")
Back to Journals » Cancer Management and Research » Volume 11
Magnesemia: an independent risk factor of hypocalcemia after thyroidectomy
Authors Wang W , Meng C, Ouyang Q , Xie J, Li X
Received 3 June 2019
Accepted for publication 7 August 2019
Published 3 September 2019 Volume 2019:11 Pages 8135—8144
DOI https://doi.org/10.2147/CMAR.S218179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Wenlong Wang*, Chaoyang Meng*, Qianhui Ouyang, Jing Xie, Xinying Li
Division of Thyroid, General Surgery Department, Xiangya Hospital, Central South University, Changsha 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinying Li
Division of Thyroid, General Surgery Department, Xiangya Hospital, Central South University, No.87 Xiangya Road, Changsha 410008, People’s Republic of China
Tel +86 07 318 975 3710
Email [email protected]
Background: This study was designed to investigate the impact of serum magnesium (Mg) levels on hypocalcemia after thyroidectomy.
Patients and methods: In total, 242 patients with differentiated thyroid cancer were retrospectively analyzed.
Results: Multivariate regression analysis showed hypomagnesemia was an independent risk factor for hypocalcemia (P<0.001). While Mg in low levels (0.66 mmol/L ≤ Po-Mg ≤0.74 mmol/L) increased the risk of hypocalcemia, postoperative serum Ca (Po-Ca) levels were significantly lower in patients with hypomagnesemia than in patients with normomagnesemia (P=0.01), and the former patients suffered significant decreases in serum Ca (P=0.02). Compared to patients with a mild decline of serum Mg after surgery (ΔMg <0.17), serum Ca decline significantly increased (P<0.001) in patients with a severe decline of serum Mg (ΔMg ≥0.17), while the change in amounts of parathyroid hormone (PTH) after surgery was similar between the two groups (P>0.05). In patients with normal Po-Ca levels, hypomagnesemia increased the risk of symptoms related to hypocalcemia by 4.478 times (OR =5.478, 95% CI 1.724–17.403).
Conclusion: Hypomagnesemia, or even a low serum Mg level within the normal range, can increase the risk of hypocalcemia. After excluding the potential effects of PTH on serum magnesium and calcium, serum Mg reduction is one of the most important factors that influences postoperative serum Ca reduction. What’s more, hypomagnesemia is closely linked with symptoms.
Keywords: hypocalcemia, hypomagnesemia, thyroidectomy, magnesium, calcium
Thyroid carcinoma is the most common type of malignant tumor in the endocrine system, accounting for 1% of the systemic malignant tumors. In recent years, the incidence of thyroid cancer has increased rapidly. In 2015, there were approximately 90,000 new cases in China (22,200 males and 67,900 females), accounting for 6.55/100,000 in the general population. In addition, in females under 30 years old, thyroid carcinoma is the most common malignant tumor,1 and 89.9% are papillary carcinoma.2 Comprehensive treatment based on surgery, including postoperative radioactive iodine ablation therapy and thyroid-stimulating hormone (TSH) suppression therapy, is necessary for patients with thyroid cancer.3
The prognosis of thyroid carcinoma is rather good. The 5-year survival rate for localized thyroid cancer is 99.9%. The ten-year overall survival and cause-specific survival by surgery for differentiated thyroid carcinoma were 89.5–90.8% and 96.6–98.6%, respectively.3 However, postoperative complications like hypoparathyroidism and recurrent laryngeal nerve injury can have a large impact on the postoperative living quality of patients.4 The prevalence of hypocalcemia caused by hypoparathyroidism can reach up to 28.8%, including transient hypocalcemia (27.9%) and permanent hypocalcemia (0.9%).5 Further, some patients may suffer from hypomagnesemia at the same time. The prevalence of postoperative hypomagnesemia is about 10–72%6–8 and is related to hypocalcemia (RR =2.65, P=0.002).9 The relationship between calcium (Ca) and magnesium (Mg) metabolism is complex and mainly relates to the interaction of these cations with parathyroid hormone (PTH).9,10 There is a hypothesis that both postoperative hypocalcemia and hypomagnesemia are the result of the reduction of postoperative PTH (Po-PTH) since Mg levels can also be affected by PTH, which stimulates Mg reabsorption in the kidney and small intestine and Mg release from bone. Therefore, PTH greatly influences the regulation of the balance of Ca and Mg. Nevertheless, most recent studies neglected the potential impact of PTH when exploring the role of serum Mg in hypocalcemia; thus, the results of these studies did not reach an agreement. Garrahy et al9 showed that postoperative hypomagnesemia is an independent risk factor of postoperative hypocalcemia. When patients have postoperative hypocalcemia with hypomagnesemia, correcting Mg levels helps to relieve symptoms related to hypocalcemia.11 However, Xiaofei7 showed that postoperative hypomagnesemia was not a risk factor of hypocalcemia, and thus, that there is no need to monitor serum Mg levels regularly during perioperative period. Preoperative preventive Mg supplements could even raise the risk of postoperative hypocalcemia.12 Therefore, more research is essential to demonstrate the relationship between Mg and postoperative hypocalcemia, and more importantly, to reach a consensus on how to prevent postoperative hypocalcemia.
Our study discusses, from different perspectives, the relationship between postoperative hypocalcemia and serum Mg levels in patients with differentiated thyroid carcinoma on the basis of excluding the confounding influence of PTH in order to provide new evidence for the prevention and management of postoperative hypocalcemia.
Materials and methods
Study criteria
This study retrospectively analyzed 261 patients who had a thyroidectomy in Xiangya Hospital of Central South University during September 2017 to May 2018, of which 19 patients were excluded due to a lack of information or not meeting the inclusion criteria. In total, 242 patients were included. All the surgeries were performed by the same surgeon, and the treatment during the perioperative period was performed by the same medical care team. Background information was collected from all patients, including age, gender, surgery records, and postoperative pathology, etc. The study protocols were approved by the Ethics Committee of Xiangya Hospital, Central South University (Changsha, China). All study participants provided written informed consent to indicate their agreement for the clinical data to be used in clinical research and publication.
Inclusion criteria included patients with differentiated thyroid cancer who underwent thyroidectomy. Exclusion criteria included a previous history of thyroid surgery, abnormal serum albumin, PTH and/or Mg, and other underlying conditions, such as chronic kidney disease, primary and secondary hyperparathyroidism, pregnancy, serious diseases, and the use of drugs that affect blood Ca, PTH, and Mg levels, including lithium, octreotide, antiepileptic, glucocorticoid, diphosphate diuretic, and estrogen.
Diagnostic criteria
Serum Ca, Mg, PTH, and albumin levels were measured before and on the first day after operation. PTH was measured using the electrochemical luminescence immunoassay. Serum Ca and Mg were measured using the O-methylphenolphthalein complexone method. The normal reference value of PTH is 15–65 pg/mL, and the normal range of serum Ca and Mg is 2.0–2.6 mmol/L and 0.66–1.07 mmol/L, respectively.
Postoperative hypocalcemia includes biochemical and symptomatic hypocalcemia, and biochemical hypocalcemia was defined as serum calcium less than 2.0 mmol/L. Patients who presented symptoms like extremities, acupuncture numbness of hands, feet and mouth, trembles, convulsion, arrhythmia, positive Chvostek and Trousseau signs were defined as symptomatic hypocalcemia.13 Serious hypocalcemia patients can have systemic skeletal muscle spasm, limb twitches, and even life-threatening respiratory muscle and myocardium involvement. Patients with serum Mg below 0.66 mmol/L were diagnosed with hypomagnesemia. Adjusted serum Ca was calculated using the following formula: Adjusted Ca=0.8*(4.0–serum albumin)+serum Ca. A decline in PTH, Ca, and Mg was defined using the following formulas: ΔPTH=Pre-surgical PTH (Pre-PTH)–Post-surgical PTH (Po-PTH); ΔCa=Pre-surgical Ca (Pre-Ca)–Post-surgical Ca (Po-Ca); ΔMg=Pre-surgical Mg (Pre-Mg)–Post-surgical Mg (Po-Mg)
Grouping method
Five grouping methods were used according to different analytical purposes. First, to investigate the risk factors of postoperative hypocalcemia, a case–control study model was used and patients were subdivided into two groups: hypocalcemia and normal (patients without hypocalcemia). Second, to explore the impact of serum Mg at the low level of the normal range, patients were grouped into three groups according to Po-Mg level: hypomagnesemia (HM, Po-Mg <0.66 mmol/L), low level of normal range (LL, 0.66 mmol/L ≤ Po-Mg ≤0.74 mmol/L), and high level of normal range (HL, Po-Mg ≥0.74 mmol/L). Third, to better illustrate the influence of serum Mg on serum Ca, patients were divided into two groups: hypomagnesemia (patients with serum Mg below 0.66 mmol/L) and normomagnesemia (patients with normal serum Mg). A fourth grouping method was adopted for the same purpose as the third, and patients were divided into two groups according to ΔMg: mild decline of serum Mg (patients with ΔMg <0.17) and severe decline of serum Mg (patients with ΔMg ≥0.17). Fifth, to investigate whether hypomagnesemia is associated with symptoms, patients were divided into four groups: B-S- (patients with normal serum Ca without symptoms), B-S+ (patients with normal serum Ca, but with symptoms), B+S- (patients with serum Ca below 2.0 mmol/L without symptoms), and B+S+ (patients with serum Ca below 2.0 mmol/L as well as symptoms).13
Postoperative management
A 2000 mL fluid infusion was routinely administered during the perioperative period; after anesthesia recovery, a small liquid diet was allowed. On the first day after surgery, patients were subjected to a serum test to reexamine serum Ca, Mg, and PTH levels. If the postoperative serum Ca and PTH were normal and the patient was without discomfort, hospital discharge was permitted on the first or second postoperative day. All patients with hypocalcemia were given oral Ca supplements (Ca carbonate 1.2–3.6 g/d). For those who had symptoms, an intravenous injection of 10% Ca gluconate 10–20 mL was given slowly twice a day, and oral administration of a Ca tablet containing vitamin D was given three times a day. Serum Ca and PTH levels were monitored, and calcitriol was given if necessary. Medications were stopped after serum Ca and PTH levels returned normal. In our study, the lowest value of serum Mg was 0.54 mmol/L. None of the patients took Mg supplements, and all patients recovered to normal serum Mg levels when reexamined a month postoperatively.
Statistical analysis
SPSS19.0 statistical software was used to analyze the data obtained in the study. The measurement data complying with proper distribution are shown as the mean value and standard deviation. An independent-sample t test or variance analysis was used for inter-group comparison. Counting data were expressed in terms of frequency and incidence, while the comparison between counting data sets was performed by the Chi-square test and the Fisher precise test. Logistic regression analysis was used for multivariate analysis, and P<0.05 was considered statistically significant.
Results
Baseline group characteristics
In total, 242 patients with differentiated thyroid cancer were analyzed, of which there were 54 males (22.3%) and 188 females (77.7%). Their age range was 21–71 years, with a median age of 43 years. All patients with papillary thyroid carcinoma underwent central lymph node dissection (CND), of which 57 (23.5%) underwent unilateral CND, and the rest underwent bilateral CND. There were 52 (21.5%) cases with lateral lymph node dissection (LND), 24 (9.9%) cases with unilateral lobectomy, and 218 (90.1%) cases with total thyroidectomy. Further, 59 (24.4%) patients were found to have parathyroid gland dissection and accepted autotransplantation into the sternocleidomastoid. During the operation, the parathyroid glands were routinely searched, and 190 (78.5%) were found to have more than three parathyroid glands. Also, 87 (36.0%) patients were diagnosed with vitamin D deficiency before surgery. There were 123 (50.8%) cases of hypoparathyroidism after operation. The incidence of postoperative hypocalcemia was 38.4%, and 56 (23.1%) patients had symptoms. Additionally, 48 (19.8%) patients suffered from hypomagnesemia after operation, accounting for 32.3% of all patients with hypocalcemia. The percentage of other traits in all patients with hypocalcemia is shown in Table 1.
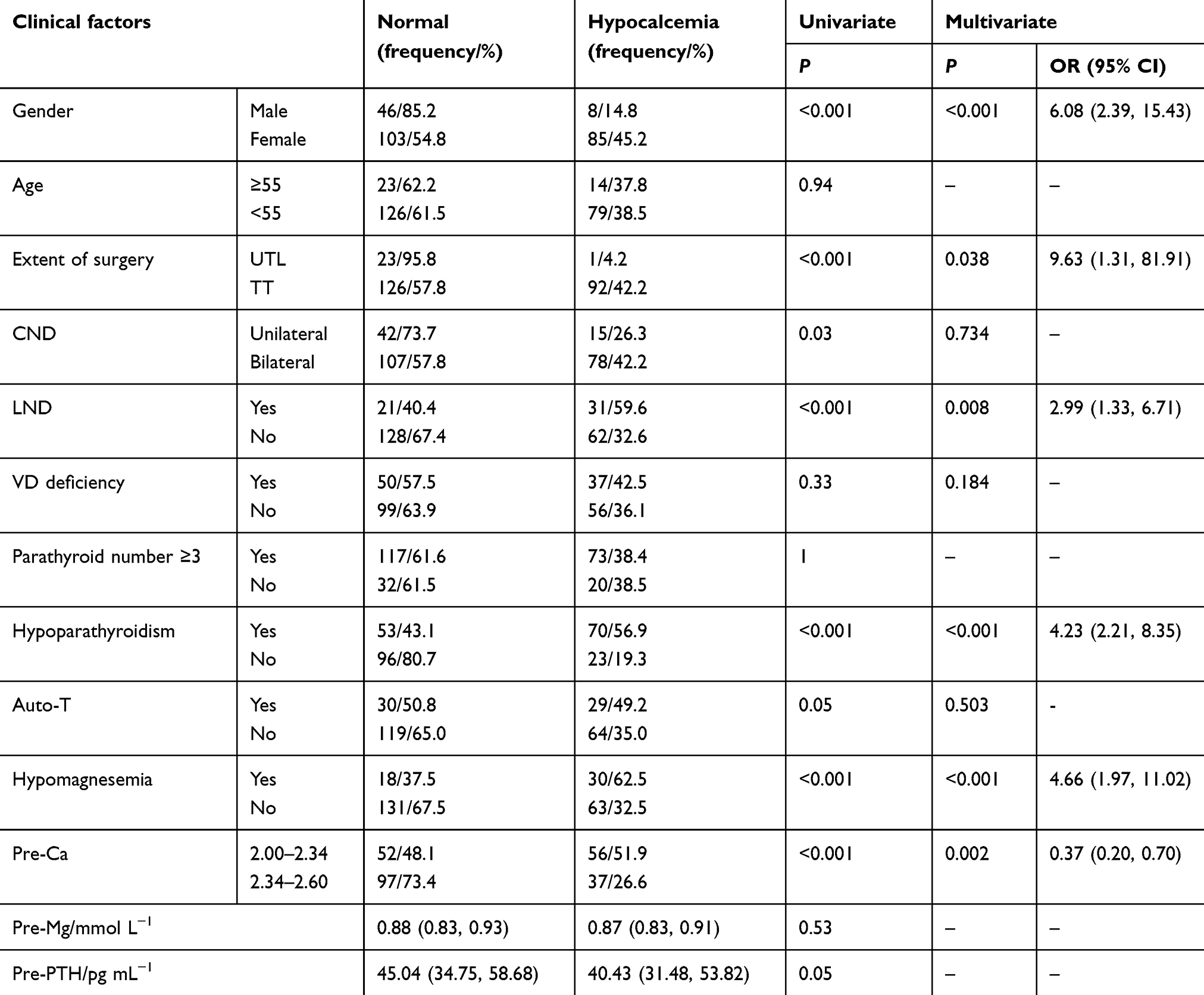 |
Table 1 Univariate and multivariate analysis of the effect of variables on the risk of postoperative hypocalcemia |
Analysis of risk factors for postoperative hypocalcemia
Univariate analysis showed that postoperative hypocalcemia was associated with gender, extent of surgery, LND, hypoparathyroidism, hypomagnesemia, Po-PTH, Po-Ca, Pre-Ca, and Po-Mg (P<0.05). The incidence of hypocalcemia in females with differentiated thyroid cancer was significantly higher than in males (45.2% vs 14.8%, P<0.001). Patients with unilateral lobectomies had lower incidence of hypocalcemia than those who underwent total thyroidectomy (4.2% vs 42.2%, P<0.001). Patients with LND were more prone to hypocalcemia after surgery (P<0.001). Hypocalcemia incidence in patients with unilateral CND, bilateral CND and LND was 26.3%, 42.2%, and 59.6%, respectively. The greater the extent of cervical lymph node dissection, the higher the risk of postoperative hypocalcemia, with a significant level of correlation (P<0.05). The incidence of hypocalcemia in the hypoparathyroidism group increased 1.92 times, compared to the normal parathyroid function group. Additionally, compared to normal patients, Po-Mg levels in patients with hypocalcemia significantly decreased (0.68±0.06 mmol/L vs 0.74±0.07, P<0.001), similar to Pre-Ca. Detailed information is shown in Table 1.
Logistic regression analysis showed that gender, extent of surgery, LND, Pre-Ca, hypoparathyroidism, and hypomagnesemia were independent risk factors for postoperative hypocalcemia (P<0.05). Female gender, total thyroidectomy, LND, hypoparathyroidism, hypomagnesemia, and Pre-Ca at the lower level of the normal range (2.00 mmol/L ≤ Pre-Ca <2.34 mmol/L) would, respectively, increase the risk of developing hypocalcemia (Table 1).
Effect of serum Mg at the low level of the normal range on hypocalcemia
To analyze whether serum Mg at the low level of the normal range is a risk factor for hypocalcemia, patients were divided into three groups according to Po-Mg level: hypomagnesemia (HM), low level of normal range (LL), and high level of normal range (HL). Compared to the LL group, the incidence of hypocalcemia was significantly higher in the HM group (62.5% vs 43.3%, P=0.028), and was significantly lower in the HL group (20.0% vs 43.3%, P=0.001). The risk of hypocalcemia in the LL group, determined by regression analysis, was lower than that of the HM group (OR =0.39, 95% CI 0.16–1.00) and higher than that of the HL group (OR =4.69, 95% CI 2.11–10.39) (Table 2).
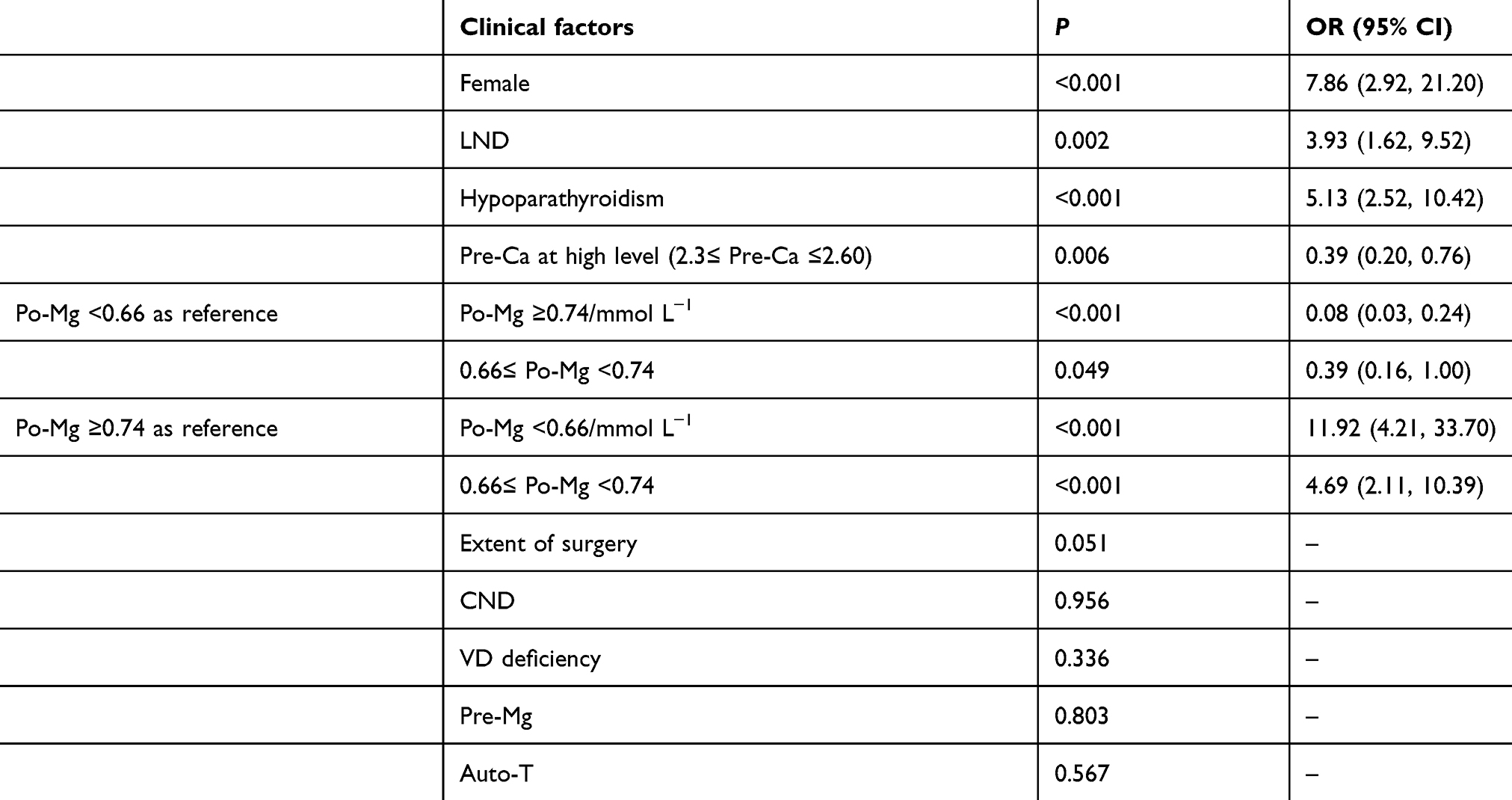 |
Table 2 Multivariate analysis of risk factors for postoperative hypocalcemia after serum Mg stratification |
Serum Mg reduction causing Ca reduction
Serum Mg and Ca can be regulated by PTH at the same time. To further explore whether serum Mg and Ca reductions are the common results of postoperative PTH decline or whether serum Mg reduction is one of the causes of serum Ca reduction, patients were divided into hypomagnesemia and normomagnesemia groups according to their Po-Mg level. The differences in Po-Ca value and ΔCa were analyzed. According to the results revealed in the section “Analysis of risk factors for postoperative hypocalcemia”, gender, extent of surgery, LND, Pre-Ca, and PTH can affect Po-Ca, so these indicators can be seen as confounding factors; however, none of these factors showed a statistical difference between these two groups, except for LND. After excluding the confounding influence of LND by excluding patients without LND, univariate analysis showed that only Po-Ca and ΔCa were significantly different between these two groups: Po-Ca levels were significantly lower (P=0.01) and ΔCa was markedly increased (P=0.02) in the hypomagnesemia group (Table 3). Furthermore, there was a significant difference in Po-Ca and ΔCa (P<0.001), but no statistical difference (P>0.05) in Pre-Ca, Pre-PTH, Po-PTH, ΔPTH, gender, or extent of surgery between the group with mild decline and one with severe decline of serum Mg after surgery. (Table 4).
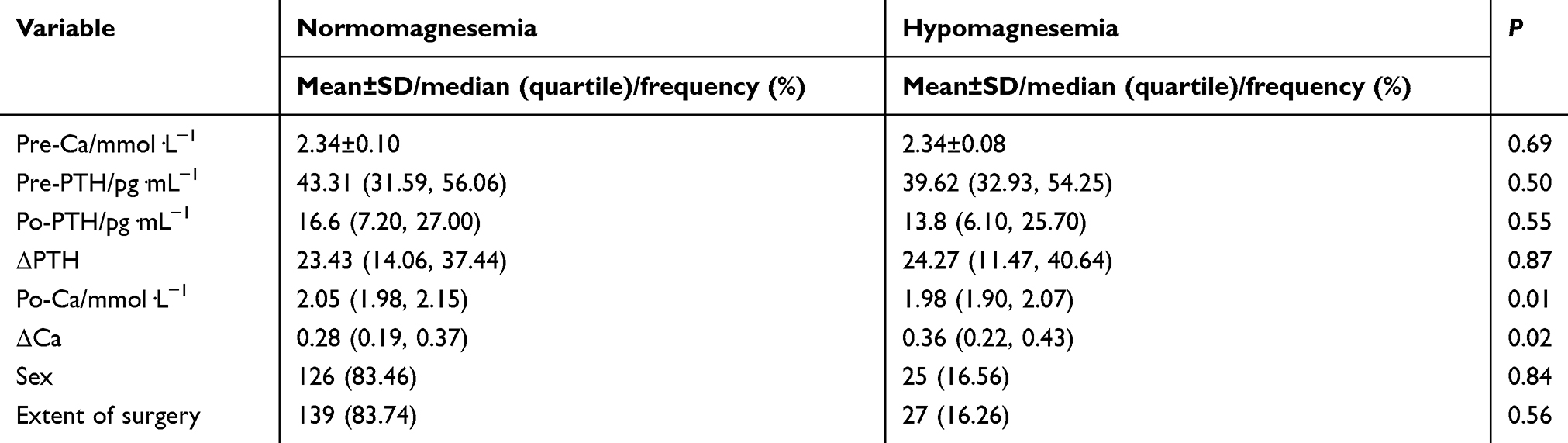 |
Table 3 Differences in Po-Ca and ΔCa levels between normomagnesemia and hypomagnesemia groups after excluding patients with LND |
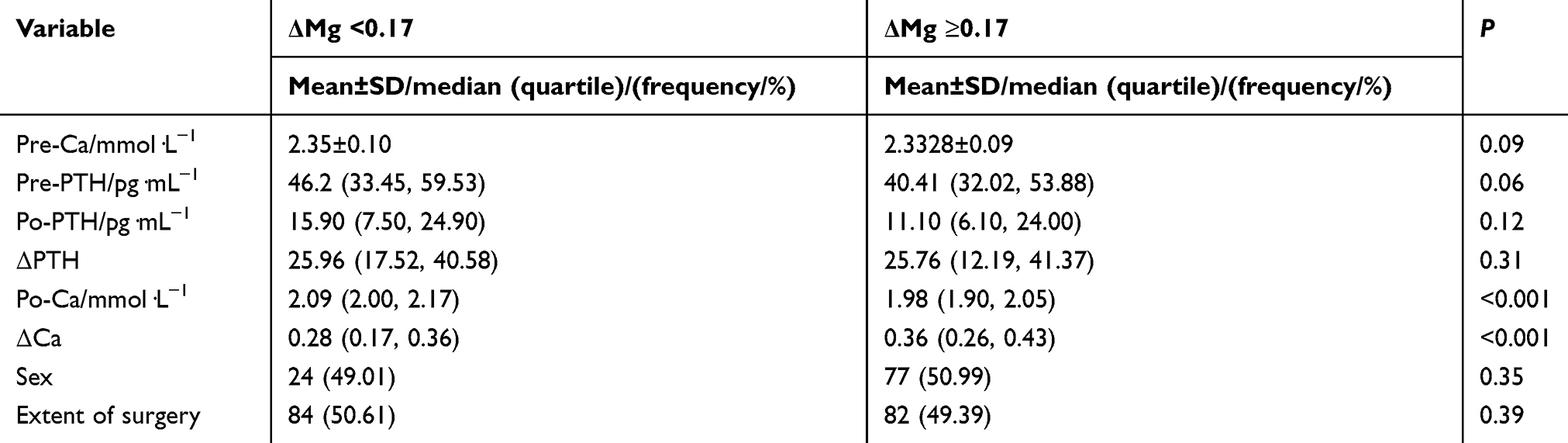 |
Table 4 Differences in Po-Ca and ΔCa between mild and severe decline of serum Mg group |
Effect of hypomagnesemia on symptoms
In order to analyze whether hypomagnesemia would increase the risk of symptoms, we subdivided patients into four groups, including B-S-, B-S+, B+S-, and B+S+. Univariate analysis showed that hypoparathyroidism (P=0.001) and hypomagnesemia (P=0.010) were significantly different between B-S- and B-S+ groups, while LND (P=0.001) and hypoparathyroidism (P=0.030) were statistically different between B+S- and B+S+ groups. Table 5 shows that the difference in Po-Mg between the B-S- and B-S+ groups was significant (P=0.01), but not between the B+S- and B+S+ groups (P=0.303) (Table 6). According to multivariate analysis, when the Po-Ca level was normal, hypoparathyroidism (OR =6.055, 95% CI 1.948–18.825) and hypomagnesemia (OR =5.478, 95% CI 1.724–17.403) were independent risk factors for symptoms. As shown by logistic regression analysis, hypomagnesemia was not a risk factor when serum Ca levels were below the normal range (P=0.223). However, in the B+S+ group, the incidence of hypomagnesemia was twice that of the B+S- group (31.3% vs 16.7%) (Tables 5 and 6).
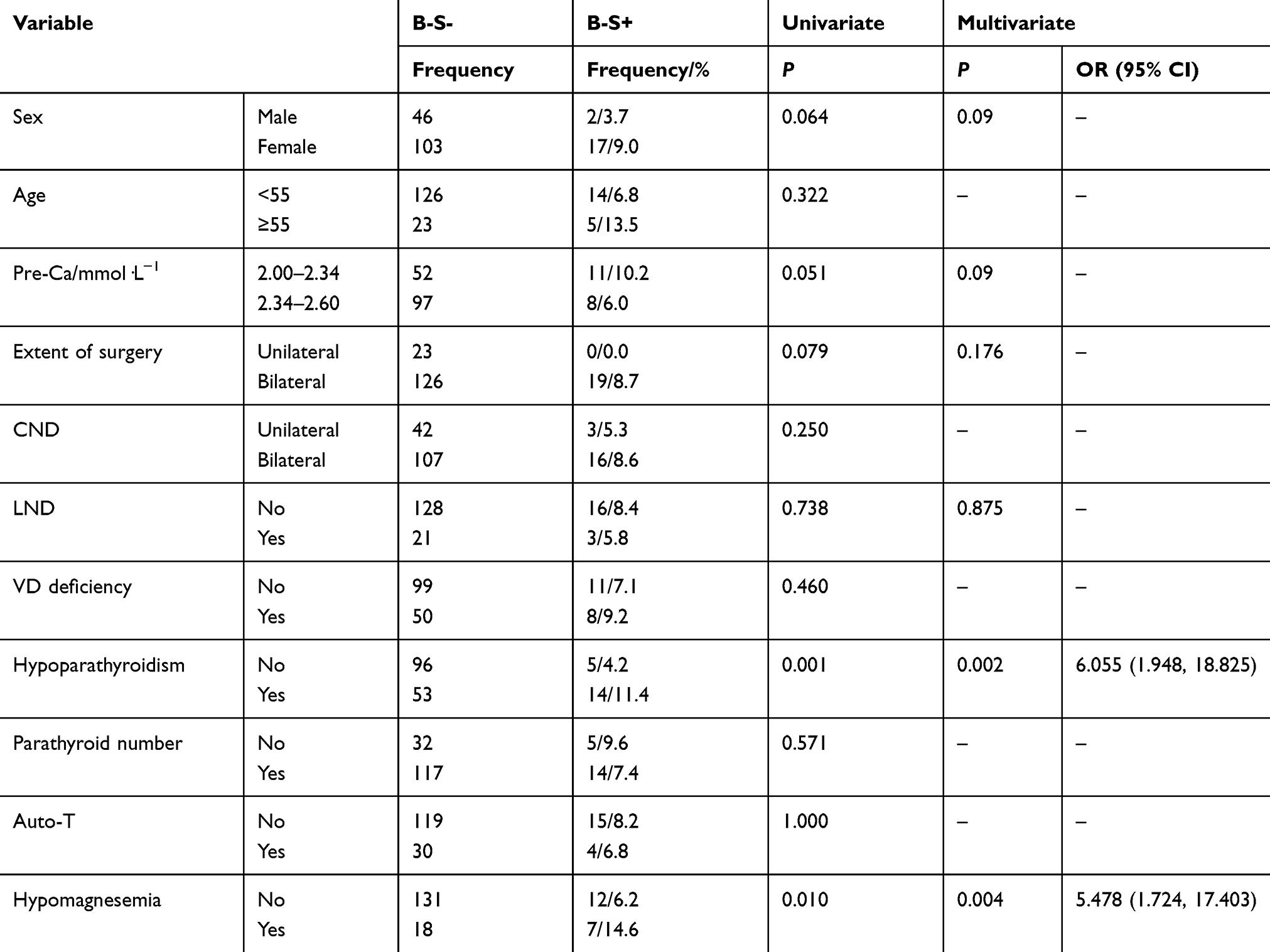 |
Table 5 Risk factors identification of symptoms in patients with normal serum Ca |
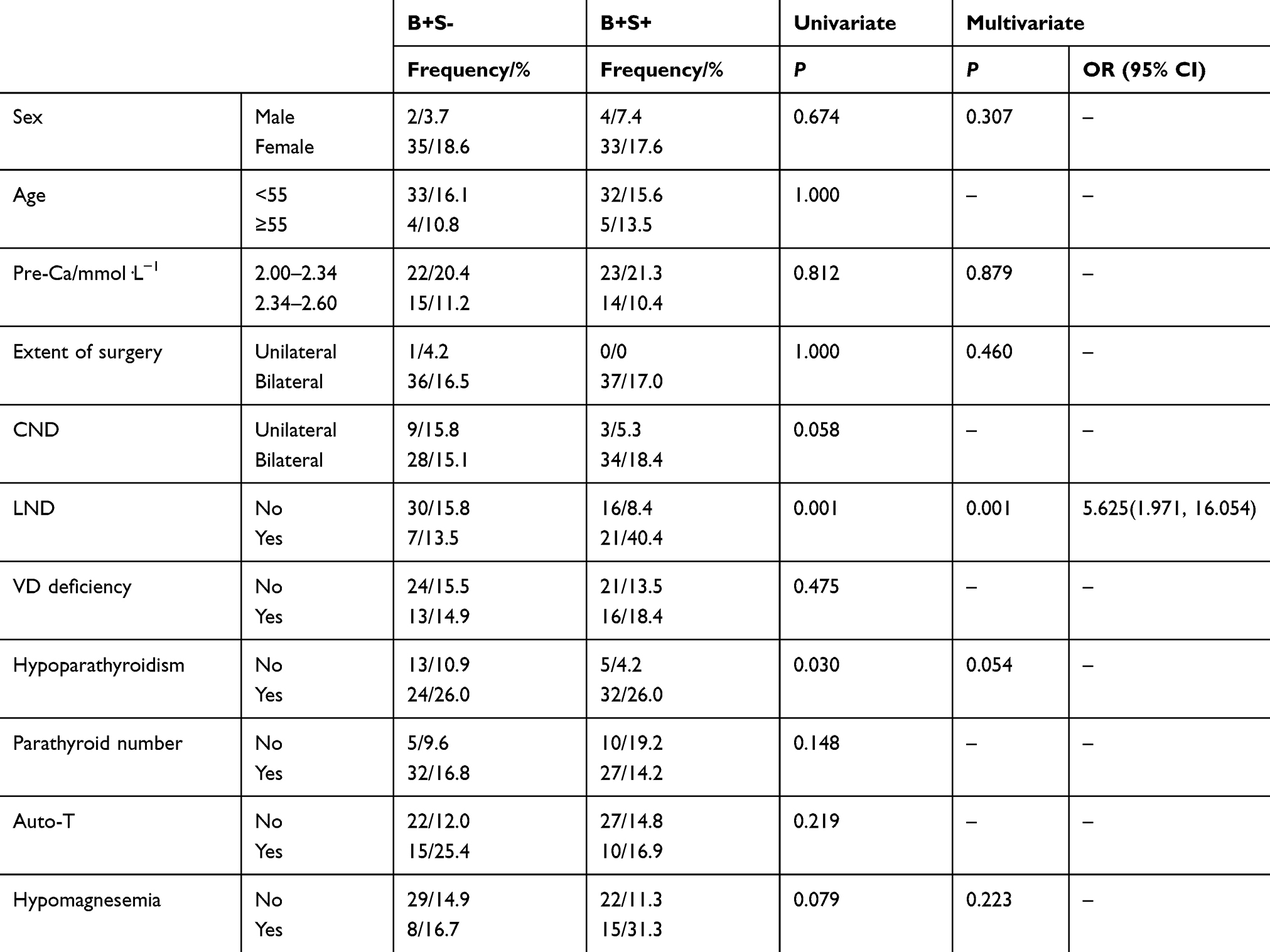 |
Table 6 Risk factors identification of symptoms in patients with serum Ca below normal range |
Discussion
Hypocalcemia is one of the most common complications following thyroidectomy. The occurrence of hypocalcemia is mainly attributed to hypoparathyroidism when parathyroid glands are devascularized, injured, or dissected during surgery.9 In addition to hypoparathyroidism, other factors decreased by more than 70%, like PTH (OR =6.69), malignancy (OR =7.18), and Grave’s disease (OR =2.40), which would increase the risk of hypocalcemia after thyroidectomy.14,15 Furthermore, toxic goiter, female gender, age of greater than 50 years, an operation duration over 120 mins, preoperative low vitamin D concentration, etc. are also associated with postoperative hypocalcemia (P<0.05).16,17 Postoperative hypocalcemia can not only cause clinical symptoms but can also become a major contributing factor of prolonged hospitalization time. Therefore, it is necessary to find risk factors for hypocalcemia following thyroidectomy to help guide clinical practice.18,19
Our study found gender, extent of surgery, LND, pre-Ca, hypoparathyroidism, and hypomagnesemia were independent risk factors for postoperative hypocalcemia. Female gender, TT, LND, hypoparathyroidism, hypomagnesemia, and pre-Ca at the lower level of the normal range (2.00 mmol/L ≤ Pre-Ca <2.34 mmol/L) increased the risk of developing hypocalcemia by 5.08, 8.63, 1.99, 3.23, 3.66, and 1.70 times, respectively. Therefore, for women, some of these factors can be targeted for preventive Ca therapy to reduce the incidence of hypocalcemia. In addition, hypomagnesemia and hypocalcemia are also closely related. The incidence of hypomagnesemia after thyroidectomy was 19.80%, and it is much higher in patients with hypocalcemia. Moreover, the risk of hypocalcemia in patients with hypomagnesemia was 4.66 times higher than that in patients with normomagnesemia. As for the cause of postoperative hypomagnesemia, Wilson et al10 suggested that it might be related to hemodilution induced by intravenous rehydration and reduced absorption of magnesium in the intestine and kidney due to postoperative hypoparathyroidism. Hypomagnesemia in patients after thyroidectomy is often accompanied by hypocalcemia.20,21 To better understand the relationship between Mg and Ca levels, some researchers have clinically demonstrated the complex relationship between serum Mg and Ca levels. Luo et al6 analyzed the clinical data of 304 patients undergoing TT and found that postoperative hypomagnesemia was an independent risk factor for biochemical hypocalcemia (OR =2.010, P=0.017). Hammerstad et al22 evaluated the risk factors for hypocalcemia in 40 patients with Graves’ disease and found that the reduction in serum Mg at 48 hrs after surgery could predict the occurrence of permanent hypocalcemia (P=0.015). Furthermore, Fatemi et al23 subjected 26 healthy people to a 3-week low-magnesium diet. After 3 weeks, accompanied by the decrease of serum Ca from 2.36±0.02 mmol/L to 2.31±0.03 mmol/L (P<0.05), serum Mg decreased from 0.80 mmol/L to 0.61 mmol/L, the Mg retention rate increased from 11±4% to 62±4% (P<0.001). Therefore, Fatemi suggested that magnesium deficiency can lead to hypocalcemia. These studies indicate that there is a close relationship between Mg and Ca.
In order to further analyze the relationship between serum Mg and hypocalcemia, patients were divided into HM, LL, and HL group according to Po-Mg levels. Compared to the LL group, the incidence of hypocalcemia was significantly higher in the HM group and much lower in the HL group. Regression analysis showed that the risk of hypocalcemia in the LL group was 0.39 times that of patients in the HM group and 4.69 times that of patients in the HL group.
This is the first study to clinically prove that serum Mg at the low level of the normal range increases postoperative hypocalcemia risk. The results of this study are in accordance with basic scientific research. It has already been shown that Mg and Ca have similar biochemical properties and share the same steady-state regulation system, including absorption from the small intestine and reabsorption and excretion from renal tubules.20,24 As the second most abundant cation in the cell, Mg2+ acts as a cofactor of more than 300 enzymatic reactions, involving energy metabolism and protein and nucleic acid synthesis.25,26 Further, Mg2+ participates in the process of synthesis and/or secretion of PTH by regulating the activity of the calcium sensitive receptor (CaSR) signal axis, which affects the sensitivity of target organs to PTH and participates in the synthesis of 1,25(OH)2D3.25,27,28 Therefore, to some extent, hypomagnesemia or a decrease in serum Mg increases hypocalcemia risk after thyroidectomy.
Simultaneously, Mg metabolism could be regulated by PTH, which can stimulate Mg reabsorption from the kidney and small intestine and cause the release of Mg from bone.10,29 At present, most clinical studies ignore the potential impact of PTH on the relationship between serum Mg and hypocalcemia, and thus, a consensus has not been reached. To further explore whether serum Mg and Ca reduction are the common results of PTH decline after thyroidectomy or whether serum Mg reduction is one of the causes of serum Ca reduction, we compared the differences in Po-Ca and ΔCa between hypomagnesemia and normomagnesemia groups. The results showed Po-Ca in the hypomagnesemia group was significantly lower than that of the normomagnesemia group, and ΔCa of the former group significantly increased. Further analysis indicated that, in contrast to patients with a mild decline of serum Mg, Po-Ca levels were remarkably lower, and ΔCa observably increased in patients with a severe decline of serum Mg. Nevertheless, there was no marked change in PTH between the hypomagnesemia and normomagnesemia group or between groups with a mild or severe decline of serum Mg. These results showed postoperative serum Mg and Ca reduction are not the common results of PTH decline, but that serum Mg reduction is one of the causes of postoperative serum Ca reduction.
In addition, we also investigated whether hypomagnesemia would increase the risk of symptoms. Currently, only a small number of studies have reported the influence of postoperative hypomagnesemia on symptoms.11,30,31 Clinical studies have found that patients with hypomagnesemia after surgery are more likely to develop symptoms and neglecting to correct hypomagnesemia may prolong the duration of these symptoms. In contrast, supplementing Ca as well as Mg is conducive to relieving symptoms and acute metabolic disorders sooner.20 Our study found that hypomagnesemia was an independent risk factor for postoperative hypocalcemia in patients with normal serum Ca, but not in those with serum Ca levels below the normal range. Nonetheless, the incidence of hypomagnesemia in group B+S+ was nearly twice that of group B+S-. Unlike in Garrahy et al’s9 study, and although multivariate analysis showed that hypomagnesemia was not an independent risk factor for the symptoms when postoperative serum Ca was below the normal range, we still believe that hypomagnesemia increases the risk of symptoms for serum Ca levels below the normal range and was the main cause of symptoms, which means the impact of other factors could be overshadowed. Similarly, Cherian et al8 studied 50 patients who underwent thyroidectomies and found that hypomagnesemia could increase the prevalence of the symptoms. It is recommended that clinicians routinely monitor serum Ca and Mg levels in patients with severe hypocalcemia and hypomagnesemia. When symptoms occur after thyroidectomy, both serum Ca and Mg should be corrected and monitored over time. This is beneficial to promoting the recovery of serum Ca and PTH and contributes to the alleviation of symptoms.
Conclusion
In summary, hypocalcemia was closely related to serum Mg after thyroidectomy. Hypomagnesemia was an independent risk factor for hypocalcemia after thyroidectomy. The decrease of serum Mg and Ca after thyroidectomy was not the common result of a decrease in PTH, but serum Mg decline was one of the important influential factors for the decrease of serum Ca after thyroidectomy. In addition, hypomagnesemia also increased the risk of symptoms; therefore, serum Ca and Mg should be routinely monitored after thyroidectomy. For patients with hypocalcemia and hypomagnesemia, Mg supplementation is conducive to reducing the occurrence of symptoms.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant No. 81672885). We thank MedEditing LLC for its linguistic assistance during the preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
2. Wang F, Zhao S, Shen X, et al. BRAF V600E confers male sex disease-specific mortality risk in patients with papillary thyroid cancer. J Clin Oncol. 2018;36(27):2787–2795. doi:10.1200/JCO.2018.78.5097
3. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines task force on thyroid nodules and differentiated thyroid cancer. THYROID. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
4. Bilimoria KY, Zanocco K, Sturgeon C. Impact of surgical treatment on outcomes for papillary thyroid cancer. Adv Surg. 2008;42(42):1–12. doi:10.1016/j.yasu.2008.03.001
5. Puzziello A, Rosato L, Innaro N, et al. Hypocalcemia following thyroid surgery: incidence and risk factors. A longitudinal multicenter study comprising 2,631 patients. ENDOCRINE. 2014;47(2):537–542. doi:10.1007/s12020-014-0209-y
6. Luo H, Yang H, Zhao W, et al. Hypomagnesemia predicts postoperative biochemical hypocalcemia after thyroidectomy. BMC Surg. 2017;17(1). doi:10.1186/s12893-017-0258-2
7. Wang X, Zhu J, Liu F, Gong Y, Li Z. Postoperative hypomagnesaemia is not associated with hypocalcemia in thyroid cancer patients undergoing total thyroidectomy plus central compartment neck dissection. Int J Surg. 2017;39:192–196. doi:10.1016/j.ijsu.2017.01.085
8. Cherian AJ, Gowri M, Ramakant P, Paul TV, Abraham DT, Paul MJ. The role of magnesium in post-thyroidectomy hypocalcemia. World J Surg. 2016;40(4):881–888. doi:10.1007/s00268-015-3347-3
9. Garrahy A, Murphy MS, Sheahan P. Impact of postoperative magnesium levels on early hypocalcemia and permanent hypoparathyroidism after thyroidectomy. Head Neck. 2016;38(4):613–619. doi:10.1002/hed.23937
10. Wilson RB, Erskine C, Crowe PJ. Hypomagnesemia and hypocalcemia after thyroidectomy: prospective study. World J Surg. 2000;24(6):722–726. doi:10.1007/s002689910116
11. Griffin TP, Murphy M, Coulter J, Murphy MS. Symptomatic hypocalcaemia secondary to PTH resistance associated with hypomagnesaemia after elective embolisation of uterine fibroid. Case Rep. 2013;2013:r2013008708. doi:10.1136/bcr-2013-008708
12. Besic N, Zagar S, Pilko G, Peric B, Hocevar M. Influence of magnesium sulphate infusion before total thyroidectomy on transient hypocalcemia – a randomised study. Radiol Oncol. 2008;42(3):143–150. doi:10.2478/v10019-008-0010-8
13. Wang W, Xia F, Meng C, Zhang Z, Bai N, Li X. Prediction of permanent hypoparathyroidism by parathyroid hormone and serum calcium 24h after thyroidectomy. Am J Otolaryngol. 2018;39(6):746–750. doi:10.1016/j.amjoto.2018.08.005
14. Docimo G, Ruggiero R, Casalino G, Del GG, Docimo L, Tolone S. Risk factors for postoperative hypocalcemia. Updates Surg. 2017;69(2):255–260. doi:10.1007/s13304-017-0452-x
15. Sitges-Serra A, Gallego-Otaegui L, Suarez S, Lorente-Poch L, Munne A, Sancho JJ. Inadvertent parathyroidectomy during total thyroidectomy and central neck dissection for papillary thyroid carcinoma. Surgery. 2017;161(3):712–719. doi:10.1016/j.surg.2016.08.0
16. Lang BH, Wong KP, Cowling BJ, Fong YK, Chan DK, Hung GK. Do low preoperative vitamin D levels reduce the accuracy of quick parathyroid hormone in predicting postthyroidectomy hypocalcemia? Ann Surg Oncol. 2013;20(3):739–745. doi:10.1245/s10434-012-2666-y
17. Thomusch O, Machens A, Sekulla C, Ukkat J, Brauckhoff M, Dralle H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. SURGERY. 2003;133(2):180–185. doi:10.1067/msy.2003.61
18. Wang Y, Bhandari A, Yang F, et al. Risk factors for hypocalcemia and hypoparathyroidism following thyroidectomy: a retrospective Chinese population study. Cancer Manag Res. 2017;9:627–635. doi:10.2147/CMAR.S148090
19. Baldassarre RL, Chang DC, Brumund KT, Bouvet M. Predictors of hypocalcemia after thyroidectomy: results from the nationwide inpatient sample. ISRN Surg. 2012;2012:1–7. doi:10.5402/2012/838614
20. Hodgkinson A, Marshall DH, Nordin BE. Vitamin D and magnesium absorption in man. Clin Sci (Lond). 1979;57(1):121–123.
21. Ramakant AJCM, Paul TVPD. The role of magnesium in post-thyroidectomy hypocalcemia. World J Surg. 2016;40(4):881–888. doi:10.1007/s00268-015-3347-3
22. Hammerstad SS, Norheim I, Paulsen T, Amlie LM, Eriksen EF. Excessive decrease in serum magnesium after total thyroidectomy for Graves’ disease is related to development of permanent hypocalcemia. World J Surg. 2013;37(2):369–375. doi:10.1007/s00268-012-1843-2
23. Fatemi S, Ryzen E, Flores J, Endres DB, Rude RK. Effect of experimental human magnesium depletion on parathyroid hormone secretion and 1,25-dihydroxyvitamin D metabolism. J Clin Endocrinol Metab. 1991;73(5):1067–1072. doi:10.1210/jcem-73-5-1067
24. Meng C, Xie J, Wang W, Xia F, Li X. Hypomagnesemia and post-thyroidectomy hypocalcemia: molecular mechanisms and clinical potential. Int J Clin Exp Med. 2018;11(11):11554–11566.
25. Gilman AG. Guanine nucleotide-binding regulatory proteins and dual control of adenylate cyclase. J Clin Invest. 1984;73(1):1–4. doi:10.1172/JCI111179
26. Xia F, Wang W, Jiang B, Chen Y, Li X. DNA methylation-mediated silencing of miR-204 is a potential prognostic marker for papillary thyroid carcinoma. Cancer Manag Res. 2019;11:1249–1262. doi:10.2147/CMAR.S184566
27. Rude RK. Renal cortical adenylate cyclase: characterization of magnesium activation. ENDOCRINOLOGY. 1983;113(4):1348–1355. doi:10.1210/endo-113-4-1348
28. Xia F, Jiang B, Chen Y, et al. Prediction of novel target genes and pathways involved in tall cell variant papillary thyroid carcinoma. MEDICINE. 2018;97(51):e13802. doi:10.1097/MD.0000000000013802
29. Xia F, Chen Y, Jiang B, et al. Long noncoding RNA HOXA-AS2 promotes papillary thyroid cancer progression by regulating miR-520c-3p/S100A4 pathway. Cell Physiol Biochem. 2018;50(5):1659–1672. doi:10.1159/000494786
30. Viljoen A, Batchelor B, Ghuran A. Woman with hypomagnesemia and hypocalcemia. Clin Chem. 2015;61(5):699–701. doi:10.1373/clinchem.2014.229005
31. Mutnuri S, Fernandez I, Kochar T. Suppression of parathyroid hormone in a patient with severe magnesium depletion. Case Rep Nephrol. 2016;2016:1–3. doi:10.1155/2016/2608538
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.