")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Magnitude of Cesarean Section Delivery and Its Associated Factors Among Mothers Who Gave Birth at Public Hospitals in Northern Ethiopia: Institution-Based Cross-Sectional Study
Authors Ayalew M, Mengistie B , Dheressa M , Demis A
Received 24 August 2020
Accepted for publication 6 November 2020
Published 16 November 2020 Volume 2020:13 Pages 1563—1571
DOI https://doi.org/10.2147/JMDH.S277747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Melese Ayalew,1 Bizatu Mengistie,2 Merga Dheressa,1 Asmamaw Demis3
1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3Department of Nursing, College of Health Sciences, Woldia University, Woldia, Ethiopia
Correspondence: Asmamaw Demis
Department of Nursing, College of Health Sciences, Woldia University, P.O.Box: 400, Woldia, Ethiopia
Email [email protected]
Background: Cesarean section is one of the most common surgeries around the world performed whenever abnormal conditions complicate labour and vaginal delivery, threatening the life or health of the mother or the baby. Although the cesarean section is a safe operation, when it is performed without medical need, it puts mothers and their babies at risk of short- and long-term health problems. However, the factors are not persistent and there is limited information concerning the levels of cesarean section delivery and its associated factors in public hospitals of North Wollo Zone. Therefore, this study aimed to assess the magnitude of cesarean section and associated factors in hospitals of North Wollo Zone, Northern Ethiopia.
Methods and Materials: An institution-based cross-sectional study design was employed among 433 mothers who gave birth in public hospitals of North Wollo Zone, Northern Ethiopia, from March 01 to 30, 2019. A systematic random sampling method was used to select the study participants. A structured questionnaire was used to collect data. Bivariable and multivariable analyses were carried out to identify independent predictors of cesarean section.
Results: The magnitude of cesarean section delivery was 30.9% (95% CI, 26.8– 35.3). Being urban resident (AOR=4.04, 95% CI: 2.19– 7.45), malpresentation (AOR=2.56, 95% CI: 1.29– 5.05), having a previous cesarean section (AOR=9.11, 95% CI: 3.77– 22.01) and antepartum haemorrhage (AOR=8.65, 95% CI: 3.82– 19.56) were statistically and positively associated with cesarean section delivery.
Conclusion: The magnitude of cesarean section delivery among mothers who gave birth at North Wollo Zone public hospitals was high. Residence, antepartum haemorrhage, having a previous cesarean section, and malpresentation were factors associated with cesarean section. Therefore, health education and giving a clear picture regarding the risks and benefits of cesarean section as well as avoiding unjustified cesarean section delivery should be encouraged.
Keywords: cesarean section, public hospitals, North Wollo Zone
Introduction
Cesarean delivery is an operative technique by which a fetus, placenta, and membranes are delivered through an abdominal and uterine incision.1 Cesarean section is one of the most common surgeries around the world and it is classified into elective, necessary, and emergency caesarian sections.2,3 The main indications for cesarean delivery are previous cesarean delivery, Cephalic pelvic disproportion, fetal distress, pregnancy-induced hypertension, failed induction, antepartum haemorrhage, obstructed labour, breech presentation, multiple gestation and chorioamnionitis.4 Worldwide, cesarean section delivery is the most frequent abdominal surgery performed among pregnant women. It is estimated that about 20 million cesarean section deliveries occur each year with rapidly growing continuously in low-, middle- and high-income countries.5–7
A study conducted between 2002 and 2012 showed that the rate of cesarean section increased from 18.2% in 2002 to 30.3% in 2012, with the most common reason being the absence of a clear indication.8,9 According to the American College of Obstetricians and Gynecologists (ACOG) report, cesarean birth significantly increased a woman’s risk of pregnancy-related fatality (35.9/100,000) compared to a woman who delivered vaginally (9.2/100,000) deaths.10 The rates of pelvic pain, deep dyspareunia, profuse bleeding requiring laparotomic hysterectomy, unintentional transvesical caesarean section requiring bladder repair, female postpartum sexual dysfunction, and spontaneous miscarriage were also common after cesarean section.11–15 Although the majority of cesarean birth is performed for a condition that might pose a threat to both the mother and her fetus, if vaginal delivery occurred, cesarean birth can never be entirely safe and when it is performed without medical need it puts mothers and their babies at risk of short-and long-term health problems which are higher than those associated with vaginal birth, therefore, is not an alternative to vaginal delivery.16–19
World Health Organization (WHO) has recommended that the cesarean section rate should lie between 5% and 15% to have an optimal impact since no additional benefit for newborns or mothers is obtained beyond this level.20 Currently, the rate of hysterectomy secondary to previous cesarean delivery increased from 27% to 57%, while placenta accreta as an indication of hysterectomy increased from 5.4% to 46.5%.21 In Africa, cesarean sections are still performed in unfavourable conditions for saving the mother and fetus with 5 to 10 times higher maternal morbidity and mortality compared with vaginal delivery due to limited resources and far distance to a health facility for people living in rural.22–24
In Ethiopia, the rate of cesarean delivery varied between regions with a range of 0.4% in Somali to 21.4% in Addis Ababa with the national pooled prevalence of 29.5%.25–27 The common neonatal complications following Caesarean section included low APGAR score, perinatal asphyxia, neonatal sepsis, meconium aspiration syndrome, early neonatal death, stillbirth, and prematurity whereas febrile morbidity, surgical site infection, maternal mortality, severe anaemia, and postpartum haemorrhage were the most common maternal complication secondary to cesarean delivery.26 However, cesarean delivery is associated with a reduced rate of urinary incontinence, faecal incontinence, pelvic pain, and pelvic organ prolapse in the mother as compared with vaginal delivery.28 There is limited information concerning the magnitude of cesarean section and associated factors in public hospitals of Northern Ethiopia. Therefore, this study aimed to assess the magnitude of the cesarean section in hospitals and associated factors in northern Ethiopia.
Methods and Materials
Study Area, Design and Period
An institution-based cross-sectional study was employed from March 1–30 2019, in public hospitals of North Wollo Zone, Northern Ethiopia. North Wollo Zone is located at about 521Km from Addis Ababa, the capital city of Ethiopia, 358 Km southeast from Bahirdar city of Amhara Regional State. Based on the 2007 Census conducted by the Central Statistical Agency of Ethiopia, the total population of North Wollo Zone is 1,500,303, an increase of 19.04% over the 1994 census, of whom 752,895 are men and 747,408 women, respectively. There are 6 hospitals, 65 health centers, and 275 health posts providing services to the community. The annual report from the North Wollo Zone Health office in 2018 indicated that the health coverage of institutional delivery was 68% and the delivery service was 79%.
Populations
The source population was all mothers who gave birth at public hospitals of North Wollo Zone and all mothers who gave birth in the selected hospitals during the actual data collection period were the study population.
Inclusion and Exclusion Criteria
All mothers who were delivered in the selected hospitals during the study period were included, whereas severely ill women who were unable to give a response and women referred to other institutions were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was calculated with Epi Info 7 software using the double population proportion formula with the assumptions; 95% confidence interval, 5% margin of error, power of 80%, the proportion of exposed to unexposed ratio of 1, and 10% of non-response rate, the final sample size was 433. From a total of six public hospitals, three hospitals (Woldia General Hospital, Lalibela Primary Hospital, and Kobo Primary Hospital) were selected by simple random sampling technique. The sample size was proportionally allocated to each respective hospital by considering client flow. Lastly, study subjects were selected using a systematic sampling technique by taking every two clients as intervals based on the average daily flow of the clients. Based on client flow, sampling with population proportional to size (PPS) was calculated for each hospital.
Data Collection Tool and Procedures
Data were collected through review of case records of mothers and face-to-face interviews using the Amharic version structured questionnaire (language spoken in the study area), adapted and further developed by using different peer-reviewed published literature. The English language questionnaire was translated back into the Amharic language (language spoken in the study area) by Amharic language speakers and was translated back to English language and a comparison was made to assist the consistency of the two versions. The questionnaire addressed women’s socio-demographic factors, obstetrics factors, and maternal medical illness factors.
Data Quality Assurance
The data collection instrument was made from the English language to the local Amharic language and back to the English language. Two days of training was given for data collectors and supervisors by the principal investigator about the techniques of data collection and was briefed on each question in the data collection tool. A pre-test was done in 5% of the sample size to ensure the validity of the tool and corrections were done before the actual data collection period. To minimize bias, interviews were conducted in an area with adequate confidentiality and privacy.
Data Processing and Analysis
The data were coded, cleaned, edited, and entered into Epi data version 4.2 to minimize logical errors and design skipping patterns. Then, the data were exported to SPSS window version 24 for analysis. Simple frequencies, summary measures, tables, and figures were used to present the data. Bivariate analysis, crude odds ratio with 95% CI, was used to see the association between each independent variable and the outcome variable by using binary logistic regression. Multi-collinearity was checked to see the linear correlation among the independent variables by using standard error and correlation matrix. Model fitness was checked using the Hosmer-Lemeshow goodness test. Adjusted odds ratio with a 95% confidence interval and level of significance at P<0.05 was estimated to identify the predictors associated with cesarean section delivery.
Ethical Approval
Ethical clearance was obtained from Haramaya University, College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (IHRERC) with Ref. No (IHRERC 040/2019, dated on Feb, 21/2019). An official letter was written to the North Wollo zonal health department, then to selected hospitals for permission. After securing permission, data were collected after signing written informed consent. This study was conducted in accordance with the declaration of Helsinki.
Results
Socio-Demographic Characteristics
In this study, a total of 433 study participants were involved, making a response rate of 100%. The mean age of the study participants was 27.27 (±5.18 SD) years. More than two-thirds, 290 (67.7%) of the participants were found within the age group of 20–30 years. Almost all, 412 (95.2%) of the study participants were Amhara by ethnicity, near three-fourths, 313 (72.3%) were Orthodox by religion, and almost all, 417 (96.3%) were married by marital status. Concerning the educational status and occupation of mothers, around 193 (44.6%) of the respondents attended secondary and college-level education, 255 (58.9%) were housewives. Out of the total sample respondents, more than two-thirds, 291 (67.2%) were from urban. Regarding family size, 370 (85.5%) of the sample respondents had 1–5 family sizes (Table 1).
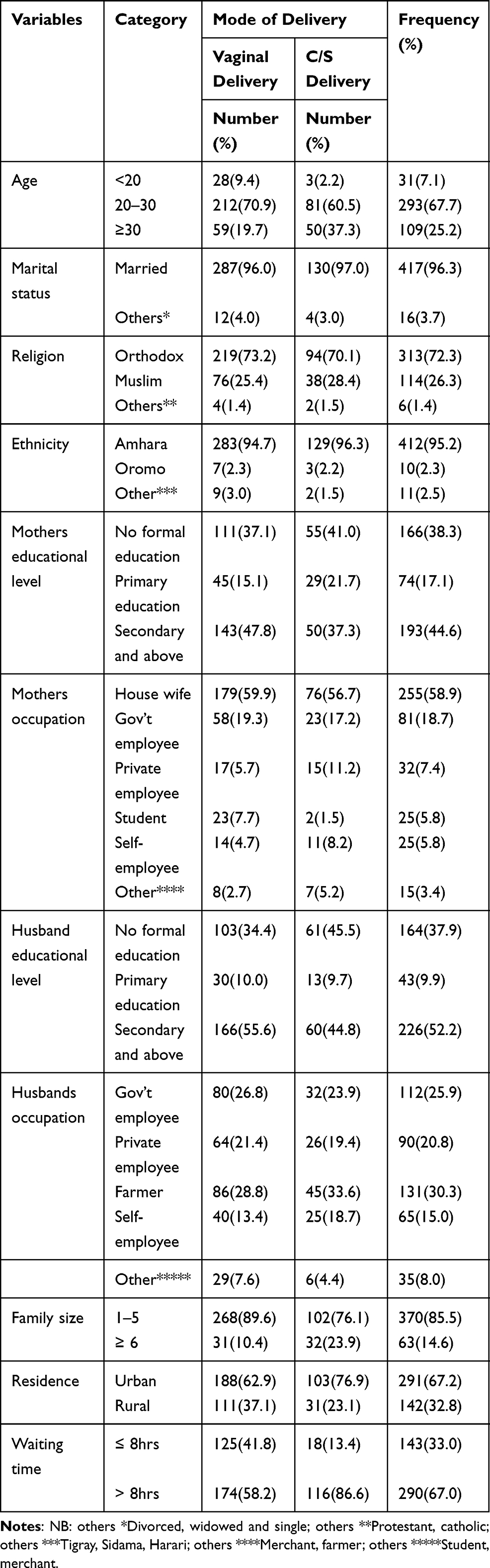 |
Table 1 Socio-Demographic and Health Facility Characteristics of Women Who Gave Birth at Public Hospitals in North Wollo Zone, Northern Ethiopia, 2019 (n=433) |
Obstetric-Related Characteristics
Regarding gravidity and parity, nearly three-fifths, 248 (57.3%) of mothers were multigravida and 199 (46.0%) were multiparous. Concerning gestational age, 351 (81.1%) mothers delivered at term. Regarding birth weight and history of stillbirth, 385 (88.9%) newborns had normal birth weight and 385 (88.9%) did not have a history of stillbirth. Of the total respondents, the majority of mothers, 384 (88.7%) did not have a medical illness (Table 2).
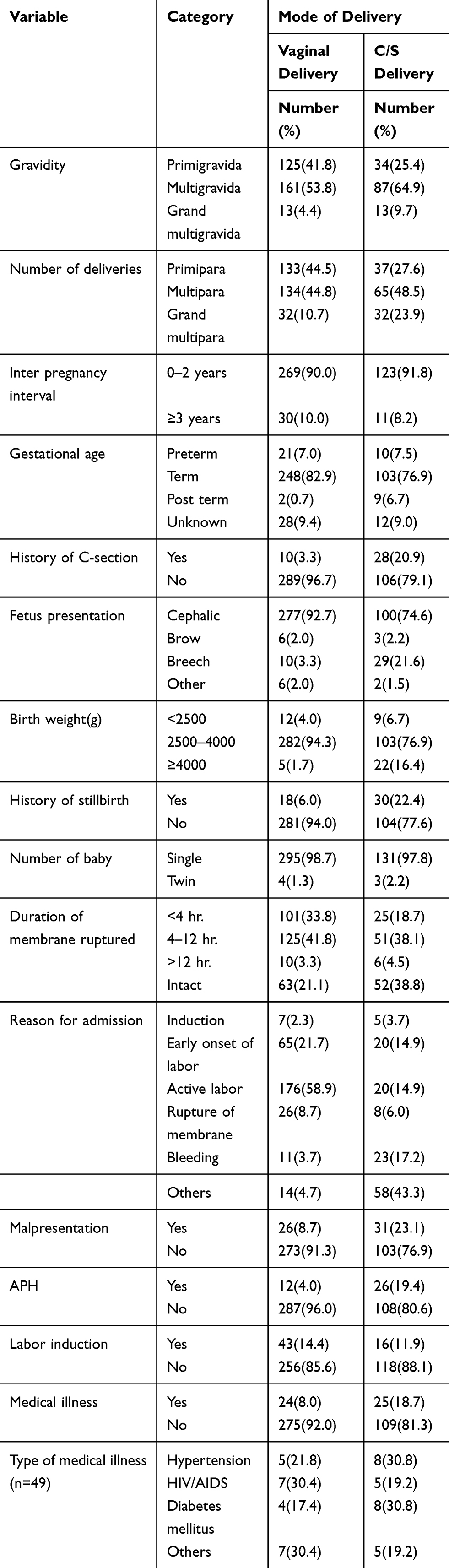 |
Table 2 Obstetrics and Medical Illness-Related Factors of Women Who Gave Birth at a Public Hospital in North Wollo Zone, Northern Ethiopia, 2019 |
The Magnitude of Cesarean Delivery
In this study, the magnitude of cesarean section delivery was 30.95% (95% CI: 26.8–35.3) delivered through cesarean section. The rate of vaginal delivery was 299 (69.05%) (Figure 1).
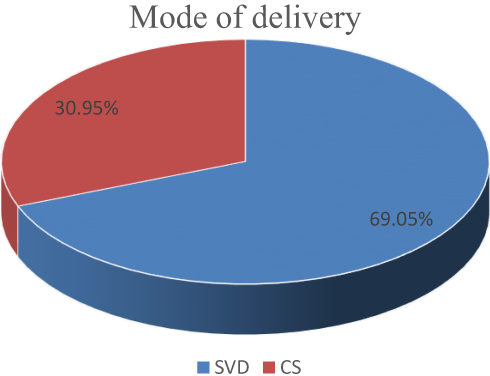 |
Figure 1 Mode of delivery among mothers who gave birth at a public hospital in North Wollo Zone, Northern Ethiopia, 2019. |
Indication for Cesarean Section
Regarding indication for cesarean section, non-reassuring fetal heart rate pattern (NRFHP), having a previous cesarean section, antepartum haemorrhage (APH), failed induction, and cephalopelvic disproportion (CPD) accounted for 32 (22.2%), 28 (19.4%), 17 (11.8%), 10 (6.9%) and 7 (4.9%) respectively (Figure 2).
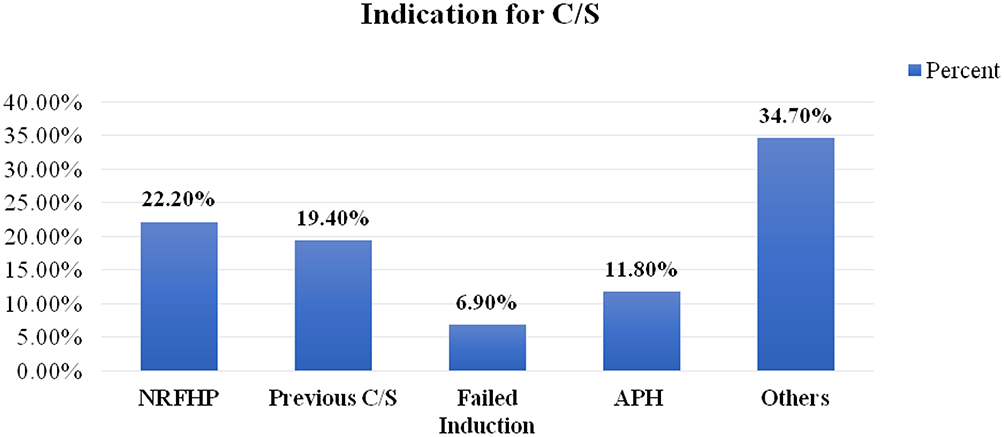 |
Figure 2 Indication for cesarean section among mothers who gave birth at a public hospital in North Wollo Zone, Northern Ethiopia, 2019. |
Factors Associated with Cesarean Section Delivery
In this study, in the final multivariable logistic regression analysis, residence, antepartum haemorrhage (APH), having a previous cesarean section, and malpresentation were significantly associated with cesarean section. Mothers who came from urban residents were 4.04 times more likely delivered through cesarean section than those who came from an urban resident (AOR=4.04, 95% CI: 2.19–7.45). The odds of giving birth by cesarean section were two and a half times higher among mothers with malpresentation compared with the counterparts (AOR=2.56, 95% CI: 1.29–5.05). Mothers who had a history of previous cesarean sections were nine times more likely to have a cesarean section than those who had not a history of previous cesarean section (AOR=9.11, 95% CI: 3.77–22.01). Mothers who had APH were 8.65 times more likely to have a cesarean section than those mothers who had not antepartum haemorrhage (APH) (AOR=8.65, 95% CI: 3.82–19.56) (Table 3).
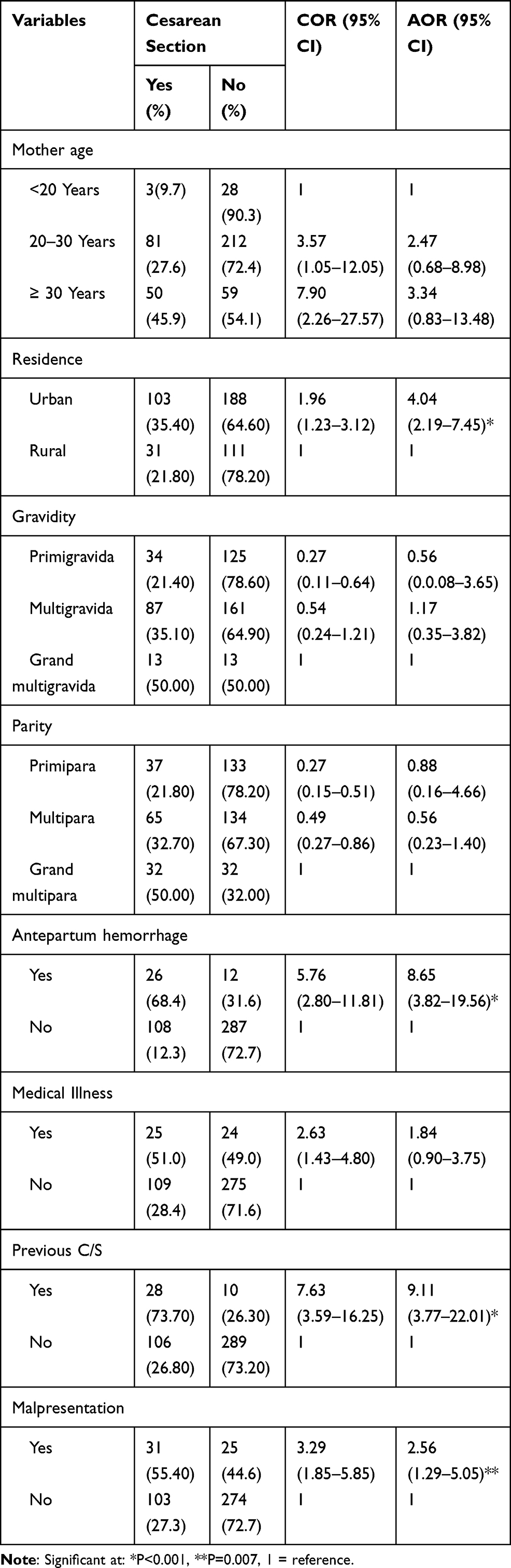 |
Table 3 Bivariable and Multivariable Analysis for Factors Associated with Cesarean Section Delivery Among Mothers Who Gave Birth at Public Hospitals in North Wollo Zone, Northern Ethiopia, 2019 (n=433) |
Discussion
This institutional-based cross-sectional study tried to identify the magnitude of cesarean section and associated factors among mothers who gave birth at North Wollo Zone public hospitals. Accordingly, the study showed that the prevalence of cesarean section was 30.95% (95% CI, 26.8–35.3). The result is in line with the studies conducted in Bangladesh (35%),29 Attat Hospital, Gurage Zone, Ethiopia (27.6%),30 Yirgalem General Hospital, SNNPE (26.9%)31 and Harar town, eastern Ethiopia (34%).32 The finding was higher than the WHO recommended optimum upper limit of 15%,20 Sub-Saharan Africa (6.2%),33 Mizan Aman General Hospital, Southwest Ethiopia (21.1%),34 Tigray, Ethiopia (24.2%),35 Addis Ababa, Ethiopia (19.2%)36 and Felege Hiwot Referral Hospital, Amhara region, Northwest Ethiopia (25.3%).37 This difference might be due to the fact that the study was conducted in North Wollo Zone public hospitals that served nearby regions (Tigray, Afar) other than its catchment area which increases referral for cesarean delivery. However, the result was lower than the study conducted in Brazil (43.5%),38 India (62%),39 and in Nalgonda (55.9%).40 This might be due to the difference in geographic location, socio-demographic, and economic status of the study participants, and differences in the sample size of the study.
Mothers who came from urban residents were four times more likely to give birth through cesarean section than those who came from rural resident. This is in line with the study conducted in Addis Ababa Ethiopia,36 Felege Hiwot Referral Hospital, Amhara region, Northwest Ethiopia,37 and Attat Hospital, Gurage Zone, Ethiopia.30 This might be due to women who came from urban residents were more likely educated and aware of the severity of labour pain, and they prefer cesarean delivery as compared with vaginal delivery.
The likelihood of cesarean section with malpresentation was 2.5 times more likely than mothers without malpresentation, which is consistent with the result obtained from Felege Hiwot Referral Hospital Amhara region, Northwest Ethiopia.37 This might be due to the fact that mothers with malpresentation were unable to give vaginal delivery due to changes in the normal presentation of the fetus with the normal course of labour which resulted in the delivery of the fetus through cesarean section.
Mothers who had a history of previous cesarean sections were nine times more likely to have a cesarean section than those who had not a history of the previous cesarean section, which is consistent with studies conducted in Pakistan41 and Harar town, eastern Ethiopia.32 This might be due to the fact that mothers who have a history of previous cesarean section delivery understand that they have not a chance to give birth via spontaneous vaginal delivery due to fear of uterine rupture and women with other obstetrics and medical complications are indicated for cesarean section.
Mothers who had antepartum haemorrhage were more likely to have cesarean section than those who had not antepartum haemorrhage. The probable reason could be due to the fact that women presented with antepartum haemorrhage, mainly major placenta praevia; as a result, the health care providers decided to have cesarean section delivery to prevent maternal and fetal complications. Additionally, an emergency cesarean section might also be performed in case of maternal risk with severe bleeding secondary to placenta praevia.
Limitations of the Study
The study did not address the views and practices of health care providers related to cesarean section delivery.
Conclusions
The magnitude of cesarean section among mothers who gave birth at North Wollo Zone public hospitals was high. Residence, antepartum haemorrhage, having a previous cesarean section, and malpresentation was significantly associated with cesarean section delivery. Therefore, health education and giving a clear picture regarding the risks and benefits of cesarean section as well as avoiding unjustified cesarean section delivery should be encouraged. Besides, health providers should follow WHO recommendations for the cesarean section. Other researchers did further investigation to assess the views, attitudes, and practices of health care providers related to cesarean section delivery.
Abbreviations
ANC, antenatal care clinic; AOR, adjusted odds ratio; APH, antepartum hemorrhage; NRFHBP, non-reassuring fetal heart beat pattern; CS, cesarean section; EDHS, Ethiopian Demographic and Health Survey; SDGs, sustainable development goals; SPSS, Statistical Package for Social Sciences; WHO, World Health Organizations.
Data Sharing Statement
The data set of this article is not openly accessible. However, it is accessible upon reasonable request from the corresponding author with the authorization of the Haramaya University ethics committee.
Acknowledgments
The authors would like to thank data collectors and supervisors for their invaluable efforts to make this study real. The author’s deep gratitude also goes to our study subjects who were volunteered and took their time to give us all relevant information for the study. The authors are also thankful to Haramaya University for financial support.
Author Contributions
All authors made substantial contributions to the conception and design, analysis, and interpretation of data; took part in drafting the article, revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The research was funded by Haramaya University with Ref. No. Hu/sgs/136/2019. The funder has no role in the development of the paper except finance.
Disclosure
This paper is based on a Thesis titled “Magnitude of Cesarean Section Delivery and Its Associated Factors among Mothers Who Gave Birth at Public Hospitals in Northern Ethiopia” by author Melese Ayalew. The authors report no conflicts of interest in this work.
References
1. Gibbons L, Belizán JM, Lauer JA, Betrán AP, Merialdi M, Althabe F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World Health Rep. 2010;30:1–31.
2. Feng XL, Wang Y, An L, et al. Cesarean section in the People’s Republic of China: current perspectives. Int J Women’s Health. 2014;6:59. doi:10.2147/IJWH.S41410
3. Stjernholm YV, Petersson K, Eneroth E. Changed indications for cesarean sections. Acta Obstet Gynecol Scand. 2010;89(1):
4. Gayathry D, Guthi VR, Bele S, et al. A study of maternal morbidity associated with caesarean delivery in tertiary care hospital. Int J Commun Med Public Health. 2017;4(5):
5. Betrán AP, Merialdi M, Lauer JA, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol. 2007;21(2):
6. Luz G, Belizán JM, Lauer JA, Betrán AP, Merialdi M, Althabe F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World Health Report. 2010;30.
7. Berhan Y, Abdela A. Emergency obstetric performance with emphasis on operative delivery outcome: does it reflect the quality of care? Ethiop J Health Dev. 2004;18(2):96.
8. Strom S, Rates, Trends and Determinants of Cesarean Section Deliveries in El Salvador: 1998 to 2008. 2013.
9. Al Rifai R. Rising cesarean deliveries among apparently low-risk mothers at university teaching hospitals in Jordan: analysis of population survey data, 2002–2012. Glob Health: Sci Pract. 2014;2(2):
10. ACOG. American College of Obstetricians and Gynecologists Profile of Ob-Gyn Practice. 2013.
11. Laganà AS, Cromi A, Tozzi R, Franchi M, Lukanović D, Ghezzi F. Uterine scar healing after cesarean section: managing an old surgery in an evidence-based environment. J Investig Surg. 2018.
12. Gulino FA, Pappalardo E, Ettore C, et al. Caesarean scar pregnancy: descriptive paper of three different types of management on a series of clinical cases. Przegla?d Menopauzalny= Menopause Rev. 2020;19(2):
13. Franchi M, Raffaelli R, Baggio S, et al. Unintentional transvesical caesarean section: incidence, risk factors, surgical technique and post-operative management. Eur J Obstet Gynecol Reprod Biol. 2019;236:26–31. doi:10.1016/j.ejogrb.2019.02.023
14. Laganà AS, Platania A, Butticè S, et al. Comment on “Impact of mode of delivery on female postpartum sexual functioning: spontaneous vaginal delivery and operative vaginal delivery vs cesarean section”. J Sex Med. 2016;13(7):
15. Laganà A, Burgio MA, Ciancimino L, Evaluation of recovery and quality of sexual activity in women during postpartum in relation to the different mode of delivery: a retrospective analysis. Minerva Ginecol. 2015;67(4):
16. Gabbe S, Pocket companion to obstetrics: Normal and problem pregnancies. 2002.
17. Ijaiya M, Aboyeji P. Caesarean delivery: the trend over a ten-year period at Ilorin, Nigeria. Niger J Surg Res. 2001;3(1):
18. Gilliam M. Cesarean delivery on request: reproductive consequences. Semin Perinatol. 2006;30(5):257–260. doi:10.1053/j.semperi.2006.07.005
19. MacDorman MF, Declercq E, Menacker F, et al. Neonatal mortality for primary cesarean and vaginal births to low‐risk women: application of an “intention‐to‐treat” model. Birth. 2008;35(1):
20. Betrán AP, Torloni MR, Zhang JJ, et al. WHO statement on caesarean section rates. BJOG. 2016;123(5):
21. Keag OE, Norman JE, Stock SJ. Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis. PLoS medicine. 2018;15(1):e1002494.
22. Neuman M, Alcock G, Azad K, et al. Prevalence and determinants of caesarean section in private and public health facilities in underserved South Asian communities: cross-sectional analysis of data from Bangladesh, India and Nepal. BMJ Open. 2014;4(12):
23. Shearer EL. Cesarean section: medical benefits and costs. Soc Sci Med. 2011;37(10):1223–1231. doi:10.1016/0277-9536(93)90334-Z
24. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 2014;38(8):1091–1110. doi:10.1016/0277-9536(94)90226-7
25. EDHS. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016. Available from: http://www.ethiodemographyandhealth.org/Measure_DHS_Ethiopia2016.pdff.
26. Gedefaw G, Demis A, Alemnew B, Wondmieneh A, Getie A, Waltengus F.Prevalence, indications, and outcomes of caesarean section deliveries in Ethiopia: a systematic review and meta-analysis. Patient Saf Surg. 2020;14(p):1–10.
27. Fesseha N, Getachew A, Hiluf M, et al. A national review of cesarean delivery in Ethiopia. Int J Gynecol Obstet. 2011;115(1):
28. Keag Oonagh E, Norman Jane E, Sarah JS, Myers JE. Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: systematic review and meta-analysis. PLoS Med. 2018;15(1):
29. Begum T, Rahman A, Nababan H, et al. Indications and determinants of caesarean section delivery: evidence from a population-based study in Matlab, Bangladesh. PLoS One. 2017;12(11):
30. Moges A, Ademe B, Akessa G. Prevalence and outcome of caesarean section in Attat Hospital, Gurage Zone, SNNPR, Ethiopia. Arch Med. 2015;7(4):
31. Tesfaye T, Hailu D, Mekonnen N, Tesfaye R. Magnitude of maternal complication and associated factors among mothers undergone cesarean section at Yirgalem general hospital, SNNPR, Ethiopia. risk. 2017;100:11.
32. Tsega F, Mengistie B, Dessie Y, Mengesha M. Prevalence of cesarean section in urban health facilities and associated factors in Eastern Ethiopia: hospital based cross sectional study. J Preg Child Health. 2015;2(3):
33. Chu K, Cortier H, Maldonado F, et al. Cesarean section rates and indications in sub-Saharan Africa: a multi-country study from Medecins sans Frontieres. PLoS One. 2012;7(9):
34. Gutema H, Shimye A. cesarean section and associated factors at mizan aman general hospital, southwest Ethiopia. J Gynecol Obstet. 2014;2(3):
35. Adhena T, Haftu A, Gebre G, Dimtsu B. Assessment of magnitude and associated factors of adverse birth outcomes among deliveries at Suhul Hospital Shire Tigray, Ethiopia from September, 2015 to February, 2016. Res Rev. 2019;6(1):
36. Bayou YT, Mashalla YJ, Thupayagale-Tshweneagae G. Patterns of caesarean-section delivery in Addis Ababa, Ethiopia. Afr J Prim Health Care Fam Med. 2016;8(2):
37. Abebe FE, Gebeyehu AW, Kidane AN, et al. Factors leading to cesarean section delivery at Felegehiwot referral hospital, Northwest Ethiopia: a retrospective record review. Reprod Health. 2015;13(1):
38. Vieira GO, Fernandes LG, de Oliveira NF, et al. Factors associated with cesarean delivery in public and private hospitals in a city of northeastern Brazil: a cross-sectional study. BMC Pregnancy Childbirth. 2015;15(1):
39. Shenoy H. Determinants of primary vs previous caesarean delivery in a tertiary care institution in Kerala, India. International Journal of Clinical Obstetrics and Gynaecology. 2019;3(5):229–236.
40. Das BN, Kanakamedala S, Mummadi MK. Factors associated with utilization of antenatal care services among rural women, Telangana, India. Int J Commun Med Public Health. 2018;5(7):
41. Hafeez M, Yasin A, Badar N, Pasha MI, Akram N, Gulzar B. Prevalence and indications of caesarean section in a teaching hospital. JIMSA. 2014;27(1):
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.