Novartis.
Dr Esther Natalie Oliva reports personal fees from Celgene, Janssen, personal fees, Daiichi, and Alexion, outside the submitted work.
Dr Wilma Barcellini received consultancy honoraria and speaker bureau from Agios, Alexion, Amgegen, Annexon, Jannsen, and Novartis.
Dr Francesca Cavallaro declares no conflicts of interest to disclose.
References
1. US Food and Drug Administration. Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims.
2. Walton MK, Powers JH
3. Parker CJ. Update on the diagnosis and management of paroxysmal nocturnal hemoglobinuria. Hematol Am Soc Hematol Educ Program. 2016;2016(1):208–216. doi:10.1182/asheducation-2016.1.208
4. Kinoshita T, Inoue N, Takeda J. Defective glycosyl phosphatidylinositol anchor synthesis and paroxysmal nocturnal hemoglobinuria. Adv Immunol. 1995;60:57–103.
5. Parker CJ. Hemolysis in PNH. In: Young NS, Moss J, editors. Paroxysmal Nocturnal Hemoglobinuria and the Glycosylphosphatidylinositol-Linked Proteins. San Diego: Academic Press; 2000:49–100.
6. Inoue N, Izui-Sarumaru T, Murakami Y, et al. Molecular basis of clonal expansion of hematopoiesis in 2 patients with paroxysmal nocturnal hemoglobinuria (PNH). Blood. 2006;108(13):4232–4236. doi:10.1182/blood-2006-05-025148
7. Endo M, Ware RE, Vreeke TM, et al. Molecular basis of the heterogeneity of expression of glycosyl phosphatidylinositol anchored proteins in paroxysmal nocturnal hemoglobinuria. Blood. 1996;87(6):2546–2557. doi:10.1182/blood.V87.6.2546.bloodjournal8762546
8. Dezern AE, Borowitz MJ. ICCS/ESCCA consensus guidelines to detect GPI-©deficient cells in paroxysmal nocturnal hemoglobinuria (PNH) and related disorders part 1—clinical utility. Cytometry B Clin Cytom. 2018;94:16–22. doi:10.1002/cyto.b.21608
9. Gurnari C, Pagliuca S, Patel BJ, et al. Implication of PIGA genotype on erythrocytes phenotype in paroxysmal nocturnal hemoglobinuria. Leukemia. 2021;35(8):2431–2434. doi:10.1038/s41375-020-01113-0
10. Bono E, McLornan D, Travaglino E, et al. Clinical, histopathological and molecular characterization of hypoplastic myelodysplastic syndrome. Leukemia. 2019;33(10):2495–2505. doi:10.1038/s41375-019-0457-1
11. Fattizzo B, Serpenti F, Barcellini W, Caprioli C. Hypoplastic myelodysplastic syndromes: just an overlap syndrome? Cancers. 2021;13(1):132. doi:10.3390/cancers13010132335
12. Fattizzo B, Levati GV, Giannotta JA, et al. Low-risk myelodysplastic syndrome revisited: morphological, autoimmune, and molecular features as predictors of outcome in a single center experience. Front Oncol. 2022;12:795955. doi:10.3389/fonc.2022.795955
13. Parker C. Eculizumab for paroxysmal nocturnal haemoglobinuria. Lancet. 2009;373(9665):759–767. doi:10.1016/S0140-6736(09)60001-5
14. Brodsky RA, Young NS, Antonioli E, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840–1847. doi:10.1182/blood-2007-06-094136
15. Hillmen P, Hall C, Marsh JC, et al. Effect of eculizumab on hemolysis and transfusion requirements in patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2004;350(6):552–559. doi:10.1056/NEJMoa031688
16. Hillmen P, Young NS, Schubert J, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355(12):1233–1243. doi:10.1056/NEJMoa061648
17. Kelly RJ, Hill A, Arnold LM, et al. Long-term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained©efficacy and improved survival. Blood. 2011;117(25):6786–6792. doi:10.1182/blood-2011-02-333997
18. Kelly RJ, Hochsmann B, Szer J, et al. Eculizumab in pregnant patients with paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2015;373 (11):1032–1039. doi:10.1056/NEJMoa1502950
19. Berzuini A, Montanelli F, Prati D. Hemolytic anemia after eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2010;363 (10):993–994. doi:10.1056/NEJMc1005108
20. Risitano AM, Notaro R, Luzzatto L, Hill A, Kelly R, Hillmen P. Paroxysmal nocturnal hemoglobinuria–hemolysis before and after eculizumab. N Engl J Med. 2010;363(23):2270–2272. doi:10.1056/NEJMc1010351
21. Risitano AM, Notaro R, Marando L, et al. Complement fraction 3 binding on erythrocytes as additional mechanism of disease in paroxysmal nocturnal hemoglobinuria patients treated by eculizumab. Blood. 2009;113(17):4094–4100. doi:10.1182/blood-2008-11-189944
22. Nishimura J, Yamamoto M, Hayashi S, et al. Genetic variants in C5 and poor response to eculizumab. N Engl J Med. 2014;370(7):632–639. doi:10.1056/NEJMoa1311084
23. Luzzatto L. Recent advances in the pathogenesis and treatment of paroxysmal nocturnal hemoglobinuria. F1000Res. 2016;23(5):F1000Faculty Rev–209.
24. Rondelli T, Risitano AM, Pefault de Latour R, et al. Polymorphism of the complement receptor 1 gene correlates with the hematologic response to eculizumab in patients with paroxysmal nocturnal hemoglobinuria. Haematologica. 2014;99(2):262–266. doi:10.3324/haematol.2013.090001
25. Hillmen P, Muus P, Röth A, et al. Long-term safety and efficacy of sustained eculizumab treatment in patients with paroxysmal nocturnal haemoglobinuria. Br J Haematol. 2013;162(1):62–73. doi:10.1111/bjh.12347
26. Fattizzo B, Kulasekararaj AG. Second-generation C5 inhibitors for paroxysmal nocturnal hemoglobinuria. BioDrugs. 2020;34:149–158. doi:10.1007/s40259-019-00401-1
27. Risitano AM, Marotta S. Toward complement inhibition 2.0: next generation anticomplement agents for paroxysmal nocturnal hemoglobinuria. Am J Hematol. 2018;93:564–577. doi:10.1002/ajh.25016
28. Robert D, Mahon FX, Richard E, Etienne G, de Verneuil H, Moreau-Gaudry FA. SIN lentiviral vector containing PIGA cDNA allows long-term phenotypic correction of CD34+-derived cells from patients with paroxysmal nocturnal hemoglobinuria. Mol Ther. 2003;7:304–316.
29. Kulasekararaj AG, Hill A, Rottinghaus ST, et al. Ravulizumab (ALXN1210) vs eculizumab in C5-inhibitor-experienced adult patients with PNH: the 302 study. Blood. 2019;133:540–549. doi:10.1182/blood-2018-09-876805
30. Schubart A, Anderson K, Mainolfi N, et al. Small-molecule factor B inhibitor for the treatment of complement-mediated diseases. Proc Natl Acad Sci USA. 2019;116:7926–7931. doi:10.1073/pnas.1820892116
31. Maibaum J, Liao SM, Vulpetti A, et al. Small-molecule factor D inhibitors targeting the alternative complement pathway. Nat Chem Biol. 2016;12:1105–1110. doi:10.1038/nchembio.2208
32. Borodovsky A, Yucius K, Sprague A, et al. Development of RNAi therapeutics targeting the complement pathway. Blood. 2013;122:2471. doi:10.1182/blood.V122.21.2471.2471
33. Lee JW, Sicre de Fontbrune F, Wong Lee Lee L, et al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood. 2019;133(6):530–539. doi:10.1182/blood-2018-09-876136
34. Babushok DV, Stanley N, Xie HM, et al. Clonal replacement underlies spontaneous remission in paroxysmal nocturnal haemoglobinuria. Br J Haematol. 2017;176(3):487–490. doi:10.1111/bjh.13963
35. Ferla V, Zaninoni A, Fattizzo B, Fermo E, Gianelli U, Barcellini W. Paroxysmal nocturnal hemoglobinuria with spontaneous clinical remission. EurJ Intern Med. 2017;43:e11–e14. doi:10.1016/j.ejim.2017.04.011
36. Gurnari C, Pagliuca S, Kewan T, et al. Is nature truly healing itself? Spontaneous remissions in paroxysmal nocturnal hemoglobinuria. Blood Cancer J. 2021;11(11):187. doi:10.1038/s41408-021-00582-5
37. Brodsky RA. How I treat paroxysmal nocturnal hemoglobinuria. Blood. 2021;112:6522–6527.
38. Peffault de Latour R, Schrezenmeier H, Bacigalupo A, et al. Allogeneic stem cell transplantation in paroxysmal nocturnal hemoglobinuria. Haematologica. 2012;97(11):1666–1673. doi:10.3324/haematol.2012.062828
39. Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood. 2013;121:4985–4996. doi:10.1182/blood-2012-09-311381
40. Gurnari C, Colak C, Zawit M, Maciejewski JP. Chronic Budd-Chiari syndrome in paroxysmal nocturnal haemoglobinuria. Lancet. 2021;398 (10304):e14. doi:10.1016/S0140-6736(21)01542-7
41. Plessier A, Esposito-Farèse M, Baiges A, et al. Paroxysmal nocturnal hemoglobinuria and vascular liver disease: eculizumab therapy decreases mortality and thrombotic complications. Am J Hematol. 2022;97(4):431–439. doi:10.1002/ajh.26474
42. Fattizzo B, Dunlop A, Ireland RM, et al. Prognostic and predictive impact of small PNH clones in a large cohort of patients with myelodysplastic syndromes and aplastic anemia: a single-center experience. Blood. 2018;132:3870. doi:10.1182/blood-2018-99-116772
43. The WHOQOL Group. World health organization quality of life assessment. What quality of life? World Health Forum. 1996;17(4):354–356.
44. Bektas M, Copley-Merriman C, Khan S, Sarda SP, Shammo JM. Paroxysmal nocturnal hemoglobinuria: patient journey and burden of disease. J Manag Care Spec Pharm. 2020;26(12–bSuppl):S8–S14. doi:10.18553/jmcp.2020.26.12-b.s8
45. Schrezenmeier H, Röth A, Araten DJ, et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the International PNH Registry. Ann Hematol. 2020;99(7):1505–1514. doi:10.1007/s00277-020-04052-z
46. Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. doi:10.1186/1477-7525-1-79
47. Aaronson NK, Ahmedzai S, Bergman B, et al. The European-Organization-for-Research-and-Treatment-of-Cancer QLQ-C30 – a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. doi:10.1093/jnci/85.5.365
48. Daly RP, Jalbert JJ, Keith S, Symonds T, Shammo J. A novel patient-reported outcome instrument assessing the symptoms of paroxysmal nocturnal hemoglobinuria, the PNH-SQ. J Patient Rep Outcomes. 2021;5(1):102. doi:10.1186/s41687-021-00376-0
49. Groth M, Singer S, Niedeggen C, et al. Development of a disease-specific quality of life questionnaire for patients with aplastic anemia and/or paroxysmal nocturnal hemoglobinuria (QLQ-AA/PNH)-report on phases I and II. Ann Hematol. 2017;96(2):171–181. doi:10.1007/s00277-016-2867-8
50. Kaiser K, Yount SE, Martens CE, et al. Assessing preferences for rare disease treatment: qualitative development of the Paroxysmal Nocturnal Hemoglobinuria Patient Preference Questionnaire (PNH-PPQ©). Patient Prefer Adherence. 2020;5(14):705–715. doi:10.2147/PPA.S233830
51. Schubert J, Hillmen P, Röth A, et al.; TRIUMPH Study Investigators. Eculizumab, a terminal complement inhibitor, improves anaemia in patients with paroxysmal nocturnal haemoglobinuria. Br J Haematol. 2008;142(2):263–272. doi:10.1111/j.1365-2141.2008.07183.x
52. Ueda Y, Obara N, Yonemura Y, et al. Effects of eculizumab treatment on quality of life in patients with paroxysmal nocturnal hemoglobinuria in Japan. Int J Hematol. 2018;107(6):656–665. doi:10.1007/s12185-018-2409-3
53. Kulasekararaj AG, Hill A, Langemeijer S, et al. One-year outcomes from a phase 3 randomized trial of ravulizumab in adults with paroxysmal nocturnal hemoglobinuria who received prior eculizumab. Eur J Haematol. 2021;106(3):389–397. doi:10.1111/ejh.13564
54. Peipert JD, Kulasekararaj AG, Gaya A, et al. Patient preferences and quality of life implications of ravulizumab (every 8 weeks) and eculizumab (every 2 weeks) for the treatment of paroxysmal nocturnal hemoglobinuria. PLoS One. 2020;15(9):e0237497. doi:10.1371/journal.pone.0237497
55. Hillmen P, Szer J, Weitz I, et al. Pegcetacoplan versus eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2021;384(11):1028–1037. doi:10.1056/NEJMoa2029073
56. Röth A, Nishimura JI, Nagy Z, et al. The complement C5 inhibitor crovalimab in paroxysmal nocturnal hemoglobinuria. Blood. 2020;135(12):912–920. doi:10.1182/blood.2019003399
57. Risitano AM, Kulasekararaj AG, Lee JW, et al. Danicopan: an oral complement factor D inhibitor for paroxysmal nocturnal hemoglobinuria. Haematologica. 2021;106(12):3188–3197. doi:10.3324/haematol.2020.261826
58. Kulasekararaj G, Risitano AM, Maciejewski JP, et al. Phase 2 study of danicopan in patients with paroxysmal nocturnal hemoglobinuria with an inadequate response to eculizumab. Blood. 2021;138(20):1928–1938. doi:10.1182/blood.2021011388
59. Risitano AM, Röth A, Soret J, et al. Addition of iptacopan, an oral factor B inhibitor, to eculizumab in patients with paroxysmal nocturnal haemoglobinuria and active haemolysis: an open-label, single-arm, phase 2, proof-of-concept trial. Lancet Haematol. 2021;8(5):e344–e354.doi:10.1016/S2352-3026(21)00028-4
60. Jang JH, Wong LL, Ko BS, et al. 12-month analysis of a Phase 2 study of iptacopan (LNP023) monotherapy for paroxysmal nocturnal hemoglobinuria.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.