")
Back to Journals » International Journal of General Medicine » Volume 15
Low ZCCHC9 Gene Expression in Peripheral Blood May Be an Acute Myocardial Infarction Genetic Molecular Marker in Patients with Stable Coronary Atherosclerotic Disease
Authors Li L , Meng H, Wang X , Ruan J, Tian X, Meng F
Received 26 October 2021
Accepted for publication 25 January 2022
Published 18 February 2022 Volume 2022:15 Pages 1795—1804
DOI https://doi.org/10.2147/IJGM.S346335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lihong Li, Heyu Meng, Xue Wang, Jianjun Ruan, Xiaomin Tian, Fanbo Meng
Department of Cardiology, The Third Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Fanbo Meng, Department of Cardiology, The Third Hospital of Jilin University, Changchun, People’s Republic of China, Tel +86-15948346855, Fax + 86-431-84995228, Email [email protected]
Purpose: ZCCHC9 is a zinc finger protein with a CCHC zinc finger structure and has important roles in several cellular processes. This study was conducted on an expanded number of samples to evaluate The usefulness of ZCCHC9 gene expression in peripheral blood as a molecular marker for the prediction of AMI (acute myocardial infarction) risk.
Patients and Methods: Peripheral blood samples were collected from 117 patients with stable CAD (coronary atherosclerotic disease) and 126 patients with AMI. The mRNA level of the ZCCHC9 gene was assessed by qRT-PCR, and its protein level was determined by Western blotting.
Results: The AMI group exhibited reduced expression of the ZCCHC9 gene, at both transcript and protein levels, than the stable CAD group. The low expression of the ZCCHC9 gene was not related to blood glucose level (P=0.635), blood lipid level, and troponin level (P=0.715), and may cause AMI through the MAPK signaling pathway. Compared with other patients, patients with low ZCCHC9 gene expression in their peripheral blood have a 2.597-fold higher risk of AMI.
Conclusion: ZCCHC9 gene expression in peripheral blood was significantly lower in patients with AMI than in stable CAD patients. Individuals with low expression of ZCCHC9 in peripheral blood have higher a probability to develop AMI than those with stable CAD. Thus, lowered ZCCHC9 gene expression can act as an independent risk factor for AMI.
Keywords: genetics, molecular marker, oxidative stress, MAPK
Introduction
The American Heart Association’s 2020 statistical report on heart disease and stroke shows that 18.2 million people aged ≥ 20 years have coronary atherosclerotic disease (CAD), and the number of deaths due to CAD was 365,914 in the United States.1 Although the CAD mortality rate in Western countries has declined in the past four decades, this situation still accounts for one-Third of the total deaths of people over 35 years of age.2 Likewise, the China Cardiovascular Health and Disease Report 2019 outlines that there are currently more than 300 million cardiovascular disease patients, and 2 out of every 5 deaths are due to cardiovascular disease, and its prevalence and mortality are rising.3 AMI (Acute myocardial infarction) is a serious symptom of CAD and the primary cause of death in CAD patients. Although great progress has been made in prevention and treatment, CAD is still the main cause of global disease and death.1,4 Therefore, the early warning of AMI is of great clinical significance.
AMI is a multi-cause disease that occurs due to a variety of environmental and genetic factors and their interactions.5 Traditional risk factors, including high serum cholesterol, smoking, diabetes, and hypertension can partially predict the prevention and prognosis of the disease.6,7 Nevertheless, some CAD patients often lack, and nearly 20% of patients do not have traditional risk factors, while 40% of patients have only one risk factor.8,9 Currently, non-traditional and genetic factors have received increasing attention, they rely mainly on genomics, transcriptomics, and proteomics research. With the continuous development of molecular biology techniques, transcriptomics plays a vital role in molecular marker discovery.10 Gene polymorphisms are linked to the risk of coronary heart disease.11 Changes in gene expression levels in peripheral blood may provide useful tools for the diagnosis and prognosis of many complex diseases including AMI.12 For example, miR-208b, and miR-499 in peripheral blood can potentially act as AMI biomarkers.13 Increased peripheral blood levels of lncRNA H19, MALAT1, and MIAT can potentially act as biological markers for the diagnosis of AMI.14 Our group has also successively confirmed through experiments that the expression levels of PIK3C2A,15 PRMT5,16 SOCS3,17 and other related genes in peripheral blood have a potential utility as molecular markers for predicting the occurrence of AMI.
The emergence of GWAS (genome-wide association studies) has allowed the identification of many alleles with a higher risk of myocardial infarction. In addition, the functions of these genes were further explored, including elevated LDL, apoptosis, coronary artery calcification, lipoprotein metabolism, smooth muscle cell proliferation, and inflammation.18 There is no report on the function of ZCCHC9 in the occurrence and development of cardiovascular disease. A previous differential gene expression profile assessment of AMI in the peripheral blood of this research group showed that the peripheral blood ZCCHC9 gene is differentially expressed in AMI patients and stable CAD patients.19
Therefore, this study aimed to clarify the relationship between ZCCHC9 mRNA and protein expression and AMI by expanding the sample size of clinical data, extracting total RNA from the peripheral blood of the subject, reverse transcription into cDNA, and PCR amplification.
Materials and Methods
Research Subjects
For the test group, AMI patients (n=126) who were Hospitalized in the China-Japan Union Hospital, Department of Cardiovascular Medicine, Jilin University from March 2018 to May 2018 and received coronary angiography were chosen, and for the control group, 117 patients with stable CAD were selected. The criteria for the selection of AMI were as per the Universal Definition of Myocardial Infarction (the fourth edition), issued in 2018.20 The exclusion criteria of the experimental group were: myocardial infarction related to PCI, stent thrombosis, stent restenosis, and myocardial infarction related to coronary artery bypass graft. The selection criteria of the control group are congruent with the guidelines issued in 2019 by the European Society of Cardiology (ESC) for chronic coronary syndrome diagnosis and management.21 The control group exclusion criteria were: patients presenting with chest pain, less than 50% coronary artery stenosis as detected by coronary angiography, and the ECG showing no pathological Q wave and secondary changes in T wave and ST-segment. Patients with pleurisy and intercostal neuritis, acute pneumonia, and other inflammations were excluded.
The clinical data of all study subjects were recorded in detail, including gender, age, smoking history, history of diabetes, history of hypertension, TG (serum triglycerides), fasting blood glucose, TC (total cholesterol), LDL-C (low-density lipoprotein cholesterol), and HDL-C (high-density lipoprotein cholesterol), and troponin I, etc.
Methods of Research
Peripheral Blood Sample Collection, Extraction of Total RNA, and cDNA Synthesis
For lymphocyte extraction 6 mL of peripheral venous blood after fasting was collected from each subject in the morning. Total RNA was extracted from the obtained lymphocytes using the Blood Total RNA Kit from Xinjing Biological Reagent Development Co., Ltd. (Hangzhou). The extraction process strictly followed the instructions on the kit. Reverse transcription was carried out using the total RNA and the first-strand synthesis premix as per the instructions of the Fastking One-step Genomic cDNA reverse transcription kit (Tiangen Biochemical Technology Co., Ltd., Beijing). The concentration of RNA of each sample for the reaction was the same. The obtained cDNA samples were stored at a temperature of −80°C for further experiments.
Quantitative Real-Time Fluorescence PCR (qRT-PCR) Detection
PCR amplification of fragments was conducted using the SYBR fluorescence quantitative PCR kit from the Biotech Fluorescence Quantitative Kit, Taq qPCR synthesis premix reagent (Shanghai). A volume of 20 µL reaction solution included: 10 µL 2xSG Fast qPCR reaction mixture, 2 µL DNF buffer, 0.4 µL each of primers (forward and reverse; final concentration 10 µmol/L), 6.2 µL sterile water (double distilled), and 1 µL of cDNA sample. To amplify the genes, the 7500 Fast Dx Real-time Fluorescence Quantitative PCR System was used. Post-amplification, the melting and amplification curves were recorded in the range of 60 °C to 95 °C. GAPDH and ZCCHC9 were used as the gene for normalization and the target gene, respectively, and the software dissociation curve of the ABI-FAST7500 instrument was used for specific amplification conditions. For each sample, the obtained cycle threshold (ct) was expressed as relative expression 2−Δct (Δct = ct value of the target gene - ct value of the reference gene).
Statistical Analysis
SPSS v25.0 software was used for statistical analysis. The normality test was used for measuring data that obeyed the normal distribution (P>0.1) were statistically described by X±S, and the difference between groups was analyzed by t-test of two independent samples. The data not following a normal distribution (P≤0.1) were described using the median and interquartile range, and the variations between groups are analyzed nonparametric rank-sum test using two independent samples. The count data was described by statistical analysis by frequency, and the difference between groups was analyzed by x2 test. Multivariate Logistic regression was carried out for risk factors associated with AMI. The association between the ZCCHC9 gene and troponin I expressions was analyzed by bivariate correlation. The statistical results were deemed statistically significant with a bilateral P≤0.05.
Results
Assessment of Clinical Data
The clinical baseline data analysis of the study subjects showed that there was no statistical difference in gender, age, history of high blood pressure, diabetes history, smoking history, TG, TC, HDL-C, and LDL-C between patients of two groups (P>0.05). However, the level of blood glucose of the AMI group after fasting was higher at significant levels (P<0.05) than that of the stable CAD group (Table 1).
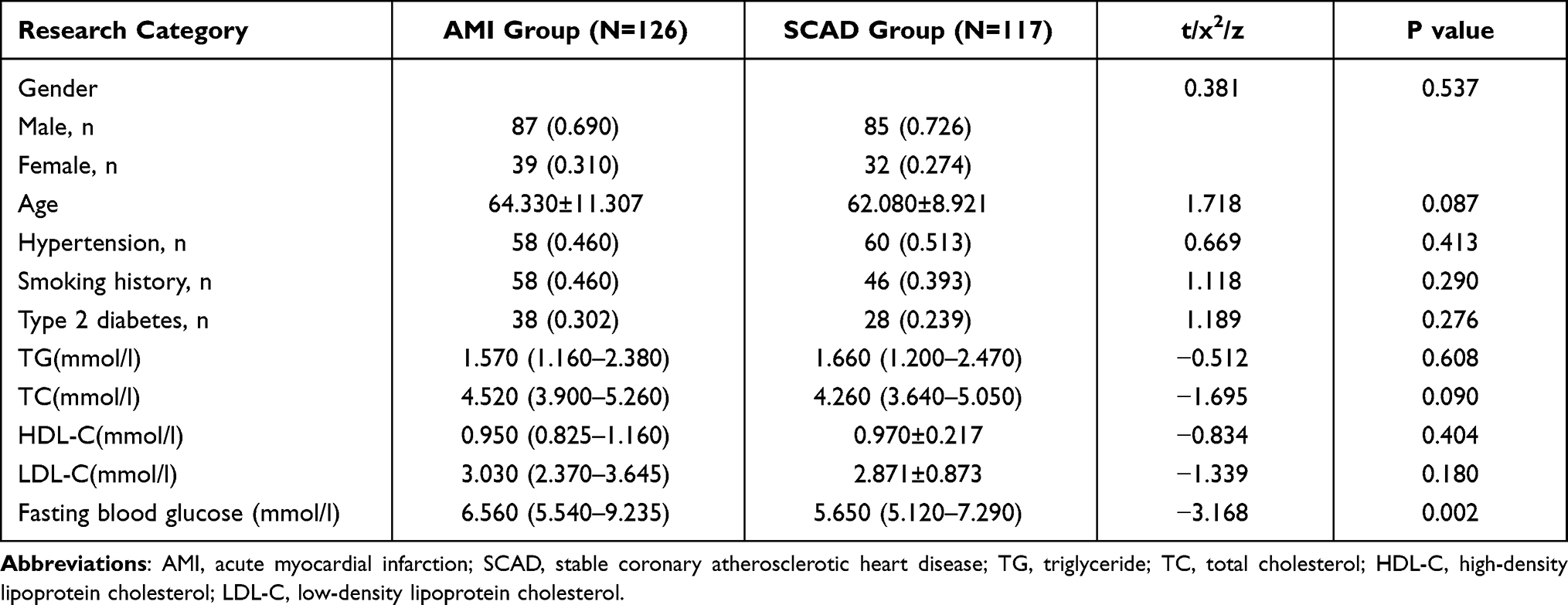 |
Table 1 The Clinical Baseline Data Were Compared for the AMI and the Stable CAD Groups |
Identification of ZCCHC9 Gene Amplification Products in Peripheral Blood
In this assay, the amplification curves (Figure 1A) of the target gene and internal reference gene were smooth “S-shaped” and all the melting curves (Figure 1B) came together as single peaks, with no multiple peaks. These results show that the amplification primers are highly specific, the reaction conditions are appropriate, with no non-specific amplification (Figure 1).
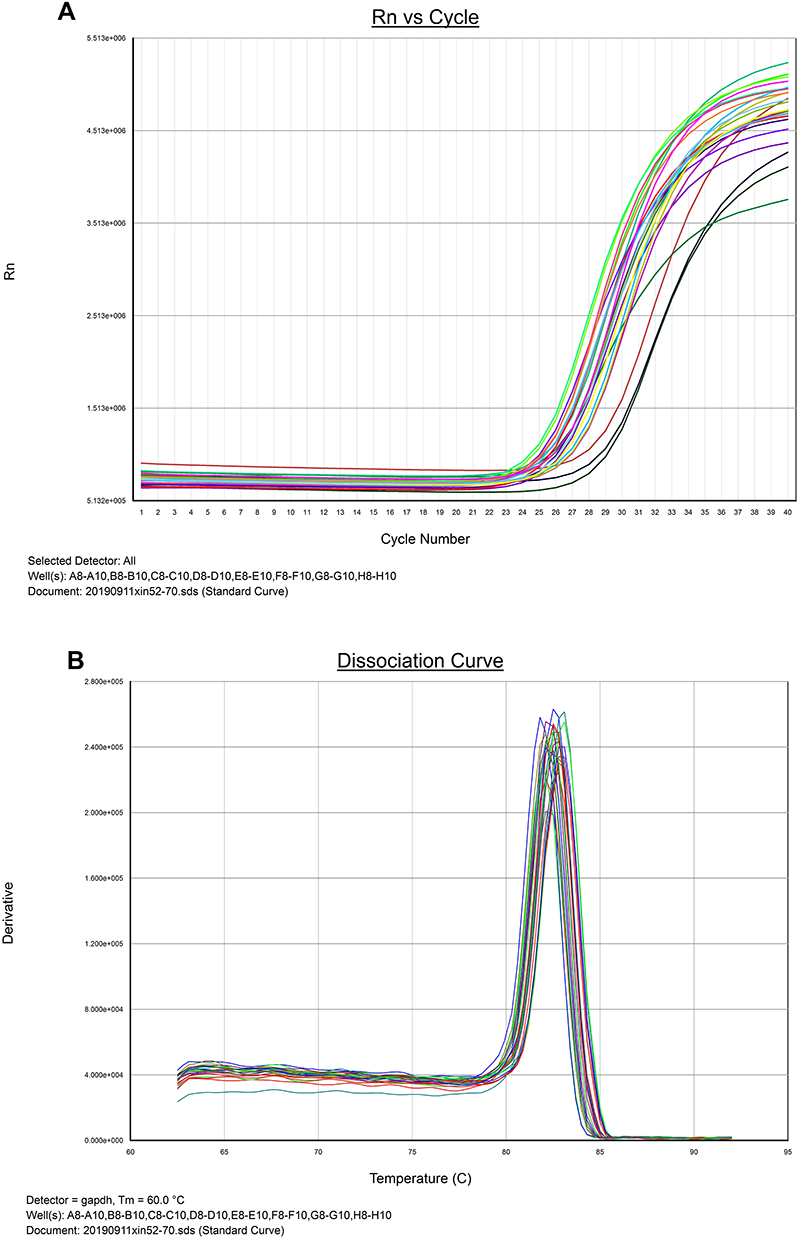 |
Figure 1 qRT-PCR amplification curve (A) and melting curve (B) of ZCCHC9 gene. |
Comparative Analysis of ZCCHC9 Gene Expression at mRNA Level
For each sample, the Δct value obtained by qRT-PCR was the average of values obtained by conducting each experiment thrice for each sample. The 2−Δct value of the AMI group was 0.516 (0.181–0.906) and that of the stable CAD group was 0.685 (0.207–1.127), and the difference in terms of statistical values was significant (P<0.05) between the two groups. The peripheral blood from AMI group samples exhibited significantly lower ZCCHC9 mRNA expression, with the relative expression 0.753 times that of the stable CAD group, as shown in Figure 2.
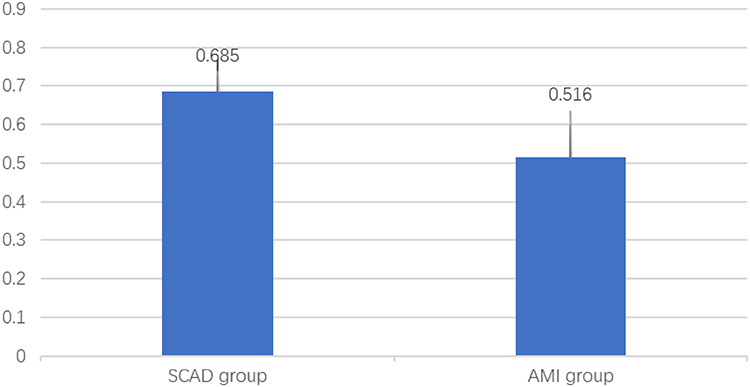 |
Figure 2 Relative expression of ZCCHC9 gene. |
Comparative Analysis of the Expression of ZCCHC9 Protein in Peripheral Blood
For this, Western blot was conducted using β-actin was used for normalization, and the experiment was repeated thrice per group to detect the target gene level in the patients’ peripheral blood. The β-actin expression in the stable CAD group and the AMI group was not significantly different (Figure 3A), while the level of the ZCCHC9 gene differed among the two groups (Figure 3B) (image J 2006 edition). The level of ZCCHC9 protein in the AMI group was found to be 0.917 times that in the stable CAD group (Figure 3).
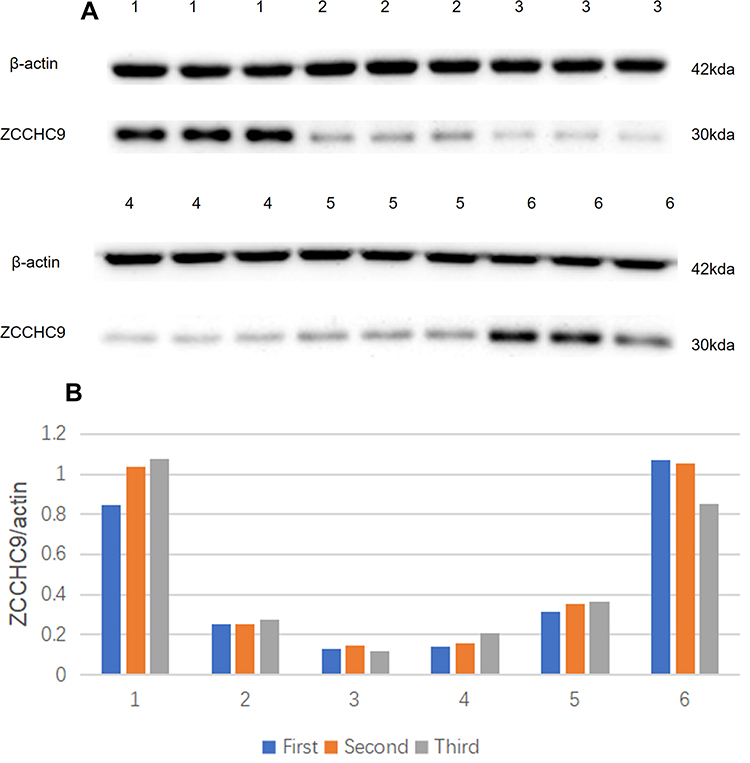 |
Figure 3 ZCCHC9 gene protein expression level. 1, 2, and 3 represent the AMI samples, and 4, 5, and 6 represent the stable CAD samples. Protein expression profiles (A) and relative experession level (B) of related genes. |
Correlation Analysis Between the ZCCHC9 Gene and Fasting Blood Glucose Expressions
The clinical baseline data of the subjects in this study revealed a statistically significant variation between the level of fasting blood glucose in the stable CAD and the AMI groups. Therefore, we further analyzed whether there is an association between fasting blood glucose and the expression of ZCCHC9 mRNA. All subjects were categorized into two groups: the normal fasting blood glucose group (≤5.6) and the elevated fasting blood glucose group (>5.6).22 We found no correlation between the expression of ZCCHC9 mRNA and the patient’s fasting blood glucose level (Table 2).
 |
Table 2 Correlation Analysis Between ZCCHC9 Gene mRNA Expression and Fasting Blood Glucose Level |
Logistic Regression Analysis of the Relationship Between ZCCHC9 Gene Expression, AMI, and the Level of Fasting Blood Glucose Level
According to the cut-off value of the relative expression of the ZCCHC9 gene, each subject was grouped either into the low gene expression group (2−Δct≤1.090), or the high gene expression group (2−Δct>1.090). The low ZCCHC9 gene expression was found to be an independent AMI risk factor (P=0.009). The low ZCCHC9 gene expression group had a 2.597-fold increase in the risk of AMI compared to that in the high ZCCHC9 gene expression group. High fasting blood glucose was found to be an independent AMI risk factor (P=0.001), and the increased fasting blood glucose raised 2.514 times the AMI risk (Table 3).
 |
Table 3 Independent AMI Risk Factors Determined Through Logistic Regression Analysis |
Bivariate Correlation Analysis Between ZCCHC9 Gene Level and Troponin I Expression
The concentration of troponin may indicate the area of myocardial infarction. The concentration of troponin I in the AMI group was 2.085 (0.120–2.473) ng/mL. After bivariate correlation analysis, there was no correlation between serum troponin concentration and ZCCHC9 gene expression in peripheral blood (r=−0.026, p=0.715). That is, no correlation was observed between ZCCHC9 gene expression in peripheral blood and the area of AMI.
Discussion
The level of the ZCCHC9 gene in the peripheral blood of the AMI group was found to be lower than that in the stable CAD group at the level of both transcript and protein.
Gene-related research shows that the ZCCHC9 gene is located on human chromosome 5. It is a zinc finger protein with a CCHC zinc-finger structure and contains 271 amino acids with a molecular weight of 29KDa. The ZCCHC9 protein contains the relatively conserved amino acid sequence Cys-X2-Cys-X4-His-X4-Cys. It can bind to DNA, RNA, and sometimes mediate protein interactions, participate in a number of cellular processes in various physiological conditions and diseases.23,24 Compared with other zinc finger proteins, CCHC-type proteins have been less studied. This study focused mainly on ZCCHC9 gene expression in peripheral blood and revealed its significantly low expression in the AMI group than in the stable CAD group.
Besides the abnormal expression of the ZCCHC9 mRNA in the AMI group than the stable CAD group, fasting blood glucose levels also showed statistical differences among the two groups. The AMI group had significantly high fasting blood glucose levels than the stable CAD group. We also found that the aberrant expression of the ZCCHC9 gene did not correlate to fasting blood glucose levels. Logistic regression analysis results in this experiment showed that fasting blood glucose at a high level was an independent AMI risk factor, and showed 2.514-folds elevated AMI risk. Likewise, regardless of fasting blood glucose and other factors, the low ZCCHC9 gene expression singly could also enhance AMI risk 2.597-folds. This is in line with the previous results. A reasonable explanation may be that the ZCCHC9 gene does not promote the occurrence of AMI by affecting blood glucose levels. Concurrently, persistent hyperglycemia, in comparison to fluctuating hyperglycemia activates oxidative stress with greater potential to increase the risk of microvascular disease and death because of cardiovascular disease.25–27
The concentration of troponin I in peripheral blood can diagnose the area of myocardial infarction and indicate the myocardial infarction severity. We also found no correlation between ZCCHC9 gene level and troponin I concentration; this could have been the case if the low ZCCHC9 gene expression causes AMI. Therefore, we assumed that the low level of ZCCHC9 is related to the onset of AMI, but the severity of AMI and the infarct size could not be evaluated accordingly.
Many zinc finger proteins have been shown to affect the MAPK signaling pathway. For example, ZCCHC13 can positively regulate the MAPK pathway to promote normal testicular development.28 ZCCHC11 inhibits the activation of tumor necrosis factor-related factor 6-dependent NF-κB, and it is an important factor in the MAPK signal cascade.29 The ZCCHC9 gene may down-regulate transcription mediated by NF-κB and serum response elements (from GeneCards https://www.genecards.org/). ZCCHC9 gene plays an important role in the MAPK signal pathway by inhibiting the transactivation activity of NF-κB and SRE. It also up-regulates the JNK pathway activity in the MAPK pathway subfamily in lung cancer cells such as A549 and NCI-H1299 to promote the proliferation and invasion of cancer cells.24,30 This indicates that ZCCHC9 has a potential role in the MAPK signaling cascade. Oxidative stress, that is, reactive oxygen species that mediate a series of biochemical reactions in cells through MAPK signaling pathways, is related to AMI.31 Thus, we can infer that the low level of ZCCHC9 may promote oxidative stress through the MAPK pathway to promote the occurrence of AMI.
Interestingly, ZCCHC9 is related to the occurrence of tumor diseases. Zinc finger proteins play a corresponding role through the binding of some specific amino acid domains to DNA/RNA and are inextricably linked to the occurrence of some tumors. That is, some tumors may be activated as a result of the change in the structure of zinc finger proteins. The MAPK signaling pathway also has a vital part in the occurrence of breast cancer,32 prostate cancer,33 lung adenocarcinoma,34 and other tumors. Further, we can reasonably speculate that there may be a common MAPK signal transduction pathway in tumorigenesis and AMI. Concurrently, many reports have shown the association between the occurrence of AMI and tumors, such as breast carcinoma,35 lung carcinoma,36 and pancreatic cancer.37 This is a rare case of AMI because cancer embolizes coronary vessels or directly invades the left atrium during the progression of the disease.
Only little is known about ZCCHC9; genome-wide expression profiling study indicated up-regulation of ZCCHC9 in the human neck cancers cells both HPV (human papillomaviruses) positive or negative and cervical cancer cells relative to normal cells.38 In our study the AMI patients had significantly low ZCCHC9 gene expression in their peripheral blood compared to that in the control group. Therefore, further research is necessary.
There were a few limitations to this study. First, the expression of the ZCCHC9 gene in cardiomyocytes was not clarified. Second, we can only speculate that there exists a common pathway between tumorigenesis and AMI, as we did not perform relevant experiments to confirm it. Finally, the plaque vulnerability and medication status of the two groups of subjects were not statistically analyzed. Therefore, a larger sample of research may be more meaningful. Moreover, further cytological study is necessary. Nevertheless, this study clearly shows that the low expression of the ZCCHC9 gene is related to the occurrence of AMI.
Conclusion
The AMI patients had significantly low ZCCHC9 gene expression in their peripheral blood compared to that in the control group and this low expression was found to be an independent risk factor for AMI. Finally, this low peripheral blood expression of the ZCCHC9 gene may serve as an AMI genetic marker in stable coronary heart disease patients.
Abbreviations
AMI, Acute myocardial infarction; CAD, coronary atherosclerotic heart disease; TG, triglyceride; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; PCI, percutaneous coronary intervention; MAPK, mitogen-activated protein kinases; NF-Kb, nuclear factor-k-gene binding.
Data Sharing Statement
Data information can be obtained by contacting the first and the corresponding authors via e-mail.
Compliance with Ethical Standards
All patients selected in the study, which is in accordance with the ethical principles of the Helsinki Declaration on medical research of human subjects. This study has been approved by Ethics Committee (2016SCZ008), The Third Hospital of Jilin University, The agreement has been reached between The Third Hospital of Jilin University and all the subjects regarding collection of their samples and information for this study. The consent forms have been signed by all the subjects.
Acknowledgments
We thank the Shenyang Huibai Biotech Co., Ltd., for their technical support in the Western blot analysis, and Dr. Zhao ZH and his team in the Heping Campus of Jilin University for their assistance in the experimental part of the work.
Part of the abstract has been published in the 31th Great Wall International Congress of Cardiology.
Funding
This research was funded by the Health Commission of Jilin Province in 2018. (Project number, 2018SCZ008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. American Heart Association Council on epidemiology and prevention statistics committee and stroke statistics subcommittee. heart disease and stroke statistics-2020 update, A report from the American Heart Association. Circulation. 2020;141(9):139–596.
2. Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016;4(13):256. doi:10.21037/atm.2016.06.33
3. The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2019, an updated summary. Chin Circ J. 2020;35(9):833–854.
4. Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. Lancet. 2017;389(10065):197–210. doi:10.1016/S0140-6736(16)30677-8
5. Gao Y, Qi GX, Guo L, Sun YX. Bioinformatics analyses of differentially expressed genes associated with acute myocardial infarction. Cardiovasc Ther. 2016;34(2):67–75. doi:10.1111/1755-5922.12171
6. Law MR, Watt HC, Wald NJ. The underlying risk of death after myocardial infarction in the absence of treatment. Arch Intern Med. 2002;162(21):2405–2410. doi:10.1001/archinte.162.21.2405
7. Alshammary AF, Alharbi KK, Alshehri NJ, Vennu V, Ali khan I. Metabolic syndrome and coronary artery disease risk: a meta-analysis of observational studies. Int J Environ Res Public Health. 2021;18(4):1773. doi:10.3390/ijerph18041773
8. Ajani UA, Ford ES. Has the risk for coronary heart disease changed among U.S. adults? J Am Coll Cardiol. 2006;48(6):1177–1182. doi:10.1016/j.jacc.2006.05.055
9. Hozawa A, Folsom AR, Sharrett AR, Chambless LE. Absolute and attributable risks of cardiovascular disease incidence in relation to optimal and borderline risk factors, comparison of African American with white subjects–Atherosclerosis Risk in Communities Study. Arch Intern Med. 2007;167(6):573–579. doi:10.1001/archinte.167.6.573
10. Wong HR. Clinical review, sepsis and septic shock–the potential of gene arrays. Crit Care. 2012;16(1):204. doi:10.1186/cc10537
11. Matam K, Khan IA, Hasan Q, Rao P. Coronary artery disease and the frequencies of MTHFR and PON1 gene polymorphism studies in a varied population of Hyderabad, Telangana region in south India. J King Saud Univ Sci. 2015;27(2):143–150. doi:10.1016/j.jksus.2014.09.002
12. Aziz H, Zaas A, Ginsburg GS. Peripheral blood gene expression profiling for cardiovascular disease assessment. Genomic Med. 2007;1(3–4):105–112. doi:10.1007/s11568-008-9017-x
13. Agiannitopoulos K, Pavlopoulou P, Tsamis K, et al. Expression of miR-208b and miR-499 in Greek patients with acute myocardial infarction. In Vivo. 2018;32(2):313–318. doi:10.21873/invivo.11239
14. Wang XM, Li XM, Song N, Zhai H, Gao XM, Yang YN. Long non-coding RNAs H19, MALAT1 and MIAT as potential novel biomarkers for diagnosis of acute myocardial infarction. Biomed Pharmacother. 2019;118:109208. doi:10.1016/j.biopha.2019.109208
15. Tan B, Liu M, Yang Y, Liu L, Meng F. Low expression of PIK3C2A gene, A potential biomarker to predict the risk of acute myocardial infarction. Medicine. 2019;98(14):15061. doi:10.1097/MD.0000000000015061
16. Tan B, Liu Q, Yang L, et al. Low expression of PRMT5 in peripheral blood may serve as a potential independent risk factor in assessments of the risk of stable CAD and AMI. BMC Cardiovasc Disord. 2019;19(1):31. doi:10.1186/s12872-019-1008-4
17. Meng H, Wang X, Ruan J, Chen W, Meng F, Yang P. High expression levels of the SOCS3 gene are associated with acute myocardial infarction. Genet Test Mol Biomarkers. 2020;24(7):443–450. doi:10.1089/gtmb.2020.0040
18. Erdmann J, Linsel-Nitschke P, Schunkert H. Genetic causes of myocardial infarction, new insights from genome-wide association studies. Dtsch Arztebl Int. 2010;107(40):694–699. doi:10.3238/arztebl.2010.0694
19. Fan L, Meng H, Guo X, Li X, Meng F. Differential gene expression profiles in peripheral blood in Northeast Chinese Han people with acute myocardial infarction. Genet Mol Biol. 2018;41(1):59–66. doi:10.1590/1678-4685-gmb-2017-0075
20. Alpert JS. The fourth edition of the universal definition of myocardial infarction. Am J Med. 2018;131(11):1265–1266. doi:10.1016/j.amjmed.2018.06.016
21. Knuuti J, Wijns W, Saraste A, et al.; ESC Scientific Document Group. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
22. Cosentino F, Grant PJ, Aboyans V, et al.; ESC Scientific Document Group. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323. doi:10.1093/eurheartj/ehz486
23. Cassandri M, Smirnov A, Novelli F, et al. Zinc-finger proteins in health and disease. Cell Death Discov. 2017;3:17071. doi:10.1038/cddiscovery.2017.71
24. Zhou A, Zhou J, Yang L, et al. A nuclear localized protein ZCCHC9 is expressed in cerebral cortex and suppresses the MAPK signal pathway. J Genet Genomics. 2008;35(8):467–472. doi:10.1016/S1673-8527(08)60064-8
25. Matthews DR, Stratton IM, Aldington SJ, Holman RR, Kohner EM; UK Prospective Diabetes Study Group. Risks of progression of retinopathy and vision loss related to tight blood pressure control in type 2 diabetes mellitus, UKPDS 69. Arch Ophthalmol. 2004;122(11):1631–1640.
26. Monnier L, Mas E, Ginet C, et al. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA. 2006;295(14):1681–1687. doi:10.1001/jama.295.14.1681
27. DECODE Study Group. Glucose tolerance and mortality, comparison of WHO and American Diabetes Association diagnostic criteria. Diabetes epidemiology, collaborative analysis of diagnostic criteria in Europe. Lancet. 1999;354(9179):617–621. doi:10.1016/S0140-6736(98)12131-1
28. Li Z, Chen S, Yang Y, Zhuang X, Tzeng CM. Novel biomarker ZCCHC13 revealed by integrating DNA methylation and mRNA expression data in non-obstructive azoospermia. Cell Death Discov. 2018;4:36. doi:10.1038/s41420-018-0033-x
29. Minoda Y, Saeki K, Aki D, et al. A novel Zinc finger protein, ZCCHC11, interacts with TIFA and modulates TLR signaling. Biochem Biophys Res Commun. 2006;344(3):1023–1030. doi:10.1016/j.bbrc.2006.04.006
30. Shi X, Jiang B, Liu H, Fan C. ZCCHC9 promotes proliferation and invasion of lung cancer through regulating the JNK pathway. J Cell Biochem. 2019;120(6):10596–10604. doi:10.1002/jcb.28346
31. Ismail MK, Samera MY, Abid SK. Oxidative stress markers and antioxidant activity in patients admitted to Intensive Care Unit with acute myocardial infarction. Int J Health Sci. 2018;12(5):14–19.
32. Qi X, Tang J, Loesch M, Pohl N, Alkan S, Chen G. p38gamma mitogen-activated protein kinase integrates signaling crosstalk between Ras and estrogen receptor to increase breast cancer invasion. Cancer Res. 2006;66(15):7540–7547. doi:10.1158/0008-5472.CAN-05-4639
33. Tanaka Y, Gavrielides MV, Mitsuuchi Y, Fujii T, Kazanietz MG. Protein kinase C promotes apoptosis in LNCaP prostate cancer cells through activation of p38 MAPK and inhibition of the Akt survival pathway. J Biol Chem. 2003;278(36):33753–33762. doi:10.1074/jbc.M303313200
34. Stutvoet TS, Kol A, de Vries EG, et al. MAPK pathway activity plays a key role in PD-L1 expression of lung adenocarcinoma cells. J Pathol. 2019;249(1):52–64. doi:10.1002/path.5280
35. Bhojwani N, Harwani A, Hartman JB, Partovi S, Gilkeson RC. Metastatic breast carcinoma to the coronaries: a rare cause of acute myocardial infarction. Methodist Debakey Cardiovasc J. 2016;12(3):179–182. doi:10.14797/mdcj-12-3-179
36. Kumagai N, Miura SI, Toyoshima H, et al. Acute myocardial infarction due to malignant neoplastic coronary embolus. J Cardiol Cases. 2010;2(3):123–127. doi:10.1016/j.jccase.2010.05.005
37. Robinson BW, Lewis RR. Myocardial metastasis from carcinoma of pancreas presenting as acute myocardial infarction. J R Soc Med. 1982;75(7):560–562.
38. Pyeon D, Newton MA, Lambert PF, et al. Fundamental differences in cell cycle deregulation in human papillomavirus-positive and human papillomavirus-negative head/neck and cervical cancers. Cancer Res. 2007;67(10):4605–4619. doi:10.1158/0008-5472.CAN-06-3619
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.