")
Back to Journals » OncoTargets and Therapy » Volume 13
Lower Serum Matrix Metalloproteinase‑9 in Metastatic Patients with Esophageal Squamous Cell Carcinoma After Concurrent Radiotherapy Was Significant for Prognosis
Authors Ye Z, Zhao H, Zhou W, Ye T, Geng C, Li X, Yuan L, Du M, Xu H, Wang Q
Received 15 September 2020
Accepted for publication 23 November 2020
Published 15 December 2020 Volume 2020:13 Pages 12857—12866
DOI https://doi.org/10.2147/OTT.S280791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Ziqi Ye,1,* Hongying Zhao,2,* Wuyuan Zhou,3 Tao Ye,4 Chong Geng,4 Xiaofeng Li,5 Lei Yuan,6 Mingyu Du,7 Heng Xu,8 Qiang Wang4
1The First Clinical Medical College, Graduate School, Nanjing Medical University, Nanjing, Jiangsu 210000, People’s Republic of China; 2Medical Oncology, Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221005, People’s Republic of China; 3Department of Hepatopancreatobillary Surgery, Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221005, People’s Republic of China; 4Department of Radiation Oncology, Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221005, People’s Republic of China; 5Department of Radiology, Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221005, People’s Republic of China; 6Department of Intervention, Xuzhou Cancer Hospital, Xuzhou, Jiangsu 221005, People’s Republic of China; 7Department of Radiation Oncology, Jiangsu Cancer Hospital and Jiangsu Institute of Cancer Research and Nanjing Medical University Affiliated Cancer Hospital, Nanjing, Jiangsu 210000, People’s Republic of China; 8Laboratory of Pharmaceutical Chemistry, Jiangsu Province Institute of Materia Medica, Nanjing Tech University, Nanjing, Jiangsu 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiang Wang
Department of Radiation Oncology, Xuzhou Cancer Hospital, No. 131, Huancheng Road, Xuzhou, Jiangsu 210005, People’s Republic of China
, Email [email protected]
Aim: This study was designed to investigate the relationships of serum matrix metalloproteinase 9 (MMP-9) level and treatment response in esophageal squamous cell carcinoma (ESCC) patients treated with chemotherapy or concurrent radiotherapy.
Methods: Blood samples from ESCC patients after chemotherapy or concurrent radiotherapy were collected at four different intervals. Serum MMP-9 was determined via Luminex assay in 134 patients with chemotherapy, 73 patients with concurrent radiotherapy, and 183 healthy controls.
Results: Serum MMP-9 level was significantly higher in patients with ESCC than in healthy controls (P < 0.001). Compared with the pre-treatment, a lower level of serum MMP-9 was maintained at four cycles of treatment in ESCC patients with concurrent radiotherapy (P < 0.001). Serum MMP-9 level was obviously lower in ESCC patients with metastasis after concurrent radiotherapy than after chemotherapy (P < 0.05). Patients with higher MMP-9 level (≥ 820.693 ng/mL) had a shorter mean survival time by 42 months versus lower MMP-9 level (< 820.693 ng/mL) after chemotherapy or concurrent radiotherapy (P < 0.001).
Conclusion: Serum MMP-9 is a potential prognostic biomarker for treatment response to chemotherapy or concurrent radiotherapy in terms of overall survival (OS) in ESCC patients.
Keywords: esophageal squamous cell carcinoma, MMP-9, chemotherapy, concurrent radiotherapy, prognosis
Introduction
Esophageal cancer (EC) is one of the common gastrointestinal cancers, which showed a drastic increase by more than sixfold in incidence rates worldwide.1,2 Now, EC ranks as the eighth most common malignant tumor and is associated with a poor prognosis.3 Although great progress has been made on the carcinogenesis and therapy for EC, the overall 5-year survival rate for persons with EC is 15% to 20% worldwide.4 New treatment strategies contributed to improvement of the 5-year survival rate in EC patients, such as neoadjuvant radiochemotherapy.5,6 Neoadjuvant radiochemotherapy plus surgery improves survival over surgery alone among patients with locally advanced esophageal squamous cell carcinoma (ESCC) in the Chinese randomized clinical trial.7 Neoadjuvant radiochemotherapy for esophageal adenocarcinoma has been widely used to treat patients with locally advanced and/or lymph node-positive tumors.7 However, squamous cell carcinoma is the predominant histology world over except the West.8 ESCC is a main pathological subtype of EC in China.9 High mortality of ESCC is closely related to its primary infiltration. Early invasion and metastasis are major reasons for poor prognosis in ESCC patients.10 Therefore, biomarkers that can be used to evaluate treatment response and prognosis should be evaluated for ESCC patients who could benefit from chemotherapy or concurrent radiotherapy.
Matrix metalloproteinase 9 (MMP‑9) is a member of the MMP family and plays an important role in tumor angiogenesis and VEGF bioavailability regulation.11 MMP‑9 accelerates tumor metastasis by promoting neovascularization and lymphangiogenesis, and has clinical significance in the diagnosis, treatment, and prognosis of various cancers, including EC.13,14 Indeed, many studies reported that MMP-9 participated in the tumorigenesis and resulted in poor prognosis in ESCC; however, most of the results are based on immunohistochemical staining of ESCC tissue specimens.15–18 Several studies have evaluated serum MMP-9 level in order to determine the diagnostic or prognostic value of ESCC.19–21 However, few studies focus on serum MMP-9 level, especially relationships to clinicopathological features and treatment response, in ESCC patients with metastasis after chemotherapy or concurrent radiotherapy.
In this study, the concentration of serum MMP-9 was determined in a large panel of patients with ESCC and healthy individuals. The relationships of serum MMP-9 level and treatment response were investigated in ESCC patients treated with chemotherapy or concurrent chemoradiotherapy, especially patients with metastasis. The prognosis value of serum MMP-9 was estimated in patients with ESCC after chemotherapy or concurrent chemoradiotherapy.
Patients and Methods
Patient Population
A total of 207 patients with histopathologically confirmed primary ESCC were enrolled from Jiangsu Cancer Hospital (Nanjing, China) between January 2012 and June 2016. The mean age of the patients was 60.66 years (SD, 7.97 years). The patients were staged according to the latest TNM staging issued in 2009 by the International Union Against Cancer. A total of 183 healthy individuals (without any abnormalities) from Nanjing between January 2013 and December 2013 were enrolled in the present study, with a mean age of 48.32 years (SD, 13.70 years). The patients were enrolled using a research protocol approved by the Biomedical Research Ethics Committee of Jiangsu Cancer Hospital. Each participant signed a written informed consent. This study was conducted according to the Declaration of Helsinki. The patients were included into either the pre-treatment or post-treatment groups. Initially, the patients were pathologically diagnosed with ESCC and had not received any prior treatment in the pre-treatment group. After R0 resection, 207 postoperative patients received chemotherapy or concurrent radiotherapy. In the chemotherapy group (Chemo group), patients received at least four times of chemotherapy with different chemotherapeutic drugs. Chemotherapy regimens include TP regimen, which was taxane (PTX, TAX, TXT or DOC) combined with platinum, PF regimen which was 5-fluorouracil and its derivatives (5-FU, FT207, or CAPE) combined with platinum and GP regimen which was gemcitabine (GEM) combined with platinum. The platinum used as chemotherapeutic drugs was one of DDP, LBP, CBP and NDP during chemotherapy. In the concurrent radiotherapy group (Chemo+Radio group), patients received concurrent radiotherapy at the first cycle of chemotherapy with different chemotherapeutic drugs. These patients received concurrent radiotherapy for 30–45 days during chemotherapy according to the patient’s status. The common radiotherapy schemes are as follows: such as GTV60-65Gy/28-33f, CTV50-55Gy/28-33f, PTV50-66Gy/28-33f. The interval of every chemotherapy therapy was about 1–2 months. GTV (Gross Tumor Volume) is a clinically visible or palpable tumor site and tumor extent that can be confirmed by diagnostic tests. CTV (Clinical Target Volume) includes microscopic subclinical neoplastic lesions besides GTV. PTV (Planning Target Volume) includes CTV itself, as well as expanded tissue coverage due to uncertainties.
Serum Samples
Pre-treatment blood samples from patients were collected. Blood samples after chemotherapy or concurrent radiotherapy were collected at four intervals (ie, first, second, third and fourth cycles of post-treatment). Before each course of therapy, samples were collected from patients for MMP-9 detection as treatment monitoring of last course. After centrifugation at 4 °C for 10 min, samples were stored at −80 °C until use.
Detection of Serum MMP-9 by Luminex Assay
The assay was performed using a Luminex multiplex technique. FLEXMAP 3D instruments and software were supplied by Luminex Corporation (Austin, TX, USA). Luminex kit for human cytokine/chemokine panels (ie, MMP-9) was purchased from Millipore (CAT no. HMMP2MAG-55K-01; Millipore, MA, USA) and performed according to the manufacturer’s instructions. The preparation processes of the samples and parameters in FLEXMAP 3D were similar to those reported in a previous work.22 The serum MMP-9 concentrations were calculated according to the standard curve.
Statistical Analysis
Serum MMP-9 concentrations were estimated using a regression. The concentrations were logarithmically transformed to achieve normal distribution. Serum MMP-9 concentrations were presented as mean ± SD. The differences between the two groups were examined using an unpaired t-test or Mann–Whitney test. The comparisons for ≥3 groups were performed by ANOVA, followed by pair-wise comparisons using Bonferroni post hoc testing. P < 0.05 was considered significance. Cox regression analysis was performed to assess potential prognostic factors. All statistical analyses were performed using the R language and environment for statistical computing (R version 3.5.2; R Foundation for Statistical Computing; www.r-project.org).
Results
Serum MMP-9 Level Increased in Patients with ESCC but Great Decreased After Chemotherapy or Concurrent Radiotherapy
Serum MMP-9 was measured in 183 healthy individuals and 207 patients with ESCC. As shown in Figure 1A, serum MMP-9 level was significantly lower in healthy controls than in ESCC patients, which was 326.0 ng/mL and 890.1 ng/mL in the controls and ESCC patients, respectively. Although serum MMP-9 level was higher in patients with concurrent radiotherapy than in patients with chemotherapy before treatment, the difference between the two groups was nonsignificant (P > 0.05). However, serum MMP-9 level was significantly lower in patients with concurrent radiotherapy after treatment compared to patients with chemotherapy (P < 0.05) (Figure 1B).
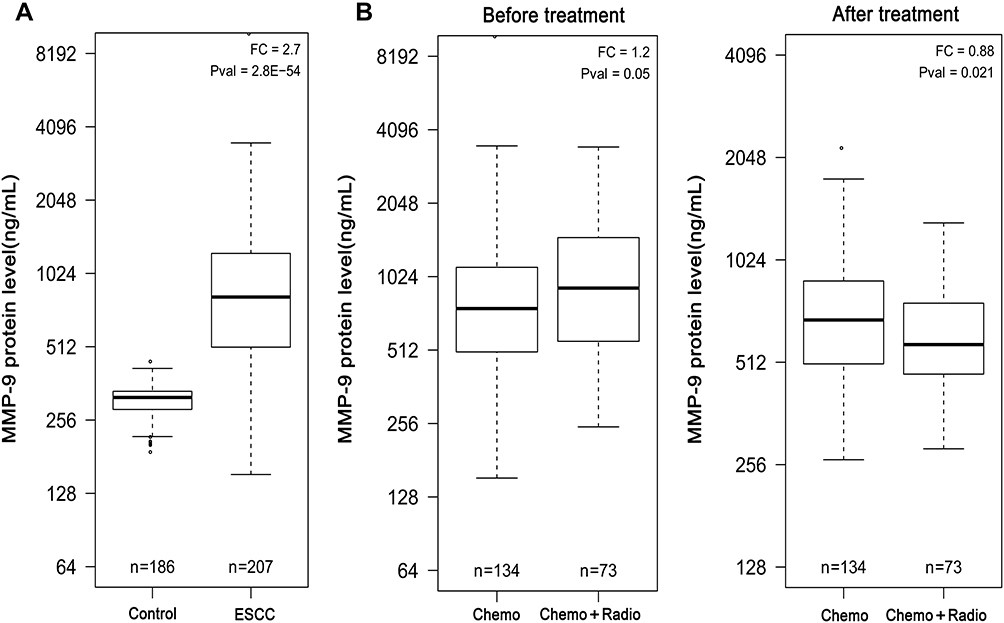 |
Figure 1 Boxplots of serum MMP-9 in healthy controls and patients before treatment and after treatment. (A) The median value of MMP-9 concentration in healthy controls and patients before treatment. (B) The median value of MMP-9 concentration between Chemo group and Chemo+Radio group in ESCC patients before treatment and after treatment, respectively. Chemo: patients received at least four times of chemotherapy. Chemo+Radio: patients received concurrent radiotherapy at the first cycle of chemotherapy. Abbreviation: FC, fold change. |
Correlation Between Serum MMP-9 and Clinicopathological Characteristics
The relation between serum MMP-9 and various clinicopathological characteristics was shown in Table 1. The differences in serum MMP-9 concentration by gender and age were nonsignificant in patients with ESCC (P > 0.05). For serum MMP-9 level in ESCC patients, the differences in stage and differentiation were also nonsignificant (P > 0.05). Serum MMP-9 level was higher in ESCC patients with metastasis than in ESCC patients with non-metastasis. However, the difference was still not significant (P > 0.05).
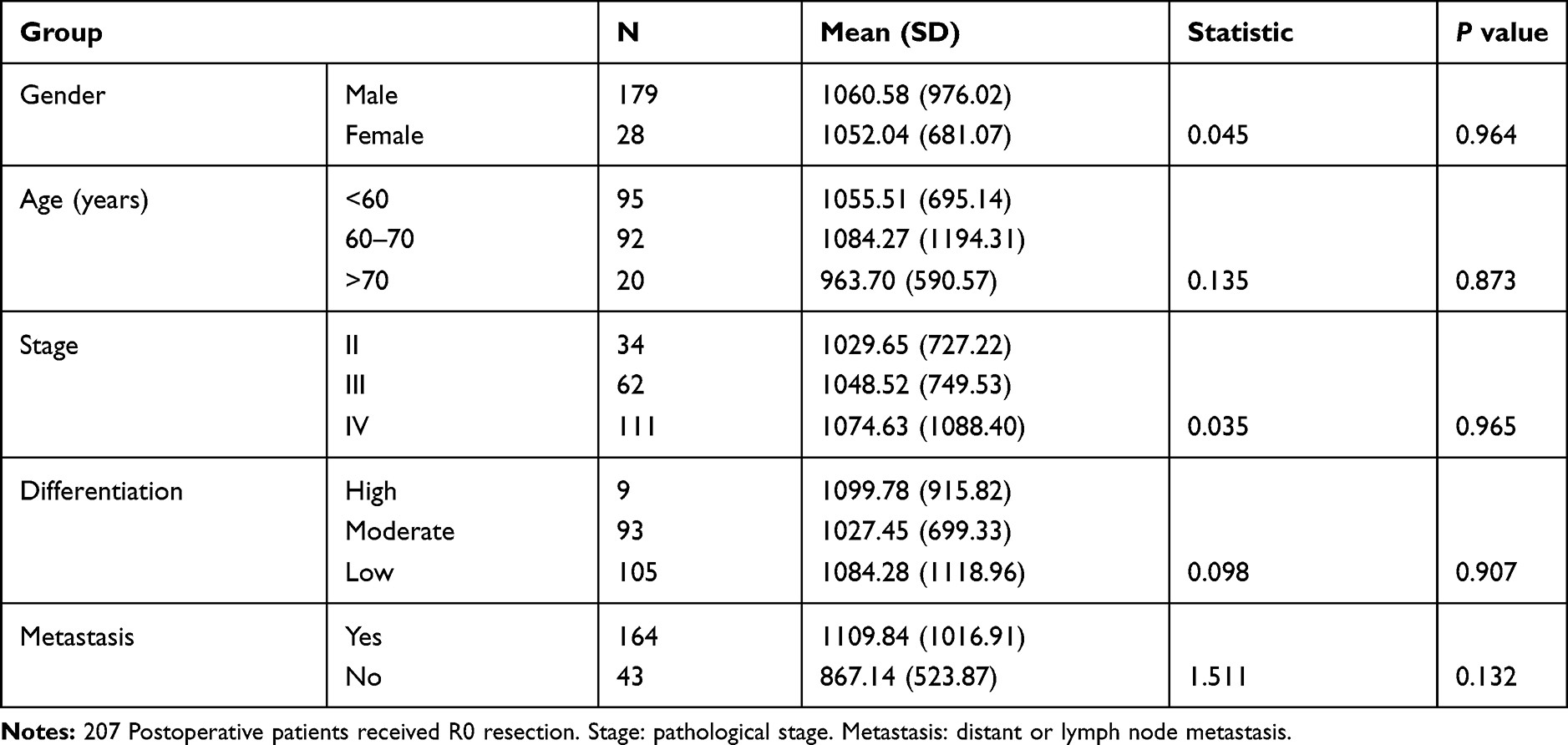 |
Table 1 Relation of Serum MMP9 to Clinicopathological Characteristics of 207 Postoperative Patients with ESCC (Concentration Unit: Ng/mL) |
The Decrease Was Significant in ESCC Patients with Metastasis After Concurrent Radiotherapy
There was no significant difference in serum MMP-9 level between ESCC patients with metastasis and ESCC patients with non-metastasis before treatment (P > 0.05). Serum MMP-9 level in ESCC patients with metastasis was equal to that in ESCC patients with non-metastasis after treatment including chemotherapy or concurrent radiotherapy (P > 0.05) (Figure 2A). However, for ESCC patients with metastasis after treatment, serum MMP-9 level was obviously lower in the Chemo+Radio group than in the Chemo group (P < 0.05). Interestingly, for ESCC patients with non-metastasis after treatment, serum MMP-9 level was not lower in the Chemo+Radio group than in the Chemo group (P > 0.05) (Figure 2B).
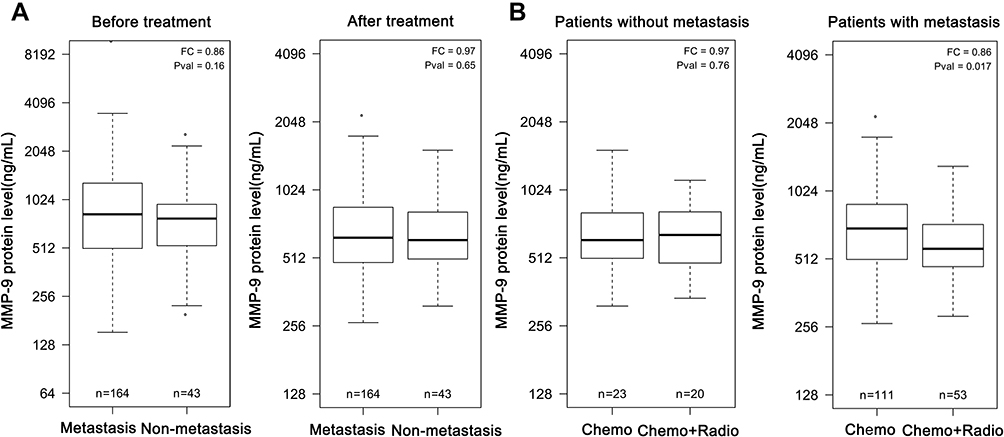 |
Figure 2 Boxplots of serum MMP-9 in ESCC patients with metastasis and non-metastasis. (A) The median value of MMP-9 concentration between metastatic and non-metastatic patients before treatment and after treatment, respectively. (B) The median value of MMP-9 concentration between Chemo group and Chemo+Radio group in ESCC patients with non-metastasis and metastasis respectively after treatment. Chemo: patients received at least four times of chemotherapy. Chemo+Radio: patients received concurrent radiotherapy at the first cycle of chemotherapy. Abbreviation: FC, fold change. |
Serum MMP-9 Significantly Decreased in Patients After Four Cycles Treatment with Concurrent Radiotherapy
A total of 134 patients with ESCC were treated with chemotherapy at four different intervals (ie, first, second, third, fourth time chemotherapy), and 73 patients were treated with once concurrent radiotherapy at the first cycle of chemotherapy. Compared with the chemo group, the chemo+radio group showed a greater mean decrease in serum MMP-9 level at the first, second, third and fourth cycles of treatments (Figure 3A). Compared with the pre-treatment, serum MMP-9 level did not significantly decrease at the first cycle of treatment in ESCC patients treated with chemotherapy alone (P > 0.05). Only at the third and fourth cycles of treatment, the serum MMP-9 level great decreased in ESCC patients treated with chemotherapy alone (P < 0.001) (Figure 4A). However, serum MMP-9 level began to significantly decrease at the first time of treatment in ESCC patients with concurrent radiotherapy (P < 0.001). Compared with the pre-treatment, serum MMP-9 level was always significantly lower at four cycles of treatment in ESCC patients with concurrent radiotherapy (P < 0.001) (Figure 4A).
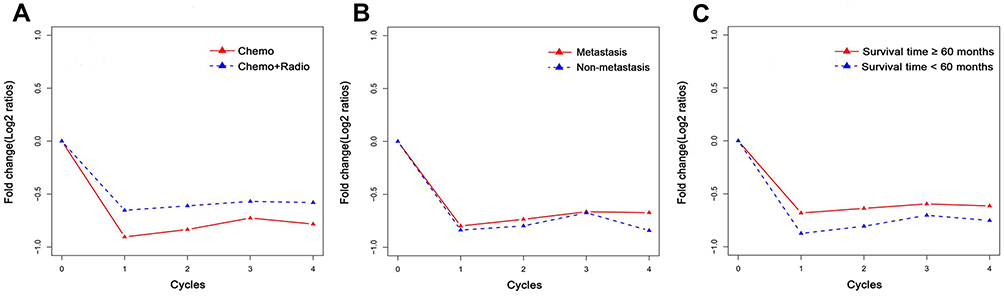 |
Figure 3 Mean change in (A) treatment modality, (B) metastasis or (C) survival time relative to the pre-treatment value. The fold change (FC) between post-treatment values and pre-treatment values are calculated and the mean fold decrease was plotted at four different time intervals (the first, second, third and fourth cycles of treatment). Chemo: patients received at least four times of chemotherapy. Chemo+Radio: patients received concurrent radiotherapy at the first cycle of chemotherapy. Metastasis: ESCC patients with metastasis. Nonmetatasis: ESCC patients with non-metastasis. |
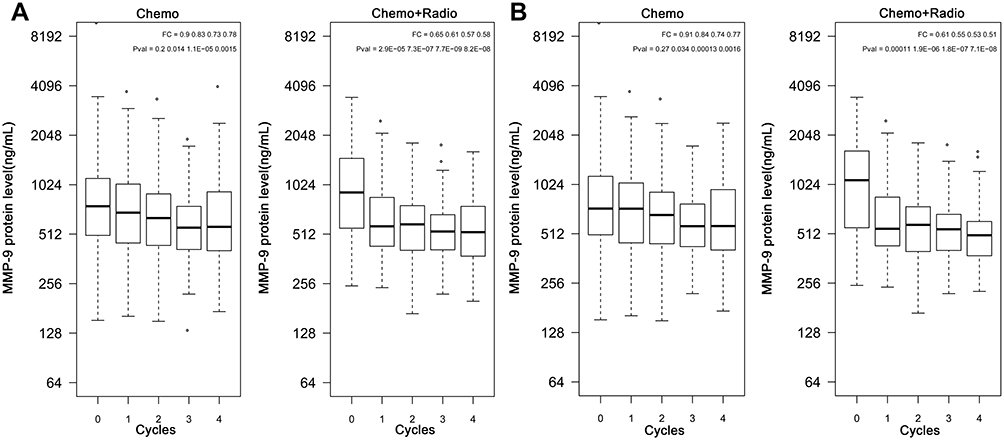 |
Figure 4 Boxplots of serum MMP-9 from pre-therapy (0 cycle) and the first, second, third and fourth cycles of post therapy (1, 2, 3, 4 cycles) in (A) 207 ESCC patients and (B) 164 ESCC patients with metastasis. Chemo: patients received at least four times of chemotherapy. Chemo+Radio: patients received concurrent radiotherapy at the first cycle of chemotherapy. |
The degree of decline in serum MMP-9 level in patients with metastasis after chemotherapy or concurrent radiotherapy was slighter than that in the non-metastatic patients at the first, second, third cycles of treatment (Figure 3B). However, patients with metastasis showed serious degree of decline in serum MMP-9 level at the fourth cycle of treatment compared to patients with non-metastasis (Figure 3B). A total of 111 patients with metastasis were treated with chemotherapy at four different intervals, and 53 patients were treated with once concurrent radiotherapy at the first cycle of chemotherapy. As shown in Figure 4B, serum MMP-9 level greatly decreased at the third and fourth cycles in metastatic patients with chemotherapy compared to the pre-treatment (P < 0.001). However, the decrease in serum MMP-9 level was extremely remarkable in patients with metastasis after concurrent radiotherapy (P < 0.001) (Figure 4B).
Prognosis Value of Serum MMP-9 in ESCC Patients
As of April 25, 2020, the overall survival (OS) of patients has been calculated. During the follow-up periods, 109 (52.7%) patients had died, and 29 (14.0%) patients were missing. As shown in Table 2, most patients with ESCC had survived more than 60 months in the survival group, while many patients with ESCC had survived less than 24 months in the death group. In the chemo group, the number of patients with OS more than 60 months accounted for 29.1%. However, the proportion of patients with OS more than 60 months was as high as 45.2% in the chemo+radio group. Furthermore, the 3-year and 5-year survival rates were 55.1% and 44.4% in ESCC patients, respectively. Interestingly, the mean increase in MMP-9 levels in 72 patients with survival time ≥60 months is larger compared to 106 patients with survival time <60 months at the first, second, third cycles of treatment including chemotherapy or concurrent radiotherapy (Figure 3C). Moreover, age, gender, stage, differentiation, metastasis and serum MMP-9 level at pre-treatment were evaluated for survival using univariate analysis. According to each tangent point, serum MMP-9 levels at pre-treatment were divided into high- and low-risk values, and then 99 times of multiple regression analysis are performed, and the best tangent point with minimal p-value is the cutoff value. Serum MMP-9 ≥926.49 ng/mL was determined as an independent factor for OS in ESCC patients before treatment among the variables evaluated. The median survival times were no difference in ESCC patients with MMP-9 <926.49 ng/mL and MMP-9 ≥926.49 ng/mL before treatment, respectively (P = 0.053) (Figure 5A). Moreover, there was no effect of treatment modality on survival time in ESCC patients treated with chemotherapy or concurrent radiotherapy (P > 0.05) (Figure 5B). Furthermore, age, gender, stage, differentiation, metastasis, treatment modality and serum MMP-9 level at four intervals (ie, first, second, third and fourth cycles of post-treatment) were evaluated for survival using univariate analyses adjusted for potential confounding factors. According to each tangent point, the respective mean of serum MMP-9 at post-treatment in 134 patients with chemotherapy and 73 patients with concurrent radiotherapy were divided into high- and low-risk values, and then 99 times of multiple regression analysis are performed, and the best tangent point with minimal p-value is the cutoff value. However, the median survival times were 57 and 15 months in ESCC patients with MMP-9 <820.693 ng/mL and MMP-9 ≥820.693 ng/mL after treatment including chemotherapy or concurrent radiotherapy, respectively (P < 0.0001) (Figure 5C). High MMP-9 levels (≥820.693 ng/mL) were associated with poor prognosis in ESCC patients after treatment. Patients with higher MMP-9 level (≥820.693 ng/mL) had a shorter mean survival time by 42 months compared to patients with lower MMP-9 level (<820.693 ng/mL) after chemotherapy or concurrent radiotherapy.
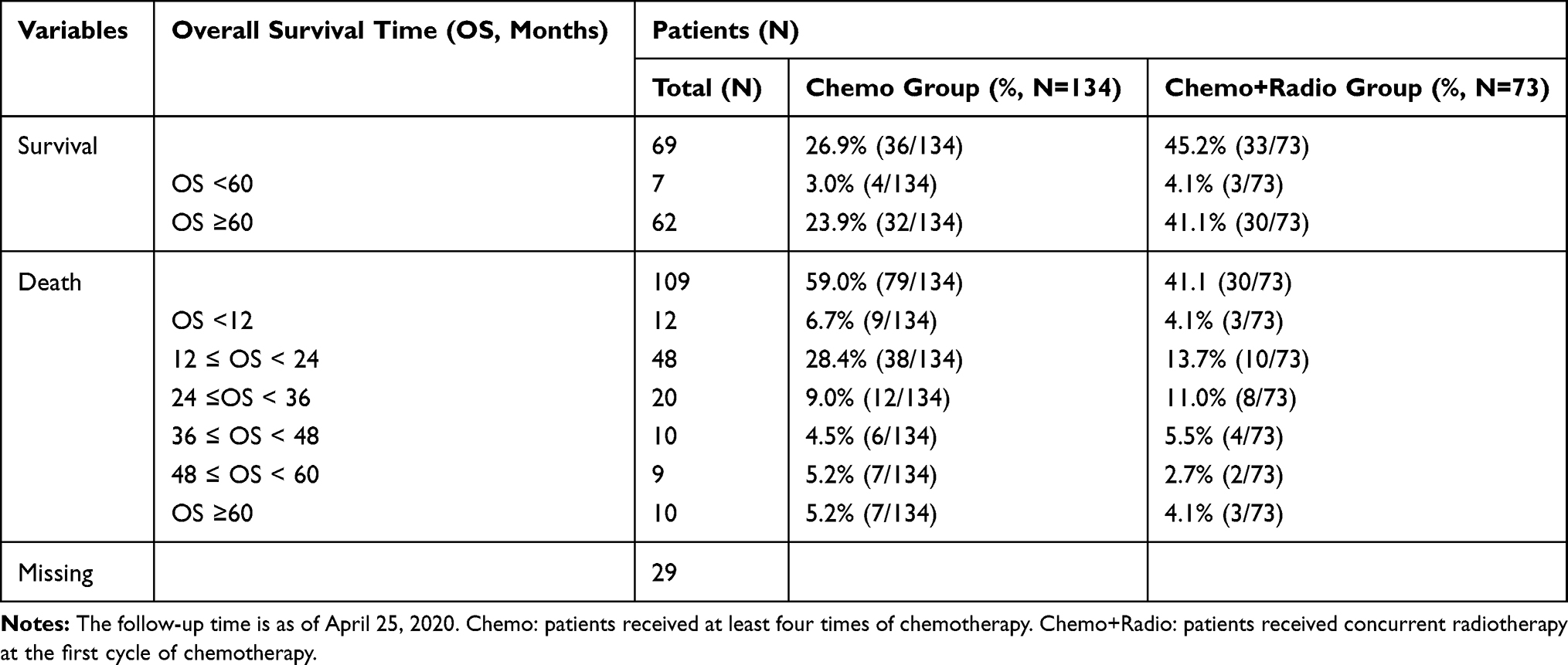 |
Table 2 The Overall Survival Time of 207 Patients with ESCC After Chemotherapy or Concurrent Radiotherapy |
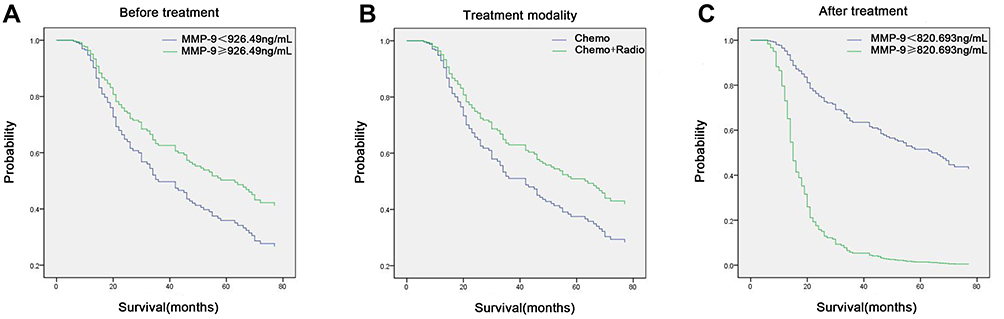 |
Figure 5 The prognosis values of serum MMP-9 in patients with ESCC. (A) Overall survival with high (≥ 926.49 ng/mL) and low (< 926.49 ng/mL) MMP-9 levels in patients before treatment. Hazard ratio =1.490 (95% CI, 0.995–2.231), P=0.053. (B) Overall survival with Chemo group and Chemo+Radio group. Hazard ratio =1.453 (95% CI, 0.947–2.227), P=0.087. (C) Overall survival with high (≥ 820.693 ng/mL) and low (< 820.693 ng/mL) MMP-9 levels in patients after chemotherapy or concurrent radiotherapy. Hazard ratio =0.155 (95% CI, 0.095–2.254), P < 0.001. Chemo: patients received at least four times of chemotherapy. Chemo+Radio: patients received concurrent radiotherapy at the first cycle of chemotherapy. Abbreviation: CI, confidence interval. |
Discussion
ESCC is an invasive cancer with relatively late stage of diagnosis, rapid clinical progression, and very poor survival.23,24 Esophagectomy is the most commonly accepted standard for treatment of localized disease; however, the results are frustrating due to high recurrence rate.25 Preoperative radiotherapy did not show benefit with addition of radiotherapy to surgery.25 The patients with localized disease who are poor candidates for surgery treated with chemoradiotherapy, which is superior to radiotherapy alone. Compared to 0% with radiotherapy alone, the 5-year survival was 26% in ESCC patients with chemoradiotherapy.26 Preoperative chemoradiotherapy has been studied to improve the cure rate. Unfortunately, the data are not impressive. In this study, 207 postoperative patients (R0 resection) with ESSC received chemotherapy including PF, TP and GP therapeutic regimens, and 72 of them received once concurrent radiotherapy at the first cycle of chemotherapy. Serum MMP-9 level was significantly higher in ESSC patients than in the controls, then obviously decreased after treatment including chemotherapy or concurrent radiotherapy. Moreover, patients treated with concurrent radiotherapy have a greater degree of decrease compare to patients with chemotherapy alone, suggesting that serum MMP-9 is a potential biomarker for evaluating therapeutic effect in ESSC patients treated with chemotherapy or concurrent radiotherapy.
Matrix metalloproteinase-9 degrades extracellular matrix, which leads to the proteolysis of microvascular basement membrane and invasion of endothelial cells, suggesting MMP-9 contributes to tumor development and metastasis in ESCC.27–29 Knockdown of MMP‑9 attenuated epithelial‑mesenchymal transition (EMT) induced by TGF‑β1 and inhibited invasiveness and migration in ESCC.30 The expression of MMP‑9 was positively associated with Vimentin and SNAI1, suggesting that the MMP-9 is involved in the regulation of ESCC migration.31 Nearly half of EC patients are accompanied by metastasis in the west.25 The failure of ESCC treatment may be caused by extensive local invasion and regional lymph node metastasis, which makes it difficult to completely resect the tumor.32 Therefore, it is particularly important for postoperative patients with metastasis to predict therapeutic effect according to serum MMP-9 after treatment including chemotherapy or concurrent radiotherapy. According to Wang et al, based on the optimal MMP cut-off values by ROC curve, elevated MMP-3 and MMP-9, but not MMP-7, correlated with distant metastasis and poor survival in patients with squamous cell carcinoma (P < 0.05).21 The expression of MMP-9 detected by IHC in ESCC patients was positively correlated with poorer differentiation (P < 0.01), and lymph node metastasis (P<0.05).17 In this study, there are 79.2% ESSC patients (164/207) with metastasis including distant metastasis or lymph node metastasis (Table 1), suggesting more attention should be paid to the treatment of ESCC patients with metastasis. The treatment modality in the study is chemotherapy or concurrent radiotherapy. There were no significant differences in serum MMP-9 level between metastatic patients and non-metastatic patients at the pre-treatment and post-treatment, respectively (P > 0.05) (Figure 2A). Although there was no effect of treatment modality on serum MMP-9 level in ESCC patients with non-metastasis, patients with metastasis had lower MMP-9 level after concurrent radiotherapy compared to chemotherapy alone (P < 0.05) (Figure 2B). Moreover, 53 patients with metastasis who received concurrent radiotherapy maintained lower MMP-9 levels during the treatment cycles (P < 0.001) (Figure 4B). Serum MMP-9 level significantly decreased at the first cycle of treatment after concurrent radiotherapy compared to the pre-treatment, suggesting concurrent radiotherapy is beneficial to the reduction of MMP-9 in ESCC patients with metastasis.
Some studies discussed the correlation between MMP-9 and ESCC,13 however, a firm conclusion has not been formed due to various reasons, such as a relatively small cohort. Furthermore, these results had different cut-off values for MMP-9 based on different treatment modalities, which make inconsistent conclusions.14,15,33 More importantly, MMP-9 was associated with prognosis in ESCC patients; however, these findings are controversial. MMP-9 was useful as a potential biomarker in diagnosis, but not in prognosis of EC through measuring serum MMP-9 of 89 patients by ELISA assay.20 However, Tanioka et al indicated the expression of MMP-9 in the invasive front was an independent prognostic indicator through multivariate analysis of MMP-9 expression in 55 patients by IHC staining.15 In the present study, serum MMP-9 level was analyzed by a relatively large group of ESCC patients, and 178 patients were successfully followed up and obtained valid data, suggesting clinical interest may be reliable for ESCC. The patients with lower MMP-9 level (<926.49 ng/mL) had not shorter OS compared with those with higher MMP-9 levels at the pre-treatment (P > 0.05). Meanwhile, there was no difference in survival time between the two treatment modalities (P > 0.05) (Figure 5). Therefore, the survival of patients after treatment with chemotherapy or concurrent radiotherapy was analyzed as a whole. Higher MMP-9 level (≥820.693 ng/mL) after chemotherapy or concurrent radiotherapy indicated shorter OS, which suggested serum MMP-9 level after treatment was positively associated with survival time in ESCC patients with chemotherapy or concurrent radiotherapy. The possible reason was that although serum MMP-9 level was high in ESCC patients at pre-treatment, serum MMP-9 dropped sharply and remained at a low level in most patients after chemotherapy or concurrent radiotherapy. It should also be pointed out that in multivariate analysis, the choice of treatment modality including chemotherapy and concurrent radiotherapy did not affect the survival time in ESCC patients (P > 0.05). In addition, 72 patients with ESCC (34.8%) had survival time >60 months, suggesting ESCC patients benefit from chemotherapy and concurrent radiotherapy.
The limitations of this study are as follows. First, although treatment response is clearly related to serum MMP-9 level, the clinical significance of these findings requires further investigation. Since serum MMP-9 level significantly decreased in ESCC patients who had longer OS, we deduce that the reduction of serum MMP-9 after treatment may be correlated with patient outcome. Second, in the study, the patients after operation were collected as the research objects. Serum MMP-9 level may be affected by surgical treatment. Finally, unlike previous studies using ELISA or IHC as a testing method, the examination by Luminex multiplex assay was performed in the study. The combination of different biomarkers and detection methods should be able to monitor the therapeutic outcome for different subsets of patients.
Conclusion
Serum MMP-9 level was significantly higher in patients with ESCC than in health controls (P < 0.05). However, serum MMP-9 level gradually decreased at the first, second, third and fourth cycles of treatment in ESCC patients after concurrent radiotherapy (P < 0.001). The mean decrease in serum MMP-9 level was larger at the fourth cycle of treatment in metastatic patients after chemotherapy or concurrent radiotherapy compared to non-metastatic patients. Compared to patients with MMP-9≥820.693 ng/mL, the median survival time was longer in ESCC patients with MMP-9 <820.693 ng/mL after chemotherapy or concurrent radiotherapy, which indicated poor prognosis in ESCC patients. Serum MMP-9 is a potential prognostic biomarker for treatment response to chemotherapy or concurrent radiotherapy in terms of OS in ESCC patients. Further investigation is needed to verify the prognostic significance of serum MMP-9 using different subsets of patients.
Acknowledgments
The present study was supported by projects of Xuzhou Science and Technology Bureau (KC9186).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pakzad R, Mohammadian-Hafshejani A, Khosravi B. The incidence and mortality of esophageal cancer and their relationship to development in Asia. Ann Transl Med. 2016;4(2):29.
2. Simard EP, Ward EM, Siegel R, Jemal A. Cancers with increasing incidence trends in the United States: 1999 through 2008. CA Cancer J Clin. 2012;62(2):118–128. doi:10.3322/caac.20141
3. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
4. Pennathur A, Gibson MK, Jobe BA, Luketich JD. Oesophageal carcinoma. Lancet. 2013;381(9864):400–412. doi:10.1016/S0140-6736(12)60643-6
5. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–2084. doi:10.1056/NEJMoa1112088
6. Shapiro J, van Lanschot JJ, Hulshof MC, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. doi:10.1016/S1470-2045(15)00040-6
7. Yang H, Liu H, Chen Y, et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): a Phase III multicenter, randomized, open-label clinical trial. J Clin Oncol. 2018;36(27):2796–2803. doi:10.1200/JCO.2018.79.1483
8. McNamara MJ, Rybicki LA, Sohal D, et al. The relationship between pathologic nodal disease and residual tumor viability after induction chemotherapy in patients with locally advanced esophageal adenocarcinoma receiving a tri-modality regimen. J Gastrointest Oncol. 2016;7(2):196–205.
9. Jemal A, Thomas A, Murray T, Thun M. Cancer statistics, 2002. CA Cancer J Clin. 2002;52(1):23–47. doi:10.3322/canjclin.52.1.23
10. Zheng S, Vuitton L, Sheyhidin I, Vuitton DA, Zhang Y, Lu X. Northwestern China: a place to learn more on oesophageal cancer. Part one: behavioural and environmental risk factors. Eur J Gastroenterol Hepatol. 2010;22(8):917–925. doi:10.1097/MEG.0b013e3283313d8b
11. Cools-Lartigue J, Spicer J, Ferri LE. Current status of management of malignant disease: current management of esophageal cancer. J Gastrointest Surg. 2015;19(5):964–972. doi:10.1007/s11605-014-2701-3
12. Kessenbrock K, Plaks V, Werb Z. Matrix metalloproteinases: regulators of the tumor microenvironment. Cell. 2010;141(1):52–67. doi:10.1016/j.cell.2010.03.015
13. Zeng R, Duan L, Kong Y, et al. Clinicopathological and prognostic role of MMP-9 in esophageal squamous cell carcinoma: a meta-analysis. Chin J Cancer Res. 2013;25(6):637–645.
14. Gu ZD, Li JY, Li M, et al. Matrix metalloproteinases expression correlates with survival in patients with esophageal squamous cell carcinoma. Am J Gastroenterol. 2005;100(8):1835–1843. doi:10.1111/j.1572-0241.2005.50018.x
15. Tanioka Y, Yoshida T, Yagawa T, et al. Matrix metalloproteinase-7 and matrix metalloproteinase-9 are associated with unfavourable prognosis in superficial oesophageal cancer. Br J Cancer. 2003;89(11):2116–2121. doi:10.1038/sj.bjc.6601372
16. Li Y, Guo H, Dong D, Wu H, Li E. Expression and prognostic relevance of cyclophilin A and matrix metalloproteinase 9 in esophageal squamous cell carcinoma. Diagn Pathol. 2013;8(1):207. doi:10.1186/1746-1596-8-207
17. Gu ZD, Chen KN, Li M, Gu J, Li JY. Clinical significance of matrix metalloproteinase-9 expression in esophageal squamous cell carcinoma. World J Gastroenterol. 2005;11(6):871–874. doi:10.3748/wjg.v11.i6.871
18. Shima I, Sasaguri Y, Arima N. Expression of epidermal growth factor (EGF), matrix metalloproteinase-9 (MMP-9) and proliferating cell nuclear antigen (PCNA) in esophageal cancer. Int J Oncol. 1995;6(4):833–839.
19. Łukaszewicz-Zajac M, Mroczko B, Kozłowski M, Nikliński J, Laudański J, Szmitkowski M. Elevated levels of serum metalloproteinase 9 in patients with esophageal squamous cell carcinoma. Pol Arch Med Wewn. 2009;119(9):558–563.
20. Mroczko B, Kozłowski M, Groblewska M, et al. The diagnostic value of the measurement of matrix metalloproteinase 9 (MMP-9), squamous cell cancer antigen (SCC) and carcinoembryonic antigen (CEA) in the sera of esophageal cancer patients. Clin Chim Acta. 2008;389(1–2):61–66. doi:10.1016/j.cca.2007.11.023
21. Wang WL, Chang WL, Yeh YC, et al. Concomitantly elevated serum matrix metalloproteinases 3 and 9 can predict survival of synchronous squamous cell carcinoma of the upper aero-digestive tract. Mol Carcinog. 2013;52(6):438–445. doi:10.1002/mc.21874
22. Ma R, Xu H, Wu J, et al. Identification of serum proteins and multivariate models for diagnosis and therapeutic monitoring of lung cancer. Oncotarget. 2017;8(12):18901–18913. doi:10.18632/oncotarget.14782
23. Vallböhmer D, Lenz H-J. Predictive and prognostic molecular markers in outcome of esophageal cancer. Dis Esophagus. 2006;19(6):425–432. doi:10.1111/j.1442-2050.2006.00622.x
24. Samantaray S, Sharma R, Chattopadhyaya TK, Gupta SD, Ralhan R. Increased expression of MMP-2 and MMP-9 in esophageal squamous cell carcinoma. J Cancer Res Clin Oncol. 2004;130(1):37–44. doi:10.1007/s00432-003-0500-4
25. Alidina A, Siddiqui T, Burney I, Jafri W, Hussain F, Ahmed M. Esophageal cancer –a review. J Pak Med Assoc. 2004;54(3):136–141.
26. Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer. Long-term follow-up of a prospective randomized trial (RTOG 85-01). JAMA. 1999;281(17):1623–1627. doi:10.1001/jama.281.17.1623
27. Zeng ZS, Cohen AM, Guillem JG. Loss of basement membrane type IV collagen is associated with increased expression of metalloproteinases 2 and 9 (MMP-2 and MMP-9) during human colorectal tumorigenesis. Carcinogenesis. 1999;20(5):749–755. doi:10.1093/carcin/20.5.749
28. Ii M, Yamamoto H, Adachi Y, Maruyama Y, Shinomura Y. Role of matrix metalloproteinase-7 (matrilysin) in human cancer invasion, apoptosis, growth, and angiogenesis. Exp Biol Med (Maywood). 2006;231(1):20–27. doi:10.1177/153537020623100103
29. Yamamoto H, Vinitketkumnuen A, Adachi Y, et al. Association of matrilysin-2 (MMP-26) expression with tumor progression and activation of MMP-9 in esophageal squamous cell carcinoma. Carcinogenesis. 2004;25(12):2353–2360. doi:10.1093/carcin/bgh270
30. Bai X, Li YY, Zhang HY, et al. Role of matrix metalloproteinase‑9 in transforming growth factor‑β1‑induced epithelial‑mesenchymal transition in esophageal squamous cell carcinoma. Oncotargets Ther. 2017;10:
31. Xu G, Ou L, Liu Y, et al. Upregulated expression of MMP family genes is associated with poor survival in patients with esophageal squamous cell carcinoma via regulation of proliferation and epithelial‑mesenchymal transition. Oncol Rep. 2020;44(1):29–42. doi:10.3892/or.2020.7606
32. Wang LS, Chow KC, Chi KH, et al. Prognosis of esophageal squamous cell carcinoma: analysis of clinicopathological and biological factors. Am J Gastroenterol. 1999;94(7):1933–1940. doi:10.1111/j.1572-0241.1999.01233.x
33. Lu CL, Ji Y, Ge D, Guo J, Ding JY. The expression of CXCR4 and its relationship with matrix metalloproteinase-9/vascular endothelial growth factor in esophageal squamous cell cancer. Dis Esophagus. 2011;24(4):283–290.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.