")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Magnitude and Associated Factors for Attitude and Practice Toward COVID-19 and Its Prevention Among the Residents of Gedeo Zone, Southern Ethiopia: A Community-Based Cross-Sectional Study
Authors Mola S , Aweke Z, Jemal B , Hussen R , Hailu S , Neme D, Mulugeta H , Zemedkun A
Received 25 August 2020
Accepted for publication 9 December 2020
Published 22 January 2021 Volume 2021:14 Pages 253—262
DOI https://doi.org/10.2147/RMHP.S277904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Simeneh Mola, Zemedu Aweke, Bedru Jemal, Robel Hussen, Sleshi Hailu, Derartu Neme, Hailemariam Mulugeta, Abebayehu Zemedkun
Dilla University, College of Medicine and Health Science, Dilla, Ethiopia
Correspondence: Simeneh Mola
Dilla University, College of Medicine and Health Science, PO Box 0419/13, Dilla, Ethiopia
Tel +251901091414
Email [email protected]
Background: COVID-19 first broke out in China, Hubei province on December 29, 2019, since then it took hundreds of thousand lives worldwide. Although all countries are taking varying degrees of measures to curb the dissemination, the virus is still spreading rapidly in all parts of the world. Adherence of people for COVID-19 precaution measures is one of the most important factors which determine the effectiveness of curbing the spread. However, without having a good attitude, the adherence of people toward precaution measures could be challenging. Therefore, this study aims to assess the attitude, practice, and associated factors of Gedeo zone of Southern Ethiopia region residents toward COVID-19 and its prevention.
Methods: A community-based cross-sectional study was conducted among 600 Gedeo zone residents of Southern Ethiopia. Bivariate and multivariate binary logistic regression were used to determine the association between dependent and independent variables. An adjusted odds ratio with 95% CI was used to show the strength of association. P-value< 0.05 was used to decide a statistically significant association.
Results: Most of the study participants (90.3%) have a good attitude toward COVID-19 and its prevention. Being a younger age group (AOR=3.82, 95% CI=1.76– 19.07), having a diploma and above (AOR=2.53, 95% CI=1.15– 7.50), having a chronic medical illness (AOR=2.73, 95% CI=1.01– 7.44), and using television/radio as a source of information (AOR=2.65, 95% CI=1.27– 5.54) were significantly associated with a good attitude toward COVID-19. On the other hand, only 20% of the study participants had good practice toward COVID-19 prevention. Educational status (P-value=0.00), occupation (P-value=0.01), and having a chronic medical illness (P-value=0.03), and use of religious teaching as information sources (P-value=0.02) were among the factors associated with good practice toward COVID-19 infection.
Conclusion: We conclude that, despite the presence of a good attitude in the majority of respondents, much work is needed to improve the poor practice of COVID-19 preventive measures.
Keywords: COVID-19, attitude, practice, associated factors, Gedeo zone, Southern Ethiopia
Background
Coronavirus disease 19 (COVID-19) is an extremely contagious viral infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and first broke out in China, Hubei province, on December 29, 2019.1,2
To date, June 7, 2020, about 7 million confirmed cases and 400,000 deaths have been reported worldwide.3 Yet the number of positive cases and deaths continues to rise rapidly. The difficulty of isolating suspected cases due to a long incubation period and its rapid contagiousness makes the disease challenging to control. The virus can also present in some peoples with few or no symptoms, which makes the spreading quicker and silent.1 Consequently, even developed nations like the US, Italy, Spain, France, and China are severely affected by the outbreak.3
So far the African continent has reported a relatively lower number of cases (131,324) and deaths (3,148).4 There is a debate on the reason for the lower number of cases and deaths. Some of the speculations are relatively lower testing rates, poor reporting habits, and the lower number of passengers coming to the continent.5–8 However, nothing can spare Africa from casualty but preparation and on-time response. Besides, there is a concern from the World Health Organization (WHO) that the disease could spread rapidly and cause devastating causalities in most African countries where it is difficult to exercise COVID-19 precaution measures.8
Since the start of the outbreak, the Ethiopian government has been taking different measures to tackle the spread based on WHO recommendations, starting from surveillance of people coming from aboard at the airport or border line to varying levels of contact tracing and isolation and quarantine of suspected cases. Awareness creations are also being given by different means such as television, radio, telecommunication, and social media to encourage peoples for handwashing, respiratory hygiene, and social distancing, and to refrain from handshaking and public gathering.9,10
Resources are also being mobilized from the citizens and foreign donors besides the preparation of health systems for possible upcoming overwhelms of hospitals by severely ill patients who require isolation, oxygen, and mechanical ventilation.11
In addition to government effort, people’s adherence to preventive measures is vital to accomplish success against the ongoing fight of COVID-19 pandemics. However, adherence for prevention measures for COVID-19 pandemics such as wearing a face mask, frequent hand washing, using soap or sanitizer, and avoiding hand shakes and public gatherings could be challenging in the absence of a good attitude in a community. The community-based follow-up study indicates that attitude has a significant impact on the lifestyle and compliance of the community. In other words the subjects with poor attitude toward health promotion seemed to run an unhealthier lifestyle and resist for any lifestyle modification recommendations compared to others.12 For any preventive programs in general to be successfully accomplished, people’s attitude must be taken into account. Therefore, this study hypothesized the association of socio-demographic factors and information sources with attitude and practice of Gedeo residents of Southern Ethiopian towards COVID-19.
Materials and Methods
A community-based cross-sectional study was conducted between March 27–31, 2020 to assess attitude, practice, and associated factors of Gedeo zone residents of Southern Nation, Nationality and People of Ethiopia (SNNPE) region towards COVID-19 and its prevention.
Southern Nation, Nationality and People of Ethiopia (SNNPE), commonly called Southern Ethiopia, is the third largest region in Ethiopia, with an estimated population of 20,768,000 (May 2018), almost a fifth of the country’s population. Gedeo is one of the 13 zones in SNNPR. It has six woreda (administrative districts) and two city administrations with a total population of 847,434 (424,742 men and 422,692 women) according to a 2007 Ethiopian center statistical agency report. Gedeo zone has one referral hospital and 38 health centers. The sample size was calculated based on the fact that no similar study had been conducted during the study period, so p and q were considered as 0.5 and margin of error (d) as 0.04 with 95% confidence interval (Z=1.96). By using a single proportion formula, sample size was determined to be 600.
n=Z2٭p٭q=600
d2
First, from the six districts and two city administrations in Gedeo zone, three districts (Yirgachefe, Gedeb, and Bule) and one city administration (Dilla) were selected using random selection. The sample size was allocated to each selected district and city proportionally based on the numbers of households by taking the list of households from respective administrative offices. Households are selected by random sampling using the sampling frame. Finally, adults (age>18 years) from each selected household were interviewed. In cases where there are more than one adult in a household, one is selected randomly.
An interviewer administered questionnaire was used during data collection. The questionnaire had different components including socio-demographic factors such as age, gender, marital status, education, occupation, religion, household size, and residence, and questions related with attitude and practice about COVID 19.
The questionnaire was prepared in English, translated into Amharic and Gedeu’ffa (commonly spoken languages in the study area), and translated back to English to check its consistency. Pretest was done on 5% of the sample in Dilla zuria district with relatively similar characteristics to the study area and minor amendment was done on the questionnaire. The data were collected by six trained health professionals supervised by three masters of public health professionals after 2 days of training regarding the questionnaires and a data collection procedure was given.
The dependent variables were the level of attitude and practice. The level of attitude and practice were assessed by questions which were derived after extensive literature review and WHO recommendations. There were nine attitude questions. All nine questions used Likert scale measurement. Each question was scored out of 5, making the total maximum score 45, and the minimum 9. Those participants who scored below 25 points on all nine questions were considered to have a poor attitude and those who scored 25 and above were considered to have a good attitude depending on the review of literature and expert recommendations.
Practice was assessed by seven questions on a Likert scale and each was scored up to 2 (0=no, 1=sometimes, 2=every time) and the overall maximum score being 14 and the minimum score 0. An overall score below 7 was considered as poor practice and 7 and above as good practice by using the cut-point of 50%.
Data were coded and entered into Epi-data 3.1 and were exported into SPSS version 25 for cleaning and analysis. Frequency tables and descriptive summaries were used to describe the study variables. Bivariate binary logistic regression analysis was used to see the crude association between dependent and independent variables. All explanatory variables which had an association in a bivariate analysis at a P-value less than or equal to 0.25 were entered into a multivariable binary logistic regression model. Multi-collinearity was checked by the variance inflation factor and tolerance level. An adjusted odds ratio with their 95% CI was used to show the strength of association. P-value<0.05 was used to declare the statistical significance of independent predictors.
Results
Socio-Demographic Characteristics of Respondents
From a total of 600 eligible respondents, 585 were analyzed and the remaining 15 were excluded due to lack of cleanness and incompleteness of the data. The mean age of the respondents was 33.7, with a standard deviation of ±11 years. About 41.9% of the study participants were female and 12.5% have no formal education. The majority (74.4%) of study participants were married and nearly half (54.4%) of the respondents live in rural areas. The socio-demographic characteristics of the respondents are shown in Table 1.
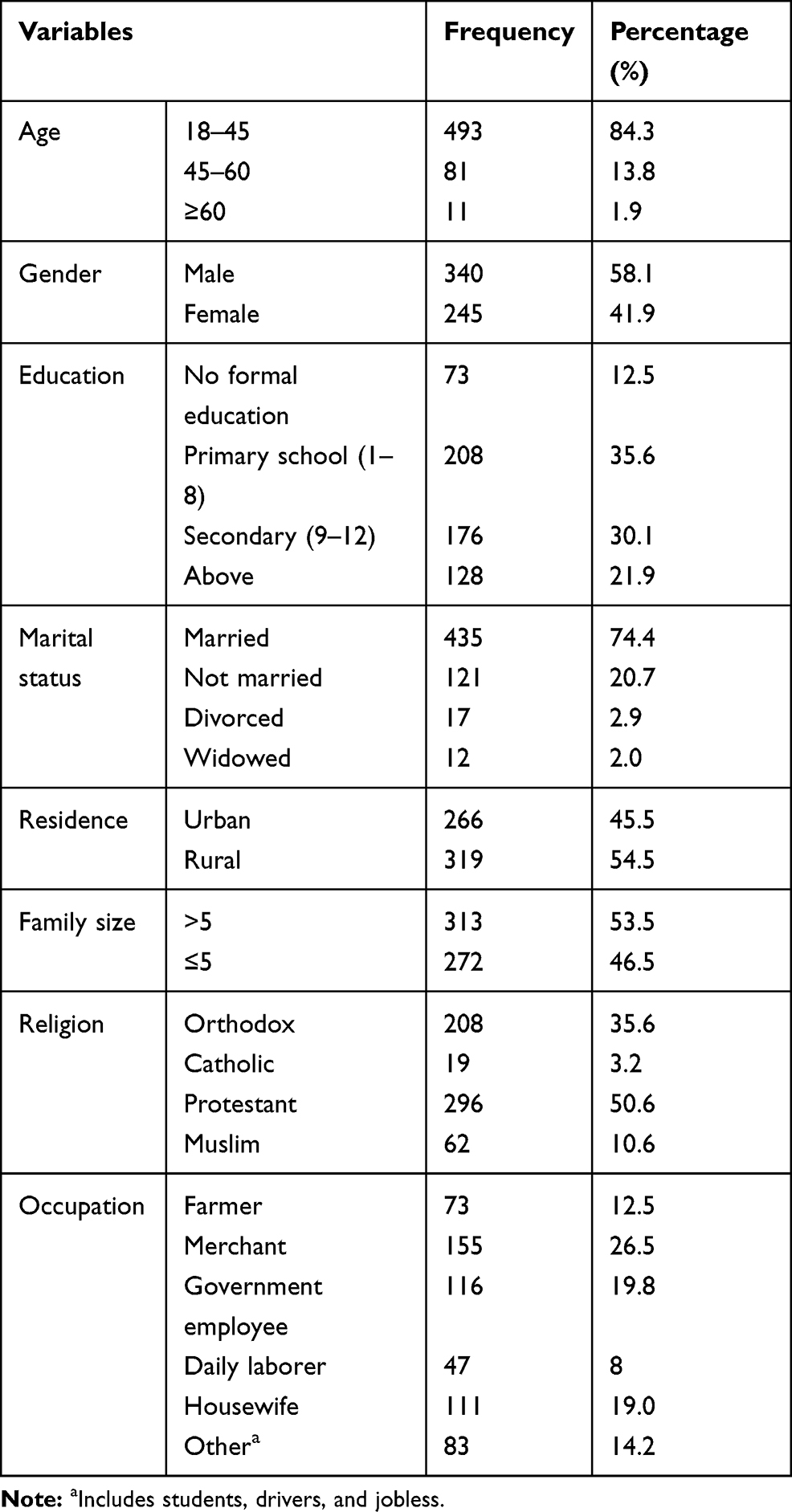 |
Table 1 Socio-Demographic Characteristics of Respondents |
Attitude Toward COVID-19 and Its Prevention
Nine questions, each question possesses five points, were used to assess the attitude of respondents. The mean score of respondents was 34.45 (±5.5) and 18 and 45 were the minimum and maximum scores, respectively. By using 25 points as a cut point, only 9.7% of the respondents scored below 25 points, but the majority of participants (90.3) had a good attitude toward COVID-19 and its prevention. As was shown in Table 2, from all respondents 61% of participants agree (strongly agree=21.4%, and agree=39.3%) that COVID-19 is a curse. Similarly, about a quarter (23.3%) of participants disagree (Strongly disagree=4.6%, and disagree=18.7%) that the virus could be transmitted in a hot climate.
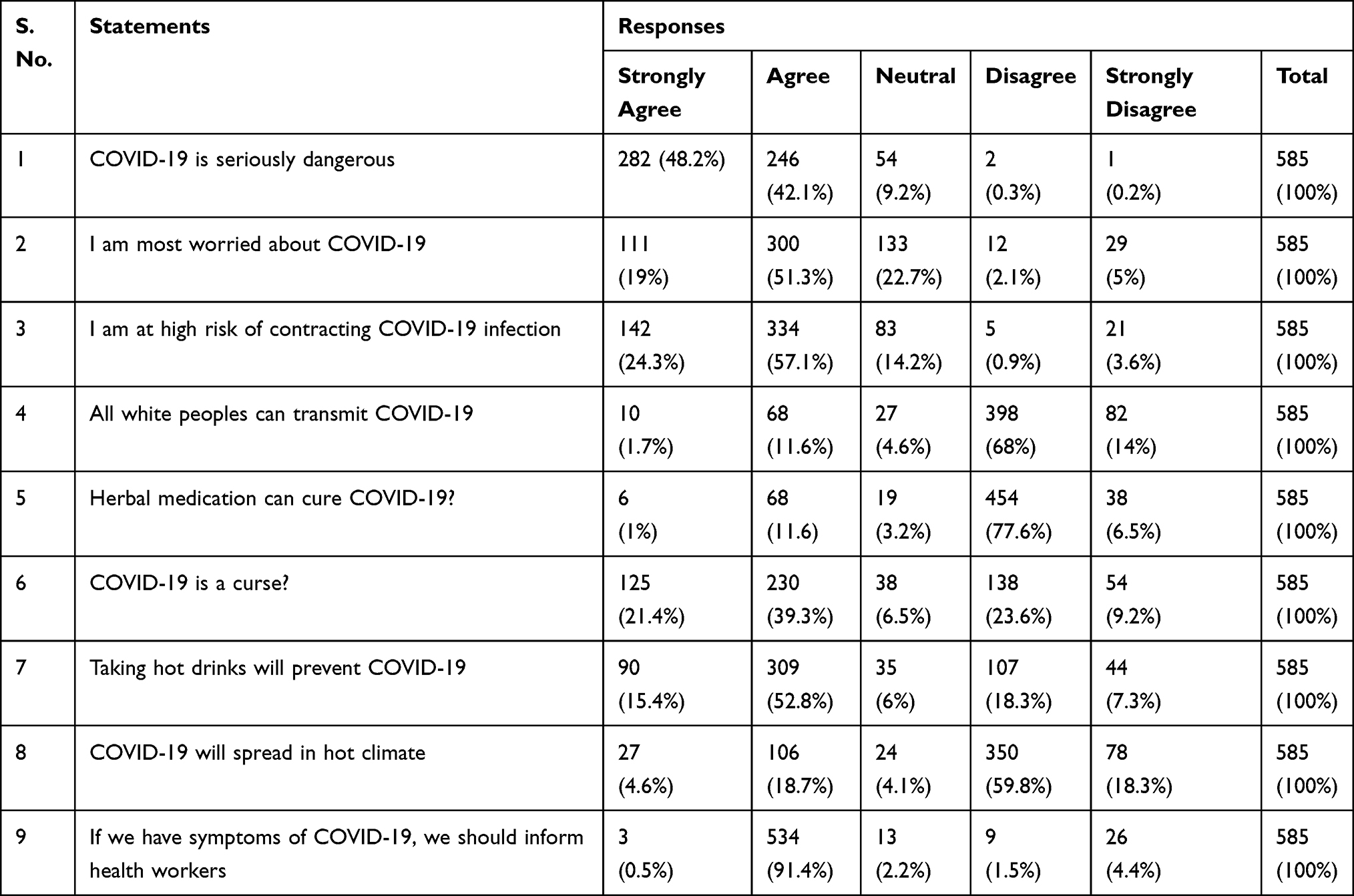 |
Table 2 Attitude Related Questions and Responses of Participants |
Practice Toward COVID-19 and Its Prevention
The majority of the respondents (80%) had poor practices toward COVID-19 prevention. Almost all respondents (93.7%) never used a face mask, while only 3.9% of respondents wore face mask every time outside the home. More than half of the respondents (58.3%) had been practicing hand washing using soap every time and 38.1% of respondents practiced sometimes, the rest did not practice hand washing using soap in a day. About 43.4% of participants practiced handshaking and only 10.3% of participants were practicing social distancing, while 61.4% and 28.3% never practiced social distancing or sometimes practiced social distancing, respectively (shown in Table 3).
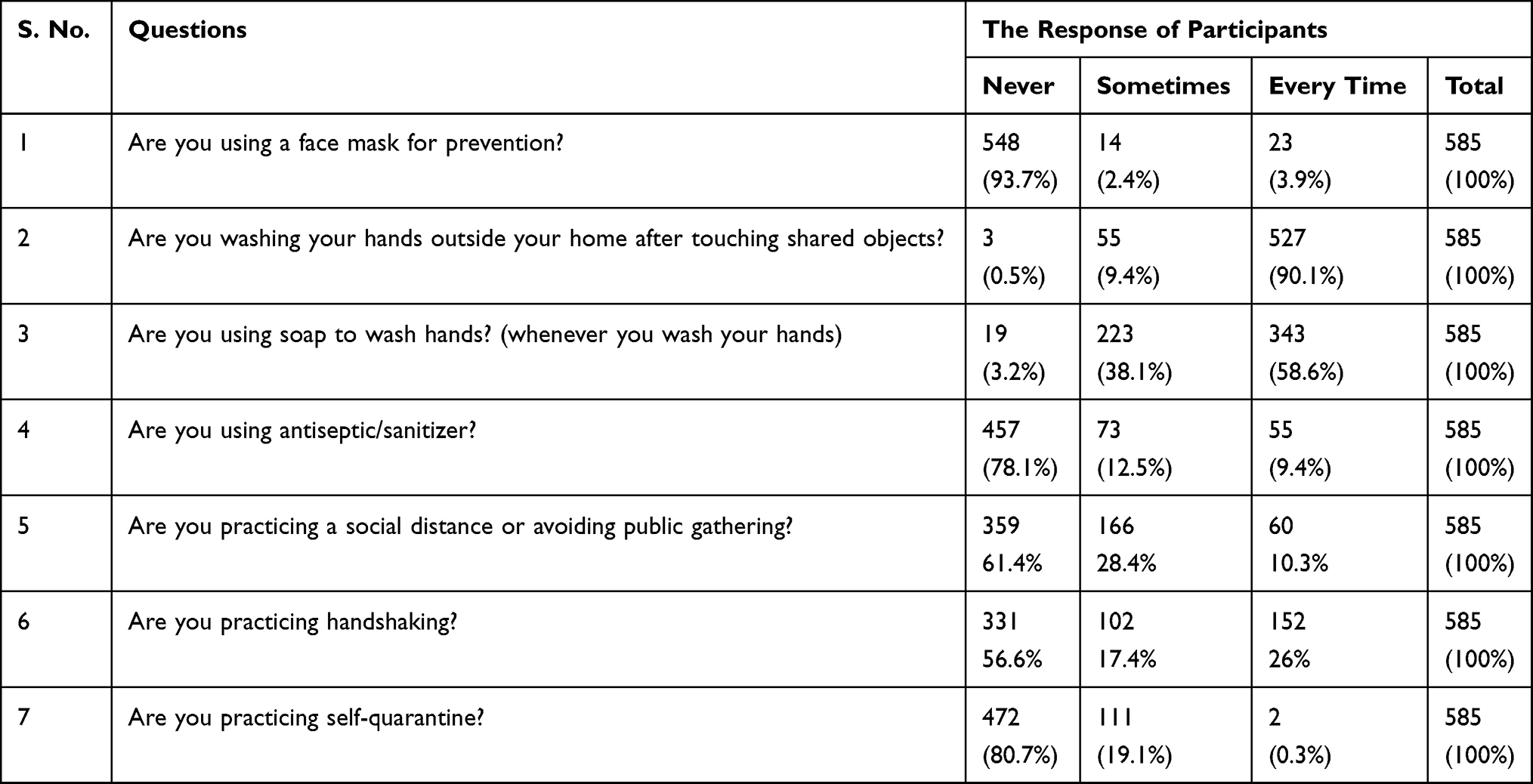 |
Table 3 Practice-Related Questions and Answers of Participants |
Associated Factors for Attitude Toward COVID-19 and Its Preventions
On multivariate analysis, we found that being aged between 18–44.9 years (AOR=3.82; 95% CI=1.76–19.07), having a chronic medical illness (AOR=2.73; 95% CI=1.01–7.44), and use of television/radio as a source of information (AOR=2.65; 95% CI=1.27–5.54) have a significant association with a good attitude. In addition, peoples who have education status of diploma or above are more likely to have a good attitude than people without any formal education, with an AOR (95% CI) of 2.53 (1.15–7.50) (shown on Table 4).
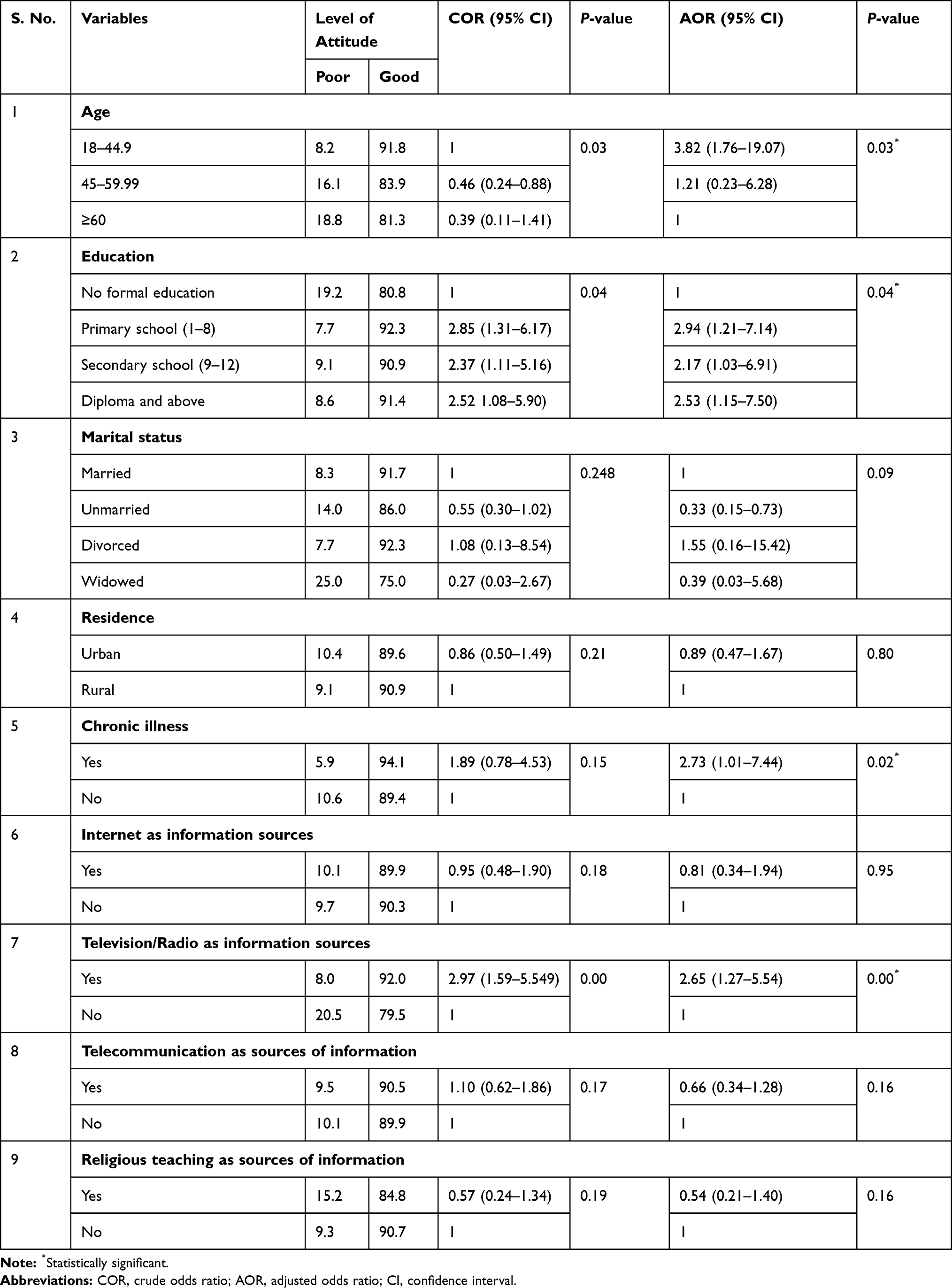 |
Table 4 Associated Factors for the Level of Attitude of Participants Toward COVID-19 |
Associated Factors for Practice Toward COVID-19 and Its Preventions
The presences of chronic illness, occupation, and uses of religious places as a source of information and educational status have an association with practice toward COVID-19 prevention. As shown in Table 5, people who have chronic medical illnesses are 1.88-times more likely to have good practices (AOR=1.88; 95% CI=1.04–3.39). Being a merchant or government employee increases the likelihood of good practice compared to farmers by 3- and 2-times, respectively. Those persons who have above secondary school educational levels are around 7-times more likely (AOR=6.90; 95% CI=2.09–22.75) to have good practice than persons who have no formal education.
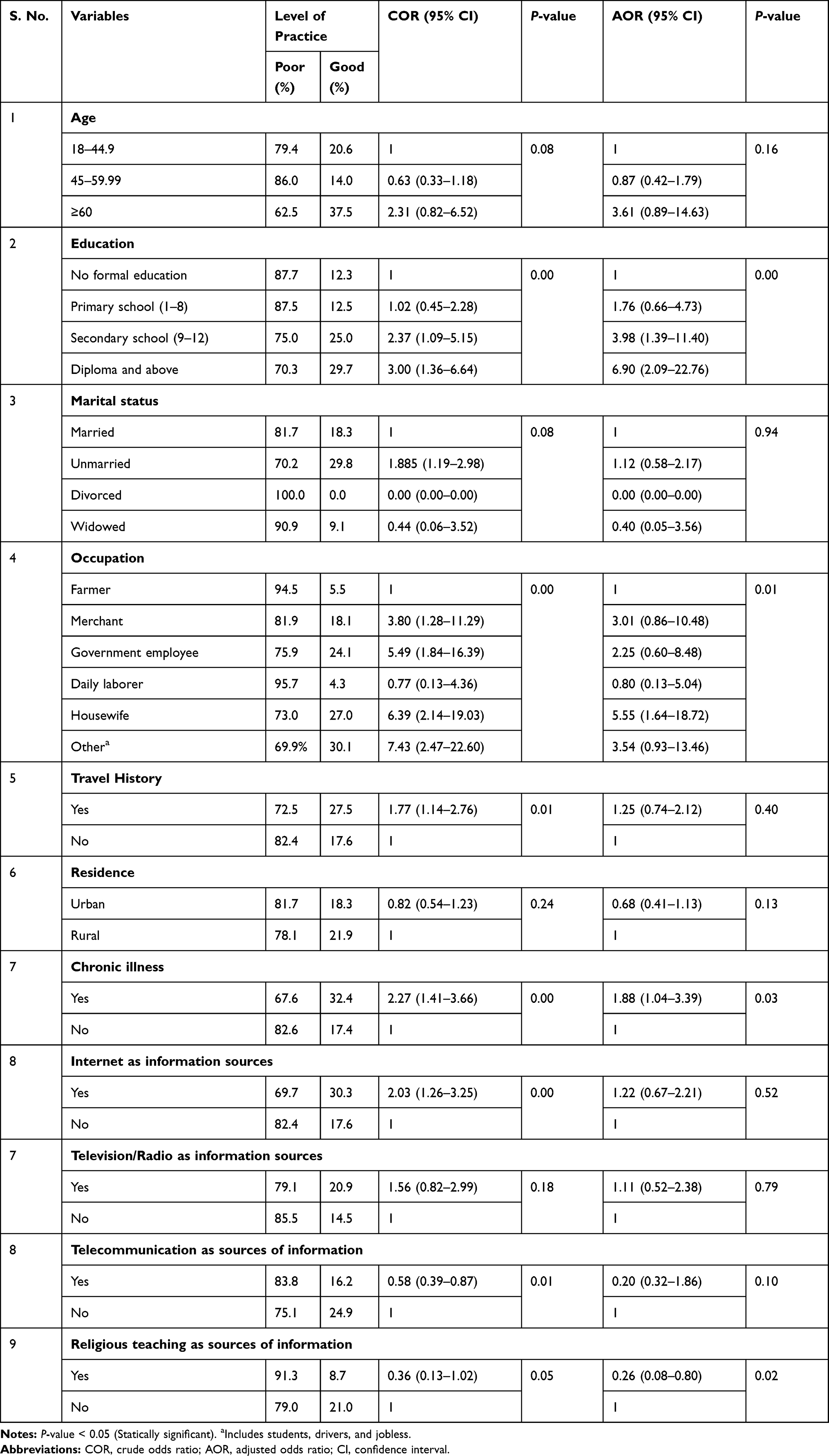 |
Table 5 Associated Factors for Level of Practice of Participants Toward COVID-19 Prevention |
Discussion
This study was conducted 2 weeks after the first confirmed COVID-19 case (March 13) in Ethiopia. At the time of data collection, there were 16 confirmed COVID-19 cases, but no deaths.13 We investigated the attitude, practice, and associated factors of Southern Ethiopian residents toward COVID-19 and its prevention.
In the present study, most of the study participants (90.3%) have a good attitude toward COVID-19 and its prevention. This finding is consistent with a study done in Iran, though it is far higher compared to a study done in Thailand which showed that 61.5% of the population have a good attitude toward COVID-19 and its prevention.14,15 The difference could be due to the fact that our study was conducted later than the study of Thailand. In between the period of two studies so many fatalities and crises happened around the world which could change the perception and attitude of mankind toward COVID-19 and its prevention.
This study also reveals that age, educational status, having a chronic medical illness, and using television/radio as a source of information have significant associations with attitude. Unlike the finding in other studies, younger age groups tend to have a good attitude. In fact, the majority of previous studies were conducted through online platforms, which are mainly utilized by the young population.17–19,21 Similarly, a study from Ethiopia on the same study area shows information sources had a strong association with knowledge levels.20 Chronic medical illness such as hypertension, diabetic mellitus, chronic respiratory diseases, and heart problems can increase the risk of hospital admission and death after contracting COVID-19 infection. In our study, patients who have chronic medical illness demonstrated a good attitude toward COVID-19 and its preventions. This finding is in line with a study done in Thailand and a bi-national survey conducted in Nigeria and Egypt by Hager et al.14,21
Practicing preventive measures like frequent hand washing using soap, uses of sanitizer, avoidance of handshaking, and public gathering and use of a face mask are of paramount importance for mitigating the spread of COVID-19 infection.16 However, our result revealed inadequate compliance of peoples for preventive measures, and only 20% of the population is practicing it favorably. For example, only 6.3% of participants have ever worn face masks or worn every day when leaving home. Comparing with the reports of Peeradone et al,14,17 in Taiwan, and Azlan et al in Malaysia in which there were 98% and 51% practice of face mask usage, respectively, our respondents have by far lower experience of face mask utilization. This huge variation can be explained primarily by a scarcity of protective equipment at the national level and secondly by the absence of apparent casualties in the country.
In addition to the lower proportion face mask users, social distancing/avoiding public gathering were practiced by only 10.3% of participants, which was much lower than the finding of Clements18 in the US, where there was 70% of social distancing practice. The variation in socioeconomic status and the magnitude of fatalities at a time of data collection in two areas can contribute to the differences.
On the other hand the majority of our participants always avoid handshaking (56.6%) and practice hand washing using soap (58.6%). These two practices relatively received better acceptance by the community in the study area. This might be due to the fact they are relatively cheaper tasks to exercise. However, in comparison to other low-income nations like Bangladesh in which there is 98.6% handwashing practice, our study revealed still there is a huge gap of hand washing in the study area which can be successfully addressed in spite of low resources.19
Educational status (P-value=0.00), occupation (P-value=0.01), and the presence of chronic illness (P-value=0.03) were significantly associated with practice against COVID-19 infection. This is finding partly in line with the study conducted by Peeradone Srichan et al,14 who demonstrated that age, gender, and educational status were factors for good practice. We found that educational level positively affects the practice of our respondents, though Azlan et al17 revealed no effect. The disagreement could be due to the variations in categorization techniques utilized for educational status.
Although the level of attitude in our study was relatively higher, it could not bring an apparent contribution for practice of the community toward COVID-19 prevention. This may be due to the shortage of necessary protective equipment such as sanitizers, face masks, soap and water supply, and the economic capacity of the community also does not allow the people to withdraw from risky activities such as public gathering. As a limitation, this study was cross-sectional, so a casual conclusion cannot be drawn. In addition, face-to-face interviews for assessment of practice may not be an accurate measurement compared to direct observations, which is less feasible and time consuming.
Conclusions
We conclude that the majority of responders have a good attitude toward COVID-19 and its preventions. However, preventive measures of COVID-19 were practiced by only a few respondents. Age, educational status, the presence chronic medical illness, and use of television as a source of information are associated factors for the level of attitude. The practice level of preventive measures is associated with educational status, occupation, presence of chronic medical illness, and use of religious teaching as sources of information.
Abbreviations
AOR, adjusted odds ratio; COVID-19, coronavirus 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SNNPE, Southern Nation, Nationality and Peoples of Ethiopia; SPSS, Statistical Package for Social Science; US, United States of America; WHO, World Health Organization.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was received from Dilla University College of medicine and health science ethical review board.
Verbal and written informed consent was obtained from each respondent before actual data collection. Issues of confidentiality were maintained by removing any identifiers from the questionnaire. The participants were informed of their right to participate and leave the study at any point in time.
Acknowledgments
We would like to thank Dilla University College of Medicine and Health Science for funding this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal the article has been submitted to; and agree to be accountable for all aspect of the work.
Funding
Dilla University has funded the research project.The sponsor has no role other than enhancing staff research and academic activity.The sponsor didn’t take part in any action of the research project other than funding.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.102433
2. Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R. COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020;24:91–98. doi:10.1016/j.jare.2020.03.005
3. WHO. Coronavirus Disease 2019 (COVID-19) Situation Report – 138. WHO; 2020.
4. WHO. COVID-19: Situation Update for the WHO African Region, External Report 7. WHO; 2020.
5. Gilbert M, Pullano G, Pinotti F, Valdano E, Poletto C, Boëlle P-Y. Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. Lancet. 2020;395(10227):871–877. doi:10.1016/S0140-6736(20)30411-6
6. Martinez-Alvarez M, Jarde A, Usuf E, et al. COVID-19 pandemic in west Africa. Lancet Global Health. 2020;8(5):e631. doi:10.1016/S2214-109X(20)30123-6
7. Sallam M, Dababseh D, Yaseen A, et al. Conspiracy beliefs are associated with lower knowledge and higher anxiety levels regarding COVID-19 among students at the University of Jordan. Int J Environ Res Public Health. 2020;17(14):4915. doi:10.3390/ijerph17144915
8. UN. Policy Brief: Impact of COVID-19 in Africa. UN; 2020.
9. WHO. COVID-19 BULLETIN ETHIOPIA. WHO; 2020.
10. Covid-19 Pandemic Preparedness And Response In Ethiopia Public Health Emergency Operation Center (Pheoc), 2020. Weekly Buletin (2).
11. WHO. Covid-19 Response Bulletin Ethiopia. WHO; 2020.
12. Mäntyselkä P, Kautiainen H, Miettola J. Beliefs and attitudes towards lifestyle change and risks in primary care – a community-based study. BMC Public Health. 2019;19(1):1049. doi:10.1186/s12889-019-7377-x
13. Notification note on additional COVID-19 Confirmed Cases: COVID-19 update Ethiopian public health institutes. 2020.
14. Srichan P, Apidechkul T, Tamornpark R, et al. Knowledge, Attitude and Preparedness to Respond to the 2019 Novel Coronavirus (COVID-19) Among the Bordered Population of Northern Thailand in the Early Period of the Outbreak: A Cross-Sectional Study. Available SSRN. 2020;24:3546046.
15. Erfani A. Knowledge, attitude and practice toward the novel coronavirus (covid-19) outbreak: a population-based survey in Iran. preprint. 2020. doi:10.2471/BLT.20.256651
16. Ranney ML, Griffeth V, Jha AK. Critical Supply Shortages — the Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N Eng J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141
17. Azlan AA, Hamzah MRH, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233668
18. Clements JM. Knowledge and Behaviors Toward COVID-19 Among US Residents During the Early Days of the Pandemic: cross-Sectional Online Questionnaire. JMIR Public Health Surveillance. 2020;6(2):e19161. doi:10.2196/19161
19. Rahman A, Sathi NJ. Knowledge, Attitude, and Preventive Practices toward COVID-19 among Bangladeshi Internet Users. Electronic J General Med. 2020;17(5):5. doi:10.29333/ejgm/8223
20. Aweke Z, Jemal B, Mola S, Hussien R. Knowledge of COVID-19 and its prevention among residents of the Gedeo zone, South Ethiopia. Sources of information as a factor. Curr Med Res Opin. 2020;12(just–accepted):1.
21. Hager E, Odetokun IA, Bolarinwa O, Zainab A, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: A bi-national survey in Africa. PLoS One. 2020;15(7):e0236918. doi:10.1371/journal.pone.0236918
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.