")
Back to Journals » International Journal of General Medicine » Volume 15
Magnitude of Preoperative Anxiety and Associated Factors Among Adult Surgical Patients in Debre Berhan Comprehensive Specialized Hospital
Authors Shewangzaw Engda A, Belay Yigzaw H , Alemnew Engdaw N, Admasu Basha E , Adem A , Dargie Wubetu A , Misganaw Kebede W, Atinafu BT , Nigussie Tarekegn F , Abate Belew M
Received 8 April 2022
Accepted for publication 23 June 2022
Published 5 July 2022 Volume 2022:15 Pages 5999—6007
DOI https://doi.org/10.2147/IJGM.S369921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abayneh Shewangzaw Engda,1 Hailu Belay Yigzaw,1 Nigus Alemnew Engdaw,1 Elyas Admasu Basha,1 Ahmed Adem,2 Abate Dargie Wubetu,1 Worku Misganaw Kebede,3 Bantealem Tilaye Atinafu,3 Fetene Nigussie Tarekegn,3 Makda Abate Belew3
1Department of Psychiatry, College of Health Sciences and Medicine, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Nursing, Psychiatry Unit, College of Health Sciences and Medicine, Samara University, Samara, Ethiopia; 3Department of Nursing, College of Health Sciences and Medicine, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Abayneh Shewangzaw Engda, Debre Berhan University, P.O. Box 445, Debre Berhan, Ethiopia, Tel +251 9 20320375, Email [email protected]
Background: Anxiety is an un-pleasurable emotional state associated with psychophysiological changes in response to an intra-psychic conflict. The perioperative period is one of the worrying events for most surgical patients. Despite preoperative anxiety having many negative consequences on post-operative physical and mental health, no adequate information on the degree to which the preoperative period exposed clients to preoperative anxiety and its associated factors.
Objective: To assess the prevalence of preoperative anxiety and associated factors among adult surgical patients in Debre Berhan Comprehensive Specialized Hospital, Ethiopia.
Methods: Institution-based cross-sectional study was conducted from June 1, 2020, to August 30, 2020. State-Trait Anxiety Inventory Scale (S-STAI) was used to measure the level of pre-operative anxiety. A systematic random sampling technique was employed to collect the data. The data were entered to Epi-Data version 4.6 and exported to SPSS version 25 for data analysis. A statistically significant association was declared at a p-value less than 0.05.
Results: A total of 330 patients were enrolled in the study with a response rate of 93.2%. The prevalence of a high level of preoperative anxiety was 53.6% (95% CI (49.6– 58.7)). Being female 3.2 (2.19, 3.71) illiterate 4.1 (2.01, 15.39), fear of death 2.12 (1.30, 3.44), results of operation 2.60 (1.75, 4.18), postoperative pain 2.35 (1.37, 4.02), and surgical complication 1.9 (1.03, 12.13) were statistically significant factors.
Conclusion: Preoperative anxiety affects more than half of surgical patients which is a high and serious health burden. Additionally, this study revealed that being female, illiterate, fear of death, having a history of surgical complications and fear of complications, and fear of postoperative pain were significantly associated with preoperative anxiety. Assessing during the preoperative period helps to detect and ameliorate the problem. Preoperative counseling and informed consent taken as a prerequisite for surgery will help in reducing preoperative anxiety.
Keywords: preoperative period, preoperative anxiety, surgical patient, Ethiopia
Background
Anxiety is an un-pleasurable emotional state associated with psychophysiological changes in response to an intrapsychic conflict. Psychological changes consist of an uncomfortable feeling of impending danger, overwhelming awareness of being powerless, inability to perceive the unreality of the threat, a prolonged feeling of tension, and exhaustive readiness for the expected danger; physiological changes consist of increased heart rate, disturbed breathing, trembling, sweating, and vasomotor changes.1,2 It is also a response to external or internal stimuli with behavioral, emotional, cognitive, and physical symptoms.3 The preoperative period is one of the most stressful times and leads to mild to extreme anxiety, which causes a significant problem with the effectiveness of surgical treatment, and postoperative pain, poor wound healing, postoperative immunosuppression, hemodynamic problems in the intraoperative period, increased analgesic need and lower postoperative satisfaction, and slowed recovery.4–7 Surgery is one of the major treatments for traumatic life events which highly triggers anxiety during the preoperative period and provokes a challenging problem in the preoperative care of patients.8–10
The degree to which each client develops preoperative anxiety depends on many factors such as family concern, financial crises due to surgery, the patient’s susceptibility to preoperative anxiety, age, gender, past experiences with the surgery, fear of unawakening from anesthesia, fear of disability and death, educational status, type and extent of the proposed surgery, current health status, fear of dependency, and the outcome of surgery.10–13
Many studies across the world report on preoperative anxiety with a wide range of prevalence and it showed, that it was a major global problem during the surgical treatment. Studies across the world (both in developed and developing countries) revealed that the prevalence of preoperative anxiety ranges from 16.7% to 97%10,14–21 and the global pooled prevalence of preoperative anxiety was 48%.22
In Ethiopia, preoperative anxiety was found to be a significant public health problem, and its prevalence ranged from 47% to 70.3%,8,11,13,23–26 and the pooled prevalence was 55.54%.27
Despite preoperative anxiety having many negative consequences on post-operative physical and mental health, no adequate information on the degree to which the preoperative period exposed clients to preoperative anxiety, and its associated factors in Ethiopia, especially in the study area.
Therefore, this study aimed to assess the prevalence of preoperative anxiety and associated factors among adult surgical patients in Debre Berhan Comprehensive Specialized Hospital, Ethiopia. It will be vital for Debre Berhan Comprehensive Specialized Hospital’s surgical and psychiatry department to address the mental and physical health issues during the surgical treatment. Besides, it will be an input for policymakers and planners to indicate appropriate measures to tackle the problem of preoperative anxiety among surgical patients.
Methods
Study Design and Period
An institution-based cross-sectional study design was employed at Debre Berhan Comprehensive Specialized Hospital from June 1, 2020, to August 30, 2020.
Study Setting
The study was conducted at Debre Berhan Comprehensive Specialized Hospital which is located in North Shoa, Amhara, Ethiopia, and 130 km far from the capital city of Ethiopia, Addis Ababa. This is one of the oldest public hospitals in the country, which provides emergency, orthopedic, and elective surgeries with a surgical bed capacity of 36 from more than 900,000 catchment population.
Participants
All adult clients evaluated and scheduled for surgery in Debre Berhan Comprehensive Specialized Hospital were the source population. The study population consisted of clients scheduled for surgery at Debre Berhan Comprehensive Specialized Hospital that were available during the data collection period. However, those who are unable to communicate, are on anxiolytic medication, are preoperatively admitted into the intensive care unit, and are discharged within 24 hours after surgery were excluded.
Sample Size Determination
The sample size was computed using the single population proportion formula. A 70.3% proportion of preoperative anxiety was taken from a related study done in Ethiopia,24 95% confidence level, 5% margin of error, and 10% non-response rate were assumed to get the final sample size.

n = sample size,
Za/2 = the value under the normal standard table for the given confidence level,
p = estimated of the population proportion,
d = margin of error, and by using the above equation, the sample size was calculated as follows:
 , n = 320.836 ~ 321 by considering the non-response rate, the last sample included became 354.
, n = 320.836 ~ 321 by considering the non-response rate, the last sample included became 354.
Sampling Techniques
A systematic random sampling method was employed to select the study participants from Debre Berhan Comprehensive and Specialized Hospital. The total number of adult surgical patients in the hospital is estimated from the average value of the total admission from June to August 2019 (the previous year) and March to May 2020. To select the sampling unit at a regular interval (every Kth unit), dividing the total number of surgical patients by the designed sample size N/n=k (1112/354 = 3) and every third patient participates in the study until the estimated sample size was achieved.
Data Collection Tools and Procedure
An interviewer-administered structured questionnaire was employed to collect the data, which was prepared in the local language (Amharic). Two data collectors (BSc. Psychiatric nurse) and one supervisor (MSc. Psychiatry) were employed, and one-day training was given on data collection tools, content, and ethical issue.
Pre-operative anxiety was measured using State Version (Y-1) of the State-Trait Anxiety Inventory Scale (S-STAI), which is validated in Ethiopia.28 The State-Trait Anxiety Inventory Scale (S-STAI) has two subscales. The State Anxiety Scale (S-Anxiety) assesses the current state of anxiety, and the Trait Anxiety Scale (T-Anxiety) assess relatively stable aspects of “anxiety proneness”. Reliability and validity of the STAI were checked (Cronbach’s alpha = 0.86). The STAI has 40 items, 20 items for each (S-Anxiety and T-Anxiety subscales). Responses for the S-Anxiety scale assess the intensity of current feelings “at this moment”: 1) not at all, 2) somewhat, 3) moderately so, and 4) very much so. Responses for the T-Anxiety scale assess the frequency of feelings “in general”: 1) rarely, 2) sometimes, 3) often, and 4) almost always. A rating of 4 indicates the presence of a high level of anxiety for ten S-Anxiety items and a high rating indicates the absence of anxiety for the remaining ten S-Anxiety items. The scoring weights for the anxiety absent items are reversed. The scores of STAI range from a minimum of 20 to a maximum score of 80. A score of more than 44 on STAI is taken as significant anxiety, and the patient is categorized as having high anxiety (STAI score >44) while (STAI score ≤44) for low anxiety.13,24,26,29–31
Data Processing and Analysis
The collected data were entered into the Epi-data version 4.6 statistical program and exported to (SPSS) version 25 for further analysis. Descriptive analysis was carried out to describe the study participant’s socio-demographic characteristics and other relevant variables. Binary and multivariable logistic regression analyses were conducted to determine the significant association between the dependent and predictor variables. Independent variables with a p-value of <0.25 in the bivariate analysis were exported for multivariable analysis. In the final model, a significant association was declared at a p-value of 0.05 or less. The results were presented in text and tables with an adjusted odds ratio (AOR) and the corresponding 95% confidence interval.
A p-value of 0.05 or below is considered to declare a statistically significant association or effect. The results were presented in text, tables, and graphs based on the types of data as appropriate.
Result
Socio-Demographic Characteristics of Participants
A total of 330 patients were incorporated in this study with a 93.2% response rate. The study enrolled 181 (54.8%) female and 149 (45.2%) male participants. Whereas 70.9% of them are married, while 64.8% were learned up to secondary school (Table 1).
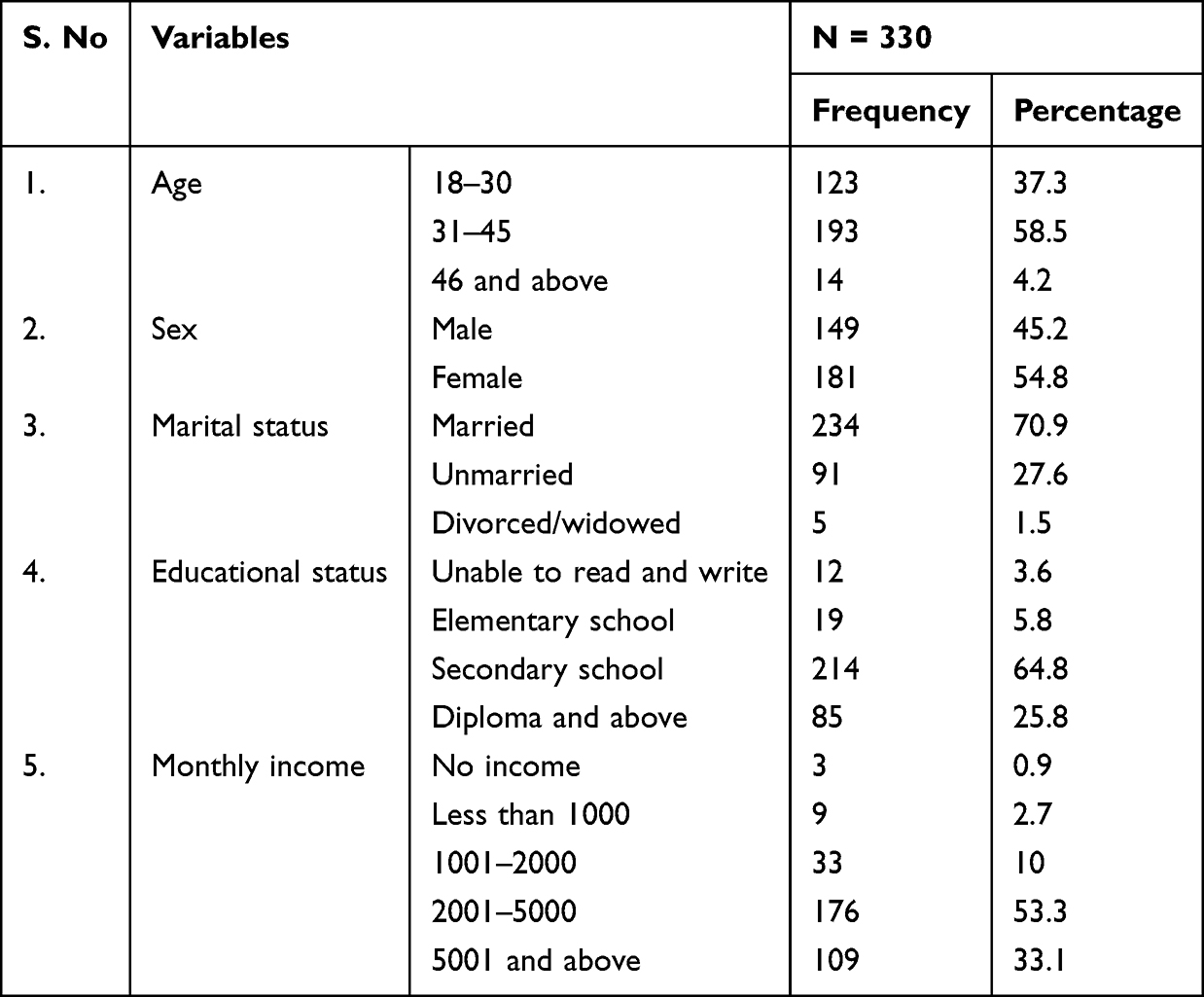 |
Table 1 Socio-Demographic Characteristics of Study Participants Among Adult Surgical Patients in Debre Berhan Comprehensive Specialized Hospital, 2020 |
Past Health Status and Awareness Related Information of Participants
Out of the total participants, 58.8% of them have a history of hospitalization and from them, only 17% experienced surgical operation. Around 5% of participants developed surgical complications (Table 2).
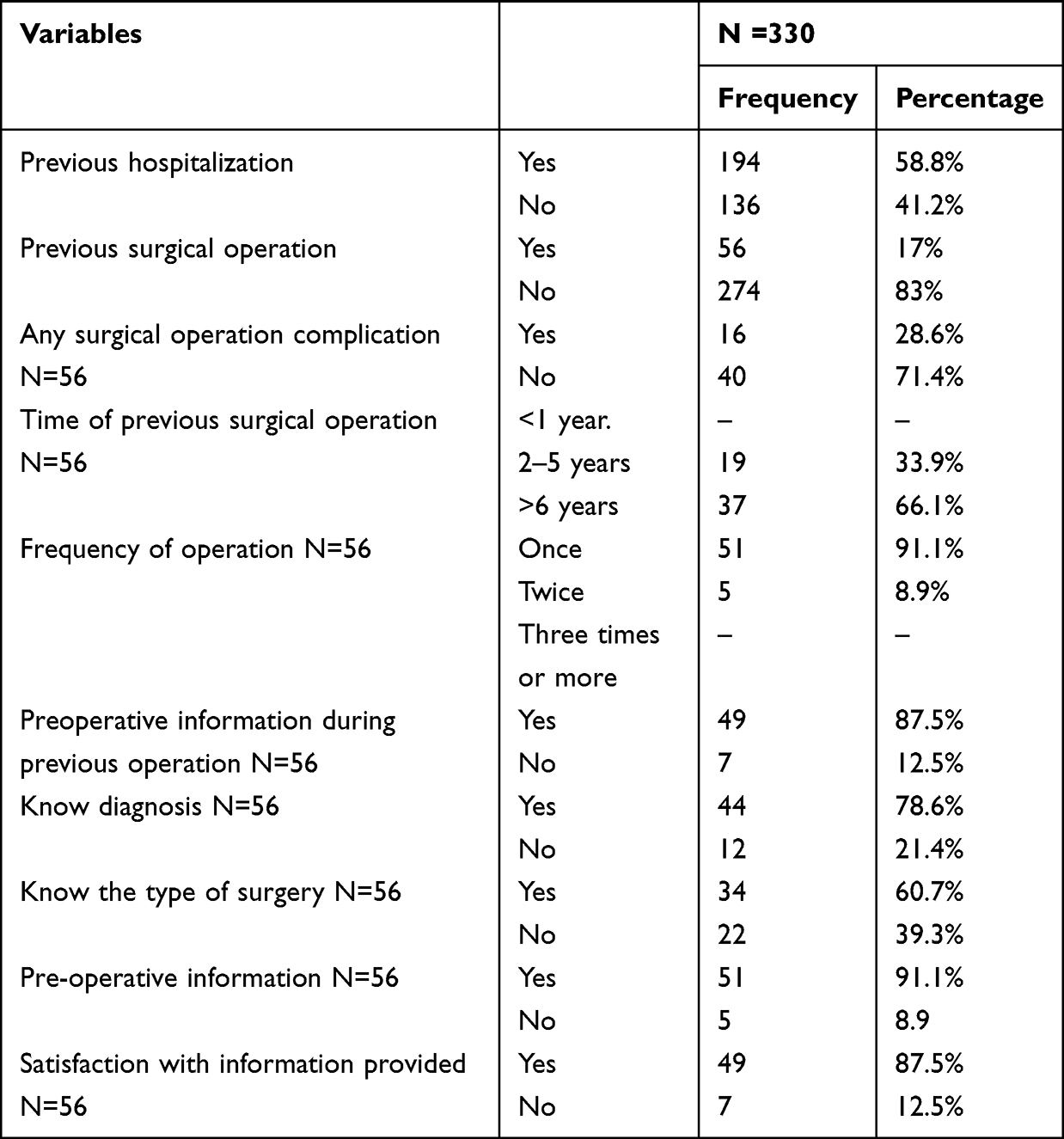 |
Table 2 Past Health Status and Awareness-Related Information of Participants Among Adult Surgical Patients in Debre Berhan Comprehensive Specialized Hospital, 2020 |
Psychological and Other Factors Characteristics of the Study Participants
Of the total participants, 148 (44.8%) experience fear of death, 121 (36.7%) are concerned about the results of the operation, and 55 (16.7%) develop excessive fear of financial loss due to operation (Table 3).
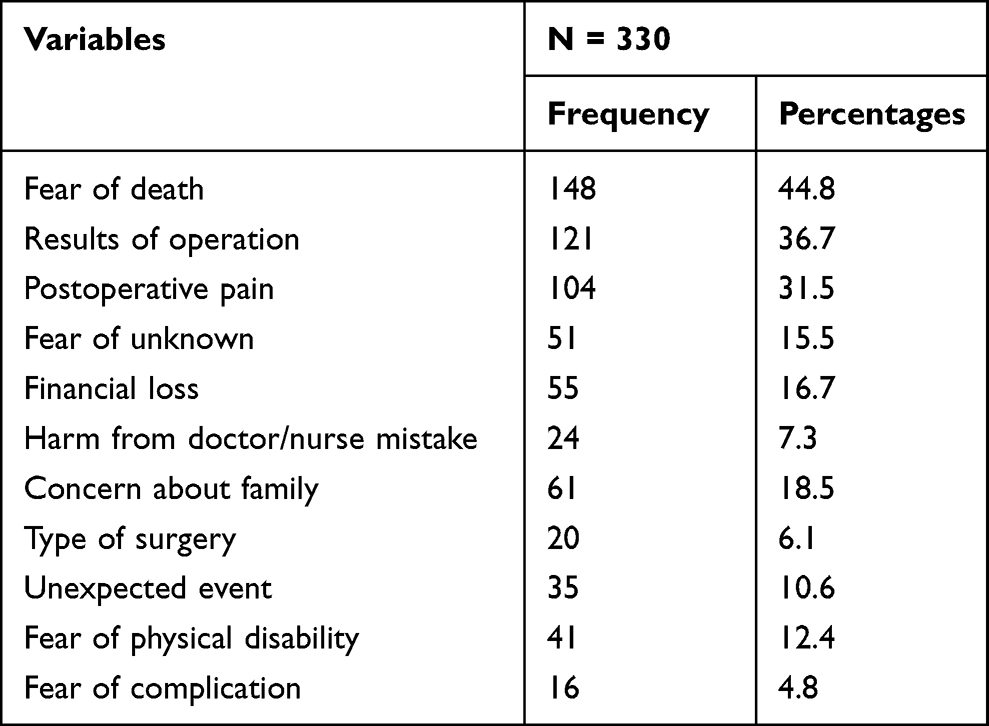 |
Table 3 Psychological and Other Factor Characteristics of the Study Participants Among Adult Surgical Patients in Debre Berhan Comprehensive Specialized Hospital, 2020 |
Prevalence of Pre-Operative Anxiety
The prevalence of preoperative anxiety among surgical patients was 53.6% (95% CI (49.6–58.7)) (high level of preoperative anxiety having S-STAI scores above 44). However, 153 (46.4%) of patients had a low level of anxiety.
Associated Factors of Preoperative Anxiety Among Patients Undergo Surgery
All the candidate variables which fulfilled a p-value less than 0.25 in the binary logistic regression were entered into multivariable analysis and a p-value <0.05 was considered significant.
Being Females was 3.2 times more likely to develop pre-operative anxiety as compared to males (AOR = 3.2, 95% CI, 2.19, 3.71).
Odd of pre-operative anxiety with a preoccupation with the result of surgery is 2.6 times higher compared to those who are not excessively concerned about the operational result (AOR = 2.6, 95% CI, 1.75, 4.18).
The uneducated surgical patients had 4.1 times more likely to develop pre-operative anxiety than they learned up to diploma and above (AOR = 4.1, 95% CI, 2.01, 15.39) (Table 4).
 |
Table 4 Bivariate and Multivariate Analysis-Associated Factors of Preoperative Anxiety Among Adult Surgical Patients in Debre Berhan Comprehensive Specialized Hospital, 2020 |
Discussion
The finding of this study revealed that the prevalence of preoperative anxiety was 53.6%. Associated factors were found to be female, illiterate, fear of death, excessive concern about operation results, fear of post-operative pain and complications, and history of surgical complications.
According to this study, the prevalence of pre-operative anxiety is higher as compared to studies done in Ethiopia (Yirgalem Hospital) (47%),8 Kenya (37%),20 China (27%),17 and India (31%).16 The discrepancy might be due to variation in study design, the ratio of male to female participants, sample size difference, and variation in an instrument; for example, study which was done in China used Hospital Anxiety and Depression Scale (HADS), but this study used State-Trait Anxiety Inventory Scale (S-STAI).
The finding of this study is comparable with the study done in Ethiopia (Wollo 48.3%),25 Nigeria (51%),19 whereas lower when compared to the study done in America (72.7%),15 Norway,32 Nepal (70.6%),10 Rumand (72.8%),21 and Ethiopia (Gonder (59.6%), Debre Markos (61%) and Jimma (70.3%)).11,13,24 The variation might be due to the variation in study participants; for instance, in studies done in America, the participants were only female, which increases the prevalence.
There are different associated factors responsible for pre-operative anxiety in clients undergoing a surgical procedure. This study revealed that the significant factors which affect pre-operative anxiety were being females who were 3.2 times more likely to develop pre-operative anxiety than males. This result was supported by a study conducted in Ethiopia,13 and Pakistan33 This might be due to metacognitive beliefs about the uncontrollability of worry and the belief that worry must be avoided. On the other hand, positive beliefs in worry are more common in girls, and punishment and meta-worry are being implemented as control strategies in females more than in males.34
Illiteracy is one of the significant risk factors for pre-operative anxiety. Surgical patients with no education attended were 4.1 times and learned up to primary school were 2.43 times more likely to encounter pre-operative anxiety than those who have a diploma and above. This finding was consistent with a study done in Ethiopia,13 and Turkey.35
Fear of death doubles the occurrence of preoperative anxiety and this is supported by a study done in Ethiopia.11 This might be due to pathophysiological responses such as hypertension and dysthymias and may cause patients to plan the surgery.
Concerning the result of an operation, it was found 2.6 times more likely to develop pre-operative anxiety than those who were not concerned about the result of the operation. This finding was consistent with a study done in Nepal,10 and Pakistan.33 Surgical patients who excessively fear post-operative pain are 2.35 times more likely to develop pre-operative anxiety. This finding is consistent with a study done in Ethiopia at Gonder,11 Pakistan,33 and America.5 Moreover, experienced fear of complication, and previous history of surgical complications are 4.1 and 1.9 times more likely to lead to preoperative anxiety than not experienced patients, respectively. This finding is supported by a study done in Ethiopia,13 and Pakistan.33 This is due to the psychological impact of previous direct or indirect surgical experience of complication and other related factors which escalate the occurrence of preoperative anxiety.
Strength of the Study
The present study lies in the fact that it is done using validated tool with a large sample size. Since there is no previous study done at the study area on preoperative anxiety, this research will serve as a vital guideline to prevent the problem and baseline for other studies.
Limitations of the Study
Since data collection was done by face-to-face interviews, preoperative anxiety may be underestimated due to social desirability bias. The study did not incorporate children and adolescents. Also, the study used a cross-sectional design, which hindered the accurate examination of the causal relationship between preoperative anxiety and its risk factors.
Conclusion
Preoperative anxiety affects more than half of surgical patients, which is a high and serious health burden. Additionally, this study revealed that being female, illiterate, fear of death, having a history of surgical complications and fear of complications, and fear of postoperative pain were significantly associated with preoperative anxiety. Assessing during the preoperative period helps to detect and ameliorate the problem. Preoperative counseling and informed consent taken as a prerequisite for surgery will help in reducing preoperative anxiety.
Abbreviations
S-STAI, State-Trait Anxiety Inventory Scale; AOR, Adjusted Odds Ratio; BSc, Bachelor of Science; CI, Confidence Interval; COR, Crude Odds Ratio; SPSS, Statistical Package for Social Science.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The study was conducted after ethical clearance was obtained from the Institutional Review Board (IRB) of Debre Berhan University Institute of Medicine and Health Sciences. An ethical clearance letter was submitted to Debre Berhan comprehensive specialized hospital manager, and an additional supportive letter was written, and it was given to the surgical department chairperson. Participants’ information was kept confidential and not shared with a third party. Written informed consent has been taken regarding their willingness to participate in the study. Participants that found to be at risk of pre-operative anxiety were referred to a psychiatric evaluation in the hospital. This study was conducted following the declaration of Helsinki in which the study involved human subjects.
Acknowledgments
First of all, we would like to thank Debre Berhan University College of Medicine and Health Sciences, Department of Surgical Nursing for giving us this chance. Then, we extend our deepest gratitude to our surgical and adult nursing staff for giving us materials, their guidance in our overall work, and also for their irreplaceable support and sharing of their experiences. Finally, we would like to express our sincere appreciation to the Debre Berhan comprehensive Specialized Hospital staff.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The whole required (material and humanitarian) cost for this research work was covered by Debre Berhan University.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Sadock BJ. Kaplan & Sadock’s Comprehensive Textbook of Psychiatry. New York; 2017:12754.
2. Sadock BJ. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. New York; 2015:1499.
3. Videbeck SVS. Psychiatric-mental health nursing; 2013.
4. Sigdel S. Perioperative anxiety. Clin Trials Patent. 2015;1(1):2.
5. Bayrak A, Sagiroglu G, Copuroglu E. Effects of preoperative anxiety on intraoperative hemodynamics and postoperative pain. J Coll Physicians Surg Pak. 2019;29(9):868–873. doi:10.29271/jcpsp.2019.09.868
6. Stamenkovic DM, Rancic NK, Latas MB, et al. Preoperative anxiety and implications on postoperative recovery: what can we do to change our history. Minerva Anestesiol. 2018;84(11):1307–1317. doi:10.23736/S0375-9393.18.12520-X
7. Tadesse M, Ahmed S, Regassa T, et al. Effect of preoperative anxiety on postoperative pain on patients undergoing elective surgery: prospective cohort study. Ann Med Surg. 2021;73:103190. doi:10.1016/j.amsu.2021.103190
8. Bedaso A, Ayalew M. Preoperative anxiety among adult patients undergoing elective surgery: a prospective survey at a general hospital in Ethiopia. Patient Saf Surg. 2019;13(1):1–8. doi:10.1186/s13037-019-0198-0
9. Bailey L. Strategies for decreasing patient anxiety in the perioperative setting. AORN J. 2010;92(4):445–460. doi:10.1016/j.aorn.2010.04.017
10. Ghimire R, Poudel P. Preoperative anxiety and its determinants among patients scheduled for major surgery: a hospital based study. J Anaesthesiol. 2018;6(2):57–60.
11. Woldegerima Y, Fitwi G, Yimer H, Hailekiros A. Prevalence and factors associated with preoperative anxiety among elective surgical patients at University of Gondar Hospital. Gondar, Northwest Ethiopia, 2017. A cross-sectional study. Int J Surg Open. 2018;10:21–29. doi:10.1016/j.ijso.2017.11.001
12. Celik F, Edipoglu IS. Evaluation of preoperative anxiety and fear of anesthesia using APAIS score. Eur J Med Res. 2018;23(1):1–10. doi:10.1186/s40001-018-0339-4
13. Mulugeta H, Ayana M, Sintayehu M, Dessie G, Zewdu T. Preoperative anxiety and associated factors among adult surgical patients in Debre Markos and Felege Hiwot referral hospitals, Northwest Ethiopia. BMC Anesthesiol. 2018;18(1):1–9. doi:10.1186/s12871-018-0619-0
14. Majumdar JR, Vertosick EA, Cohen B, Assel M, Levine M, Barton-Burke M. Preoperative anxiety in patients undergoing outpatient cancer surgery. AsiaPac J Oncol Nurs. 2019;6(4):440–445. doi:10.4103/apjon.apjon_16_19
15. Maheshwari D, Ismail S. Preoperative anxiety in patients selecting either general or regional anesthesia for elective cesarean section. J Anaesthesiol Clin Pharmacol. 2015;31(2):196. doi:10.4103/0970-9185.155148
16. Vadhanan P, Tripaty DK, Balakrishnan K. Pre-operative anxiety amongst patients in a tertiary care hospital in India – a prevalence study. J Society Anesthesiol Nepal. 2017;4(1):5–10. doi:10.3126/jsan.v4i1.17377
17. Wang Y, Shen J, Lu J, Yang X. Preoperative anxiety and depression in patients undergoing cardiac surgery and related influencing factors. Zhonghua Yi Xue Za Zhi. 2008;88(39):2759–2762.
18. Almalki MS, Hakami OAO, Al-Amri AM. Assessment of preoperative anxiety among patients undergoing elective surgery. Egypt J Hosp Med. 2017;69(4):2329–2333. doi:10.12816/0041537
19. Akinsulore A, Owojuyigbe AM, Faponle AF, Fatoye FO. Assessment of preoperative and postoperative anxiety among elective major surgery patients in a tertiary hospital in Nigeria. Mid East J Anaesthesiol. 2015;23(2):235–240.
20. Chanda C. Assessment of preoperative anxiety amongst patients presenting for elective surgery at the Kenyatta National Hospital. Kenya: University of Nairobi; 2012.
21. Ryamukuru D, Ndateba I, Mukamana D, Mukantwari J, Adejumo O, Collins A. Assessment of anxiety in patients awaiting surgery in a referral hospital in Rwanda. Rwanda J Med Health Sci. 2019;2(2):112–117. doi:10.4314/rjmhs.v2i2.6
22. Abate SM, Chekol YA, Basu B. Global prevalence and determinants of preoperative anxiety among surgical patients: a systematic review and meta-analysis. Int J Surg Open. 2020;25:6–16. doi:10.1016/j.ijso.2020.05.010
23. Takele G, Neme A, Ayelegne D, Boru B. Preoperative anxiety and its associated factors among patients waiting elective surgery I St. Luke’s Catholic Hospital and Nursing College, Woliso, Oromia, Ethiopia 2018. Emerg Med Crit Care. 2020;4:21–27.
24. Nigussie S, Belachew T, Wolancho W. Predictors of preoperative anxiety among surgical patients in Jimma University specialized teaching hospital, South Western Ethiopia. BMC Surg. 2014;14(1):1–10. doi:10.1186/1471-2482-14-67
25. Wondmieneh A. Preoperative anxiety and associated factors among adult elective surgery patients in North Wollo Zone, Northeast Ethiopia. Open Access Surg. 2020;13:85–94. doi:10.2147/OAS.S285562
26. Ferede YA, Bizuneh YB, Workie MM, Admass BA. “Prevalence and associated factors of preoperative anxiety among obstetric patients who underwent cesarean section”: a cross-sectional study. Ann Med Surg. 2022;74:103272. doi:10.1016/j.amsu.2022.103272
27. Yohanes YB, Yazew KG. Preoperative anxiety in Ethiopia: a systematic review and meta-analysis; 2020.
28. Mulatu MS. Psychometric properties of scores on the preliminary Amharic version of the State-Trait Anxiety Inventory in Ethiopia. Educ Psychol Meas. 2002;62(1):130–146. doi:10.1177/0013164402062001009
29. Millar K, Jelicic M, Bonke B, Asbury A. Assessment of preoperative anxiety: comparison of measures in patients awaiting surgery for breast cancer. Br J Anaesth. 1995;74(2):180–183. doi:10.1093/bja/74.2.180
30. Kim W-S, Byeon G-J, Song B-J, Lee HJ. Availability of preoperative anxiety scale as a predictive factor for hemodynamic changes during induction of anesthesia. Korean J Anesthesiol. 2010;58(4):328. doi:10.4097/kjae.2010.58.4.328
31. Ayele B, Tadesse M, Tilahun R, Nega B. Translation of the Amsterdam Preoperative Anxiety and Information Score (APAIS) into the amharic version and its validation for evaluation of preoperative anxiety. Ethiop J Health Sci. 2021;31(2). doi:10.4314/ejhs.v31i2.18
32. Haugen AS, Eide GE, Olsen MV, Haukeland B, Remme ÅR, Wahl AK. Anxiety in the operating theatre: a study of frequency and environmental impact in patients having local, plexus or regional anaesthesia. J Clin Nurs. 2009;18(16):2301–2310. doi:10.1111/j.1365-2702.2009.02792.x
33. Jawaid M, Mushtaq A, Mukhtar S, Khan Z. Preoperative anxiety before elective surgery. Neurosci J. 2007;12(2):145–148.
34. Bahrami F, Yousefi N. Females are more anxious than males: a metacognitive perspective. Iran J Psychiatry Behav Sci. 2011;5(2):83.
35. Erkilic E, Kesimci E, Soykut C, Doger C, Gumus T, Kanbak O. Factors associated with preoperative anxiety levels of Turkish surgical patients: from a single center in Ankara. Patient Prefer Adherence. 2017;11:291. doi:10.2147/PPA.S127342
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.