")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Magnitude of Overweight and Obesity and Associated Factors Among Public and Private Secondary School Adolescent Students in Mekelle City, Tigray Region, Ethiopia, 2019: Comparative Cross-Sectional Study
Authors Andargie M, Gebremariam K, Hailu T, Addisu A, Zereabruk K
Received 30 July 2020
Accepted for publication 4 November 2020
Published 2 March 2021 Volume 2021:14 Pages 901—915
DOI https://doi.org/10.2147/DMSO.S262480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Antonio Brunetti
Malede Andargie,1 Kidanu Gebremariam,2 Tesfay Hailu,2 Alefech Addisu,2,3 Kidane Zereabruk4
1Department of Epidemiology, Tigray Regional Health Bureau, Kafta Humera Health Office, Humera, Tigray, Ethiopia; 2School of Public Health, College of Health Sciences and Comprehensive Specialized Hospital, Mekelle University, Mekelle, Tigray, Ethiopia; 3Ethiopia Ministry of Health, Addis Ababa, Ethiopia; 4School of Nursing, College of Health Sciences and Comprehensive Specialized Hospital, Aksum University, Aksum, Tigray, Ethiopia
Correspondence: Kidane Zereabruk
School of Nursing, College of Health Sciences and Comprehensive Specialized Hospital, Aksum University, Aksum, Tigray, 298, Ethiopia
Tel +251 914591272
Email [email protected]
Background: Overweight and obesity emerged as one of the most serious public health concerns in adolescents. Overweight and obesity are problems of not only high income but also low-middle income countries. Therefore, this study aimed to assess the magnitude and associated factors of overweight and obesity among public and private secondary school adolescents in Mekelle city, Tigray, Ethiopia, 2019.
Materials and Methods: A school-based comparative cross-sectional study was conducted in Mekelle city, from April to May 2019. A multi-stage sampling technique was used to select 858 participants. Chi-square test was checked before bivariate logistic regression analyses. All variables at a p-value < 0.25 in bivariate logistic regression were entered into a multivariable logistic regression to determine the association between a set of independent variables with the dependent variable. Finally, statistical significance was declared at a p-value < 0.05.
Results: The magnitude of overweight and obesity in private and public schools were 11.8% and 3.9%, respectively. Consuming dinner not daily [AOR=5.3:95% CI=1.93– 14.6] and working moderate-intensity sports at least 10 minutes/day continuously [AOR=0.19:95% CI=0.04– 0.9] were associated factors of overweight and obesity in public school adolescent students. Being female [AOR=2.03:95% CI=1.08– 3.8], time taken from home to public physical activities ≤ 15 minutes [AOR=3.6:95% CI=1.13– 11.51], using transport from school to home [AOR=2.2:95% CI=1.06– 4.18] and good knowledgeable adolescents [AOR=0.5:95% CI=0.27– 0.9] were associated factors of overweight and obesity in private schools.
Conclusion: The magnitude of overweight and obesity was higher among private schools. Consuming dinner not daily and working moderate-intensity sports at least 10 minutes/day continuously were the associated factors for the occurrence of overweight and obesity in public school adolescent students. Being female, time taken from home to public physical activity facilities ≤ 15 minutes, using transport from school to home, and nutritional knowledge status of adolescents were associated factors for overweight and obesity in private school adolescent students.
Keywords: overweight and obesity, Mekelle City, secondary school adolescents, magnitude, associated factors
Background
Overweight and obesity are defined as abnormal or excessive fat accumulated that may impair health. 1 Overweight and obesity in adolescents can be assessed using body mass index (BMI) cut-off points of world health organization (WHO), communicable disease control (CDC), and international obesity task force (IOTF).2,3 Virtually, all age groups and socioeconomic classes of the population are affected by the consequences of overweight and obesity. From these adolescents are one of the most vulnerable groups to overweight and obesity.4
According to WHO definitions, adolescences are age groups between 10 and 19 years5 which comprise up to 1.2 billion (20%) of the world’s population and more than half of them live in Asia and Sub-Saharan Africa and about 25% of the populations of Ethiopia are adolescents.6,7 During the adolescence period, adolescents gain up to 50% of their adult weight, 20% or more than that of their adult height, and 50% of their adult skeletal mass.8
Adolescents overweight and obesity is critical which strongly track into adulthood and having a great chance to develop non-communicable diseases like type 2 diabetes mellitus and cardiovascular diseases.9,10
Worldwide, the trend of overweight and obesity and its impact have increased.11 Currently, overweight and obesity are problems of not only high income but also low-middle income countries.12,13
Adolescents overweight and obesity strongly track into adulthood and having a great chance to develop non-communicable diseases like type 2 diabetes and cardiovascular diseases.14
Overweight and Obesity among adolescents have emerged as one of the most serious public health concerns in the 21st century.15 The magnitude and the severity of this problem are reached at an alarming rate and more than quadrupled in the past three decades in adolescents.11,16
According to the 2017 world health organization fact sheets over 340 million children and adolescents aged 5–19 years were overweight and obese. The prevalence of overweight and obesity has risen from 4% to 18% and from 1% to 7% with 18% and 19% among adolescents, respectively.12,13 Ethiopia is one of the low-income countries showing the experience of a shift from underweight to overweight and obesity, particularly in urban settings.17 Some studies in Ethiopia indicated that overweight and obesity were found to be increased.18 According to the 2016 EDHS report, the prevalence in the Tigray region is increasing especially in females who were more than two folds.7
In Ethiopia, studies showed that several factors such as sedentary life, economic changes, physical inactivity inside and outside schools, taking a high proportion of saturated fats, high-fat snacks, and sweetened beverages may contribute toward the occurrence of obesity and overweight among adolescents.6,19–21
Overweight and obesity have negative impacts on both the physical and psychological well-being of adolescents.22 Overweight and obesity are risk factors for cardiovascular disease, insulin resistance, cancer-related problems, and type 2 diabetes mellitus.14 It contributes to premature mortality and long-term morbidity.23,24 Overweight and obesity have also increased the economic burden, medical expenses, and it can reduce life expectancy by as many as 20 years.11,25
Despite the physical education session given in all Ethiopian secondary schools, the prevalence of overweight and obesity among adolescents is increasing.20,26,27 Recently, there was no well-documented information about overweight and obesity and its associated factors in Mekelle city secondary school adolescent students. Therefore, this study aimed to assess the magnitude and associated factors of overweight and obesity among public and private secondary school adolescents in Mekelle city, Tigray region, Northern Ethiopia, 2019.
Methods and Materials
Study Design, Setting, and Period
A school-based comparative cross-sectional study design was conducted from April to May 2019 in Mekelle public and private schools, which is located 783 kilometers from the capital city of Ethiopia, Addis Ababa. According to the 2018 zonal educational office statistics, there were 9 and 15 public, private secondary schools, respectively. Currently, there are a total of 20,836 students (9853 from public and 10,983 from private’s schools).
Inclusion and exclusion Criteria
Adolescents aged between 10 and 19 years old in Mekelle city for the academic year 2019–2020 who were attending 9th−12th grade in public and private schools were enrolled in this study. All students who were attending public and private schools during the study period were included. But those who had an obvious visible physical deformity and pregnant students were excluded from the study.
Sample Size Determination
The sample size was determined using Epi info software version 7.2.2.16 with the following assumptions, P1= (4.3%),28 from public school adolescents, P2= (12.7%),28 from private school adolescents, Z1-α/2=1.96 at 95% level of confidence, and with 80% of power.
r=the proportion of n1 to n2 was 1 to 1
This yields an estimated sample size of 390. By adding a 10% non-response rate, the sample size was 429, and considering design effect 2 which gives 858. Therefore, the final sample size was 858.
Sampling Methods and Procedures
A three-stage random sampling technique was used to select the study participants. Among the 23 high schools which were schooling students from grades 9–12, 50% of schools were considered into sampling. Using a multi-stage sampling method, 12 schools (four public- and eight private schools) were selected. The sample size for each grade was allocated proportionally to size by considering the sum of the student size in each grade of all schools in each category.
However, in each class, a systematic random sampling method was employed in which the students were given numbers serially according to their classroom registrations thereby giving each student an equal chance. In the case of absentees, the next roll number was included. Finally, simple random sampling was used to select the first number, and thereafter students were picked at a regular interval (sample interval) so as to meet the sample size requirement in the school. This sampling interval (SI) was determined by dividing the total number of students in the selected class by the sample size.
Study Variables
Dependent Variable
Overweight and obesity status
Independent Variables
Age, school type, sex, socio-economic status, grade level, religion, family size, parent’s education, patterns’ jobs, home ownership, and order of birth.
Dietary intake, skipping meal, different food items consumption frequency, daily meal frequency (eating habit), eating outside home, and types of foods served in school cafeterias.
Physical activity sessions per week, home to school distance, proximity of public physical activity, facilities at home, having a television in the bed room, and time spent on television, physical activity level, mode of transport, work beside education and school physical education club.
Data Collection Tools and Procedures
We used food frequency questionnaire (FFQ) to assess the nutritional determinants and WHO Global Physical Activity Questionnaire (GPAQ)3 to assess physical activity and sedentary behavior of adolescents. The GPAQ was developed by WHO for physical activity surveillance in developing countries like Ethiopia. Both questionnaires were modified according to the objective of the study.
Quantitative data were collected using a pretested structured self-administered questionnaire which was adopted from published papers. Semi close-ended questionnaire was used as a data collection tool. Data were collected by trained college diploma completed nurses. Eight data collectors and two supervisors were participated to undertake the interview and the overall activity was coordinated by the principal investigator.
Anthropometric Measurements
The adolescent’s height and weight were measured using standardized and calibrated equipment of stadiometer Seca Germany. Adolescent’s height was measured with bare foot, removing any pins and braids from the hair that could affect the measurement. Weight of adolescents was measured with light clothing of school uniform and recorded to nearest 0.1 kg using UNICEF Seca digital weighing scale (Germany).29
The scales were carefully handled and calibrated every five adolescents.30 The measurement was performed by two data collectors for a single respondent the other researcher would take the measurements and the second data collector would record for the avoidance of inter-observer bias.
Data Quality Assurance
Data quality was ensured by giving training for data collectors, supervisors and they were provided day-to-day supervision during the whole period of data collection. First, the questionnaire was developed in English then it was translated into Tigrigna (local language) and back-translated to English by language experts. The final draft of the questionnaire was pretested on 10% (88) of other secondary school adolescents who have not participated in the study for completeness and appropriateness to the local context. Based on the findings necessary amendments have done. Every questionnaire was checked by both data collectors and supervisors for its completeness and accuracy. Verification of measurements was done in 10% of respondents by the principal investigator after data collections were finished to check the consistency of inter-observer and between day measurement differences.
Data Analysis Procedures
Data were entered into Epi info version 7.1.2 and exported to SPSS version 22 for statistical analysis. Anthropometric data were entered and analyzed using the WHO Anthro-plus software.
Descriptive statistics were expressed using frequency, percentage, mean (SD), median (IQR). A Chi-square test was checked before the bivariate logistic regression analysis. The bivariate logistic regression analysis was carried out using crude odds ratio to identify candidate variables for multivariable logistic regression in determining factors associated with overweight and obesity. All variables at p-value <0.25 in bivariate logistic regression were entered into a multivariable logistic regression to determine the association between a set of independent variables with the dependent variable. The model fitness was checked using the Hosmer-Lemeshow goodness of fit test which was fitted (0.09). Variance inflation factor (VIF) was used to assess multicollinearity between the independent variables and all continuous variables were checked for normal distribution using the normality test. The odds ratio was estimated at a confidence interval of 95% to show the strength of an association and statistical significance was declared at a p-value <0.05. Finally, the data were presented with frequency, proportion, figures and tables.
Operational Definition
Overweight and Obesity
Overweight and obesity was determined using body mass index per age per gender (BMI) (a measure of weight adjusted for height, calculated as weight in kilogram divided by the square of height in meter (kg/m2) with BMI for age Z-score (BAZ) ≥ +1SD BMI per age were classified as overweight and obesity.3,21
Knowledge About Overweight and Obesity Among Adolescents
Eleven knowledge questions were used to assess knowledge towards overweight and obesity, each of which was scored 1 point for those who scored were above mean and zero for those who scored below or equal to mean. The overall knowledge score was calculated by adding up the scores for each respondent across all the eleven questions. Those who scored above mean were taken as having good knowledge while those who scored less than or equal to mean were considered as having poor knowledge about overweight and obesity.20
Results
Socio-Demographic Characteristics
A total of 858 adolescents participated in this study with a response rate of 99.4%. Half of the respondents were from private schools. The mean and standard deviation age of the study participants was 16.5 ± 1.45 with 16±1.37 in private and 16.99±1.37 years in public school adolescents. More than 70% (605) of students belonged to the age group of 14–17 years in both schools.
There were 208 (49.1%) and 215 (49.9%) female students in private and public schools, respectively. Private school adolescent student’s families have higher educational status compared to public school students. From the total, 182 (42.9%) in private and 251 (58.5%) in public schools had ≤5 total family size. Majority of the respondents 387 (91.3%) among private and 414 (96.5%) among public schools adolescent students were orthodox religious followers. Ninety (21%) respondents’ mothers were merchants and 89 (20.9%) civil servants in public schools, whereas 122 (28.8%) respondents’ mothers were merchant and 90 (21.2%) civil servants in private schools (Table 1).
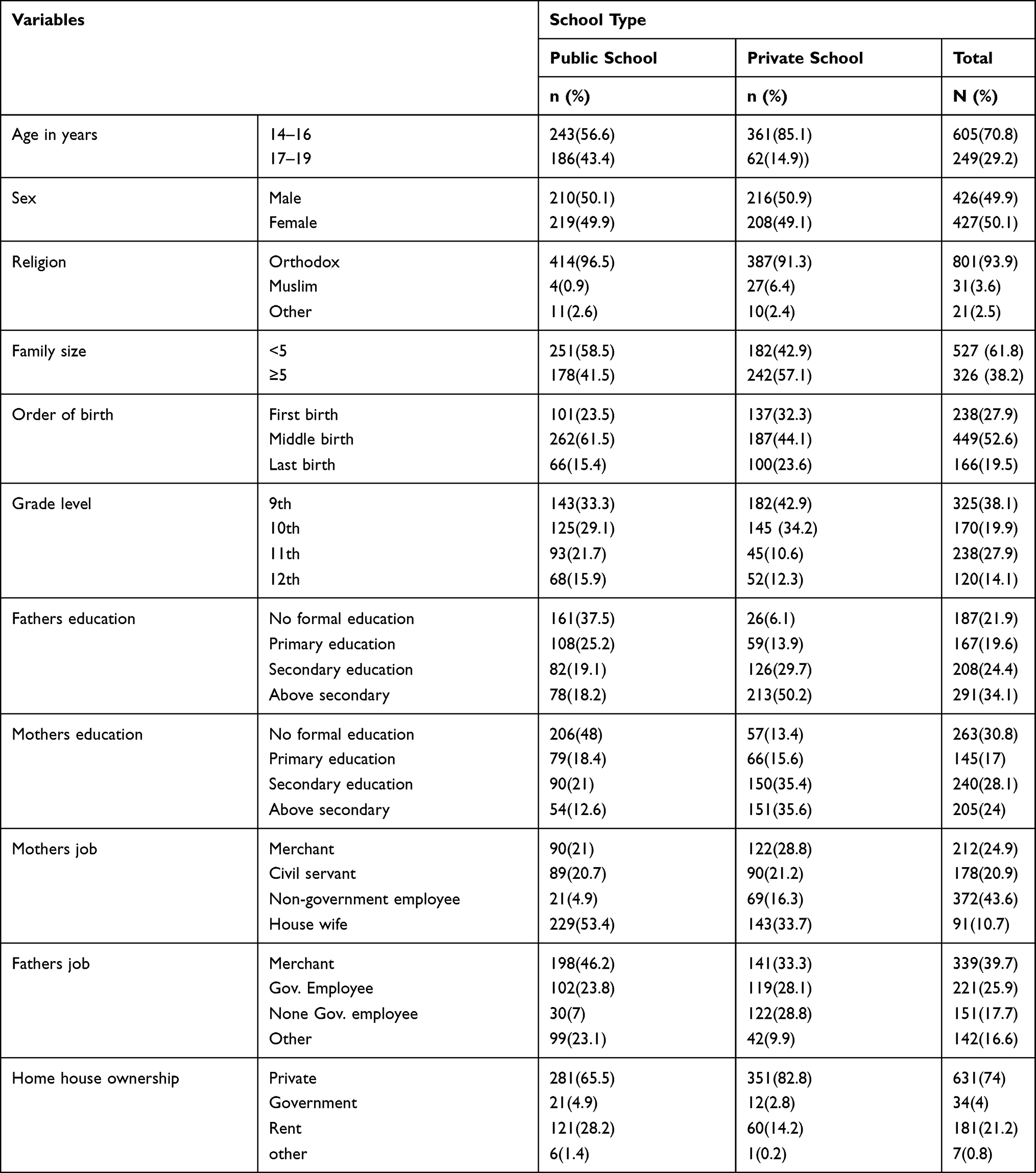 |
Table 1 Socio-Demographic Characteristics of Public and Private Secondary School Adolescent Students in Mekelle City, November, 2019 |
Nutritional Status of Adolescents (Different Food Items Consumption Frequency)
Of 378 (44.3%) respondents, 232 (54.7%) in private school and 146 (34%) in public school students consumed cereals and bread food items ≥ twice per day. Of 268 (31.4%) respondents, 117 (27.6%) of private and 147 (34.3%) of the public students consume vegetables once a day and 260 (30.5%) respondents, 157 (37%) of private, 103 (24%) of public students consumed fruits 2–4 per week.
Out of the total respondents, 117 (27.3%) of the public schools and 105 (24.8%) of private schools were eating milk and its derivatives once a day. From 267 (31.3%) respondents, 157 (37%) of private, 110 (25.6%) of public school students took eggs 2–4 times per week. Of 125 (14.7%) respondents, 162 (19%) of private, 71 (16.6%) of public school students took oil and fat once per day but 349 (41%) respondents, 188 (34.4%) of private, 163 (38%) of public students they consumed oil and fat 1–3 per month (Table 2).
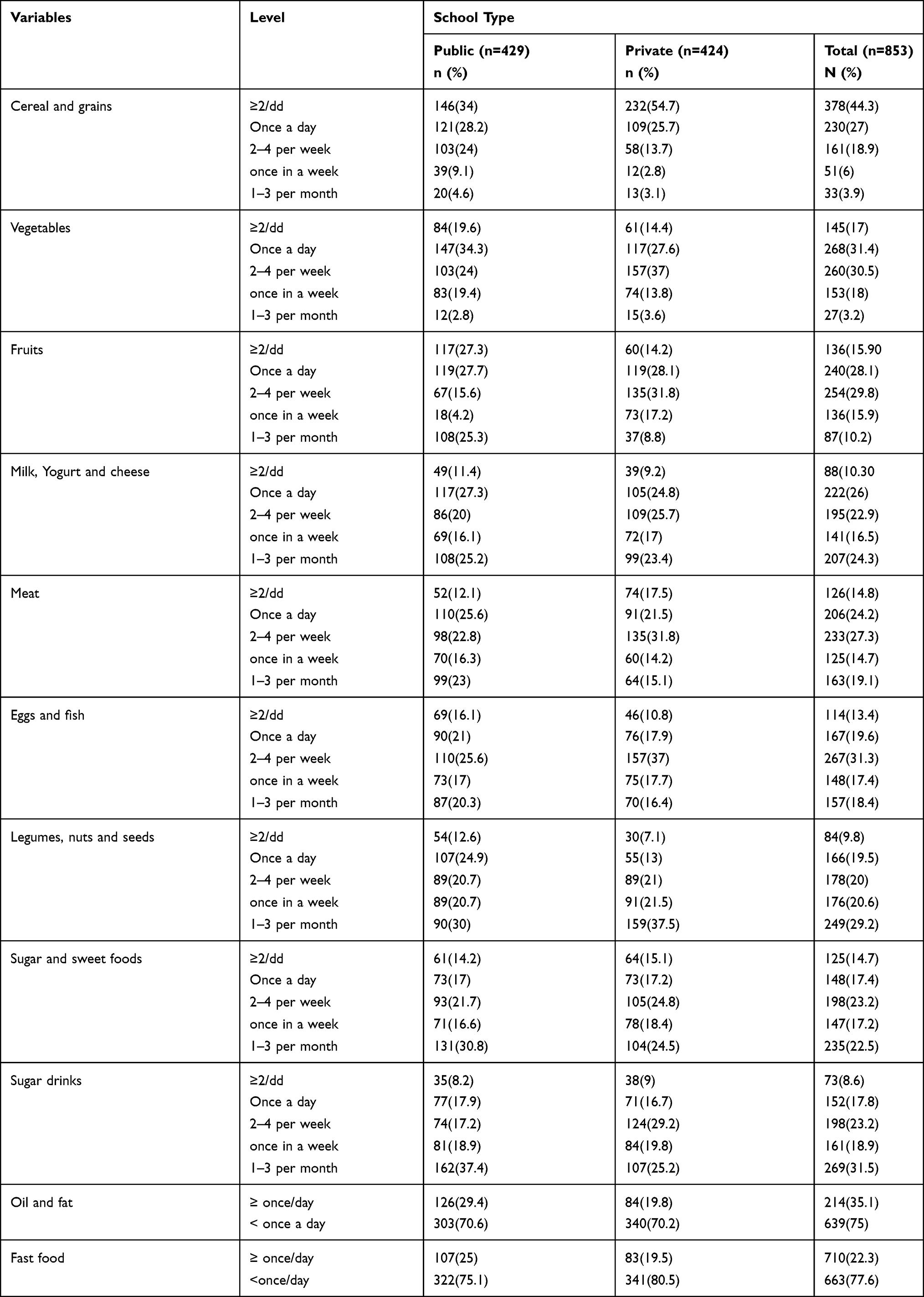 |
Table 2 Different Food Item Consumption Frequency of Adolescents Among Public and Private Students of Mekelle City, November, 2019 |
Frequency of Meal Pattern and Physical Activity
Of 427 (50.1%) study participants, 163(38.4%) of private, 264(61.5%) of public school adolescents were consuming meal frequency ≤3 per day. More than 40% 171(40.3%) from private and 149(34.7%) from public school students were sleeping more than 8 hours per day and 206(48.6%) of private school and 37(78.6%) of public school respondents were walked from home to school or vice versa on foot. Students from private schools were used higher total physical activities level than public schools which accounts for 258(60.8%), and 64(14.9%) respectively. Sixty percent students from the private schools and 44.5% students from the public schools were receiving public physical activity facilities from home ≤15 minutes distance. (Table 3)
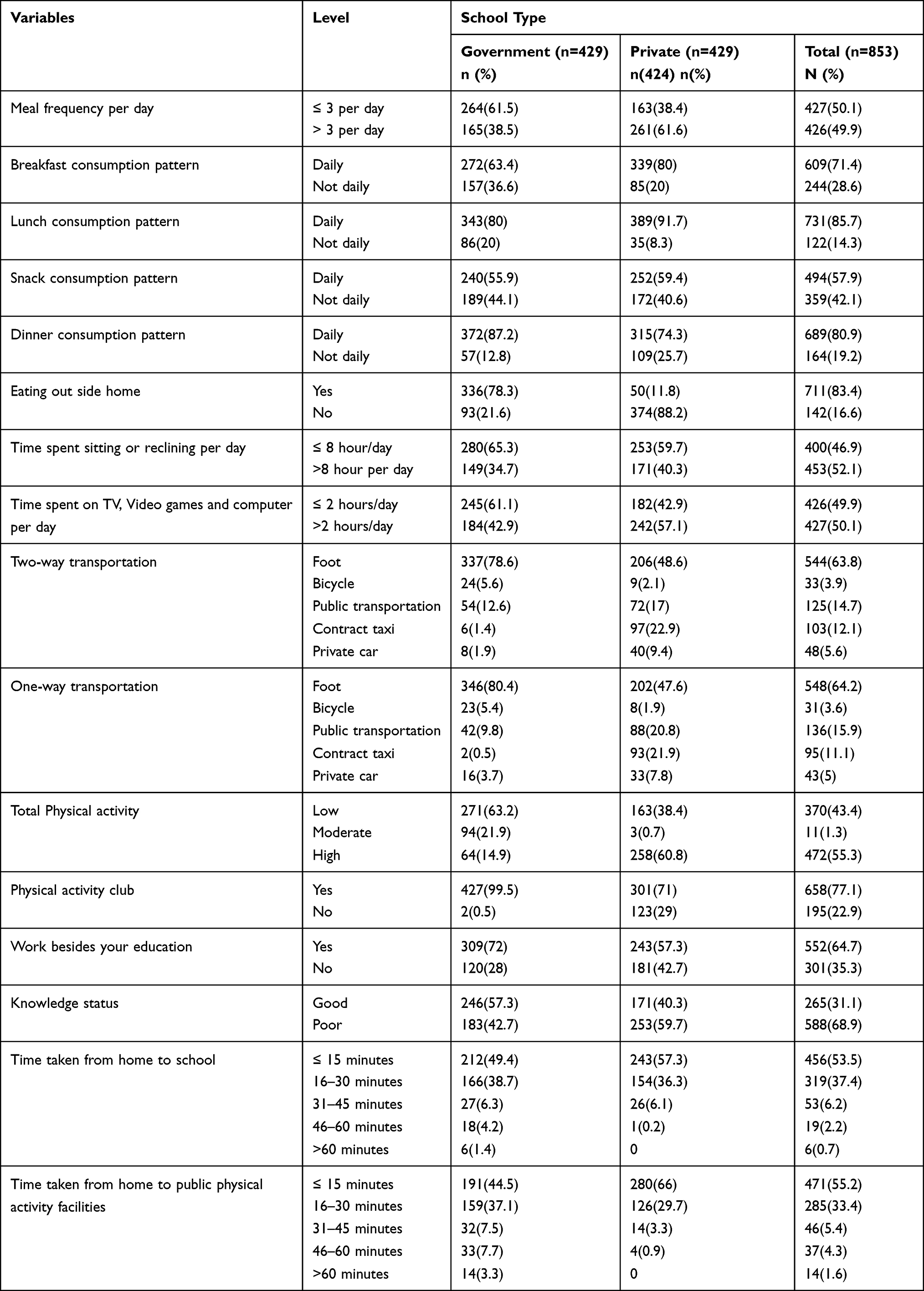 |
Table 3 Frequency of Meal, Sedentary Lifestyle and Physical Activity of Adolescent Students Among Public and Private Secondary Schools in Mekelle City November, 2019 |
Nutritional Status of Adolescents in Private and Public School Adolescent Students
Based on the WHO 2007 reference chart, the BAZ of the study population slightly deviated to the left which indicates most participants were thin and severely thin as compared with WHO references (Figure 1).
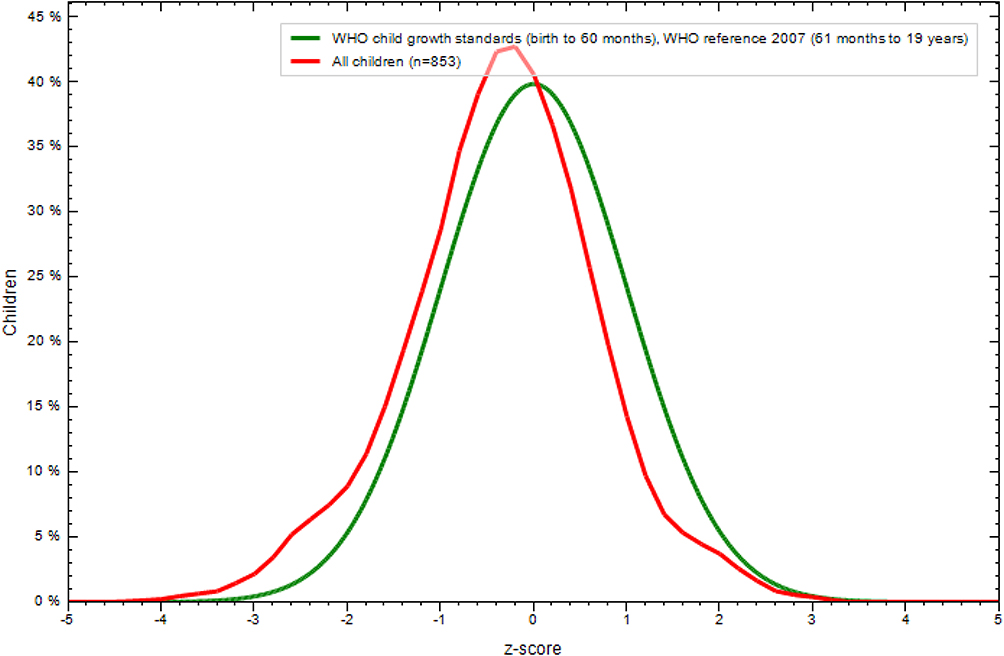 |
Figure 1 Comparison of BMI for age Z-score (BAZ) of high school adolescent students with the 2007 WHO growth reference population in Mekelle city November, 2019. |
Females were more overweight and obese and males were thinner and severely thin than females (Figure 2).
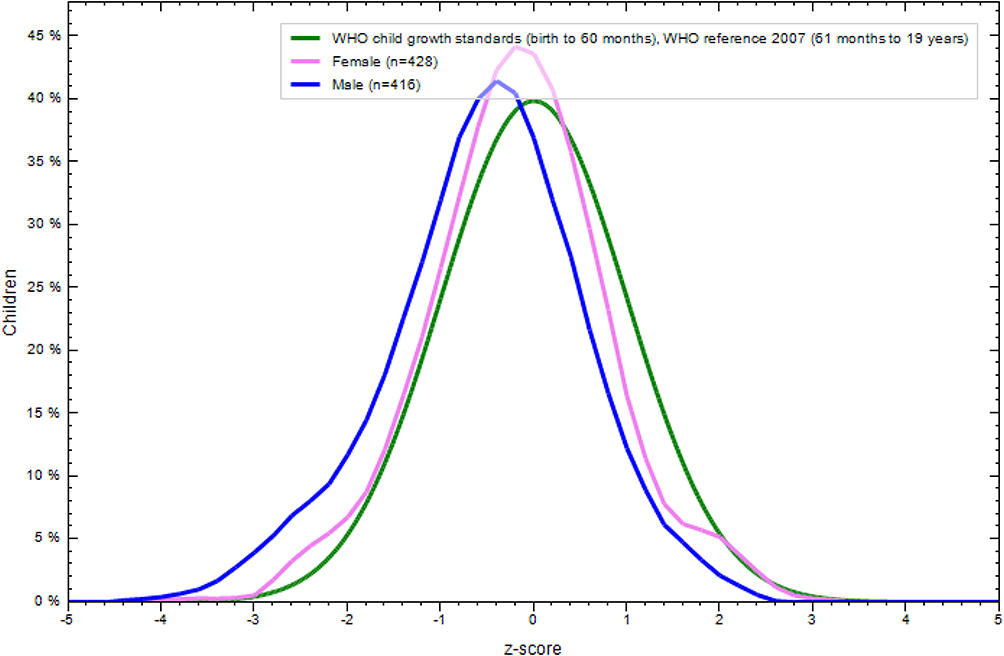 |
Figure 2 Comparison of BMI for age Z-score (BAZ) of the study population classified by sex with the 2007 WHO growth reference population in Mekelle city November, 2019. |
Magnitude of Overweight and Obesity
The overall magnitude of overweight and obesity was found to be 7.9% (95% CI=6.1–9.7%) with magnitude of overweight 55 (6.5%) (95% CI=5.0–8.1%) and obesity 12 (1.4%) (95% CI=0.7–2.2%) among high school adolescents. According to school type magnitude of overweight and obesity was 11.8% (95% CI=8.7–15.3%) in private and 3.9% (95% CI=2.1–5.9%) in public schools (Table 4).
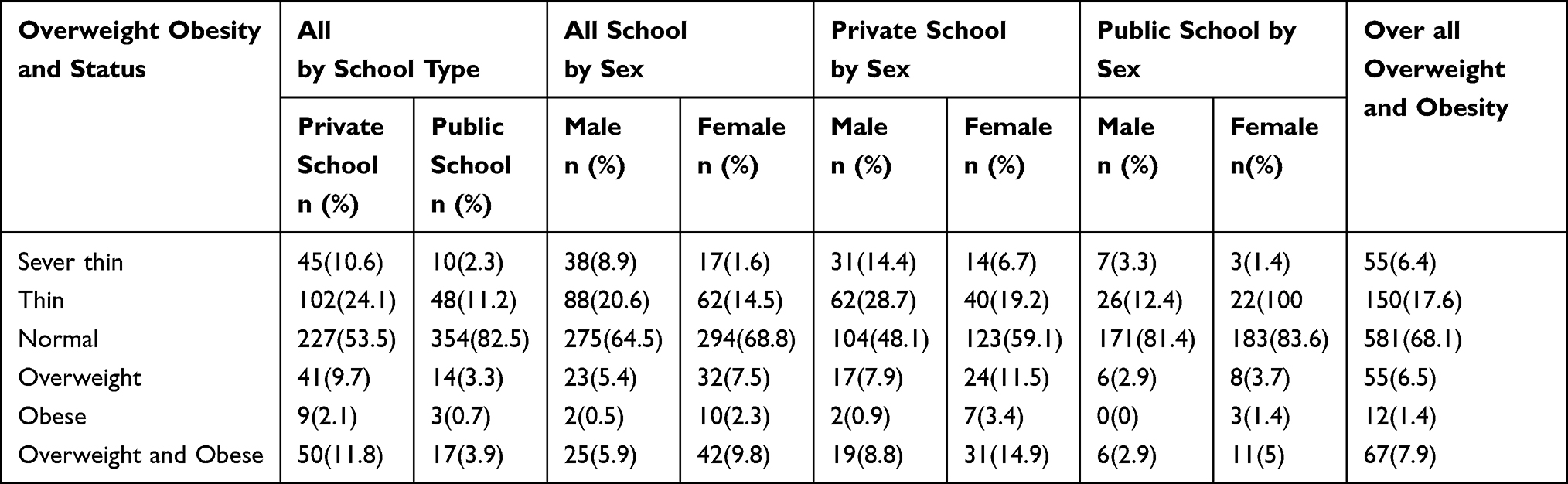 |
Table 4 Description of School and Sex Specific Magnitude of Overweight and Obesity Among Private and Public Schools and All Secondary School Adolescent Students in Mekelle City November, 2019 |
Factors Associated with Overweight and Obesity in Public and Private School Adolescent Students (Model-I and Model-II)
Sex, mother’s education, snack consumption pattern, dinner consumption pattern, total physical activity, work besides education, meat, sugar and sweet food, two-way transportation, one-way transportation, moderate-intensity sports at least 10 minutes continuously, knowledge status, time from home to public physical activity facilities were entered to multivariable logistic regression analyses. After adjusting and controlling confounding being a female, working moderate-intensity sports at least 10 minutes/day continuously, dinner consumption pattern, time taken from home to public physical activities ≤15 minutes, using transport, and Knowledge status were statically significant with overweight and Obesity in both private and public schools. The odds of overweight and obesity was 5 times higher among those consuming dinner not daily than consuming daily [AOR=5.3:95% CI=1.93–14.6] and working moderate-intensity sports at least 10 minutes/day continuously were 81% less likely to develop overweight and obesity than non-doing continuously in public school adolescent students [AOR=0.19:95% CI=0.04–0.9].
The odds of overweight and obesity among females were 2 times higher as compared to males [AOR=2.03; 95% CI=1.08–3.8]. The odds of overweight and obesity among those who perform public physical activities ≤15 minutes were 3.6 times higher than those perform walking ≥30 minutes distance[AOR=3.6;95% CI=1.125–11.507]. Respondents who use transport from school to home were 2 times more likely to develop overweight and as compared to walking on foot/bicycle obesity [AOR=2.2;95% CI=1.06–4.18]. Those respondents who had good knowledge were less likely to have obesity and overweight as compared to poor knowledge adolescents [AOR=0.5; 95% CI=0.27–0.9] (Table 5).
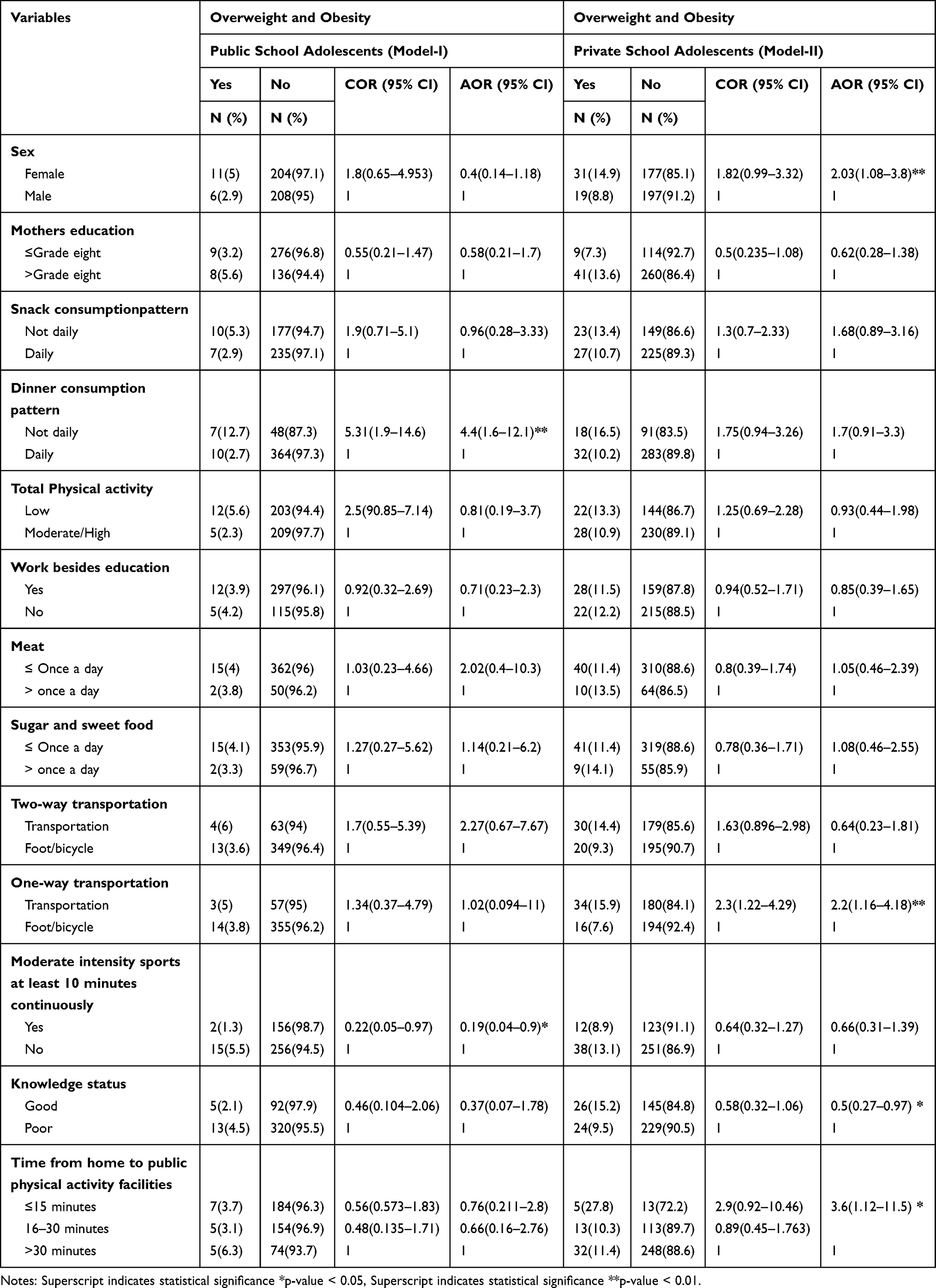 |
Table 5 Factors Associated with Overweight and Obesity Among Public and Private Secondary School Adolescent Students in Mekelle City, Ethiopia November, 2018 (Model-I and Model-II) |
Discussion
This school-based comparative cross-sectional study showed that the combined magnitude of overweight and obesity was 7.9% (95% CI=6.1–9.7%). The magnitude of overweight and obesity was 11.8% (95% CI=8.7–15.3%), and 3.9% (95% CI=2.1–5.9%) in private and public schools, respectively. Consuming dinner not daily and working moderate-intensity sports at least 10 minutes/day continuously were the associated factors for the occurrence of overweight and obesity in public school adolescent students. Being female, time taken from home to public physical activity facilities ≤15 minutes, using transport from school to home and nutritional knowledge status of adolescents were associated factors for overweight and obesity in private school adolescent students.
The magnitude of overweight and obesity in this study is in line with the study conducted in Addis Ababa but lower than that of studied in Hawassa.18,26 The magnitude of overweight and obesity in this study is higher than studies conducted in Gondar21 and earlier study in Mekelle city.31 The variability between settings it might be due to the change in lifestyle which includes reduced physical activity, the effect of modernization, urbanization, economic variability from time to time (time gap), set up differences, and adoption of western diets which are high in saturated fat, sugar, and refined foods.
This study revealed that the magnitude of overweight and obesity was significantly higher in private schools than in public schools. This study was in line with studies in India, in Surendranagar in Asia, Nairobi in Kenya.32–35 Furthermore, a study in Gondar and Addis Ababa showed that the prevalence of overweight and obesity among private schools was higher than in public schools.21,26 This could be explained by adolescents in private schools usually come from families with higher socioeconomic status which exposed them to high energy-dense foods and allow them to use vehicles to transport from and to school, decreased physical activity, less likely to work besides learning and more sedentary lifestyles. May also have fewer restrictions on food selection like sweets, more animal products, snacks, vegetables, and fruit choices compared with those in public schools.
This study found that being female was associated with overweight and obesity. This is similar to studies conducted in Sudan, Nigeria, Bahirdar, and Gondar settings.21,36–38 On the contrary, a study conducted in Vietnam showed that both overweight and obesity rates in male students were significantly associated with overweight and obesity.39 This difference may be due to reduced physical activity observed in females, females spent most of their time at home and their movement from place to place is much restricted due to cultural influence than males. Males are more physically active than females especially during the adolescent stage concerning body image particularly adolescent females may lead to problematic eating behaviors such as irregular eating meals such as omitting dinner and breakfast than males that may result in an increase in weight gain.40
In this study using a car as a means of transport from home to school or from school to home was significantly associated with overweight and obesity. This was in line with a study done in Addis Ababa and Bahirdar.28,37 Another study in Brazil also showed that those who traveled by car to school had an increased odds of overweight than those who walked to school by one-half folds.41 This might be due to the similar socio-economic status of the people. Time spend doing moderate-intensity activities on a typical day at least 10 minutes per day was a protective factor for overweight and obesity. This is consistent with a study done in Brazil,41 in Gondar moderate or vigorous sports activity for at least 10 minutes continuously was protective.21 This could be explained as physical activity results in energy expenditure thereby decreasing adiposity in the body.
In this study dinner consumption not daily was more likely to overweight and obesity than for those who ate daily. This was in line with studies conducted in Addis Ababa lacking daily dinner was associated with these problems.26 This study also agrees with another study from the US in which frequent restrictive dieting contributes to slowed metabolic rate, binge eating, and weight gain.42 This might be true in our context adolescents who are overweight and obese were trying to participate to control their weight by decreasing the number of meal frequency by omitting their meal might be the factor for weight gain.
Currently, studies showed that individuals with obesity were more at risk for COVID‐19 positive.43 Emerging data indicate a substantial decrease in global physical activity levels during the period of social isolation adopted worldwide to contain the spread of the coronavirus disease 2019 (COVID-19). Confinement-induced decreases in physical activity levels and increases in sedentary behavior may provoke a rapid deterioration of cardiovascular health and premature deaths among populations with increased cardiovascular risk.44
Limitation of the Study
The study was a potential for recall bias in the food frequency questions but during data collection, adequate information was given to participants about the importance of the study. The study was conducted in one city, and generalization to other areas might be difficult. A cross-sectional study by itself has a limitation, in which the exposure and outcome are simultaneously assessed, there is generally no evidence of the temporal relationship between exposure and outcome.
Conclusion
This study revealed that the overall magnitude of overweight and obesity was higher as compared to EDHS 2016 at the national or regional level. The magnitude of overweight and obesity was higher among private than public school adolescent students. Consuming dinner not daily and working moderate-intensity sports at least 10 minutes/day continuously were the associated factors for the occurrence of overweight and obesity in public school adolescent students. Being female, time taken from home to public physical activity facilities ≤15 minutes, using transport from school to home and nutritional knowledge status of adolescents were associated factors for overweight and obesity in private school adolescent students.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CDC, centers of disease control and prevention; cardiovascular diseases; DALYS, disability-adjusted life’s years lost; FFQ, food frequency questionnaire; GDP, growth development progress; GPAQ, Global Physical Activity Questionnaire; IOTP, International Obesity Task for References; MENA, Middle East and North Africa; OR, odds ratio; OWO, overweight and obesity; SES, socio-economic status; TPA, total physical activities; WHO, World Health Organizations.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Mekelle University Colleges of Health Science Institutional Review Board with a reference number of ERC1504/2018. The supporting letter was obtained from the school of Public health to the zonal education bureau and to all secondary schools. All participants were informed about the purpose of the study, and this study was conducted in accordance with the Declaration of Helsinki. Prior to data collection; Information was given to the participants and participants’ voluntary participation, confidentiality, anonymity, and freedom to withdraw from the study at any time were assured and their participation had no impact on the health of the participants. As a result, consents were obtained from the participants. Finally, written informed consent was obtained from all the study participants.
Consent to Publication
A written informed consent was obtained from all parents of the participants for publication of the result.
Acknowledgments
The authors thank Mekelle University and the supervisors, data collectors, and study subjects.
Funding
There is no funding to report.
Disclosure
All authors declared that they have no competing interests.
References
1. Organization WH. Obesity and overweight. Fact sheet N 311; 2012. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/.
2. Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat 11. 2002;(246):1–190.
3. World Health Organization. WHO Growth Reference, for School-Aged Children & Adolescents. Bulletin of the World Health Organization. 2007;85:660–667.
4. World Health Organization (WHO). Controlling the Global Obesity Epidemic; 2014.
5. Hoelscher DM, Kirk S, Ritchie L, Cunningham-Sabo L; Academy Positions Committee. Position of the Academy of nutrition and Dietetics: interventions for the prevention and treatment of pediatric overweight and obesity. J Acad Nutr Diet. 2013;113(10):1375–1394.
6. World Health Organization. Strengthening the Health Sectoral Response to Adolescent Health and Development. geneva; 2010.
7. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey. Addis Ababa E, and Rockville, Maryland, USA: CSA and ICF …; 2016.
8. Kurz KM. Adolescent nutritional status in developing countries. PNS. 1996;55:321–331. doi:10.1079/PNS19960032
9. Lura L; Expert Consultative Group for Every Woman Every Child on Adolescent Health. Realising the health and wellbeing of adolescents. BMJ. 2015;351:h4119. doi:10.1136/bmj.h4119
10. Fowler-Brown A, Kahwati LC. Prevention and treatment of overweight in children and adolescents. Am Fam Physician. 2004;69(11):2591–2598.
11. World Health Organization. Global Recommendations on Physical Activity for Health. Geneva:; 2010.
12. Daboné C, Delisle HF, Receveur O. Poor nutritional status of schoolchildren in urban and peri-urban areas of Ouagadougou (Burkina Faso). Nutr J. 2011;10(1):34. doi:10.1186/1475-2891-10-34
13. Lebow J, Sim LA, Kransdorf LN. Prevalence of a history of overweight and obesity in adolescents with restrictive eating disorders. J Adolescent Health. 2015;56(1):19–24. doi:10.1016/j.jadohealth.2014.06.005
14. Fowler-Brown A, Kahwati L. Prevention and treatment of overweight in children and adolescents. American family physician. 2004;69:2591–2598.
15. Park MH, Falconer C, Viner RM, et al. The impact of childhood obesity on morbidity and mortality in adulthood: a systematic review. Obesity Rev. 2012;13(11):985–1000. doi:10.1111/j.1467-789X.2012.01015.x
16. Al-Shamsi R. The Prevalence and Selected Determinants of Overweight and Obesity Among Children and Adolescent in the City of Al-Ain, UAE. University of Maryland: College Park; 2008.
17. Tebekaw Y, Teller C, Colón-Ramos U. The burden of underweight and overweight among women in Addis Ababa, Ethiopia. BMC Public Health. 2014;14(1126):1–11. doi:10.1186/1471-2458-14-1126
18. TESFALEM TESHOME PS, Debebe MOGES. Prevalence and associated factors of overweight and obesity among high school adolescents in urban communities of Hawassa, Southern Ethiopia. Current Res Nutrition Food Sci J. 2013;1(1):23–36. doi:10.12944/CRNFSJ.1.1.03
19. Kokila Selvaraj P. Sivaprakasam prevalence of overweight and obesity among medical students of Kanchipuram District. National J Research Community Med. 2013;2(Issue 2):079–148.
20. Mulugeta S, Mekitie W, Alemayehu A, et al. Magnitude and determinants of overweight and obesity in Addis Ababa high school adolescents. International Journal of Medical and Health Sciences. 2016;10(4):215–221. doi:10.5281/zenodo.1124189.
21. Gebregergs GB, Beyen TK. Overweight and obesity, and associated factors among high school students in Gondar Town, North West Ethiopia. J Obes Wt Loss Ther. 2013;3(2):1–5.
22. World Health Organization). WHO. Draft Final Report of the Commission on Ending Childhood Obesity. Geneva: World Health Organization; 2015.
23. Reilly J, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. 2011;35(7):891. doi:10.1038/ijo.2010.222
24. Douglas west Kate staff. In, Public Health Resource Unit, Breaf Intervention and Child Hood Obesity; 2012 June:4.
25. Ottova VEM, Rajmil L, Detten born-Betz L, Ravens-Sieberer U. Overweight and its impact on the health-related quality of life in children and adolescents: results from the European KIDSCREEN survey. Qual Life Res. 2012;21:59–69. doi:10.1007/s11136-011-9922-7
26. Alemu EAA, Yitayal M. Prevalence of overweight and/or obesity and associated factors among high school adolescents in Arada Sub city, Addis Ababa, Ethiopia. J Nutr Food Sci. 2014;4:261.
27. Gebremedhin S. Prevalence and differentials of overweight and obesity in preschool children in SubSaharan Africa. BMJ Open. 2015;5:e009005. doi:10.1136/bmjopen
28. Yoseph Gebreyohannes SS, Demtsu B, Bugssa. G. Nutritional status of adolescents in selected government and private secondary Schools of Addis Ababa, Ethiopia. Int J Nutrition Food Sciences. 2014;3(6):504–514. doi:10.11648/j.ijnfs.20140306.13
29. Gibson RS. Principles of Nutritional Assessment. USA: Oxford university press; 2005.
30. Gebremariam H, Seid O, Assefa H. Assessment of nutritional status and associated factors among school going adolescents of Mekelle City, Northern Ethiopia. Int J Nutr Food Sci. 2015;4(1):118–124.
31. Hadush Gebremariam OS, Assefa, H. Assessment of nutritional status and associated factors among school going adolescents of Mekelle City, Northern Ethiopia. Int J Nutrition Food Sciences. 2015;4(1,)):118–124. doi:10.11648/j.ijnfs.20150401.26
32. SONYA JAGADESAN RH, Miranda PRIYA, Unnikrishnan RANJIT. Po, overweight and obesity, among school children and, adolescents in chennai. Indian Pediatr. 2014;51(7):544–549. doi:10.1007/s13312-014-0444-6
33. Subashini K, Nalinakumari SD, Rao MVV, Kumar S, Brahmam G. A study of the geographical clustering of districts in Uttar Pradesh using nutritional anthropometric data of preschool children. Indian J Med Res. 2013;137(1):73.
34. Katkuri S, Yashwant A, Kokiwar P, Kotina S, Rao A, Chauhan P. A study of prevalence of obesity and its correlates among government and private school children in Hyderabad: a comparative study. International Journal of Research in Medical Sciences. 2015;3(11):3032.
35. Kyallo F, Makokha A, Mwangi AM. AM, Alice Mboganie Mwangi2 Overweight and obesity among public and private primary school children in Nairobi, Kenya. Health. 2013;5(08):85. doi:10.4236/health.2013.58A3012
36. E a M ANA A, Mohammed Ahmed A. Lifestyle patterns associated with overweight and obesity among adults in Jabra Area in Khartoum State - Sudan: a community based study. WWJMRD. 2016;2(12):21–24.
37. ZelalemAlamrewAnteneh M, Tekletsadek K, Tsegaye M, Alemu D. Risk factors o, overweight and, obesity, among high school, students in Bahir Dar City, North West Ethiopia:, school based cross-sectional study. Adv Prev Med. 2015.
38. Ojofeitimi EO. Pa, determinants, of obesity among, adolescent females in private, and public schools in the Olorunda, Local Government Area of Osun State, Nigeria: a comparative study. J Public Health Africa. 2011;2:1.
39. Huong Thi Le NTTV, Huyen DTT, Toan NV. Overweight, obesity and associated factors among secondary school students in a northern city of Vietnam in 2011. Health. 2013;5(01):24. doi:10.4236/health.2013.51004
40. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. The lancet. 2014;384(9945):766–781..
41. Barriuso LM, Albaladejo E, Villanueva R, Santos R, Regidor JM. Socioeconomic position and childhood-adolescent weight status in rich countries: A systematic review, 1990–2013. BMC Pediatr. 2015;15:129.
42. World Health Organization WHO. Fiscal Policies for Diet and Prevention of Noncommunicable Diseases: Technical Meeting Report.
43. Popkin BM, Du S, Green WD, et al. Individuals with obesity and COVID‐19: A global perspective on the epidemiology and biological relationships. Obesity Rev. 2020;21(11):e13128. doi:10.1111/obr.13128
44. Peçanha T, Goessler KF, Roschel H, Gualano B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am J Physiology Heart Circulatory Physiol. 2020;318(6):H1441–H1446.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.