")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Magnitude of Viral Load Suppression and Associated Factors among Clients on Antiretroviral Therapy in Public Hospitals of Hawassa City Administration, Ethiopia
Authors Anito AA, Lenjebo TL , Woticha E , Solomon F
Received 28 August 2022
Accepted for publication 11 November 2022
Published 18 November 2022 Volume 2022:14 Pages 529—538
DOI https://doi.org/10.2147/HIV.S387787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Abenezer Abraham Anito,1,* Tsegaye Lolaso Lenjebo,2,* Eskinder Woticha,2 Fithamlak Solomon3
1Ohio State University Global One Health Initiative, Addis Ababa, Ethiopia; 2School of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3School of Medical Laboratory, Wolaita Sodo University, Wolaita Sodo, Ethiopia
*These authors contributed equally to this work
Correspondence: Abenezer Abraham Anito, Tel +251-94-142-0184 ; +251-90-201-3026, Email [email protected]
Background: A majority of clients on first-line antiretroviral therapy with an initial high viral load will resuppress following an adherence intervention. Some sociodemographic and clinical characteristics were found to affect resuppression. Few reports on the outcome of the intervention and its associated factors in our country, with inconsistent results and some missed clinical factors of potential association, have compelled this study. The study aimed to assess the proportion of viral load suppression and associated factors among clients on antiretroviral therapy in public hospitals of Hawassa City Administration, Ethiopia.
Methods: An institution-based cross-sectional study with retrospective document review was conducted among 342 participants on antiretroviral therapy enrolled for counseling since its start in November 2016. Data were captured using a pretested and structured checklist from all client charts with complete data, entered into EpiData 3.1.0 and exported to SPSS 27 for analysis. The proportion of viral load suppression was determined. Bivariate and multivariate logistic regressions were performed to identify associated factors. Statistical significance was determined at a 95% CI and P< 0.05.
Results: The proportion of viral load suppression was found to be 40.9% (35.7%– 46.5%). Nevirapine-based antiretroviral treatment regimens (AOR 0.125, 95% CI 0.034– 0.464), malnutrition (AOR 0.565, 95% CI 0.329– 0.971), poor adherence (AOR 0.504, 95% CI 0.287– 0.886), lower CD4 count (AOR 0.149, 95% CI 0.071, 0.314), and fewer counseling sessions (AOR 0.330, 95% CI 0.149– 0.729) were significantly associated with viral load suppression.
Conclusion: The proportion of viral load suppression is lower than that recommended by the World Health Organization. Nevirapine-based regimens, poor nutritional status, poor adherence, lower CD4 count, and fewer counseling sessions risk a lower proportion of viral load suppression. This calls for the need to devise strategies to address these factors and to revisit program implementation.
Keywords: viral load suppression, antiretroviral therapy, enhanced adherence counseling, Hawassa, Ethiopia
Introduction
A major global public health problem, HIV has been made a manageable chronic condition with the use of antiretroviral therapy (ART). Besides the significant reduction in the overall mortality, first ART regimen has offered the best opportunity for viral load (VL) suppression.1,2 As part of global efforts against the burden, the “90–90-90” target aimed for 90% of those on ART to attain VL suppression by 2020 as the third target. Since then, different trends have been seen, among which was an estimated 59% by the end of 2019. Huge disparity was also noted among countries, ranging from 68% (Switzerland) to 7% (China).3,4
VL suppression is a measure of treatment outcome based on which adherence support is provided for the sustained engagement of clients in the care and their adherence. Therefore, VL testing is recommended at 6 and 12 months and then yearly. Based on the results, enhanced adherence counseling (EAC) is provided for those who still have high VL (>1000 cells/mL of blood) after a minimum of 6 months on ART.5–8 With this, a viral suppression rate of 46.1% was reported in a systematic review, though rates have varied from as low as 9% to 58.9% in different countries.8–13 Better yet, around 70% of patients on first-line ART who have an initial high VL will resuppress following such adherence interventions.2 However, in Africa, lower rates of VL suppression from suboptimal monitoring and poor adherence have been seen along with ART drug resistance of relatively higher prevalence estimates (7.2%–11.0%).6,14–16
In Ethiopia, only 65% of people living with HIV were on treatment in 2018. Even worse, data were lacking for the VL suppression target.17 A study in the southwest (using surrogate markers) revealed a 66% suppression rate, making the target unlikely to be attained by the set year 2020, as was also predicted by a study in northern Ethiopia.18,19 Adding to this burden, lower VL-suppression rates after EAC were seen in Bahir Dar (38.7%), in contrast to the substantial rates reported by a study in North Wollo (66.4%).20,21
With regard to factors associated with VL suppression after EAC, age, sex, marital status, occupation, level of education and residence are among the sociodemographic characteristics.2,8,10,12,14,20–28 Clinical factors, nutritional status, duration on ART, ART regimen, WHO clinical stage, adherence, initial CD4 count, initial VL, count and EAC sessions completed have also been reported to have significant associations.7–10,12,14,20–24,27–37 Some important variables of potential association (ie, prophylaxis against opportunistic infections and nutritional status) with VL suppression were not considered in previous studies.
Studies in Ethiopia have been limited as to the knowledge of the researchers, and their reports on outcomes of EAC have also shown inconsistency. In addition to the clinical variables not studied yet, there has been no similar study done in the area, resulting in lack of evidence regarding VL suppression and associated factors among patients receiving EAC intervention. As such, this study aimed to assess the level VL suppression and associated factors among clients on ART in public hospitals of Hawassa City Administration, Ethiopia.
Methods
Study Area and Period
The study was conducted in public hospitals of Hawassa City Administration, Ethiopia. The city administration has three public hospitals and five health centers under it. Among these, all the public hospitals and some of the health centers provide HIV/AIDS treatment and follow-up services. Adare General Hospital (AGH) and Hawassa University Comprehensive Specialized Hospital (HUCSH) have run an EAC program since November 2016. There were a total of 294 clients enrolled for EAC in HUCSH and 272 clients in AGH from 2016 to 2021. The study was conducted from May 24 to June 25, 2021.
Study Design
This was an institution-based cross-sectional study with retrospective document review.
Population
All clients on ART who had been enrolled for follow-up were considered the source population. The study population comprised clients on ART who had been enrolled for EAC. Finally an individual on ART who had been enrolled for EAC from 2016 to 2021.
Eligibility Criteria
Clients on ART enrolled for EAC sessions with high VL (>1000 cells/mL) were recruited. Clients who were lost to follow-up or transferred before completing all three EAC sessions and those who had incomplete records, ie, no second VL result, were excluded from the study.
Sample-Size Determination
The sample size for the first objective of the study (to determine the proportion of VL suppression) was computed with assumptions of 95% CI of 1.96, VL suppression 66.4%,20 and margin of error 5% using OpenEpi, which gave us 342. For calculating the sample size for the second objective of the study which was to identify factors associated with VL suppression, assumptions were 95% CI and 80% power. The proportion of VL suppression (the outcome variable) in the exposed group and unexposed group of associated factors were taken from previous studies20 (Table 1).
 |
Table 1 Sample-size calculation for the second objective of the study |
Sampling Technique
The study participants were taken proportionally from the public hospitals that have been providing EAC since the start of the program based on the number of clients enrolled. All client records fulfilling the inclusion criteria — 179 from HUCSH and 163 from AGH — were included in the final review. As record incompleteness was the challenge during the pilot study, every client with a second VL record was automatically included and further completeness checks undertaken subsequently in order to capture data from other sources, ie, VL registers, EAC registers, and laboratory log books. Finally, all client records with complete information were included in the review.
Data-Collection Tools and Techniques
Identification numbers of medical records for clients started on EAC were obtained from the EAC registers at the ART clinic. By using the identification numbers, medical record charts were drawn by card-room workers. After thorough screening of all the client charts based on the eligibility criteria, trained data collectors identified client charts meeting the inclusion criteria and collected all the required information from only those records. The data-collection form contained both sociodemographic and clinical factors and was completed by chart abstraction. Different registers, follow-up forms, and laboratory results were also used to get the most recent as well as full data for incomplete charts.
Data Quality Control
Two diploma nurses were recruited as data collectors and one supervisor monitored the overall data-collection process. The supervisor and data collectors were trained for 2 consecutive days on the requirements of the protocol and data to be collected. The training also focused on the purpose of the study, familiarization with the tools and further clarity, techniques of data collection and confidentiality, and respective roles and responsibilities. The data-collection form was pretested on 34 client charts retrieved in order to minimize problems with the tool. It was carried out at Bushilo Health Center which was outside the study area. During the data-collection process, both groups were regularly supervised by the principal investigator. Each data-collection form was audited for completeness and legibility at the end of each day by the principal investigator and supervisor to ensure accuracy.
Data Management and Analysis
After the collected data had been checked for consistency and completeness, it was entered into EpiData 3.1.0, then exported to SPSS 27 for analysis. Descriptive statistics, ie, frequencies and percentages, were computed. Binary logistic regression analysis was used to fit each independent variable into a bivariate logistic regression model separately to explore the association with the dependent variable (viral suppression). Independent variables with P<0.25 on bivariate logistic regression analysis were considered for multivariate logistic regression analysis. Hosmer and Lemeshow’s goodness-of-fit test was used to check model fitness. Multivariate logistic regression was carried out to identify factors independently associated with VL suppression. The level of significance was ascertained by OR with 95% CI at P<0.05.
Variables and Measurement
The outcome variable of the study was VL suppression. As a measurement tool, VL is used to identify people on ART in need of an adherence interventions, a majority of which resuppress and are able to continue their treatment after adherence support.36,38 High VL is regarded as >1000 copies/mL of blood and is confirmed 6 months after initiation of ART. VL suppression is said to be attained when the count is ≤1000 copies/mL of blood.7,14,20 Independent variables comprised both sociodemographic (age, sex, marital status, residency, religion, education, and occupation) and clinical characteristics (duration on ART, ART regimen, initial CD4 count, initial VL count, functional status, nutritional status, WHO clinical stage, opportunistic infections at first enrollment, co-trimoxazole preventive therapy, isoniazid preventive therapy, and number of EAC sessions attended).
Enhanced Adherence Counseling
EAC is an intervention provided in monthly sessions for 3 months (EAC 1–3) by an adherence counselor who understand clients’ drug administration, the barriers to adherence (ie, substance abuse), social support (ie, depression evaluation,) and opportunities to improve adherence using the five As (assess, advise, assist, agree, arrange).7,18 It is said to be completed after an optimum level of adherence to treatment for 3 months, when the second VL is determined, but for those with significant barriers to adherence, it is advised to extend the counseling for 6 months.39
Ethics
Ethics clearance was obtained from the Institutional Review Board of College of Health Sciences and Medicine, Wolaita Sodo University. As the study was a retrospective analysis of deidentified data, a waiver of consent was obtained given that it was conducted in accordance with the Declaration of Helsinki.
Results
Baseline Characteristics
Sociodemographic Characteristics
Of the 342 study participants, 101 (29%) were aged 30–39 years and 173 (50.6%) were female. Around half (40.9%) were single and 45.3% had an education of secondary and above. Unemployed participants numbered 133 (38.9%). With regard to residence, a majority (87.7%) resided in urban areas (Table 2).
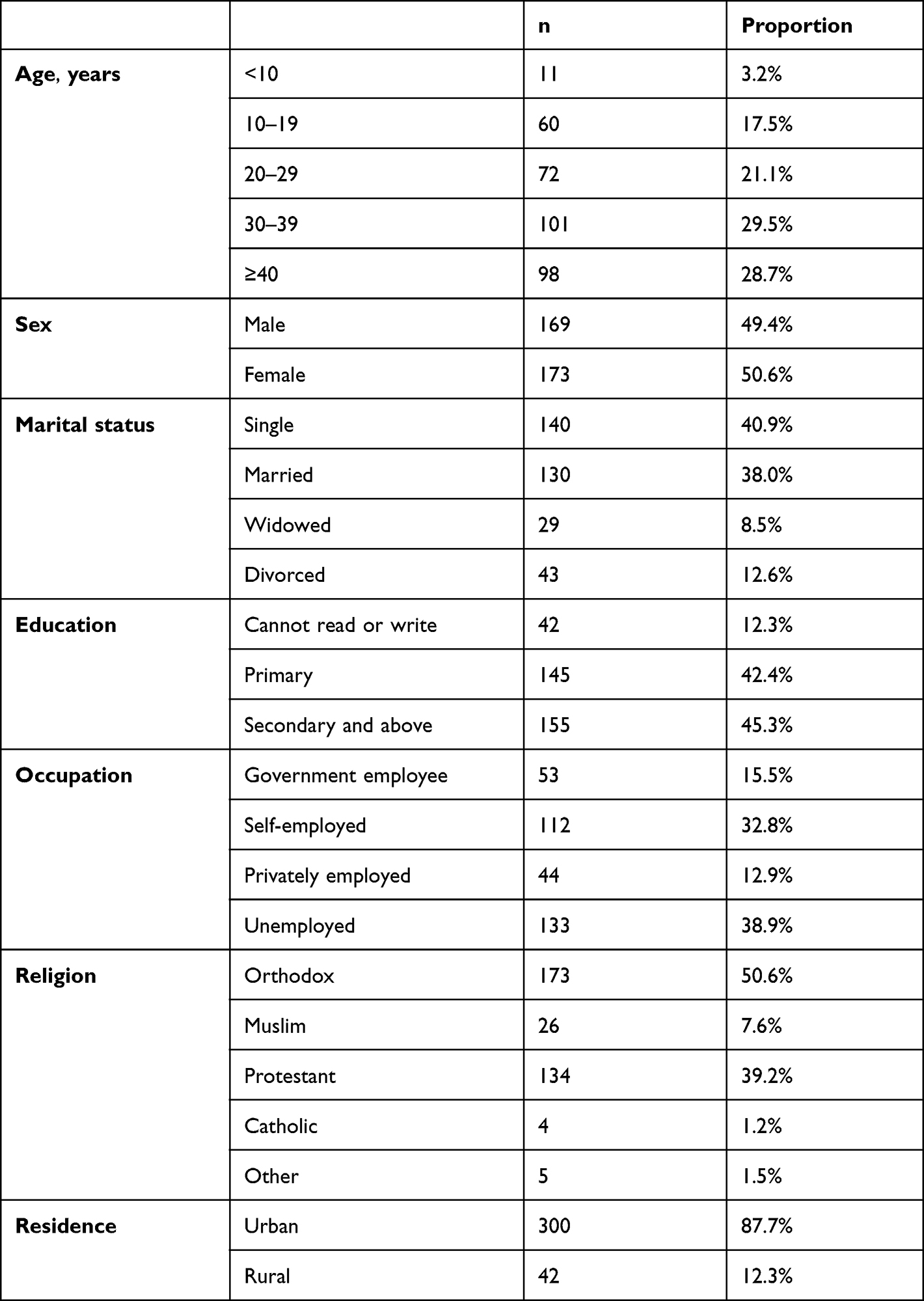 |
Table 2 Sociodemographic characteristics (n=342) |
Clinical Characteristics
Among the 342 participants, 197 (57.6%) had been taking ART medication for ≥5 years. Efavirenz(EFV)-based regimens were the most commonly prescribed (57.3%). At the time of their enrollment for EAC, around 43% of the participants were diagnosed with at least one opportunistic infection and 56.7% had WHO clinical stage 1 illness, 31.6% had CD4 counts <200 cells/mL, and 44.4% had VL >10,000 copies/mL. About two-thirds (63.5%) had good adherence, and most (84.2%) had completed all three sessions of the EAC (Table 3).
 |
Table 3 Clinical characteristics (n=342) |
Factors Associated with Viral Load Suppression among Clients Enrolled for Enhanced Adherence Counseling
On bivariate analysis, marital status, occupation, ART regimen, opportunistic infection, nutritional status, baseline adherence level, initial CD4 and VL count, and EAC sessions attended had P<0.25. After running the multivariate analysis, the ART regimen, nutritional status, baseline adherence level, initial CD4 count, and number of EAC sessions attended were the ones that showed significant associations with VL suppression. Participants on NVP-based ART regimens at the time of EAC enrollment were less likely to have suppressed VL later than those on a protease inhibitor (PI)-based regimen (AOR 0.125, 95% CI 0.034–0.464). Those on an EFV-based regimen at enrollment had a lower probability of VL suppression than those on a PI-based regimen (AOR 0.223, 95% CI 0.063–0.795).
Participants who did not have normal nutritional status had a 43.5% lower probability of resuppressing than those with normal nutritional status (AOR 0.565, 95% CI 0.329–0.971). Poor adherence was also found to decrease the probability of viral suppression by nearly 50% from that among those with good adherence (AOR 0.504, 95% CI 0.287–0.886). Compared to those with a CD4 count ≥500 cells/mL, participants in each group of the decreasing CD4-count categories (350–499, 200–349, <200 cells/mL) showed an increasing significance of association and a lower probability of resuppression (58.3%, 62.5%, and 85.1%, respectively). With regard to EAC sessions attended, it was obvious that those who had attended only one or two of the scheduled sessions had a lower probability of VL suppression than those who had completed them (AOR 0.330, 95% CI 0.149–0.729; Table 4).
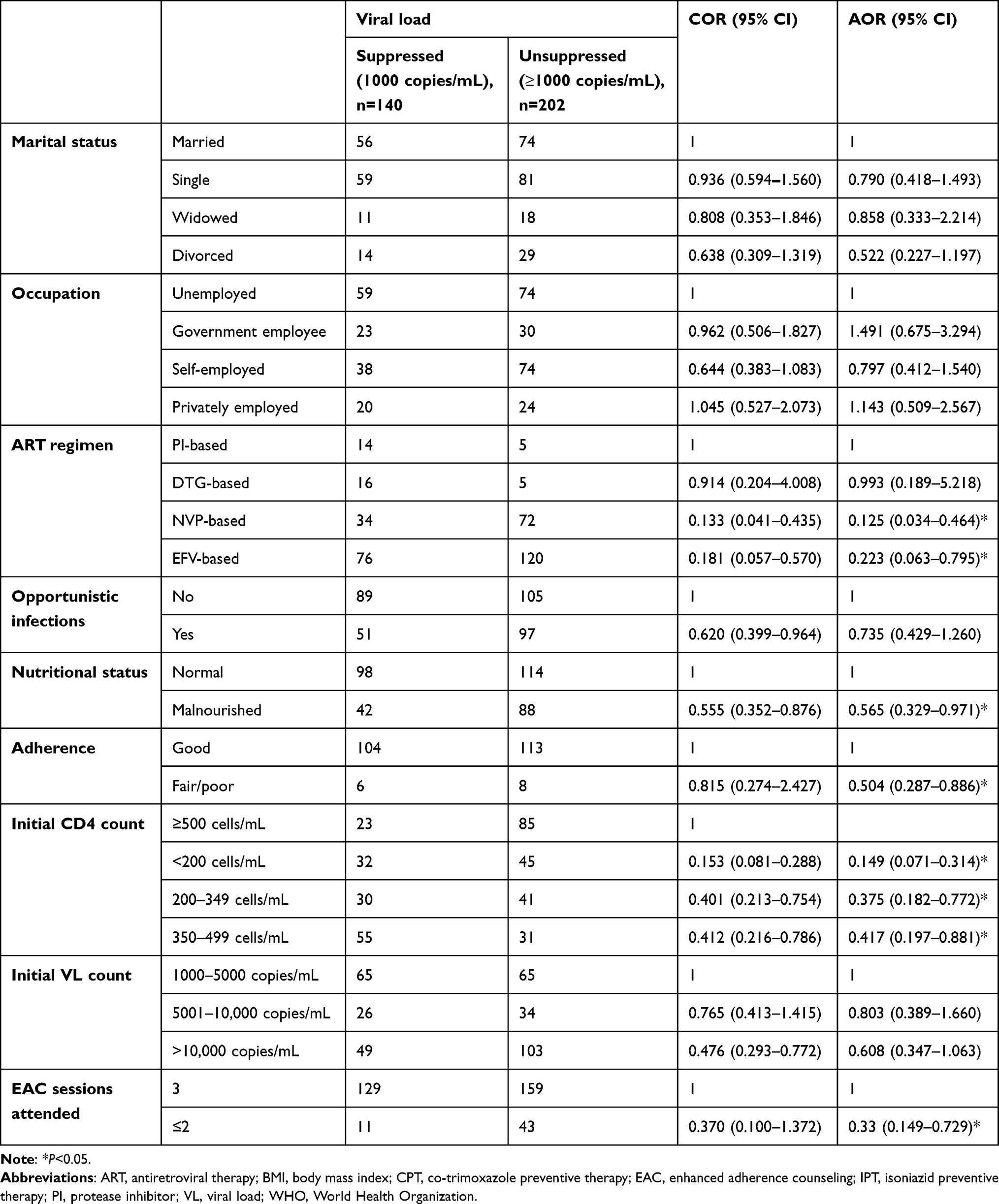 |
Table 4 Sociodemographic and clinical characteristics associated with viral suppression |
Discussion
Findings from the study revealed that VL suppression among clients on ART enrolled for EAC was 40.9% (35.7%–46.5%). Moreover, NVP-based ART regimens, malnutrition, poor adherence, lower CD4 counts, and fewer EAC sessions were significantly associated with VL suppression. Our finding on the proportion of VL suppression reveals a much lower figure than the recommended 70% by the WHO and even the 66.4% reported in North Wollo, Ethiopia.2,20 The disparity with the latter study can be explained by differences in study population, sample size, and the period covered. Consistent results were also seen in a systematic review of mostly African studies (46.1%) and even a similar study done in Bahir Dar, Ethiopia (38.7%).8,21
Despite the fact that our finding stood behind the target recommendation, it is still higher than the 28% seen in India and 10% in Tanzania.11,12 This is possibly due to differences in the study population, a smaller sample (ie, the Tanzanian study, where only around 50 clients who were enrolled for EAC were studied), and the study period. An even lower figure (<10%) from a Ugandan study revealed the existence of mutation in most clients who failed to resuppress.13 This can explain why results from the current study have figures far exceeding that.
NVP- and EFV-based ART regimens showed almost 90% and 77.7% lower probability of VL suppression than the PI-based regimen, respectively. Similarly, a study from UK and Ireland among children revealed durable suppression in those on PI-based regimens than those on non-nucleoside reverse transcriptase inhibitor–based regimens.9 In contrast, our finding stands against a study in Sierra Leone, where a PI-based regimen was associated with failure in VL suppression.30 This can be attributed to the study population, which included adults aged >18 years, who take a PI-based regimen only in special circumstances, making them more liable to other potential factors, ie, adherence problems from pill burden.
Poor nutritional status resulted in a 46% lower probability of resuppression than normal nutritional status. This is supported by findings from a previous study in northeast Ethiopia.29 Participants with poor adherence at the time of EAC enrollment had at least a 50% lower probability of attaining VL suppression following EAC than those with good adherence. Suboptimal adherence has demonstrated similar outcomes in other studies.12,14,21,22,24,29,30,33 Lower CD4 count was associated with failing VL suppression following EAC. As per other studies in Ethiopia, low current and baseline CD4 T-cell count predict failure in VL suppression.21,28,29 This is supported by studies in Sierra Leone and Zimbabwe.30,34 Approximately 70% lower probability of attaining VL suppression was seen among those who had attended only one or two sessions of EAC. Similar results have been reported from studies in Swaziland and Zimbabwe.10,34
Strengths and Limitations
The strength of this study lies basically in the study area, as both public hospitals have been providing the service since the implementation of the EAC program. The large sample is believed to increase the validity of the results. The study also included all age-groups, which makes it sound for analysis and brings a wider range of evidence. Some limitations, ie, capturing data from patients’ charts, made it difficult to find records of exact times. In those cases, even though data collectors tried to use recent data, it is not unlikely that this might have caused some variation in outcomes. The wider range of age-groups, which actually increased the number of participants, including children and adolescents, may also have affected outcomes, as ART regimens, adherence, and other factors, ie, nutritional status, vary among these groups.
Conclusion
The proportion of VL suppression among clients enrolled for EAC is far lower than that recommended by the WHO. NVP-based ART regimens, poor nutritional status, poor adherence, lower CD4 counts, and fewer EAC sessions were identified as risk factors that lower proportion of VL suppression in such clients.
Acknowledgment
We would like to thank the institutions, data collectors, and supervisors for the realization of this study and Wolaita Sodo University for overall facilitation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. HIV/AIDS [Internet]. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. Clinical guidelines: antiretroviral therapy 4.1 Preparing people living with HIV for ART [Internet]. Available from: https://www.who.int/hiv/pub/arv/chapter4.pdf.
3. UNAIDS [Internet]. Accelerating towards 90–90–90. Available from: https://www.unaids.org/en/resources/presscentre/featurestories/2018/july/90-90-90-targets-workshop.
4. Levi J, Raymond A, Pozniak A, Vernazza P, Kohler P, Hill A. Can the UNAIDS 90- 90-90 target be achieved? A systematic analysis of national HIV treatment cascades. BMJ Glob Heal. 2016;1(2):e000010. doi:10.1136/bmjgh-2015-000010
5. Global health sector strategy on HIV 2016–2021 towards ending AIDS [Internet]. Available from: https://apps.who.int/iris/bitstream/handle/10665/246178/WHO-HIV-2016.05-eng.pdf.
6. World Health Organization. The use of antiretroviral drugs for treating and preventing hiv infection; 2016:99–152. Available from: https://apps.who.int/iris/bitstream/handle/10665/208825/9789241549684_eng.pdf?sequence=1&isAllowed=y.
7. Akolo M, Kimani J, Gelmon L. Enhanced adherence counseling 1, 2, 3: our success story in achieving viral suppression in hiv positive key population clients. AIDS Res Hum Retroviruses. 2018;34:260.
8. Ford N, Orrell C, Shubber Z, Apollo T, Vojnov L HIV viral resuppression following an elevated viral load: a systematic review and meta-analysis. J Int AIDS Soc. 2019;22:e25415.
9. Childs T, Shingadia D, Goodall R, et al. Outcomes after viral load rebound on first-line antiretroviral therapy in HIV-infected children in the UK/Ireland: an observational cohort study on behalf of the CHIPS Steering Committee. Lancet HIV. 2015;2(4):e151–e158. doi:10.1016/S2352-3018(15)00021-1
10. Etoori D, Ciglenecki I, Ndlangamandla M, et al. Successes and challenges in optimizing the viral load cascade to improve antiretroviral therapy adherence and rationalize second-line switches in Swaziland. J Int AIDS Soci. 2018;21(10):e25194. doi:10.1002/jia2.25194
11. Laxmeshwar C, Acharya S, Das M, et al. Routine viral load monitoring and enhanced adherence counselling at a public ART centre in Mumbai, India. PLoS One. 2020;15(5):e0232576. doi:10.1371/journal.pone.0232576
12. Kroidl A, Burger T, Urio A, et al. High turnaround times and low viral resuppression rates after reinforced adherence counselling following a confirmed virological failure diagnostic algorithm in HIV-infected patients on first-line antiretroviral therapy from Tanzania. Trop Med Int Health. 2020;25(5):579–589. doi:10.1111/tmi.13373
13. Birungi J, Cui Z, Okoboi S, et al. Lack of effectiveness of adherence counselling in reversing virological failure among patients on long-term antiretroviral therapy in rural Uganda. HIV Med. 2019;21(1):21–29.
14. Bulage L, Ssewanyana I, Nankabirwa V, et al. Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014-July 2015. BMC Infect Dis. 2017;17(1). doi:10.1186/s12879-017-2428-3
15. Gregson J, Gupta RK, Gregson J, et al. HIV-1 drug resistance before initiation or re-initiation of first-line antiretroviral therapy in low-income and middle-income countries: a systematic review and meta-regression analysis. Artic Lancet Infect Dis. 2018;18:346–355. doi:10.1016/S1473-3099(17)30702-8
16. Cc I, Shahmanesh M, Koole O, et al. Clinical outcomes after first-line HIV treatment failure in South Africa: the next cascade of care on behalf of the H-DREAM Network. HIV Med. 2020;21(7):457–462.
17. Ethiopia. UNAIDS. Available from: https://www.unaids.org/en/regionscountries/countries/ethiopia.
18. Desta AA, Woldearegay TW, Futwi N, et al. HIV virological non-suppression and factors associated with non-suppression among adolescents and adults on antiretroviral therapy in northern Ethiopia: a retrospective study. BMC Infect Dis. 2021;20(1):4. doi:10.1186/s12879-019-4732-6
19. Gesesew HA, Ward P, Woldemichael K, Mwanri L. HIV care continuum outcomes: can Ethiopia meet the UNAIDS 90- 90-90Targets? Ethiop J Health Sci. 2020;30(2):179–188. doi:10.4314/ejhs.v30i2.5
20. Diress G, Dagne S, Alemnew B, Adane S, Addisu A. Viral load suppression after enhanced adherence counseling and its predictors among high viral Load HIV seropositive people in North Wollo Zone Public Hospitals, Northeast Ethiopia, 2019: retrospective Cohort Study. AIDS Res Treat. 2020;2020. doi:10.1155/2020/8909232
21. Genet A, Mekonnen Z, Yizengaw E, Mekonnen D. First line antiretroviral treatment failure and associated factors among people living with HIV in northwest Ethiopia. Afr Health Sci. 2021;21(1):263–272. doi:10.4314/ahs.v21i1.34
22. Gebrehiwet Hailu G, Gebregziabher Hagos D, Kahsay Hagos A, Gebreyesus Wasihun A, Asmelash Dejene T. Virological and immunological failure of HAART and associated risk factors among adults and adolescents in the Tigray region of Northern Ethiopia. PLoS One. 2018;13. doi:10.1371/journal.pone.0196259
23. Billioux A, Nakigozi G, Newell K, et al. Durable suppression of HIV-1 after virologic monitoring-based antiretroviral adherence counseling in Rakai, Uganda. PLoS One. 2015;10(5):e0127235. doi:10.1371/journal.pone.0127235
24. Maina EK, Mureithi H, Adan AA, Muriuki J, Lwembe RM, Bukusi EA. Incidences and factors associated with viral suppression or rebound among HIV patients on combination antiretroviral therapy from three counties in Kenya. Int J Infect Dis. 2020;97(97):151–158. doi:10.1016/j.ijid.2020.05.097
25. Nelson JA, Kinder A, Johnson AS, et al. Differences in selected HIV care continuum outcomes among people residing in Rural, Urban, and Metropolitan Areas-28 US Jurisdictions. J Rural Heal. 2018;34(1):63–70. doi:10.1111/jrh.12208
26. Kiweewa IF, Esber A, Musingye E, et al. HIV virologic failure and its predictors among HIV-infected adults on antiretroviral therapy in the African Cohort Study. PLoS One. 2019;14(2):e0211344. doi:10.1371/journal.pone.0211344
27. Jobanputra K, Parker L, Azih C, et al. Factors associated with virological failure and suppression after enhanced adherence counselling, in children, adolescents and adults on antiretroviral therapy for HIV in Swaziland. PLoS One. 2015;10(2):e0116144. doi:10.1371/journal.pone.0116144
28. Bayu B, Tariku A, Balcha Bulti A, Ayanaw Habitu Y, Derso T, Fetene Teshome D. Determinants of virological failure among patients on highly active antiretroviral therapy in University of Gondar Referral Hospital, Northwest Ethiopia: a case–control study. HIV/AIDS Res Palliat Care. 2017;Volume 9:153–159. doi:10.2147/HIV.S139516
29. Ahmed M, Merga H, Jarso H. Predictors of virological treatment failure among adult HIV patients on first-line antiretroviral therapy in Woldia and Dessie hospitals, Northeast Ethiopia: a case-control study. BMC Infect Dis. 2019;19(1):305. doi:10.1186/s12879-019-3924-4
30. Lakoh S, Jiba DF, Vandy AO, et al. Assessing eligibility for differentiated service delivery, HIV services utilization and virologic outcomes of adult HIV-infected patients in Sierra Leone: a pre-implementation analysis. Global Health Action. 2021;14(1). doi:10.1080/16549716.2021.1947566
31. Scale-up of HIV Viral Load Monitoring. Seven Sub-Saharan African Countries [Internet]. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6446a3.htm.
32. How to Optimize HIV Treatment. Treatment, care, and prevention for people with HIV. Clinicians HIV CDC. Available from: https://www.cdc.gov/hiv/clinicians/treatment/treatment-clinicians.html.
33. Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM. Adherence to antiretroviral therapy and virologic failure a meta-analysis. Medicine. 2016;95:e3361.
34. Bvochora T, Satyanarayana S, Takarinda KC, et al. Enhanced adherence counselling and viral load suppression in HIV seropositive patients with an initial high viral load in Harare, Zimbabwe: operational issues. PLoS One. 2019;14(2):e0211326. doi:10.1371/journal.pone.0211326
35. Lejone TI, Ringera I, Cheleboi M, et al. The treatment cascade in children with unsuppressed viral load-a reality check in Rural Lesotho, Southern Africa. J Acquir Immune Defic Syndr. 2018;77(3):250–256. doi:10.1097/QAI.0000000000001597
36. Nasuuna E, Kigozi J, Babirye L, Muganzi A, Sewankambo NK, Nakanjako D. Low HIV viral suppression rates following the intensive adherence counseling (IAC) program for children and adolescents with viral failure in public health facilities in Uganda. BMC Public Health. 2018;18(1):1048. doi:10.1186/s12889-018-5964-x
37. Garone DB, Conradie K, Patten G, et al. High rate of virological re-suppression among patients failing second-line antiretroviral therapy following enhanced adherence support: a model of care in Khayelitsha, South Africa. Afr J HIV Med. 2013;14(4):166–169. doi:10.4102/sajhivmed.v14i4.51
38. Bonner K, Mezochow A, Roberts T, Ford N, Cohn J, Bonner K. Viral load monitoring as a tool to reinforce adherence: a systematic review MSF Field research citation viral load monitoring as a tool to reinforce adherence: a systematic review viral load monitoring as a tool to reinforce adherence: a systematic review. J Acquir Immune Defic. 2013;64(1):74–78.
39. FMOH FMOH. National Comprehensive HIV Prevention, Care and Treatment Training for Health Care Providers Participant Manual. Ministry of Health; 2017.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.