")
Back to Journals » International Journal of Women's Health » Volume 13
Magnitude of Unintended Pregnancy and Associated Factors Among Pregnant Women in Debre Markos Town, East Gojjam Zone, Northwest Ethiopia: A Cross-Sectional Study
Authors Nigussie K , Degu G, Chanie H, Edemealem H
Received 12 August 2020
Accepted for publication 15 December 2020
Published 28 January 2021 Volume 2021:13 Pages 129—139
DOI https://doi.org/10.2147/IJWH.S275346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Kumneger Nigussie,1 Genet Degu,1 Habtamu Chanie1 ,† Hayimro Edemealem2
1Department of Midwifery, College of Health Science, Debre Markos University, Debre Markos, Ethiopia; 2Department of Statistics, College of Natural and Computational Science, Debre Markos University, Debre Markos, Ethiopia
†Mr Habtamu Chanie passed away on April 27, 2020
Correspondence: Kumneger Nigussie
Department of Midwifery, College of Health Science, Debre Markos University, P.O. Box 269, Debre Markos, Ethiopia
Tel +251939636117
Email [email protected]
Background: Unintended pregnancy is an important public health concern in both developing and developed countries due to its serious consequences for women, infants, families and communities, including the risk of unsafe abortion, delayed prenatal care, poor maternal mental health, poor child health outcomes and unemployment.
Objective: The aim of the study was to assess the prevalence and associated factors of unintended pregnancy among pregnant women in the town of Debre Markos in 2019.
Methods: The magnitude and associated factors of unintended pregnancy were assessed using a community-based cross-sectional study design. A multi-stage sampling technique was used to select five Kebeles (basic administrative units), and households were selected from the selected Kebeles using simple random sampling. A total of 580 samples were collected through standardized pretested questionnaires. Bivariate and multivariate logistic regression were used to analyze the relationship between the UP and independent variables.
Results: Of the pregnant women, 202 (34.8%) (95% CI: 30.9– 38.7) participants had an unintended current pregnancy; of those 144 (24.8%) were mistimed pregnancies. Women aged 24 years were three times more likely to have an unintended pregnancy than those aged 35 years. Divorced and widowed women were four times more likely than women who were currently married to experience an unintended pregnancy. Gravidity 1– 2 and 3– 4 were 94% and 86% less likely than gravidity > 5 to experience an unintended pregnancy, and women who made family planning decisions on their own were less likely to have an unintended pregnancy.
Conclusion: According to this study, the prevalence of unintended pregnancy was 34.8% and unintended pregnancy was significantly correlated with women’s age, marital status, gravidity and who made decisions on family planning. There is an obvious need to devise communication strategies on fertility and contraceptive issues between couples through peer education, and to encourage correct use of long-acting modern methods of family planning.
Keywords: mistimed pregnancy, unintended pregnancy, unwanted pregnancy, women
Background
An unintended pregnancy is an unwanted or mistimed pregnancy. A mistimed pregnancy occurs in women who conceived sooner or later than the desired time. An unwanted pregnancy happens in women who do not want any more children at the time of conception.1,2 Unintended pregnancy (UP) is a health problem in developed and middle- and low-income countries.3 Most unintended pregnancies are caused by non-use and/or failure of contraceptives, low chance of women’s autonomy in different aspects and less commonly from rape,4 which indicates that UP can be prevented by proper use of contraceptives.
Unintended pregnancy is a health issue worldwide. The magnitude and effect of unintended pregnancy is a question for all societies and countries around the world.5 Worldwide, 38% of pregnancies are unintended every year.6
Globally, out of 213 million pregnancies in 2012, 85 million were unwanted, 50% of which resulted in abortion, many of which occurred with inappropriate procedures and/or in unsafe conditions. Andalso, these pregnancies resulted in 13% miscarriage and 38% unplanned births, putting a huge strain on health systems. The unintended pregnancy rate is significantly higher in the United States than in many other developed countries and it is 36% higher in developing countries than developed countries. In Africa, from a total of 49.1 million pregnancies, 39% were unintended pregnancies. In sub-Saharan Africa, it is estimated that 14 million unwanted pregnancies occur every year.7–9
Unintended pregnancies often occur outside marriage in Africa (22.5%),10 where premarital sex is not recognized. This results in illegal, unsafe abortions (4.7–13.2%)11 performed under unhygienic conditions by people without the requisite expertise and in locations that do not meet minimum medical standards.12
Maternal and child health indicators in Ethiopia show considerable room for improvement. The health care that a woman receives during pregnancy, at the time of delivery and soon after delivery is important for the survival and well-being of both the mother and the child. Pregnancy planning allows women to better control their life trajectory and contributes to the future child’s health and development.13
Unintended pregnancy is affected by many factors and varies from country to country. Factors include religion, sex without effective contraception, sexual harassment, poor sexual contact among partners, lower economic status, promiscuity, fear of hormonal contraceptives, low maternal education, unmarried status, age, use of substances, number of children and residence.14 Unintended pregnancy is such a terrible outcome. It affects the health, economic, and social status, and also affects the family, community, and the whole world. Some unintended pregnancy complications raise the risk of morbidity and mortality in both the mother and child. These include unplanned childbearing with low birth weight infants, delayed prenatal care, reduced likelihood of breastfeeding, low educational and behavioral outcomes of the child, poor maternal relationship with the child, women suffering physical violence during and after pregnancy, strain, and other related pregnancy factors.15
Induced abortion is a common result of UP and is most of the time clandestinely conducted with significant negative consequences including shock, organ failure, potential reproductive complications and HIV infection. In addition, a country’s economy can also be impacted by the poor health outcome in both maternal and child care.16
Many programs promoting the acceptability of avoiding, delaying, spacing and limiting childbearing by providing different modern family planning methods, increasing provision of high-quality and youth-friendly services for adolescents and increasing the sense of urgency among girls and women to exert control over their lives and make their own decisions have been designed and try to intervene to reduce unintended pregnancy rates.17 The problem of unintended pregnancy in the community is critical, but it is under-reported due to the fact that the legal, social, and cultural norms are not open to discussing the sensitive issue of unintended pregnancies followed by abortion.
Few studies have been conducted to determine the prevalence and associated factors of unintended pregnancy in the Amhara region, particularly in the East Gojjam Zone, and most studies have been based on facilities. Also, the studies in Ethiopia were studied more than five years ago. Therefore, further research is required to satisfy this information gap and attempt to intervene in order to minimize and avoid this problem. This study was therefore conducted from March 1 to April 15, 2019 to determine the magnitude and associated factors of unintended pregnancy among pregnant women in Debre Markos town.
Methods
Description of Study Area
The study was conducted in Debre Markos town. Debre Markos is located on the Addis Ababa to Bahir Dar main road. It is located 300 km from Addis Ababa and 265 km from Bahir Dar. It has 1 referral hospital, 3 governmental health centers, 7 health posts, 16 private pharmacies, 22 private clinics, 2 diagnostic laboratories and 12 traditional healer service providers. There are 7 Kebeles (basic administrative units) in Debre Markos town.
Study Design and Study Period
The community-based cross-sectional study was employed to retrieve relevant information in Debre Markos town. The study was conducted from March 1–April 15, 2019.
Sources and Study Population
The sources of the population for the study were all pregnant women who registered with health extension workers. During the study period in 2019, Kebeles were selected from the study population at Debre Markos town.
Sample Size Determination
The sample size was determined using the formula for a single population proportion taking a prevalence estimate of 23.5% from a previous research conducted in Debre Brehan town.19 Assuming 95% confidence interval and margin of error 5% (d = 0.05), the total sample size was calculated including 5% non-response rate and multiplied by two (design effect).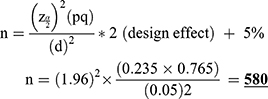
Sampling Technique
A two-stage sampling technique was applied to select the study samples from the seven Kebeles. At the first stage, five Kebeles were selected by using a simple random sampling technique (lottery method). This sample involved 20% and above of the study population to be represented in the sample. A list of pregnant women was made by the health extension workers. Health extension workers visit house to house at least once in the week and register all pregnant women. In the second stage, pregnant women in the household were selected by using a simple random sampling method (lottery method) from the sampling frame.
Inclusion and Exclusion Criteria
All pregnant women who registered with health extension workers in the selected Kebeles who lived in Debre Markos town for at least six months were included. Women who were deaf, dumb and mentally disabled were excluded.
Study Variables
Dependent Variable
Unintended pregnancy of pregnant women.
Independent Variables
Socio-demographic factors (age, marital status, place of residence and number of children), socioeconomic factors (occupation, level of education, income), obstetric factors (number of children, parity, gravidity, and bad obstetric history), behavioral factors (use of alcohol, cigarettes, khat and other substances), factors related to contraception (awareness and use of contraceptives, spousal communication, women’s autonomy on family planning (FP) and husband disapproval on FP).
Data Collection Instrument and Procedure
The questionnaire was prepared by reviewing previous studies. It was first prepared in English and translated to Amharic and again translated back to English by language experts. Data were collected by four BSc and three diploma midwifery professionals in a face to face interview using structured and pre-tested questionnaires. For additional details, please refer to the Supplementary Material: Study Questionnaire.
Data Quality Control
Pre-testing was done on 29 participants from Kebele three and these samples were included in the final sample. Training was given for the data collectors and supervisor before the actual data collection. The training covered the aim of the study, procedure, inclusion and exclusion criteria, data collection technique going through the questionnaires, one by one, the art of interviewing, a way of collecting the data, and clarification. Moreover, during data collection, the supervisors checked how the data collection process was progressing. At the end of each data collection day, the principal investigator and supervisors also checked the completeness of filling questionnaires. Every questionnaire was checked before data entry by the principal investigator.
Data Processing and Analysis
All collected data were checked for completeness, coded and entered into Epi-data 3.14 and SPSS version 20 statistical software was used to analyze the data. Bivariable analysis was carried out to check the relation between the independent variables and the outcome variables. In order to evaluate the independent predictor of unintended pregnancy, all explanatory variables associated with the outcome variable in bivariable analysis were used in multivariable logistic regression. For bivariable analysis, P-values of less than or equal to 0.2 were considered a cut-off point for statistical significance. The odds ratio with confidence interval 95% and P-value 0.05 was used to assess the relationship between the amount and direction of the variables and unintended pregnancy.
Operational Definition
Unintended pregnancy: Is the combination of unwanted and mistimed at the time of conception.
Mistimed pregnancy: A woman does not want to become pregnant at the time of conception but will want to become pregnant in the future.
Unwanted pregnancy: A woman does not want to become pregnant at conception and at any time in the future.
Short gap: The gap between consecutive births less than 2 years.
Women’s autonomy: The capacity and freedom of a woman to act independently on her own without needing the authority of others; for example, the ability to go to places alone, such as visiting health facilities or the market without asking anyone’s permission, making decisions regarding contraceptive use or household purchases.
Alcohol use: Any unit of home brewed (e.g. Tela, Teje, Areka) as well as fabricated alcoholic beverages used during pregnancy.
Khat use: Any amount of khat use during pregnancy period
Results
Socio‐Demographic and Economic Characteristics
A total of 580 participants were interviewed with a 100% response rate. Of the total respondents 355 (61.2%) were between the ages of 25–34 years, 439 (75.7%) were currently married, and 529 (91.2%) were residing in urban areas. In addition, the majority of the study participants had college and above education level 249 (42.9%), and 204 (35.2%) were housewives, followed by 146 (25.2%) government employees. Nearly all of the respondents were Amhara (545; 94.0%), and 504 (86.9%) were adherents of orthodox religion.
With respect to monthly income, more than one-fourth of respondents (160; 27.6%) reported 2001–3000 birr, and 73 (12.6%) reported less than 500 birr monthly income. A total of 416 (71.7%) went to the health facility to receive various health services, of which 366 (88.0%) took less than 40 minutes (Table 1).
 |
Table 1 Socio-Demographic and Socioeconomic Characteristics of Pregnant Women in Debre Markos Town (N=580) |
Reproductive (Obstetrics) History of Respondents
Of the total participants, 362 (62.4%) were 1–2 times pregnant with the current one and 272 (46.9%) were 1–2 times parity. Nearly half of the 276 (47.6%) respondents had 1–2 living children (Table 2).
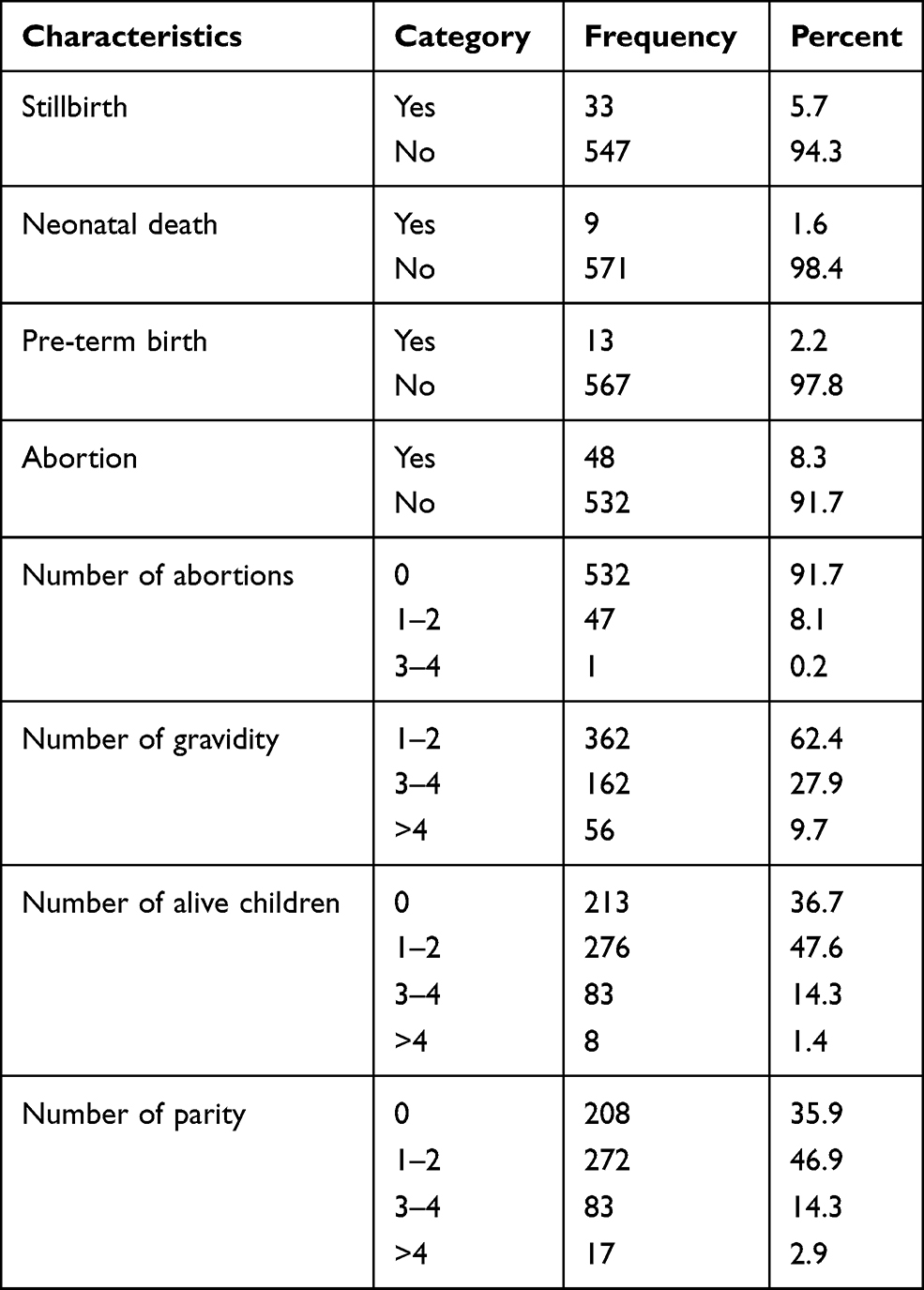 |
Table 2 Reproductive (Obstetric) History of Pregnant Women in Debre Markos Town (N=580) |
Of the total number of participants (580) in this study, 378 (65.2%) wanted and had planned for the current pregnancy, while 202 (34.8%) of respondents indicated that their current pregnancy was unintended (Figure 1). The major reason for unintended pregnancy was not having enough money to take care of the baby and a short gap from previous births, 49 (24.3%) and 47 (23.3%), followed by 45 (22.3%) not in a marriage, respectively. Sixty-five (36.7%) reported that they used contraception either incorrectly or had a method failure to avoid unintended pregnancy, followed by 46 (23.1%) failing to take contraception on time, 27 (15.3%) for fear of side effects and 21 (11.9%) for fear of going to a clinic (Table 3).
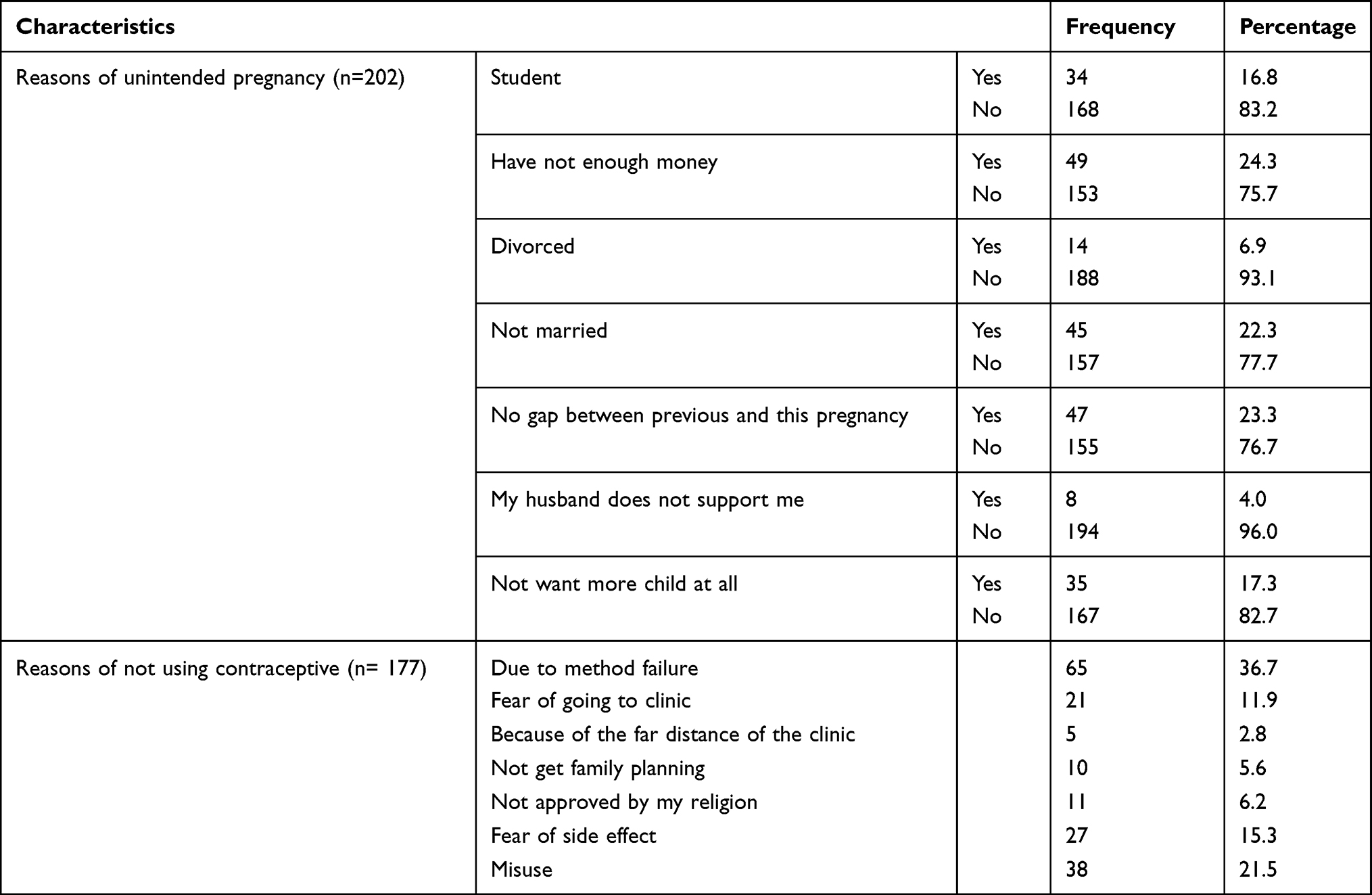 |
Table 3 Reasons of Unintended Pregnancy and Not Using FP in Debre Markos Town (N= 202) |
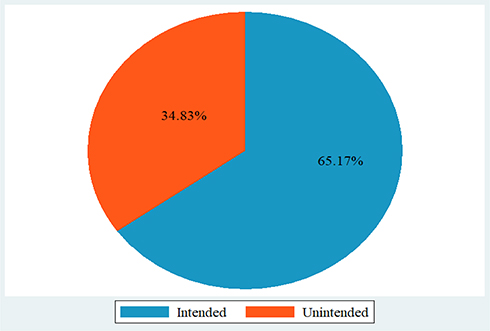 |
Figure 1 Pregnancy intention among pregnant women, in Debre Markos town. |
Behavioral Characteristics of Respondents
From all respondents, 14.1% had used a substance at the time of the survey, of which 79.3% had used alcohol, 14.6% had used khat, 8.5% used another substance and 100% of the women did not use cigarettes or view pornographic material (Table 4).
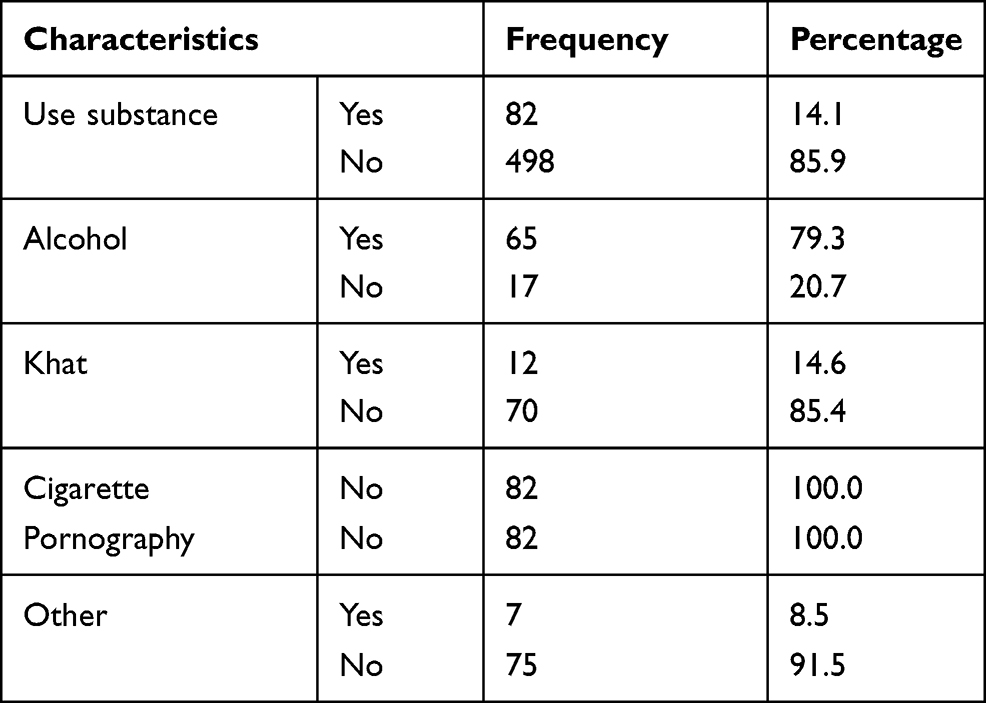 |
Table 4 Behavioral Characteristics of Pregnant Women in Debre Markos Town |
Knowledge and Practice on Contraceptive Use
With regard to contraceptives, about 568 (98%) of participants were aware of contraceptive methods; among them, the most common methods were injectable (96.7%) and pills (92.3%) (Figure 2). Modern female contraceptive practice was used by 414 (71.4%), among which the most widely used contraceptive is injectable (46.1%) and implants (31.6%) (Figure 3). With respect to decision-making, spousal communication and FP approval, most of them (226; 54.7%) discussed and agreed decisions together with their husbands, followed by 187 (45.3%) just women.
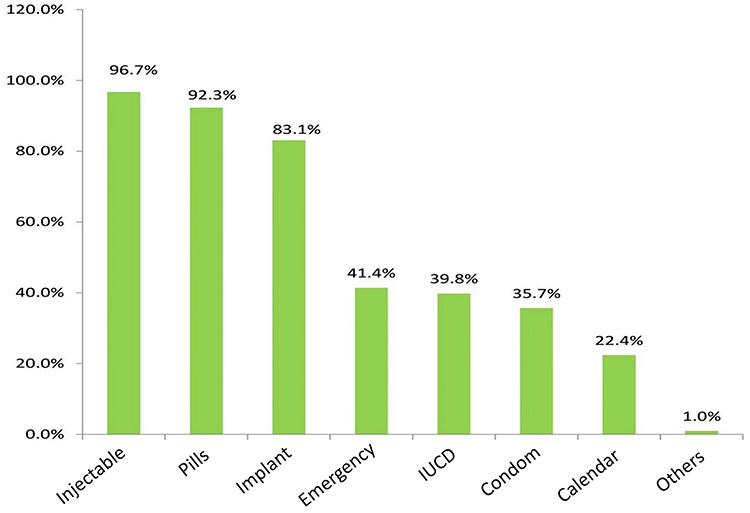 |
Figure 2 Distributions of family planning knowledge among pregnant women. |
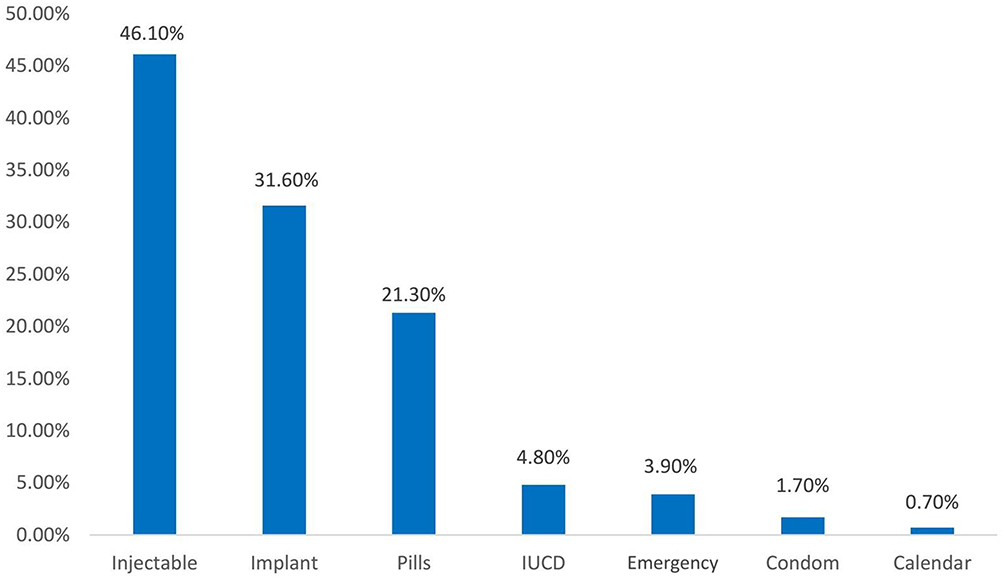 |
Figure 3 Intention to use modern contraceptive methods among pregnant women. |
Factors Associated with Unintended Pregnancy
In bivariable analysis, age of respondent, marital status, educational status, occupation, monthly income, residence, gravidity, number of children, number of parity, stillbirth, abortion, pre-term birth, knowledge of FP, practice of FP, family planning decision, spousal communication on family planning, husband approval to use FP and uses of substance were associated with unintended pregnancy at P < 0.2, but other variables were not significant.
Variables which had a significant level of P < 0.2 were inserted into the model in the multivariable logistic regression analysis process. The variables educational status, occupation, monthly income, residence, number of children, number of parity, stillbirth, etc. in multivariable logistic regression are statistically insignificant and the model adequacy checked using AIC (Akaike information criterion). Table 4 lists the variables (age, marital status, gravidity, and decision on FP) in the model withfor minimum AIC, which is relatively the better model.
The Adjusted OR (AOR) findings showed in the multivariate logistic regression, being divorced and widowed, age ≤ 24, gravidity 1–2 and 3–4 and decision making on FP by only women had a statistically significant association with an unintended pregnancy (Table 5).
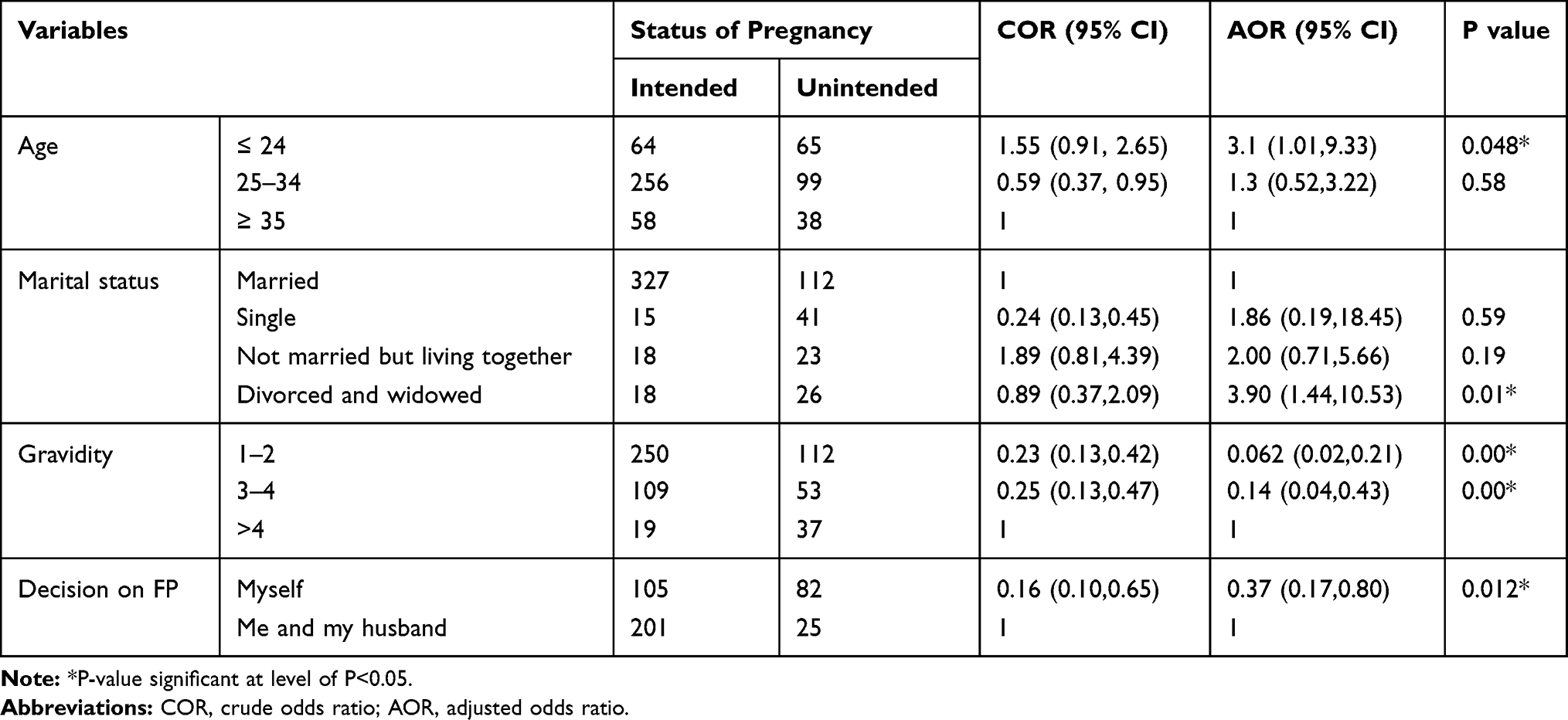 |
Table 5 Multiple Logistic Regressions Analysis for Factors Associated with Unintended Pregnancy |
Accordingly, pregnant women aged ≤ 24 years were three times more likely to experience unintended pregnancy compared with women of 35 years of age (AOR= 3.1, 95% CI: 1.01–9.33) at P = 0.048. The risk of unintended pregnancy among divorced and widowed women was four times higher than women currently married (AOR= 3.90, 95% CI: 1.44–10.53) at P = 0.01. Women with a gravidity of 1–2 and 2–3 were 94% and 86% less likely to face unintended pregnancy compared with women with a gravidity of ≥ 4 (AOR = 0.062, 95% CI: 0.02–0.21) and (AOR= 0.14, 95% CI: 0.04–0.43) with both P = 0.00, respectively. Pregnant women who made their own decision on FP were 63% less likely to encounter UP than those who agreed through their husbands (AOR = 0.37, 95% CI: 0.17–0.80) at P = 0.012.
Discussion
The aim of this study was to assess the magnitude and factors associated with unintended pregnancy among pregnant women in the town of Debre Markos. The study revealed that unintended pregnancy prevalence was 202 (34.8%). This result was lower than the study findings in Damote Gale Woreda, Arsi Negele Woreda, Malaysia, Britain, South Africa, with a prevalence of 42.4%, 41.5%, 42.9%, 45.2% and 64.33%, respectively.19–23 The result may be lower because there is a tendency to report a pregnancy as intended once it has occurred.24
This result was comparable to a similar study of 34%, 36.6%, 36.4%, 37.8%, 37% and 38.2%, respectively, in Hossana Town, Duguna Fango District in Wolaita Zone, Addis Ababa, the United States and Pakistan.25–30 However, it is slightly higher than the result reported in Belessa Woreda, Wolkaite Woreda, Debre Birhan town, and Ghana with the prevalence of 13.7%, 26%, 23.5%, and 29.8%, respectively.18,31–33 It may be attributed to the majority of the participants in this study being urban women who are currently bearing large numbers of children and struggling with the cost of living.34 In general, the variation may be due to variations in socio-cultural characteristics and health coverage, and differences in accessibility and affordability of maternal health facilities, including access to modern contraception, among the areas of study.
The women not having enough money, a short gap from previous pregnancy and system failure, most specifically pills, were among the key reasons for unintended pregnancy listed by study participants. The mere awareness of contraception did not prevent unwanted pregnancy. This result was in agreement with studies conducted in Gelemso and Jimma town, Oromia region, Ethiopia.35,36
Some studies found that older women were more likely to experience unplanned pregnancy compared with younger women, such as studies conducted in Belessa Woreda, Malaysia and Tanzania.21,32,37 In contrast, in this study, younger women have higher unintended pregnancy rates compared with older women. This finding was in line with the studies conducted in Pakistan and Dilla University.29,38 This could be due to the potential poor knowledge of reproductive health, less opportunity for young women to freely access family planning services and being exposed to peer pressure. Similarly, older women are also predominantly in marital union and they are more likely to plan their pregnancies.
The odds of divorced and widowed women having an unintended pregnancy were higher than women who are currently married. This result is consistent with the studies in the towns of Debre Birhan, South Africa, Oromia region and Kenai.6,18,23,36 This result may be due to the social, legal and cultural norms of the society, low economic capacity of women, and lower psychological readiness in these women.
Several studies have shown that the rate of unintended pregnancy grows as the gravidity increases. In addition, the results of this study showed that women with a gravidity of 1–2 and 2–3 were 94% and 86% respectively less likely to experience unwanted pregnancy relative to those women who had gravidity of ≥ 4. This finding is in line with studies in Debre Birhan, where women who had as many as 5 pregnancies were more likely than those with 1–2 to have an unintended pregnancy;18 in Hosanna Town, women with >3 pregnancies were more likely than those with1–2 pregnancies to claim unintended pregnancy.26 The possible explanations might belarge family number, fertility rate, and women’s fear of using long acting family planning.
The autonomy of women in family planning and decision taking has a clear beneficial impact on unintended pregnancy. Women who had control in FP decision-making themselves were less likely than women who shared the decision making with their husband to experience UP. This finding is consistent with prior research conducted in Belessa Woreda in 2018, where the odds of unintended pregnancy among women who used family planning alone was 60% lower than those who only followed their husband’s decisions, and in Addis Ababa in 2017, women with decision-making autonomy were four times less likely to be exposed to unintended pregnancy than those with husbands who made decisions alone.27,32 This shows that women having freedom to make their own decisions is good not just for the the family as a whole, but also for other aspects.
Limitations
Under this study the interviewer’s questionnaire does not eliminate biases such as social desirability (the respondents may not respond to sensitive interviewer questions); due to this, respondents may respond that the pregnancy is unwanted, and if the pregnancy persists, this pregnancy may also be reported as desirable later.
Conclusion and Recommendation
From the study result, the conclusion is that there was no single factor affecting unintended pregnancy, rather many factors were interwoven to affect the event’s occurrence. The findings of this study showed that age of women, marital status, gravidity and decision making in family planning, were significant predictors of recent unintended pregnancies in Debre Markos town.
For widowed and divorced women, the risk of unintended pregnancy has been shown to be high. . Our outcome confirms the high risk of unintended pregnancy for widowed and divorced women. The risk of unintended pregnancy has also been considered to be high for young adults. As a consequence, unintended pregnancy has been associated with adolescent pregnancy. Our results suggest that younger women are at higher risk of unintended pregnancy, so interventions aimed at reducing unintended pregnancy should target younger women.
Furthermore, attention must be paid to educating husbands, as most household decisions, including the timing of pregnancy and the number of children desired, are greatly influenced by the male partner. In addition, there is a need for better information about the use of long-acting modern contraceptive methods.
The Ministry of Health should enhance family planning access and promote women’s empowerment. Health facilities should design programs to train the community to bring sustainable behavioral changes in reproductive health, promote husband and wife communication about FP, and promote the correct use of long‐acting modern family planning methods. Youth associations, teachers and women’s groups, religious sectors should give education and advice for younger women to avoid unintended pregnancy. Religious fathers and government officials in the Amhara region should educate and advise widowed or divorced women’s to respect and support each other in the culture of the community. Health professionals, voluntary aid associations and policy makers should design different policies that help women to restrict family sizes (i.e. family planning policy) and give support to empower women economically. To complement the results from this report, a qualitative study in the community is strongly recommended to provide an in-depth discussion on unwanted pregnancies and associated factors.
Abbreviations
CSA, Central Statistical Agency; DHS, Demographic and Health Survey; FMOH, Federal Ministry of Health; FP, family planning; IRRB, Institutional Research Review Board; MCH, maternal and child health; MDG, Millennium Development Goal; MMR, maternal mortality rate; NGO, non-governmental organization; SPSS, Statistical Package for Social Science; UP, unintended pregnancy; WHO, World Health Organization.
Data Sharing Statement
The data set used and analyzed for this study is available from the corresponding author on reasonable request.
Ethical Standard
Prior to data collection, an Ethical clearance and approval letter was received from Health Research Ethics Review Committee (HRERC) of Debre Markos University, College of Health Sciences. Then the letter was sent to the governmental health institution in Debre Markos town and the respective area managers were informed about the purpose and deliverables of the research undertaking. Informed written consent was obtained from all pregnant women during data collection. Confidentiality was ensured by not writing the name of the respondents on the questionnaire. This study was done in accordance with the World Medical Association Declaration of Helsinki.
Acknowledgments
The researcher gratefully thanks Debre Markos University for funding this research. We would like also to thank Debre Markos town administration and health department for allowing us to conduct this research in the community. We highly acknowledge study participants for providing all necessary information, data collectors and Mr. Habtamu Chanie for editing and revision of the manuscript. Finally, I would like to say that God has put the soul of Mr. Habtamu Chanie in heaven and condolence to his families and friends.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Cochran WG. Sampling Techniques.3rd edition, John Wiley & Sons. Inc:New York ; 1977.
2. EDHS. Ethiopian demographic and health survey; 2016.
3. Exavery A, Kanté AM, Hingora A, Mbaruku G, Pemba S, Phillips JF. How mistimed and unwanted pregnancies affect timing of antenatal care initiation in three districts in Tanzania. BMC Pregnancy Childbirth. 2013;13(1):35.
4. Bradley SE, Croft T, Rutstein SO. The Impact of Contraceptive Failure on Unintended birth and induced Abortion:estimates and strategies for reduction: ICF Macro, DHS analythical Studies No 22, Calverton Maryland, USA;2011.
5. Santelli J, Rochat R, Hatfield‐Timajchy K, et al. The measurement and meaning of unintended pregnancy. Perspect Sex Reprod Health. 2003;35(2):94–101.
6. Ikamari L, Izugbara C, Ochako R. Prevalence and determinants of unintended pregnancy among women in Nairobi, Kenya. BMC Pregnancy Childbirth. 2013;13(1):69.
7. Sedgh G, Singh S, Hussain R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud Fam Plann. 2014;45(3):301–314.
8. Ackley BJ, Ladwig GB, Msn R, Makic MBF, Martinez-Kratz M, Zanotti M. Nursing Diagnosis Handbook E-Book: An Evidence-Based Guide to Planning Care. Mosby; 2019.
9. Williamson LM, Wight D, Petticrew M, Hart GJ. Limits to modern contraceptive use among young women in developing countriesa systematic review of qualitative research. ReproductiveHealth. 2009;6(3).
10. Arega WL, Zewale TA, Bogale KA. Premarital sexual practice and associated factors among high school youths in Debretabor town, South Gondar zone, North West Ethiopia, 2017. BMC Res Notes. 2019;12(1):314.
11. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–e333.
12. WHO. Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality. Geneva:World Health Organization;2008.
13. Organization WH. Engaging Men in Changing Gender-Based Inequity in Health: Evidence from Programme Interventions. Geneva: WHO; 2007.
14. Yadufashije D, Sangano GB, Samuel R. The study of factors influencing teenagers pregnancy in Africa. Int J Interdiscip Innovative Res Dev. 2017.
15. Cook SM, Cameron ST. Social issues of teenage pregnancy. Obstet Gynaecol Reprod Med. 2017;27(11):327–332.
16. Logan C, Holcombe E, Manlove J, Ryan S. The Consequences of Unintended Childbearing. Washington DC: Child Trands and National Campaign to Prevent Teen Pregnancy. 2007;28:142–151.
17. Glinski A, Sexton M, Petroni S. Understanding the adolescent family planning evidence base; 2014.
18. Getu Melese K, Gebrie MH, Berta Badi M, Fekadu Mersha W. Unintended pregnancy in Ethiopia: community based cross-sectional study. Obstet Gynecol Int. 2016;2016.
19. Fite RO, Mohammedamin A, Abebe TW. Unintended pregnancy and associated factors among pregnant women in Arsi Negele Woreda, West Arsi Zone, Ethiopia. BMC Res Notes. 2018;11(1):671.
20. Geda NR, Lako TK. A population based study on unintended pregnancy among married women in a district in Southern Ethiopia. J Geogr Reg Plann. 2011;4(7):417–427.
21. Muslimah Yusof AAS, Omar M, Ahmad NA. Unplanned pregnancy and its associated factors. Glob J Health Sci. 2018;10:8.
22. Wellings K, Jones KG, Mercer CH, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet. 2013;382(9907):1807–1816.
23. Haffejee F, O’Connor L, Govender N, et al. Factors associated with unintended pregnancy among women attending a public health facility in KwaZulu-Natal, South Africa. S Afr Fam Pract. 2018;60(3):1–5.
24. Joyce T, Korenman S. The stability of pregnancy intentions and pregnancy-related maternal behaviors,”. Matern Child Health J. 2000;4(3).
25. Getachew FD. Level of unintended pregnancy and its associated factors among currently pregnant women in Duguna Fango district, Wolaita zone, southern Ethiopia. Malays J Med Biol Res. 2015;2(2):75–88.
26. Hamdela B, Tilahun T. Unwanted pregnancy and associated factors among pregnant married women in Hosanna Town, Southern Ethiopia. PLoS One. 2012;7(6):e39074.
27. Kassie T, Moges G, Ali A, Tefera W. Magnitude and factors associated with unintended pregnancy among pregnant women in Addis Ababa Ethiopia. Glob J Med Public Health. 2017;6(4):15.
28. Mulatu T, Cherie A, Negesa L. Prevalence of unwanted pregnancy and associated factors among women in reproductive age groups at selected health facilities in Addis Ababa, Ethiopia. J Women’s Health Care. 2017;6(392):2167–0420.1000392.
29. Habib MA, Raynes-Greenow C, Nausheen S, et al. Prevalence and determinants of unintended pregnancies amongst women attending antenatal clinics in Pakistan. BMC Pregnancy Childbirth. 2017;17(1):156.
30. Mosher WD, Jones J, Abma JC. Intended and unintended births in the United States; 1982–2010; 2012.
31. Abayu H, Birhanu Z, Nega A, Kidanemariam A. Prevalence and associated factors of unintended pregnancy in Welkaite Woreda, Tigray and North Ethiopia cross sectional study by 2012. J Preg Child Health. 2015;2(2):1–5.
32. Tsegaye AT, Mengistu M, Shimeka A. Prevalence of unintended pregnancy and associated factors among married women in west Belessa Woreda, Northwest Ethiopia, 2016. Reprod Health. 2018;15(1):201.
33. Ameyaw EK. Prevalence and correlates of unintended pregnancy in Ghana: analysis of Ghana Demographic and Health Survey. Maternal Health NeonatolPerinatol. 2018;4(17).
34. Ethiopia D. Final Report Central Statistical Agency Addis Ababa. Ethiopia; 2011.
35. Beyene GA. Prevalence of unintended pregnancy and associated factors among pregnant mothers in Jimma town, southwest Ethiopia: a cross sectional study. Contracept Reprod Med. 2019;4(1):8.
36. Mohammed F, Musa A, Amano A. Prevalence and determinants of unintended pregnancy among pregnant woman attending ANC at Gelemso General Hospital, Oromiya Region, East Ethiopia: a facility based cross-sectional study. BMC Women’s Health. 2016;16(1):56.
37. Calvert C, Baisley K, Doyle AM, et al. Risk factors for unplanned pregnancy among young women in Tanzania. J Fam Plann Reprod Health Care. 2013;39(4):e2.
38. Mohammed Feyisso AG, Yimam H, Hailu S. Magnitude of unintended pregnancy and its determinants among pregnant women visiting Dilla University Referral Hospital, South Ethiopia. J Women’s Health Care. 2017;6(4).
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.