")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 13
Magnitude of Child Sexual Abuse and Its Associated Factors Among Children Treated in Public Hospitals of Addis Ababa Ethiopia
Authors Alemayehu B , Tafesse N , Chanyalew E
Received 23 February 2022
Accepted for publication 22 June 2022
Published 23 July 2022 Volume 2022:13 Pages 67—76
DOI https://doi.org/10.2147/AHMT.S363699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Belayneh Alemayehu,1 Nebiyou Tafesse,2 Eden Chanyalew1
1Department of Nursing and Midwifery, Tirunesh Beijing General Hospital, Addis Ababa, Ethiopia; 2Department of Public Health, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Belayneh Alemayehu, Department of Nursing and Midwifery, Tirunesh Beijing General Hospital, Addis Ababa, Ethiopia, Tel +251920772457, Email [email protected]
Background: Child sexual abuse is a serious breach of basic human rights and is responsible for numerous adverse squeals and widespread global public health concern. The highest prevalence of child sexual abuse was seen in Africa. In Ethiopia, a study was conducted in Jimma town, and the study indicates that the prevalence of violence among high-school children was 62.5%. Despite this fact, it often remains unrecognized and unidentified. Thus, the aim of the study was to assess the magnitude of child sexual abuse and its associated factors among children treated in public hospitals of Addis Ababa, Ethiopia.
Methods: An institutional-based cross-sectional quantitative design study was conducted on 422 children. Study participants were selected by systematic random sampling. The data were collected through a face-to-face interview. The data were analyzed by SPSS version 26. By considering a 95% confidence level and a P value of < 0.05, binary logistic regression was used to identify factors associated with child sexual abuse.
Results: A total of 422 children participated. Among these, 42.7% of them experienced sexual abuse. Children older than 15 years were 2 times more likely to face sexual abuse than those whose age is less than 10 years [AOR = 2.27 (95% CI: 1.23– 4.19)]. Children who chew khat and smoke were abused more likely compared with their counterparts. The odds of having sexual abuse in a child with mental illness were six times more likely than children who do not have mental illness [AOR = 5.945 (95% CI: 1.642– 21.528)].
Conclusion and Recommendations: The magnitude of child sexual abuse in Addis Ababa was high. Children age, sex, khat chewing, physical disability, mental illness, smoking, and alcohol use were factors associated with child sexual abuse. Children with mental illness and physical disabilities should be treated and supported with special attention.
Keywords: child sexual abuse, associated factors, Addis Ababa, Ethiopia
Background
A “child” is a person below the age of 18 years, unless the laws of a particular country set the legal age for adulthood younger.1 The international/regional legal framework, the convention on the rights of the child, states that a child is every human being below the age of 18 years unless, under the law applicable to the child, the majority is attained earlier.2
Child Sexual Abuse is “the involvement of a child in sexual activity that he or she does not fully comprehend and is unable to give informed consent to, or for which the child is not developmentally prepared, or else that violates the laws or social taboos of society”.3 The term child sexual abuse includes a range of activities like intercourse, attempted intercourse, oral-genital contact, fondling of genitals directly or through clothing, exhibitionism, exposing children to adult sexual activity or pornography, and the use of the child for prostitution, and can be perpetrated by people in all age groups.4
Child sexual abuse (CSA) is a common and serious problem worldwide. Sexual abuse has devastating and long-lasting effects on a child.5 The global prevalence of child sexual abuse has been estimated at 19.7% for females and 7.9% for males.6 A systematic review was done among 55 studies from 24 countries and it shows that the prevalence of child sexual abuse estimates ranged from 8% to 31% for girls and 3% to 17% for boys.7 The highest prevalence rate of CSA was seen in Africa (34.4%) and Europe, America, and Asia had prevalence rates of 9.2%, 10.1%, and 23.9%, respectively. Child sexual abuse is pervasive in sub-Saharan Africa (SSA) and most commonly perpetuated by family members, relatives, neighbors, and others known to the child victim.7 In Ethiopia, a study was conducted in Gandhi Memorial Hospital, Addis Ababa, on child sexual abuse and 17.1% had a previous history of sexual abuse by the same or a different perpetuator.8 Another study was conducted in Jimma town. The study indicates that the prevalence of violence among high-school children was 62.5%.9 Despite this, 48.6% of the Ethiopian population is children, and those have risk for encountered the challenges of child trafficking, child labor, sexual abuse, orphans, vulnerable people, and other related problems.8
CSA is a serious breach of basic human rights and is responsible for numerous adverse squeals and widespread global public health concerns that require collective, as well as individual, proactive measures to safeguard the rights of children.9
Child sexual abuse is a serious public health problem everywhere in the world, and sexual abuse is a serious, insidious, and persistent form of child abuse that is difficult to identify, is often not reported, and therefore often remains hidden.10 It is vital to study child sexual abuse to provide an evidence-based intervention. Although child sexual abuse is the major problem in Ethiopia in general and Addis Ababa in particular. However, there are limited studies on child sexual abuse and associated factors in Addis Ababa, so the aim of the study was to assess the magnitude and associated factors of child sexual abuse among children treated in selected public hospitals in Addis Ababa, Ethiopia, in 2021.
Methods
Study Design and Settings
An institution-based cross-sectional study design was employed from April 15 to May 15, 2021, in public hospitals in Addis Ababa, Ethiopia. Addis Ababa has 13 public hospitals, which give services to the public. Tikur Anbessa Specialized Hospital, ALERT Hospital, Amanuel Hospital, Eka Kotebe General Hospital, Saint Paulo’s, St. Peter Hospital, and AABET Hospital are under the Federal Ministry of Health, and the rest of the six (Menelik Hospital, Zewditu Hospital, Yekatit 12 Hospital Medical College, RasDesta Hospital, Tirunesh Beijing Hospital, Gandhi Hospital) are directly led by Addis Ababa Health Bureau. Of these, only 10 public hospitals provide child care services and 3 hospitals were randomly selected. The target population of this study was all children aged 7–18 years in the study area.
Participants
The study participants were those children aged 7–18 years who visited the selected hospital with their parents or guardians during the data collection period, and we excluded children who were very sick and unable to communicate.
Sample Size Determination
The sample size was determined using a single population proportion formula using the following assumptions:
N = (Z a/2)2(p) (1- p)/d2;
where N = sample size,
Z a/2 =1.96 (standardized normal distribution curve value for the 95% confidence interval),
p = the prevalence of child sexual abuse was found to be 48.2%, taken from the previous study.11
D = 0.05 (degree of margin of error)
n= (1.96)2(0.482)(0.518)= (3.8416)(0.249676) =384
(0.05)2 0.0025
By adding a 10% non-response rate, the final sample size was 422.
Sampling Procedure and Technique
There are 10 public hospitals in city government of Addis Ababa, which give service for children. From 10 public hospitals, 3 hospitals was selected by simple random sampling in a lottery method, and then samples were distributed proportionally based on the total average number of children treated per month in 3 public hospitals (Menelik II Referral Hospital =459, Yekatit 12 Hospital Medical College=530 and Tirunesh Beijing General Hospital=428) and the sample were proportionally allocated as follows: Menelik II Referral Hospital=137, Yekatit 12 Hospital Medical College=158 and Tirunesh Beijing General Hospital=127.
The study participants were selected using a systematic random sampling technique for every K value interval. We calculated the sampling interval (K) by K = N/n, where N = the total average number of children treated per month in three public hospitals (1417), and n = the final sample size (422). Accordingly, every third child enrolled in the study is based on the sequence of their exit after treatment. The first participant was selected by the lottery method, which was the second child.
Study Variables
The dependent variable was child sexual abuse. Independent variables were as follows: child’s socio-demographic variables (age, sex, educational status, living arrangement, child interaction with parents, level of family control, gender difference), parental socio-demographic and socio-economic characteristic variables (parent’s educational status, marital status, marital conflict, family size, parents’ occupation, and monthly income), child’s health status variables (mental illness, physical disability), and history of substance use (chewing khat, smoking, drinking alcohol).
Operational Definitions
Child sexual abuse: Child sexual abuse is any interaction between a child and an adult (or another child) in which the child is used for the sexual stimulation of the perpetrator or an observer.12
Rape: Unlawful sexual activity and usually sexual intercourse carried out forcibly or under threat of injury against the will of children.13
Attempted rape: The attempt to have non-consensual sexual intercourse with a child whereby he/she was having a chance of escaping the attempt.14
Mental illnesses: A health problem that significantly affects children how they feel, think, behave, and interact with other people.15
Physical disability: Child’s lack of ability or restriction to perform an activity within the range normal for others.16
Children: A person between the age group of 7–18 years.
Data Collection Procedure and Tool
Face-to-face interviews with a pre-tested structured questionnaire were used to collect data. The questionnaire was first prepared in English and then Translated to Amharic Language, as the study subjects speak Amharic and then Back to English to check consistency. Three diploma nurses and one BSc nurse were recruited for data collection, and supervisor to ensure data quality adequate and appropriate training and guidance were provided to the data collectors and supervisors. The questionnaire was pretested in 21 (5%) of the sampled population at ALERT Hospital. After the pretest, the questionnaire was modified based on the findings related to clarity, wordings and logical sequence. The tool had four parts (child’s socio-demographic variables; parental socio-demographic and socio-economic characteristics; history of substance use; and child’s health status). To assure the quality of data, trained research assistants were collecting the data under the supervision of the principal investigator. Filled questionnaires were checked daily for consistency and completeness.
Data Processing and Analysis
The collected data were entered into Epidata version 3.1 and then exported to SPSS version 26 for analysis. The data were cleaned by running frequency, checking missing values, and checking the presence of outliers. Descriptive statistics like mean, frequencies, and percentages were used to summarize data, and text and tables were used to present data. A binary logistic regression model was used to fit the data in order to identify factors associated with child sexual abuse. All explanatory variables that were associated with the outcome variable in the bivariable analysis were included in the multivariable analysis. The crude and adjusted odds ratios together with their corresponding 95% confidence intervals were computed. A P-value <0.05 was considered to declare a result statistically significant in this study.
Results
Socio-Demographic Characteristics of the Study Participants
In this study, 422 children participated, with a response rate of 100%. Among the total study participants, 200 (47.4%) were male. The mean age of the children was 13.5 (SD ± 3.34) years, with a minimum and maximum of 7 and 18 years, respectively. Concerning the level of education, more than half 249 (59%) of the total study participants were educated up to grade eight, but 16 (3.8%) had no formal schooling, and 181 (42.9%) of them lived with both parents. However, those who lived alone and with a person who had no relationship were 3 (0.7%) and 6 (1.4%), respectively, among the total study participants. Eight (1.9%) had a frequent disagreement with their parents or guardians (Table 1).
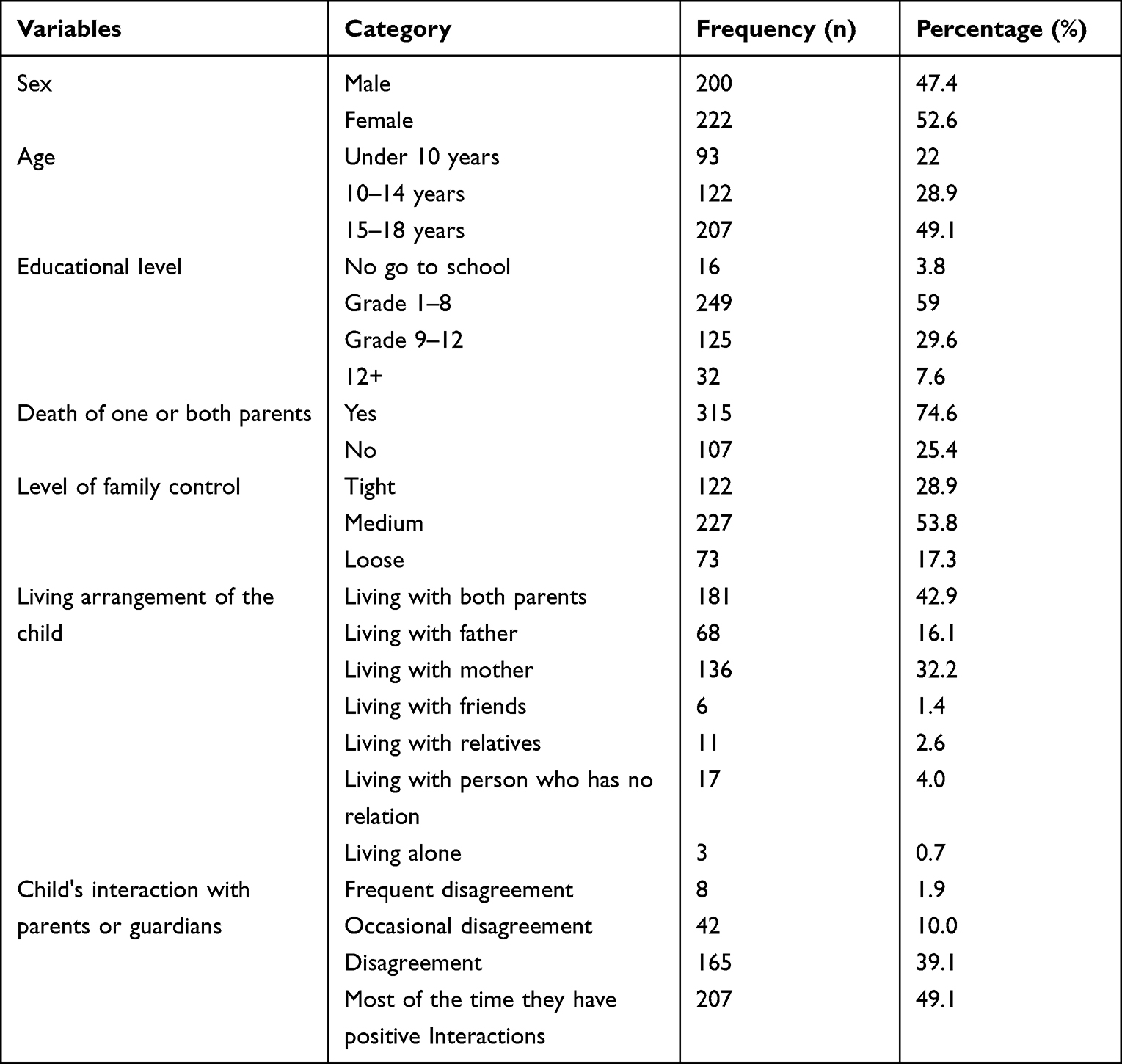 |
Table 1 Socio-Demographic Characteristics of Children in the Sample (n=422) |
Parental Socio-Demographic and Economic Characteristics
The maximum number of family members was 12 and the minimum was 2, with a mean of 5.26 (SD +-1.661). In assessing the educational level of children, 153 (36.3%) of the total parents had no history of formal school. One hundred and twenty-one (28.7%) of them were male parents, and 115 (27.5%) were educated up to grade eight. One-third of the parents (30.6%) were divorced from their marital status, and one-fifth (21.6%) of the total parents were deceased. The participants’ parents’ monthly income ranged from 30,000 to 1200 birr, with a median of 5400. When evaluating the occupational status of the participant’s parents, more than three-fourths of the parents (78%) were government employees. Two hundred and twenty-five (53.3%) respondents reported that they had conflicts with their parents (Table 2).
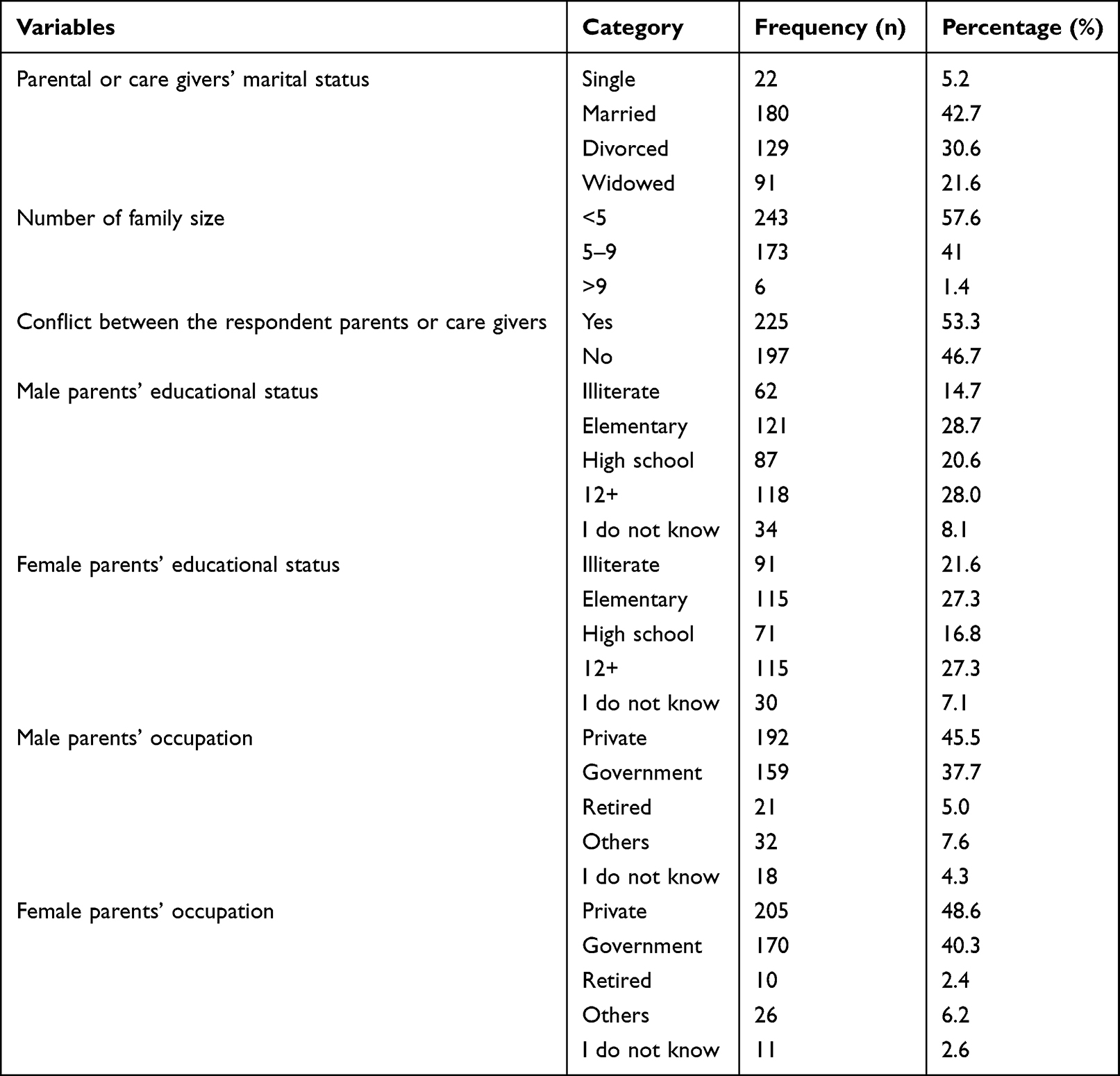 |
Table 2 Parental Socio-Demographic and Economic Characteristics of Children in the Sample (n=422) |
History of Substance Use and Health Status of the Respondents
Of the total study respondents, 96 (22.7%) of them reported a history of khat chewing. One-fifth of 88 (20.9%) of them reported a history of alcohol use. Cigarette smoking was reported by 54 (12.8%) of the study participants. In terms of the health status of the respondents, 16 (3.8%) had mental illness and 8 (1.9%) had a physical disability (Table 3).
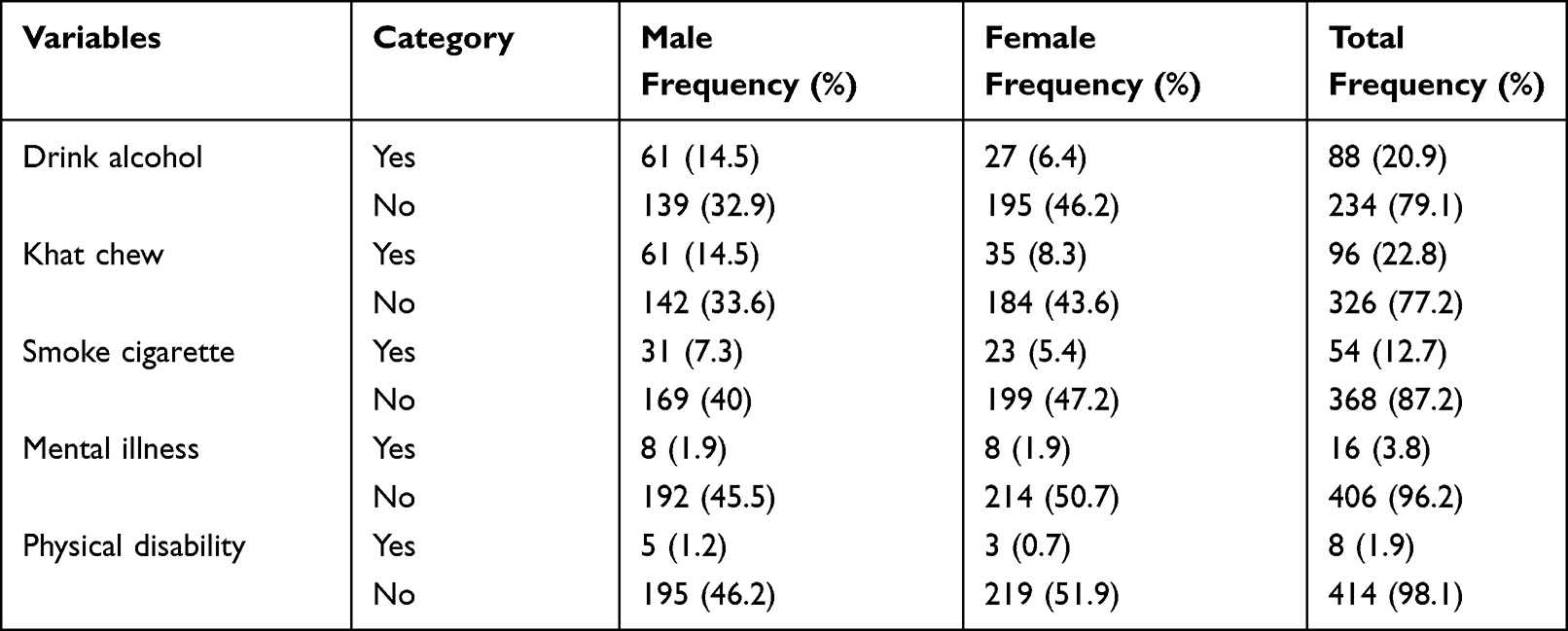 |
Table 3 History of Substance Use and Health Status of Children Treated in Addis Ababa Public Hospitals (n=422) |
Magnitude of Child Sexual Abuse
Among the total study participants, 180 (42.7%) were sexually abused, and 98 (23.2%) had experienced involuntary kissing. Of the total of involuntarily kissed participants, 79 (80.6%) were females. Attempted rape was reported by 58 (13.7%) of respondents, and rape was reported by 39 (9.2%) of the participants. Forty-three respondents (10.2%) of the total study participants were encouraged to behave sexually, and 47 (11.1%) of respondents were forced to look sexual activities (Table 4). Fifty-six (13.3%) respondents reported that their perpetrator was a boy/girl/friend.
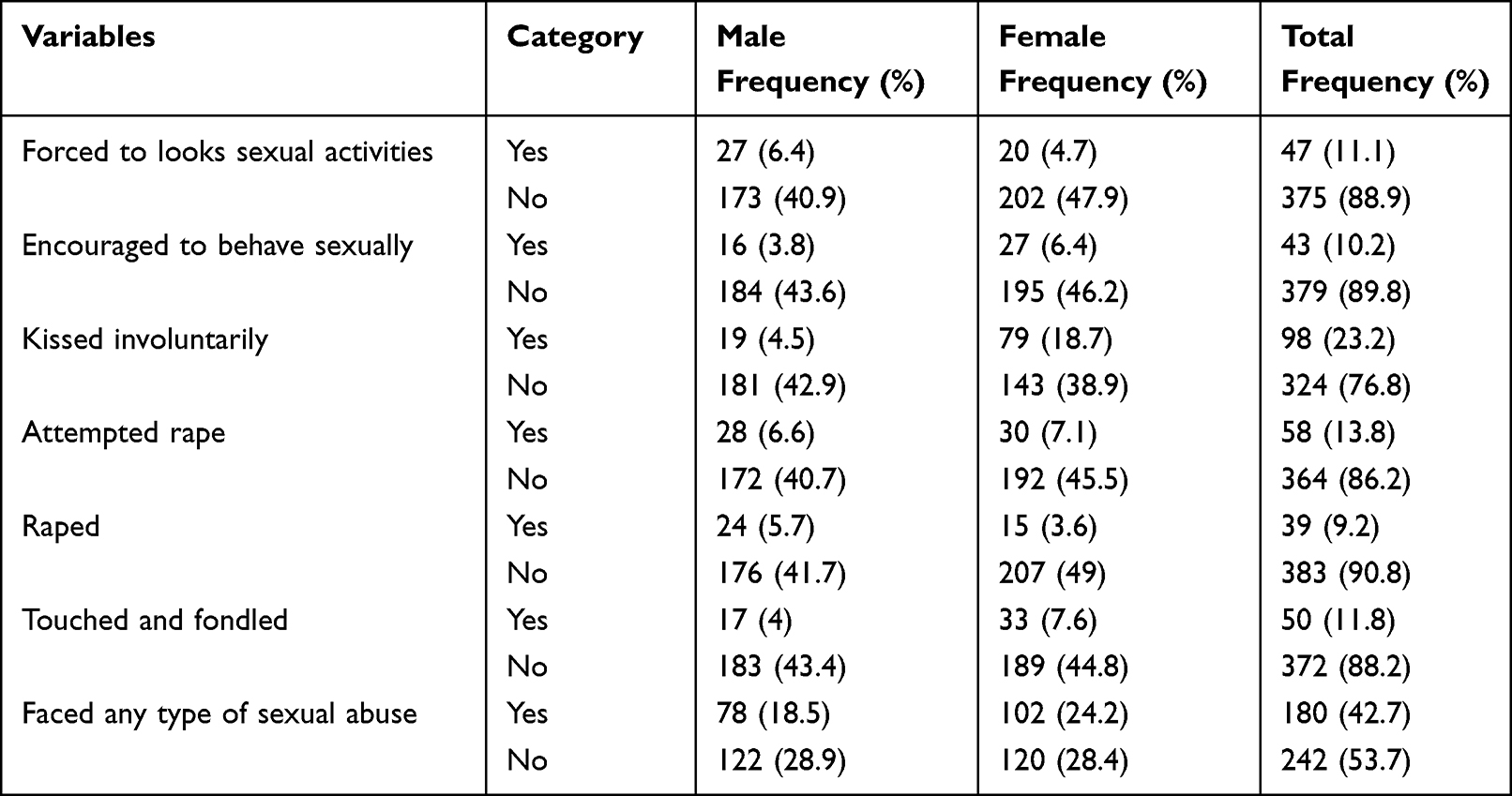 |
Table 4 Types of Sexual Abuse Experiences Among Children Treated in Public Hospital of Addis Ababa Ethiopia 2021 (n=422) |
Factors Associated with Child Sexual Abuse
Variables that had an association with child sexual abuse at p-value <0.2 in bivariable logistic regression were children’s age, sex, alcohol drinking, physical disability, mental illness, khat chewing, smoking cigarettes, and the death of one or both biological partners. All these variables were entered into multivariable logistic regression to identify factors that were associated with child sexual abuse. However, in multivariable logistic regression, except for the death of one or both biological partners (children’s age, sex, alcohol drinking, physical disability, mental illness, khat chewing, and smoking) were associated with child sexual abuse at a P-value of 0.05.
According to the findings, children over the age of 15 are twice as likely as those under the age of 10 to experience sexual abuse [AOR = 2.27 (95% CI: 1.23–4.19)]. Females were twice as likely as males to experience any type of sexual abuse [AOR: 1.93 (95% CI: 1.23–3.02)]. Children who have ever chewed khat are four times more likely to be abused [AOR = 3.617 (95% CI: 2.09–6.23)]. This study also revealed that the odds of having child sexual abuse were six times more likely among children who had ever smoked compared with those who did not smoke [AOR = 5.865 (95% CI 2.81–12.22)]. Children who had a mental illness were six times more sexually abused than their counterparts [AOR = 5.94 (95% CI: 1.64–21.52)]. Children who had a physical disability were nine times more sexually abused than those who had no physical disability [AOR = 8.82 (95% CI: 1.06–73.20)] (Table 5).
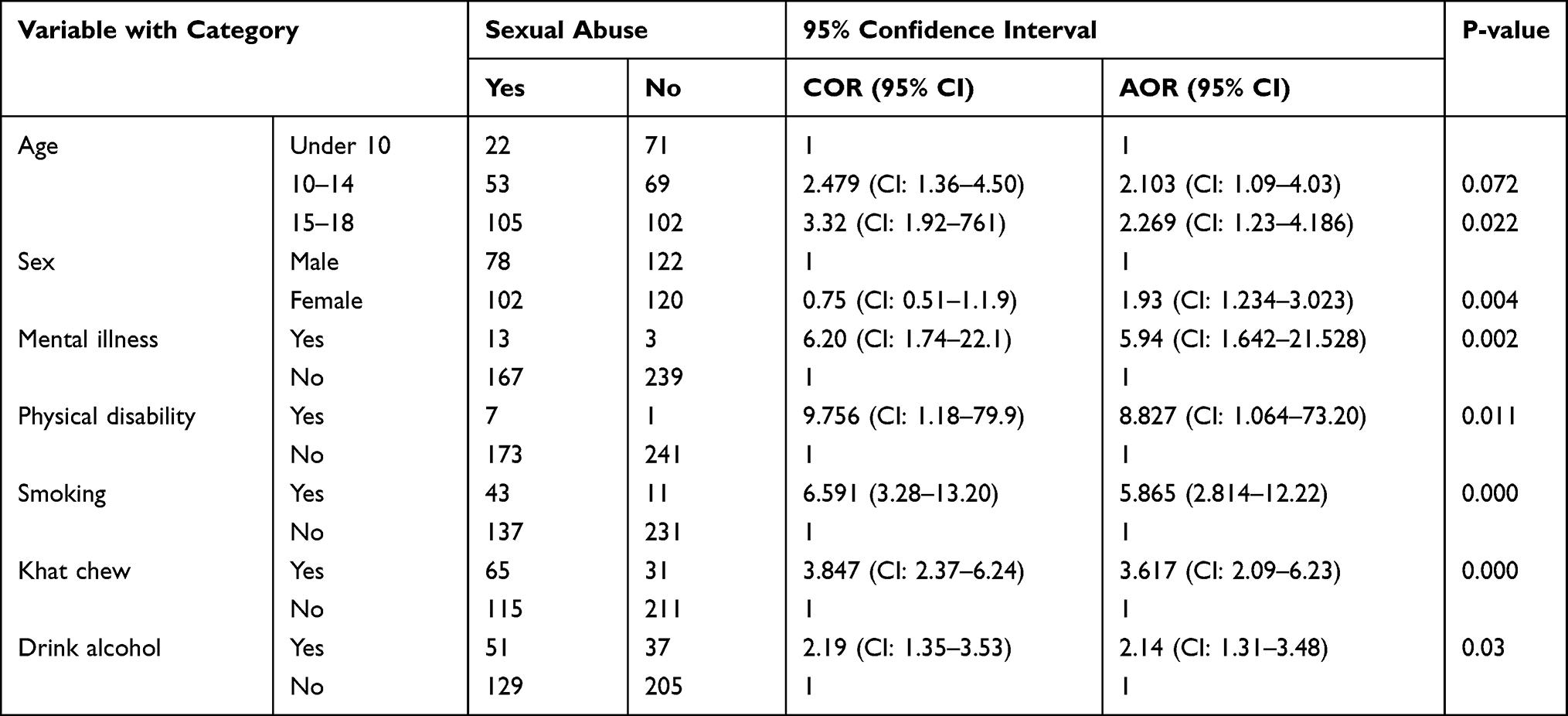 |
Table 5 Bi- and Multivariable Logistic Regression Output on Factors Associated with Child Sexual Abuse Among Children Treated in Public Hospitals Addis Ababa Ethiopia 2021 |
Discussion
Child sexual abuse damages children’s psychological and physical health and hinders their development. Despite this fact, it often remains unrecognized and unidentified. Thus, this study has tried to assess the magnitude of child sexual abuse and its associated factors among children treated in Addis Ababa public hospitals.
In this study, the magnitude of child sexual abuse among children treated in Addis Ababa public hospitals was 42.7% (CI: 38.4%–47%). The finding of this study is lower than the previous study conducted in Addis Ababa and southwest Ethiopia, which revealed that the prevalence of child sexual abuse was 48.2% and 68.7%, respectively.17,18 This variation might be the study area and study method used. However, the finding of this study is higher than the study done in Swaziland and Uganda in which the prevalence was 33.2% and 33.1%, respectively.19,20 This variation could be due to difference in culture, lifestyle, socio-economy and interventions made across the countries.
In contrast, the finding of this study is lower than the finding of a meta-analysis on the prevalence of child sexual abuse disclosure in forensic settings, which was 64.1%.21 A possible justification for this difference might be the difference in study design. This research is done in a single area.
In this study, children over the age of 15 were twice as likely as children under the age of 10 to have experienced any type of sexual abuse. The possible justification for this might be that at the age of 15 years and above, there is high sexual desire. However, the finding was contradicted by a study conducted in Korea that revealed that children under the age of 12 were found to be 1.5 times more likely to be sexually victimized than those who were at least 13 years old.22 The possible justification might be the difference in culture, religious practice, morals, and values of the community.
According to this study, children who had ever chewed khat were four times more likely to be abused than those who had never chewed khat. This might be due to the stimulant effect of khat. Chewing khat exposes children to pornographic movies and shameless feelings of sexual intercourse and activity. This finding is supported by a study conducted in Bahir Dar23 and Addis Ababa.17
This study also revealed that the odds of having child sexual abuse were six times more likely among children who had ever smoked compared with those who did not smoke. A study conducted in Portugal reported that smokers rather than nicotine dependence had a high desire for sexual intercourse and actual engagement.24 However, many types of research contradict the findings of this research because of the inhibitory effect of nicotine on sexual desire.
The odds of child sexual abuse among children who had mental illness were six times more likely compared with children without mental illness. This might be due to decreased orientation to sexual engagement and activities. Similarly, children with physical disabilities were nine times more likely to face any type of sexual abuse than their counterparts. This might be due to being alone and unable to defend against sexual harassment such as rape. In this study, more than one-fifth (23%) of the respondents were faced with both attempted and actual rape.
The finding of this study reported that the highest perpetrators of child sexual abuse were boy/girlfriends, which was 13.3%. Those children sexually abused by family members, teacher Strangers were 8.8%, 10.2%, 10.4% respectively. This finding is consistent with studies conducted among school students in Jimma that reported a greater number of respondents was perpetrated by someone they closely knew and the most common perpetrators were found to be friends, teachers, peers, and close relatives.9
In this study, children who drank alcohol were two times more likely to be abused than non-users, and children who smoked cigarettes were six times more likely to be abused than non-smokers. The finding is in line with a study conducted in South Korea, which found that those who used alcohol and smoked cigarettes were two times more likely to be sexually victimized compared to those who were not involved in delinquent behaviors.22
In this study, the type of child sexual abuse involved 9.2% of rape and 13.8% of attempted rape. In line with a cross-sectional study conducted in the Democratic Republic of the Congo, sexual abuse involved 12% of rape and 15% of attempted rape.25
A study conducted in Hawassa indicated that 14% of the students were raped at least once in their lifetime, while 26.6% faced an attempted rape.26 This consistency could be the study method used.
In this study, among all study participants, 78 (18.5%) of males and 102 (24.2%) of females were sexually abused. The finding is consistent with a review study done in Nordic countries, which showed a prevalence of child sexual abuse of between 3% and 23% for boys and 11–36% for girls,27,28 and higher than the study conducted in India, with 7.84% and 13.53% for males and females, respectively. This might be explained by the difference in the study setting and socio-cultural contexts between the study populations.
This study was limited by its cross-section nature, whereby it may not explain the temporal relationship between the outcome variable and some explanatory variables; this limits the interpretation of the estimated associations. Assess personal and sensitive issues related to sexuality by requesting qualitative studies. Thus, the findings of this study should be interpreted within these limitations.
Conclusion and Recommendations
The magnitude of child sexual abuse among children treated in Addis Ababa was high. Factors contributing to the occurrence of child sexual abuse were the child’s age, sex, mental illness, and physical disability. In addition, substance uses, such as chewing khat and smoking cigarettes, were the other factors that were significantly associated with child sexual abuse.
Ministry of Youth and Children and Ministry of Health should give emphasis to creating awareness on impact of sexual abuse. Both governmental and nongovernmental associations work hard to prevent children with mental illness and physical disabilities from sexual abuse. Social supporters, youth associations, and educational sectors should prevent them from substance use. Moreover, social and political stakeholders should work in collaboration to tackle child sexual abuse, and researchers are encouraged to carry out further studies with strong study designs and qualitative methods to identify additional factors.
Abbreviations
AIDS, acquired immuno deficiency syndrome; AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; CSA, child sexual abuse; HIV, human immunodeficiency virus; SPSS; Statistical Package for Social Science; SRS, simple random sampling; SSA; sub-Saharan Africa; STI, sexually transmitted infections; US, United States; WHO, World Health Organization.
Data Sharing Statement
All relevant data are within the paper.
Ethical Statement
This study was ethically approved by the Research and Ethical Review Board of the Department of Public Health, Yekatit 12 Hospital Medical College, and Ethical clearance was obtained from Addis Ababa Public Health Research and Emergency Management Directorate. Written Informed was taken from each study participant’s parents or their immediate caregivers. All relevant ethical principles under the Helsinki Declaration were followed and respected.
Acknowledgments
The authors want to thank Yekatit 12 Hospital Medical College, participant children and their family/guardians, data collectors and supervisors for their unreserved cooperation and support for the successful completion of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this study.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. MacPherson S. The convention on the rights of the child. Soc Policy Adm. 1989;23(1):99–101. doi:10.1111/j.1467-9515.1989.tb00500.x
2. African Child Policy Forum (ACPF). Towards a more child-friendly Africa; 2013. Available at: http://www.africanchildforum.org.
3. World Health Organization. Guidelines for medico-legal care for victims of sexual violence; 2003. Available from: https://apps.who.int/iris/handle/10665/42788. Accessed July 20, 2022.
4. Putnam FW. Ten-year research update review: child sexual abuse. J Am Acad Child Adolesc Psychiatry. 2003;42(3):269–278. doi:10.1097/00004583-200303000-00006.
5. Pereda N, Guilera G, Forns M, Gómez-Benito J. The prevalence of child sexual abuse in community and student samples: a meta-analysis. Clin Psychol Rev. 2009;29(4):328–338. doi:10.1016/j.cpr.2009.02.007
6. Barth J, Bermetz L, Heim E, Trelle S, Tonia T. The current prevalence of child sexual abuse worldwide: a systematic review and meta-analysis. Int J Public Health. 2013;58(3):469–483. doi:10.1007/s00038-012-0426-1
7. Lalor K. Child sexual abuse in Sub-Saharan Africa: child protection implications for development policy makers and practitioners. Dev Res Briefings. 2005;3:0–25.
8. Ababa A, Assabu G, Tefera M, Abebe A, Busse H. The magnitude of sexual abuse and its physical effects among female children seen at Gandhi Memorial Hospital. Ethiop J Health Dev. 2019;33(3).
9. Disasa FA, Belete YS, Aragaw YA, Wold AT, Kumsa AT. Violence against children and associated factors among high school students in Jimma Town. 2020[preprint]. Available at: https://www.researchsquare.com/article/rs-83277/v1. Accessed July 20, 2022. doi:10.21203/rs.3.rs-83277/v1
10. Aydin B, Akbas S, Turla A, Dundar C, Yuce M, Karabekiroglu K. Child sexual abuse in Turkey: an analysis of 1002 cases. J Forensic Sci. 2015;60(1):61–65. doi:10.1111/1556-4029.12566
11. Takele M, Haye TB, Kitaw LD, Uqubay N, Gebremedhin KB. Overview of child sexual and substance abuse among children in Ethiopia. J Family Med Prim Care. 2020;9(12):6140–6146. doi:10.4103/jfmpc.jfmpc_272_202020
12. The National Child Traumatic Stress Network. Sexual Abuse; 2022. Available at: https://www.nctsn.org/what-is-child-trauma/trauma-types/sexual-abuse. Accessed July 20, 2022.
13. Breen MD, Easteal P, Holland K, Sutherland G, Vaughan C. Exploring Australian journalism discursive practices in reporting rape: The pitiful predator and the silent victim. Discourse & Communication. 2017;11(3):241-258. doi:10.1177/1750481317697858.
14. Lisak D, Miller PM. Repeat rape and multiple offending among undetected rapists. Violence Vict. 2002;17(1):73–84. doi:10.1891/vivi.17.1.73.33638
15. Szasz TS. The myth of mental illness. American Psychologist. 1960;15(2):113–118. doi:10.1037/h0046535 What is mental illness?.
16. Martin S. Physical disability and physical activity: a review of the literature on correlates and associations. Eur J Adapt Phys Act. 2010;3(2):37–55. doi:10.5507/euj.2010.008
17. Takele M, Haye T, Kitaw L, Uqubay N, Gebremedhin K. Overview of child sexual and substance abuse among children in Ethiopia. Fam Med Prim Care Rev. 2020;9(12):6140–6146. doi:10.4103/jfmpc.jfmpc_272_20
18. Worku D, Gebremariam A, Jayalakshmi S. Child sexual abuse and its outcomes among high school students in southwest Ethiopia. Trop Doct. 2006;36(3):137–140. doi:10.1258/004947506777978325
19. Mathoma AM, Maripe-Perera DB, Khumalo LP, Mbayi BL, Seloilwe ES. Knowledge and perceptions of parents regarding child sexual abuse in Botswana and Swaziland. J Pediatr Nurs. 2006;21(1):67–72. doi:10.1016/j.pedn.2005.08.002
20. Devries KM, Mak JYT, García-Moreno C, et al. The global prevalence of intimate partner violence against women data from 81 countries was used to estimate global prevalence of intimate partner violence against women. Science. 2016; 340(6140):1527–1528.
21. Azzopardi C, Eirich R, Rash CL, MacDonald S, Madigan S. A meta-analysis of the prevalence of child sexual abuse disclosure in forensic settings. Child Abuse Negl. 2019;93:291–304. doi:10.1016/j.chiabu.2018.11.020
22. Han IY, Lee YW, Seo KY, Hong JS. Prevalence of and risk factors for male sexual abuse: the case of South Korea. J Loss Trauma. 2011;16(1):84–101. doi:10.1080/15325024.2010.519290
23. Abate A, Tareke M, Tirfie M, Semachew A, Amare D, Ayalew E. Chewing khat and risky sexual behavior among residents of Bahir Dar City administration, Northwest Ethiopia. Ann Gen Psychiatry. 2018;17(1). doi:10.1186/s12991-018-0194-2
24. Costa RM, Peres L. Smoking is unrelated to female sexual function. Subst Use Misuse. 2015;50(2):189–194. doi:10.3109/10826084.2014.962054
25. Nelson BD, Collins L, VanRooyen MJ, Joyce N, Mukwege D, Bartels S. Impact of sexual violence on children in the Eastern Democratic Republic of Congo. Med Confl Surviv. 2011;27(4):211–225. doi:10.1080/13623699.2011.645148
26. Asfaw M. Sexual violence and its consequence among female night school students Hawassa town, Southern Ethiopia: A cross-sectional study; 2010. Available from: http://etd.aau.edu.et/handle/123456789/12041. Accessed July 20, 2022.
27. Kaur S, Kaur S, Varshney K. Recent trends in child rape crisis in Delhi (India): a forensic overview. Forensic Sci Int. 2019. doi:10.1016/j.fsir.2019.100047
28. Kloppen K, Haugland S, Svedin CG, Mæhle M, Breivik K. Prevalence of child sexual abuse in the Nordic Countries: a literature review. J Child Sex Abus. 2016;25(1):37–55. doi:10.1080/10538712.2015.1108944
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.