")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Magnitude of Satisfaction and Associated Factors Among Caregivers of Children with Disabilities Towards Community-Based Rehabilitation Service in Central and North Gondar Zone, Northwest Ethiopia: A Community-Based Cross-Sectional Study
Authors Fentanew M, Yitayal MM, Chala KN , Kassa T
Received 21 June 2021
Accepted for publication 3 September 2021
Published 16 September 2021 Volume 2021:14 Pages 2565—2575
DOI https://doi.org/10.2147/JMDH.S325737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Molla Fentanew, Melisew Mekie Yitayal, Kalkidan Nigussie Chala, Tesfa Kassa
Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, Gondar, Ethiopia
Correspondence: Tesfa Kassa
University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Email [email protected]
Introduction: Community-based rehabilitation service (CBR) is a community development strategy set for persons with disabilities and their families. Measuring caregivers’ satisfaction is a recommended approach to know the overall satisfaction of rehabilitation service. Therefore, this study aimed to assess the magnitude of satisfaction and associated factors among caregivers of children with disabilities towards community-based rehabilitation in Central and North Gondar zone, North West Ethiopia.
Methods: A community-based cross-sectional study was conducted from March to September 2020. The data were collected by socio-demographic variables, types of services, types of disabilities, and Client Satisfaction Questionnaire (CSQ-8). Data analysis was done by SPSS Version-20 statistical software. Descriptive statistics, bi-variable, and multivariable logistic regression analysis were computed. The multivariable logistic regression analysis model a P-value < 0.05 was used to identify the associated factors with caregivers’ satisfaction.
Results: The study showed that the overall caregivers’ satisfaction with community-based rehabilitation service among caregivers of children with disabilities was 60.9% (95% CI; 55– 66%). Female gender (AOR: 0.19, 95% CI: 0.05– 0.68), older age (AOR: 0.160, 95% CI: 0.03– 0.85), being farmer (AOR: 0.14, 95% CI: 0.05– 0.42), North Gondar zone residence (AOR: 7.02, 95% CI: 6.78– 8.59), high monthly income (AOR: 2.48, 95% CI: 1.09– 5.61), got two or more type of service (AOR: 3.65, 95% CI: 2.64– 12.39), service duration 8– 14 years (AOR: 4.36, 95% CI: 1.44– 7.04) and service frequency 5– 8 times per month (AOR: 3.91, 95% CI 2.18– 7.01) were factors associated with the caregivers’ satisfaction on community based-rehabilitation service.
Conclusion and Recommendation: The magnitude of caregivers’ satisfaction with community-based rehabilitation services in the study area was more than half. Female gender, older age, being farmer, high monthly income, North Gondar zone residence, the high number of services, duration of services started and frequency of follow-up were factors significantly associated with caregiver’s satisfaction.
Keywords: caregivers’ satisfaction, children with disability, community-based rehabilitation, Central and North Gondar zone, Ethiopia
Introduction
Community-Based Rehabilitation (CBR) is a community development strategy set by the World Health Organization (WHO) for enhancing the lives of Persons With Disabilities (PWDs) and their caregivers within their community.1 The CBR service give emphasize on utilization of locally available resources by including the caregivers of PWDs, the community, and beneficiaries.2,3
Globally, 150 million children living with disabilities,4,5 the vast majority (80%) of these children live in resource-poor countries.6,7
In Africa, the United Nations Children’s Fund (UNICEF) estimates that between 5% and 10% of children had disabilities where 90% of these children do not attend school, moreover the burden is higher on caregivers.8 A study done in rural Eastern Ethiopia showed that the magnitude of childhood disability was 4.8%.9
Most Children With Disabilities (CWDs) required assistance from their caregivers.10 In Low and Middle-Income Countries (LMICs) caregivers providing a bulk of care for their children.11,12 Evidence shows that caregivers of CWDs in low resource countries had a different emotional and physical impact on their family life.13–15
To reduce different burdens on caregivers of CWDs, CBR services are available in more than 90 countries across the world.16 The implementation of CBR-service is varying from one country to another depending on the availability of resources.17–19
The overall approach of CBR-service is to focus on PWDs and their families including existing services.20 The CBR-service has five components among of these healthcare, education, financial support and assistive device are mainly provided by UOG- CBR-service in our study areas.
Satisfaction is the emotional reaction or psychological state of a person regarding the services he/she received.21 It varies from person to person due to many factors that could be affected the caregiver’s satisfaction. Some of those factors stated in studies are age, income, level of education, working conditions, and the types of CBR service.11,22,23
Measuring caregivers’ satisfaction is a recommended approach at all levels of health and other types of services for improvement.24 Regarding this measure caregivers’ satisfaction towards CBR-service plays a significant role in the improvement of service.25,26
Different studies were conducted on the burden of disability and the importance of CBR service.8,9 However, there is a lack of caregiver’s satisfaction with CBR-service. In Ethiopia, from our extensive search of previously published works, we found that there is a lack of data on satisfaction with CBR-service among caregivers of CWDs. Therefore, our study aimed to assess the caregiver’s satisfaction and associated factors among caregivers of CWDs towards community-based rehabilitation.
Methods
Study Design and Settings
A community-based cross-sectional study design was conducted in Central and North Gondar Zone, Amhara Regional state, Ethiopia from March to September 2020 to assess satisfaction and associated factors among caregivers of CDWs.
The Zone is administratively divided into Central and North Gondar. The University of Gondar (UOG) community-based rehabilitation program had giving service to 1100 CWDs for the last fourteen years. All caregivers of CWDs in Central and North Gondar zones whose children get CBR-service were the source population and all caregivers of CWDs at Central and North Gondar zone whose children have to get UOG-CBR-service and available during the data collection period were the study populations. Caregivers of CWDs whose children have to get CBR service for three months and above were included. Whereas caregivers of CWDs whose children have got additional services from other non-governmental organizations were excluded from the study.
Sample Size and Sampling Techniques
The sample size was calculated using a single population proportion formula (n = (Zα/2)2*P (1-P)/(d)2) with the following assumptions of 50% of caregivers’ satisfaction with CBR service expected margin of error (d) 5% and 95% confidence level. n = (1.96)2(0.5) (0.5)/ (0.05)2 = 384. However, the estimated number of caregivers of CWDs in the Central and North Gondar zone was 1100, which was less than 10,000. For that situation, the target population was small enough (if N < 10,000). Then, using the finite population correction formula and adding 10% of the non-response rate the final sample size was 312.
Initially, the proportional allocation was applied for each selected Woredas (the administrative name of a place like regions, zones, Woredas, and Kebeles). A systematic random sampling technique was used to select 312 study participants from 1100 caregivers of CWDs in the Central and North Gondar zone. The sampling interval (k) was calculated 1100 divided by 312. “K” =3, then the first study participant was randomly selected by lottery method from “intervals (“1 to k” =1 to 3) it was 2 and other study participants were selected systematically in every “kth” interval from each proportion of study population.
Variables
The dependent variable of the study was Caregivers’ satisfaction with CBR service, whereas the independent variables were Socio-demographic characteristics of the caregivers (age, sex, residence, religion, educational status, marital status, occupation, household income, family size, household composition, having helpers, and relationship), Children socio-demographics characters (age, gender, birth order), types of disabilities (physical, visual, hearing, intellectual, and multiple), type of the services (health, education, mobility device, financial support), number of services received, duration of service started and frequency of service.
Operational Definition
Caregivers
Any person who has the responsibility of taking care of CWD. He or she may be a parent, relative, or other paid worker who lives with CWD, who is going to be interviewed.
Community-Based Rehabilitation
This is a community action to ensure the life of CWDs and their caregivers. Which includes health care, education, financial support, mobility devices.
Child
Means any human being from birth to the age of 18 years.27
Disability
Any restriction or lack of ability to perform an activity in a manner within the range considered normal for a human being.28
Children with Disabilities
Are children with chronic physical, visual, hearing, learning, and multiple types of disabilities (ie, have restriction in movement, seeing, hearing, learning or combination of those) who need health and other services.29,30
Satisfaction
Is the amount of caregivers’ expectation regarding UOG-CBR- service and it is quantified by the Client Satisfaction Questionnaire (CSQ-8) tool. After computing the sum of eight items of the CSQ-8 tool; since the data were normally distributed, dissatisfied rated below the mean and satisfied; from the mean and above.31
Data Collection Tool and Procedure
The data were collected by trained physiotherapists by interviewing the participants using a structured questionnaire and (CSQ-8). The CSQ-8 is designed for direct measures of service satisfaction with a wide range of caregivers’ groups and service types. It is a standard self-reported questionnaire constructed to measure satisfaction with service received by individuals and caregivers.32 It consists of eight items, with each rated on a 4-point Likert-type scale. The CSQ-8 has a minimum score of 8 and the maximum score of 32. A higher score represents greater satisfaction. The CSQ-8 is applicable for ongoing as well as terminated CBR-service and other health services. This scale has been broadly adopted, nationally, internationally and used for scientific work, program evaluation, and research.33
The willingness of study participants (caregivers of CWDs) checked by informed consent and who were willing to participate in the study were included by using the inclusion and exclusion criteria. After obtaining informed consent four trained physiotherapists (bachelor science) were collected the data through interviewing the study participants.
Data Quality Control and Analysis
Before data collection, data training was given for data collectors on the study objectives, data collection instruments, techniques, producers, the importance of privacy, and ensuring the confidentiality of the respondents. Data collectors were supervised daily and every night; the consistency and completeness of data were checked by Principal Investigator (PI). The original English version of the data collection tool was translated into Amharic and re-translated back into English by language expertise to maintain its consistency.
Pretest was done on 16 caregivers (5% of the sample size) in the Central Gondar zone Maraki sub-town. The understandability, consistency, and appropriateness of the questionnaire were checked. Finally, all findings from the pre-test were incorporated into the final questionnaire and necessary amendments were done before the actual data collection. All aspects of the data collection process were supervised by the PI to ensure data quality.
The collected data was edited, coded, cleaned, and entered into EPI info 7 software and export to SPSS version 20 software for analysis. Bi-variable and multivariable logistic regressions analysis was employed to show the relationship between dependent and independent variables. All possible predictors which were significant in the bivariate analysis (p-value < 0.25) were included in the multivariable logistic model.
The Hosmer-Lemeshow goodness-of-fit test was used to assess the fitness of the model. Multicollinearity among the explanatory variables was checked using the Variance Inflation Factor (VIF>10). To control for possible confounding and identify independent factors associated with caregivers’ satisfaction on CBR-service a final multivariable model was built using the backward stepwise method. The level of statistical significance was declared at a p-value of less than 0.05. Adjusted odds ratio with its 95% CI was used to show the strength of association between each explanatory variable and the outcome variable. The results of the analysis were presented in descriptive texts, tables, and graphs.
Results
Sociodemographic Characteristics of Caregivers and Children with Disability
A total of 312 study participants responded to the interviewer-administered questionnaire with a response rate of 100%. Among the total study participants, 269 (86.2%) were females, the mean age of caregivers was 39.37 (SD=7.89), religious 265 (84.9%) were orthodox, marital status 175 (56.1%) were married, residence 269 (86.2%) live in urban, educational status 174 (55.8%) had no formal education, and occupational status 128 (41.0%) were daily labor (Table 1).
 |
Table 1 Sociodemographic Characteristics of Caregivers with the Community-Based Rehabilitation in Central and North Gondar Zone in 2020 (n=312) |
The mean age of children with disabilities was 11.20 years. Most of the children with disabilities 169 (54.2%) were males and 286 (91.7%) of caregivers had one child with disabilities only (Table 2).
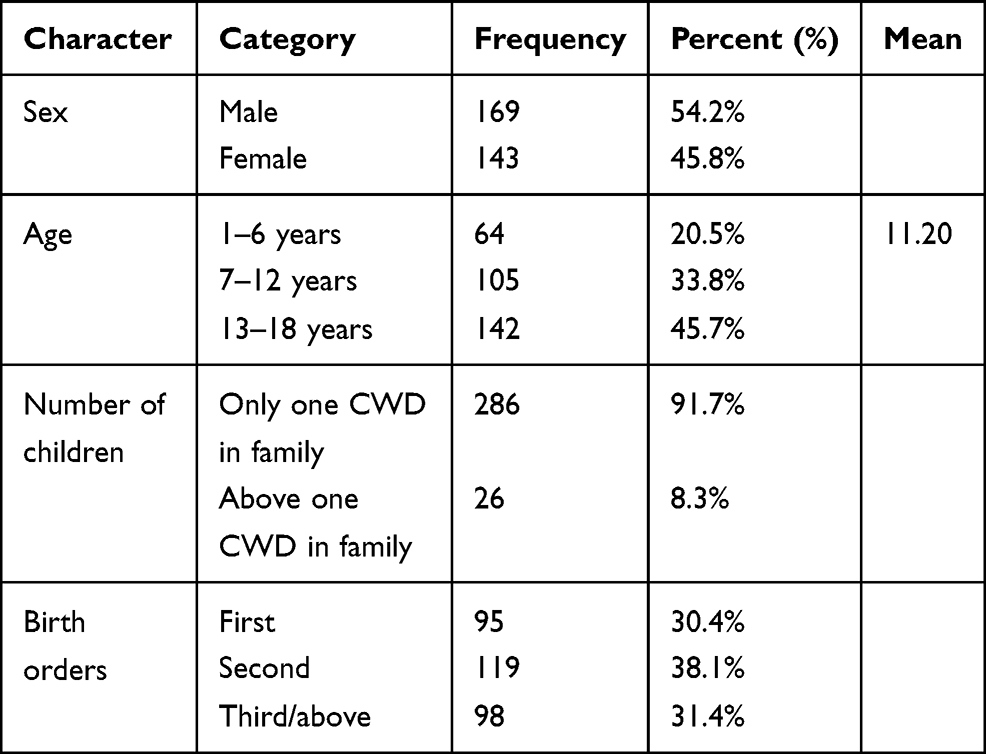 |
Table 2 Sociodemographic Character of Children with Disability with the Community-Based Rehabilitation in Central and North Gondar Zone in 2020 (n=312) |
The Relationship of Caregivers and Children with Disability
Household composition of caregivers 176 (56.4%) had two parents live together, 111 (35.6%) were single mothers, the majority of caregivers 259 (83%) were mothers, 242 (77.8%) had helpers, from having helpers 97 (31%) were daughters (Table 3).
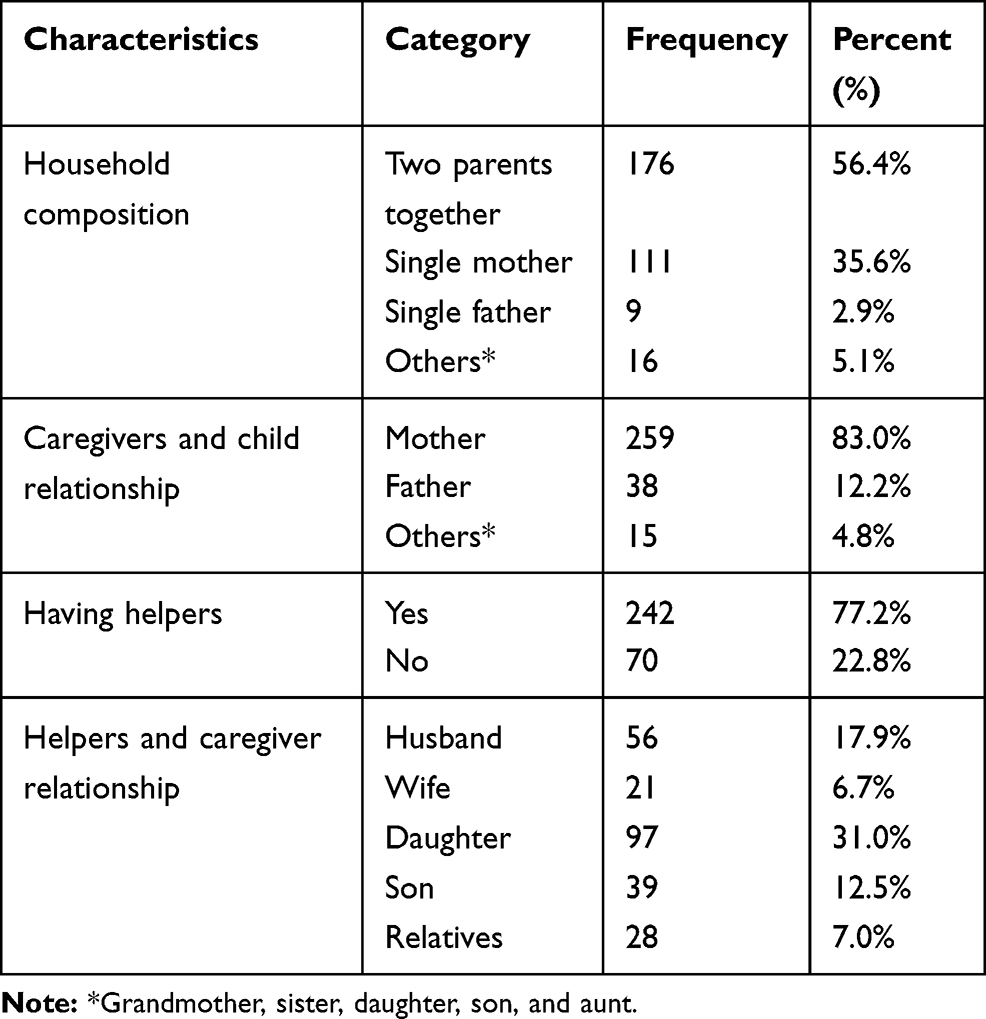 |
Table 3 The Relationship of Caregivers, Children with Disabilities, and Helpers with the Community-Based Rehabilitation in Central and North Gondar Zone in 2020 (n=312) |
Type of Disability of Children with Disability
Among a total of children with disabilities included in the study, 36.2% had a physical disability, 31.8% had multiple disabilities, 15.1% had intellectual/learning disability, 9.9% had a hearing disability, and 7.1% had vision disability (Figure 1).
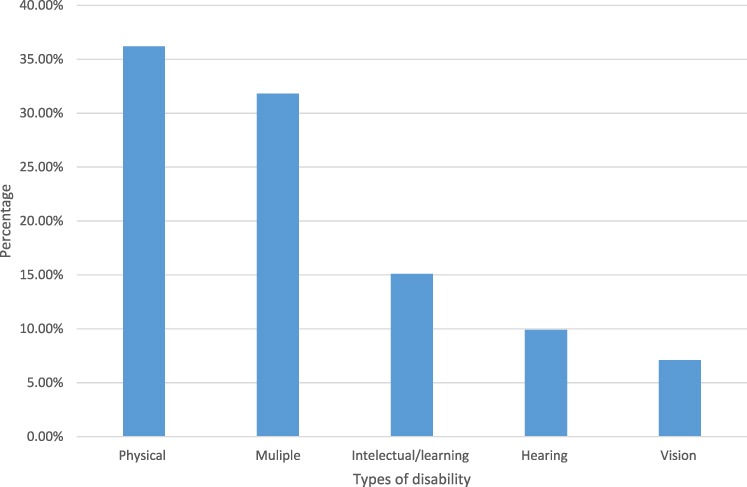 |
Figure 1 Type of disability of children with disabilities they received service with the community-based rehabilitation in central and north Gondar zone in 2020 (N=312). |
Types, Frequency, and Duration of Community-Based Rehabilitation Service
From total children with disabilities, 117 (37.5%) received health service, 34 (10.9%) received educational service, 17 (5.4%) received mobility devices, 9(2.9%) received financial support, and 177 (56.6%) received one type of service (Table 4).
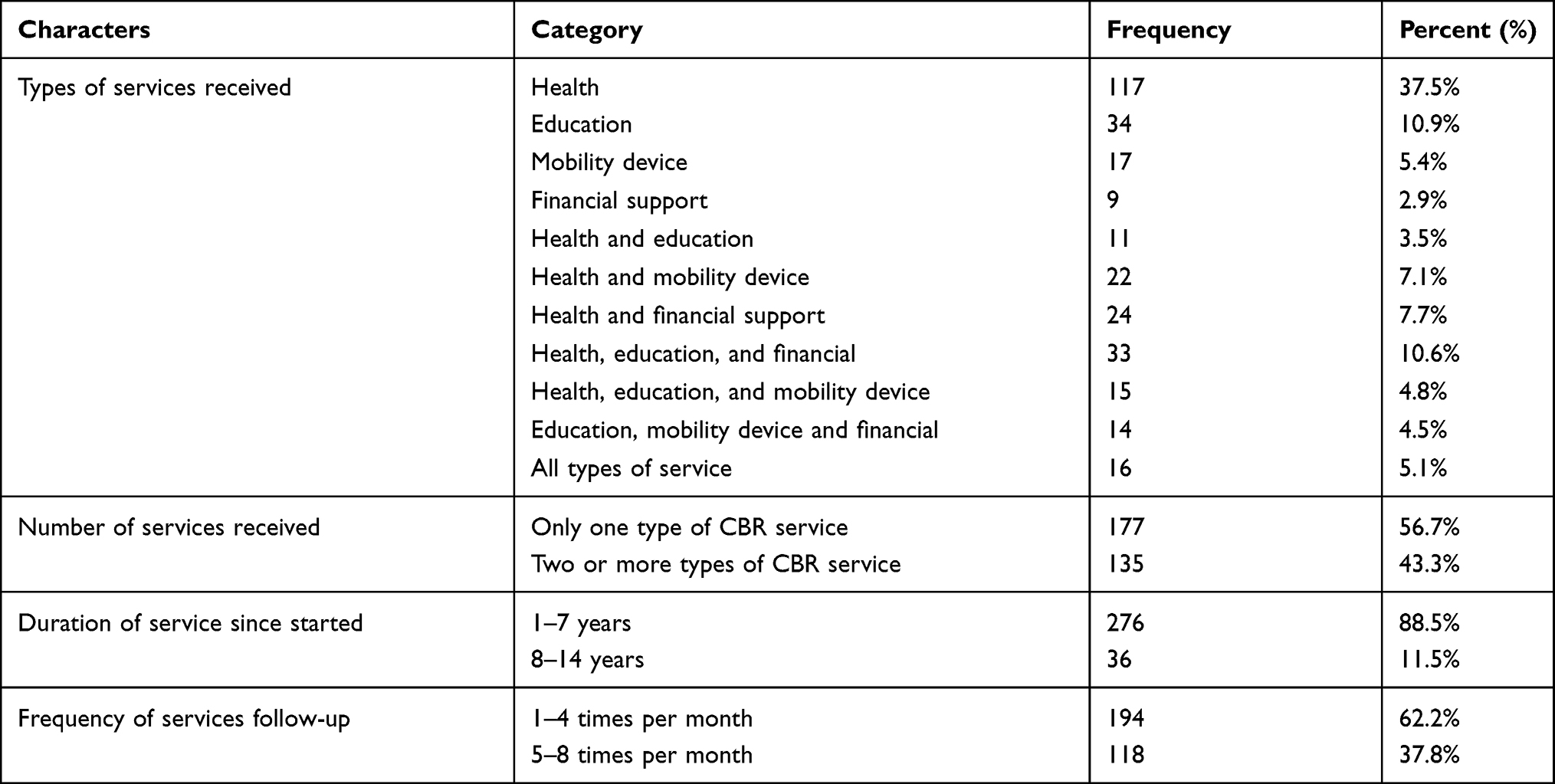 |
Table 4 Types of Services, Way of Attending Services, Frequency and Duration of Service with Community-Based Rehabilitation in Central and North Gondar Zone in 2020 (n=312) |
Caregivers’ Satisfaction with UOG-CBR- Services
Regarding the respondent’s satisfaction, 189 (60.9%) of caregivers scored in the CSQ-8 satisfied category. Whereas 123 (39.4%) scored dissatisfied category. The dissatisfaction rates were found in kind of wanted CBR service 211 (67.6%) followed by the problem-solving capacity of CBR-service 186 (59.6%) and the quality of CBR service 178 (57.1%) (Figure 2).
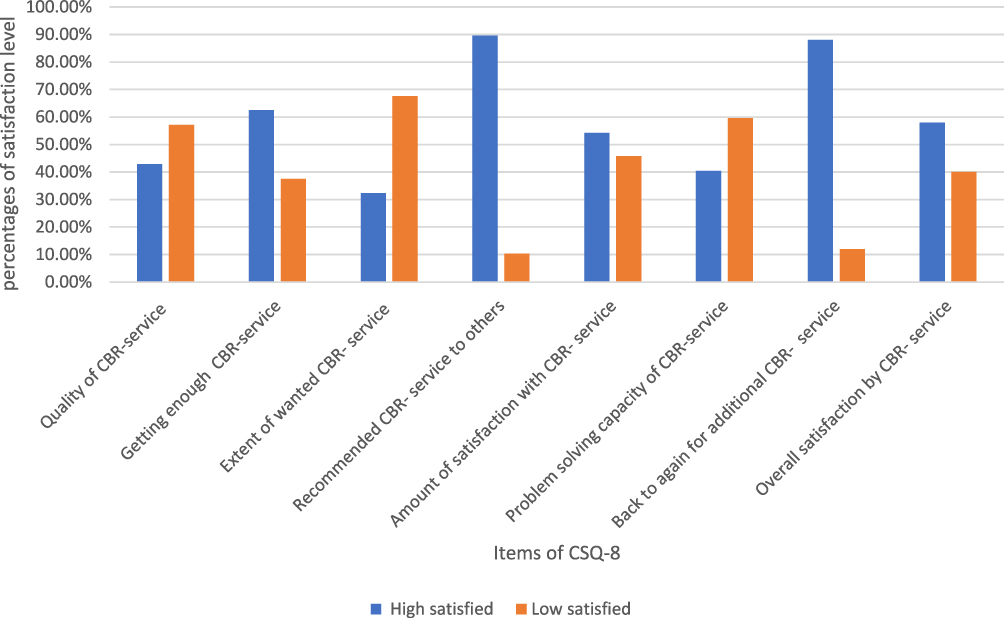 |
Figure 2 The caregivers’ satisfaction on cbr-service on csq-8 items in central and North Gondar Zone, Ethiopia, 2020 (N=312). |
Associated Factors for Caregivers’ Satisfaction
Regarding socio-demographic characters of caregivers; female gender of caregivers AOR=0.19 (0.054–0.68), older age (>50 years) of caregivers AOR=0.16 (0.03–0.85), farmer occupational status AOR=0.14 (0.05–0.42), location of North Gondar zone AOR=7.02 (6.78–8.59) and high monthly income AOR=2.48 (1.09–5.61) were associated significantly.
With related to the type of disability, physical disability is significantly associated AOR=2.73 (1.20–6.17). Regarding factors related to CBR-service; two or more types of service received AOR=3.65 (1.03–6.57), the duration of service started 8–14 years at AOR=4.36 (1.44–7.04) and frequency of follow-up 5–8 times per month at AOR=3.91 (2.18–7.01) were significantly associated (Table 5).
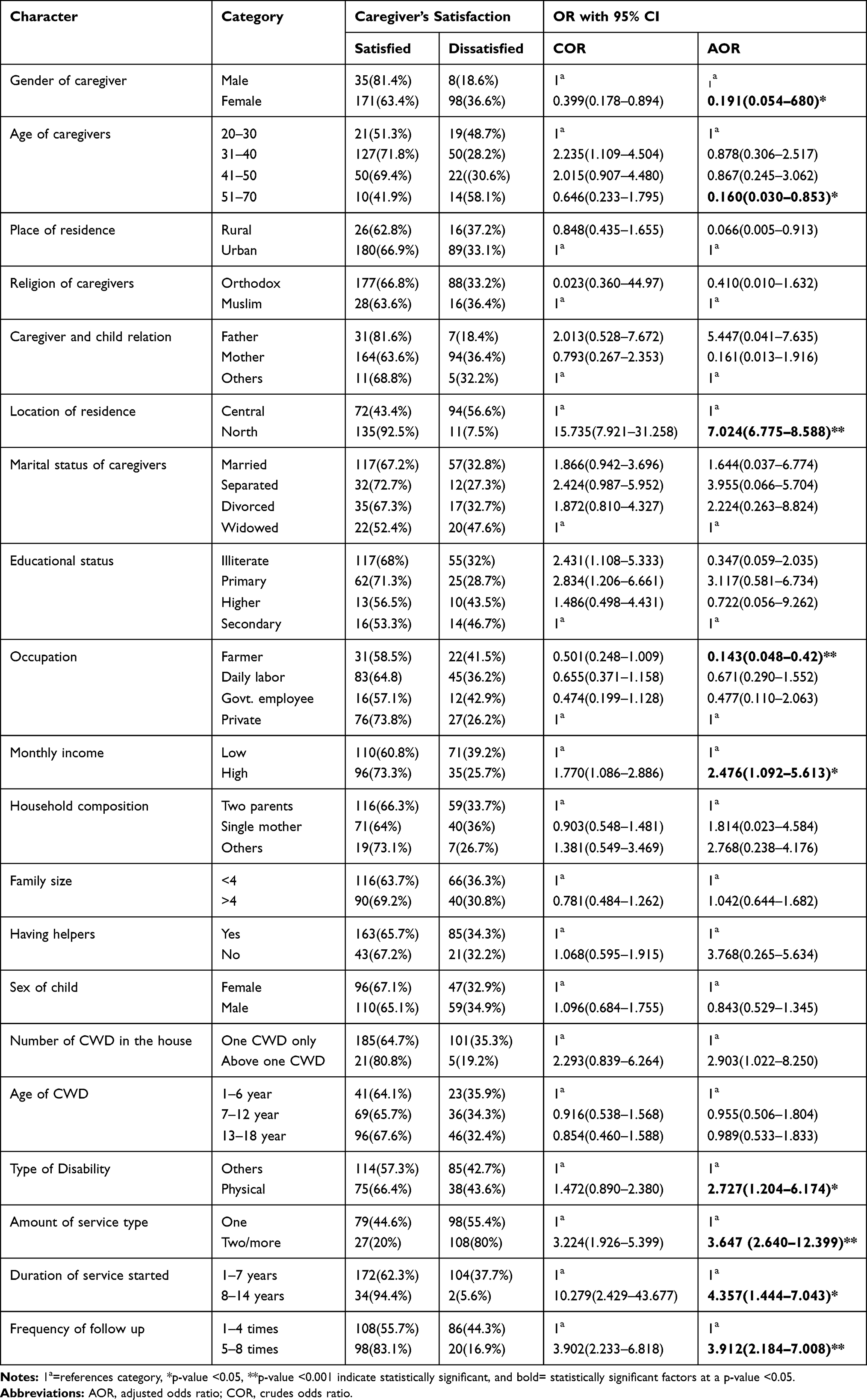 |
Table 5 Association of Factors for Caregivers’ Satisfaction Towards CBR-Services in Central and North Gondar Zone, Northwest Ethiopia, in 2020 |
Discussion
According to our study, the overall satisfaction of caregivers with CBR service utilized in the study area is 60.9% (95% CI 55–66%).
This result is similar to the previous study conducted in Ethiopia (62.1%),34 And, it is lower than the study done in Ethiopia (72%),33 Spain (74.1%),35 and Malaysia (89%).16 In contrast it is higher than the previous study done in Ethiopia (37.4%).36 The possible reasons for the discrepancy might be attributed to variation in socio-cultural characteristics, sample size, study design, amount of service, type, and quality of service.
In our study, the number of services delivered for children with disabilities was significantly correlated to caregiver satisfaction. The odd of caregivers of CWDs whose children received two or more types of CBR services was 3.65 times more likely satisfied than they received one type of CBR service (AOR=3.65,95% CI 1.03–6.57). This might explain by the increment of the amount and type of CBR service that has to meet the demands of CWDs and their caregivers. This result consisted of a study conducted in Australia.37
Regarding gender of caregivers’ females are decreased their satisfaction by 81% than males (AOR=0.19, 95% CI 0.05–0.68). It is contrary to the study conducted in Canada.34,38 The differences might be the small sample size in the previous study and the quality of service delivered. The odd of being older age of caregivers with CWDs were reduced their satisfaction by 84% times than the younger age of caregivers (AOR=0.160, 95% CI 0.03–0.85). This finding agrees with a study conducted in France.39
The odd of being a farmer is 86% times less likely reduced their satisfaction than others occupational status (AOR=0.14, 95% CI 0.05–0.42).40 The possible explanation might be that being farmers can have more expectations from CBR-service than others. Mostly, satisfaction might be influenced by educated participants in their occupation, exposure to different services, and information access.
The odds of having a physical disability were 2.73 times more likely satisfied than those whose children had other types of disability (AOR=2.73, 95% CI 1.20 to 6.17). This might explain by children with physical disabilities have low burdens on their caregivers than children with intellectual and multiple types of disabilities. As a result, a child who has only movement restrictions can learn and communicate easily than a child who has multiple disabilities. This result agrees with a study done in Turkey.21
Regarding service duration and frequency of follow-up, the caregivers of CWDs whose children started service for a long duration are 4.36 times more likely satisfied than those who had a short duration of service. The caregivers of CWDs whose children had follow-up 5–8 times per month are 3.91 times more likely satisfied than the caregivers of CWDs had follow-up 1–4 times per month (AOR=3.91 with 95% CI 1.44 −7.01). Regarding the previous study, the duration and frequency did not predict the caregiver’s satisfaction.41,42 The possible explanation might be the duration of the previous study was a short duration and rehabilitation service for CWDs need a long duration with increased frequency of follow-up to achieve a better outcome.
The caregivers of CWDs who live in the North Gondar zone were 7.02 times more likely satisfied than the caregivers who live in the central Gondar zone with (AOR=7.02, 95% CI 6.78 to 8.59). This might be explained by differences in supervisors’ supervision, commitments of CBR-field workers, and sessions of follow-up. This result agrees with a study done in Malaysia on caregiver’s satisfaction on CBR-service was varies across different states.16
The limitation of the study was since it is a quantitative approach, did not consider the qualitative part of the study.
Conclusion
Our study revealed that more than half of caregivers were satisfied with UOG-CBR-service. Female gender of caregivers, older age of caregivers, and farmer occupational status of caregivers have significantly reduced caregivers’ satisfaction. On the other hand, physical types of disability, high monthly income, North Gondar zone of the residence, increased number of services, duration of services, and the frequency of follow-up were increased caregivers’ satisfaction with CBR services.
Abbreviations
CBR, Community Based Rehabilitation; CSQ-8, Client Satisfaction Questionnaire item eight; CWDs, Children with Disabilities; PWDs, Person with Disabilities; SPSS, Statistical Package for Social Sciences; UOG, University of Gondar; WHO, World Health Organization.
Ethical Approval and Consent to Participate
The proposal was reviewed, approved and ethical clearance was obtained from the Research and Ethical Review Committee and Institutional Review Board (IRB) of the University of Gondar, college of medicine and health science.
The purposes and the importance of the study were explained to the participants of the study and informed consent was obtained from each participant. Confidentiality was maintained at all levels of the study. The Participant’s involvement in the study was voluntary; participants who were unwilling to participate in the study and those who wish to quit their participation at any stage were informed to do so without any restrictions. To ensure the confidentiality of data, study participants were identified using codes and unauthorized persons had no access to the collected data. The information that might expose the identity of the study participants was not collected. Only the principal investigator had access to the computerized data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khasnabis C, Motsch KH. The participatory development of international guidelines for CBR. Lepr Rev. 2008;79(1):17–29. doi:10.47276/lr.79.1.17
2. Community-Based Rehabilitation: CBR Guidelines. Geneva: World Health Organization; 2010.
3. Finkenflügel H, Wolffers I, Huijsman R. The evidence base for community-based rehabilitation: a literature review. Int J Rehabil Res. 2005;28(3):187–201. doi:10.1097/00004356-200509000-00001
4. Groce NE, Kerac M, Farkas A, Schultink W, Bieler RB. Inclusive nutrition for children and adults with disabilities. Lancet Glob Health. 2013;1(4):e180–e1. doi:10.1016/S2214-109X(13)70056-1
5. Shevell M, Ashwal S, Donley D, et al. Practice parameter: evaluation of the child with global developmental delay: report of the Quality Standards Subcommittee of the American Academy of Neurology and The Practice Committee of the Child Neurology Society. Neurology. 2003;60(3):367–380. doi:10.1212/01.WNL.0000031431.81555.16
6. Gormley KJ. Falls prevention and support: translating research, integrating services and promoting the contribution of service users for quality and innovative programmes of care. Int J Older People Nurs. 2011;6(4):307–314. doi:10.1111/j.1748-3743.2011.00303.x
7. Donald KA, Kakooza AM, Wammanda RD, et al. Pediatric Cerebral Palsy in Africa: where Are We? J Child Neurol. 2015;30(8):963–971. doi:10.1177/0883073814549245
8. Hansen AMW, Siame M, van der Veen J. A qualitative study: barriers and support for participation for children with disabilities. Afr J Disabil. 2014;3(1):112.
9. Geda B, Berhane Y, Assefa N, Worku A. In Rural Eastern Ethiopia Hearing Loss Is the Most Frequent Disability during Childhood: a Community Based Survey. PLoS One. 2016;11(5):e0152791–e.
10. Fitaw Y, Boersma JM. Prevalence and impact of disability in north-western Ethiopia. Disabil Rehabil. 2006;28(15):949–953. doi:10.1080/09638280500404552
11. Trute B, Hiebert-Murphy D, Wright A. Family-centred service coordination in childhood health and disability services: the search for meaningful service outcome measures. Child Care Health Dev. 2008;34(3):367–372.
12. Sloper P, Greco V, Beecham J, Webb R. Key worker services for disabled children: what characteristics of services lead to better outcomes for children and families? Child Care Health Dev. 2006;32(2):147–157. doi:10.1111/j.1365-2214.2006.00592.x
13. Gona JK, Mung’ala-Odera V, Newton CR, Hartley S. Caring for children with disabilities in Kilifi, Kenya: what is the carer’s experience? Child Care Health Dev. 2011;37(2):175–183. doi:10.1111/j.1365-2214.2010.01124.x
14. Hartley S, Ojwang P, Baguwemu A, Ddamulira M, Chavuta A. How do carers of disabled children cope? The Ugandan perspective. Child Care Health Dev. 2005;31(2):167–180. doi:10.1111/j.1365-2214.2004.00464.x
15. Mobarak R, Khan NZ, Munir S, Zaman SS, McConachie H. Predictors of stress in mothers of children with cerebral palsy in Bangladesh. J Pediatr Psychol. 2000;25(6):427–433. doi:10.1093/jpepsy/25.6.427
16. Hasan H, Abdul Aziz AF, Aljunid SM. Parents’ and caregivers’ satisfaction with community‐based rehabilitation (CBR) services for children with disability in east coast states in Peninsular Malaysia. Health Soc Care Community. 2020;29:215–226.
17. Majnemer A, Shikako-Thomas K, Lach L, et al. Rehabilitation service utilization in children and youth with cerebral palsy. Child Care Health Dev. 2014;40(2):275–282. doi:10.1111/cch.12026
18. Sinha AG, Sharma R. Factors Influencing Utilization of Physiotherapy Service among Children with Cerebral Palsy in Jalandhar District of Punjab. J Neurosci Rural Pract. 2017;8(2):209–215. doi:10.4103/0976-3147.203852
19. Padmamohan J, Nair MKC, Devi SR, Nair SR, Nair ML, Kumar GS. Utilization of rehabilitation services by rural households with disabled preschool children. Indian Pediatr. 2009;46(Suppl):s79–s82.
20. Iemmi V, Kumar KS, Blanchet K, et al. Community‐based rehabilitation for people with physical and mental disabilities in low‐and middle‐income countries. Cochrane Database Syst Rev. 2017;2017(3).
21. Küçük EE, Küçük Alemdar D. Life Satisfaction and Psychological Status of Mothers with Disabled Children: a Descriptive Study. Community Ment Health J. 2018;54(1):102–106. doi:10.1007/s10597-017-0135-6
22. Ben Thabet J, Sallemi R, Hasïri I, et al. Psycho-emotional impact of a child’s disability on parents. Archives de pediatrie: organe officiel De la Societe francaise de pediatrie. 2013;20(1):9–16. doi:10.1016/j.arcped.2012.10.024
23. Taanila A, Syrjälä L, Kokkonen J, Järvelin MR. Coping of parents with physically and/or intellectually disabled children. Child Care Health Dev. 2002;28(1):73–86. doi:10.1046/j.1365-2214.2002.00244.x
24. Beighton C, Wills J. Are parents identifying positive aspects to parenting their child with an intellectual disability or are they just coping? A qualitative exploration. J Intellect Disabil. 2017;21(4):325–345. doi:10.1177/1744629516656073
25. Benedict RE. Disparities in use of and unmet need for therapeutic and supportive services among school-age children with functional limitations: a comparison across settings. Health Serv Res. 2006;41(1):103–124. doi:10.1111/j.1475-6773.2005.00468.x
26. Bramlett MD, Read D, Bethell C, Blumberg SJ. Differentiating subgroups of children with special health care needs by health status and complexity of health care needs. Matern Child Health J. 2009;13(2):151–163. doi:10.1007/s10995-008-0339-z
27. Herrenkohl RC. The definition of child maltreatment: from case study to construct. Child Abuse Negl. 2005;29(5):413–424. doi:10.1016/j.chiabu.2005.04.002
28. Leonardi M, Bickenbach J, Ustun TB, Kostanjsek N, Chatterji S. The definition of disability: what is in a name? Lancet. 2006;368(9543):1219–1221. doi:10.1016/S0140-6736(06)69498-1
29. McPherson M, Arango P, Fox H, et al. A new definition of children with special health care needs. Pediatrics. 1998;102(1):137–139. doi:10.1542/peds.102.1.137
30. Katsui H, Lehtomaki E, Malle AY, Chalklen S. Questioning human rights: the case of education for children and youth with disabilities in Ethiopia In. Disability in the Global South. Springer; 2016:187–198.
31. Kelly PJ, Kyngdon F, Ingram I, Deane FP, Baker AL, Osborne BA. The Client Satisfaction Questionnaire-8: psychometric properties in a cross-sectional survey of people attending residential substance abuse treatment. Drug Alcohol Rev. 2018;37(1):79–86. doi:10.1111/dar.12522
32. Plante TG, Couchman CE, Diaz AR. Measuring treatment outcome and client satisfaction among children and families. J Mental Health Administrat. 1995;22(3):261–269. doi:10.1007/BF02521121
33. Desta H, Berhe T, Hintsa S. Assessment of patients’ satisfaction and associated factors among outpatients received mental health services at public hospitals of Mekelle Town, northern Ethiopia. Int J Ment Health Syst. 2018;12(1):38.
34. Yimer S, Yohannis Z, Getinet W, et al. Satisfaction and associated factors of outpatient psychiatric service consumers in Ethiopia. Patient Prefer Adherence. 2016;10:1847–1852. doi:10.2147/PPA.S115767
35. Aguirrezabal A, Duarte E, Marco E, Rueda N, Cervantes C, Escalada F. [Patient and caregiver satisfaction with rehabilitation services after stroke]. Revista de calidad asistencial: organo de la Sociedad Espanola de Calidad Asistencial. 2010;25(2):90–96. doi:10.1016/j.cali.2009.11.002. Spanish.
36. Mergia M, Shegaze M, Ayele G, et al. Mothers’ satisfaction with health extension services and the associated factors in Gamo Goffa zone, Southern Ethiopia. PLoS One. 2020;15(5):e0232908. doi:10.1371/journal.pone.0232908
37. Raghavendra P, Murchland S, Bentley M, Wake-Dyster W, Lyons T. Parents’ and service providers’ perceptions of family-centred practice in a community-based, paediatric disability service in Australia. Child Care Health Dev. 2007;33(5):586–592. doi:10.1111/j.1365-2214.2007.00763.x
38. Pelchat D, Lefebvre H, Proulx M, Reidy M. Parental satisfaction with an early family intervention program. J Perinat Neonatal Nurs. 2004;18(2):128–144. doi:10.1097/00005237-200404000-00008
39. Rahi JS, Manaras I, Tuomainen H, Hundt GL. Meeting the needs of parents around the time of diagnosis of disability among their children: evaluation of a novel program for information, support, and liaison by key workers. Pediatrics. 2004;114(4):e477–82. doi:10.1542/peds.2004-0240
40. Zuurmond M, O’Banion D, Gladstone M, et al. Evaluating the impact of a community-based parent training programme for children with cerebral palsy in Ghana. PLoS One. 2018;13(9):e0202096. doi:10.1371/journal.pone.0202096
41. Cope S, Mohn-Johnsen S. The effects of dosage time and frequency on motor outcomes in children with cerebral palsy: a systematic review. Dev Neurorehabil. 2017;20(6):376–387. doi:10.1080/17518423.2017.1282053
42. Cornec G, Drewnowski G, Desguerre I, et al. Determinants of satisfaction with motor rehabilitation in people with cerebral palsy: a national survey in France (ESPaCe). Ann Phys Rehabil Med. 2019.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.