")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 7
Managing cardiovascular disease risk in patients treated with antipsychotics: a multidisciplinary approach
Authors Shulman M, Miller A, Misher J, Tentler A
Received 17 May 2014
Accepted for publication 8 July 2014
Published 31 October 2014 Volume 2014:7 Pages 489—501
DOI https://doi.org/10.2147/JMDH.S49817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Matisyahu Shulman,1 Avraham Miller,2 Jason Misher,3 Aleksey Tentler4
1Department of Psychiatry, Zucker Hillside Hospital, Glen Oaks, NY, USA; 2The Ruth and Bruce Rappaport Faculty of Medicine, The Technion Israel Institute of Technology, Haifa, Israel; 3Department of Medicine, Hofstra North Shore-LIJ School of Medicine, Hempstead, NY, USA; 4Department of Internal Medicine, Rutgers New Jersey Medical School, Rutgers, The State University of New Jersey, Newark, NJ, USA
Background: The use of antipsychotic medication in the United States and throughout the world has greatly increased over the last fifteen years. These drugs have significant side effect burdens, many of them relating to cardiovascular health.
Objective: To review the available evidence on the major cardiovascular issues that arise in patients taking antipsychotic medication.
Method: A PubMed literature review was performed to identify recent meta-analyses, review articles, and large studies. Further articles were identified through cited papers and based on expert consultation when necessary.
Results: Clinical guidance on the following adverse effects and antipsychotics was reviewed: electrocardiogram (ECG) changes, (specifically, prolonged QT and risk of torsades de pointes), weight gain, dyslipidemia, metabolic syndrome, and myocarditis. Specific attention was paid to monitoring guidelines and treatment options in the event of adverse events, including dose change, medication switch, or adjuvant therapy.
Keywords: schizophrenia, prolonged QT, increased mortality, weight gain, myocarditis
Introduction
The use of antipsychotic medication in the United States and throughout the world has greatly increased over the last fifteen years. The number of individuals prescribed antipsychotic medication in the United States increased between 1997 and 2007 from 2.2 million to 3.9 million.1 The use of antipsychotics in some pediatric populations has had an even more dramatic increase and atypical antipsychotic use in the pediatric population in the United States increased by 60% from 2002 to 2007.2,3
This increase is partially due to the introduction of second-generation antipsychotic medications that are more appealing to physicians and consumers due to decreased extra pyramidal effects. Traditionally used only for severe mental illness, the second-generation antipsychotics are now routinely prescribed as adjuvant treatment of mood disorders. These drugs are not without significant side effect burdens, many of them relating to cardiovascular health.
Individuals with severe mental illness have significantly increased mortality and a resultant shorter life expectancy when compared to healthy controls. A recent review estimated this decrease to be as great as a 10 to 20 year reduction in average lifespan in this population.4 Multiple factors likely contribute to this increase in mortality but cardiac problems have been identified as a major contributor.5 A large study of a Veterans Administration cohort found that the odds ratio for all-cause mortality was nearly double in subjects with atypical antipsychotic use. This study found a significantly increased risk of cerebrovascular events and transient ischemic attacks, as well as an increased risk of coronary artery disease and congestive heart failure, although this increase did not meet significance.6 Increased risk for cardiovascular issues in the mentally ill population is likely due to multiple factors including medication side effects, poor access to medical care, underlying organic comorbidity, and poor compliance with medical care. Additionally, patients with mental illness often have higher incidence of poor cardiovascular risk factors including smoking, sedentary lifestyle, etc.7
The popularity of second-generation antipsychotics and the complex interaction between side effect burden and psychiatric benefit creates a growing need for a multidisciplinary approach to provide optimal outcomes.8,9 Communication between mental health and medical care providers should ideally occur throughout the treatment process. The diagnosis and severity of each patient’s psychiatric symptoms must be weighed against the individual’s medical risk factor profile to determine a rational pharmacotherapeutic approach. This review attempts to summarize the available evidence on clinical issues arising related to the cardiac management of patients taking antipsychotic medications. The cardiovascular negative effects related to antipsychotic drugs reviewed in this article include: sudden death, electrocardiogram (ECG) and corrected QT segment (QTc) changes, metabolic syndrome, diabetes, hyperlipidemia, and myocarditis.
Methods
A PubMed literature review was performed using the following search terms: antipsychotics AND cardiac care, antipsychotics AND orthostatic hypotension, antipsychotics AND prolonged QTC, antipsychotics AND metabolic syndrome, antipsychotics AND sudden death, antipsychotics AND myocarditis. The reviewers focused on recent meta-analyses, review articles, and large studies. Further articles were identified through cited papers and based on expert consultation when necessary.
Results
PubMed literature review and bibliographic search of identified studies yielded 61 relevant articles. Expert consultation provided five additional articles.
QT prolongation and sudden death related to antipsychotic use
ECG changes, specifically prolongation of the QT interval, have been noted as an adverse effect of many medications including antipsychotics. QT prolongation is clinically relevant as it is associated with increased risk for the life-threatening arrhythmia torsades de pointes (polymorphic ventricular tachycardia). Being aware of this possibility and correctly recognizing drug-induced torsades de pointes is vital since treatment with a medication such as amiodarone, (used for a similar-appearing monomorphic ventricular tachycardia and for ventricular fibrillation), may worsen the condition.10
The length of the QT segment on the ECG represents the time it takes for ventricular depolarization and repolarization. Assuming a narrow QRS complex, it is primarily used as an indicator of the time it takes for the ventricles to repolarize. Because the QT segment can vary with heart rate changes the QTc is often used as a more accurate representation of ventricular repolarization. The QTc is roughly measured by dividing the measured QT segment by the square root of the R to R interval.11 Values for QTc ≤0.44 seconds in men and ≤0.46 seconds in women are considered normal.12 As alterations in ventricular repolarization can impact underlying cardiac rhythms, the QTc becomes very clinically relevant in analyzing ECGs.
The mechanism of ventricular depolarization and repolarization is accomplished through various ion channels within the cardiac myocytes. Accordingly, any alterations in relevant electrolyte levels will impact the duration of ventricular depolarization and repolarization. Normally the ventricles are not depolarized until the completion of a full repolarization period. In situations in which ventricular repolarization is prolonged (usually >0.50 seconds)13 a signal of depolarization can reach the ventricles before the ventricle is fully repolarized. These so-called “early afterdepolarizations” can induce torsades de pointes and other fatal cardiac arrhythmias.14
Controversy regarding sudden cardiac death
Historically, there has been some controversy as to the extent that arrhythmias have contributed to sudden cardiac death in patients taking antipsychotic medication. The earliest reports of sudden cardiac death related to antipsychotic use date back to the mid-1960s15 but the cause of these deaths remained unclear.16,17 The connection between antipsychotic medication, arrhythmias, and resultant sudden cardiac death gained greater attention in the late 1990s.18,19
Antipsychotic agents were shown to block repolarizing potassium currents in vitro20 and to prolong the QT interval.21 Prolonged QTc was assumed to be a risk factor for sudden cardiac death from unstable ventricular tachyarrhythmias precipitated by torsades de pointes.14 In 2009 Ray et al published findings of a study investigating increased risk of sudden cardiac death as an adverse effect of atypical antipsychotic medications.22 Using a Medicaid database to retrospectively calculate the incidence of sudden cardiac death among users of typical and atypical agents they found that both antipsychotic classes were associated with an approximate doubling of the risk of sudden cardiac death relative to non-users. This risk was dose-dependent in both medication classes and was assumed to be due to drug-induced arrhythmias.
These findings were disputed by the American Psychiatric Association (APA) Council on Research who argued that the use of death certificates in the study may have led to an overestimation of the incidence of sudden cardiac death due to drug-induced arrhythmias and an underestimation of other cardiovascular morbidity in users of antipsychotic drugs.23 This argument was strengthened by a review of the root causes of 100 consecutive cases of sudden death in a cohort of psychiatric subjects. This review found that about half of the cases of sudden unexpected death were likely due to acute coronary syndrome, upper airway obstruction, pulmonary emboli, or thrombotic strokes. The remainder of the cases were found to have high incidence of cardiovascular risk factors, and it was argued that these deaths did not necessarily result from direct arrhythmogenic effects of medications.24
Clinical approach to QT changes
Regardless of the exact extent to which sudden cardiac death results from drug-induced arrhythmia, the connection between QT prolongation and sudden cardiac death has been confirmed in a meta-analysis of 23 observational studies showing a dose-related effect of antipsychotic drugs on QT interval and subsequent mortality. Drug-induced prolongation of the QT interval by 50 milliseconds was shown to correlate with an increase of all-cause mortality by 20%, cardiovascular mortality by 29%, and sudden cardiovascular mortality by 29%.25 A recent observational study of subjects without concomitant risk factors also found a dose-dependent relationship between QT prolongation and antipsychotic use.26
Because of the increased risk of death associated with QT prolongation the APA practice guidelines suggest that an absolute QTc interval of >500 milliseconds or an increase of 60 milliseconds from baseline requires either a decrease in dosage or discontinuation of antipsychotic medication.23 Patients with agitation or psychosis in this situation should be treated with benzodiazepines, mood stabilizers, or electroconvulsive therapy (ECT) as alternatives to antipsychotic medications.
Risk factors
Recognizing patients at risk for arrhythmia is an important part of clinical decision making. A list of risk factors for QTc prolongation is provided in Table 1. A large case-control study found that drug-induced prolonged QTc was associated with hypokalemia, hepatitis C virus, HIV infection, and T-wave abnormalities.27 The study authors noted that 85% of patients with drug-induced prolonged QTc had two or more of the above risk factors. Surprisingly, no association was found between drug-induced QTc prolongation and presence of cardiovascular risk factors or coronary artery disease. Other risk factors for prolonged QT include female sex,28 age,29 agitation,31 and use of multiple QT prolonging medications.32
 | Table 1 Risk factors for prolonged QTc |
Age was also noted to be a factor in a meta-analysis of two large studies (n=56,000) that noted QTc increases with age in healthy individuals independent of medications.29 It should also be noted that, in the pediatric population, a recent nested case-control trial did not find an association with antipsychotic drug use and prolonged QTc.30
Agitation leading to hospitalization has also been argued to be a risk factor for prolonged QT as a recent study observed that about 25% of patients admitted to the psychiatric hospital were found to have abnormal or borderline QT as compared to about 9% at discharge.31
Routine ECG monitoring
Despite the risk of QT prolongation, the APA practice guidelines do not suggest routine monitoring of healthy individuals before starting most antipsychotic medication.33 The guidelines suggest ECG monitoring for patients with cardiac risk factors starting high risk medications (eg, ziprasidone), for patients with signs of arrhythmia (syncope), for patients on a second agent causing prolonged QTc, and for all patients starting the first-generation antipsychotic pimozide.23 The National Institute for Health and Care Excellence (NICE) clinical guidelines additionally suggest routine testing in all patients admitted to an inpatient unit along with those at increased risk.34
Specific agents
Antipsychotic medications have been found to increase QTc as a class but variance does exist between medications. Initially, several first-generation antipsychotics were noted to have the largest effect on QTc, among them sertindole, thioridazine, and droperidol. Consequently, the use of these agents significantly decreased and thioridazine was withdrawn from the market by its producer in 2005 due to torsadogenic concerns. It is no longer available worldwide and its withdrawal likely led to a significant increase in hospitalizations in some countries highlighting the need for risk-benefit analysis and interdisciplinary discussion when considering medication withdrawals.35
Of the second-generation antipsychotics available in the United States, ziprasidone and iloperidone have been noted to have the greatest effect on QTc. Others agents available elsewhere such as amisulpride and sertindole have also been implicated to an even greater degree.36
Of note, ziprasidone was not found to cause increased mortality in comparison to olanzapine in a large open label study of more than 18,000 patients. The study authors note that the study was not sufficiently powered to identify increased risk of torsades or sudden cardiac death.37
Consideration of QTc effects are also important in the context of the common off-label use of haloperidol via intravenous infusion for agitation or delirium in the hospital setting. Although haloperidol, a commonly used first-generation antipsychotic, has been found to have only mild effects on QTc when given in the intramuscular (IM) or oral form, the US Food and Drug Administration (FDA) has issued a warning regarding its administration intravenously or at high doses due to numerous case reports of torsades and death associated with intravenous haloperidol.38 The FDA suggests ECG monitoring in any case intravenous administration is used. The guidelines also advise “caution” in cases of electrolyte imbalances, particularly hypokalemia or hypomagnesemia. The same would apply in patients with underlying cardiac abnormalities, hypothyroidism, or familial long QT syndrome, and in those who are taking other drugs known to prolong the QT interval. Further studies have confirmed a statistically significant increased risk of prolonged QTc with the use of intravenous haloperidol when compared to commonly used second-generation antipsychotics. Despite this warning, observational studies have shown that patients given haloperidol often have modifiable risk factors for arrhythmia and it appears that further education and implementation strategies are needed in this area.39
In situations when an antipsychotic with minimal torsadogenic risk is required several options exist. One meta-analysis of seven commonly used antipsychotic agents found that aripiprazole caused a mean decrease of QTc.40 It should be noted that FDA monitoring of adverse events did find an increased signal for torsades de pointes in aripiprazole versus other medications not known to affect QTc.41
Although introduced only recently and having limited direct comparison data, lurasidone has also been noted to have minimal effect on QTc in clinical trials.42 A more recent Bayesian meta-analysis of 15 commonly used antipsychotic agents found that the QTc interval was not significantly affected by either aripiprazole or lurasidone.36
The recommendations for ECG and electrolyte monitoring of patients on antipsychotic drugs (based on the APA and NICE guidelines) are summarized in Table 2.
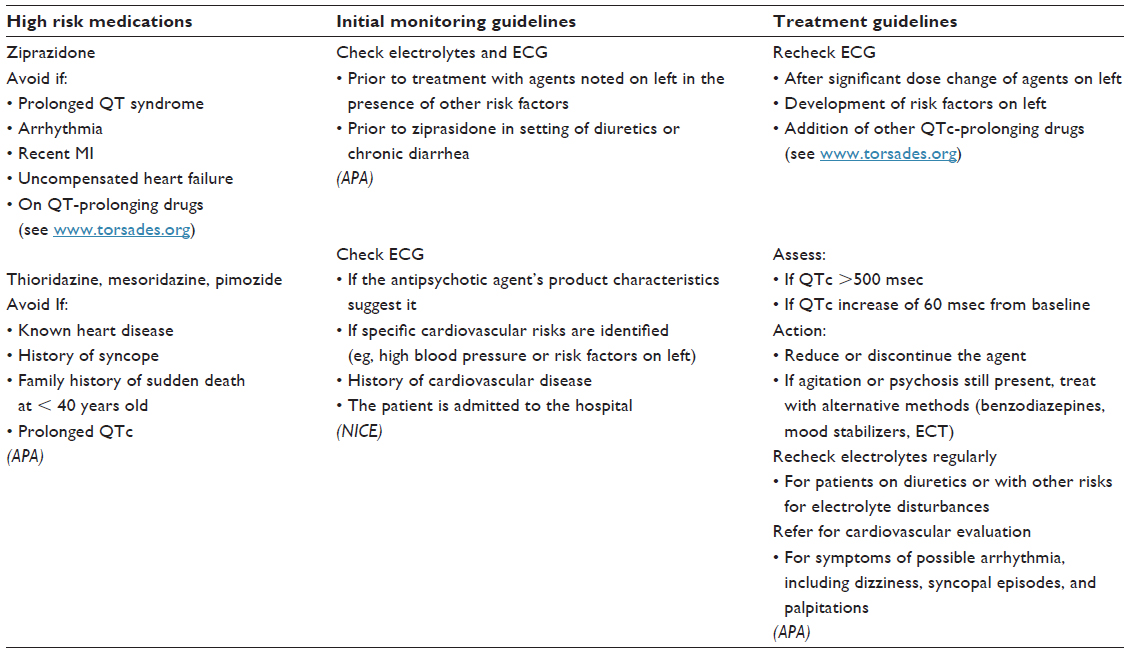 | Table 2 Summary of clinical guidelines for antipsychotic medications and ECG changes |
Metabolic syndrome and long-term risk factors
Weight gain and metabolic abnormalities were noted as an adverse outcome to the original antipsychotic chlorpromazine soon after its introduction. Most other typical antipsychotics did not show significant side effects in this area. With the advent of clozapine in the 1970s and risperidone in the 1980s, this issue became a more common problem as the newer agents were observed to cause significant changes in patients’ weight and metabolic profiles.43
Some evidence exists that patients with schizophrenia may develop weight gain, obesity, and metabolic syndrome independent of antipsychotic drug use, although this was noted to have a prevalence of only about 10% of all early episode and untreated patients.44 In the chronic schizophrenia population the percentage is much higher. A meta-analysis found the overall prevalence of metabolic syndrome in chronic schizophrenia patients to be approximately 32%.44 Cross-sectional studies in several countries have found the prevalence of metabolic syndrome in patients taking antipsychotic medication to be as high as 45%–50% with a correspondingly high risk for coronary artery disease in this group.45,46
In approaching the issues of antipsychotic induced metabolic syndrome, diabetes, and dyslipidemia several approaches have been developed, and clinicians would again be best served using a collaborative approach. Once a patient has developed metabolic abnormalities or a syndrome due to antipsychotic drug use, several options have been explored. These include switching to another agent, decreasing the dose of the offending agent, lifestyle interventions, or further pharmacotherapy to treat the issue. Each intervention has limitations and available evidence on an optimal approach is still inconclusive. A proposed treatment algorithm for dealing with antipsychotic induced weight gain and metabolic syndrome is provided in Figure 1.
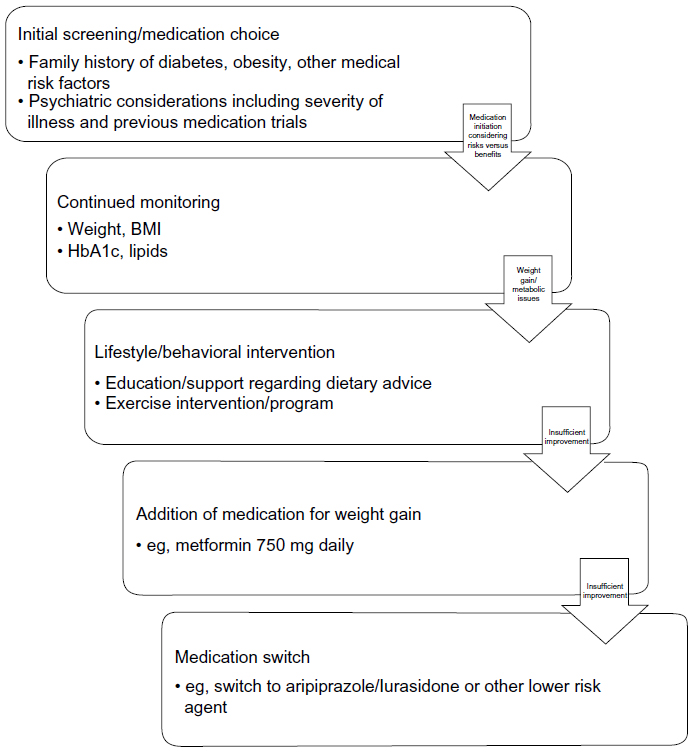 | Figure 1 Metabolic and weight gain treatment and monitoring algorithm. |
Monitoring
Regular monitoring for metabolic issues in at-risk individuals is an important first step in determining a treatment plan. The risk factors include: personal and family history of obesity, diabetes, dyslipidemia, hypertension, or cardiovascular disease. The consensus guidelines for monitoring of patients starting antipsychotic medication are to measure the baseline weight and height (so that body mass index can be calculated), waist circumference (at the level of the umbilicus), blood pressure, fasting plasma glucose, and fasting lipid profile.47
Continued monitoring includes weight checks every few weeks, as well as checking the fasting glucose, lipids, and blood pressure after 12 weeks of treatment. The fasting glucose can then be checked yearly, and fasting lipids every 5 years. Patients should also be screened for personal or family history of diabetes, at baseline and yearly.47 Unfortunately, clinicians have been found to have poor adherence to these guidelines.48–51 Clearly, there is a need for programs to help educate providers and to facilitate monitoring of these cardiac risk factors.
Initial drug choice
Choosing an initial agent with a more favorable profile has been argued by some as the best approach in preventing the development of weight gain and metabolic syndrome. Identifying patients who are at risk for metabolic syndrome or who would likely be at highest risk from a medical standpoint may be helpful in this regard as other considerations such as price or comorbid conditions may take precedence in some cases. Recent work has been undertaken to identify genetic polymorphisms most at risk for metabolic side effects, although this technology is still in the experimental stages.52
Many factors should be considered when choosing an antipsychotic agent including history of drug trials, efficacy, tolerability, and cost. The second-generation antipsychotics associated with low risk are more expensive than older higher-risk agents, although the decreased risk of metabolic side effects might mitigate some or all of these costs. A cost analysis based on the results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) trial found that the use of ziprasidone versus olanzapine would save about US $500,000 per 100,000 Medicaid patients in direct medical costs relating to metabolic issues.53 It should be noted that the study did not consider other costs related to poorer psychiatric outcome with ziprazidone due to higher discontinuation rate and lower efficacy as compared with olanzapine.
Another important consideration is tolerability and effectiveness for psychiatric symptoms. Although clozapine and olanzapine have been implicated as the worst offenders in regards to metabolic side effects, it may be necessary to use these agents due to their favorable profiles in treating psychosis. Olanzapine was shown to have statistically significant longer duration of use until discontinuation in the CATIE trial,54 while clozapine has been shown to be an effective treatment for subjects in whom other antipsychotics are not effective.55
Hierarchy of medications
In determining a rank order for medications with regards to metabolic and weight changes only limited evidence exists of head to head comparison trials for most medications. The CATIE trial did provide convincing evidence that olanzapine caused greater change in weight and metabolic parameters. This was a large blinded randomized controlled trial of multiple antipsychotic agents and found that olanzapine caused significantly greater weight gain than risperidone, quetiapine, and perphenazine. The same trial found ziprasidone to be weight neutral.54 A meta-analysis of comparison trials confirmed that olanzapine and clozapine were the worst offenders with regard to weight gain and metabolic side effects. The same study found that risperidone, quetiapine, aripiprazole, and ziprasidone were not significantly different in the area of weight gain; however, quetiapine caused significantly more increase in cholesterol than risperidone or ziprasidone. It should also be noted that this review found that most first-generation antipsychotics cause some weight gain as well.56 A recent review of aripiprazole trials found that this drug is relatively weight neutral when compared with other second-generation antipsychotics.57
Without evidence from direct head to head trials secondary approaches must be used to determine a hierarchy for propensity to cause weight gain and metabolic issues. It should be noted that even medications that have been determined to be weight neutral may cause weight gain in a subset of patients while causing weight loss in others. The percentage of patients gaining 7% or more of their body weight in a placebo control trial can be compared to determine which agents are most likely to cause weight gain. For example 8% of schizophrenic subjects taking aripiprazole in placebo control trials gained 7% or more of their body weight.58 This number was lower in ziprasidone and lurasidone with only about 4% and 3% of subjects gaining 7% or more of their body weight.59,60 A list of agents with available information on the percentage of patients who gained 7% or greater of their body weight is provided in Tables 3 and 4. The existence of this subset requires providers to be vigilant in the monitoring of patients taking even the “weight neutral” medications. With regards to the number needed to harm in regards to 7% weight gain this number was found to be as high as six for schizophrenic patients taking olanzapine.68
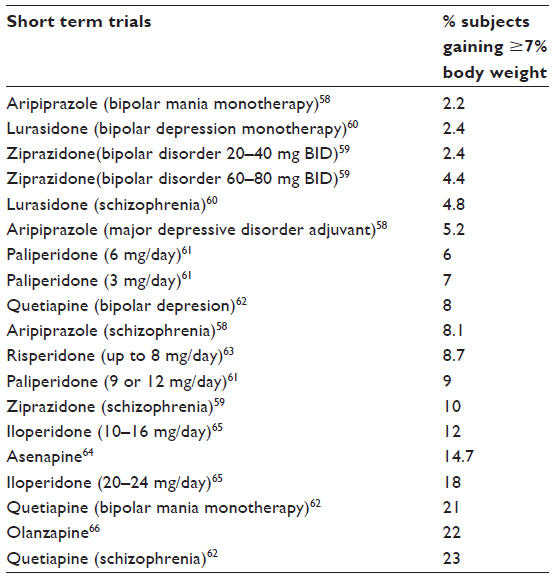 | Table 3 Weight gain by agent |
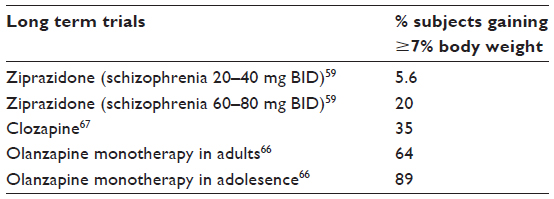 | Table 4 Weight gain by agent |
A recent review article used a more complex approach to indirectly compare agents based on data from multiple trials in which both drugs were compared to a common agent (or placebo). By comparing effect sizes determined in each trial a hierarchy was created for multiple effects including weight gain and metabolic parameters. This trial found that haloperidol, ziprasidone, lurasidone, and aripiprazole cause significantly less weight gain than most other commonly used agents including risperidone, quetiapine, and chlorpromazine. Olanzapine was again confirmed as causing significantly more weight gain than risperidone and quetiapine, but did not differ significantly from chlorpromazine, clozapine, iloperidone, sertindole or zotepine.
Based on the above evidence antipsychotic drugs have generally been stratified into high, intermediate, and low risk profile. A 2011 review concluded that clozapine, olanzapine, and (first-generation agent) chlorpromazine are considered highest risk, quetiapine, risperidone, sertindole, and paliperidone are considered intermediate risk. Lurasidone, ziprasidone, aripiprazole, amisulpride, and most first-generation agents are considered to be low risk or weight neutral.69 Additional meta-analysis of newer agents found that asenapine caused the highest percentage of patients’ significant weight gain followed by iloperidone and paliperidone. Lurasidone was confirmed as having no significant effect on body weight.70
Dose reduction or switch
In the event that a patient does experience antipsychotic-induced weight gain clinicians are faced with several options. As a rule, multiple treatments are available for a particular psychiatric condition, making the possibility of switching to an alternate agent a viable option. For example, if an antipsychotic is being used as an adjuvant treatment for major depression other options such as lithium or levothyroxine augmentation, cognitive behavioral therapy, or electroconvulsive therapy might be considered.
Caution is advised, however, when changing a stable psychiatric regimen in schizophrenic or schizoaffective patients, as a history of good treatment response to a particular agent does not necessarily translate to positive response with other agents. The CATIE trial, for example, found that subjects who switched medications had higher probability of discontinuing the new agent than those whose regimen remained stable.71 The decision to switch agents or to lower the dose of a medication that has caused metabolic side effects should therefore be a collaborative one between the cardiologist or internist involved, the psychiatrist, and, if possible, the patient.
Switching medication to an agent with a more favorable metabolic profile appears to be effective in at least partially reversing weight gains. A recent review on aripiprazole trials found that a switch to aripiprazole was successful in improving weight and metabolic parameters.57 Similarly, a general review article found that most studies showed some benefit with switching from higher-risk agents to those with lower risk.72 In contrast, a recent meta-analysis concluded that a switch strategy to another agent was generally weight-neutral overall and that patients did not lose the weight previously gained.73 This was true even with a switch to aripiprazole, ziprasidone or amisulpride. There may still be impetus to switch to an agent with a better profile since weight gain induced by olanzapine or clozapine often continues increasing even after the initial 6 week period.
Lowering the dose of a medication that has induced weight gain is another possible approach and has been used in dealing with this issue as well. Some studies, however, have suggested that this side effect may not be fully dose-related, and therefore this option may not be sufficiently effective.74
Lifestyle change
Lifestyle changes have been shown to provide some benefit in this area. In a study of a schizophrenic population a three part behavioral intervention of group weight-management sessions, individual weight-management sessions, and group exercise sessions was found to have significant improvements in weight compared to those who received treatment as usual.75 A review article of 18 studies involving behavioral interventions found that lifestyle interventions in the psychiatric population showed positive results, although these were less robust than similar studies in the general population.76
Meta-analysis has found that such interventions had a larger effect size than pharmacologic interventions in independent studies.72 The authors noted that in the only head-to-head comparison trial the opposite was found and metformin was more effective at producing weight loss than behavioral interventions. Such interventions are unfortunately not available to many patients, and the effectiveness of patient education and general suggestions of lifestyle change without more intensive interventions have not been fully determined.
Pharmacologic interventions
The addition of a second agent to counteract the metabolic effects or weight gain is a possible option if lifestyle changes are impractical, insufficient, or have failed. Several meta-analyses have been performed on a variety of pharmacologic interventions.72,77 In these, metformin has been identified as the medication having the strongest evidence for efficacy to reduce both weight gain and metabolic changes based on eleven available randomized control trials. Metformin (750 mg daily) is also an appealing choice in that it is relatively low-cost and has been found to be generally well-tolerated in trials.78,79 Other agents found to be effective in meta-analyses were: aripiprazole adjuvant therapy, topiramate, sibutramine, and reboxetine.
Several other agents have recently been suggested as possible therapies in this case. A recent trial found that melatonin was helpful in decreasing weight gain in bipolar patients with antipsychotic-induced weight gain.80 Vitamin D381 and omega 3 fatty acids have been proposed as possible therapies in the case of antipsychotic induced weight gain as well.
General approach to hyperlipidemia
Although not included in meta-analyses because of a lack of randomized control trials, the use of a statin for primary prevention of cardiovascular events in psychiatric patients, including those on antipsychotics has not been found to have significant contraindications.82 There is concern that statins may have a compounding effect with antipsychotic medication in increasing the risk of diabetes as statins have been found to increase the risk for insulin resistance. Thus far, studies investigating the use of a statin in patients on antipsychotic medications over a short period did not find an increase in fasting glucose or HbA1c levels.83,84 There does not appear to be evidence against using statins for patients on antipsychotics as determined by general guidelines for hyperlipidemia.
The American College of Cardiologists and the American Heart Association published guidelines for a general approach to hyperlipidemia in 2013.85 The foundation of the approach is lifestyle modification (diet, exercise, tobacco avoidance, healthy weight) which as noted above may be difficult to implement in a population with significant mental illness. Pharmacologic therapy is recommended for otherwise healthy patients over 21 years of age with low-density lipoprotein (LDL) greater than or equal to 190 mg/dL, for diabetic patients who are 40–75 years of age with LDL above or equal to 70 mg/dL, for patients 21–75 years of age who have clinical cardiovascular disease, and for those who are 40–75 years of age with a 10 year cardiovascular disease risk greater than or equal to 7.5% and LDL above or equal to 70 mg/dL.
The guidelines do not find evidence for efficacy of non-statin drugs (fibrates and niacin) to prevent cardiovascular events, and therefore do not generally recommend their use. Statin therapy is classified into three categories based on effects on LDL cholesterol: high-intensity for a 50% or more decrease (eg, atorvastatin 40–80 mg daily), moderate-intensity for 30%–50% decrease (eg, atorvastatin 10–20 mg daily), and low-intensity for less than 30% decrease (eg, pravastatin 10–20 mg).85
In contrast to the prior guidelines that focused on achieving specific LDL targets, the new guidelines recommend a specific intensity of statin therapy (eg, using high-intensity statins in patients with diabetes or cardiovascular disease), independent of previously used target LDL being reached as long as the patient can tolerate the medication without side effects.
In cases of patients taking medications with potential interactions with statins the recommendation is to use a lower-intensity statin, even when a higher-intensity statin would normally be recommended (eg, moderate-intensity instead of high-intensity). Before statin initiation in general the alanine aminotransferase (ALT) level should be checked and this is especially important in psychiatric patients as many antipsychotics (eg, olanzapine, quetiapine, and clozapine) can also cause transaminitis.86
Starting statins in patients on antipsychotics
An initial creatinine kinase (CK) level is only necessary in patients with a personal or family history of intolerance to statins, muscle disease, or who are on other medications that can interact with a statin to increase risk of myopathy. It should be noted that antipsychotics such as clozapine, loxapine, haloperidol, melperone, risperidone, and olanzapine have been known to cause significant CK elevations,87 and checking CK levels before starting a statin would be prudent. After initiation of statin therapy routine CK or ALT testing is not recommended, but should be done if the patient develops signs of hepatotoxicity (ALT) or muscle symptoms (CK).
When starting a statin in a patient who is taking antipsychotics, it is also important to consider possible metabolic interactions between these medications. For example, an increase in risperidone blood levels after addition of a statin has been documented and there have been case reports of rhabdomyolysis and compartment syndrome in a patient on risperidone after the addition of a statin.88,89
As mentioned above, statins could potentially have an effect of increasing blood glucose and hastening the onset of diabetes in patients at risk. The guidelines’ expert consensus notes that the occurrence of a major cardiovascular event is a much greater risk to health than the increase in blood glucose potentially causing diabetes.85 There have also been two randomized control trials of statins versus placebo in young, healthy patients that showed a significant worsening of cognitive indices relative to placebo (which would be worrisome for psychiatric patients whose cognitive abilities may be impaired at baseline),90 but a review of subsequent studies did not find evidence to support this finding.91
Myocarditis
As noted above, clozapine has been found to be an effective treatment in a subset of patients who do not respond to other antipsychotic agents.55 This agent also has its own unique side effect burden. A full discussion of the use and management of clozapine is beyond the scope of this article, however, one potentially life-threatening cardiovascular side effect of clozapine will be discussed.
Incidence of clozapine induced myocarditis has been estimated to be as high as approximately 1% of patients starting clozapine92 although others have found a lower incidence of about one in five hundred.93 It should be noted that although no definitive increased risk for myocarditis has been identified with other agents, quetiapine has been raised as a possible cause in several reported cases of myocarditis as well.94
The majority of clozapine-induced myocarditis occurs within the first 4 weeks of treatment, usually between days 14 and 21, although cases have been reported more than a year after treatment initiation.92,95 No specific monitoring guidelines have been recommended in the United States although guidelines have been proposed in Australia including baseline C-reactive protein (CRP), cardiac enzymes, and echocardiography.95
Certainly, all patients starting clozapine should be monitored for the signs and symptoms of this life threatening side effect and advised to seek medical treatment if these signs arise. The disease course of the illness generally begins with dyspnea, or flu-like symptoms, occurring along with diarrhea and dysuria followed 1 to 5 days later by hypotension or other signs of heart failure.95,96 Persistent tachycardia, chest pain, fever, or eosinophilia were all found to be predictive of myocarditis compared with healthy clozapine patients.92
Any of these findings should warrant immediate emergency medical care for workup of myocarditis. Case control studies have indicated that an increase in CRP is the first laboratory abnormality in cases of clozapine associated myocarditis. An increase in troponin I or troponin T and creatine kinase-MB (CKMB) follow, along with left ventricular dysfunction on echocardiography.95 It should be noted that eosinophilia was not present in all cases of myocarditis and even an eosinophil count of zero does not rule out myocarditis.95 Clozapine must be stopped if the diagnosis is suspected and rechallenge after a case of confirmed myocarditis is not recommended.97
Multidisciplinary approach
The above discussion highlights the complexity of the interplay between medical risks and psychiatric benefits of antipsychotic medications. The optimum approach to these issues would involve a multidisciplinary team approach including clinicians with expertise in mental illness, internal medicine, as well as psychiatric rehabilitation therapists, registered dietitians, and others who have specific training in educational and program based interventions for a psychiatric population. This would allow psychiatric providers to work closely with an internal medicine team to plot an appropriate course for each patient. It would also allow for input from rehabilitation therapists and dietary experts in providing interventions to increase physical activity and education regarding lifestyle choices including healthy eating habits and smoking cessation.
Such an approach is only possible in a controlled setting where patients spend all or much of their time and receive the majority of their care, such as in an inpatient unit or partial hospital program. A possible structure of the team in such a situation reverses the usual care model and makes the psychiatric provider the patient’s “primary physician” and the medical team the consultant. This approach has been effective at the Zucker Hillside Hospital in Long Island where a special medical consult team works with the psychiatric team to deal with medical issues arising from psychiatric care. These settings also allow for integration of extensive rehabilitation services to provide programs involving exercise along with dietary interventions.
In the outpatient setting most patients’ situations make such an approach impossible. Patients may be followed by multiple providers and disciplines and these may include a primary care physician who would communicate with the patient’s psychiatric provider and refer to dietary and rehabilitation programs as necessary. Unfortunately, many psychiatric patients do not have a primary care doctor, while others may not have an outpatient psychiatrist and are prescribed antipsychotic medication by a primary care provider. It is often difficult to coordinate referrals to registered dietitians or rehabilitation therapy in these situations and interdisciplinary communication is often strained by physical distance and scheduling issues. More programs are needed to improve integration and access for the mentally ill to outpatient services and to facilitate communication between specialties.
Conclusion
Many potential medical complications may arise in patients taking antipsychotic medications. Current literature shows that many antipsychotic agents prolong the QTc interval, which in turn is strongly associated to sudden cardiac death from fatal arrhythmias. It is therefore recommended that if an antipsychotic agent with the potential to prolong QTc is ordered for a patient a baseline ECG should be taken for patients with history or signs of arrhythmia (eg, syncope) and for those taking another agent that which could prolong QTc. Consideration and optimization of risk factors (if possible), drug choice, and appropriate continued ECG monitoring are also required to minimize risk of torsades or sudden death. A review of the APA and NICE guidelines is provided in Table 2.
Antipsychotic induced weight gain and metabolic abnormalities is another important area of clinical concern. In determining a treatment approach cardiovascular risk factors and weight gain must be considered against antipsychotic efficacy and psychiatric morbidity. In cases where an agent that has caused weight gain is required, lifestyle and diet changes may be used to improve outcomes but are difficult to implement. The addition of another agent may be a more practical approach in many situations. A proposed treatment algorithm in this case is provided in Figure 1.
Careful monitoring and early collaboration between medical disciplines to deal with these issues is the optimal approach to best manage these complicated situations. Unfortunately adherence to treatment guidelines has been poor in this area. Further study must focus on determining strategies to increase compliance with existing guidelines along with further investigation of behavioral and pharmacologic approaches.
Acknowledgment
The authors would like to acknowledge Christoph Correll, MD for his help in identifying relevant reviews in the area of antipsychotic induced weight gain.
Disclosure
The authors have no conflicts of interest to disclose.
References
ahrq.gov [homepage on the Internet]. Medical Expenditure Panel Survey Publication Details. US Deaprtment of Health and Human Services; 2014. Available from: http://meps.ahrq.gov/mepsweb/data_stats/Pub_ProdResults_Details.jsp?pt=Statistical Brief&opt=2&id=941. Accessed August 6, 2014. | |
Ronsley R, Scott D, Warburton WP, et al. A population-based study of antipsychotic prescription trends in children and adolescents in British Columbia, from 1996 to 2011. Can J Psychiatry. 2013;58(6):361–639. | |
Matone M, Localio R, Huang YS, dosReis S, Feudtner C, Rubin D. The Relationship between Mental Health Diagnosis and Treatment with Second-Generation Antipsychotics over Time: A National Study of US Medicaid-Enrolled Children. Health Serv Res. 2012;47(5):1836–1860. | |
Laursen TM, Munk-Olsen T, Vestergaard M. Life Expectancy and Cardiovascular Mortality in Persons with Schizophrenia. Curr Opin Psychiatry. 2012;25(2):83–88. | |
Wildgust HJ, Beary M. Are there Modifiable Risk Factors Which will Reduce the Excess Mortality in Schizophrenia? J Psychopharmacol. 2010;24(Suppl 4):37–50. | |
Acharya T, Acharya S, Tringali S, Huang J. Association of Antidepressant and Atypical Antipsychotic Use with Cardiovascular Events and Mortality in a Veteran Population. Pharmacotherapy. 2013;33(10):1053–1061. | |
Saravane D, Feve B, Frances Y, et al. Avec le soutien institutionnel du laboratoire Lilly [Drawing up guidelines for the attendance of physical health of patients with severe mental illness]. Encephale. 2009;35(4):330–339. French. | |
Arnoldy R, Curtis J, Samaras K. The Effects of Antipsychotic Switching on Diabetes in Chronic Schizophrenia. Diabet Med. 2014;31(3):e16–e19. | |
Bradford DW, Cunningham NT, Slubicki MN, et al. An Evidence Synthesis of Care Models to Improve General Medical Outcomes for Individuals With Serious Mental Illness. J Clin Psychiatry. 2013;74(8):e754–e764. | |
Ayad RF, Assar MD, Simpson L, Garner JB, Schussler JM. Causes and management of drug-induced long QT syndrome. Proc (Bayl Univ Med Cent). 2010;23(3):250–255. | |
Bazett HC. An analysis of the time-relations of electrocardiograms. Heart. 1920;7:353–370. | |
Molnar J, Zhang F, Weiss J, Ehlert FA, Rosenthal JE. Diurnal pattern of QTc interval: how long is prolonged? Possible relation to circadian triggers of cardiovascular events. J Am Coll Cardiol. 1996;27(1):76–83. | |
Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart. 2003;89(11):1363–1372. | |
Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350(10):1013–1022. | |
Hollister LE, Kosek JC. Sudden Death During Treatment With Phenothiazine Derivatives. JAMA. 1965;192:1035–1038. | |
Cancro R, Wilder R. A Mechanism of Sudden Death in Chlorpromazine Therapy. Am J Psychiatry. 1970;127(3):368–371. | |
Moore MT, Book MH. Sudden Death in Phenothiazine Therapy. Psychiatr Q. 1970;44(3):389–402. | |
Denvir MA, Sood A, Dow R, Brady AJ, Rankin AC. Thioridazine, diarrhoea and torsades de pointe. J R Soc Med. 1998;91(3):145–147. | |
Glassman, AH. Bigger JT Jr. Antipsychotic Drugs: Prolonged QTc Interval, Torsade De Pointes, and Sudden Death. Am J Psychiatry. 2001;158(11):1774–1782. | |
Kongsamut S, Kang J, Chen XL, Roehr J, Rampe D. A Comparison of the Receptor Binding and HERG Channel Affinities for a Series of Antipsychotic Drugs. Eur J Pharmacol. 2002;450(1):37–41. | |
Thomas SH. Drugs, QT Interval Abnormalities and Ventricular Arrhythmias. Adverse Drug React Toxicol Rev. 1994;13(2):77–102. | |
Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical Antipsychotic Drugs and the Risk of Sudden Cardiac Death. N Engl J Med. 2009;360(3):225–235. | |
omh.ny.gov [homepage on the Internet]. Lieberman JA, Merrill D, Parameswaran S, for the APA Council on Research. APA Guidance on the use of Antipsychotic Drugs and Cardiac Sudden Death. Available from: https://www.omh.ny.gov/omhweb/advisories/adult_antipsychotic_use_attachement.html. Accessed May 13, 2014. | |
Manu P, Kane JM, Correll CU. Sudden Death in Psychiatric Patients. J Clin Psychiatry. 2011;72(7):936–941. | |
Zhang Y, Post WS, Blasco-Colmenares E, Dalal D, Tomaselli GF, Guallar E. Electrocardiographic QT interval and mortality: a meta-analysis. Epidemiology. 2011;22(5):660–670. | |
Ozeki Y, Fujii K, Kurimoto N, et al. QTc prolongation and antipsychotic medications in a sample of 1017 patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(2):401–405. | |
Girardin FR, Gex-Fabry M, Berney P, Shah D, Gaspoz JM, Dayer P. Drug-induced long QT in adult psychiatric inpatients: the 5-year cross-sectional ECG Screening Outcome in Psychiatry study. Am J Psychiatry. 2013;170(12):1468–1476. | |
Sumic JC, Baric V, Bilic P, Herceg M, Sisek-Sprem M, Jukic V. QTc and psychopharmacs: are there any differences between monotherapy and polytherapy. Ann Gen Psychiatry. 2007;6:13. | |
Rabkin SW. Aging Effects on QT Interval: Implications for Safety of antipsychotic drugs. J Geriatr Cardiol. 2014;11(1):20–25. | |
Correll CU, Harris J, Figen V, Kane JM, Manu P. Antipsychotic drug administration does not correlate with prolonged rate-corrected QT interval in children and adolescents: results from a nested case-control study. J Child Adolesc Psychopharmacol. 2011;21(4):365–368. | |
Johnsen E, Aanesen K, Sriskandarajah S, Kroken RA, Løberg EM, Jørgensen HA. QTc Prolongation in Patients Acutely Admitted to Hospital for Psychosis and Treated with Second Generation Antipsychotics. Schizophr Res Treatment. 2013;2013:375020. | |
Curtis LH, Østbye T, Sendersky V, et al. Prescription of QT-prolonging drugs in a cohort of about 5 million outpatients. Am J Med. 2003;114(2):135–141. | |
psychiatryonline.org [homepage on the Internet]. American Psychiatric Association Practice Guidelines for the Treatment of Psychiatric Disorders; 2006. Available from: http://psychiatryonline.org/content.aspx?bookid =28§ionid=1665359. Accessed May 13, 2014. | |
National Institute for Health and Care Excellence. NICE Clinical Guideline 178: Psychosis and Schizophrenia in Adults: Treatment and Management. National Institute for Health and Care Excellence; 2014. Available from: http://www.nice.org.uk/nicemedia/live/14382/66534/66534.pdf. Accessed May 13, 2014. | |
Purhonen M, Koponen H, Tiihonen J, Tanskanen A. Outcome of patients after market withdrawal of thioridazine: a retrospective analysis in a nationwide cohort. Pharmacoepidemiol Drug Saf. 2012;21(11):1227–1231. | |
Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. | |
Strom BL, Eng SM, Faich G, et al. Comparative mortality associated with ziprasidone and olanzapine in real-world use among 18,154 patients with schizophrenia: The Ziprasidone Observational Study of Cardiac Outcomes (ZODIAC). Am J Psychiatry. 2011;168(2):193–201. | |
US Food and Drug Administration. “Drugs.” Information for Healthcare Professionals: Haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate). Available from: http://www.fda.gov/Drugs/DrugSafety/ucm085203.htm. Accessed May 13, 2014. | |
Muzyk AJ, Rayfield A, Revollo JY, Heinz H, Gagliardi JP. Examination of baseline risk factors for QTc interval prolongation in patients prescribed intravenous haloperidol. Drug Saf. 2012;35(7):547–553. | |
Chung AK, Chua SE. Effects on prolongation of Bazett’s corrected QT interval of seven second-generation antipsychotics in the treatment of schizophrenia: a meta-analysis. J Psychopharmacol. 2011;25(5):646–666. | |
Poluzzi E, Raschi E, Koci A, et al. Antipsychotics and torsadogenic risk: signals emerging from the US FDA Adverse Event Reporting System database. Drug Saf. 2013;36(6):467–479. | |
Kane JM. Lurasidone: a clinical overview. J Clin Psychiatry. 2011; 72 Suppl 1:24–28. | |
Allison DB, Mentore JL, Heo M, et al. Antipsychotic-Induced Weight Gain: A Comprehensive Research Synthesis. Am J Psychiatry. 1999; 156(11):1686–1696. | |
Mitchell AJ, Vancampfort D, De Herdt A, Yu W, De Hert M. Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta-analysis of first episode, untreated and treated patients. Schizophr Bull. 2013;39(2):295–305. | |
Said MA, Sulaiman AH, Habil MH, et al. Metabolic syndrome and cardiovascular risk among patients with schizophrenia receiving antipsychotics in Malaysia. Singapore Med J. 2012;53(12):801–807. | |
Krane-Gartiser K, Breum L, Glümrr C, et al. Prevalence of the metabolic syndrome in Danish psychiatric outpatients treated with antipsychotics. Nord J Psychiatry. 2011;65(5):345–352. | |
Holt RI. Consensus development conference on antipsychotic drugs and obesity and diabetes: response to consensus statement. Diabetes Care. 2004;27(8):2086–2087. | |
Mitchell AJ, Delaffon V, Vancampfort D, Correll CU, De Hert M. Guideline concordant monitoring of metabolic risk in people treated with antipsychotic medication: systematic review and meta-analysis of screening practices. Psychol Med. 2012;42(1):125–147. | |
Barnes TR, Paton C, Cavanagh MR, Hancock E, Taylor DM; UK Prescribing Observatory for Mental Health. A UK audit of screening for the metabolic side effects of antipsychotics in community patients. Schizophr Bull. 2007;33(6):1397–1403. | |
Morrato EH, Newcomer JW, Kamat S, Baser O, Harnett J, Cuffel B. Metabolic screening after the American Diabetes Association’s consensus statement on antipsychotic drugs and diabetes. Diabetes Care. 2009;32(6):1037–1042. | |
Haupt DW, Rosenblatt LC, Kim E, Baker RA, Whitehead R, Newcomer JW. Prevalence and Predictors of Lipid and Glucose Monitoring in Commercially Insured Patients Treated with Second-Generation Antipsychotic Agents. Am J Psychiatry. 2009;166(3):345–353. | |
Malhotra AK, Correll CU, Chowdhury NI, et al. Association between common variants near the melanocortin 4 receptor gene and severe antipsychotic drug-induced weight gain. Arch Gen Psychiatry. 2012;69(9):904–912. | |
Ward A, Quon P, Abouzaid S, Haber N, Ahmed S, Kim E. Cardiometabolic consequences of therapy for chronic schizophrenia using second-generation antipsychotic agents in a medicaid population: clinical and economic evaluation. P T. 2013;38(2):109–115. | |
Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209–1223. | |
Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789–796. | |
Rummel-Kluge C, Komossa K, Schwarz S, et al. Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysis. Schizophr Res. 2010;123(2–3):225–233. | |
Citrome L, Kalsekar I, Baker RA, Hebden T. A review of real-world data on the effects of aripiprazole on weight and metabolic outcomes in adults. Curr Med Res Opin. 2014;30(8):1629–1641. | |
Aripiprazole [package insert]. Rockville, MD: Otsuka America Pharmaceutical, Inc; 2014. Available from: http://www.otsuka-us.com/Documents/Abilify.PI.pdf. Accessed June 19, 2014. | |
Ziprazidone [package insert]. New York, NY: Pfizer Inc; 2014. Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=584. Accessed June 19, 2014. | |
Lurasidone [package insert]. Marlborough, MA: Sunovion Pharmaceuticals Inc; 2013. Available from: http://www.latuda.com/LatudaPrescribingInformation.pdf. Accessed June 19, 2014. | |
Paliperidone [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2011. Available from: http://www.invega.com/prescribing-information. Accessed September 26, 2014. | |
Quetiapine [package insert]. Wilmington, DE: AstraZeneca; 2014. Available from: http://www1.astrazeneca-us.com/pi/seroquel.pdf. Accessed June 19, 2014. | |
Risperidone [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2014. Available from: http://www.janssenpharmaceuticalsinc.com/assets/risperdal.pdf. Accessed June 19, 2014. | |
Asenapine [package insert]. Whitehouse Station, NJ: Merck & Co; 2013. Available from: http://www.merck.com/product/usa/pi_circulars/s/saphris/saphris_pi.pdf. Accessed June 19, 2014. | |
Iloperidone [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2014. Available from: http://www.pharma.us.novartis.com/product/pi/pdf/fanapt.pdf. Accessed June 19, 2014. | |
Olanzapine [package insert]. Indianapolis, IN: Lilly USA, LLC; 2013. Available from: http://pi.lilly.com/us/zyprexa-pi.pdf. Accessed June 19, 2014. | |
Clozapine [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2013. Available from: https://www.pharma.us.novartis.com/product/pi/pdf/Clozaril.pdf. Accessed June 19, 2014. | |
Citrome L. Quantifying risk: the role of absolute and relative measures in interpreting risk of adverse reactions from product labels of antipsychotic medications. Curr Drug Saf. 2009;4(3):229–237. | |
De Hert M, Detraux J, van Winkel R, Yu W, Correll CU. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114–126. | |
De Hert M, Yu W, Detraux J, Sweers K, van Winkel R, Correll CU. Body weight and metabolic adverse effects of asenapine, iloperidone, lurasidone and paliperidone in the treatment of schizophrenia and bipolar disorder: a systematic review and exploratory meta-analysis. CNS Drugs. 2012;26(9):733–759. | |
Essock SM, Covell NH, Davis SM, Stroup TS, Rosenheck RA, Lieberman JA. Effectiveness of switching antipsychotic medications. Am J Psychiatry. 2006;163(12):2090–2095. | |
Maayan L, Correll CU. Management of antipsychotic-related weight gain. Expert Rev Neurother. 2010;10(7):1175–1200. | |
Bak M, Fransen A, Janssen J, van Os J, Drukker M. Almost all antipsychotics result in weight gain: a meta-analysis. PLoS One. 2014;9(4):e94112. | |
Baptista T, Kin NM, Beaulieu S, de Baptista EA. Obesity and related metabolic abnormalities during antipsychotic drug administration: mechanisms, management and research perspectives. Pharmacopsychiatry. 2002;35(6):205–219. | |
Daumit GL, Dickerson FB, Wang NY, et al. A behavioral weight-loss intervention in persons with serious mental illness. N Engl J Med. 2013;368(17):1594–1602. | |
Cabassa LJ, Ezell JM, Lewis-Fernández R. Lifestyle interventions for adults with serious mental illness: a systematic literature review. Psychiatr Serv. 2010;61(8):774–782. | |
Mizuno Y, Suzuki T, Nakagawa A, et al. Pharmacological Strategies to Counteract Antipsychotic-Induced Weight Gain and Metabolic Adverse Effects in Schizophrenia: A Systematic Review and Meta-analysis. Schizophr Bull. Epub March 17, 2014. | |
Wu RR, Zhao JP, Guo XF, et al. Metformin addition attenuates olanzapine-induced weight gain in drug-naive first-episode schizophrenia patients: a double-blind, placebo-controlled study. Am J Psychiatry. 2008;165(3):352–358. | |
Wu RR, Zhao JP, Shao P, et al. Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain: a randomized controlled trial. JAMA. 2008;299(2):185–193. | |
Romo-Nava F, Alvarez-Icaza González D, Fresán-Orellana A, et al. Melatonin attenuates antipsychotic metabolic effects: an eight-week randomized, double-blind, parallel-group, placebo-controlled clinical trial. Bipolar Disord. 2014;16(4):410–421. | |
Nwosu BU, Meltzer B, Maranda L, et al. A potential role for adjunctive vitamin D therapy in the management of weight gain and metabolic side effects of second-generation antipsychotics. J Pediatr Endocrinol Metab. 2011;24(9–10):619–626. | |
Andrade C. Primary prevention of cardiovascular events in patients with major mental illness: a possible role for statins. Bipolar Disord. 2013;15(8):813–823. | |
De Hert M, Kalnicka D, van Winkel R, et al. Treatment with rosuvastatin for severe dyslipidemia in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry. 2006;67(12):1889–1896. | |
Hanssens L, De Hert M, Kalnicka D, et al. Pharmacological treatment of severe dyslipidaemia in patients with schizophrenia. Int Clin Psychopharmacol. 2007;22(1):43–49. | |
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–S45. | |
McEvoy GK, editor. AHFS Drug Information®. 56th ed. Bethesda, MD: American Society of Health-System Pharmacists; 2014. | |
Meltzer HY, Cola PA, Parsa M. Marked elevations of serum creatine kinase activity associated with antipsychotic drug treatment. Neuropsychopharmacology. 1996;15(4):395–405. | |
Walker JL, Smith GH, Gaston MS, Robinson CM. Spontaneous compartment syndrome in association with simvastatin-induced myositis. Emerg Med J. 2008;25(5):305–306. | |
Patier JL, Ferrere F, Moreno-Cobo MA, Echaniz A. Rabdomiólisis producida por la asociación de sinvastatina y risperidona [Rhabdomyolysis caused by the association of simvastatin and risperidone]. Med Clin (Barc). 2007;129(11):439. Spanish. | |
Golomb BA, Evans MA. Statin adverse effects : a review of the literature and evidence for a mitochondrial mechanism. Am J Cardiovasc Drugs. 2008;8(6):373–418. | |
Richardson K, Schoen M, French B, et al. Statins and Cognitive Function: A Systematic Review. Ann Intern Med. 2013;159(10):688–697. | |
Haas SJ, Hill R, Krum H, et al. Clozapine-associated myocarditis: a review of 116 cases of suspected myocarditis associated with the use of clozapine in Australia during 1993–2003. Drug Saf. 2007;30(1):47–57. | |
Kilian JG, Kerr K, Lawrence C, Celermajer DS. Myocarditis and cardiomyopathy associated with clozapine. Lancet. 1999;354(9193):1841–1845. | |
[No authors listed]. Quetiapine and cardiac muscle disorders. Prescrire Int. 2013;22(140):184. | |
Ronaldson KJ, Fitzgerald PB, Taylor AJ, Topliss DJ, McNeil JJ. A new monitoring protocol for clozapine-induced myocarditis based on an analysis of 75 cases and 94 controls. Aust N Z J Psychiatry. 2011;45(6):458–465. | |
Ronaldson KJ, Taylor AJ, Fitzgerald PB, Topliss DJ, Elsik M, McNeil JJ. Diagnostic characteristics of clozapine-induced myocarditis identified by an analysis of 38 cases and 47 controls. J Clin Psychiatry. 2010;71(8):976–981. | |
Manu P, Sarpal D, Muir O, Kane JM, Correll CU. When can patients with potentially life-threatening adverse effects be rechallenged with clozapine? A systematic review of the published literature. Schizophr Res. 2012;134(2–3):180–186. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.