")
Back to Journals » Infection and Drug Resistance » Volume 12
Lower Rates Of Naturally Occurring Resistance-Associated Substitutions (RASs) In Hepatitis C Virus (HCV)-Infected Chronic Kidney Disease (CKD) Patients Than In HCV-Infected Patients With Only Liver Disease
Authors Gupta E , Choudhary MC , Upadhyay N, Singh G, Nayak SL, Kumar M, Sarin SK
Received 25 June 2019
Accepted for publication 31 October 2019
Published 22 November 2019 Volume 2019:12 Pages 3635—3640
DOI https://doi.org/10.2147/IDR.S220335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Ekta Gupta,1 Manish Chandra Choudhary,2 Nimisha Upadhyay,1 Gaurav Singh,1 Suman Lata Nayak,3 Manoj Kumar,4 Shiv Kumar Sarin4
1Department of Clinical Virology, ILBS, New Delhi, India; 2Department of Molecular and Cellular Medicine, ILBS, New Delhi, India; 3Department of Nephrology, ILBS, New Delhi, India; 4Department of Hepatology, ILBS, New Delhi, India
Correspondence: Ekta Gupta
Department of Clinical Virology, Institute of Liver & Biliary Sciences, New Delhi 110070, India
Email [email protected]
Purpose: Baseline viral load and existence of resistance-associated substitutions (RASs) are associated with direct-acting antiviral agent (DAA) treatment failure in patients with chronic hepatitis C virus (HCV) infection.
Patients and methods: This study was done on HCV-infected patients with different clinical conditions, group 1 included HCV-infected patients with only liver disease (n= 24) and group 2 had HCV-infected patients with coexisting chronic kidney disease (CKD) (n =26). Baseline RAS in the viral genome, before treatment initiation, was examined in both the groups to understand the host disease status on their occurrence.
Results: Predominant genotype (gt) differed in both the groups, in group 1 it was gt3 while it was gt1 in group 2. Overall, the occurrence of RASs at baseline was seen in 10 patients (20%); in group 1 it was seen in 8 (33.3%) as compared to only 2 (7.6%) in group 2; p < 0.001. RAS in both NS5a and NS5b regions of the virus was seen in group 1 while in group 2, RASs were seen only in the NS5a region of the virus at 30K position. In group 1, multiple RASs were also seen. The existence of RAS at baseline in both the groups did not affect the attainment of post-treatment cure for the virus in terms of sustained virological response (SVR).
Conclusion: Host disease status influences the occurrence of baseline RAS in the virus.
Keywords: Hepatitis C Virus infection, drug resistance, direct-acting antivirals
Introduction
Hepatitis C virus (HCV) is a global health problem and affects 185 million people worldwide.1 HCV therapy has been revolutionized with the recent introduction of direct-acting antiviral agents (DAAs), and with this, the elimination of HCV is now a reality.2 DAAs are targeted against three distinct nonstructural HCV proteins (NS3–4A protease, NS5A, and NS5B polymerase) which are now been routinely used for clinical cure and have shown an excellent cure rate in terms of achieving a sustained virological response rate (SVR) of more than 90%.3 DAAs are molecules that target specific nonstructural proteins of the HCV viral genome, thereby interfering with viral replication and infection. There are different classes of DAAs like NS3/4A protease inhibitors, NS5A inhibitors and NS5B polymerase inhibitors, which are defined by their site of action on the viral genome. The recommended treatment involves the use of pan-genotypic drugs targeting two regions of the virus NS5a and NS5b.4 This treatment usually responds very well in the clearance of the virus; however treatment failures, if any, are associated with host factors like advanced stages of liver fibrosis, host immune responses, and viral factors such as baseline viral load and existence of resistance-associated substitutions (RASs) in the viral genome. These RASs can be naturally occurring (wild-type virus) or could develop during the course of the treatment known as post-treatment RAS.4 Baseline resistance testing, before the initiation of treatment, is not recommended routinely except in few limited conditions.5 HCV is an approximately 9.5kb RNA virus that replicates rapidly with an error rate of 1 to 3 errors per replication cycle. These changes often lead to the development of a variant virus. In a subset of patients with chronic HCV infection, baseline RASs, particularly in the region of NS5A, are known to negatively impact treatment response.6 Hence, the role of these naturally occurring substitutions should be studied for treatment decisional support.
The prevalence of HCV infection in patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD) is much more than that seen in the general population.7,8 Treating HCV infection and clearing the virus in this population will not only improve their quality of life but also decrease the further risk of nosocomial spread of the virus. Host immune dysregulations are more in CKD patients compared with the general population.9,10 Therefore, we presume that the naturally occurring RASs might be different in CKD patients with HCV infection as compared to HCV patients without CKD infection. Moreover, the prevalence of RASs in HCV-infected CKD has never been studied; hence, the present study is done to study naturally occurring RAS in HCV-infected CKD patients and compare their occurrence with HCV-infected patients with only liver disease.
Methods
Study Population
This was a retrospective study with the involvement of 50 adult patients with confirmed HCV infection (HCV RNA > 3 Log10 IU/mL) whose blood samples were received in the Department of Clinical Virology for HCV RNA testing. They were divided into two separate groups, Group 1 consisted of 24 patients infected with HCV with normal renal function (serum creatinine ≤1 g/dL), manifesting only liver disease and Group 2 included 26 HCV-infected patients with established chronic kidney disease (eGFR <60 mL/min). Baseline blood samples of these patients, which were available in repository of the department, were retrieved keeping the patient’s information unlinked and anonymized. Baseline RAS was done in all the samples and the clinical records of follow-up of each patient were obtained from the Hospital Information system (HIS) for data analysis.
At the time of this study, none of the enrolled patients had been treated with DAAs before. However, 33.3% (8/24) of Group 1 and 19.2% (5/26) of Group 2 had previously been treated with pegylated Interferon-alpha (PEG-IFNα) and ribavirin (RBV). As per the Institutes’ policy, patients received 400 mg sofosbuvir (acting at the NS5b region of the virus) in combination with daclatasvir (acting at the NS5a region of the virus) for 12 weeks in noncomplicated cases, while in complicated cases, an addition of weight-based ribavirin (1000 or 1200 mg) daily for 24 weeks was given. All the patients were followed up till the completion of the treatment and SVR 12 was measured in all of them.
Ethical Approval
The study was approved by the Institutional Review Board of the Institute of Liver and Biliary Sciences, New Delhi, India, IEC No. IEC/2017/49/NA06. For HCV CKD, the samples were received under the ClinicalTrials.gov identifier number: NCT02563665.Since the study was done on the archived samples, the waiver was taken from the Ethics committee to take consent from the patients. All the participants whose samples were used for the study were de-identified (anonymized and unlinked) as per the existing national guidelines which are in compliance with the Declaration of Helsinki.11
Laboratory Methods
Clinical details and information about routine laboratory investigations were obtained from the HIS. Archived plasma samples were retrieved from −80°C of the Virology laboratory, and the following laboratory investigations were done.
HCV RNA Assay
HCV RNA was quantified in plasma samples by Abbott Real Time HCV quantitative assay (Abbott, Wiesbaden, Germany) on Automated m2000sp/m2000rt platform, as per the manufacturer’s instructions. The lower limit of detection (LOD) and lower limit of quantification (LLOQ) of this assay is similar, ie, 12 IU/mL, and linear range of the assay is from 12 to 108IU/mL.
Routine HCV Genotyping
HCV genotyping was done by PCR sequencing of the NS5b region. Viral RNA isolation was done using high pure viral nucleic acid kit (Roche Diagnostics, GmbH, Mannheim, Germany) according to the manufacturer’s instructions. 10 μL of HCV RNA was reverse-transcribed to cDNA using Quantitect reverse transcription kit (Qiagen, GmbH, Mannheim, Germany). cDNA was subjected to PCR using in-house designed primers (Table 1). PCR was performed using Phusion high-fidelity DNA polymerase (Thermoscientific Inc., Waltham, MA, USA). Amplified products were purified by gel-excision using QIAquick gel extraction kit (QIAGEN, GmbH, Germany). Forward and reverse sequence reads were aligned and assembled using DNA Baser v3.5.1 (Heracle BioSoft SRL, Romania). Genotype and subtype assignment were done by comparing the obtained sequences with the reported sequences on the Basic Local Alignment Search Tool (BLAST, USA) database of NCBI.
 |
Table 1 Details Of The Primer Sequences Used In The Study For Resistance-Associated Substitution Detection |
Sequencing Of NS5a and NS5b Region For RAS Detection
Part of NS5a and NS5b DAA target regions were amplified by a single round PCR reaction with in-house designed primers using Phusion hot-start DNA polymerase. For the NS5a region, different primer sets were used to amplify samples of gt1 and gt3 generating a PCR amplicon of size 554 bp and 602bp, respectively. For the NS5b region, a pan-genotypic primer set was used generating an amplicon size of 631 bp (Table 1). The resulting PCR products were excised from the gel and purified using the QIAquick Gel Extraction Kit (Qiagen). Sanger sequencing was performed with primers as denoted in the Big Dye Terminator v3.1 Cycle Sequencing Kit on an ABI Prism 3130xl Genetic Analyzer (Applied Biosystems, Foster City, CA).
RAS Analysis
Sequences were proofread and aligned using ClustalX version in BioEdit program v7.2.5 (Carlsbad, CA, USA). RAS analysis was done using geno2pheno [HCV].12 When no RASs were detected, amplicons were designated as wild-type and wherever RASs were detected it was denoted at that particular amino acid position. Substitutions at amino acid positions 28, 30, 31, and 93 in NS5a and 159,282,316 in NS5b were considered as relevant RASs as they have been previously reported as clinically relevant.13–16
Wherever RAS was detected, its occurrence was confirmed by checking both the forward and reverse sequences separately, and reproducibility of the data was also checked by repeated performance.
Statistical Analysis
Statistical analysis was done using the Statistical SPSS software, version 13.0 (Chicago, IL, USA). Continuous variables were expressed as mean ± SD or median (range) as appropriate and categorical variables were expressed as percentage. All statistical tests were 2-tailed, and results were statistically significant with a p-value was less than 0.05.
Results
Overall HCV genotyping was performed in 50 HCV-infected patients, and the predominant genotype that was seen was gt3 with subtype 3a was the most common. Distribution of genotypes in HCV-infected CKD was different from HCV-infected non-CKD patients. The predominant genotype seen in Group 1 was gt3, while the predominant genotype seen in Group 2 was gt1 (Table 2).
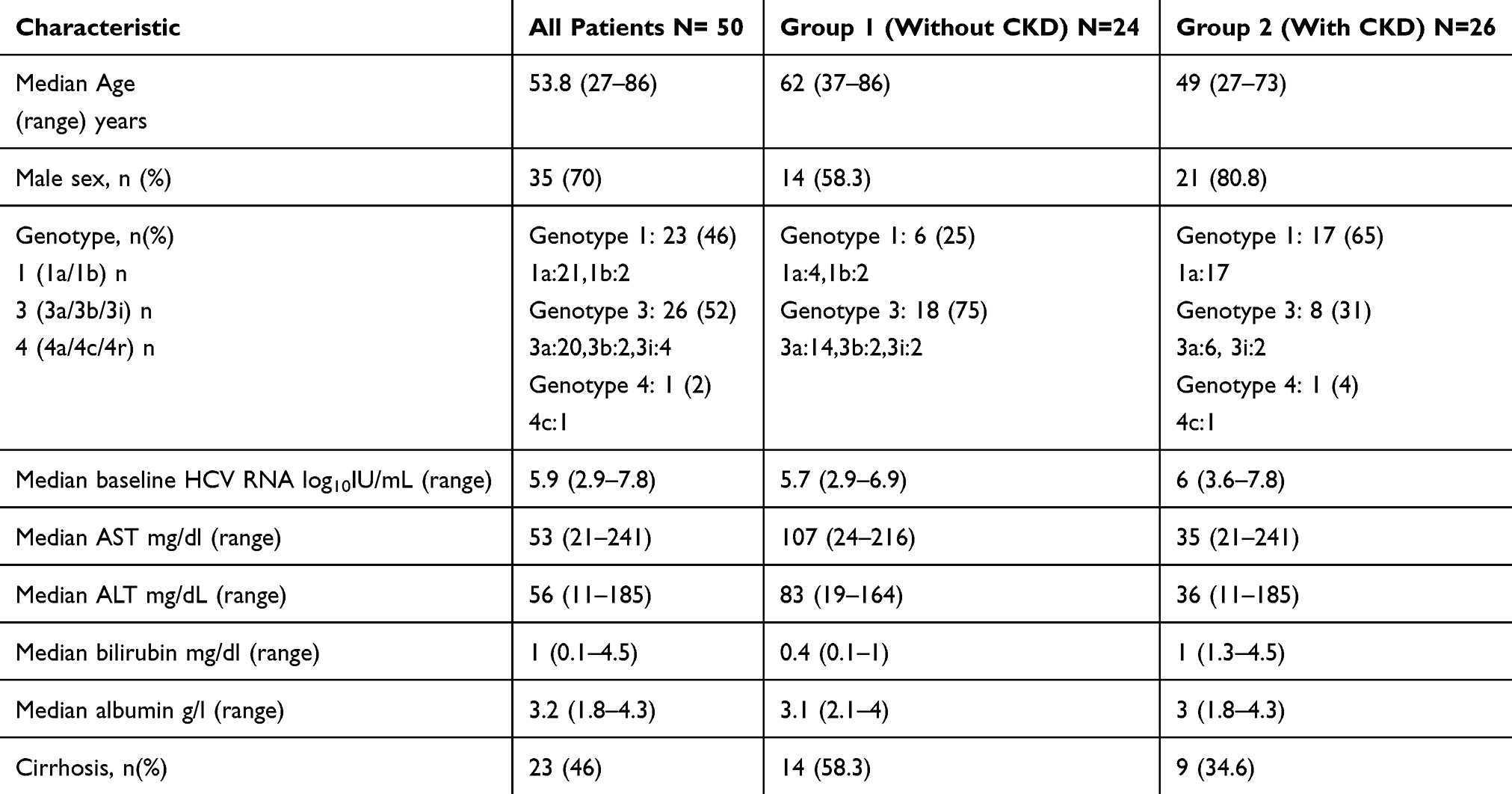 |
Table 2 Baseline Characteristics Of The Study Population |
Baseline Resistance-Associated Substitutions
The occurrence of RASs at baseline was seen in 10 patients (20%); in Group 1, they were seen in 8 (33.3%) as compared to only 2 (7.6%) in Group 2; p < 0.001. In HCV-infected patients with CKD (Group 2), baseline RASs were seen in only 2 patients at amino acid position 30K of the NS5a region of the virus, and both the patients belonged to the gt3a (Table 3).
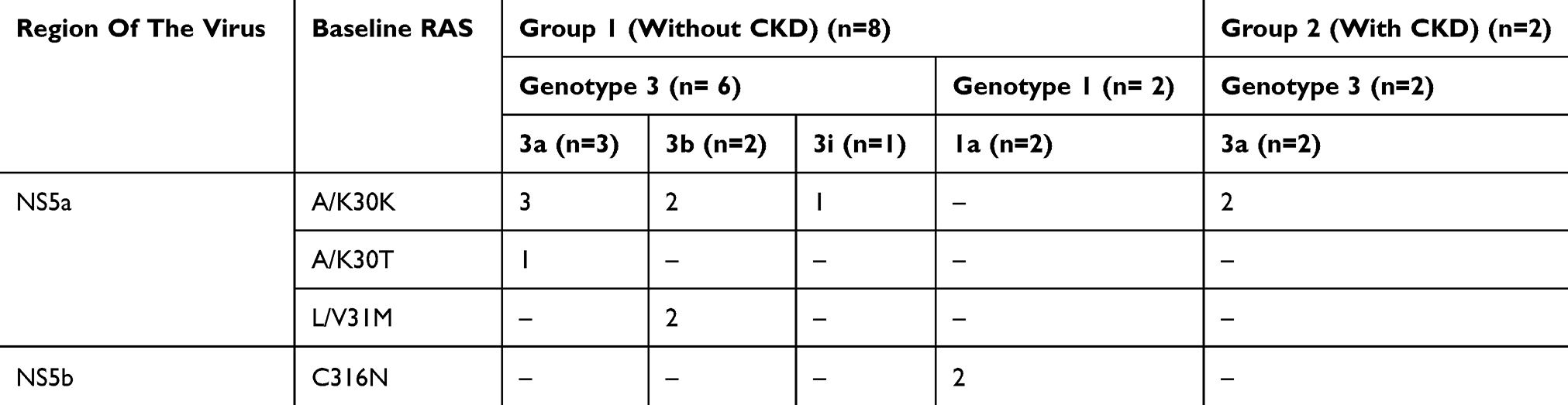 |
Table 3 Distribution Of Baseline RASs Seen In HCV-Infected Patients |
In Group 1 patients without CKD, baseline RASs were seen predominantly in patients infected with genotype 3 of the virus (at the amino acid position 30K in all 6 of the gt3-infected patients). 2 patients showed the presence of RAS in the NS5b region at amino acid position 316N, and they both were of gt1a as shown in Table 3. We did not see any baseline RAS at clinically relevant amino acid positions 28, 93 of NS5a region and 159, 282 of the NS5b region. In Group 1, RASs at more than one site and more than one RAS were also seen. In 2 patients, RASs were seen at 30K position along with 31M, and in one patient the position was the same but 2 different substitutions were seen at both 30K and 30T. This observation was not seen in the Group 2 patients (Table 3).
Genotype-Wise Distribution Of HCV RAS Mutations
The association of HCV genotype and the occurrence of baseline RAS was evaluated, and it was seen in the study that all the NS5b baseline RASs were seen in gt1-infected patients. Genotype 1 was the predominant type in Group 2, but it did not show any existence of baseline RAS. Although the study group is very small to comment on this occurrence, further large studies should be done to evaluate this effect. NS5a RASs at baseline were more commonly seen in genotype 3-infected patients especially genotype 3a (data not shown).
Baseline RAS And SVR
In Group 1, the overall SVR was attained in 70.8% (17/24) patients. In gt1, it was seen in 83.3% (5/6) while in gt3-infected patients it was seen in 66.6% (12/18). Among 7 patients who did not achieve SVR, baseline RASs were detected in 2 (28.5%). Both these patients had baseline RAS at more than one position with coexistence of RAS at A/K 30K along with L/V 31M. Although in our study, we did not find influence of baseline RAS on the attainment of SVR. But if RAS was present at more than 2 clinically relevant positions, it resulted in treatment failure.
SVR was attained in all the patients in Group 2; even in the 2 patients with demonstrable A/K 30K RAS was detected at baseline.
Discussion
DAAs are indeed game changers in achieving the goal of HCV elimination with a response rate of >90% which is remarkable. But in a subset of patients, approximately 2%-5%, this is not attained due to resistance shown to these drugs. Substitutions in the viral genome could be responsible for this. Occurrence of RAS is influenced by a lot of factors including viral and host factors and the type of treatment. Host status is known to influence the circulating genotype of the virus. In the present study, we highlighted the difference seen in the infecting virus type seen in two different kinds of patient population. Baseline RASs were more commonly seen in patients with only liver disease than in patients with coexisting CKD. Naturally occurring RASs in the viral genome are dependent on the host immune responses and the duration of the existence of the virus in the patient. Long-standing infection will have more variant type of virus in the host due to longer exposure to continuous immune pressure along with high replication rate of the virus. This is a common feature in a long-standing HCV infection. During intra-patient infection evolution of the virus, HCV evolves rapidly resulting in quasispecies. In the present study, multiple RASs were also seen at higher frequency in patients with only liver disease. This highlights the fact that the virus in CKD patients is less modulated. There is limited information about the evolution of HCV in this population; however, few researchers have pointed out to the occurrence of more variant kind of virus in this patient group.17 In our study, not only did the predominant genotype of the circulating virus differed in both the patient groups but also the naturally existing substitutions in the virus at the drug acting sites differed in both the groups. The association of RAS with the gt of the virus in the present study also highlights the differences seen in both patient groups. Globally, lot of literature is available regarding the prevalence of RAS in gt1 especially gt 1a. Limited studies have been done in gt3-infected patients. In our study, the occurrence of RAS was more in gt3 than in gt1. This highlights the need to study RAS in this type of population.
Limited literature is available regarding the prevalence of baseline RAS in CKD patients. There is one study on CKD patients on hemodialysis and renal transplant recipients, which shows an occurrence of RASs in 38.2%.18 In this study, the authors did not find clinically relevant RAS conferring high-level resistance in in vitro setup. Similarly, in our study, the existence of RASs in both the groups did not influence the treatment outcome.
There were few limitations in the study, one was that the small sample size was small and second it was a retrospective study. We suggest long-term prospective studies should be done in HCV-infected CKD patients, especially with gt3 infection. Another limitation was the utilization of the Sanger sequencing technique as the method for the identification of RAS. Sanger sequencing technique does not pick up variation occurring in the genome below 20%; hence, variations in the viral genome up to 20% are usually missed by this method. Clinical recommendation strongly suggests that variations occurring in a patient viral genome at a frequency of less than 20% might not be clinically relevant and will not have much effect on the resistance status of the infection.3,19 Therefore, detection of RAS by Sanger sequencing technique is justified. Host immune responses in both the groups were also not evaluated. Still, this preliminary study warrants that HCV virus status in terms of gt distribution and RAS detection in the different patient groups should be evaluated.
Conclusions
The prevalence of RAS at baseline in HCV-infected patients with liver disease was higher than HCV-infected patients with CKD. The type of host might influence the occurrence of these RAS in the virus, thereby controlling the response to the treatment.
Acknowledgement
We wish to acknowledge Mr. Keshav Singh for compiling data and for collection and archiving of patient samples related to this manuscript.
Disclosure
The authors do not have any conflicts of interest in this work.
References
1. Thomas DL. Global control of hepatitis C: where challenge meets opportunity. Nat Med. 2013;19(7):850–858. doi:10.1038/nm.3184
2. Vermehren J, Park JS, Jacobson IM, Zeuzem S. Challenges and perspectives of direct antivirals for the treatment of hepatitis C virus infection. J Hepatol. 2018;69(5):1178–1187. doi:10.1016/j.jhep.2018.07.002
3. Perez AB, Chueca N, Garcia F. Resistance testing for the treatment of chronic hepatitis C with direct acting antivirals: when and for how long? Germs. 2017;7(1):40–44. doi:10.11599/issn.2248-2997
4. Ahmed M. Era of direct acting anti-viral agents for the treatment of hepatitis C. World J Hepatol. 2018;10(10):670–684. doi:10.4254/wjh.v10.i10.670
5. Panel A-IHG. Hepatitis C guidance 2018 update: AASLD-IDSA recommendations for testing, managing, and treating hepatitis C virus infection. Clin Infect Dis. 2018;67(10):1477–1492. doi:10.1093/cid/ciy585
6. Zeuzem S, Mizokami M, Pianko S, et al. NS5A resistance-associated substitutions in patients with genotype 1 hepatitis C virus: prevalence and effect on treatment outcome. J Hepatol. 2017;66(5):910–918. doi:10.1016/j.jhep.2017.01.007
7. Cacoub P, Desbois AC, Isnard-Bagnis C, Rocatello D, Ferri C. Hepatitis C virus infection and chronic kidney disease: time for reappraisal. J Hepatol. 2016;65(1 Suppl):S82–S94. doi:10.1016/j.jhep.2016.06.011
8. Fabrizi F, Messa P, Basile C, Martin P. Hepatic disorders in chronic kidney disease. Nat Rev Nephrol. 2010;6(7):395–403. doi:10.1038/nrneph.2010.37
9. Girndt M, Sester U, Sester M, Kaul H, Kohler H. Impaired cellular immune function in patients with end-stage renal failure. Nephrol Dial Transplant. 1999;14(12):2807–2810. doi:10.1093/ndt/14.12.2807
10. Eleftheriadis T, Antoniadi G, Liakopoulos V, Kartsios C, Stefanidis I. Disturbances of acquired immunity in hemodialysis patients. Semin Dial. 2007;20(5):440–451. doi:10.1111/j.1525-139X.2007.00283.x
11. National Ethical guidelines for Biomedical and health research involving human participants. Available from: https://www.icmr.nic.in/sites/default/files/guidelines/ICMR_Ethical_Guidelines_2017.pdf.
12. Kalaghatgi P, Sikorski AM, Knops E, et al. Geno2pheno[HCV] - a web-based interpretation system to support hepatitis C treatment decisions in the era of direct-acting antiviral agents. PLoS One. 2016;11(5):e0155869. doi:10.1371/journal.pone.0155869
13. Krishnan P, Tripathi R, Schnell G, et al. Resistance analysis of baseline and treatment-emergent variants in hepatitis C virus genotype 1 in the AVIATOR study with paritaprevir-ritonavir, ombitasvir, and dasabuvir. Antimicrob Agents Chemother. 2015;59(9):5445–5454. doi:10.1128/AAC.00998-15
14. Nelson DR, Cooper JN, Lalezari JP, et al. All-oral 12-week treatment with daclatasvir plus sofosbuvir in patients with hepatitis C virus genotype 3 infection: ALLY-3 phase III study. Hepatology. 2015;61(4):1127–1135. doi:10.1002/hep.v61.4
15. Lawitz E, Sulkowski MS, Ghalib R, et al. Simeprevir plus sofosbuvir, with or without ribavirin, to treat chronic infection with hepatitis C virus genotype 1 in non-responders to pegylated interferon and ribavirin and treatment-naive patients: the COSMOS randomised study. Lancet. 2014;384(9956):1756–1765. doi:10.1016/S0140-6736(14)61036-9
16. Kwo P, Gitlin N, Nahass R, et al. Simeprevir plus sofosbuvir (12 and 8 weeks) in hepatitis C virus genotype 1-infected patients without cirrhosis: OPTIMIST-1, a phase 3, randomized study. Hepatology. 2016;64(2):370–380. doi:10.1002/hep.28467
17. Alves da Silva R, de Souza Todao J, Kamitani FL, et al. Molecular characterization of hepatitis C virus in end-stage renal disease patients under hemodialysis. J Med Virol. 2018;90(3):537–544. doi:10.1002/jmv.v90.3
18. Tavares RCF, de Castro Amaral Feldner AC, Pinho JRR, et al. Prevalence of resistance-associated substitutions to direct-acting antiviral agents in hemodialysis and renal transplant patients infected with hepatitis C virus. Infect Drug Resist. 2018;11:1993–2000. doi:10.2147/IDR
19. Pawlotsky JM. Hepatitis C virus resistance to direct-acting antiviral drugs in interferon-free regimens. Gastroenterology. 2016;151:70–86. doi:10.1053/j.gastro.2016.04.003
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.