")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Major affective disorders in chronic obstructive pulmonary disease compared with other chronic respiratory diseases
Authors Pothirat C , Chaiwong W , Phetsuk N, Pisalthanapuna S, Chetsadaphan N, Inchai J
Received 16 April 2015
Accepted for publication 4 June 2015
Published 7 August 2015 Volume 2015:10(1) Pages 1583—1590
DOI https://doi.org/10.2147/COPD.S86742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Chaicharn Pothirat, Warawut Chaiwong, Nittaya Phetsuk, Sangnual Pisalthanapuna, Nonglak Chetsadaphan, Juthamas Inchai
Division of Pulmonary, Critical Care and Allergy, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailan
Background: Chronic obstructive pulmonary disease (COPD) and other chronic respiratory diseases (CRDs) have significant impacts on quality of life including psychomotor domain.
Purpose: To evaluate three major affective disorders in subjects with COPD compared with other CRDs and nonill population.
Materials and methods: The Thai version of Mini International Neuropsychiatric Interview (MINI) was used as a diagnostic instrument for three major affective disorders (generalized anxiety disorder, major depressive disorder, and panic disorder) by face-to-face interview in assessing patients with CRDs [COPD, asthma, rhinasthma, all asthma (asthma and rhinasthma), and chronic rhinitis], and nonill subjects. Logistic regression analyses were used to determine the relation between major affective disorders and CRDs adjusting for age, sex, and disease severity.
Results: Major affective disorders were more prevalent in CRDs than nonill groups (adjusted OR =2.6 [95% CI, 1.8-3.9], P<0.001). COPD patients had significantly more generalized anxiety and panic disorder (adjusted OR =4.0 [95% CI, 1.4-11.9], P=0.011, and 4.4 [95% CI, 1.1-18.1], P=0.038, respectively) but not major depressive disorder (adjusted OR =2.7 [95% CI, 0.8-9.0, P=0.105]) than nonill group. Comparing with all asthma, COPD patients had lower occurrence of major depressive and panic disorders (adjusted OR =0.1 [95% CI, 0.0-0.4], P=0.002, and 0.1 [95% CI, 0.0-0.9], P=0.043, respectively). There was no difference in major mood disorders in COPD, rhinasthma, and chronic rhinitis patients. Major affective disorders were not increased by disease severity in COPD.
Conclusion: Major affective disorders were significantly higher in CRDs than nonill population. Generalized anxiety and panic disorders were significantly high in COPD patients. Moreover, major depressive and panic disorders in COPD were significantly lower than all asthma. The prevalence of major affective disorders may not be related to severity of COPD.
Keywords: respiration disorders, asthma, airway obstruction, rhinitis, mood disorders
Introduction
Chronic respiratory diseases (CRDs) including chronic obstructive pulmonary disease (COPD), asthma, and chronic rhinitis have significant public health implications in terms of cost of care as well as in quality of life.1–3 In addition to chronic airflow obstruction, COPD impacts of secondary skeletal muscle dysfunction on exercise capacity and survival are well established.4,5 Affective disorders, generalized anxiety, and depressive symptoms are common in patients with even the mildest form of COPD.6 These are major comorbidities in COPD7–10 and are associated with poor prognosis.9,11 Previous studies reported a high prevalence of mental illness in patients with other CRDs (asthma and rhinitis).12–18 Each of these CRDs has a great impact on psychological health.18 However, the comparisons between psychological impairments associated with COPD and the other CRDs are rarely addressed. Psychological impairments and respiratory health status in Thai adult populations have never been systematically studied. We therefore conducted a study on the prevalence of the three major affective disorders in patients with COPD compared to the other CRDs (chronic rhinitis, asthma, all asthma, and rhinasthma) and the nonill population.
Materials and methods
Study population and design
A cross-sectional survey study was setup to evaluate and compare the prevalence of the three major affective disorders in patients with COPD and other CRDs (asthma, rhinasthma, all asthma, chronic rhinitis) and nonill population. This study was one part of a cross-sectional population-based study setup to identify the prevalence of CRDs in adults older than 40 years living in municipal areas of Chiang Mai province (Chiang Mai Lung Health Study). The sample size was calculated using Slovin’s formula.19 A minimal sample size of 398 was determined with 30% of patients expected to deny the participation; consequently, we planned to enroll ~517 subjects. Selection of the community areas was performed by random-route methodology. The chosen areas were then divided into several blocks based on the geographical area and number of streets, and systematic sampling of households within these randomized blocks was conducted. The subjects who resided in detached houses were randomly selected from every third house within each block, and only one patient was interviewed per household.
The subjects were interviewed face-to-face via a standardized respiratory health questionnaire administered by trained interviewers. The respiratory questionnaire was adapted from the European Community Respiratory Health Survey (ECRHS),20 and included questions on general health, chronic respiratory symptoms, and physician-diagnosed respiratory diseases. All relevant data including age, sex, smoking history, family history of atopic diseases, respiratory symptoms, previous medical history, diagnoses of respiratory diseases, and asthma medication use were reviewed. The subjects were invited to the pulmonary administrative office at Chiang Mai University Hospital to confirm the information by face-to-face interview and physical evaluation by pulmonologists in the study team. Each participant underwent a standard chest radiograph and post-bronchodilator (BD) pulmonary function test according to standard American Thoracic Society (ATS)/European Respiratory Society (ERS) post-BD spirometry.21 Results were reviewed and interpreted by a radiologist and pulmonologists. The spirometric values as % predicted were calculated using National Health and Nutrition Examination Survey (NHANES) III reference equations.22 However, for Asians, a correction factor of 0.88 was applied to the forced vital capacity (FVC) and forced expiratory in first second (FEV1) was predicted.23
Assessment of major affective disorders
The Mini International Neuropsychiatric Interview (MINI) is a standardized clinical diagnostic interview schedule for DSM-IV Axis-I disorders.24 It can be reliably administered by lay interviewers who have appropriate training. The Thai version of MINI (translated from the English version of the MINI, Version 5)25 was used as the “gold standard” diagnostic tool for identifying the presence of three major affective disorders (generalized anxiety disorder, major depressive disorder, and panic disorder) by face-to-face interview in assessing patients with CRDs and the nonill population in this study.
Inclusion and exclusion criteria
Randomly selected subjects who had completed the Thai version of MINI questionnaires were included. Subjects excluded from the study were those with complicated acute respiratory disorders; those with other associated significant physical illnesses such as ischemic heart disease, diabetes mellitus, uncontrolled hypertension, renal failure, hepatic failure, congestive heart failure or carcinoma; and those with a previous history of psychiatric illness. Informed consent was obtained from all participants, and the study was approved by the Ethics Committee of the Faculty of Medicine, Chiang Mai University.
Clinical definitions
Nonill subjects includes subjects with no history of chronic respiratory symptoms, no previous diagnosis of any CRD, normal general physical examination, and a normal chest radiograph. Chronic rhinitis subjects were with recurrent or chronic symptoms of nose blockage, posterior nasal drip, sneezing, or runny nose off and on without fever in the past year. Asthma was defined by a positive history of wheezing in the past year (current wheezer) and receiving asthma medication, post-BD FEV1/FVC >0.7 (for a chronic smoker >5 pack-years) or <0.7 (for a nonsmoker or smokers <5 pack-years), with no pulmonary infiltration, pleural effusion, bronchiectasis, or mass on chest radiographs. Rhinasthma was defined by diagnoses of chronic rhinitis combined with asthma. All asthma population were asthma and rhinasthma subjects. COPD was defined by detection of airflow obstruction based on fixed threshold criterion (a ratio of post-BD forced expiratory volume in the first second to FVC [FEV1/FVC] less than 0.7)1 in chronic smokers >5 pack-years with normal or abnormal chest radiographs compatible with the disease (presence of diffuse pulmonary hyperinflation with flattened diaphragms). The severity of chronic rhinitis, asthma, and COPD was determined using Allergic Rhinitis and Its Impact on Asthma (ARIA),26 Global Initiative for Asthma (GINA),2 and Global Initiative for Chronic Obstructive Lung Disease (GOLD)1 criteria, respectively.
Statistical analysis
Results for numerical values were expressed as mean ± standard deviation (SD) and those for categorical data were expressed as absolute frequencies and percentages. Independent sample t-tests and Fisher’s exact test were used to compare differences between groups with and without respiratory diseases for continuous and categorical data, respectively. The prevalence of three major affective disorders (generalized anxiety disorder, major depressive disorder, and panic disorder) was compared between those with and without respiratory disease using Fisher’s exact test. Logistic regression analyses were used to determine the relation between major affective disorders and CRDs adjusting for age, sex, and disease severity. Results were displayed as adjusted odds ratio (OR) together with 95% confidence interval (CI). P-value <0.05 was considered as statistically significant. All analyses were carried out with the SPSS statistical package, version 16 for Windows (SPSS Inc., Chicago, IL, USA).
Results
The demographic data of all patients are shown in Table 1. A total of 571 participants were interviewed using MINI. Of those, 343 were subjects with CRDs, and 228 were nonill subjects as controls. The mean age and age group >60 years old in CRDs were significantly higher than the nonill group (P=0.002 and 0.005, respectively). Major affective disorder (at least one) was significantly higher in the CRDs group than the nonill group (adjusted OR =2.7, 95% CI, 1.8-3.9). Generalized anxiety disorder was the most common major affective disorder detected in patients with CRDs (17.8%) followed by major depressive (10.8%) and panic (6.7%) disorders.
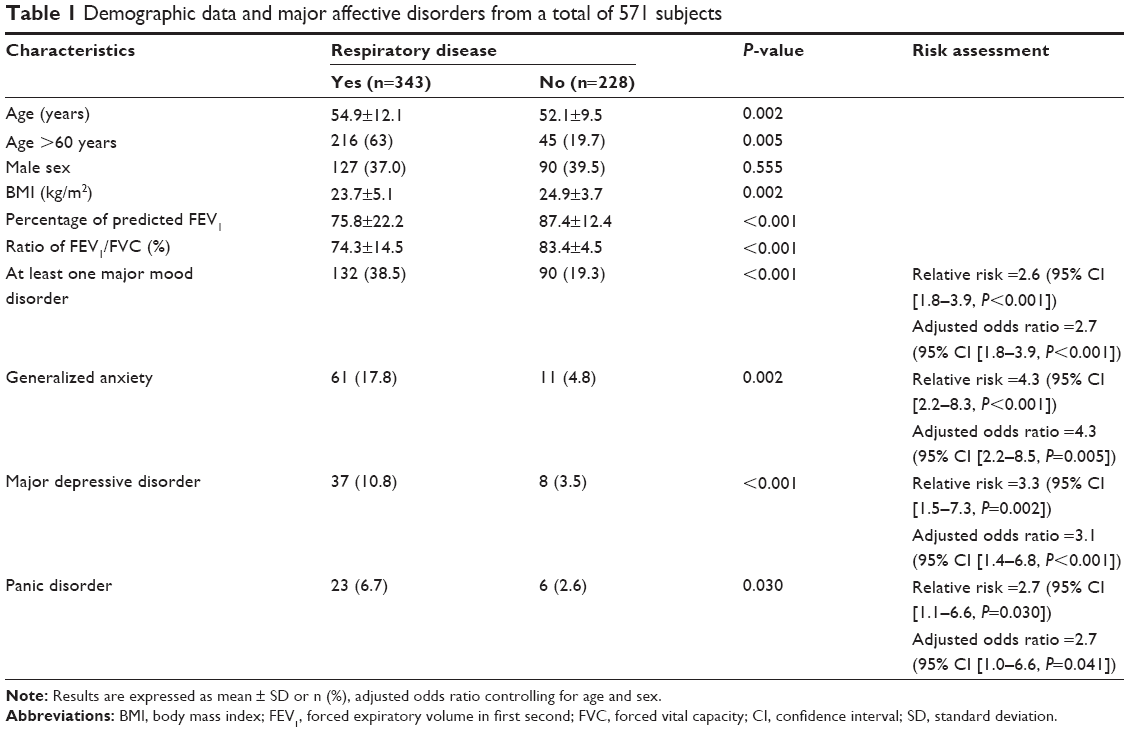 | Table 1 Demographic data and major affective disorders from a total of 571 subjects |
The demographic profile of CRDs subgroups is presented in Table 2. COPD patients were older, predominantly male and had a lower BMI than nonill subjects. All CRD subgroups except chronic rhinitis had significantly lower lung function (percentage of predicted FEV1 and ratio of FEV1/FVC) than the nonill group.
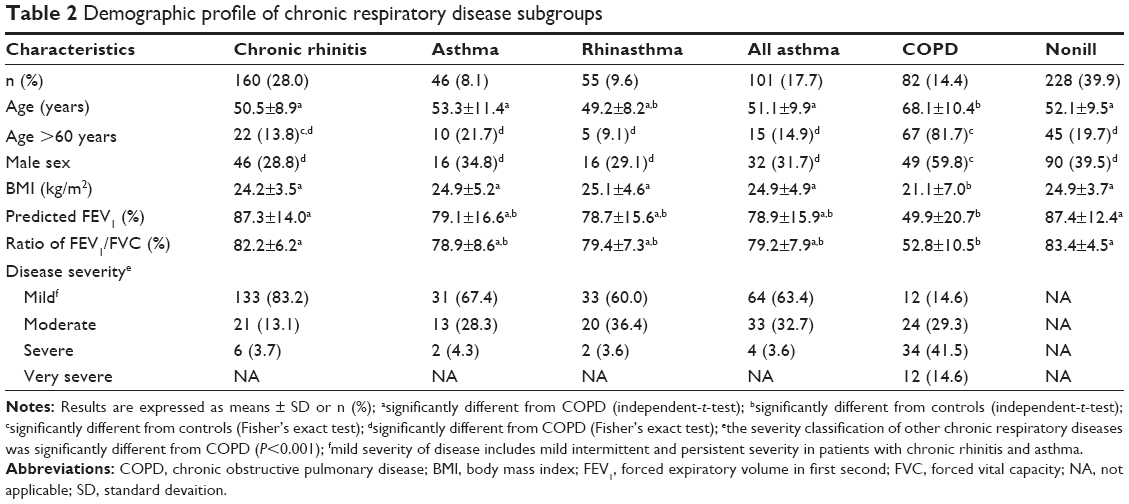 | Table 2 Demographic profile of chronic respiratory disease subgroups |
The odds ratio of major affective disorders adjusted for age and sex in CRDs are presented in Table 3. Generalized anxiety disorder was significantly higher in all CRDs than the nonill group. Major depressive disorder was significantly higher in asthma (P<0.001), rhinasthma (P=0.041), and all asthma (P<0.001). Panic disorder was significantly higher in asthma (P=0.014), all asthma (P=0.018), and COPD (P=0.038). Taken all together, the prevalence of at least one affective disorder was significantly increased in all subgroups of CRDs except COPD.
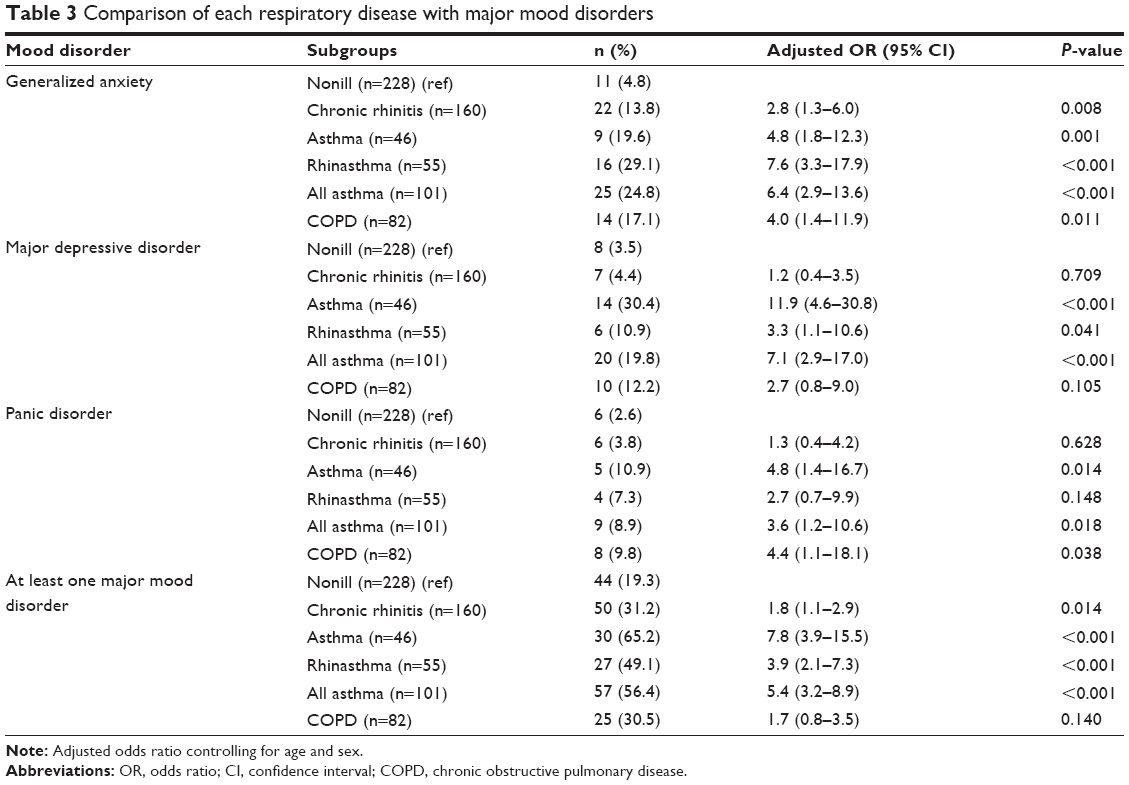 | Table 3 Comparison of each respiratory disease with major mood disorders |
Comparison of major affective disorders in COPD with the other CRDs prior to and after adjustment for age, sex, and severity of disease is demonstrated in Table 4. COPD was associated with a higher prevalence of generalized anxiety, major depressive and panic disorders as compared with the nonill group prior to adjustment for age and sex. However, after adjustment major depressive disorder became insignificant. The prevalence of major depressive disorder in COPD was significantly less than asthma and all asthma (P=0.001 and P=0.002). The prevalence of panic disorders in COPD was significantly less than all asthma (P=0.043). Comparing COPD with rhinasthma and chronic rhinitis, there was no significant difference in prevalence of major affective disorders between them.
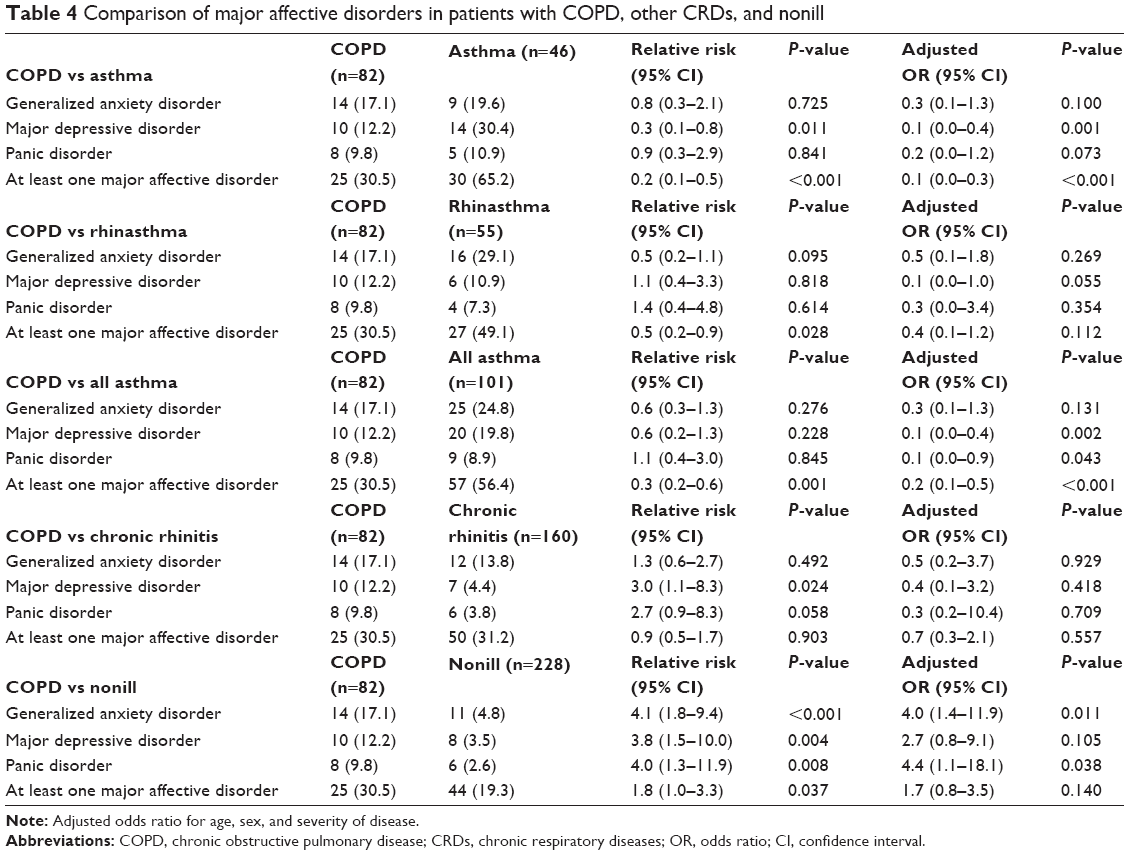 | Table 4 Comparison of major affective disorders in patients with COPD, other CRDs, and nonill |
Table 5 presents a comparison of COPD severity to prevalence of major affective disorders. The prevalence of affective disorders in COPD stages II–IV including generalized anxiety, major depressive disorder, panic disorder, and at least one major mood disorder tended to be increased when compare to COPD stage I; however, they did not reach statistical significances after adjustment for age and sex.
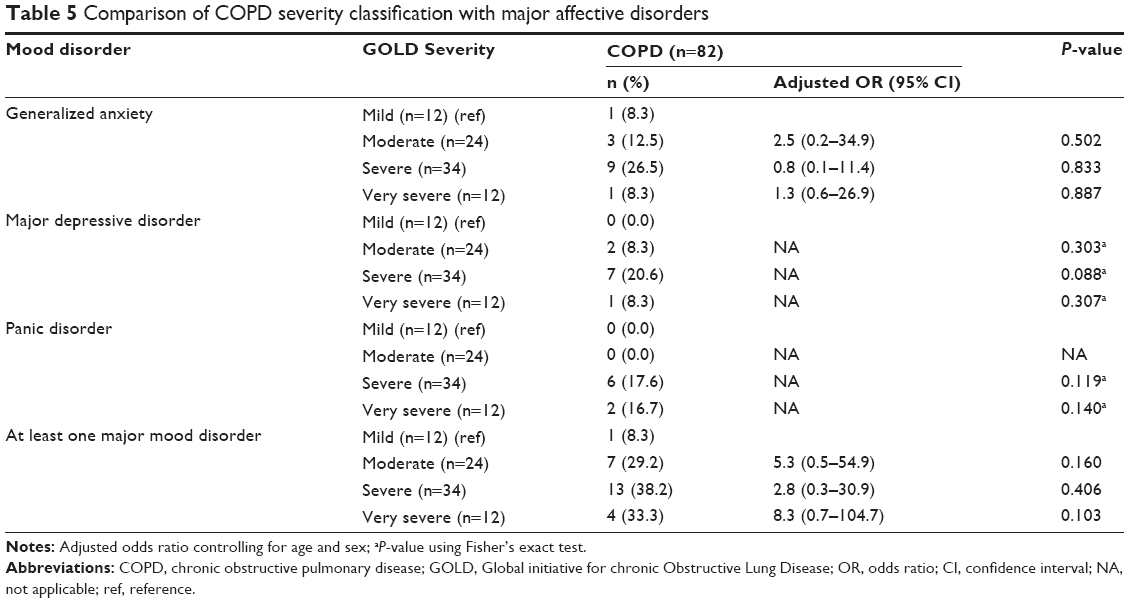 | Table 5 Comparison of COPD severity classification with major affective disorders |
Discussion
COPD was associated with high prevalence of generalized anxiety, major depressive and panic disorders as compared with nonill group, which was similar to previous studies.15,16,18,27 Psychological distress may complicate the course of COPD.28 The more severe the disease (dyspnea, related physical inactivity, and frequent exacerbation), the greater the social isolation, which leads to more fear and depression. Panic-driven responses to dyspnea, a characteristic feature of COPD, have been associated with increased psychopathology in respiratory disorders.29 However, major depressive disorder prevalence was insignificantly different between the COPD and nonill groups after adjustment for age and sex. Due to a lack of in-depth Thai psychological studies to use for comparison, we could not fully explain the reason that major depressive disorder in our COPD subjects was not increased.
Comparing major affective disorders between COPD and other CRDs, a major depressive disorder was more prevalent in those with asthma than COPD. This could be due to the fact that symptoms of COPD and major depressive disorders are very similar and often overlap. Fatigue, decreased interest, lack of energy, sleep disturbance, appetite change, poor concentration, and loss of sexual interest are easily ascribed to COPD unless a formal evaluation is done to screen for affective disorders.30 Psychological stress has been thought to play an important role in asthma as these patients tended to have higher levels of stress and negative emotions such as panic, fear, irritability, and depression.31 Increased psychiatric morbidity in asthma is consistently reported in previous studies32,33 and our study results are consistent with those findings. Asthma was previously thought to be a psychosomatic disease because of the episodic nature in which symptoms would suddenly appear without warning or apparent cause.34 Patients with chronic rhinitis had significantly higher generalized anxiety disorder as compared with the nonill group. Previous studies reported sleep difficulties associated with allergic rhinitis leading to poor quality of life and emotional problems such as irritability, anxiety, and fatigue.35,36 A similar finding of high prevalence of anxiety was reported in a study of allergic rhinitis with bronchial asthma.18,37 Patients with both rhinitis and asthma had higher generalized anxiety disorder than chronic rhinitis or asthma patients. Having both asthma and rhinitis may contribute to an increased likelihood of co-occurring anxiety as suggested by a previous study.38 At least one major mood disorder was observed across all severity classes of COPD and prevalence increased with severity category. Generalized anxiety disorder was prevalent in all COPD severity stages, whereas major depressive and panic disorders were found only in severe to very severe stages. There was no significant difference of severity classification associated with major affective disorders which contrasted to a previous study showing that a higher airflow obstruction is associated with generalized anxiety.16 The explainable reason would be the sample size for this study did not include enough COPD subjects, especially in stages I and IV.
Taken all together, high prevalence of affective disorders in COPD, as well as other CRDs, may be due to various confounding factors. Screening for symptoms of affective mood disorders by simple and quickly validated questionnaires such as MINI during out-patient visits will be helpful in early diagnosis and appropriate treatment or referral.39 While clinical guidelines are well established to diagnose and treat COPD, practice guidelines target isolated diseases and do not encompass comorbidities, presenting a challenge in COPD care.40 Like many chronic diseases, COPD affects multiple aspects of the patient and varies with each patient. Vigilant review of clinical practice guidelines is necessary to optimize evidence-based care. Providers should be alert to the high risk of psychological comorbidities and should screen patients for depression and anxiety upon initial presentation.10 Early recognition, supportive care, and treatment can ease the burden of psychological comorbidities in patients with COPD. A holistic, integrated treatment plan will serve to optimize patient outcomes, decrease the burden of symptoms, prevent/manage exacerbations, slow disease progression, reduce disease morbidity, and overall, improve the quality of life of the patient. In summary, psychological assessment should evolve as a priority in clinical assessment of COPD patients.
The strength of this study is that it was designed as a combination of epidemiological and clinical studies. The results therefore were more informative than either study alone. In our study, all CRDs were optimally investigated prior to diagnosis made by an experienced pulmonologist. The quite large sample size allowed us to examine different categories of CRDs and their affective disorders. However, some limitations of this study should be mentioned. First, the association between medications for CRDs and the further development of affective disorders was not investigated in our study, because the medications varied for each CRD. Further, a clinical study would be required to investigate this association. Second, this study did not provide some information, such as family history, personal life style, education level, socioeconomic status, and environmental factors. Without this information, we were unable to examine their influence of these confounding factors. Third, the quite small number of COPD patients prevented adequate statistical inference for relationships in disease severity and affective disorders.
Conclusion
Major affective disorders were significantly higher in CRDs patients than in nonill population. Generalized anxiety and panic disorders, but not major depressive disorder, were significantly high in COPD. Moreover, major depressive and panic disorders in COPD were significantly lower than the all asthma population. The prevalence of major affective disorders may not be related to severity of COPD.
Acknowledgments
The authors wish to thank the patients who kindly took part in this study and to acknowledge staff members from the Division of Pulmonary, Critical Care and Allergy, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University for their contributions to this study.
Author contributions
The first author developed study design and carried out acquisition and interpretation of data, statistical analysis, manuscript preparation, and critical revision of intellectual content. The remaining authors contributed to acquisition and interpretation of data, revision of the article for important intellectual content, and final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. | ||
Bateman, Hurd SS, Barnes PJ, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31(1):143–178. | ||
Meltzer EO, Blaiss MS, Naclerio RM, et al. Burden of allergic rhinitis: allergies in America, Latin America, and Asia-Pacific adult surveys. Allergy Asthma Proc. 2012;33(suppl 1):S113–S141. | ||
Maltais F, LeBlanc P, Whittom F, et al. Oxidative enzyme activities of the vastus lateralis muscle and the functional status in patients with COPD. Thorax. 2000;55(10):848–853. | ||
Marquis K, Debigare R, Lacasse Y, et al. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166(6):809–813. | ||
Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: the roles of gender and disease severity. Respir Med. 2006;100(10):1767–1774. | ||
Hanania NA, Müllerova H, Locantore NW, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Study Investigators. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am J Respir Crit Care Med. 2011;183(5):604–611. | ||
Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127(4):1205–1211. | ||
Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167(1):60–67. | ||
Maurer J, Rebbapragada V, Borson S, et al; ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 suppl):S43–S56. | ||
Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229–234. | ||
Meltzer EO, Nathan R, Derebery J, et al. Sleep, quality of life, and productivity impact of nasal symptoms in the United States: findings from the Burden of Rhinitis in America Survey. Allergy Asthma Proc. 2009;30(3):244–254. | ||
Kolbe J, Vamos M, Fergusson W, Elkind G, Garrett J. Differential influences on asthma self-management knowledge and self-management behavior in acute severe asthma. Chest. 1996;110(6):1463–1468. | ||
Laszlo G, Nicholson EM, Denison J, Goddard PR. Adverse effect of previous bronchial asthma on disability in chronic airflow obstruction. Lancet. 2000;356(9231):737–738. | ||
Brenes GA. Anxiety and chronic obstructive pulmonary disease: prevalence, impact, and treatment. Psychosom Med. 2003;65(6):963–970. | ||
Spitzer C, Glaser S, Grabe HJ, et al. Mental health problems, obstructive lung disease and lung function: findings from the general population. J Psychosom Res. 2011;71(3):174–179. | ||
Bavbek S, Kumbasar H, Tuğcu H, Misirligil ZJ. Psychological status of patients with seasonal and perennial allergic rhinitis. Investig Allergol Clin Immunol. 2002;12(3):204–210. | ||
Sharma BB, Singh S, Sharma VK, et al. Psychiatric morbidity in chronic respiratory disorders in an Indian service using GMHAT/PC. Gen Hosp Psychiatry. 2013;35(1):39–44. | ||
Cochran W. Sampling Techniques. 3rd ed. New York: John Wiley and Sons Inc; 1977. | ||
Burney PG, Luczynska C, Chinn S, Jarvis D. The European Community Respiratory Health Survey. Eur Respir J. 1994;7(5):954–960. | ||
Miller MR, Hankinson J, Brusasco V, et al; ATS/ERS Task Force. Standardization of spirometry. Eur Respir J. 2005;26(2):319–338. | ||
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159(1):179–187. | ||
Hankinson JL, Kawut SM, Shahar E, Smith LJ, Stukovsky KH, Barr RG. Performance of American Thoracic Society-recommended spirometry reference values in a multiethnic sample of adults: the multi-ethnic study of atherosclerosis (MESA) lung study. Chest. 2010;137(1):138–145. | ||
Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(suppl 20):S22–S33. | ||
Kittirattanapaiboon P, Khamwongpin M. The validity of the Mini International Neuropsychiatric Interview (M.I.N.I.)-Thai version. J Ment Health Thai. 2005;13(3):126–136. | ||
Bousquet J, Khaltaev N, Cruz AA, et al; World Health Organization; GA(2)LEN; AllerGen. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(suppl 86):S8–S160. | ||
Goodwin RD, Pine DS. Respiratory disease and panic attacks among adults in the United States. Chest. 2002;122(2):645–650. | ||
Pembroke TP, Rasul F, Hart CL, Davey Smith G, Stansfeld SA. Psychological distress and chronic obstructive pulmonary disease in the Renfrew and Paisley (MIDSPAN) study. J Epidemiol Community Health. 2006;60(9):789–792. | ||
Freire RC, Perna G, Nardi AE. Panic disorder respiratory subtype: psychopathology, laboratory challenge tests, and response to treatment. Harv Rev Psychiatry. 2010;18(4):220–229. | ||
Cooper CB. Determining the role of exercise in patients with chronic pulmonary disease. Med Sci Sports Exerc. 1995;27(2):147–157. | ||
Nayak AS. The asthma and allergic rhinitis link. Allergy Asthma Proc. 2003;24(6):395–402. | ||
de Miguel Diez J, Hernandez Barrera V, Puente Maestu L, Carrasco Garrido P, Gomez Garcia T, Jimenez Garcia R. Psychiatric comorbidity in asthma patients. Associated factors. J Asthma. 2011;48(3):253–258. | ||
Goral A, Lipsitz JD, Muhsen K, Gross R. Depressive symptoms, risk factors and sleep in asthma: results from a national Israeli Health Survey. Gen Hosp Psychiatry. 2012;34(1):17–23. | ||
Bloomberg GR, Chen E. The relationship of psychologic stress with childhood asthma. Immunol Allergy Clin North Am. 2005;25(1):83–105. | ||
Sardana N, Craig TJ. Congestion and sleep impairment in allergic rhinitis. Asian Pac J Allergy Immunol. 2011;29(4):297–306. | ||
Muliol J, Maurer M, Bousquet J. Sleep and allergic rhinitis. J Investig Allergol Clin Immunol. 2008;18(6):415–419. | ||
Slattery MJ, Essex MJ. Specificity in the association of anxiety, depression, and atopic disorders in a community sample of adolescents. J Psychiatr Res. 2011;45(6):788–795. | ||
Goodwin RD, Jacobi F, Thefeld W. Mental disorders and asthma in the community. Arch Gen Psychiatry. 2003;60(11):1125–1130. | ||
De S. Prevalence of depression in stable chronic obstructive pulmonary disease. Indian J Chest Dis Allied Sci. 2011;53(1):35–39. | ||
Garcia-Olmos L, Alberquilla A, Ayala V, et al. Comorbidity in patients with chronic obstructive pulmonary disease in family practice: a cross sectional study. BMC Fam Pract. 2013;14:11. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.