")
Back to Journals » International Journal of Women's Health » Volume 15
Management of Wrong Blood Transfusion to an RhD Negative Woman in Labor
Authors Titze TL, Hamnvik LHD , Hauglum IM, Carlsen AET, Tjeldhorn L, Nguyen NT, Akkök ÇA
Received 26 September 2022
Accepted for publication 6 December 2022
Published 4 January 2023 Volume 2023:15 Pages 1—6
DOI https://doi.org/10.2147/IJWH.S390661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Thomas Larsen Titze,1 Lars Henrik Dahl Hamnvik,2 Inga Marie Hauglum,1 Anne Elisabeth Tonay Carlsen,2 Lena Tjeldhorn,3 Nhan Trung Nguyen,3 Çiğdem Akalın Akkök3
1Department of Laboratory Medicine, Vestre Viken Health Trust, Drammen, Norway; 2Department of Hematology, Vestre Viken Health Trust, Drammen, Norway; 3Department of Immunology and Transfusion Medicine, Oslo University Hospital, Oslo, Norway
Correspondence: Çiğdem Akalın Akkök, Department of Immunology and Transfusion Medicine, Oslo University Hospital, Ullevaal, Kirkeveien 166, Oslo, N-0407, Norway, Tel +47 92 03 47 47, Fax + 47 22 11 88 50, Email [email protected]
Abstract: Blood transfusion is life-saving in massive hemorrhage. Before pre-transfusion tests with ABO and RhD typing results are available, O RhD negative packed red blood cell (PRBC) units are used without cross-matching in emergency. RhD negative girls and women of child-bearing age should always receive RhD negative blood transfusions to prevent RhD-alloimmunization because anti-D-related hemolytic disease of fetus and newborn (HDFN) can result in mild to severe anemia, and in a worst-case scenario death of an RhD positive fetus and/or newborn. However, “wrong blood to wrong patient” happens unintentionally. Here we report an emergency blood transfusion with one unit of RhD positive PRBCs to an RhD negative young woman when estimated blood loss was 2500 mL during delivery and surgical removal of retained placenta. Realizing the mistake, management with high dose anti-D immunoglobulin (Ig) was initiated to remove the RhD positive red blood cells (RBCs) from the patient’s circulation. Such mitigation is recommended only for girls and women of child-bearing age. Follow-up was performed by flow cytometry until RhD positive RBCs were no longer detected. Ten months after the delivery, antibody screening was negative. However, we still do not know whether we managed to prevent RhD-alloimmunization.
Keywords: anti-D antibody, anti-D immunoglobulin, alloimmunization, fetomaternal hemorrhage, pregnancy, Rhesus
Introduction
Alloimmunization to red blood cell (RBC) antigens occurs mostly due to antigen-positive blood transfusion to antigen-negative individuals or pregnancy with an antigen-positive fetus when the pregnant woman herself is antigen-negative. Less frequently, transplantation of allogeneic hematopoietic stem cells and solid organ can induce alloimmunization. RH1 (D antigen = RhD) is the most immunogenic blood group antigen. While almost 30% of the patients make anti-D following transfusion of one unit of packed red blood cells (PRBC),1 D-alloimmunization occurs in 17% of all RhD negative women after two pregnancies with RhD positive babies unless no postnatal anti-D immunoglobulin (Ig) was given.2 Anti-D can cause moderate to severe hemolytic disease of fetus and newborn (HDFN) and is the most common antibody in pregnancy despite several measures to prevent immunization. Untreated severe anemia in HDFN may, in a worst-case scenario, lead to fetal death. In Norway, as in many other countries, ABO and RhD match is a prerequisite in blood transfusion. Additionally, K negative blood is given to K negative girls and women of childbearing age. However, unintentional RhD positive blood transfusion to RhD negative girls and women of childbearing age happens and mitigation to prevent D-alloimmunization is recommended when the mistake is realized in time.
We present a case and the management of an RhD negative woman who inadvertently received one unit of RhD positive PRBC.
Case Presentation
A 29-year-old blood group A RhD negative female with G2P1 and negative antibody screen received routine antenatal anti-D Ig at gestational week (GW) 28 when fetal RHD genotyping predicted an RhD positive fetus. Following vaginal delivery at GW40+4 her retained placenta required surgical removal. Estimated blood loss was 700 mL before and 1800 mL during the procedure. She received emergency transfusions with two units of blood group O PRBCs and two units of fresh-frozen plasma (Octaplasma®, Octapharma AG, Lachen, Switzerland). Antibody screening was not performed. As the newborn was RhD positive, the mother was given a standard dose of 1500 IU of anti-D Ig approximately 36 hours post-partum. Almost 24 hours after the transfusions, the local blood bank realized that one of the PRBC units transfused during the surgery was RhD positive, ie, the woman had received 250 mL of RhD positive mismatched PRBC. Aiming to avoid D-alloimmunization, therapeutic administration of anti-D Ig was initiated 66 hours after birth. Under close monitoring, 10 doses of anti-D Ig, ie, 15,000 IU in total, over a period of 44 hours were given intravenously. The dose was calculated based on the recommendations from World Health Organization and the manufacturer that 100 IU anti-D Ig neutralizes 1 mL PRBCs: 250 mL PRBCs × 100 IU = 25,000 IU.5 However, the manufacturer suggests a maximum dose of 15,000 IU due to possible risk of hemolysis. We therefore reduced the dose accordingly. The treatment was uncomplicated with adequate urine production and no sign of kidney impairment. She had a slight increase in reticulocyte count from 66 to 102 × 109/L (range: 30–95 × 109/L). Except for a mild increase in lactate dehydrogenase to a maximum of 321 U/L (reference range: 105–205 U/L) five hours after the last dose of anti-D Ig, other biochemical parameters of hemolysis (hemoglobin, haptoglobin, bilirubin), in addition to creatinine and electrolytes were normal. Hemoglobin was stable around 10 g/dL (range: 11.3–15.3 g/dL) during the whole period.
Flow cytometry was utilized to monitor the amount of RhD positive RBCs in the woman’s blood circulation (Figure 1A–D). Blood samples in EDTA tubes were collected once per day four consecutive days from the start of therapeutic administration of high dose anti-D Ig and analyzed the day after they were collected. Flow cytometric follow-up was finalized when no RhD positive RBCs were detected 4 days after initiation of anti-D Ig. The patient was discharged from the hospital in a good condition. Antibody screens after 26 and 41 weeks were negative using the standard indirect antiglobulin technique (IAT) at 37°C, but the first sample was weakly positive by enzyme technique showing an anti-D pattern. In the latter sample, screening was negative also by enzyme technique.
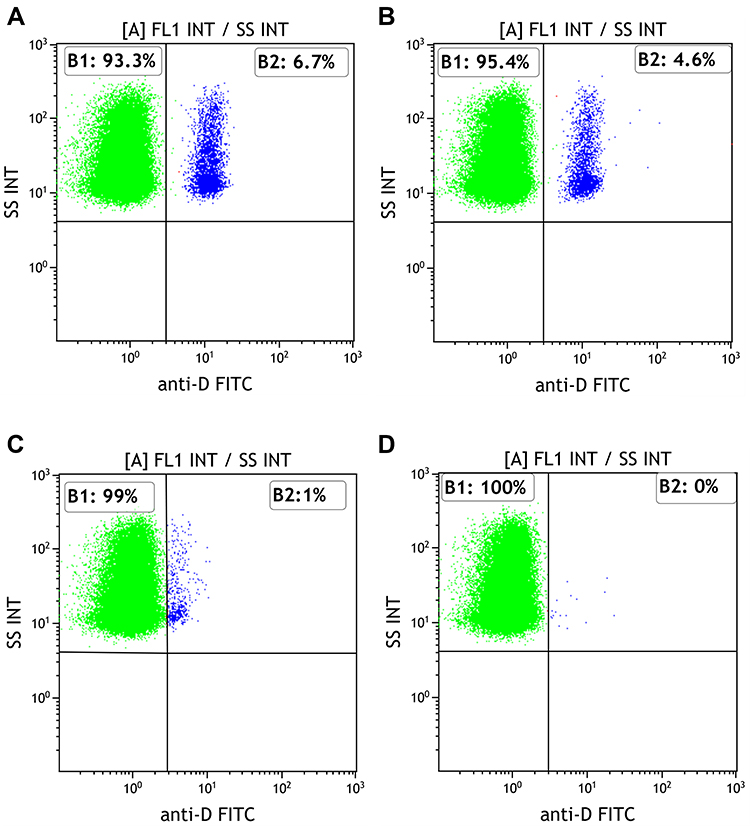 |
Figure 1 Fluorescence histograms of the patient’s red blood cells (RBCs) which were incubated with FITC-conjugated monoclonal anti-D. Blood samples were collected once per day over four consecutive days and analyzed the day after they were collected. The first dose of anti-D Ig was administered approximately 66 hours after the transfusion of RhD positive PRBC unit. The following 9 doses were given intravenously at 68, 71, 76, 84, 88, 92, 98, 105 and 110 hours over a period of 44 hours. (A) The first blood sample before administration of the first dose of therapeutic high dose anti-D immunoglobulin showed 6.7% RhD positive RBCs inadvertently transfused. (B) The second sample showed 4.6% RhD positive RBCs. (C) The third sample showed 1.0% RhD positive RBCs. (D) The fourth sample showed 0% RhD positive RBCs. |
Materials and Methods
Flow Cytometric Analyses
RBCs were washed twice in phosphate-buffered saline (PBS, Product Code P4417, Sigma, USA). Two and a half µL of FITC-conjugated monoclonal anti-D antibody (Clone BRAD 3, Product Code 9433FI, Human IgG3, IBGRL, UK) were added to approximately 5,000,000 RBCs and incubated for 30 minutes at 37°C in the dark. Finally, RBCs were resuspended in 1 mL of PBS and analyzed with flow cytometer (Navios EX, Beckman Coulter, USA) using the sheath fluid recommended by the manufacturer. Fifty thousand events were collected, and log fluorescence data were shown on forward scatter versus side scatter dot plot. The analysis gate was set to include the viable RBC population (typically at least 99% of all cells) based on the forward light scatter properties of the RBCs that correspond to cell size, excluding aggregated cells. Control RBCs of a random RhD negative donor and unlabeled RBCs from the patient were included in each run. The signal from the FITC-conjugated antibody was detected. Results are shown in Figure 1.
Discussion
An RhD negative woman received transfusion of one unit of RhD positive PRBCs accidentally. Realizing the mistake, management with anti-D Ig in therapeutic doses to avoid D-alloimmunization was initiated after the woman’s clinical condition, including kidney function, was evaluated by the clinician and it was concluded that she could tolerate high dose anti-D Ig and probable adverse effects of hemolysis of the RhD positive RBCs. It is recommended that mitigation with anti-D Ig should be initiated within 72 hours after D-mismatched transfusion.3,6 We started after 66 hours, which is within this limit. The impact of the high dose anti-D Ig, measured by quantitation of residual D positive RBCs, was performed by flow cytometry that is a fast and objective method recommended by British Society for Haematology.3
Mismatched RhD positive blood transfusion to an RhD negative patient who already has alloimmune anti-D will primarily lead to extravascular hemolysis of the transfused RhD positive RBCs as anti-D is mainly IgG subclass, while some also have IgM subclass. Administration of high dose anti-D Ig to remove inadvertently transfused RhD positive blood from the circulation also causes extravascular hemolysis. However, kidney failure, although rare, indicating intravascular hemolysis has previously been reported.4 Therefore, we chose close monitoring of our patient, also regarding intravascular hemolysis, and found only mild findings of extravascular hemolysis.
One unit of PRBCs is approximately 250 mL. There is almost consensus about the adequate dose of anti-D Ig necessary to mitigate RhD-mismatched transfusions. While Ayache et al advocate 20 μg/mL D positive RBCs (or 20 μg/2 mL of whole blood) corresponding to 100 IU per mL D positive RBCs,3 World Health Organization, as well as the manufacturer recommendation to hemolyze one mL PRBC is 100–125 IU anti-D Ig5 (Rhophylac «CSL Behring» -Felleskatalogen and Rhophylac 300 micrograms / 2 mL, solution for injection in pre-filled syringe - Summary of Product Characteristics (SmPC) - (emc) (medicines.org.uk)),6 Our patient received 15,000 IU, which is the maximum recommended dose.
Antibody screening is not performed routinely at admission to the hospital in connection with delivery unless there is risk of bleeding; our patient was not screened accordingly. We interpreted the weak anti-D pattern shown by enzyme technique 26 weeks after delivery as the remnants of prophylaxis that then faded in the next sample after 41 weeks. Enzyme technique is a more sensitive method, but antibodies detected by this technique are generally clinically insignificant.7 Despite negative antibody screen of the latter sample, we cannot exclude that primary anti-D immunization may have occurred. Antibody under the detectable level by the standard IAT can be boosted (secondary immune response) by fetomaternal hemorrhage and become detectable in a subsequent pregnancy with an RhD positive fetus. Thus, we still do not know if we succeeded in preventing anti-D development, as antibody screening early in a subsequent pregnancy with an RhD positive fetus will reveal the ultimate outcome. In a subsequent pregnancy, she will then be offered the routine follow-up as for all RhD negative pregnant women.8
When more than one unit of mismatched RhD positive blood is transfused, red cell exchange transfusion (RCEX) may efficiently reduce the amount of RhD positive RBCs.3,9,10 Consequently, the anti-D Ig dose to remove RhD positive blood from the patient’s blood circulation will be lower. Howbeit, whether RCEX, being an invasive procedure with probable adverse effects, is necessary when one unit or less is transfused is debatable.
Anti-D production was induced in 93% of RhD negative male volunteers by a single unit of 200 mL RhD positive frozen/thawed RBCs followed by 0.5–1.0 mL six monthly booster doses (n = 28).11 Pollack et al reported 81.8% D-alloimmunization when they transfused healthy volunteers (n = 43) with 500 mL RhD positive whole blood.12 However, alloimmunization frequency is dramatically different between healthy individuals and patients.13–17 Development of anti-D is reported to be 5% at the lowest (1 of 18 patients)18 but also as high as 50%19 in patients who received RhD positive blood transfusion. The reason for this discrepancy is unknown, but differences in immune responses between healthy individuals and patients, as well as mainly younger age of the volunteers compared to immunocompromised patients either due to disease, treatment, or trauma (trauma-induced immunosuppression), together with sample size differences and the length of observation time may have implications for the immunization rates. Studies on healthy individuals are usually prospective with few/no dropouts, while a significant amount of follow-up antibody screens may be missing due to mainly retrospective design of patient studies. Antibody evanescence may also play a role causing falsely lower alloimmunization rates if a systematic follow-up after RhD positive blood transfusion cannot be carried out.20 Seheult et al, by using a prediction model, simulated the overall risk of HDFN in future pregnancies of RhD negative women of child-bearing age following transfusion with RhD positive RBCs in trauma setting. The authors found that the predicted risk of HDFN was 3.4% if the woman was 18-years old at the time of the transfusion, while the risk was predicted to be approximately 0% at age 43 or older.21 On the other hand, even though pregnancy-induced anti-D immunization is studied thoroughly, to our knowledge, there are no studies on anti-D immunization due to perinatal mismatched blood transfusion.
In Norway, the frequency of RhD negativity is 15% and approximately 6% of the population is O RhD negative.22 Despite being a very limited source, O RhD negative PRBCs are used not only for O RhD negative patients but also in emergency until a patient’s blood group is determined.23,24 RhD positive PRBCs, on the other hand, can be transfused to RhD negative women older than 50 years and to men, especially when the stock of RhD negative units is critically low.9,13,23,24 Some blood banks only allocate O RhD negative PRBCs for emergency use, while others have both O RhD negative and O RhD positive, aiming to transfuse O RhD positive units to females older than 50 years and male patients.9,13 Alloimmunization of these patients is a calculated risk with a sole consequence in transfusion setting, ie, patients with anti-D can only receive RhD negative PRBCs in future transfusions. This strategy does not jeopardize RhD positive fetuses and newborns due to hemolytic disease, as RhD negative women of childbearing age always receive transfusion with RhD-matched PRBCs. However, allocation of RhD positive units in emergency use may cause unintentional transfusion of RhD positive units to RhD negative women of childbearing age due to clerical errors, which was the case in this report, when RhD positive PRBCs were issued to a young RhD negative woman in labor. Before this incident, RhD positive and RhD negative PRBCs were kept in the same refrigerator, yet in different boxes. We now have two separate blood bank refrigerators with more clearly printed labels for each blood group.
Conclusion
High dose anti-D Ig (15,000 IU) to prevent RhD alloimmunization in a woman who received an RhD incompatible blood transfusion unintentionally was tolerated well, without any serious complications. Although anti-D was not detected after 10 months following the incompatible transfusion, its formation cannot be entirely excluded.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the data protection officer for research at Vestre Viken Health Trust, Drammen, Norway.
Informed Consent Statement
Written informed consent from the patient for the publication of this case report with details was obtained.
Acknowledgment
The authors are grateful to the patient who consented to the submission of this report.
Funding
The work has not received any funding or financial support from any commercial organization.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Frohn C, Dümbgen L, Brand J-M, Görg S, Luhm J, Kirchner H. Probability of anti-D development in D- patients receiving D+ RBCs. Transfusion. 2003;43(7):893–898. doi:10.1046/j.1537-2995.2003.00394.x
2. Klein HG. Mollison’s Blood Transfusion in Clinical Medicine.
3. Qureshi H, Massey E, Kirwan D, et al. BCSH guideline for the use of anti-D immunoglobulin for the prevention of haemolytic disease of the fetus and newborn. Transfus Med. 2014;24(1):8–20. doi:10.1111/tme.12091
4. Karp JK, Ness PM. Acute renal failure with hemolysis in a D-mismatched transfusion recipient treated with RhIG. Transfusion. 2009;49(6):1269. doi:10.1111/j.1537-2995.2008.02088.x
5. Organization WSG on the P of RS& WH. Prevention of Rh Sensitization. World Health Organization; 1971.
6. Ayache S, Herman JH. Prevention of D sensitization after mismatched transfusion of blood components: toward optimal use of RhIG. Transfusion. 2008;48(9):1990–1999. doi:10.1111/j.1537-2995.2008.01800.x
7. Enko D, Habres C, Wallner F, Mayr B, Halwachs-Baumann G. Frequencies and specificities of “enzyme-only” detected erythrocyte alloantibodies in patients hospitalized in Austria: is an enzyme test required for routine red blood cell antibody screening? J Blood Transfus. 2014;2014:532919. doi:10.1155/2014/532919
8. Sørensen K, Baevre MS, Tomter G, et al. The Norwegian experience with nationwide implementation of fetal RHD genotyping and targeted routine antenatal anti-D prophylaxis. Transfus Med. 2021;31(5):314–321. doi:10.1111/tme.12772
9. Werch JB. Prevention of Rh sensitization in the context of trauma: two case reports. J Clin Apher. 2010;25(2):70–73. doi:10.1002/jca.20225
10. Nester TA, Rumsey DM, Howell CC, et al. Prevention of immunization to D+ red blood cells with red blood cell exchange and intravenous Rh immune globulin. Transfusion. 2004;44(12):1720–1723. doi:10.1111/j.0041-1132.2004.04161.x
11. Urbaniak SJ, Robertson AE. A successful program of immunizing Rh-negative male volunteers for anti-D production using frozen/thawed blood. Transfusion. 1981;21(1):64–69. doi:10.1046/j.1537-2995.1981.21181127486.x
12. Pollack W, Ascari WQ, Crispen JF, O’Connor RR, Ho TY. Studies on Rh prophylaxis. II. Rh immune prophylaxis after transfusion with Rh-positive blood. Transfusion. 1971;11(6):340–344. doi:10.1111/j.1537-2995.1971.tb04425.x
13. Raval JS, Madden KM, Neal MD, Moore SA. Anti-D alloimmunization in Rh(D) negative adults with severe traumatic injury. Transfusion. 2021;61(Suppl 1):S144–S149. doi:10.1111/trf.16493
14. Williams LA, Sikora J, Aldrees R, Pham HP, Marques MB. Anti-Rh alloimmunization after trauma resuscitation. Transfus Apher Sci. 2019;58(6):102652. doi:10.1016/j.transci.2019.09.005
15. Tchakarov A, Hobbs RBY. Transfusion of D+ red blood cells to D- individuals in trauma situations. Immunohematology. 2014;30(4):149–152. doi:10.21307/immunohematology-2019-110
16. Gonzalez-Porras JR, Graciani IF, Perez-Simon JA, et al. Prospective evaluation of a transfusion policy of D+ red blood cells into D- patients. Transfusion. 2008;48(7):1318–1324. doi:10.1111/j.1537-2995.2008.01700.x
17. Yazer MH, Triulzi DJ. Detection of anti-D in D- recipients transfused with D+ red blood cells. Transfusion. 2007;47(12):2197–2201. doi:10.1111/j.1537-2995.2007.01446.x
18. Meyer E, Uhl L. A case for stocking O D+ red blood cells in emergency room trauma bays. Transfusion. 2015;55(4):791–795. doi:10.1111/trf.12925
19. Flommersfeld S, Mand C, Kühne CA, Bein G, Ruchholtz S, Sachs UJ. Unmatched type O RhD+ red blood cells in multiple injured patients. Transfus Med Hemother. 2018;45(3):158–161. doi:10.1159/000485388
20. Stack G, Tormey CA. Detection rate of blood group alloimmunization based on real-world testing practices and kinetics of antibody induction and evanescence. Transfusion. 2016;56(11):2662–2667. doi:10.1111/trf.13704
21. Seheult JN, Stram MN, Pearce T, et al. The risk to future pregnancies of transfusing Rh(D)-negative females of childbearing potential with Rh(D)-positive red blood cells during trauma resuscitation is dependent on their age at transfusion. Vox Sang. 2021;116(7):831–840. doi:10.1111/vox.13065
22. HE Heier Immunologi Og Transfusjonsmedisin [Immunology and Transfusion Medicine]. Oslo: Universitetsforlag; 1995. Available from: https://urn.nb.no/URN:NBN:no-nb_digibok_2008031004043.
23. The Norwegian Medical Association TNA for I& TM. Clinical transfusion book; 2017. Available from: https://www.legeforeningen.no/contentassets/91aac334a9904f7abe1ba881fa40792a/tranfusjonshandboken-010217.pdf.
24. National guidelines for transfusion medicine services in Norway; 2017. Available from: https://helsedirektoratet.no/retningslinjer/veileder-for-transfusjonstjenesten-i-norge.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.