")
Back to Journals » Journal of Healthcare Leadership » Volume 12
Managing Complex Healthcare Change: A Qualitative Exploration of Current Practice in New South Wales, Australia
Authors Le-Dao H , Chauhan A , Walpola R , Fischer S , Schwarz G , Minbashian A, Munro A, D'Arcy E , Allan J , Harrison R
Received 6 August 2020
Accepted for publication 3 November 2020
Published 10 December 2020 Volume 2020:12 Pages 143—151
DOI https://doi.org/10.2147/JHL.S274958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Russell Taichman
Huong Le-Dao,1 Ashfaq Chauhan,1 Ramesh Walpola,1 Sarah Fischer,2,3 Gavin Schwarz,4 Amirali Minbashian,4 Alice Munro,5 Ellie D’Arcy,5 Julaine Allan,6 Reema Harrison1
1School of Population Health, University of New South Wales, Sydney, New South Wales, 2052, Australia; 2Clinical Excellence Commission, New South Wales Health, Sydney, 2065, Australia; 3School of Psychology, Deakin University, Sydney, 3220, Australia; 4Business School, University of New South Wales, Sydney, New South Wales, 2052, Australia; 5Western New South Wales Local Health District, Bathurst, New South Wales 2795, Australia; 6School of Health and Society, University of Wollongong, Wollongong, New South Wales 2500, Australia
Correspondence: Reema Harrison Room 229, School of Population Health
University of New South Wales, 2052, Australia
Tel +61 2 93853324
Email [email protected]
Purpose: As the cost of healthcare continues to rise, healthcare organizations internationally are seeking long-term solutions to eradicate inefficiency, achieve value-based healthcare, and minimize hospital inpatient services. This requires transformational change in healthcare organizations, and associated change management and leadership capability at multiple levels. Despite the critical need for effective change leadership and management in healthcare, limited evidence exists that this currently occurs in addition to the capability and capacity for managing change in health systems.
Methods: Semi-structured interviews were undertaken with 16 healthcare managers and leaders at a range of levels in nine healthcare organizations across the public health system of one Australian state (New South Wales), including metropolitan, regional and rural geographical areas. Thematic content analysis was undertaken with the emergent data.
Results: Four key themes emerged from the data: 1) lack of adoption of frameworks and methods for change management for any scope or scale of change, 2) inadequate resources for delivering, managing and leading change, 3) insufficient leadership, capacity and capability in managing change, and 4) the need for support and culture that supports change at all levels of the system.
Conclusion: Ensuring dedicated resources for change and sufficient capacity and capability amongst health professionals and managers at every level in a health system are required for effective management of change. An enabling culture for change, supported by adequate education and training in change leadership and management are critical in order for the benefits of health service and system changes to be realised.
Keywords: transformation, leadership, capacity, capability, culture, change management
Introduction
Increasing health system expenditure is a major concern for governments internationally. Globally, the largest contributors to the increasing cost of health care are a combination of the rising costs of pharmaceuticals, the increasing cost of health service provision, and the aging population.1 Ongoing budget constraints and the limited resources which can be allocated to health expenditure require health systems to develop long-term solutions to eradicate operational and economic inefficiencies whilst maintaining the delivery of high quality and safe care.2 As such, health agencies have had to undertake significant transformations in the manner in which health services are being delivered.
Transformation is a dynamic process that can be defined as “a change that alters an entire organization, including strategy, structure, core processes, power distribution, controls systems, culture, and people’s work”.3 A key feature of this process is that it occurs across all levels of an organization. However, across health settings, the operational complexities of delivering healthcare, entrenched practitioner behaviors, and deep-rooted hierarchies have resulted in practitioner resistance to change.4 Resistance to change may also be from initiative fatigue, experience of previous programmes that have been abandoned, or simply disagreeing that the proposed change is a good idea. Given the impetus for reducing economic and operational inefficiencies, it is imperative for leaders of any health organization to take an active role in supporting and managing the change process.5,6 Despite this recognition, previous studies have identified that many adopt a one-size-fits-all approach to managing change and that approach is often unsuccessful in bringing about change.7,8 Managing healthcare change has to utilize a change method that is fit-for-purpose and tailored for the specific system and setting.9 In a complex adaptive system such as healthcare, identifying the optimal change methodology may be challenging, but there is evidence that the guiding principles of best practice in change management are applicable.10
The Australian healthcare system employs a hybrid model between federal and state governments, supported by the private sector.11 The federal government funds primary care, specialist services and medicines, with state governments responsible for funding their respective public hospitals and some outpatient services. As such, the rising cost of healthcare is born primarily by all states and territories. For the most populous state – New South Wales (NSW) – the state Government funded a health budget of more than $26 billion in 2019–20 for the next 4 years for its 7.54 million residents; a record high.12,13 Of this funding, $13 billion has been allocated to: recruitment; responding to the health system challenges; delivering patient value; redeveloping health infrastructure; and enhancing effectiveness and efficiency of care. To deliver these priorities, health system transformation must occur to ensure the optimization of service levels in hospitals, ambulance and emergency health services towards enhanced patient care outcomes, experience and system sustainability.14,15
In the context of system-wide transformation, multiple changes are required at all levels within the healthcare system along with the associated management of this collective of change; change management. Change management describes
the process of continually renewing an organization’s direction, structure, and capabilities to serve the ever-changing needs of external and internal customers.16
A recent review into a health system transformation through capital works; the commissioning of the South East Regional Hospital in NSW, highlighted suboptimal change management during the transition to a new facility.17 The review acknowledged several cultural and governance problems that existed prior to moving to the new facility, but also a number of other factors including poor planning, poor stakeholder engagement and communication and inadequate resourcing that hindered the process of managing the change required through this transformation.17 The review was particularly critical of the leadership of both hospital and state infrastructure in managing this change. These findings reflect international evidence of the limitations in the management of healthcare change, with healthcare leader’s and employee’s capacity and capability in managing change identified as a key challenge.3,18 Despite recognition of inadequacies in the current health system attempts to manage change, there remains limited understanding of the specific change management methodologies that are being implemented by healthcare employees and leaders, as well as the perceived value and limitations of methods currently being used. This knowledge is critical to inform health systems how they might improve how change is led and managed.
The present study aimed to explore leaders’ and employee’s experiences of the management of change in the NSW health system, the change management (CM) methods they have experienced (implemented or involved with), the perceived value and limitations of the change management methods they have experienced, and their perspectives regarding the sufficiency of support for the management of change in the NSW health system.
Methods
Design
A qualitative exploratory design was employed using semi-structured interviews.19 The Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines were used in reporting this study.20 Semi-structured interviews were selected as a flexible and suitable method to enable in-depth data collection with the flexibility to pursue interesting lines of enquiry related to the change management processes and techniques used and experienced by each participant.
Ethics Approval
Ethics approval for this research project was obtained from the University of New South Wales Human Research Ethics Committee (HC190534), and the Northern Sydney Local Health District Human Research Ethics Committee (2019/ETH13325), with local governance approvals from Northern Sydney Local Health District (LHD) and Western NSW LHD. All participants were informed about the purpose of this study, and that this study complied with the Declaration of Helsinki. Informed consent included consent to quote the transcripts in the manuscript.
Setting
The sample was drawn from five LHDs across metropolitan, regional and rural locations in the state of NSW, in addition to five government health agencies with responsibilities for supporting change projects and their leadership. This research was conducted in collaboration with participating LHD and health agencies with these partners involved in all stages of the research.
Sampling
A purposive sample of participants who had exposure to the management of change in NSW Health were invited to take part to capture experiences from different geographic locations, facility types, levels within each service and types of change experienced. We sought to gather perspectives from rural, regional and metropolitan locations, across services that address a range of healthcare conditions. We also sought to gather insights from those involved in very large-scale change projects such as new hospital developments down to local level change experiences. Eligible participants had to have worked in one of the 10 participating organizations for at least 12 months prior to enrolment. Participants were recruited via the social media platforms of Twitter, Facebook and LinkedIn, email to staff members identified in relevant roles through our study partners at each site and using a snowballing technique. Considering the diversity of change experiences across various locations and services that potential participants could be involved in, we did not seek to achieve data saturation but, rather to gather sufficient diversity of experience to address the research aim of capturing experiences in the NSW health system.21 However, the number of interviews conducted was within the accepted range of what the literature considers adequate for theoretical saturation.22–24
Procedure
The interviews, lasting 30–35 minutes, were conducted either face to face, via telephone or online and audio recorded. An interview schedule was developed to explore the research aims. Initially, participants were asked to introduce themselves and their role in the organization. This was followed by a series of open-ended questions exploring the areas of: 1) current context of change and nature of the changes they have experienced; 2) change management methods experienced, including their perceived value and limitations; and 3) need for support in the management of change specifically for health and the NSW health context. The schedule was reviewed after a pilot interview and refined in terms of question ordering. Audio recordings were transcribed verbatim. Interviews were conducted iteratively alongside the analysis to address the research aims.25,26
Data Analysis
Thematic analysis was undertaken to identify, analyse and report patterns in the qualitative data.27 An inductive approach was used to identify themes as they emerged from the data.28 Two researchers from management and psychology backgrounds read the transcripts independently and, after familiarizing themselves with the breadth and content of the data, undertook focused line-by-line analysis. Preliminary themes were generated from the initial coding and discussed with a third researcher who independently analysed a sub-set of the interview data to form an initial group of categories. The categories were then labelled with reference to the raw data and refined over the course of the analysis. Two further researchers independently reviewed the transcripts as part of a team-based approach to enhance the reliability or the analytic process.29 Any discrepancies were resolved through discussion between team members.30
Results
All 16 participants were healthcare leaders; 8 were from the LHDs and 8 were from the health agencies. Participants included front-line healthcare staff involved in change projects, middle and senior management of health services, management of hospital redevelopment projects, change project leads to senior executive of health agencies and LHDs. The change experiences participants described occurred in the past 12 months and were predominantly resulting from priorities set by health system administration agencies or senior executives of their organization. Projects included hospital redevelopment, clinical redesign, digital health services, and projects resulting from participating in a current strategic initiative of value-based health care (VBHC), which aims to deliver care that improves health outcomes that matter to patients, experiences of receiving care, experiences of providing care and effectiveness and efficiency of care.31
Four themes emerged from participants’ responses that articulate their experiences of managing change including the methods used, change resources, capacity and capability of employees and leaders, and the need for an enabling culture for change. Illustrative quotes representing participants’ voice can be found in Table 1.
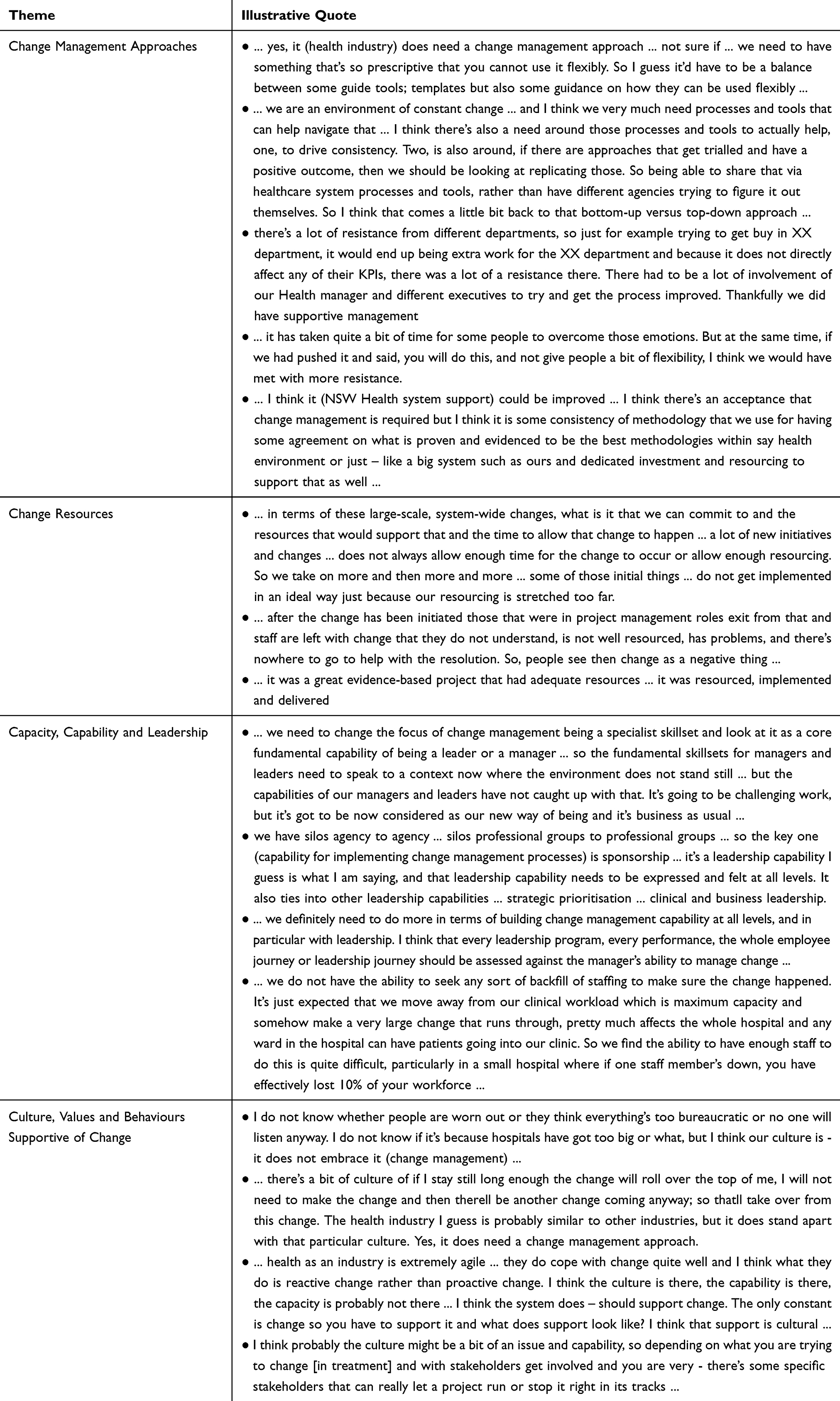 |
Table 1 Themes and Illustrative Quotes That Articulate the Factors Contributing to Successful Change in the Participants’ Experience |
Change Management Methods
Participants’ responses indicated limited use of formal methodologies in managing change, with seven participants discussing one of the more formal methodologies. Of these seven participants, five discussed the use of PROSCI, three discussed the use of Accelerated Implementation Methodology (AIM), three discussed the use of the NSW Health Infrastructure’s 4-Step Change Management Process and one cited the use of Kotter. It was not clear from participants whether these methods were applied across the full lifecycle of a change process; from initiation, implementation, evaluation and to ensuring sustainability. Participants based in more senior leadership roles or within agencies expressed greater awareness of formal change management methodologies. As such, the execution of these methodologies at the clinical front line was often discussed at a high level.
Most participants reported the belief that more consistency in the use of change management methodology when managing change would enhance the execution of the change projects with which they have been involved. Yet few reported in their experiences of successfully implementing these methodologies. More often, participants gave examples of instances in which aspects of particular change techniques were contextualised and applied locally; they reflected on the challenge of sharing knowledge generated through this bottom-up approach. Whilst no single method was identified as the preferred method for managing change irrespective of the type or scale of change, a single set of principles that can be used flexibly for managing change for use across NSW Health, accompanied by guidance templates and tools, was identified by some participants as helpful for healthcare employees and leaders to manage change. One participant proposed that bottom-up approaches in which successful change management approaches were replicated across the system would be valuable. The issue of change resistance was often raised in the context of discussing change management methods. Change resistance was commonly discussed, with participants highlighting the critical importance of ensuring alignment of change to current departmental goals and of management flexibility and buy-in; fundamental aspects identified in change management methodologies. When change resistance was perceived to be a challenge, it was often linked by participants with change fatigue.
Change Resources
Resource availability, in terms of human capital, time allocated to change work and financial assets for change, was discussed by participants as indicative of the level of commitment in the health system. A lack of resources to support the management of change throughout a project lifecycle was consistently mentioned. There was a disconnect between the desire for change to be worked through a managed process and the lack of dedicated investment of resources for change, which was largely felt by those at the clinical front-line. Clinicians in particular identified a need for adequate resources, particularly the funding of change activities and human capital for change in addition to business as usual, to be offered throughout the change life cycle to ensure success. When resources were scarce, participants perceived this to impede successful change and the realization of gains as a result of premature withdrawal or reduction of resources. On the ground, the reality was often that change managers and support staff were withdrawn towards the close of the main implementation stage leading to challenges in sustaining both success and momentum. Where adequate resources were available through the project lifecycle, participants highlighted examples of successful change projects with which they had been involved.
Capacity, Capability and Leadership
Extending from the need for human capital for change, participants discussed workforce issues impacting the collective knowledge, skills, behaviors and ability for managing change in the healthcare system. At every level, participants identified a lack of employee and leader capacity and capability in managing change as a central challenge. Leadership, engagement and sponsorship were often discussed as an important driver for change success. These comments were often made as high-level statements about the need for change management as a major leadership competency and to be embedded in training. Few concrete examples of inadequate leadership capability for change were presented. Examples were primarily presented of employee’s lack of capacity to make change happen and sustain this. Change work was often appended to existing workloads with no dedicated time or training to enable it to be effective or prioritised. Clinician participants also identified that a lack of commitment to change may be driven by individual concerns about their own capabilities, indicating change readiness was lacking at an individual level throughout the system. Those in leadership roles identified difficulties in motivating employees to change, communicating the need for change effectively and sustaining any improvements achieved over time. Frontline healthcare staff were described as lacking awareness of the need for change and of the progress of projects with which they are involved. A perceived need for more effective communication and engagement with the clinical and non-clinical workforce was apparent.
Enabling Culture for Change
Participants described the health system as a complex adaptive system that has the potential to be an agile context for change. Participants at all levels identified the capacity of the health system to respond to change reactively rather than proactively as a key feature of the current management of change; the need for change is brought on by a focusing event and change management then occurs. In this reactive model, the management of change is a necessary and procedural activity. The participants highlighting an enabling culture as the critical ingredient to enhance employee’s desire to stimulate, lead and embrace change proactively. Diverse responses in relation to culture highlighted the variation between different stakeholders and organizations in the health system. Several participants perceived there to be an absence of an enabling culture across their health system, which was identified as a key barrier to bringing about change. Cultural artefacts identified by these participants included perceptions of bureaucracy, competing priorities and employee change fatigue that led to employees feeling unable to embrace or engage with change. Others – often within healthcare agencies – reported that the culture to enable and support change was present in the health system, but that capacity was a key challenge. Across the sample, it was apparent that the growth of capability and capacity amongst all healthcare employees, from the frontline to senior executive, was considered valuable to create the supportive environment required as a foundation to enable change.
Discussion
Through the qualitative exploration of healthcare employees’ and leaders’ experiences with change, we sought to understand the conditions that support effective change in healthcare and methods currently being used to manage change. Four distinct themes emerged from participants’ responses that articulate the factors contributing to successful change in their experience: 1) change management methods, 2) change resources, 3) capacity, capability and leadership engagement and sponsorship for managing change, and 4) an enabling culture that supports change at all levels of the public health system. It is perceived that there is no preference for a specific CM approach but that an evidence-based approach which enables flexibility and is supported by health system-wide guidance and resources for employees is needed. Whilst the approaches utilized may meet these requirements, it was evident that the use of either a structured approach or a specific CM method had not been adopted across the system.32–34 The capacity, culture and capability within the system came through most strongly as needed to proactively drive change and see changes through to be sustained.
Healthcare is a complex adaptive system; with multiple dynamic interacting variables that, as systems evolve, introduce further complexity.35,36 Change management methods and their application must therefore also be adaptive and flexible to enable adoption in health systems.36 Whilst many participants commented on the need for additional resource for change, for any methods to be effectively employed, culture, capacity and capability for change must be addressed to gain the most value from change processes within the context of a finite budget for change in health systems. These cognitive and affective prerequisites of change readiness are recognized as essential across industries but appeared to be lacking in many of the change experiences described in the present study.37 Before considering and adopting an approach, there must already be a positive culture for change within the health system, and individuals who are equipped with the skills and knowledge required to lead and navigate change efforts.
Implications
Participants’ responses indicate that a culture for change is determined by the capacity, capability and leadership for change, coupled with the resource availability for change to be successful. Cultural change is a long process and intervention must be multi-level. Culture can be influenced by the political environment with shifting priorities and by financial pressure and stress on resources.38,39 To create a culture that enables change within such an environment, system or macro-level leaders (eg governance agencies or peak-bodies) and/or health organization’s Boards and the Executives must be committed to and initiate the change in order for it to be successful.40 According to participants, commitment is demonstrated through their change leadership capability, giving resources to change managers to lead effectively and giving permission and endorsement (eg in the form of time in addition to other responsibilities) for staff to engage in the change management activities, and this is reinforced in the literature.37,40 At the meso-level, middle-managers should initiate and execute changes endorsed and resourced by the macro-level.41 Finally, at the micro-level, healthcare staff must be empowered to make change locally and be provided with the resources required to do so.40,41 It is critical to identify the required resource for change at all levels early in the proposal, which may be informed in part by active learning systems that promote knowledge exchange across and beyond the health system.42,43
It was apparent from the study data that whilst change management methodologies can provide a framework and tools to support the management of change, one size does not fit all; each team and project is different and enabling the change requires flexible, adaptable approaches. An important question for healthcare leaders to ask is “are we change ready?”37,44,45 Leaders may consider a multitude of factors in determining readiness: Is there evidence of collective change readiness? Do we have sufficient resources to manage change? How can the organizational executive support change and create an enabling culture? There are examples in the literature on what constitutes organizational readiness for change that align with these findings.46 Weiner (2009) considers stakeholders’ willingness and confidence in the ability to execute change as determinants for change readiness. The findings of this study provide a greater context for change commitment and efficacy from which healthcare leaders may consider readiness for managing change and how they may invest resource optimally to set them up for success.
Limitations and Future Directions
The study findings must be considered in the context of the research limitations. As a multi-site, single state and country project with 16 participants, the generalizability of evidence beyond the NSW and Australian health system cannot be determined. Whilst there were a small number of included participants, there was a wide array of positions interviewed spanning the NSW health system, with significant breadth and depth of interview data. However, this study presents an unbiased, in depth and rigorous approach, which adds to the limited evidence of effective change leadership and management in health care. The qualitative evidence generated indicates that the exploration of causal relationships between leadership, capacity and capability, and culture for change with a study design that supports this may be of value. The current design enabled the generation of evidence of beliefs regarding the factors that may contribute to effective change that may be tested in follow-up work.
Conclusion
This study reports experiences and perceptions of managing health systems change in an Australian context, highlighting that health systems change is often complex, with multiple dynamic interacting components and stakeholder interests for leaders and managers to navigate. Developing and sustaining an enabling culture to support change underpinned by capability and capacity to bring about change across the health system workforce is critical.
Data Sharing Statement
Access to the research data from this project may be discussed with the lead author and is subject to appropriate ethical approvals.
Ethical Approval and Consent
The study received ethics approval from the Health Research Ethics Committee at the University of New South Wales and the Human Research Ethics Committee at the Northern Sydney Local Health District.
Written consent was obtained from each participant to participate in this study along with the use of their individual de-identified details in this manuscript.
Acknowledgments
We wish to thank our partners of NSW Health who contributed to the shaping of this research paper. Their dedication in gaining insight into how change is implemented and managed at NSW Health for better patient value and staff experience.
- Adrienne Stern and Harry Illingworth of Hornsby Ku-ring-gai Health Service
- Ian Richards of NSW Clinical Excellence Commission
- Lea Kirkwood and Tricia Cummins of NSW Agency for Clinical Innovation
The research team appreciate the NSW Health staff and partners who contributed their time and advice in the development and conduct of this project. Particularly, their time during the global CoVID-19 pandemic.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Dieleman JL, Squires E, Bui AL, et al. Factors associated with increases in US health care spending, 1996–2013. JAMA. 2017;318(17):1668–1678. doi:10.1001/jama.2017.15927
2. World Health Organisation. Health financing for universal coverage; 2020. Available from: https://www.who.int/health_financing/topics/efficiency/system-inefficiencies/en/.
3. Rothwell WJ, Stavros JM, Sullivan RL. Practicing Organization Development: Leading Transformation and Change. John Wiley & Sons; 2015.
4. Austin J, Bentkover J, Chait L. Leading Strategic Change in an Era of Healthcare Transformation. Springer; 2016.
5. Anderson LA, Anderson D. The Change Leader’s Roadmap: How to Navigate Your Organization’s Transformation. John Wiley & Sons; 2010.
6. Anderson D, Anderson LA. Beyond Change Management: How to Achieve Breakthrough Results Through Conscious Change Leadership. John Wiley & Sons; 2010.
7. Kotter JP, Cohen DS. The Heart of Change: Real-Life Stories of How People Change Their Organizations. Harvard Business Press; 2012.
8. Kotter JP, Schlesinger LA. Choosing Strategies for Change. Harvard Business Review; 1979.
9. Creasey T, Taylor T. even greatest contributors to change management success. People Strategy. 2014;37(1):12.
10. Willis CD, Saul J, Bevan H, et al. Sustaining organizational culture change in health systems. J Health Organ Manag. 2016;30(1):2–30. doi:10.1108/JHOM-07-2014-0117
11. Willis E, Reynolds L, Keleher H. Understanding the Australian Health Care System. Elsevier Health Sciences; 2016.
12. New South Wales Ministry of Health. More than $25 billion for total health budget; 2018. Available from: https://www.health.nsw.gov.au/news/Pages/20180619_00.aspx.
13. New South Wales Ministry of Health. Record $10.1 billion health infrastructure spend; 2019. Available from: https://www.health.nsw.gov.au/news/Pages/20190619_00.aspx.
14. New South Wales Government Treasury. The NSW Budget 2019–2020 – my Budget; 2020. Available from: https://www.budget.nsw.gov.au/my-budget.
15. New South Wales Government Treasury. Budget Statement 2019–2020; 2020.
16. By RT. Organisational change management: a critical review. J Change Manag. 2005;5(4):369–380. doi:10.1080/14697010500359250
17. Reid M, Nowitzke A. Review of South East Regional Hospital. NSW Health. 2017.
18. Waring J, Bishop S, Clarke J, et al. Healthcare leadership with political astuteness (HeLPA): a qualitative study of how service leaders understand and mediate the informal ‘power and politics’ of major health system change. BMC Health Serv Res. 2018;18(1):918. doi:10.1186/s12913-018-3728-z
19. Kallio H, Pietilä AM, Johnson M, Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi‐structured interview guide. J Adv Nurs. 2016;72(12):2954–2965. doi:10.1111/jan.13031
20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
21. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2019:1–16. doi:10.1080/2159676X.2019.1704846
22. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
23. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
24. Mason M, editor. Sample Size and Saturation in PhD Studies Using Qualitative Interviews. Forum qualitative Sozialforschung/Forum: qualitative social research; 2010.
25. Bowen GA. Naturalistic inquiry and the saturation concept: a research note. Qual Res. 2008;8(1):137–152. doi:10.1177/1468794107085301
26. Morse JM, Field P-A. Qualitative Research Methods for Health Professionals. Thousand Oaks, CA: SAGE publications; 1995.
27. Braun V, Clarke V, Hayfield N, Terry G. Thematic analysis. In: Handbook of Research Methods in Health Social Sciences; Springer Singapore. 2018:1–18.
28. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
29. Boyatzis RE. Transforming Qualitative Information: Thematic Analysis and Code Development. Sage; 1998.
30. Burla L, Knierim B, Barth J, Liewald K, Duetz M, Abel T. From text to codings: intercoder reliability assessment in qualitative content analysis. Nurs Res. 2008;57(2):113–117. doi:10.1097/01.NNR.0000313482.33917.7d
31. Koff E, Lyons N. Implementing value-based health care at scale: the NSW experience. Med J Aust. 2020;212(3):104–6. e1. doi:10.5694/mja2.50470
32. Jones-Schenk J, Bleich MR, Jones-Schenk J. 70% failure rate: an imperative for better change management. J Contin Educ Nurs. 2019;50(4):148–149. doi:10.3928/00220124-20190319-03
33. Wong Q, Lacombe M, Keller R, Joyce T, O’Malley K. Leading change with ADKAR. Nurs Manage. 2019;50(4):28–35. doi:10.1097/01.NUMA.0000554341.70508.75
34. Tang KN. Change management. In: Leadership and Change Management. Springer; 2019:47–55.
35. Braithwaite J, Wears RL, Hollnagel E. Resilient health care: turning patient safety on its head. Int J Qual Health Care. 2015;27(5):418–420. doi:10.1093/intqhc/mzv063
36. Braithwaite J, Churruca K, Ellis LA, et al. Institutional editor: Australian Institute of Health Innovation. Complexity science in healthcare. In: Aspirations, Approaches, Applications and Accomplishments a White Paper. Sydney, Aust: Australian Institute of Health Innovation, Macquarie University; 2017.
37. Rafferty AE, Jimmieson NL, Armenakis AA. Change readiness: a multilevel review. J Manag. 2013;39(1):110–135.
38. Kuipers BS, Higgs M, Kickert W, Tummers L, Grandia J, Van der Voet J. The management of change in public organizations: a literature review. Public Adm. 2014;92(1):1–20. doi:10.1111/padm.12040
39. Schultz T, Shoobridge J, Harvey G, Carter L, Kitson A. Building capacity for change: evaluation of an organisation-wide leadership development program. Aust Health Rev. 2019;43(3):335–344. doi:10.1071/AH17158
40. Higgs M, Rowland D. Building change leadership capability: the quest for change competence’. J Change Manag. 2000;1(2):116–130. doi:10.1080/714042459
41. Heyden ML, Fourné SP, Koene BA, Werkman R, Ansari S. Rethinking ‘top-down’ and ‘bottom-up’ roles of top and middle managers in organizational change: implications for employee support. J Manag Stud. 2017;54(7):961–985. doi:10.1111/joms.12258
42. Kislov R, Wilson PM, Knowles S, Boaden R. Learning from the emergence of NIHR Collaborations for Leadership in Applied Health Research and Care (CLAHRCs): a systematic review of evaluations. Implement Sci. 2018;13(1):111.
43. Heskestad RN, Aase K, Storm M. Inter-organisational learning among health care professionals: a learning arena to address transitional care of the elderly. Int J Integr Care. 2016;16(6).
44. Armenakis AA, Harris SG, Mossholder KW. Creating readiness for organizational change. Hum Relations. 1993;46(6):681–703. doi:10.1177/001872679304600601
45. Rafferty AE, Minbashian A. Cognitive beliefs and positive emotions about change: relationships with employee change readiness and change-supportive behaviors. Hum Relations. 2019;72(10):1623–1650. doi:10.1177/0018726718809154
46. Weiner BJ. A theory of organizational readiness for change. Per NIlson. In: Handbook on Implementation Science. Edward Elgar Publishing; 2020.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.