")
Back to Journals » International Journal of General Medicine » Volume 13
Management Strategies of Melkersson-Rosenthal Syndrome: A Review
Authors Dhawan SR , Saini AG, Singhi PD
Received 29 August 2019
Accepted for publication 22 January 2020
Published 26 February 2020 Volume 2020:13 Pages 61—65
DOI https://doi.org/10.2147/IJGM.S186315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sumeet R Dhawan,1 Arushi G Saini,2 Pratibha D Singhi2,3
1Department of Pediatrics, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, 133207, India; 2Pediatric Neurology Unit, Department of Pediatrics, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India; 3Medanta, The Medicity, Gurgaon, Haryana, India
Correspondence: Pratibha D Singhi Medanta, The Medicity, Gurgaon, Haryana, India
Tel +91 8168186894
Email [email protected]
Abstract: Melkerrson-Rosenthal syndrome is a rare disorder of unknown aetiology and characterized by the triad of oro-facial edema, facial nerve palsy, and furrowing of the tongue. Two or more of the above are essential for making a clinical diagnosis. The mainstay of treatment is corticosteroids. Intralesional triamcinolone acetonide may be used for the treatment of oro-facial edema. Another treatment option for oro-facial edema includes intralesional betamethasone, along with oral doxycycline. The review discusses the management strategies in Melkersson-Rosenthal syndrome.
Keywords: facial palsy, Bell’s palsy, facial edema, lip edema, orofacial granulomatosis, recurrent facial palsy, fissured tongue, lingua plicata
Introduction
Melkersson-Rosenthal syndrome (MRS) is a clinical syndrome characterized by the triad of oro-facial edema, facial nerve palsy, and furrowing of the tongue. The syndrome was first described in 1928 by Ernst Gustaf Melkersson in a 35-year female with oro-facial edema and facial paralysis.1 Associations of facial paralysis and fissured tongue (by Rosenthal) were described in 1931.2,3 The onset of symptoms is most commonly between 25 and 40 years (range 1–69 years), with a female preponderance (sex ratio of 2:1).4,5 MRS is rare in children, and only a handful of 30 cases have been described.6,7 Onset in children is common between 7 and 12 years of age, with the youngest child described at 22 months of age. The diagnosis is frequently delayed with the median time to the diagnosis being 4–9 years.7
Diagnostic Features
Melkersson-Rosenthal syndrome (MRS) is a clinical syndrome characterized by the triad of oro-facial edema, recurrent facial nerve palsy, and furrowing/fissuring of the tongue (also known as lingua plicata). Two or more of the above are essential for making a clinical diagnosis.8 Only one of the two clinical features is sufficient for diagnosis in the presence of histopathological evidence of granulomatous cheilitis in the biopsy of the eyelid or the lip. The term oligosymptomatic MRS is used when two clinical features are present, and monosymptomatic when only one symptom is present. The monosymptomatic cases are diagnosed when there is biopsy evidence of a non-necrotising, granulomatous cheilitis in patients with isolated facial or lip edema (Miescher MRS).9 In some cases, only lymphocytic inflammation around the blood vessels may be present, and frank granulomas may be absent. The histopathological findings may be missed if sampling is not done during the acute episodes.
The diagnosis is difficult in cases of isolated facial paralysis or isolated eyelid edema alone. Rarely, all the three features are present (20–75%).4,5 Isolated eyelid edema is a part of several diseases such as orbital malignancies, orbital pseudotumor, Grave’s disease, and allergic disorders.10 Incomplete presentations often present to the dermatologist or the otorhinolaryngologist and may be missed if the suspicion is low, especially at a young age. However, the presence of recurrent facial nerve palsies in children should alert the treating physician to the presence of an underlying MRS. Facial palsy is usually the first clinical feature and precedes oro-facial edema by months to years. Facial paralysis may be unilateral or bilateral. Recurrent facial paralysis is seen in 10% of the cases.11 Facial paralysis is seen in 30–90% of cases, and is associated with facial edema in 13–50% of cases.5 In a series by Tang et al, facial paralysis was bilateral in 40% of the cases.4 The duration of facial palsy increases as the disease progresses, with a tendency to become longer in duration.
Fissured tongue (lingua plicata) is defined as grooves on the dorsum of the tongue which are at least 2 mm deep and 15 mm long.12 It is seen in 30–80% of cases of MRS.5 Fissuring may lead to secondary infections, hypertrophy, loss of papillae, loss of taste, and dysesthesia. Fissuring may be familial/hereditary. In a series of cases of MRS, 9% had fissuring since childhood, and 11% of the family members also had fissuring.4 Besides the three cardinal symptoms, migraine, headache, and dizziness were present in half of the patients.9 Other neurological symptoms which may be seen in MRS include tinnitus, deafness, facial paresthesias, difficulty in swallowing, hypogeusia, conjunctival congestion, aphthous ulcers, reduced or excessive facial sweating, excessive tears in the eye and visual disturbances. Other cranial nerves like trigeminal, olfactory, auditory, glossopharyngeal, and hypoglossal nerves can also be involved.13 Non-neurological symptoms include uveitis, diverticulitis, and ulcerative colitis. Recurrent episodes of MRS may lead to personality changes, anxiety, and depression.
Edema is painless, non-pitting and most commonly seen in the upper limbs, but may also be seen in lower lip, tongue, buccal area, eyelids, neck, gingiva, nose, upper arms, genitalia, and the larynx.4,5,7 Partial or non-resolution of edema may lead to fibrosis and may lead to permanent disfiguration of the face.
Etiology
The etiology if MRS is unclear. The etiopathogenesis of this rare pediatric disorder has been linked to HSV1 infections, hereditary granulomatous disorders, mycobacterial infections (tuberculosis, leprosy), chronic infections, Down’s syndrome, psoriasis, thyroiditis, multiple sclerosis, keratitis, Wegener’s granulomatous, diabetes mellitus, sarcoidosis, ulcerative colitis, and allergic disorders.5,7,14 Influenza respiratory infection may trigger a relapse of MRS. Gene mutations causing UNC-93B deficiency may predispose to HSV-1 infections.15 This deficiency selectively impairs immunity against HSV-1 but not against other organisms.16 Cases with a herpes-like lesion at the onset of facial edema have been described. Mutations in FATP1 (fatty acid transport protein) have been described in one family.17 In another family, four generation of family members were affected due to an autosomal dominant transmission.18 Rare complications of MRS include sinusitis, candida infection, facial erythema, IgA nephropathy, vitiligo, thyroid hormonal abnormalities, and lacunar strokes.4 In the absence of clear-cut etiologies of MRS, terms MRS, cheilitis granulomatosa, granulomatous cheilitis, and monosymptomatic MRS are used interchangeably in different publications.19 Inflammatory bowel disease like Crohn’s disease may present with oral manifestations such as lip swelling with fissures on lips, mucositis, gingivitis, glossitis, and cobblestone appearance of the oral mucosa.20 There may occasionally be seen in MRS and confuse the clinical picture. Investigations are primarily directed to the exclusion of systemic etiologies (Box 1).
Treatment Corticosteroids
There is a significant role of abnormal immune function, immune deregulation, allergic tendencies in patients with MRS. So, short courses of immunosuppressants are often used in the treatment of MRS. There is no specific treatment for MRS. Traditionally, corticosteroids have been the mainstay of treatment.7 There are no randomized trials to suggest the corticosteroid type and duration that should be used. Therapy with corticosteroids leads to improvement in 50–80% of patients and reduced relapse frequency by 60–75%.7 Typically, oral corticosteroids are used for 1 week and tapered over 2 weeks. High-dose pulse methylprednisolone has been used in severe cases.
Treatment of Oro-Facial Edema
Intralesional triamcinolone acetonide (TA) (1–1.5 mL of 10–20 mg/mL solution) and lignocaine may be used in local edema.21 In another study, a higher dose of intralesional TA of 40 mg/mL was used.22 TA was injected at four sides in each lip. Additional TA was injected in cheek and nasolabial folds. Three such weekly injections were given. The course was repeated after 6 months in case of persisting edema or recurrence. This treatment strategy leads to a significant decrease in the severity of edema as well as edema recurrences. The study was a retrospective study with 22 patients. Fourteen patients received only single injection and did not have any recurrence.22 The mean disease-free period after injection of TA was 28 months. All treated patients were disease-free after 2–4 weeks of injection with TA. Alternatively, intralesional betamethasone, along with oral doxycycline, may be used if TA is not available.23 Eutectic lignocaine (prilox) may be used to reduce pain before intralesional injections. Intralesional TA is likely to be beneficial in cheilitis granulomatosa without systemic disease. Doxycycline and minocycline have been postulated to inhibit of synthesis of protein kinase C.23 Corticosteroid-antibiotic combinations with minocycline, and roxithromycin have also been used because of the possible anti-inflammatory effect in these two antibiotics.24 We suggest oral corticosteroid if both facial paralysis and oro-facial edema are present, and intralesional injections if oro-facial edema alone is present or is refractory to oral corticosteroid.
Ancillary Treatment
Vitamins like thiamine, niacin, riboflavin, pyridoxine, ascorbic acid, and vitamin E have often been used along with corticosteroids. Other treatments tried with unproven benefits include benzoate-free diet, cinnamon-free diet, and acyclovir.25,26 Fumaric acid esters have an anti-proliferative effect on lymphocytes and macrophages. These medicines are used in the treatment of psoriasis and have shown some benefit in orofacial granulomatosis.27
Other Immunosuppressants
In patients with other systemic involvement, immunosuppressants are also used. In possible cases of collagen vascular diseases, methotrexate,28 thalidomide,29 intravenous immunoglobulins, clofazimine,30 dapsone,31,32 anti-TNF therapy (infliximab),33 anti-histaminic drugs and hydroxychloroquine have been used in isolated cases.4,5,7 In a case report by Moll et al, a 69-year-old woman with MRS, type-2 diabetes and psoriasis was treated successfully by Adalimumab after 4 years of failed therapy.34 It is hypothesized that tumour necrosis factor is responsible for granuloma formation and so anti-TNF like Adalimumab has been used in the treatment of psoriasis, Crohn’s disease and sarcoidosis.34 In another case, a 39-year woman with vulvar lump (histopathology showing tuberculoid-type granulomas) with a past history of MRS was successfully treated with Infliximab (chimeric monoclonal antibody).33 In another case of 24-year woman with intralesional steroid refractory lip edema was treated successfully with Infliximab. In another series of 14 patients with oro-facial granulomatosis treated with Infliximab and Adalimumab, short-term response was seen in 70% of patients.35 Adalimumab was effective in two patients who failed Infliximab. The authors suggest that patients with oral sulcus involvement, intestinal Crohn’s disease and an elevated C‐reactive protein are likely candidates of anti-YNF therapy.35
Surgical Management
Surgical management may be done in recurrent facial palsies. The timing of surgery is uncertain. Total facial nerve decompression may be done by the middle cranial fossa approach. Standard mastoidectomy is done, and the facial nerve is decompressed from internal auditory meatus to geniculate ganglion. In one such study, none of the patients experienced a relapse of facial palsy compared to the patients who were treated medically.36 Nearly 90% of patients who were operated recuperated to a near-normal status.36 An alternate surgical approach like subtotal nerve decompression from stylomastoid foramen to geniculate ganglion can also be made.37 This approach has a minor risk of conductive hearing loss.
Surgeries of lips may also be done for persistent lip edema. In one such case, based on Conway’s technique, en-block removal of mucosa dorsal to vermillion was done.38 Part of orbicularis muscle and grossly edematous tissue were also removed.38 Helium laser ablation is an alternative procedure for cheiloplasty. Both these procedures may cause loss of sensation in the affected lip and do not affect disease recurrence.24
Conclusion
Short duration oral corticosteroids are the mainstay in the treatment of MRS. Intralesional triamcinolone acetonide may be used in oro-facial edema. Refractory/recurrent MRS may need second-line immunosuppressants like methotrexate and thalidomide. Surgical decompression of the facial nerve may be considered in medically refractory recurrent facial nerve palsies. Cheiloplasty may be considered in cases of failure of triamcinolone acetonide.
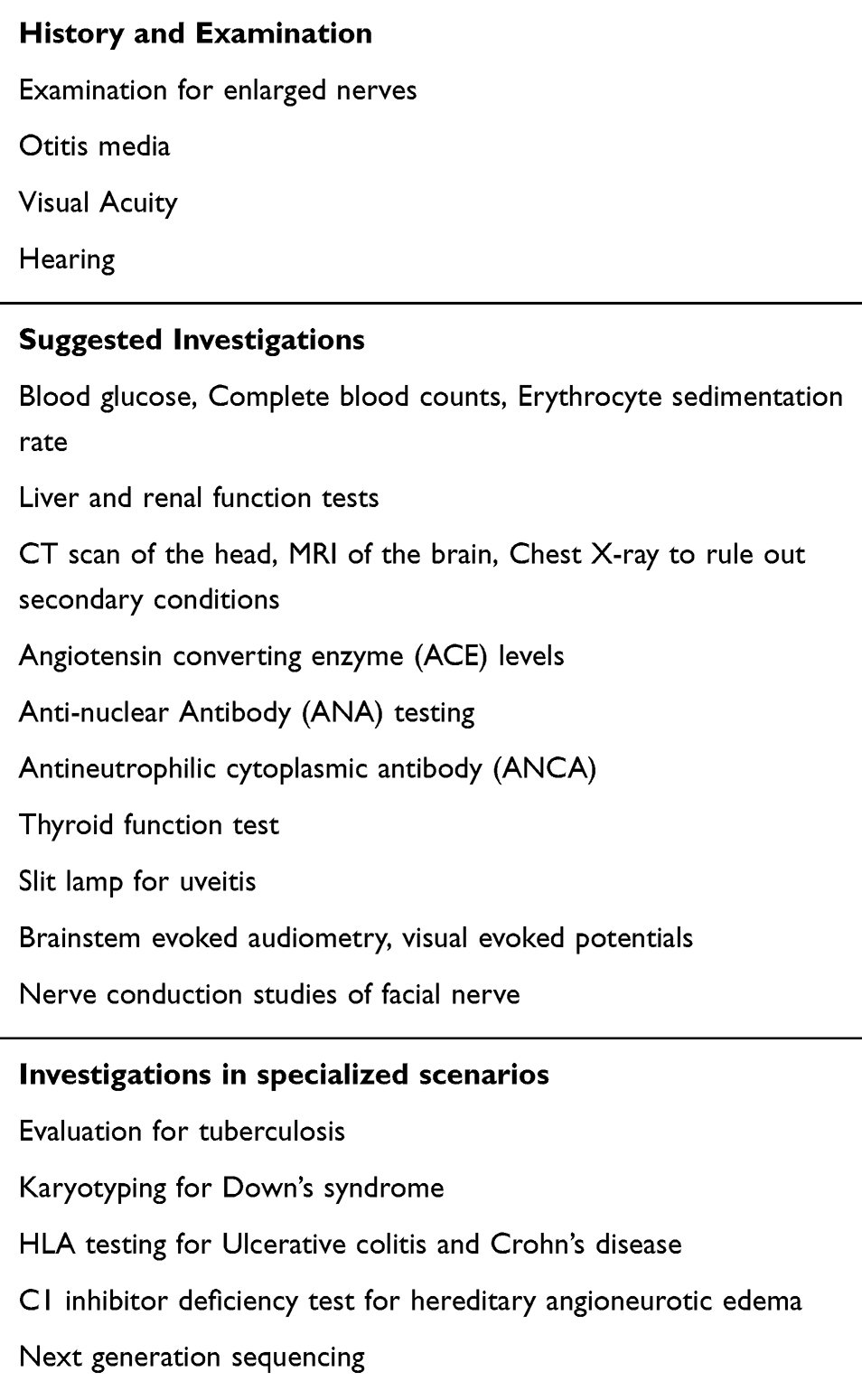 |
Box 1 Investigations in Patients with Suspected Melkersson-Rosenthal Syndrome |
Disclosure
The authors report no conflicts of interest in this work.
References
1. Melkersson E. Ett fall av recideverande facial spares. Samband Med Angioneurotisk Odem Hygeia (Stockholm). 1928;90:737–741.
2. Rosenthal C. Clinisch-erbbiologischer beitrag zur Konstitutions-Pathologie-Gemeknsames Auftreten von (rezidivierender familiarer) Facialislahmung, angioneurotische angioneurotischem und Lingua Plicata in Arthritiomus Famielien. Z Ges Neurol Psychiatr. 1931;131:475. doi:10.1007/BF02865984
3. Değerli Ş, Başman A, Gümüşok M, Kaya M, Alkurt MT. Melkersson-Rosenthal syndrome: a case report. J Istanb Univ Fac Dent. 2017;51(1):42–45. doi:10.17096/jiufd.96279
4. Tang J-J, Shen X, Xiao J-J, Wang X-P. Retrospective analysis of 69 patients with Melkersson-Rosenthal syndrome in mainland China. Int J Clin Exp Med. 2016;9(2):3901–3908.
5. Orlando MR, Atkins JS. Melkersson-Rosenthal syndrome. Arch Otolaryngol Head Neck Surg. 1990;116(6):728–729. doi:10.1001/archotol.1990.01870060086017
6. Saini AG, Sankhyan N, Padmanabh H, Das A, Singhi P. Recurrent facial palsy and electrophysiological findings in oligosymptomatic Melkersson Rosenthal syndrome. Indian J Pediatr. 2016;83(10):1188–1190. doi:10.1007/s12098-016-2137-8
7. Savasta S, Rossi A, Foiadelli T, et al. Melkersson–Rosenthal syndrome in childhood: report of three paediatric cases and a review of the literature. Int J Environ Res Public Health. 2019;16(7):1289. doi:10.3390/ijerph16071289
8. Dodi I, Verri R, Bravi B. A monosymptomatic Melkersson-Rosenthal syndrome in an 8 years old boy. Acta Bio Medica Atenei Parmensis. 2006;77(1):20–23.
9. Kanerva M, Moilanen K, Virolainen S, Vaheri A, Pitkaranta A. Melkersson-Rosenthal syndrome. Otolaryngol Head Neck Surg. 2008;138(2):246–251. doi:10.1016/j.otohns.2007.11.015
10. Rawlings N, Valenzuela A, Allen L, Heathcote J. Isolated eyelid edema in Melkersson–Rosenthal syndrome: a case series. Eye. 2012;26(1):163. doi:10.1038/eye.2011.285
11. Wang J, Li P, Jin X, Xu Y, Zhang X. Outcomes of recurrent facial palsy in Melkersson Rosenthal syndrome. Ann Otol Rhinol Laryngol. 2015;124(3):232–234. doi:10.1177/0003489414551981
12. Axell T. A prevalence study of oral mucosal lesions in an adult Swedish population. Odontol Revy Suppl. 1976;36:1–103.
13. Zeng W, Geng S, Niu X, Yuan J. Complete Melkersson–Rosenthal syndrome with multiple cranial nerve palsies. Clin Exp Dermatol. 2010;35(3):272–274. doi:10.1111/ced.2010.35.issue-3
14. Okudo J, Oluyide Y. Melkersson-Rosenthal syndrome with orofacial swelling and recurrent lower motor neuron facial nerve palsy: a case report and review of the literature. Case Rep Otolaryngol. 2015;2015:1–3. doi:10.1155/2015/214946
15. Zhang S-Y, Abel L, Casanova J-L. Mendelian predisposition to herpes simplex encephalitis. In: Dulac O, Lassonde M, Sarnat HB, editors. Handbook of Clinical Neurology. Vol. 112. Elsevier; 2013:1091–1097.
16. Casrouge A, Zhang SY, Eidenschenk C, et al. Herpes simplex virus encephalitis in human UNC-93B deficiency. Science. 2006;314(5797):308–312. doi:10.1126/science.1128346
17. Xu X, Guan L, Lv Y, et al. Exome sequencing identifies FATP1 mutation in Melkersson-Rosenthal syndrome. J Eur Acad Dermatol Venereol. 2017;31(5):e230. doi:10.1111/jdv.14042
18. Lygidakis C, Tsakanikas C, Ilias A, Vassilopoulos D. Melkersson‐Rosenthal’s syndrome in four generations. Clin Genet. 1979;15(2):189–192. doi:10.1111/j.1399-0004.1979.tb01760.x
19. Wehl G, Rauchenzauner M. A systematic review of the literature of the three related disease entities cheilitis granulomatosa, orofacial granulomatosis and Melkersson–Rosenthal syndrome. Curr Pediatr Rev. 2018;14(3):196–203. doi:10.2174/1573396314666180515113941
20. Troiano G, Dioguardi M, Giannatempo G, et al. Orofacial granulomatosis: clinical signs of different pathologies. Med Princ Pract. 2015;24(2):117–122. doi:10.1159/issn.1011-7571
21. Bacci C, Valente M. Successful treatment of cheilitis granulomatosa with intralesional injection of triamcinolone. J Eur Acad Dermatol Venereol. 2010;24(3):363–364. doi:10.1111/jdv.2010.24.issue-3
22. Fedele S, Fung P, Bamashmous N, Petrie A, Porter S. Long‐term effectiveness of intralesional triamcinolone acetonide therapy in orofacial granulomatosis: an observational cohort study. Br J Dermatol. 2014;170(4):794–801. doi:10.1111/bjd.2014.170.issue-4
23. Oudrhiri L, Chiheb S, Marnissi F, Zamiati S, Benchikhi H. Successful treatment of Miescher’s cheilitis in Melkersson-Rosenthal syndrome with betamethasone injections and doxycycline. Pan Afr Med J. 2012;13.
24. Banks T, Gada S. A comprehensive review of current treatments for granulomatous cheilitis. Br J Dermatol. 2012;166(5):934–937. doi:10.1111/bjd.2012.166.issue-5
25. Campbell H, Escudier M, Patel P, Challacombe S, Sanderson J, Lomer M. cinnamon‐and benzoate‐free diet as a primary treatment for orofacial granulomatosis. Aliment Pharmacol Ther. 2011;34(7):687–701. doi:10.1111/j.1365-2036.2011.04792.x
26. Espinoza I, Navarrete J, Benedetto J, Borzutzky A, Roessler P, Ortega-Pinto A. Orofacial granulomatosis and diet therapy: a review of the literature and two clinical cases. An Bras Dermatol. 2018;93(1):80–85. doi:10.1590/abd1806-4841.20185828
27. Kleine R, Brohl L, Amon U. Fumarsäureestertherapie bei einer jungen Patientin mit ausgeprägter Cheilitis granulomatosa [Treatment of granulomatous cheilitis with fumaric acid esters in a young woman]. Hautarzt. 2011;62(12):940–942. German. doi:10.1007/s00105-011-2174-1
28. Tonkovic-Capin V, Galbraith SS, Rogers RS
29. Medeiros M
30. Bygum A, Toft-Petersen M. Melkersson-Rosenthals syndrom behandlet med clofazimin [Melkersson-Rosenthal syndrome treated with clofazimine]. Ugeskr Laeger. 2008;170(3):159. Danish.
31. Emiroglu N, Su O, Cengiz FP, Onsun N. Successful treatment of Melkersson-Rosenthal syndrome with dapsone: a case report and review of the literature. Dermatol Online J. 2016;22(10).
32. Sobjanek M, Wlodarkiewicz A, Zelazny I, Nowicki R, Michajlowski I, Sokolowska-Wojdylo M. Successful treatment of Melkersson-Rosenthal syndrome with dapsone and triamcinolone injections. J Eur Acad Dermatol Venereol. 2008;22(8):
33. Wickramasinghe N, Gunasekara CN, Fernando WS, Hewavisenthi J, de Silva HJ. Vulvitis granulomatosa, Melkersson-Rosenthal syndrome, and Crohn’s disease: dramatic response to infliximab therapy. Int J Dermatol. 2012;51(8):966–968. doi:10.1111/ijd.2012.51.issue-8
34. de Moll EH, Lebwohl MG. Melkersson-Rosenthal syndrome successfully treated with adalimumab. Cutis. 2018;101(2):122–124.
35. Elliott T, Campbell H, Escudier M, et al. Experience with anti‐TNF‐α therapy for orofacial granulomatosis. J Oral Pathol Med. 2011;40(1):14–19. doi:10.1111/jop.2010.40.issue-1
36. Tan Z, Zhang Y, Chen W, Gong W, Zhao J, Xu X. Recurrent facial palsy in Melkersson Rosenthal syndrome: total facial nerve decompression is effective to prevent further recurrence. Am J Otolaryngol. 2015;36(3):334–337. doi:10.1016/j.amjoto.2014.12.001
37. Yetiser S, Satar B, Kazkayasi M. Immunologic abnormalities and surgical experiences in recurrent facial nerve paralysis. Otol Neurotol. 2002;23(5):
38. Innocenti A, Innocenti M, Taverna C, et al. Miescher’s cheilitis: surgical management and long term outcome of an extremely severe case. Int J Surg Case Rep. 2017;31:241–244. doi:10.1016/j.ijscr.2017.01.062
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.