")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Management of Venous Thromboembolism in Children: Current Recommendations and Therapeutic Options
Authors Bosch A , Albisetti M
Received 30 April 2020
Accepted for publication 5 July 2020
Published 28 July 2020 Volume 2020:16 Pages 673—679
DOI https://doi.org/10.2147/TCRM.S218622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Alessandra Bosch, Manuela Albisetti
Division of Hematology, University Children’s Hospital, Zurich, Switzerland
Correspondence: Manuela Albisetti
Division of Hematology, University Children’s Hospital, Steinwiesstrasse 75, Zurich CH-8032, Switzerland
Tel +41 44 266 7138
Fax +41 44 266 7171
Email [email protected]
Abstract: Venous thromboembolism has an increasing significance in the pediatric patient population. Due to the lack of well-designed pediatric clinical trials, recommendations for the treatment of venous thromboembolic events in children have low evidence and are mainly extrapolated from adult guidelines. This review summarizes and compares recommendations for the treatment of several venous thromboembolic events in children from CHEST, ASH, and the UK guidelines.
Keywords: thromboembolism, thrombosis, children, treatment, guidelines
Introduction
Thrombosis in pediatric patients has an increasing rate of incidence, especially in hospitalized patients. On the one hand, this is due to increasing complications of care of critically ill children and neonates, and, on the other hand, due to more awareness and sensitive diagnostic tools which identify thrombosis.1
The most substantial risk factor for venous thromboembolism (VTE) in children has been described as central venous access devices (CVAD). However, pediatric VTE not only occurs with congenital heart disease, trauma and surgery, infection (local or systemic), malignancy, prematurity, oral contraceptives, immobilization, in the presence of antiphospholipid antibodies, but also with inherited thrombophilia.2–5
Treatment of VTE in the pediatric setting is in most cases not evidence based, as well-designed clinical trials in pediatric populations and studies on anticoagulants have not been performed extensively. For this reason, treatment guidelines are mainly extrapolated from adult studies. However, the pathophysiology of VTE, the hemostatic system, and the underlying medical conditions of children are substantially different from those of adults.6 This means also that complications from anticoagulation treatments such as bleeding risks may differ from adult patients.
The current standard of care for the treatment of VTE in children includes low molecular weight heparin (LMWH), unfractionated heparin (UFH), and vitamin K antagonists (VKA). Depending on the center of care and the available expertise and experience, local, systemic thrombolysis and/or physical thrombectomy may be available and performed.7–9
In this review, we summarize and compare recommendations for the treatment of several VTE manifestations in children from the CHEST, ASH, and UK guidelines.7–9 The new direct oral anticoagulants (DOACs) are not considered in this review, as these are not yet considered a standard of care in the pediatric patient population.
Current Recommendations and Therapeutic Options
The CHEST, ASH, and UK guidelines base their recommendations on the GRADE system. UK and CHEST classify their strong recommendations as “1” and their conditional recommendations or suggestions as “2,” while ASH classifies these as “strong recommendation” and as “conditional recommendation,” respectively. Strong recommendations are based on desirable effects of a treatment that outweigh the harms and costs, whereas conditional recommendations are made, if only low-quality evidence is available, and the benefits are uncertain, or the harm of treatment outweighs the desirable effects.6–8,10
CHEST and UK guidelines further grade the quality of evidence as A (high quality: based on randomized clinical trials; further research results will be unlikely to change the actual standard), moderate B (further research outputs may change the current standards), and low C (further research outputs will very likely change the current standards). ASH grades the quality of evidence from low to high. To maintain manageable reading, we will refer to ASH’s strong as “1” and conditional recommendation as “2,” and the quality of evidence from high to low as “A to C,” respectively.6–8,10
An overview of the recommendations on the management of venous thromboembolism in children is given in Table 1, whereas the therapeutic options are summarized in Table 2.
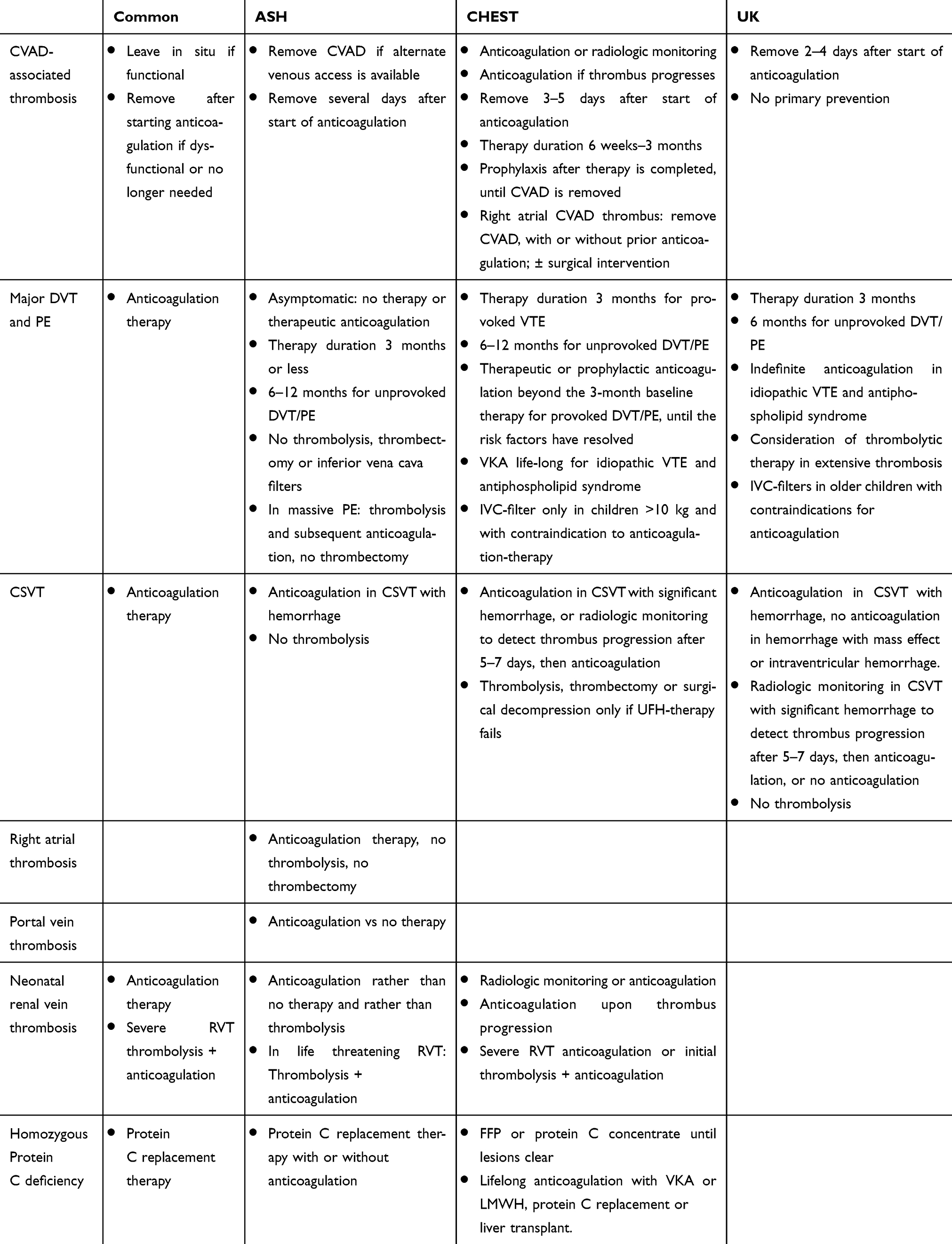 |
Table 1 Comparison of Guideline Recommendations on the Management of Venous Thromboembolism in Children |
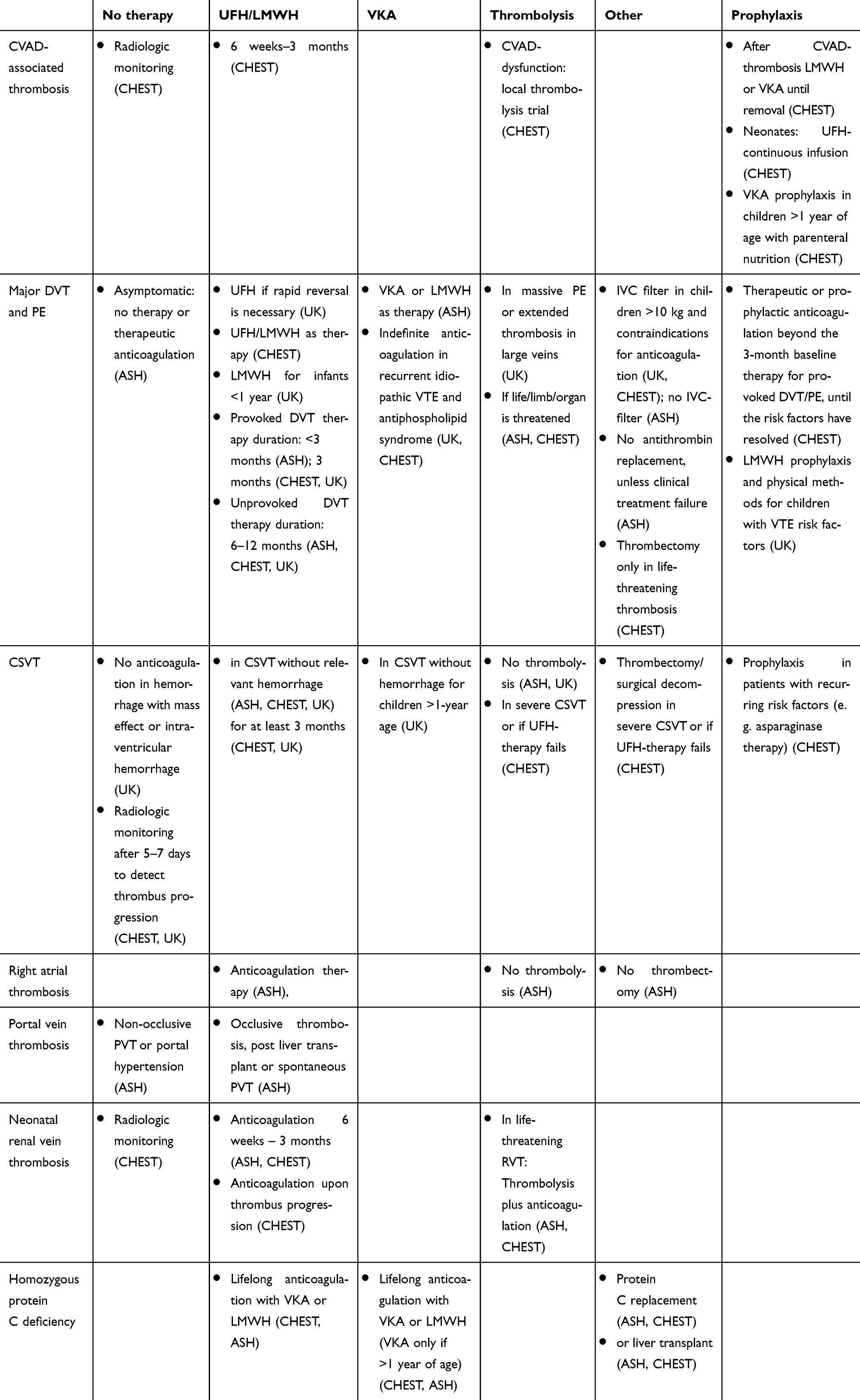 |
Table 2 Therapeutic Options on Specific Pediatric Venous Thromboembolic Events |
CVAD-Associated Thrombosis
Due to limited venous access conditions, pediatric patients often rely on CVAD. If a symptomatic thrombosis occurs, the patient requires CVAD and the device is functional, ASH suggests leaving the CVAD in situ (2C), in line with CHEST which suggests either initial anticoagulation therapy or radiologic monitoring after diagnosis of a CVAD-thrombosis (2C), and if the thrombus progresses, anticoagulation is suggested (2C). In the case of anticoagulation, the CHEST guideline suggests the administration of LMWH or UFH for a total duration of 6 weeks to 3 months (2C). CVAD-related superficial vein thrombosis should be treated if the CVAD is functioning and further required, and/or in patients with worsening symptoms (ASH 2C).
If the symptoms progress under anticoagulation therapy, the CVAD is further required by the patient and is still functioning, ASH suggests either removal or no removal (2C). If alternative venous access is available, the CVAD should be removed. If no alternative is accessible, the CVAD should stay in situ with the risk of infection and thrombus progression.
Should a CVAD remain in situ after therapy completion, prophylactic anticoagulation with VKA or LMWH is suggested by CHEST until CVAD removal (2C). Should the thrombosis recur during prophylactic therapy, CHEST suggests further therapeutic anticoagulation until the CVAD is removed or for a minimum of 3 months (2C). CHEST suggests against thrombolytic therapies, unless a limb, organ, or life is threatened by the thrombus (2C).
If the CVAD does not function, or is no longer needed by the patient, ASH and CHEST recommend removing the CVAD (ASH 1C, CHEST 1B). However, the removal should be delayed if the dysfunction is related to a thrombus, due to the risk of thrombus embolization. After several days of initiation of an anticoagulation therapy the device should be removed (ASH 2C). The UK guideline suggests the removal after 2–4 days (2C), while CHEST suggests the removal 3–5 days after the start with therapeutic anticoagulation (2C).
For a right-atrial CVAD-related thrombus, CHEST suggests the removal of the CVAD with or without previous anticoagulation (2C), and depending on the size and the patient risks a surgical intervention (2C).
Primary prevention of CVAD-related thrombosis is not suggested by the UK guideline (2B), whereas it suggests the consideration of the use of heparin-bonded CVADs for short-term use (2C). CHEST also recommends against thrombo-prophylaxis for children with short-term CVADs (1B). CHEST suggests regular CVAD-flushing with saline or heparin or intermittent recombinant urokinase (2C). For blocked CVADs, CHEST recommends one or two recombinant urokinase or tissue plasminogen activator trials to restore the patency (2C). If CVAD is further dysfunctional, radiologic imaging is advised to rule out CVAD-related thrombosis (2C).
In neonates, CHEST recommends an UFH-continuous infusion to maintain CVAD function (1A), and for CVAD-dysfunction in neonates, local thrombolysis with tissue plasminogen activator is suggested (2C).
CHEST further suggests VKA thromboprophylaxis in children over 1 year of age receiving parenteral nutrition via a CVAD (2C).
Major Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
In asymptomatic DVT and PE, ASH suggests either therapeutic anticoagulation or no therapy (2C).
ASH and CHEST recommend therapeutic anticoagulation in patients with symptomatic DVT or PE (ASH 1C; CHEST 1B). The therapy for symptomatic DVT and PE should consist of UFH or LMWH for at least 5 days according to the CHEST recommendations (1B). UFH can be administered initially if a rapid reversal of anticoagulation is necessary (UK 2C). Afterward, LMWH or UFH are recommended by CHEST, whereas ASH suggests LMWH or oral VKAs (2C). UK suggests LMWH as the therapy of choice in infants under the age of 1 year (2C). ASH advises against antithrombin (AT) replacement in addition to standard anticoagulation. Anticoagulation alone should be used in patients with DVT, PE (2C). However, if therapy failure occurs clinically during standard anticoagulation alone and AT levels are low, AT replacement is suggested (2C).
For UFH a therapeutic range is defined as an anti-Xa activity of 0.35–0.7 U/mL (CHEST 2C), and CHEST suggests avoiding long-term use of UFH in children (2C). For LMWH the therapeutic range is defined as an anti-Xa activity of 0.5–1.0 U/mL 4–6 hours after s.c. injection (CHEST 2C). For oral VKA-therapy, a start as early as day 1 is recommended, with the continuation of LMWH/UFH until at least day 6, or later if the INR does not exceed 2.0 on day 6 (1B CHEST). ASH suggests either LMWH or VKA as the standard DVT/PE anticoagulation therapy aiming at a goal-INR of 2.5 (ASH 2, UK 1B). According to CHEST, the therapeutic range for VKA is best monitored via the INR in a range of 2.0–3.0 (2C).
A therapy duration of 3 months or less (ASH 2C) or 3 months according to CHEST for provoked DVT seems sufficient (2C), while unprovoked DVT or PE should be treated for 6–12 months (ASH 2C and CHEST 2C), whereas the UK recommends 3 months and 6 months, respectively (1C). For VTE occurring in the presence of thrombophilic risk factors (e.g. nephrotic syndrome/asparaginase therapy), the intensity and duration of therapy should be the same as in the absence of these. According to the CHEST suggestion, in children with VTE or recurrent VTE and ongoing risk factors for thrombotic events, either therapeutic or prophylactic anticoagulation is suggested beyond the 3-month baseline therapy, until the risk factors have resolved (2C). In recurrent unprovoked VTE and pediatric patients with antiphospholipid syndrome, indefinite anticoagulation is recommended (UK 1C). CHEST recommends a life-long VKA treatment (1A).
ASH discourages the use of thrombolysis, thrombectomy, or inferior vena cava filters in children with DVT and/or PE, and rather recommends anticoagulation alone (2C). On the other hand, in massive PE, i.e., patients with hemodynamic compromise, thrombolysis and subsequent anticoagulation are suggested, while thrombectomy is discouraged in the ASH guidelines (2C). The UK guidelines recommend consideration of thrombolytic therapy in extensive thrombosis in pelvic veins, superior and inferior vena cava (SVC and IVC) and in intracardiac sites, as well as in massive PE (1C). In older children with contraindications for systemic anticoagulation and DVT in lower limbs, removable IVC filters should be considered (1C). This is in line with CHEST, which suggests an IVC-filter only in children >10 kg and with contraindication to anticoagulation therapy (2C). ASH suggests against IVC-filters, and rather anticoagulation alone should be considered as a treatment for symptomatic DVT (2C). CHEST and ASH agree that thrombolysis should only be performed if the life, organ, or limb of a patient is threatened (CHEST 2C, ASH 2). UK suggests thrombolytic therapy to be considered if extensive thrombosis occurs in the IVC, SVC, pelvic veins, intracardial, or with massive PE (1C). Further, CHEST suggests that thrombectomy be only performed in life-threatening thrombosis, followed by standard anticoagulation therapy (2C).
Children and adolescents with numerous VTE risk factors should be considered for LMWH-prophylaxis (UK 2C). The UK advises against aspirin in VTE-prophylaxis (2C). The UK guidelines also recommend physical methods to reduce VTE risk in older children and adolescents who are at risk (1C). Especially in children with a high risk and under anticoagulation-prophylaxis, physical methods can complement the prevention (2C).
Central Sino Venous Thrombosis (CSVT)
ASH recommends anticoagulation therapy in CSVT without hemorrhage (1C), in line with the CHEST and UK guidelines, which specify the therapeutic approach with LMWH or UFH (1B). UK recommends VKA therapy with INR goal 2.5 in children >1 year old (1C) and suggests LMWH therapy in children <1 year (2C). This is in line with the CHEST neonatal recommendation.
Further, ASH suggests anticoagulation therapy in CSVT with hemorrhage (2C), while the UK guidelines distinguish CSVT hemorrhage with and without mass effect or intraventricular hemorrhage. UK discourages anticoagulation in CSVT with relevant hemorrhage and rather suggests radiologic monitoring. Further, UK suggests treatment in less significant hemorrhage and infarction (2C). CHEST suggests anticoagulation in CSVT with significant hemorrhage, or radiologic monitoring to detect thrombus progression after 5–7 days. If thrombus progression occurs, anticoagulation is suggested (2C). ASH and UK advise against thrombolysis (ASH 2C; UK 1C). CHEST suggests thrombolysis, thrombectomy, or surgical decompression only if UFH-therapy fails to improve the clinical presentation or in severe CSVT (2C).
CHEST suggests a treatment duration of at least 3 months. The UK guidelines further suggest a therapy duration of 3 months in CSVT with an identifiable risk factor (e.g. infection) (1C); 6 months without risk factor (1C) or longer if the risk factor is ongoing (e.g. asparaginase therapy), recurrent idiopathic CSVTs occur, or the patient remains symptomatic with venous hypertension (UK 2C). This is in line with CHEST’s recommendation (2C). CHEST also suggests prophylactic anticoagulation in patients with recurring risk factors (asparaginase/nephrotic syndrome) at times of exposure (2C).
In patients with persistent venous-hypertension symptoms, reimaging should be performed before anticoagulation is terminated. Also, reimaging should be considered if neurologic symptoms progress (UK 2C).
Other Thrombotic Events
Right Atrial Thrombosis (Non-CVAD Related)
ASH suggests anticoagulation therapy and advises against thrombolysis or surgical thrombectomy (2C).
Portal Vein Thrombosis (PVT)
ASH recommends anticoagulation with occlusive thrombosis, post liver transplant, or spontaneous PVT, whereas no therapy is suggested in non-occlusive PVT or portal hypertension (2C).
Neonatal Renal Vein Thrombosis (RVT)
For unilateral RVT without organ impairment, the CHEST guideline proposes radiologic monitoring or anticoagulation with UFH or LMWH for 6 weeks to 3 months. Should thrombus progression occur, anticoagulation therapy is suggested (2C). Meanwhile, ASH suggests anticoagulation alone rather than no anticoagulation (2C) and rather than thrombolysis (1C). In the case of RVT with thrombus extension into the IVC, the same anticoagulation therapy is suggested by CHEST (2C). In the case of bilateral RVT with organ dysfunction, LMWH/UFH or initial thrombolysis with tissue plasminogen activator and subsequent LMWH/UFH therapy are suggested by CHEST (2C), in line with ASH, which suggests thrombolysis followed by anticoagulation in neonatal life-threatening RVT (2C).
Homozygous Protein C Deficiency
For neonates presenting with purpura fulminans due to homozygous protein C deficiency, CHEST recommends the administration of FFP 10–20 mL/kg 12-hourly or protein C concentrate 20–60 units/kg until the lesions clear (1A). ASH also suggests a protein C replacement therapy with or without anticoagulation, rather than anticoagulation alone in the neonatal period (2C). After which, lifelong treatment with VKA or LMWH (1C), protein C replacement (1B), or liver transplantation (1C and ASH 2C) is recommended by CHEST.
Structural Venous Anomalies
Secondary VTE due to structural venous anomalies should be treated as first spontaneous VTEs (see above) according to the CHEST guidelines. For recurrent VTEs, indefinite anticoagulation is recommended until the venous anomalies are removed or repaired surgically (2C).
Conclusion
Several recommendations for the treatment of VTE in children have been published in the last decade. Although these recommendations are of low evidence, and in part extrapolated from adult guidelines, they provide an important type of standard of care that helps pediatricians to decide the best consensus treatment approach for VTE in their patients. The CHEST, ASH, and UK guidelines show consistencies in their recommendations and outline how to treat pediatric VTE in a reasonably standardized manner.
Currently, multicenter randomized clinical trials with new direct oral anticoagulants (DOACs) are ongoing. These will not only provide new and potentially advantageous therapeutic options for pediatric VTE, but also deliver scientifically valuable data on the efficacy and safety of new treatment options, and their risks and side effects compared to standard anticoagulants for the treatment and prevention of thrombotic events in children with different clinical conditions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raffini L, Huang YS, Witmer C, Feudtner C. Dramatic increase in venous thromboembolism in children’s hospitals in the United States from 2001 to 2007. Pediatrics. 2009;124(4):1001–1008. doi:10.1542/peds.2009-0768
2. Mahajerin A, Branchford BR, Amankwah EK, et al. Hospital-associated venous thromboembolism in pediatrics: a systematic review and meta-analysis of risk factors and risk-assessment models. Haematologica. 2015;100(8):1045–1050. doi:10.3324/haematol.2015.123455
3. Setty BA, O’Brien SH, Kerlin BA. Pediatric venous thromboembolism in the United States: a tertiary care complication of chronic diseases. Pediatr Blood Cancer. 2012;59(2):258–264. doi:10.1002/pbc.23388
4. Takemoto CM, Sohi S, Desai K, et al. Hospital-associated venous thromboembolism in children: incidence and clinical characteristics. J Pediatr. 2014;164(2):332–338. doi:10.1016/j.jpeds.2013.10.025
5. Revel-Vilk S, Chan A, Bauman M, et al. Prothrombotic conditions in an unselected cohort of children with venous thromboembolic disease. J Thromb Haemost. 2003;1(5):915–921. doi:10.1046/j.1538-7836.2003.00158.x
6. Andrew M, Vegh P, Johnston M, et al. Maturation of the hemostatic system during childhood. Blood. 1992;80(8):1998–2005. doi:10.1182/blood.V80.8.1998.1998
7. Monagle P, Chan AKC, Goldenberg NA, et al. Antithrombotic therapy in neonates and children: antithrombotic therapy and prevention of thrombosis, 9th ed: american college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e737S–e801S. doi:10.1378/chest.11-2308
8. Monagle P, Cuello CA, Augustine C, et al. American society of hematology 2018 guidelines for management of venous thromboembolism: treatment of pediatric venous thromboembolism. Blood Adv. 2018;2(22):3292–3316. doi:10.1182/bloodadvances.2018024786
9. Chalmers E, Ganesen V, Liesner R, et al. Guideline on the investigation, management and prevention of venous thrombosis in children. Br J Haematol. 2011;154(2):196–207. doi:10.1111/j.1365-2141.2010.08543.x
10. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.