")
Back to Journals » Infection and Drug Resistance » Volume 16
Management of Bacterial and Fungal Infections in the ICU: Diagnosis, Treatment, and Prevention Recommendations
Authors Rawson TM, Antcliffe DB, Wilson RC, Abdolrasouli A, Moore LSP
Received 28 February 2023
Accepted for publication 22 April 2023
Published 4 May 2023 Volume 2023:16 Pages 2709—2726
DOI https://doi.org/10.2147/IDR.S390946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Timothy M Rawson,1– 3 David B Antcliffe,2,4 Richard C Wilson,1– 3 Alireza Abdolrasouli,5 Luke SP Moore1,6,7
1Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance, Hammersmith Hospital, London, UK; 2Centre for Antimicrobial Optimisation, Imperial College London, Imperial College London, London, UK; 3David Price Evan’s Group in Infectious Diseases and Global Health, Department of Pharmacology and Therapeutics, University of Liverpool, Liverpool, UK; 4Division Anaesthesia, Pain Medicine and Intensive Care, Department of Surgery and Cancer, Imperial College London, London, UK; 5Department of Medical Microbiology, King’s College Hospital, London, UK; 6Chelsea & Westminster NHS Foundation Trust, London, UK; 7North West London Pathology, Imperial College Healthcare NHS Trust, London, UK
Correspondence: Timothy M Rawson, Health Protection Research Unit in Healthcare Associated Infections & Antimicrobial Resistance, Hammersmith Hospital, Du Cane Road, London, W12 0NN, United Kingdom, Email [email protected]
Abstract: Bacterial and fungal infections are common issues for patients in the intensive care unit (ICU). Large, multinational point prevalence surveys have identified that up to 50% of ICU patients have a diagnosis of bacterial or fungal infection at any one time. Infection in the ICU is associated with its own challenges. Causative organisms often harbour intrinsic and acquired mechanisms of drug-resistance, making empiric and targeted antimicrobial selection challenging. Infection in the ICU is associated with worse clinical outcomes for patients. We review the epidemiology of bacterial and fungal infection in the ICU. We discuss risk factors for acquisition, approaches to diagnosis and management, and common strategies for the prevention of infection.
Keywords: bacterial infection, fungal infection, critical care, diagnostics, therapeutics
Introduction
Bacterial and fungal infections are common diagnoses for patients in the intensive care unit (ICU).1 In 2017, Vincent et al reported a 24-hour point prevalence survey of 1150 centres in 88 countries.2 Of 15,165 patients with infection data available, 8135 (54%) had proven or suspected infection and 10,640 (70%) received at least one antimicrobial agent. Secondary infection acquired in the ICU was observed in 1760/8135 (22%).2 Gram-negative organisms predominated (3540/5259; 67%) in those with clinically significant microbiology and fungal infection accounted for 16% (864/5259) of cases.2 These data were similar to the previous multinational point prevalence studies, such as EPIC II that was performed in 2009 and reported that 51% of patients were considered infected, antibiotics were prescribed for 71% of patients, and Gram-negative infections accounted for 62% and fungal infections 19% of cases.3
Mortality rates in the ICU are higher in patients with bacterial or fungal infection compared to those without infection.2–9 In-hospital mortality for ICU patients with infection is approximately 30%.2 Secondary bacterial or fungal infection and the presence of drug-resistant infections are independent risk factors for mortality with an increased odds of death compared to community-acquired infection (OR: 1.32; 95% CI 1.10–1.60).2
Infections in the ICU are frequently caused by drug-resistant bacteria and increasingly drug-tolerant/resistant fungi.3,7,10 Termed antimicrobial resistance (AMR), these infections already have a significant impact on hospitalised patients.
Globally, rates of AMR will vary between regions.11,12 Gram-negative organisms pose a major challenge including extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriales, derepressed AmpC organisms, carbapenemase-producing Enterobacteriales (CPE), carbapenem-resistant Acinetobacter baumannii (CRAB), and carbapenem-resistant Pseudomonas aeruginosa.12 Gram-positive challenges include methicillin-resistant Staphylococcus aureus (MRSA) and glycopeptide-resistant Enterococcus (GRE) species.12
Antifungal tolerant and resistant fungal infections are an emerging threat,13,14 not least given the high rate of associated mortality in critical care, and the relative inability to rapidly diagnose and deliver effective antimicrobial therapy.13 Among fungal pathogens, the global emergence and spread of multidrug-resistant Candida auris has caused several healthcare-associated outbreaks.15–17 Blood stream infections among non-albicans Candida species with decreased susceptibility to first-line antifungal therapies including azoles and echinocandins have been reported.18 Examples include fluconazole and echinocandin resistance in Nakaseomyces glabrata (formerly Candida glabrata) isolates19 and the recent emergence of fluconazole-resistant Candida parapsilosis. Candida parapsilosis has been demonstrated to persist and cause outbreaks in neonatal and adult ICUs.20–22
Among filamentous fungi, resistance of Aspergillus fumigatus, the most common respiratory fungal pathogen, to triazole antifungal agents is clinically significant. Aspergillus infections caused by azole-resistant strains are seen in both azole-naïve and those who have undergone long-term azole therapy and present a clear challenge in diagnosis and treatment with increased associated mortality.23 The number of infections caused by moulds with intrinsic resistance to one or more class of antifungal agent is increasing with notable examples including Mucorales, Fusarium species, Scedosporium species and Lomentospora prolificans.24
Admission to the ICU is associated with numerous risk factors for the development of nosocomial infection, including ventilator/hospital-acquired pneumonia (VAP/HAP), catheter-associated blood stream infection, surgical site infection, and urinary tract infection (UTI).3 The use of central venous catheters, invasive mechanical ventilation, sedation and paralysis, complex surgical procedures, broad-spectrum antimicrobial use, and patient immune status all increase patient risk of secondary infections.2,8 Patient outcomes are often worse for those who experience secondary bacterial and fungal infection in the ICU3 and place a significant financial burden on healthcare services.1
Recent experience during the COVID-19 pandemic highlighted the challenge of bacterial and fungal infections in patients admitted to ICU.25 Overall, bacterial and fungal co-infection was rare in COVID-19, but in patients admitted to ICU rates were high.26 It is likely that a breakdown in infection prevention and control (IPC) practices, increased use of broad-spectrum antimicrobials, and changes in the hospital environment brought about by COVID-19 have driven observed outbreaks of multidrug-resistant bacterial infections within the ICU environment during this period.25,27,28
Both seasonal influenza29 and the COVID-19 pandemic30 have resulted in larger proportions of the critically ill patients at risk of secondary fungal co-infections. Fungal pathogens that have been observed to cause co-infections in patients with COVID-19 include Aspergillus, Mucorales and Candida species. The epidemiology, clinical and host risk factors, immunological mechanisms, and metabolic responses that underline the pathogenesis of COVID-19 fungal co-infections are complex and reviewed extensively by Hoenigl et al.31
This review will explore the diagnosis, management, and strategies for prevention of bacterial and fungal infection in the ICU. It will review current and future diagnostic and management approaches for patients with suspected bacterial and fungal infections in the ICU. It will consider the evidence-base around prevention of secondary infections.
Challenges in the Diagnosis of Bacterial and Fungal Infection in ICU
The diagnosis of infection in ICU patients can be challenging.32 Organ support may mask traditional diagnostic factors such as features of the systemic inflammatory response syndrome (SIRS) including hypotension or fever and clinical features of specific organ infections.33 Furthermore, SIRS can often be of non-infective origin. Clinical history and examination may be limited, and diagnostics often have a long turnaround time compared to the urgency with which to make a decision regarding therapeutic strategy.32 Whilst prediction tools have been developed to support the early detection of sepsis, they remain limited in their overall performance in many cases.33–35
Current guidelines recommend that diagnosis of sepsis is based on clinical judgement moving away from the reliance on more objective decision support tools.32 Early recognition, investigation, and appropriate management are vital to optimise clinical outcomes when sepsis is suspected.32
Whilst early appropriate antimicrobial therapy is often associated with superior clinical outcomes for patients with severe infection, unnecessarily broad therapy has been associated with increased mortality and complications for individual patients.9 Beyond patients with septic shock, there remains controversy around time-to-antibiotic-based guidelines if appropriate diagnostic steps have not been implemented before commencement of antimicrobial therapy.36
Appropriate investigation and timely initiation of therapy is vital to deliver optimal care. The formulation of syndromic diagnosis and the use of appropriate diagnostics require an understanding of clinical risk factors and diagnostic tools that are available to support different aspects of clinical decision-making.
Risk Factors for Bacterial and Fungal Infection
Table 1 outlines common risk factors associated with bacterial and fungal infection for frequent infective syndromes within the ICU. Risk of infection will vary between organism, site of infection, patient, and local factors.2 Compared to the general hospital population, rates of bacterial and fungal infection are often significantly greater within the ICU.2 Common factors associated with increased risk of infection include intrinsic factors, such as immunosuppression, comorbidities, and critical illness.10 Modifiable risk factors include organ support, such as mechanical ventilation, haemofiltration and total parenteral nutrition (TPN); surgical procedures; and the requirement for prolonged admission to the ICU.10
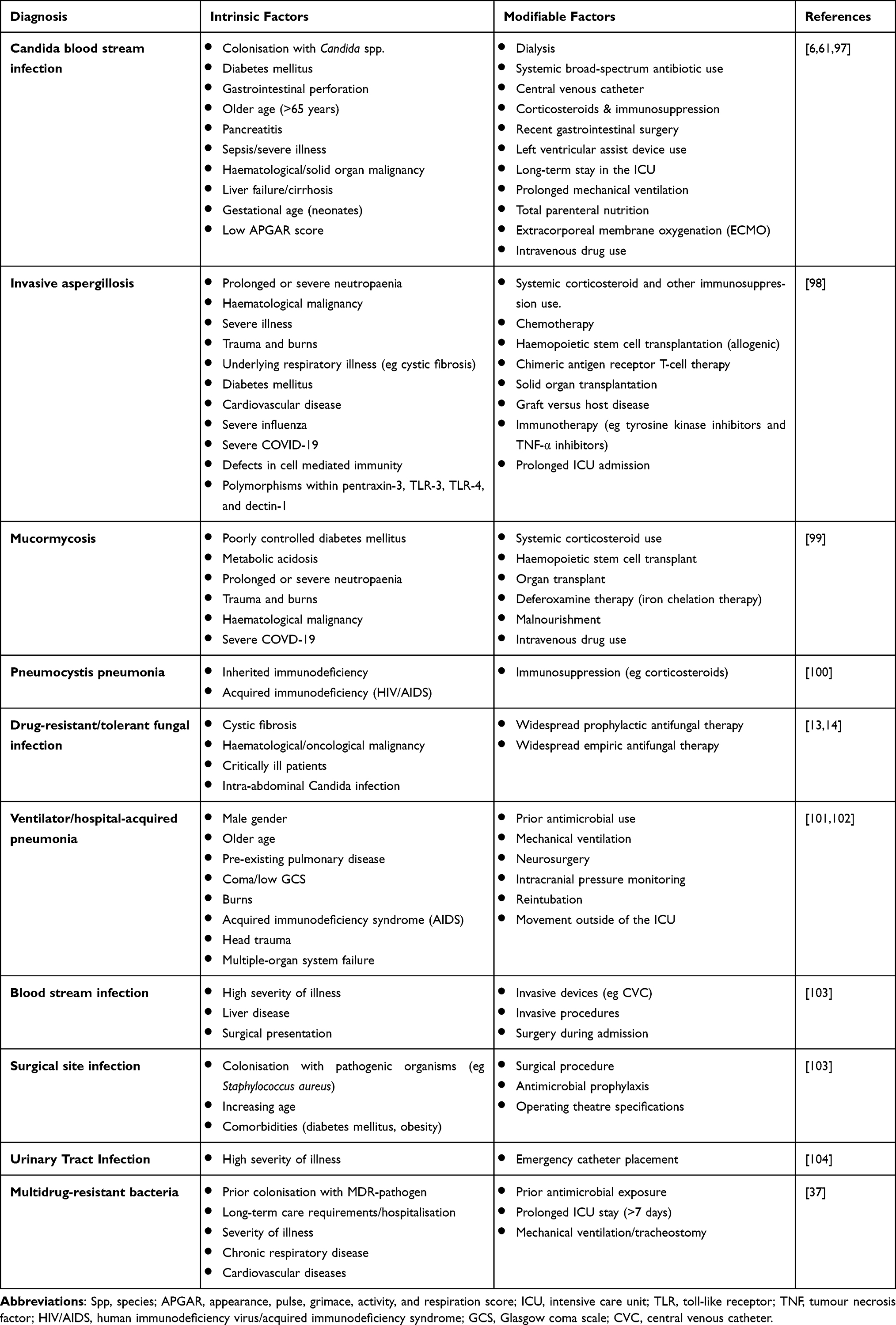 |
Table 1 Risk Factors for the Development of Bacterial and Fungal Infections in the Intensive Care Unit |
Epidemiology of drug-resistant infections will likely vary between geographical regions, but common risk factors should be considered for those at risk of carriage and infection with multidrug-resistant (MDR) organisms. For MDR-bacteria, common risk factors include long-term care facility residence, recent hospital admission, previous broad-spectrum antimicrobial use, known colonisation, and recent travel to high prevalence areas.11,12,37 Antifungal-tolerant and drug-resistant fungal infections are an emerging concern in ICU with risk factors including known colonisation, long-term suppressive or prophylactic antifungal use, and previous exposure to antifungal therapy (eg haematological, cystic fibrosis, prolonged ICU patients).13,14
Traditional Diagnostic Pathways
Traditional laboratory diagnostic pathways for bacterial and fungal infection rely upon culture-based approaches that can be supported by information from the clinical assessment, radiological investigations, and biomarkers. Figure 1 outlines common diagnostics that can support decision-making for bacterial and fungal infections. The figure highlights that diagnostic decision-making is never a single event. The physician must have a baseline understanding of the information provided by specific diagnostic tests and the confidence with which this information can be interpreted. Generally, diagnostics can be used to support commencement, targeting, individualisation, and cessation of antimicrobial therapy. Table 2 summarises the strengths and weaknesses of individual diagnostic modalities at each stage in the decision-making pathway.
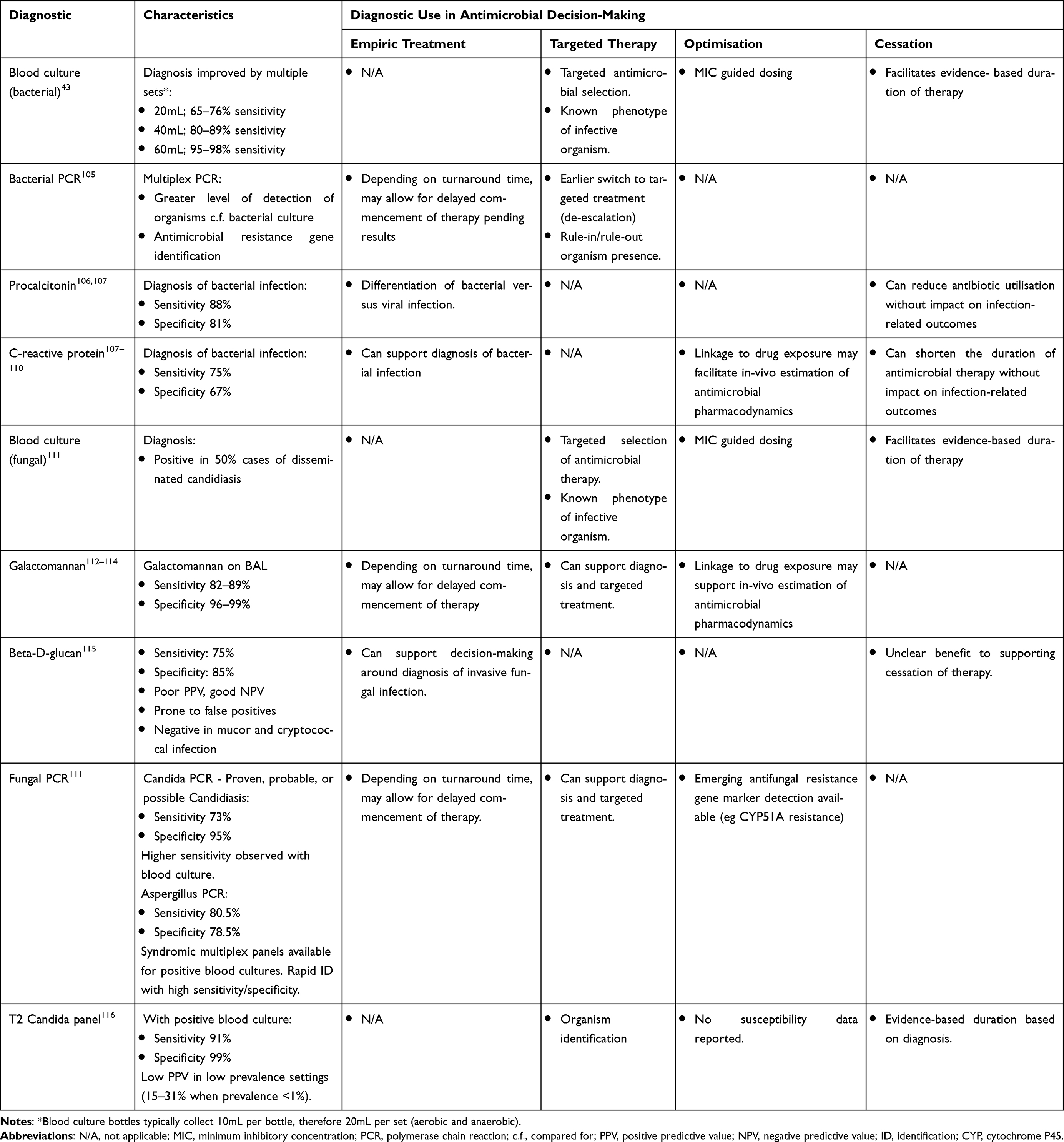 |
Table 2 Common Diagnostics Used to Support Antimicrobial Decision-Making for Bacterial and Fungal Infections |
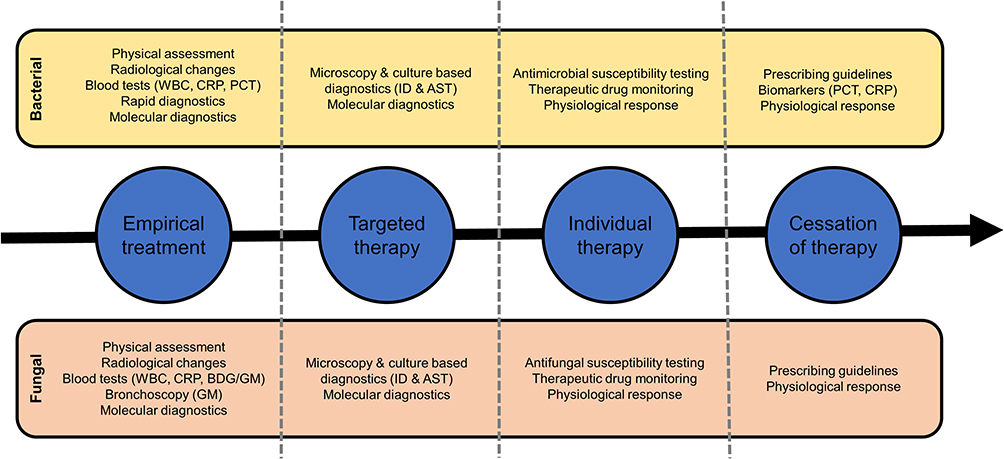 |
Figure 1 Common factors that influence antimicrobial decision-making at different steps in the pathway. Abbreviations: WBC, white blood cell count; CRP, C-reactive protein; PCT, procalcitonin; ID, organism identification; AST, antimicrobial susceptibility testing; BDG, beta-D-glucan; GM, galactomannan. |
It is important to consider the influence that a diagnostic test may have at different stages of decision-making.38 Ensuring the appropriate use of diagnostic investigations helps to ensure that optimal treatment decisions are made by providing reliable and correct information. This concept is a key component of diagnostic stewardship and is important in ensuring that the diagnostic laboratory can optimally support clinical decision-making.39 This in-part relies on the requesting physician having knowledge of a test's sensitivity, specificity, and predictive values to ensure that its result can be appropriately interpreted and applied to the wider decision-making context.40
Advances in Diagnostics
For more than 100 years, microbiological diagnostics have mainly relied upon culture-based approaches to the identification and phenotypic characterisation of microorganisms (Figure 2).41 Culture-based diagnostics provide a phenotypic antimicrobial susceptibility profile that allows the targeted prescription of antimicrobials with a high probability of success based on organism, drug pharmacokinetic/pharmacodynamic (PK/PD), and host factors.42 Traditional culture-based approaches are associated with slow turnaround times, limited sensitivity, and are open to variation between laboratories. This means that often the organism’s identity and antimicrobial susceptibility report will not be available for 48–72 hours after a sample has been collected.41 This leads to delays in the delivery of targeted and individualised therapy and provides a window of inappropriate therapy, whether wrong spectrum or unnecessarily broad.
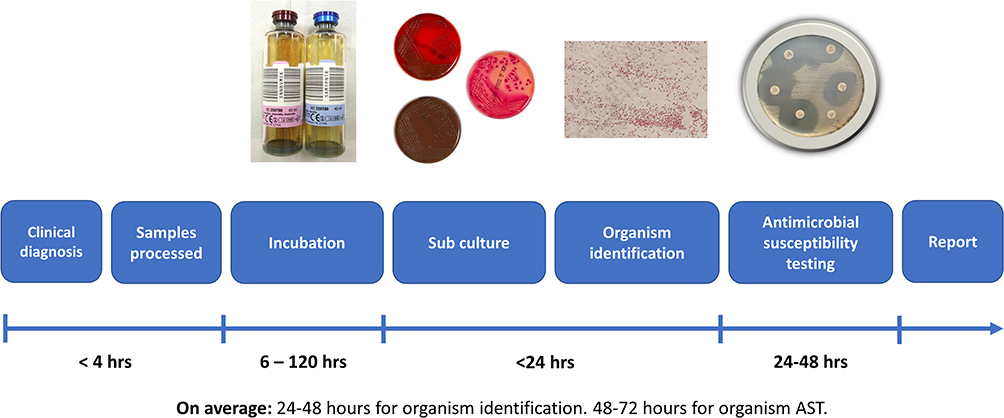 |
Figure 2 Traditional turn around time for culture-based diagnostics for blood cultures. Turn around times referenced in this figure are adpated from from the UK SMI B 37: investigation of blood cultures (for organisms other than Mycobacterium species) 2022 https://www.gov.uk/government/publications/smi-b-37-investigation-of-blood-cultures-for-organisms-other-than-mycobacterium-species. Abbreviation: AST, antimicrobial susceptibility testing. |
Recent technological developments have aimed to reduce the turnaround-time of organism identification and susceptibility reporting. This includes improving the collection and delivery of samples to the microbiology laboratory,43 the development of rapid antimicrobial susceptibility (AST) methodology,44,45 and adoption of new technology for organism identification and AMR detection.46,47
The uptake of Matrix-Assisted Laser Desorption/Ionization – Time of Flight Mass Spectrometry (MALDI-TOF MS) is an example of technology that can facilitate rapid turn-around in organism identification and in certain cases the detection of antimicrobial resistance such as differentiation of methicillin susceptible from methicillin-resistant Staphylococcus aureus.48–51 Turn-around time can be shortened further using MALDI-TOF MS through direct from sample identification protocols, which have demonstrated reasonable levels of sensitivity and specificity and allow quicker time to organism identification and thus targeted antimicrobial therapy.49
The development of molecular diagnostic tools provides an additional diagnostic modality that can support optimal antimicrobial decision-making for infection management in the ICU. Molecular diagnostics aim to bypass the culture-step in the diagnostic pathway facilitating rapid organism detection and identification directly from clinical specimens. Molecular diagnostics can also provide a mechanism for detection of known genotypic antimicrobial resistance.52,53 Near-patient testing allows the deployment of molecular sample-to-answer platforms within the ICU environment and can reduce time to organism identification and targeted antimicrobial therapy by around 24 hours.54 To date, there has been a paucity of clinical trial data to support the application of molecular diagnostics. Where clinical trials have been performed, these have often failed to define appropriate outcome measures based on the likely impact on decision-making of the diagnostics being evaluated.55 One example was a multi-centre randomised control trial of a respiratory multiplex-PCR platform linked to procalcitonin for the diagnosis of bacterial infections in patients admitted to the ICU with COVID-19.56 This trial failed to demonstrate an impact of antibiotic prescribing but did demonstrate the improved sensitivity of such non-culture-based approaches for organism identification in populations with high rates of empiric antimicrobial prescribing prior to microbiological sampling.56 Within this study, bacterial identification using multiplex-PCR was twice as high in the context of most patient (83%) receiving empiric antimicrobial therapy prior to microbiological sampling.56
Rapid AST can be performed for positive blood cultures using standard laboratory approaches or automated systems.44,45,47 In current randomised control trials, these tools have demonstrated improved antimicrobial stewardship targets (both reduced time to effective therapy and reduced inappropriate treatment) but failed to demonstrate improvements in clinical outcomes including mortality.57–59 For example, one study randomised positive blood cultures from patients with Gram-negative bacteraemia to undergo conventional versus rapid AST testing using an automated commercial method with a primary end point of time to narrowest effective therapy.59 Rapid AST did not impact time to narrowest effective therapy but did significantly decrease time to oral antimicrobial switch and shortened length of hospital stay by two days.59
Management of Bacterial and Fungal Infection in the ICU
Initiation of early and appropriate antimicrobial therapy as part of a bundle of interventions is one of the most effective means of improving clinical outcomes for patients with secondary bacterial or fungal infection in the ICU.32 Table 3 summarises the prevalence of common infective syndromes in the ICU and highlights examples of available international guidelines for their management.
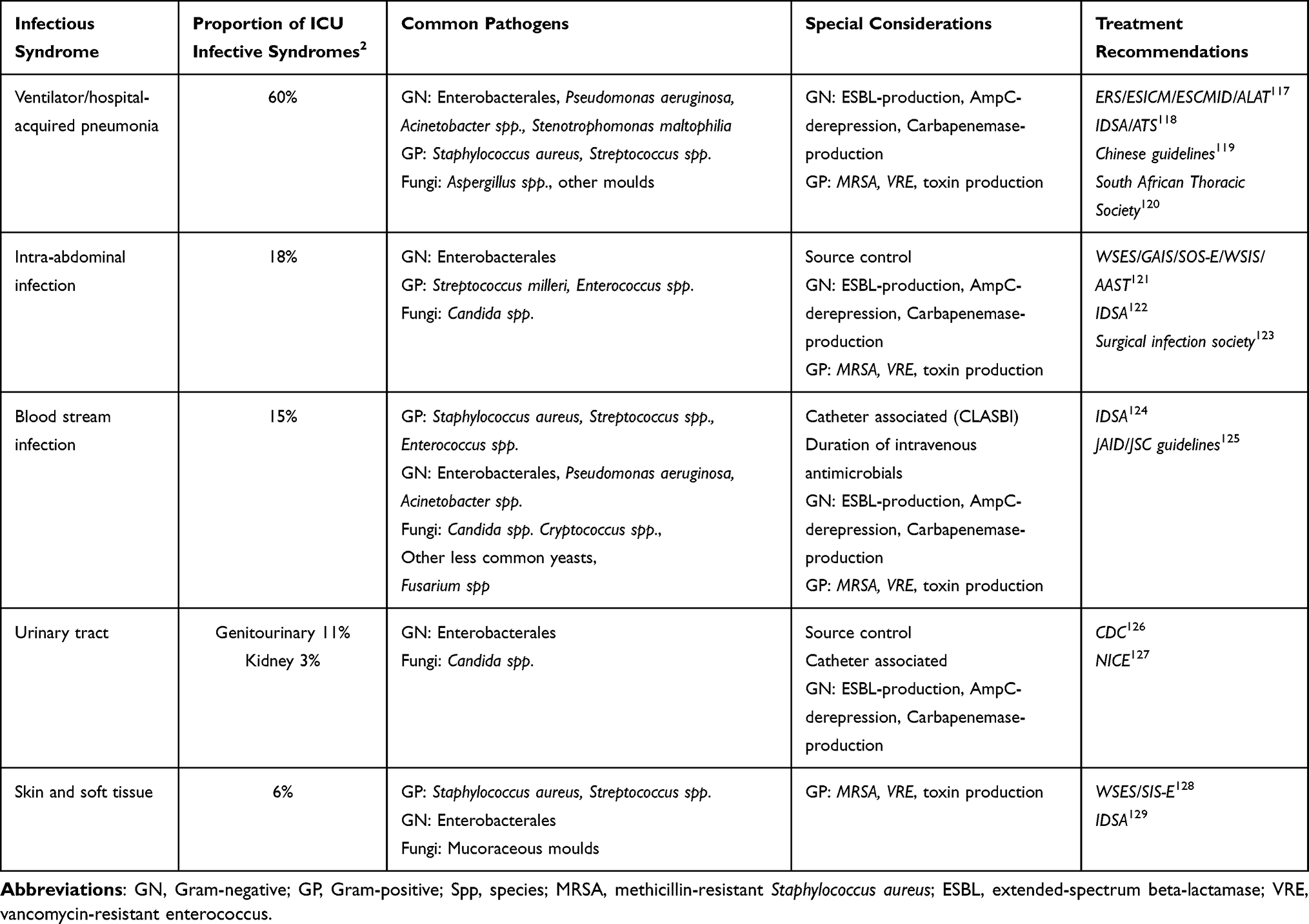 |
Table 3 Prevalence, Common Causative Organisms, and Treatment Recommendations for Common Infective Syndromes Diagnosed in Intensive Care Patients |
When managing infection in the ICU, it is important to consider host, antimicrobial, and organism factors that can influence the outcome of treatment.60 The presumed site of infection may require specific considerations (Table 3), such as line removal or source control, and the nature of the organism and its phenotype can play an important role in antimicrobial selection and duration of treatment. Critically ill patients will often have highly variable pharmacokinetics (PK), making dose optimisation challenging. Environmental factors often mean that organisms with higher levels of a drug tolerance/resistance are also present, making selection and optimisation of antimicrobial therapy difficult.11,12 It is important to have knowledge of local epidemiology to ensure that optimal empiric treatment decisions are made and antimicrobial pharmacodynamics (PD) optimised. Linking antimicrobial decision-making into the holistic management of infection in the ICU is vital, including fluid resuscitation, haemodynamic management, ventilation, and consideration of additional therapeutic interventions including blood sugar control, corticosteroids, and restrictive transfusion strategies.32
Empiric Antimicrobial Therapy
Empirical antimicrobial selection aims to cover common causative organisms for an infection whilst awaiting definitive results to facilitate targeted treatment to be delivered. Empiric treatment should aim to provide an appropriate antimicrobial spectrum for common causative organisms and prevalent drug-resistant phenotypes. It should select agents with appropriate PK/PD properties for the suspected site and severity of infection.
A major challenge in the ICU is the greater prevalence of drug-resistant infections and the often potential severe consequences of selecting an inappropriate empiric treatment regimen.11,12 This means that broad-spectrum antimicrobials with anti-pseudomonal spectrum are often required. In areas with high prevalence of MRSA, glycopeptides are often co-administered empirically.32 For suspected fungal infection, the commencement of echinocandin therapy is recommended for suspected candidaemia with amphotericin-B often used empirically for invasive mould infections.13,61 The diagnosis of infection often requires consideration of numerous factors summarised in Figure 1. Based on a syndromic diagnosis (eg respiratory tract, urinary tract, skin-soft-tissue infection) guidelines are developed taking into account common causative organisms and local resistance patterns. Table 3 summarises common causative organisms, special considerations, and national/international guidance that is often taken into consideration for common syndromic diagnoses in the ICU.
In addition to ensuring an appropriate spectrum of therapy is delivered as part of empiric treatment, optimisation of drug delivery must also be considered.60 Critical illness is a major cause of PK/PD variation that is associated with increased risk of mortality, especially in sepsis.62 To address observed variability in antimicrobial PK/PD, prolonged or continuous infusion of beta-lactam and glycopeptide antibiotics is often recommended to ensure optimised targeted attainment.63,64
Targeted/Individualised Antimicrobial Therapy
In septic shock, the administration of antimicrobial therapy within an hour of recognition has been suggested to be important to reduce mortality.32 In patients without shock, current guidelines support commencement of therapy within up to 3 hours of recognition.32 Whilst delaying empiric treatment decisions until culture-based diagnostic results are available is often not possible in critically ill patients with bacterial or fungal infection, developments in point-of-care molecular diagnostic platforms may provide a greater abundance of information with which to deliver targeted therapy sooner.65–67 For example, Banerjee et al demonstrated that linkage of a multiplex molecular diagnostic facilitated rapid organism identification, targeted therapy, and more rapid de-escalation of treatment when linked with antimicrobial stewardship support for patients with positive blood cultures.54
Once culture-based diagnostics provide appropriate organism and susceptibility results, switching from broad-spectrum empiric therapy to targeted treatment can reduce potential adverse events for patients and reduce the propagation of AMR.68 Despite a lack of randomised control trial data supporting the safety of early de-escalation of antimicrobial therapy in sepsis,69 observational data have demonstrated that early de-escalation is safe and does not impact on mortality.70 Furthermore, a large retrospective analysis of over 17,000 patients admitted to hospitals in the USA with sepsis identified an increased risk of mortality associated with unnecessarily broad antimicrobial therapy within this cohort.9
The role of therapeutic drug monitoring (TDM) to ensure optimal drug exposure in critically ill patients is now recognised. Guidance on antimicrobial TDM in critically ill patients is emerging from beta-lactam antibiotics, and agents with narrow therapeutic windows, such as vancomycin and linezolid.71 The overall impact of antimicrobial and antifungal TDM on patient outcomes is still to be determined,72 but it is likely to be an important consideration to ensure that optimal PK/PD targets are achieved in patients with highly variable pharmacokinetics.
The Importance of Source Control and Other Non-Antimicrobial Factors
In addition to optimal antimicrobial selection, infection management must ensure adequate source control where possible.73–75 The objective of source control is to remove any source of persistent infection, prevent ongoing contamination, and restore pre-morbid function and anatomy where possible.74 Source control can be divided into three broad categories: drainage of collections or abscesses, debridement or removal of infected devices, and definitive control measures.75 Current guidelines recommend prompt performance of source control, when safe to do so, to ensure optimal outcomes for individual patients.32
Within the ICU, source control is often focussed on reducing or eliminating invasive interventions that are no longer required. Whilst routine replacement of central venous catheters has not been shown to reduce infection risk and is not recommended,76 such devices should be reviewed regularly and removed when they are no longer required or replaced if there is suspicion of catheter associated infection.76,77 If infection is suspected, catheters should be placed at a new site and re-wiring the old line should be avoided. Daily sedation holds and spontaneous breathing trials have been suggested as a means to reduce the need for mechanical ventilation,78 although this approach has not been consistently found to reduce the duration of mechanical ventilation.79,80
Infection Prevention in the ICU
A high proportion of secondary bacterial and fungal infections in the ICU are preventable.1 Table 4 summarises key infection prevention measures that can be applied generally and to different syndromic settings within the ICU.
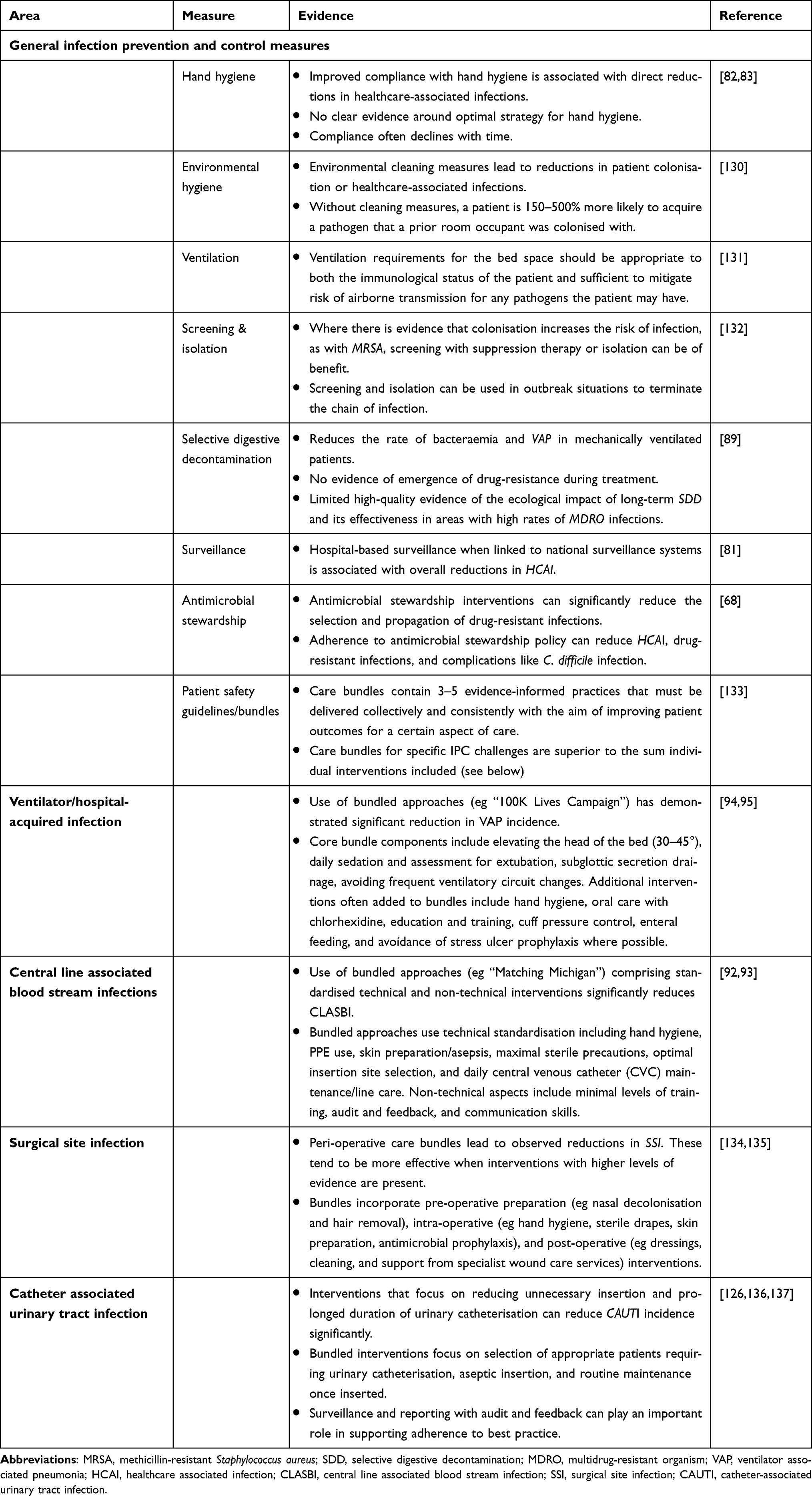 |
Table 4 Summary of Common Infection Prevention and Control Approaches in the Intensive Care Unit |
Infection prevention in the ICU relies on a multi-modal approach that encompasses hand hygiene, environmental hygiene, screening and isolation approaches, surveillance, antimicrobial stewardship, and implementation of specific patient safety guidelines and bundles.81 Hand hygiene is probably the most important infection prevention intervention. There is robust evidence that links rates of hand hygiene compliance with incidence of nosocomial infection.82,83 The aim of hand hygiene is to reduce transient micro-organisms that are acquired by healthcare staff during the course of their working day. These transient organisms are easily transmitted on contact with patients and therefore are a primary route for the spread of nosocomial pathogens.82,83 The use of alcohol-based hand gels and soap and water washing is the mainstay of hand hygiene. An example of the impact of breakdown in hand hygiene measures within the ICU was observed globally during the COVID-19 pandemic, with outbreaks of organisms such as Corynebacterium striatum observed following breakdown in hand washing and glove changes between patients due to adaptions in personal protective equipment (PPE) policy to protect healthcare workers.84
The selection of transmission-based precautions to reduce the transmission of drug-resistant bacteria (eg MRSA and GRE) is often controversial. Randomised control trial data have failed to demonstrate significant reductions in transmission through the implementation of barrier precautions in colonised patients.85 Hand hygiene adherence is likely to have the greatest overall impact in reducing transmission of drug-resistant organisms, such as GRE.86 For organisms that can have persistence in the environment, such as Clostridioides difficile spores, hand hygiene, environmental control, and appropriate barrier precautions can reduce transmission to other patients.87
Surveillance is an ongoing challenge that can be performed at local, regional, and national levels. Within England and the United Kingdom, reporting of certain infections such as MRSA blood stream infections and central-line associated blood stream infections are mandatory and can help to drive a culture of safety and accountability. The screening and reporting of AMR can help identify outbreaks and inform development of local antimicrobial policy.88
Selective Decontamination of the Digestive Tract (SDD) has been proposed to reduce the risk of ventilator-associated pneumonia in patients requiring invasive mechanical ventilation.89,90 SDD is the application of topical nonabsorbable antibiotics and antifungal agents to the upper gastrointestinal tract combined with a short course of intravenous antibiotics. A recent large randomised trial of SDD showed that although SDD did not reduce mortality there was a reduction in the rate of bacteraemia (5.6% vs 8.1%) and the number of drug-resistant infections (23.1% vs 34.6%).91 A subsequent meta-analysis of studies of SDD has shown that SDD may reduce mortality, VAP, and ICU-acquired bacteraemia.89 Whilst observational data in areas with relatively low prevalence of drug-resistant infections suggest that SDD does not promote the development of AMR, high-quality data on the unintended consequences of SDD at an ecological level remains to be established.90
Within hospitals, including critical care departments, IPC policy aims to implement multi-modal interventions that facilitate safe, effective, and high-quality care for patients. In addition to general IPC measures, care bundles are recognised to reduce infection risk for a range of nosocomial infections (Table 4). Care bundles are a collection of interventions that implemented together have a greater impact than the sum of individual interventions used within it. The “Matching Michigan” campaign for the prevention of central line associated blood stream infections92,93 and ‘100K lives campaign’ for ventilator associated pneumonia94,95 are examples of bundled interventions that have significantly reduced rates of infection following their implementation. The Surviving Sepsis Campaign is an example of a bundled intervention that has been demonstrated to reduce mortality in patients with sepsis.96
Conclusion
Bacterial and fungal infection in ICU patients are important events that must be considered by all those involved in the care of critically ill patients. A large proportion of infections are preventable through the implementation and adherence to multi-modal IPC policies. The diagnosis of infection can be complex and evolve over time as additional information becomes available. The advent of molecular diagnostics and rapid methods for determination of AST are providing us with information on organism characteristics sooner. This must be applied to a wider decision-making context to ensure that these new technologies have significant benefit for patients.
Acknowledgments
The authors would also like to acknowledge (i) the National Institute of Health Research Imperial Biomedical Research Centre and the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Healthcare Associated Infection and Antimicrobial Resistance at Imperial College London in partnership with Public Health England and the NIHR Imperial Patient Safety Translational Research Centre; (ii) The Department of Health and Social Care funded Centre for Antimicrobial Optimisation (CAMO), Imperial College London, provides state-of-the-art research facilities and consolidates multidisciplinary academic excellence, clinical expertise, Imperial’s NIHR/Wellcome funded Clinical Research Facility (CRF), and partnerships with the NHS to support and deliver innovative research on antimicrobial optimisation and precision prescribing; (iii) the National Institute for Health Research (NIHR) Imperial Biomedical Research Centre (BRC).
The views expressed in this publication are those of the author(s) and not necessarily those of the DHSC, NHS, or the NIHR.
Disclosure
TMR received honoraria for consultancy from Sandoz (2020), honoraria for the delivery of educational activities from BioMerieux (2021–2022), and speakers fees from Roche Diagnostics Ltd (2021).
LSPM has consulted for or received speaker fees from bioMerieux (2013–2023), Pfizer (2018–2023), Eumedica (2016–2022), Umovis Lab (2020–2021), Shionogi (2021–2023), Kent Pharma (2021), Sumitovant (2021–2023) and Pulmocide (2021), and received research grants from the National Institute for Health Research (2013–2023), CW + Charity (2018–2023), Infectopharm (2022–2023), and LifeArc (2020–2021).
All other authors declare no competing interests.
References
1. Guest Julian F, Tomas K, Dinah G, Neil W. Modelling the annual NHS costs and outcomes attributable to healthcare-associated infections in England. BMJ open. 2020;10(1):e033367. doi:10.1136/bmjopen-2019-033367
2. Louis VJ, Yasser S, Mervyn S, et al. Prevalence and outcomes of infection among patients in intensive care units in 2017. JAMA. 2020;323(15):1478. doi:10.1001/JAMA.2020.2717
3. Louis VJ, Jordi R, John M, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–2329. doi:10.1001/JAMA.2009.1754
4. Magill Shelley S, Edwards Jonathan R, Wendy B, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2014;370(13):1198–1208. doi:10.1056/nejmoa1306801
5. Magnason S, Kristinsson KG, Stefansson T, et al. Risk factors and outcome in ICU-acquired infections. Acta Anaesthesiol Scand. 2008;52(9):1238–1245. doi:10.1111/J.1399-6576.2008.01763.X
6. Pen YS, Yin CY, Shui HH, Der WF. A risk factor analysis of healthcare-associated fungal infections in an intensive care unit: a retrospective cohort study. BMC Infect Dis. 2013;13(1):1–10. doi:10.1186/1471-2334-13-10/TABLES/3
7. Montagna MT, Caggiano G, Lovero G, et al. Epidemiology of invasive fungal infections in the intensive care unit: results of a multicenter Italian survey (Aurora Project). Infection. 2013;41(3):645. doi:10.1007/S15010-013-0432-0
8. Aleksa D, Branko M, Ivana M, et al. Hospital-acquired infections in the adult intensive care unit—Epidemiology, antimicrobial resistance patterns, and risk factors for acquisition and mortality. Am J Infect Control. 2020;48(10):1211–1215. doi:10.1016/J.AJIC.2020.01.009
9. Chanu R, Kadri Sameer S, Dekker John P, et al. Prevalence of antibiotic-resistant pathogens in culture-proven sepsis and outcomes associated with inadequate and broad-spectrum empiric antibiotic use. JAMA Netw Open. 2020;3(4):e202899–e202899. doi:10.1001/JAMANETWORKOPEN.2020.2899
10. Ecdc. AER for 2017: healthcare-associated infections acquired in intensive care units; 2017.
11. De Waele Jan J, Murat A, Massimo A, et al. Antimicrobial resistance and antibiotic stewardship programs in the ICU: insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med. 2018;44(2):189–196. doi:10.1007/S00134-017-5036-1/FIGURES/3
12. Matteo B, De Waele Jan J, Philippe E, et al. Preventive and therapeutic strategies in critically ill patients with highly resistant bacteria. Intensive Care Med. 2015;41(5):776–795. doi:10.1007/S00134-015-3719-Z
13. Judith B, Krysan Damian J. Drug resistance and tolerance in fungi. Nat Rev Microbiol. 2020;18(6):319–331. doi:10.1038/s41579-019-0322-2
14. Fisher Matthew C, Ana A-I, Judith B, et al. Tackling the emerging threat of antifungal resistance to human health. Nat Rev Microbiol. 2022;20(9):557–571. doi:10.1038/s41579-022-00720-1
15. Silke S, Ferry H, Rhodes Johanna L, et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control. 2016;5(1):35. doi:10.1186/s13756-016-0132-5
16. Eyre David W, Sheppard Anna E, Hilary M, et al. A candida auris outbreak and its control in an intensive care setting. N Engl J Med. 2018;379(14):1322–1331. doi:10.1056/NEJMoa1714373
17. Chow Nancy A, Lalitha G, Tsay Sharon V, et al. Multiple introductions and subsequent transmission of multidrug-resistant Candida auris in the USA: a molecular epidemiological survey. Lancet Infect Dis. 2018;18(12):1377–1384. doi:10.1016/S1473-3099(18)30597-8
18. Jensen RH, Johansen HK, Søes LM, et al. Posttreatment antifungal resistance among colonizing candida isolates in candidemia patients: results from a systematic multicenter study. Antimicrob Agents Chemother. 2016;60(3):1500–1508. doi:10.1128/AAC.01763-15
19. Pristov KE, Ghannoum MA. Resistance of Candida to azoles and echinocandins worldwide. Clin Microbiol Infect. 2019;25(7):792–798. doi:10.1016/j.cmi.2019.03.028
20. Eva A, Ana G, Paula L-E, et al. Fluconazole-resistant Candida parapsilosis clonally related genotypes: first report proving the presence of endemic isolates harbouring the Y132F ERG11 gene substitution in Spain. Clin Microbiol Infect. 2022;28(8):1113–1119. doi:10.1016/j.cmi.2022.02.025
21. Ashutosh S, Singh Pradeep K, Bansidhar T, et al. Emergence of clonal fluconazole-resistant Candida parapsilosis clinical isolates in a multicentre laboratory-based surveillance study in India. J Antimicrob Chemother. 2019;74(5):1260–1268. doi:10.1093/jac/dkz029
22. Magobo Rindidzani E, Lockhart Shawn R, Govender Nelesh P, et al. Fluconazole‐resistant Candida parapsilosis strains with a Y132F substitution in the ERG11 gene causing invasive infections in a neonatal unit, South Africa. Mycoses. 2020;63(5):471–477. doi:10.1111/myc.13070
23. van der Linden Jan WM, Eveline S, Kampinga Greetje A, et al. Clinical implications of azole resistance in aspergillus fumigatus, the Netherlands, 2007–2009. Emerg Infect Dis. 2011;17(10):1846–1854. doi:10.3201/eid1710.110226
24. Martin H, Jon S-G, Walsh Thomas J, et al. Global guideline for the diagnosis and management of rare mould infections: an initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology and the American Society for Microbiolo. Lancet Infect Dis. 2021;21(8):e246–e257. doi:10.1016/S1473-3099(20)30784-2
25. Rawson TM, Wilson RC, Holmes A. Understanding the role of bacterial and fungal infection in COVID-19. Clin Microbiol Infect. 2020. doi:10.1016/j.cmi.2020.09.025
26. Damien C, Aurore C, Olivier P, et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann Intensive Care. 2020;10(1):1–9. doi:10.1186/S13613-020-00736-X/FIGURES/1
27. Rawson Timothy M, Damien M, Raheelah A, Moore Luke SP, Holmes Alison H. Antimicrobial use, drug-resistant infections and COVID-19. Nat Rev Microbiol. 2020;18:1–2. doi:10.1038/s41579-020-0395-y
28. Rawson TM, Moore LS, Castro-Sanchez E, et al. COVID-19 and the potential long term impact on antimicrobial resistance. J Antimicrob Chemother. 2020;75:1687. doi:10.1093/jac/dkaa194
29. Verweij Paul E, Rijnders Bart JA, Brüggemann Roger JM, et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med. 2020;46(8):1524–1535. doi:10.1007/s00134-020-06091-6
30. Philipp K, Matteo B, Arunaloke C, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021;21(6):e149–e162. doi:10.1016/S1473-3099(20)30847-1
31. Martin H, Danila S, Rosanne S, et al. COVID-19-associated fungal infections. Nat Microbiol. 2022;7(8):1127–1140. doi:10.1038/s41564-022-01172-2
32. Laura E, Andrew R, Waleed A, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):E1063–E1143. doi:10.1097/CCM.0000000000005337
33. Mervyn S, Deutschman Clifford S, Warren SC, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801. doi:10.1001/jama.2016.0287
34. Yu Sean C, Nirmala S, Kevin B, et al. Comparison of early warning scores for sepsis early identification and prediction in the general ward setting. JAMIA Open. 2021;4(3). doi:10.1093/jamiaopen/ooab062
35. Michael M, Bastian R, Max H, Jutzeler Catherine R, Karsten B. Early prediction of sepsis in the ICU using machine learning: a systematic review. Front Med. 2021;8. doi:10.3389/fmed.2021.607952
36. Mervyn S, Matt I-K, Manu S-H. Sepsis hysteria: excess hype and unrealistic expectations. Lancet. 2019;394(10208):1513–1514. doi:10.1016/S0140-6736(19)32483-3
37. Gang C, Kailiang X, Fangyuan S, Yuxia S, Ziyuan K, Bangjiang F. Risk factors of multidrug-resistant bacteria in lower respiratory tract infections: a systematic review and meta-analysis. Can J Infect Dis Med Microbiol. 2020;2020. doi:10.1155/2020/7268519
38. Miles RT, Esmita C, Moore LSP, et al. Mapping the decision pathways of acute infection management in secondary care among UK medical physicians: a qualitative study. BMC Med. 2016;14(1):208. doi:10.1186/s12916-016-0751-y
39. Kevin M, Parker Sarah K, Todd James K, Dominguez Samuel R. Implementation of rapid molecular infectious disease diagnostics: the role of diagnostic and antimicrobial stewardship. J Clin Microbiol. 2017;55(3):715–723. doi:10.1128/JCM.02264-16
40. Robert T. Sensitivity, specificity, and predictive values: foundations, pliabilities, and pitfalls in research and practice. Front Public Heal. 2017;5:1–7. doi:10.3389/fpubh.2017.00307
41. Public Health England. UK standards for microbiology investigations. Bacteriology. 2015;55(5.2):1–21.
42. Khan Zeeshan A, Siddiqui Mohd F, Seungkyung P. Current and emerging methods of antibiotic susceptibility testing. Diagnostics. 2019;9(2):49. doi:10.3390/diagnostics9020049
43. Brigitte L, Sylvie D, Arendrup Maiken C, Jacques PJ, Pierre T. How to optimize the use of blood cultures for the diagnosis of bloodstream infections? A State-of-the art. Front Microbiol. 2016;7:697. doi:10.3389/FMICB.2016.00697
44. Anna Å, Emma J, Erika M, et al. EUCAST rapid antimicrobial susceptibility testing (RAST) in blood cultures: validation in 55 European laboratories. J Antimicrob Chemother. 2020;75(11):3230–3238. doi:10.1093/JAC/DKAA333
45. Emma J, Erika M, Gunnar K. The EUCAST rapid disc diffusion method for antimicrobial susceptibility testing directly from positive blood culture bottles. J Antimicrob Chemother. 2020;75(4):968–978. doi:10.1093/JAC/DKZ548
46. van Belkum A, Bachmann TT, Gerd L, et al. Developmental roadmap for antimicrobial susceptibility testing systems. Nat Rev Microbiol. 2018;17(1):51–62. doi:10.1038/s41579-018-0098-9
47. van Belkum A, Burnham Carey Ann D, Rossen JWA, Frederic M, Olivier R, Michael DW. Innovative and rapid antimicrobial susceptibility testing systems. Nat Rev Microbiol. 2020;18(5):299–311. doi:10.1038/s41579-020-0327-x
48. Antony C, Guy P, Gilbert G. Applications of MALDI-TOF mass spectrometry in clinical diagnostic microbiology. FEMS Microbiol Rev. 2012;36(2):380–407. doi:10.1111/j.1574-6976.2011.00298.x
49. Osthoff M, Gürtler N, Bassetti S, et al. Impact of MALDI-TOF-MS-based identification directly from positive blood cultures on patient management: a controlled clinical trial. Clin Microbiol Infect. 2017;23(2):78–85. doi:10.1016/j.cmi.2016.08.009
50. Timbrook Tristan T, Morton Jacob B, McConeghy Kevin W, Caffrey Aisling R, Eleftherios M, LaPlante Kerry L. The effect of molecular rapid diagnostic testing on clinical outcomes in bloodstream infections: a systematic review and meta-analysis. Clin Infect Dis. 2017;64(1):15–23. doi:10.1093/cid/ciw649
51. Buchan Blake W, Ledeboer Nathan A. Emerging technologies for the clinical microbiology laboratory. Clin Microbiol Rev. 2014;27(4):783–822. doi:10.1128/CMR.00003-14
52. Wickes Brian L, Wiederhold Nathan P, Harvey TA, Prum RO. Molecular diagnostics in medical mycology. Nat Commun. 2018;9(1):1–13. doi:10.1038/s41467-018-07556-5
53. Antti V, Hytönen Vesa P, Laitinen Olli H. Modern tools for rapid diagnostics of antimicrobial resistance. Front Cell Infect Microbiol. 2020;10:308. doi:10.3389/FCIMB.2020.00308/BIBTEX
54. Ritu B, Teng Christine B, Cunningham Scott A, et al. Randomized trial of rapid multiplex polymerase chain reaction–based blood culture identification and susceptibility testing. Clin Infect Dis. 2015;61(7):1071–1080. doi:10.1093/cid/civ447
55. Miles RT. Understanding how diagnostics influence antimicrobial decision-making is key to successful clinical trial design. Clin Microbiol Infect. 2023. doi:10.1016/j.cmi.2023.03.010
56. Muriel F, Nseir S, Mégarbane B. Respiratory multiplex PCR and procalcitonin to reduce antibiotic exposure in severe SARS-CoV-2 pneumonia: a multicenter randomised controlled trial. Clin Microbiol Infect. 2023. doi:10.1016/j.cmi.2023.01.009
57. Anne HC, Bertrand E, Nancy W, et al. Impact of rapid antimicrobial susceptibility testing in gram-negative rod bacteremia: a quasi-experimental study. J Clin Microbiol. 2020;58(9). doi:10.1128/JCM.00360-20
58. Vanesa A-V, Cristina S, Timothy P. Impact of rapid susceptibility testing on antimicrobial therapy and clinical outcomes in Gram-negative bloodstream infections. J Antimicrob Chemother. 2022;77(3):771–781. doi:10.1093/jac/dkab449
59. Christensen Alyssa B, Brent F, Tobias P, et al. Impact of a laboratory-developed phenotypic rapid susceptibility test directly from positive blood cultures on time to narrowest effective therapy in patients with gram-negative bacteremia: a prospective randomized trial. Open Forum Infect Dis. 2022;9(7). doi:10.1093/ofid/ofac347
60. Rawson Timothy M, Wilson Richard C, O’Hare D, et al. Optimizing antimicrobial use: challenges, advances and opportunities. Nat Rev Microbiol. 2021;19(12):747–758. doi:10.1038/s41579-021-00578-9
61. Pappas Peter G, Lionakis Michail S, Cavling AM, Luis O-Z, Jan KB. Invasive candidiasis. Nat Rev Dis Prim. 2018;4(1):1–20. doi:10.1038/nrdp.2018.26
62. Roberts Jason A, Paul Sanjoy K, Murat A, et al. DALI: defining antibiotic levels in intensive care unit patients: are current ??-lactam antibiotic doses sufficient for critically ill patients? Clin Infect Dis. 2014;58(8):1072–1083. doi:10.1093/cid/ciu027
63. Michael O, Martin S, Gianmarco B, Hafiz A-AM, Roberts JA. Prolonged administration of β-lactam antibiotics - a comprehensive review and critical appraisal. Swiss Med Wkly. 2016;146:w14368. doi:10.4414/smw.2016.14368
64. Roberts Jason A, Mohd-Hafiz A-A, Davis Joshua S, et al. Continuous versus intermittent β-lactam infusion in severe sepsis. a meta-analysis of individual patient data from randomized trials. Am J Respir Crit Care Med. 2016;194(6):681–691. doi:10.1164/rccm.201601-0024OC
65. Kollef Marin H, Shorr Andrew F, Matteo B, et al. Timing of antibiotic therapy in the ICU. Crit Care. 2021;25(1). doi:10.1186/S13054-021-03787-Z
66. Solen K, Benoit V, Laurence A-L, François TJ. Molecular diagnostic methods for pneumonia: how can they be applied in practice? Curr Opin Infect Dis. 2021;34(2):118–125. doi:10.1097/QCO.0000000000000713
67. Maria PA, Adam S, Anna H, Adam I, Harris Patrick NA. New microbiological techniques for the diagnosis of bacterial infections and sepsis in ICU INCLUDING POINT OF CARE. Curr Infect Dis Rep. 2021;23(8). doi:10.1007/S11908-021-00755-0
68. David B, Primrose GB, Francesco B, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(9):990–1001. doi:10.1016/S1473-3099(17)30325-0
69. Silva Brenda NG, Andriolo Régis B, Atallah Álvaro N, Reinaldo S. De-escalation of antimicrobial treatment for adults with sepsis, severe sepsis or septic shock. Cochrane Database Syst Rev. 2013;2018(12). doi:10.1002/14651858.CD007934.pub3
70. Barberena MR, Viteri GJA, Castillo ZWJ, Kessler BF. De-escalation, adequacy of antibiotic therapy and culture positivity in septic patients: an observational study. Rev Bras Ter Intensiva. 2016;28:315–322. doi:10.5935/0103-507X.20160044
71. Abdul-Aziz Mohd H, Alffenaar Jan Willem C, Matteo B, et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: a Position Paper. Intensive Care Med. 2020;46(6):1127–1153. doi:10.1007/s00134-020-06050-1
72. Stefan H, Friedhelm B, Thorsten B, et al. Effect of therapeutic drug monitoring-based dose optimization of piperacillin/tazobactam on sepsis-related organ dysfunction in patients with sepsis: a randomized controlled trial. Intensive Care Med. 2022;48(3):311–321. doi:10.1007/s00134-021-06609-6
73. Leonel L, Belen E, Sergio R-E. Current understanding in source control management in septic shock patients: a review. Ann Transl Med. 2016;4(17):330. doi:10.21037/atm.2016.09.02
74. De Waele Jan J, Massimo G, Ignacio M-L. Source control in the management of sepsis and septic shock. Intensive Care Med. 2022;48(12):1799–1802. doi:10.1007/s00134-022-06852-5
75. Marshall John C, Al Naqbi A. Principles of source control in the management of sepsis. Crit Care Clin. 2009;25(4):753–768. doi:10.1016/j.ccc.2009.08.001
76. O’Grady Naomi P, Mary A, Burns Lillian A, et al. Guidelines for the Prevention of Intravascular Catheter-related Infections. Clin Infect Dis. 2011;52(9):e162–e193. doi:10.1093/cid/cir257
77. Peter P, Dale N, Sean B, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–2732. doi:10.1056/NEJMoa061115
78. Girard Timothy D, Kress John P, Fuchs Barry D, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371(9607):126–134. doi:10.1016/S0140-6736(08)60105-1
79. Augustes R, Ho KM. meta-analysis of randomised controlled trials on daily sedation interruption for critically ill adult patients. Anaesth Intensive Care. 2011;39(3):401–409. doi:10.1177/0310057X1103900310
80. Sangeeta M. Daily sedation interruption in mechanically ventilated critically ill patients cared for with a sedation protocol. JAMA. 2012;308(19):1985. doi:10.1001/jama.2012.13872
81. Julie S, Anthony T, Walter Z, et al. Core components for effective infection prevention and control programmes: new WHO evidence-based recommendations. Antimicrob Resist Infect Control. 2017;6(1):6. doi:10.1186/s13756-016-0149-9
82. Didier P, Stéphane H, Stephan H, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Lancet. 2000;356(9238):1307–1312. doi:10.1016/S0140-6736(00)02814-2
83. Sarah T-S, Hans P, Widmer Andreas F. Hand hygiene in the intensive care unit. Crit Care Med. 2010;38:S299–S305. doi:10.1097/CCM.0b013e3181e6a23f
84. Kim Janice J, Turner Nancy E, Emily H, et al. Corynebacterium striatum outbreak among ventilated COVID-19 patients in an acute care hospital – California, 2021. Open Forum Infect Dis. 2021;8(Supplement_1):S495–S496. doi:10.1093/ofid/ofab466.998
85. Charles HW, Huckabee Charmaine M, O’Grady Naomi P, et al. Intervention to reduce transmission of resistant bacteria in intensive care. N Engl J Med. 2011;364(15):1407–1418. doi:10.1056/NEJMoa1000373
86. De Angelis G, Cataldo MA, De Waure C, et al. Infection control and prevention measures to reduce the spread of vancomycin-resistant enterococci in hospitalized patients: a systematic review and meta-analysis. J Antimicrob Chemother. 2014;69(5):1185–1192. doi:10.1093/jac/dkt525
87. Gerding Dale N, Muto Carlene A, Owens J, Robert C. Measures to Control and Prevent Clostridium difficile Infection. Clin Infect Dis. 2008;46(s1):S43–S49. doi:10.1086/521861
88. Nizam D. Surveillance and outbreak management. Man Infect Prev Control. 2019;2019:68–94.
89. Hammond Naomi E, John M, Ian S, et al. Association between selective decontamination of the digestive tract and in-hospital mortality in intensive care unit patients receiving mechanical ventilation. JAMA. 2022;328(19):1922. doi:10.1001/jama.2022.19709
90. Miles RT, Prockter MLS, Christopher HJ, Hugo D, Helen HA. Plasmid-mediated colistin resistance mechanisms: is it time to revise our approach to selective digestive decontamination? Lancet Infect Dis. 2016;16(2):149–150. doi:10.1016/S1473-3099(15)00539-3
91. Catherine B, Emma B, Timothy C, et al. Effect of selective decontamination of the digestive tract on hospital mortality in critically ill patients receiving mechanical ventilation. JAMA. 2022;328(19):1911. doi:10.1001/jama.2022.17927
92. Niccolò B, Jonas M, Marci D, et al. Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2022;43(5):553–569. doi:10.1017/ice.2022.87
93. Julian B, Annette R, Peter H, et al. ‘Matching Michigan’: a 2-year stepped interventional programme to minimise central venous catheter-blood stream infections in intensive care units in England. BMJ Qual Saf. 2013;22(2):110–123. doi:10.1136/bmjqs-2012-001325
94. Jordi R, Hartmut L, Giuseppe C, Robert M. A European care bundle for prevention of ventilator-associated pneumonia. Intensive Care Med. 2010;36(5):773–780. doi:10.1007/s00134-010-1841-5
95. Hellyer Thomas P, Victoria E, Peter W, John SA. The Intensive Care Society recommended bundle of interventions for the prevention of ventilator-associated pneumonia. J Intensive Care Soc. 2016;17(3):238–243. doi:10.1177/1751143716644461
96. Levy Mitchell M, Phillip DR, Townsend Sean R, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010;36(2):222–231. doi:10.1007/s00134-009-1738-3
97. Julien P, Lauro D, Anne B, et al. Risk factors for candidemia: a prospective matched case-control study. Critical Care. 2020;24:1. doi:10.1186/s13054-020-2766-1
98. Jenks Jeffrey D, Nam Hannah H, Martin H. Invasive aspergillosis in critically ill patients: review of definitions and diagnostic approaches. Mycoses. 2021;64(9):1002–1014. doi:10.1111/MYC.13274
99. Ibrahim Ashraf S, Brad S, Walsh Thomas J, Kontoyiannis Dimitrios P. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54(SUPPL. 1):1–7. doi:10.1093/cid/cir865
100. Lewis WP, Price Jessica S, Matthijs B. Pneumocystis jirovecii pneumonia: epidemiology, clinical manifestation and diagnosis. Curr Fungal Infect Rep. 2019;13(4):260–273. doi:10.1007/s12281-019-00349-3
101. Diling W, Chenfang W, Siye Z, Yanjun Z. Risk factors of ventilator-associated pneumonia in critically III patients. Front Pharmacol. 2019;10. doi:10.3389/FPHAR.2019.00482
102. Bonten Marc JM, Kollef Marin H, Hall Jesse B. Risk factors for ventilator-associated pneumonia: from epidemiology to patient management. Clin Infect Dis. 2004;38(8):1141–1149. doi:10.1086/383039/2/38-8-1141-TBL003.GIF
103. François TJ, Etienne R, François B, Alexis T, Matteo B. Bloodstream infections in critically ill patients: an expert statement. Intensive Care Med. 2020;46(2):266. doi:10.1007/S00134-020-05950-6
104. Kiang LE, Alvin T, Gillian L, et al. Risk factors associated with urinary tract infections in intensive care patients. Infect Dis Heal. 2016;21(2):62–66. doi:10.1016/J.IDH.2016.03.004
105. Rampini Silvana K, Bloemberg Guido V, Keller Peter M, et al. Broad-range 16S rRNA gene polymerase chain reaction for diagnosis of culture-negative bacterial infections. Clin Infect Dis. 2011;53(12):1245–1251. doi:10.1093/cid/cir692
106. Pepper Dominique J, Junfeng S, Chanu R, et al. Procalcitonin-guided antibiotic discontinuation and mortality in critically ill adults: a systematic review and meta-analysis. Chest. 2019;155(6):1109. doi:10.1016/J.CHEST.2018.12.029
107. Liliana S, France G, Amre Devendra K, Patrick S-L, Jacques L. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis. 2004;39(2):206–217. doi:10.1086/421997
108. Von Dach E, Albrich Werner C, Sophie BA, et al. Effect of C-reactive protein–guided antibiotic treatment duration, 7-day treatment, or 14-day treatment on 30-day clinical failure rate in patients with uncomplicated gram-negative bacteremia: a randomized clinical trial. JAMA. 2020;323(21):2160–2169. doi:10.1001/JAMA.2020.6348
109. Rawson Timothy M, Esmita C, Moore Luke SP, et al. Exploring the Use of C-Reactive Protein to Estimate the Pharmacodynamics of Vancomycin. Ther Drug Monitor. 2018;40(3):315–321. doi:10.1097/FTD.0000000000000507
110. Ramos-Martín V, Neely MN, McGowan P, et al. Population pharmacokinetics and pharmacodynamics of teicoplanin in neonates: making better use of C-reactive protein to deliver individualized therapy. J Antimicrob Chemother. 2016;71:dkw295. doi:10.1093/jac/dkw295
111. Clancy Cornelius J, Hong NM. Diagnosing invasive candidiasis. J Clin Microbiol. 2018;56(5). doi:10.1128/JCM.01909-17
112. Małgorzata M, Thierry C, Maurizio S, Daniel P, Claudio V. The use of mannan antigen and anti-mannan antibodies in the diagnosis of invasive candidiasis: recommendations from the Third European Conference on Infections in Leukemia. Crit Care. 2010;14(6). doi:10.1186/CC9365
113. Tomer A, Itzhak L, Hannah S, Dafna Y, Leonard L, Mical P. Diagnostic accuracy of PCR alone compared to galactomannan in bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis: a systematic review. J Clin Microbiol. 2012;50(11):3652–3658. doi:10.1128/JCM.00942-12/SUPPL_FILE/ZJM999092057SO2.PDF
114. Huurneman Luc J, Michael N, Anette V, et al. Pharmacodynamics of voriconazole in children: further steps along the path to true individualized therapy. Antimicrob Agents Chemother. 2016;60(4):2336–2342. doi:10.1128/AAC.03023-15
115. Karageorgopoulos Drosos E, Vouloumanou Evridiki K, Fotinie N, Argyris M, Rafailidis Petros I, Falagas Matthew E. β-D-glucan assay for the diagnosis of invasive fungal infections: a meta-analysis. Clin Infect Dis. 2011;52(6):750–770. doi:10.1093/CID/CIQ206
116. Kidd Sarah E, Chen Sharon CA, Wieland M, Halliday Catriona L, New A. Age in molecular diagnostics for invasive fungal disease: are we ready? Front Microbiol. 2020;10:2903. doi:10.3389/FMICB.2019.02903/BIBTEX
117. Antoni T, Niederman Michael S, Jean C, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur Respir J. 2017;50(3):1700582. doi:10.1183/13993003.00582-2017
118. Kalil Andre C, Metersky Mark L, Michael K, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
119. Shi Y, Huang Y, Tian-Tuo Z, et al. Chinese guidelines for the diagnosis and treatment of hospital-acquired pneumonia and ventilator-associated pneumonia in adults (2018 Edition). J Thorac Dis. 2019;11(6):2581–2616. doi:10.21037/jtd.2019.06.09
120. Boyles Tom H, Adrian B, Calligaro Greg L, et al. Erratum to South African guideline for the management of community-acquired pneumonia in adults. J Thorac Dis. 2018;10(8):E673–E675. doi:10.21037/jtd.2018.07.137
121. Massimo S, Federico C, Yoram K, et al. WSES/GAIS/SIS-E/WSIS/AAST global clinical pathways for patients with intra-abdominal infections. World J Emerg Surg. 2021;16(1):49. doi:10.1186/s13017-021-00387-8
122. Solomkin Joseph S, Mazuski John E, Bradley John S, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the surgical infection society and the infectious diseases society of America. Clin Infect Dis. 2010;50(2):133–164. doi:10.1086/649554
123. Mazuski John E, Tessier Jeffrey M, May Addison K, et al. The surgical infection society revised guidelines on the management of intra-abdominal infection. Surg Infect. 2017;18(1):1–76. doi:10.1089/sur.2016.261
124. Mermel Leonard A, Michael A, Emilio B, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases Society of America. Clin Infect Dis. 2009;49(1):1–45. doi:10.1086/599376
125. Soichi A, Masashi K, Shin K, Hiroshi S, Toshihiko M. The JAID/JSC guidelines for management of infectious diseases 2017 – sepsis and catheter-related bloodstream infection. J Infect Chemother. 2021;27(5):657–677. doi:10.1016/j.jiac.2019.11.011
126. CDC. Guidelines for prevention of catheter-associated urinary tract infections; 2020.
127. NICE guidelines. Urinary tract infection: antimicrobial prescribing; 2018.
128. Massimo S, Xavier G, Hardcastle Timothy C, et al. WSES/SIS-E consensus conference: recommendations for the management of skin and soft-tissue infections. World J Emerg Surg. 2018;13(1):58. doi:10.1186/s13017-018-0219-9
129. Stevens Dennis L, Bisno Alan L, Chambers Henry F, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases Society of America. Clin Infect Dis. 2014;59(2):e10–e52. doi:10.1093/cid/ciu296
130. Alexandra P, Schmid Marie N, Pierre P, et al. Impact of environmental hygiene interventions on healthcare-associated infections and patient colonization: a systematic review. Antimicrob Resist Infect Control. 2022;11(1):38. doi:10.1186/s13756-022-01075-1
131. NHS England and NHS Improvement. Health Technical Memorandum 03–01 Specialised ventilation for healthcare premises Part A: the concept, design, specification, installation and acceptance testing of healthcare ventilation systems; 2021.
132. Tacconelli E. Screening and isolation for infection control. J Hosp Infect. 2009;73(4):371–377. doi:10.1016/j.jhin.2009.05.002
133. Lavallée Jacqueline F, Gray Trish A, Dumville J, Wanda R, Nicky C. The effects of care bundles on patient outcomes: a systematic review and meta-analysis. Implement Sci. 2017;12(1):142. doi:10.1186/s13012-017-0670-0
134. National Institute for Health & Care Excellence (NICE). Surgical site infections: prevention and treatment. NICE. 2022;2019:15.
135. Niels W, Boldingh Quirine JJ, Boermeester Marja A, de Jonge Stijn W. Perioperative care bundles for the prevention of surgical-site infections: meta-analysis. Br J Surg. 2022;109(10):933–942. doi:10.1093/bjs/znac196
136. Evelyn L, Nicolle Lindsay E, Coffin Susan E, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(5):464–479. doi:10.1086/675718
137. Jennifer M, Rogers Mary AM, Krein Sarah L, Fakih Mohamad G, Olmsted Russell N, Sanjay S. Reducing unnecessary urinary catheter use and other strategies to prevent catheter-associated urinary tract infection: an integrative review. BMJ Qual Saf. 2014;23(4):277–289. doi:10.1136/bmjqs-2012-001774
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.