")
Back to Journals » Cancer Management and Research » Volume 12
Low Prognostic Nutritional Index Predicts Poor Clinical Outcomes in Patients with Stage IIIB Non-small-cell Lung Carcinoma Undergoing Chemoradiotherapy
Authors Ozdemir Y , Topkan E , Mertsoylu H , Selek U
Received 1 February 2020
Accepted for publication 6 March 2020
Published 16 March 2020 Volume 2020:12 Pages 1959—1967
DOI https://doi.org/10.2147/CMAR.S248034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Yurday Ozdemir,1 Erkan Topkan,1 Huseyin Mertsoylu,2 Ugur Selek3,4
1Department of Radiation Oncology, Baskent University Medical Faculty, Adana, Turkey; 2Department of Medical Oncology, Baskent University Medical Faculty, Adana, Turkey; 3School of Medicine, Department of Radiation Oncology, Koc University, Istanbul, Turkey; 4MD Anderson Cancer Center, Department of Radiation Oncology, The University of Texas, Houston, TX, USA
Correspondence: Yurday Ozdemir
Department of Radiation Oncology, Baskent University Medical Faculty, Adana 01120, Turkey
Tel +90 505 594 2169
Fax +90 322 344 4452
Email [email protected]
Purpose: To investigate the prognostic utility of the prognostic nutritional index (PNI) in stage IIIB non-small-cell lung carcinoma (NSCLC) patients undergoing concurrent chemoradiotherapy (CRT).
Methods: A total of 358 stage IIIB NSCLC patients who received a total dose of 60– 66 Gy (2 Gy/fraction) radiotherapy and ≥ 1 cycle(s) of platinum-based chemotherapy were analyzed. The receiver operating curve analysis was utilized to identify the optimal PNI cut-off value demonstrating a significant connection with the overall survival (OS), locoregional progression-free survival (LRPFS), and progression-free survival (PFS).
Results: At a median follow-up time of 22.5 months (range: 2.4– 123.5), 30.2% and 14% of the patients were still alive and free of disease progression, respectively.The median OS, LRPFS, and PFS were 25.2 [95% confidence interval (CI): 36.3– 46.6 months], 15.4 (95% CI: 26.6– 35.3 months), and 10.7 (95% CI: 36.8– 69.9 months), individually, for the whole study accomplice. The ROC analysis revealed an optimum rounded cut-off that associated meaningfully with each of the OS [area under the curve (AUC): 84.1%; sensitivity: 75.9%;72.4% specificity], LRPFS (AUC: 92.4%; sensitivity: 87.9%; 85.1% specificity), and PFS (AUC: 80.1%; sensitivity: 73.7%; 71.6% specificity) at a value of 40.5. Comparative analyses revealed that the patients presenting with PNI≤ 40.5 had significantly inferior OS (16.8 vs 36.7; P< 0.001), LRPFS (11.5 vs 19.5; P< 0.001), and PFS (8.6 vs 13.6; P< 0.001) outcomes compared to patients with PNI> 40.5. In univariate analyses, lower T-stage (1– 2 vs 3– 4; P< 0.001), lower N-stage (N2 vs N3; P< 0.001), anemia status (absent vs present; P< 0.001), weight loss status (< 5% vs ≥ 5%; P< 0.001), and PNI group (≤ 40.5 vs > 40.5; P< 0.001) were the factors found to be associated with OS, LRPFS and PFS results. The results of multivariate analysis exhibited that the PNI was independently associated with each of the OS (P< 0.001), LRPFS (P< 0.001), and PFS (P< 0.001) outcomes.
Conclusion: The pretreatment PNI appears to be a robust novel prognostic factor that stratifies patients with stage IIIB NSCLC into two significantly distinct survival groups after CRT.
Keywords: prognostic nutritional index, non-small-cell lung carcinoma, prognosis, chemoradiotherapy, survival results
Introduction
The standard of care in patients with unresectable stage III non-small-cell lung carcinoma (NSCLC) is chemoradiotherapy (CRT), which offers a 5-year overall survival (OS) rate of only 16%.1,2 Despite the fact that well-established conventional prognostic tools (ie, tumor-node-metastasis [TNM], histological subtype, and genetic biomarkers) may stratify patients into significantly distinct outcome groups, unexpected recurrences or CRT resistance can still occur, which are common obstacles for the treatment approach and confer a relatively worse prognosis contrasted to patients presenting with indistinguishable TNM stages.3,4 Moreover, the high cost and inconvenience of reliable genetic biomarker detection restrict the use of customized treatments based on such genetic biomarkers, especially in countries with limited incomes.4 These limitations may cause difficulties in predicting treatment responses, which can lead to insufficient disease management (eg, using less aggressive forms of therapy) or over-treatment, resulting in either treatment failure or treatment-related toxicity, respectively.5 Therefore, novel practical prognostic tools with a lower cost are required to anticipate host treatment responses and improve patient selection for customized therapies in a more accurate manner.6–9
Notwithstanding the conventional prognostic variables, systemic inflammation has been deemed to be a crucial ingredient of the tumor microenvironment that plays remarkable roles in tumor growth, progression, and metastasis steps.10 Several inflammation-based biomarkers including C-reactive protein and albumin are likewise respected as the reliable indicators of the host immune-nutritional status which might be utilized to predict the prognosis for various malignancies during chemotherapy, CRT, or the postoperative period.11–13 The prognostic nutritional index (PNI), calculated by joining the serum albumin levels and serum lymphocyte count was first introduced as an indicator of postoperative complications after gastrointestinal surgery, and therefore, was reported to link with survival outcomes and immune-nutritional status in several cancer types.14–17 The PNI assuredly evaluates the potential impact of the blend of hypoalbuminemia and lymphocytopenia. Hypoalbuminemia does not merely symbolize a status of nutritional deprivation but also indicates an increased systemic inflammation status, which is almost perpetually associated with elevated C-reactive protein levels. Lymphocytes are the critical cellular members of the immune and inflammation systems which possess vital local and systemic immune/inflammation functions. In this respect, lymphocytopenia indicates a markedly depressed inflammatory immune response and resultant poor disease prognosis.18,19 Even though the value of PNI has been assessed in various stages of NSCLC previously, to our best knowledge, the strength of PNI has never been studied before in a homogenous patient group comprised only of stage IIIB NSCLC patients undergoing definitive CRT. For this reason, we herein aimed to objectively evaluate the prognostic significance of PNI for patients with stage IIIB-NSCLC who underwent CRT.
Materials and Methods
Patient Selection
Patients meeting the following inclusion criteria were retrospectively analyzed: 1) histologically confirmed to have adeno- or squamous cell carcinoma; 2) clinical stage IIIB according to the seventh TNM classification of lung cancer; 3) Eastern Cooperative Oncology Group (ECOG) performance status score of 0–1; 4) body-mass index with ≥20.0 kg/m2; 5) no history of other cancers; 6) no previous history of radiotherapy or chemotherapy; 7) available electronic patient data; 8) available pretreatment blood tests, including albumin and lymphocyte counts collected within two weeks of CRT; 9) available chest computerized tomography and fluorodeoxyglucose-positron emission/computed tomography (FDG-PET/CT) scans; and 9) no evidence of brain metastasis on magnetic resonance imaging acquired within one month of the treatment. Patients who received induction chemotherapy or immunotherapy at any disease stage were excluded from the analysis.
Ethics, Consent and Permissions
The design of the present study was approved by the institutional review board of Baskent University Medical Faculty before acquisition of any patient data. All patients provided written informed consent before the commencement of treatment either themselves or legally authorized representatives for collection and analysis of blood samples, pathologic specimens, and publication of their results.
Concurrent CRT
Target volumes were determined according to the co-registered planning computed tomography and FDG-PET/CT scans. Treatment techniques have been reported elsewhere.20 Briefly, all patients received 60–66 Gy in 30–33 fractions for 5 days per week concurrently with 1–3 cycles of cisplatin (80 mg/m2) combined with either of docetaxel: CD combination) or vinorelbine (30 mg/m2, D1, 8: CV combination). Elective nodal irradiation was not performed.
Prognostic Nutritional Index (PNI)
PNI was calculated as follows: 10× albumin concentration (g/dL) + 0.005 × total lymphocyte counts (per mm3) of peripheral blood.14 Blood samples were obtained at a maximum period of 2 weeks before CRT due to the half-lives of albumin (≈21 days) and lymphocytes (>2 weeks).21
Toxicity and Treatment Response Assessments
During CRT, patients were examined weekly for toxicity. Acute (≤90 days after CRT) and late (>90 days) toxicities were assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) v3. Post-CRT follow-up was performed every three months for the first two years post-treatment and then every six months or more often thereafter.
The first treatment response, as assessed by FDG-PET/CT, was compared to pre-CRT scans at the 12-week follow-up visit. In the case of progression or relapse, this was repeated for the subsequent chest computed tomography or abdominal ultrasound scans. Treatment response was based on EORTC-1999 guidelines and the PET Response Criteria in Solid Tumors (PERCIST) after 2009.
Statistical Analysis
The primary outcome was the clinical influence of pre-CRT PNI values on OS. The cut-off value for PNI, which may correlate with survival outcomes, was identified using a receiver operating characteristic22 curve. Secondary end-point included the relation between pre-CRT PNI values and locoregional progression-free survival (LRPFS) and progression-free survival (PFS). The intervals between the first day of CRT and the related endpoints, including the date of recurrence/progression, death, or last follow-up, were used to calculate survival times. Medians and ranges were utilized for continuous variables, while frequency distributions were used for categorical variables. Frequency distributions were compared using Chi-square tests, Student’s t-tests, Pearson’s X2, and Spearman correlations. The influence of potential risk factors on OS, LRPFS, and PFS was assessed with Kaplan-Meier curves and Log rank tests. Multivariate analysis was utilized to identify independent prognostic variables with a stepwise Cox proportional hazards regression model. P < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 358 patients with stage IIIB-NSCLC were included. Baseline clinicopathological patient characteristics for the entire study population and per PNI group are summarized in Table 1. The median age of patients was 61 years (range: 29–80 years), and 66.5% of the patients were male. All patients had an ECOG performance status of 0–1, and approximately half of the cohort (50.5%) had basal weight loss > 5%. Furthermore, approximately half of the patients (n = 188; 52.5%) had adenocarcinoma, while 180 (47.5%) had squamous cell carcinoma.
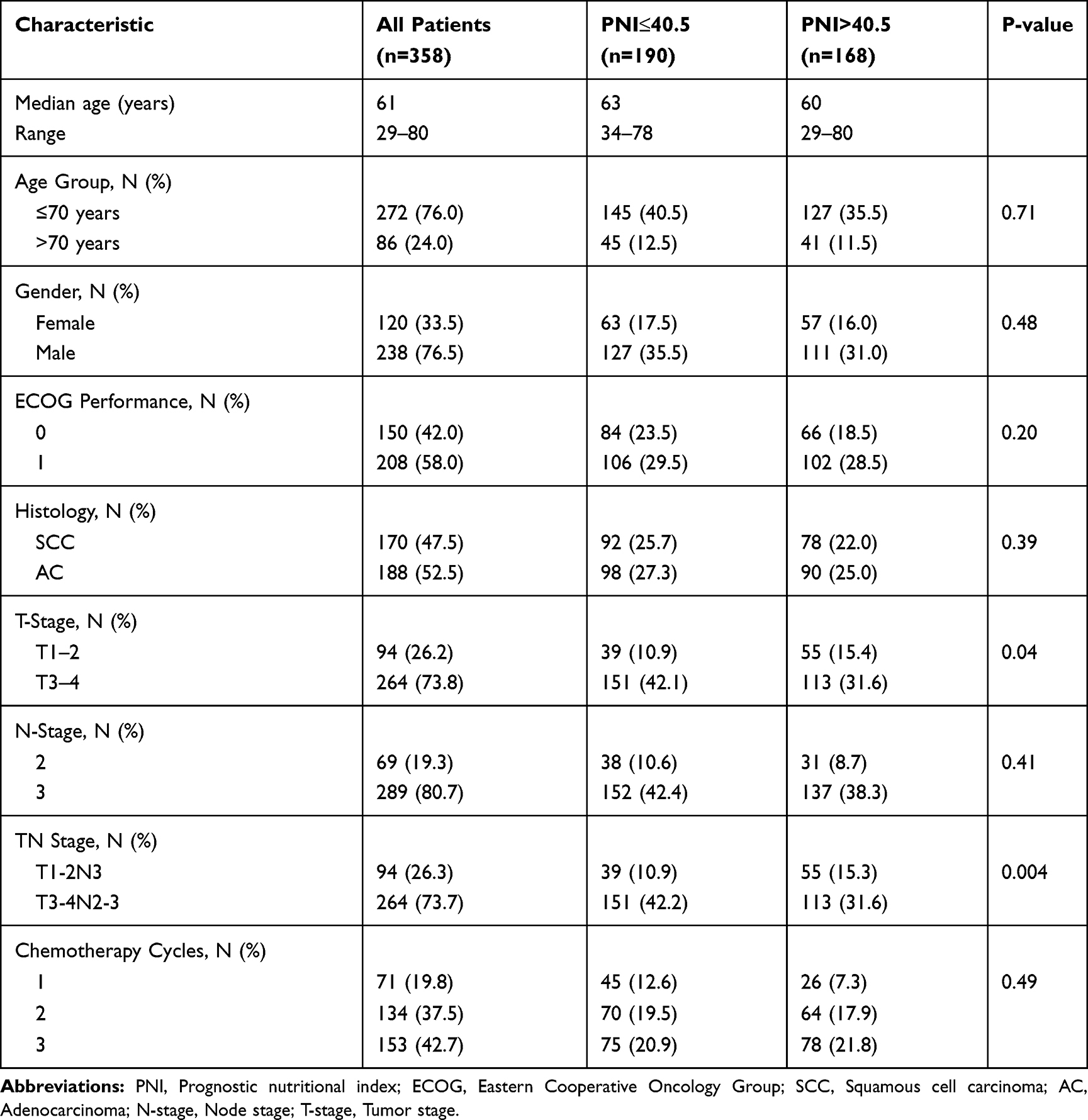 |
Table 1 Baseline Characteristics of Patients According to PNI |
Selection of Cut-off Values for PNI
ROC analysis was used to determine a cut-off value for PNI that was linked with survival outcomes. This yielded optimal cut-off values of 40.5, 40.3, and 40.6 for OS (area under the curve [AUC]: 84.1%, sensitivity: 75.9%, specificity: 72.4%), LRPFS (AUC: 92.4%, sensitivity: 87.9%, specificity: 85.1%), and PFS (AUC: 80.1%, sensitivity: 73.7%, specificity: 71.6%), respectively (Figure 1). Because the three values were nearly identical, a common cut-off value of 40.5 was used for further analyses. Therefore, patients were categorized into two groups defined as PNI > 40.5 or ≤ 40.5, which described 190 (53%) and 168 (47%) patients, respectively.
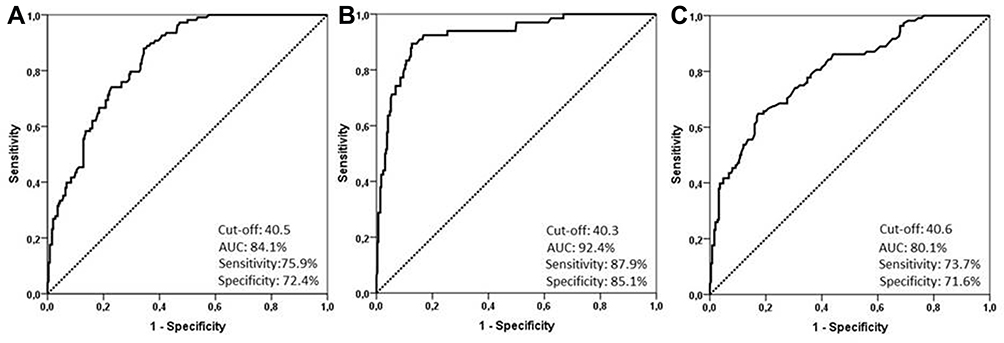 |
Figure 1 Receiver operating characteristic curve analysis for the optimal cut-off value of PNI. (A) overall-survival, (B) locoregional progression-free survival, (C) progression-free survival. |
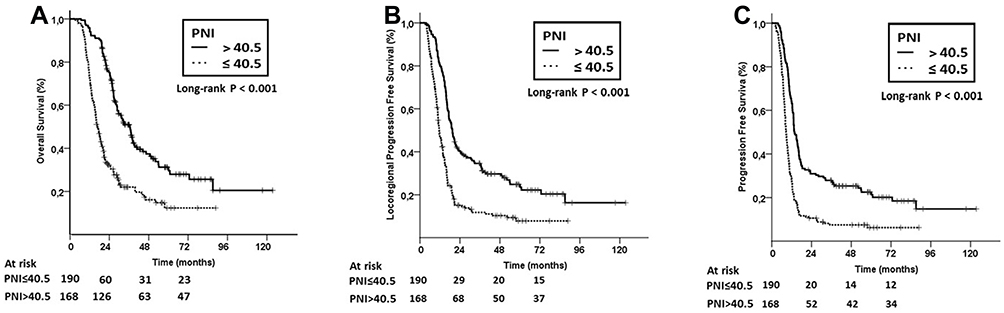 |
Figure 2 Survival outcomes according to PNI. (A) Overall survival; (B) Locoregional progression-free survival, (C) Progression-free survival. |
Association of PNI with Clinicopathological Characteristics
The distributions of patient demographics based on PNI level are shown in Table 1. Patients in the PNI ≤ 40.5 group were more likely to have higher T (T3–4 vs T1–2; P = 0.001) and TN (T1-2N3 vs T3-4 N2; P = 0.004) stages.
PNI and Survival Outcomes
The median follow-up time was 22.5 months (range: 2.4–123.5). During the final analysis, 108 patients (30.2%) were alive and 14% (n = 50) were free of disease progression. For the entire population, the estimated median OS, LRPFS, and PFS were 25.2 (95% confidence interval [CI]: 36.3–46.6), 15.4 (95% CI: 26.6–35.3), and 10.7 months (95% CI: 36.8–69.9), respectively. Importantly, PNI-based stratification demonstrated that patients with PNI ≤ 40.5 had significantly lower median OS (16.8 vs 36.7; P < 0.001), LRPFS (11.5 vs 19.5; P < 0.001), and DFS (8.6 vs 13.6; P < 0.001) relative to the higher PNI group (Table 2, Figure 2). This corresponded to 5-year OS, LRPFS, and PFS rates of 12.3% vs 31.3%, 7.8% vs 24.8%, and 6.2% vs 22.5%, respectively.
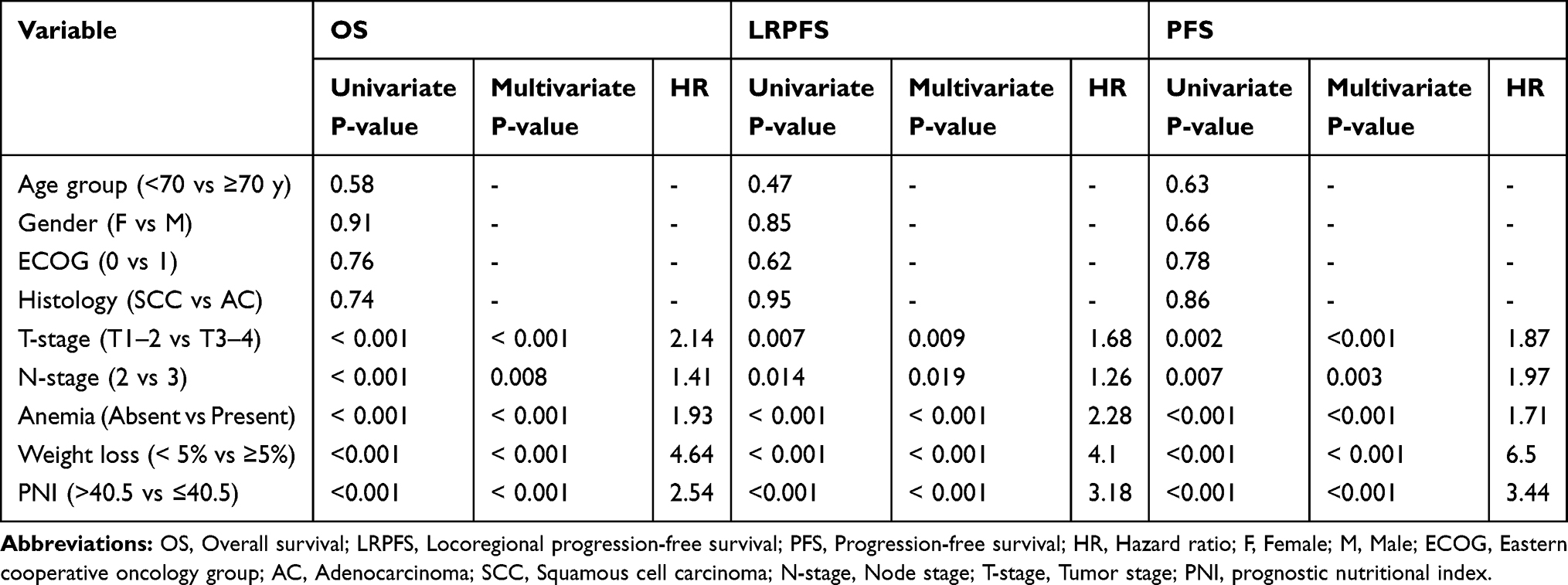 |
Table 2 Outcomes of Univariate and Multivariate Analyses |
Prognostic Analysis of Parameters
Univariate analysis revealed that lower OS rates were significantly associated with higher T stage (T3–4 vs T1–2; P <0.001), higher N stages (N3 vs N2; P =0.004) and lower PNI (<40.5 vs ≥40.5; P<0.001), which altogether retained their independent significance in multivariate analysis (Table 2).
Discussion
The results of the present study uncovered that pre-treatment PNI is an independent novel prognostic tool that efficiently laminates stage IIIB NSCLC patients into two distinct prognostic groups following definitive CRT. Particularly, PNI ≤ 40.5 was linked with lower median OS (16.8 vs 36.7 months; P<0.001), LRPFS (11.5 vs 19.5; P<0.001), and PFS (8.6 vs 13.6; P<0.001) outcomes compared to PNI > 40.5 counterpart.
A growing body of evidence proposes that basic nutritional status and systemic inflammation, the key determinants of host status and distinctive features of cancer progression and metastasis are connected with the long-term prognosis of cancer patients.23–25 Importantly, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and concentration of C-reactive protein are some of the indices that can be employed to monitor this concept.6,26 Another immune-nutritional biomarker is PNI, which consolidates absolute lymphocyte count and albumin. Importantly, following a milestone study by Onodera et al, further investigations disclosed that PNI is associated with survival outcomes in various malignancies.4,14-17,27–30 Critically, while past examinations have meticulously researched the relationship among the PNI and NSCLC, these studies used eligibility criteria that included patients with a considerable degree of heterogeneity in terms of disease stage, histological subtypes and treatments.31–33 Such non-uniformities restrict the judicial interpretation of the actual prognostic worth of PNI in this patient population.4 Therefore, we investigated the prognostic ability of PNI in a relatively homogeneous group comprised exclusively of stage IIIB NSCLC patients treated with exclusive CRT.
Our most noticeable finding was the noteworthy relationship between PNI ≤ 40.5 and poor median OS (16.8 vs 36.7 months; P < 0.001) relative to patients with PNI > 40.5. Albeit different PNI cut-off values have been reported previously for NSCLC patients, again these studies were restrained by heterogeneous patient attributes which hindered the ability to reveal the precise relationship between the specified PNI cut-offs and survival outcomes.34,35 For instance, Kos et al reported that the mean OS for patients with PNI < 49.5 and ≥ 49.5 were 7 and 33 months in a sum of 138 NSCLC patients, respectively.34 Nonetheless, patients were categorized according to the median cut-off value rather than on a more reliable statistical tool, such as the ROC curve analysis. Moreover, the study population included patients with heterogeneous disease stages ranging from stage I to IV, and only 15% of them received CRT as the primary treatment. In another study incorporating 144 patients with epidermal growth factor receptor (EGFR) mutations who were treated with EGFR tyrosine kinase inhibitors, PNI < 48.78 was significantly associated with poor survival rates, increased systemic inflammation, and ominous clinical outcomes.35 By marked contrast, our study population was comparatively more homogenous both in terms of disease stage and treatment modality, whereby only a single CRT protocol with identical radiotherapy doses was used. Additionally, the use of PET/CT for staging and radiotherapy planning may have afforded more accurate patient stratification in terms of staging and the ideal choice of the initial definitive therapy as either CRT or induction chemotherapy.
Like the results for OS, patients with PNI ≤ 40.5 also had significantly lower PFS (8.6 vs 13.6 months; P< 0.001) and LRPFS (11.5 vs 19.5 months; P< 0.001) rates relative to patients with PNI > 40.5. Although the definite reason for this link remains obscure, these data indicate that PNI can be used to identify the patients who are more likely to develop metastasis and loco-regional recurrences. Therefore, PNI might be a useful tool for this patient population. Formerly, a study involving surgically treated NSCLC patients reported a significant correlation between low PNI and larger tumor size concerning the tumor aggressiveness and therefore, more frequent relapses.33 While patients are commonly stratified based on TNM staging as a measure of disease extent, this strategy is constrained by the fact that TNM-7 staging includes a retrospective database that lacks the validity of existing T stages and does not consolidate PET/CT as a functional staging tool.36 Although our present analysis was performed on a relatively homogeneous cohort that, according to the AJCC-7 criteria, only included stage IIIB patients, the demonstration of significantly distinct outcomes between the PNI-stratified groups emphatically features the prescient viability of factors beyond the classic TNM conventions, including the immune-nutritional marker PNI.
The ability to accurately stratify patients with comparative prognosis to customize treatment strategies without a doubt relies upon objective and accurate prognostic tools.36 Accordingly, accessible previous literature and the current data altogether indicate that PNI has robust prognostic utility.4 Although the underlying exact mechanism remains unclear, two ingredients of PNI, namely albumin and absolute lymphocyte count37 are well-recognized measures of nutrition, immunity, and systemic inflammation.27 On the other hand, based on the equation used to calculate PNI (10 × albumin + 0.005 × ALC); the resultant score is affected basically by the albumin levels, rather than the ALC. Nevertheless, considering the immune and nutritional features of albumin, this does not lessen the prognostic quality of PNI with regards to the systemic immunity. Thus, reduced albumin levels ought to be considered not only for the corresponding effect of increased catabolism but also as a reflection of increased systemic inflammation, which is consequently associated with poor survival outcomes.38
As an intriguing issue of current oncologic practice, integration of various immunotherapeutics such as immune checkpoint inhibitors to the radiotherapy is proved to remodel the tumor microenvironment and enhance the presentation of neoantigens, upregulation of tumoral programmed death ligand-1 (PD-L1) and major histocompatibility complex class 1 (MHC-C1) expression.39–41 Recently, durvalumab, a selective IgG1 monoclonal antibody which blocks PD-L1 binding to PD-1 and CD-80 allowing T cells to recognize and kill tumor cells, has been approved as the adjuvant standard of care after CRT with Level 1 proof for treatment of unresectable NSCLC.42 To our best information, to date, no study particularly addressed the prognostic significance of PNI in NSCLC patients treated with the standard CRT followed by durvalumab or other immunotherapeutics. Nevertheless, neutrophil to lymphocyte ratio which is another inflammation index has been addressed as a prognostic indicator in some limited studies,43–45 and a meta-analysis.46 Reputably, Jiang et al conducted a comprehensive meta-analysis literature search to assess the relationship between pretreatment neutrophil to lymphocyte ratio and OS or PFS in advanced-stage cancer patients treated with immunotherapy.The pooled results of this meta-analysis of 27 studies with 4647 patients unveiled that high pretreatment neutrophil to lymphocyte ratio was closely linked with significantly shorter OS (HR = 1.98; P < 0.001) and PFS (HR = 1.78; P < 0.001). In sub-group analyses, results confined to the advanced NSCLCs demonstrated that high pretreatment neutrophil to lymphocyte ratio was robustly connected with meaningfully shorter OS (HR = 2.07; P < 0.001) and PFS (HR = 1.50; P = 0.005) in this specific patients’ group as well.Albeit our study population included patients with conventional chemotherapy regimens, because the albumin and lymphocyte counts are closely associated with the patients’ nutritional, inflammation, and immune status at any time point, it appears rational to anticipate that PNI may likewise assist useful in locally advanced NSCLC patients undergoing standard CRT followed by the adjuvant immunotherapy. However, the potential prognostic worth of PNI in this particular treatment strategy needs to be carefully investigated to achieve concluding remarks on this interesting issue of foremost significance.
This study had several strengths like the embodiment of a relatively large population with the exclusive histological subtypes of adenocarcinoma and squamous cell carcinoma. Second, PET/CT for staging and treatment response assessment was performed consistently for the whole cohort. Third, the exclusion of patients with induction chemotherapy may have limited the unforeseeable potential inclinations. Alternatively, our study had some impediments as a retrospective and a single-institutional cohort. First, other medical conditions, including infection, non-malignant inflammation, drugs, and patient stress, are eccentric factors that may have influenced the levels of albumin and leucocytes. Second, the lack of molecular characterization may introduce some potential bias regarding the improved survival rates in patients with epidermal growth factor receptor mutation, anaplastic lymphoma kinase, and programmed cell death-1/programmed cell death ligand-1. Third, considering the dynamic pattern of PNI, not only the baseline PNI, but also the impact of the PNI changes between the CRT and post-CRT periods, may likewise have altered the results presented here. However, this issue has been investigated in a group of 261 patients with locally advanced rectal cancer, where the patients were stratified arbitrarily into three groups according to the PNI difference (dPNI) between the neo-adjuvant CRT and pre-surgical measurements: dPNI < 5; dPNI of 5–10 and dPNI > 10; the dPNI was found to be firmly linked with survival outcomes.47 Finally, our results ought not to be generalized to all stage IIIB NSCLC patients as they are restricted to a highly selected patients group with ECOG scores of 0–1, <80 years of age and BMI≥20 kg/m2.
Conclusions
To our knowledge, this study is the first to demonstrate the efficacy of PNI in predicting survival outcomes in patients with stage IIIB NSCLC undergoing definitive CRT. Accordingly, our results demonstrated that the pre-treatment PNI is an independent novel prognostic tool that efficiently stratifies stage IIIB NSCLC patients into two distinct prognostic groups at the PNI ≤ 40.5 value following definitive CRT with regards to the OS, LRPFS, and PFS outcomes.
Data Sharing Statement
Data is owned and saved by Baskent University Medical Faculty and are available from the Baskent University Institutional Data Access/Ethics Committee (contact via Baskent University Ethics Committee) for researchers meeting the criteria for access to confidential data: contact address, [email protected].
Ethics and Consent Statement
The design of the present study was approved by the institutional review board of Baskent University Medical Faculty before acquisition of any patient data. All patients provided written informed consent before the commencement of treatment either themselves or legally authorized representatives for collection and analysis of blood samples, pathologic specimens, and publication of their results.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no funding and no conflicts of interest in this work.
References
1. Furuse K, Fukuoka M, Kawahara M, et al. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. J Clin Oncol. 1999;17(9):2692–2699. doi:10.1200/JCO.1999.17.9.2692
2. Curran WJ
3. Tong YS, Tan J, Zhou XL, et al. Systemic immune-inflammation index predicting chemoradiation resistance and poor outcome in patients with stage III non-small cell lung cancer. J Transl Med. 2017;15(1):221. doi:10.1186/s12967-017-1326-1
4. Wang Z, Wang Y, Zhang X, Zhang T. Pretreatment prognostic nutritional index as a prognostic factor in lung cancer: review and meta-analysis. Clin Chim Acta. 2018;486:303–310. doi:10.1016/j.cca.2018.08.030
5. Oh IJ, Ahn SJ. Multidisciplinary team approach for the management of patients with locally advanced non-small cell lung cancer: searching the evidence to guide the decision. Radiat Oncol J. 2017;35(1):16–24. doi:10.3857/roj.2017.00108
6. Roxburgh CS, McMillan DC. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010;6(1):149–163. doi:10.2217/fon.09.136
7. Paramanathan A, Saxena A, Morris DL. A systematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumours. Surg Oncol. 2014;23(1):31–39. doi:10.1016/j.suronc.2013.12.001
8. Berry MF, Hanna J, Tong BC, et al. Risk factors for morbidity after lobectomy for lung cancer in elderly patients. Ann Thorac Surg. 2009;88(4):1093–1099. doi:10.1016/j.athoracsur.2009.06.012
9. Shiono S, Abiko M, Sato T. Postoperative complications in elderly patients after lung cancer surgery. Interact Cardiovasc Thorac Surg. 2013;16(6):819–823. doi:10.1093/icvts/ivt034
10. Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357(9255):539–545. doi:10.1016/S0140-6736(00)04046-0
11. Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;21(2):137–148. doi:10.1016/j.immuni.2004.07.017
12. Kostner AH, Kersten C, Lowenmark T, et al. The prognostic role of systemic inflammation in patients undergoing resection of colorectal liver metastases: C-reactive protein (CRP) is a strong negative prognostic biomarker. J Surg Oncol. 2016;114(7):895–899. doi:10.1002/jso.24415
13. Arrieta O, Michel Ortega RM, Villanueva-Rodriguez G, et al. Association of nutritional status and serum albumin levels with development of toxicity in patients with advanced non-small cell lung cancer treated with paclitaxel-cisplatin chemotherapy: a prospective study. BMC Cancer. 2010;10(1):50. doi:10.1186/1471-2407-10-50
14. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005. Japanese.
15. Nozoe T, Ninomiya M, Maeda T, et al. Prognostic nutritional index: a tool to predict the biological aggressiveness of gastric carcinoma. Surg Today. 2010;40(5):440–443. doi:10.1007/s00595-009-4065-y
16. Feng JF, Chen QX. Significance of the prognostic nutritional index in patients with esophageal squamous cell carcinoma. Ther Clin Risk Manag. 2014;10:1–7. doi:10.2147/TCRM.S56159
17. Mohri Y, Inoue Y, Tanaka K, et al. Prognostic nutritional index predicts postoperative outcome in colorectal cancer. World J Surg. 2013;37(11):2688–2692. doi:10.1007/s00268-013-2156-9
18. Rosenberg SA. Progress in human tumour immunology and immunotherapy. Nature. 2001;411(6835):380–384. doi:10.1038/35077246
19. d’Engremont C, Vernerey D, Pointet AL, et al. Additive value of pre-operative and one-month post-operative lymphocyte count for death-risk stratification in patients with resectable pancreatic cancer: a multicentric study. BMC Cancer. 2016;16(1):823. doi:10.1186/s12885-016-2860-6
20. Topkan E, Parlak C, Selek U. Impact of weight change during the course of concurrent chemoradiation therapy on outcomes in stage IIIB non-small cell lung cancer patients: retrospective analysis of 425 patients. Int J Radiat Oncol Biol Phys. 2013;87(4):697–704. doi:10.1016/j.ijrobp.2013.07.033
21. Fulcher DA, Basten A. B cell life span: a review. Immunol Cell Biol. 1997;75(5):446–455. doi:10.1038/icb.1997.69
22. Li B, Li D, Lau DH, et al. Clinical-dosimetric analysis of measures of dysphagia including gastrostomy-tube dependence among head and neck cancer patients treated definitively by intensity-modulated radiotherapy with concurrent chemotherapy. Radiat Oncol. 2009;4(1):52. doi:10.1186/1748-717X-4-52
23. Schwegler I, von Holzen A, Gutzwiller JP, et al. Nutritional risk is a clinical predictor of postoperative mortality and morbidity in surgery for colorectal cancer. Br J Surg. 2010;97(1):92–97. doi:10.1002/bjs.6805
24. Stotz M, Pichler M, Absenger G, et al. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br J Cancer. 2014;110(2):435–440. doi:10.1038/bjc.2013.785
25. Hubbard TJ, Lawson-McLean A, Fearon KC. Nutritional predictors of postoperative outcome in pancreatic cancer (Br J Surg 2011; 98: 268–274). Br J Surg. 2011;98(7):1032. (). doi:10.1002/bjs.v98.7
26. Qi Q, Geng Y, Sun M, et al. Clinical implications of systemic inflammatory response markers as independent prognostic factors for advanced pancreatic cancer. Pancreatology. 2015;15(2):145–150. doi:10.1016/j.pan.2014.12.004
27. Saito H, Kono Y, Murakami Y, et al. Influence of prognostic nutritional index and tumor markers on survival in gastric cancer surgery patients. Langenbecks Arch Surg. 2017;402(3):501–507. doi:10.1007/s00423-017-1572-y
28. Nakatani M, Migita K, Matsumoto S, et al. Prognostic significance of the prognostic nutritional index in esophageal cancer patients undergoing neoadjuvant chemotherapy. Dis Esophagus. 2017;30(8):1–7. doi:10.1093/dote/dox020
29. Zhang W, Ye B, Liang W, Ren Y. Preoperative prognostic nutritional index is a powerful predictor of prognosis in patients with stage III ovarian cancer. Sci Rep. 2017;7(1):9548. doi:10.1038/s41598-017-10328-8
30. Geng Y, Qi Q, Sun M, et al. Prognostic nutritional index predicts survival and correlates with systemic inflammatory response in advanced pancreatic cancer. Eur J Surg Oncol. 2015;41(11):1508–1514. doi:10.1016/j.ejso.2015.07.022
31. Go SI, Jeon H, Park SW, et al. Low pre-treatment nutritional index is significantly related to poor outcomes in small cell lung cancer. Thorac Cancer. 2018;9(11):1483–1491. doi:10.1111/tca.2018.9.issue-11
32. Jin S, Cao S, Xu S, et al. Clinical impact of pretreatment prognostic nutritional index (PNI) in small cell lung cancer patients treated with platinum-based chemotherapy. Clin Respir J. 2018;12(9):2433–2440. doi:10.1111/crj.2018.12.issue-9
33. Okada S, Shimada J, Kato D, et al. Clinical significance of prognostic nutritional index after surgical treatment in lung cancer. Ann Thorac Surg. 2017;104(1):296–302. doi:10.1016/j.athoracsur.2017.01.085
34. Kos FT, Hocazade C, Kos M, et al. Assessment of prognostic value of “neutrophil to lymphocyte ratio” and “prognostic nutritional index” as a systemic inflammatory marker in non-small cell lung cancer. Asian Pac J Cancer Prev. 2015;16(9):3997–4002. doi:10.7314/APJCP.2015.16.9.3997
35. Sheng J, Yang YP, Ma YX, et al. Low prognostic nutritional index correlates with worse survival in patients with advanced NSCLC following EGFR-TKIs. PLoS One. 2016;11(1):e0147226. doi:10.1371/journal.pone.0147226
36. Vlahos I. Dilemmas in lung cancer staging. Radiol Clin North Am. 2018;56(3):419–435. doi:10.1016/j.rcl.2018.01.010
37. Zumsteg ZS, Riaz N, Jaffery S, et al. Carotid sparing intensity-modulated radiation therapy achieves comparable locoregional control to conventional radiotherapy in T1-2N0 laryngeal carcinoma. Oral Oncol. 2015;51(7):716–723. doi:10.1016/j.oraloncology.2015.02.003
38. Miura K, Hamanaka K, Koizumi T, et al. Clinical significance of preoperative serum albumin level for prognosis in surgically resected patients with non-small cell lung cancer: comparative study of normal lung, emphysema, and pulmonary fibrosis. Lung Cancer. 2017;111:88–95. doi:10.1016/j.lungcan.2017.07.003
39. Filippi AR, Di Muzio J, Badellino S, et al. Locally-advanced non-small cell lung cancer: shall immunotherapy be a new chance? J Thorac Dis. 2018;10(S13):S1461–S1467. doi:10.21037/jtd
40. Ko EC, Raben D, Formenti SC. The integration of radiotherapy with immunotherapy for the treatment of non-small cell lung cancer. Clin Cancer Res. 2018;24(23):5792–5806. doi:10.1158/1078-0432.CCR-17-3620
41. Kordbacheh T, Honeychurch J, Blackhall F, et al. Radiotherapy and anti-PD-1/PD-L1 combinations in lung cancer: building better translational research platforms. Ann Oncol. 2018;29(2):301–310. doi:10.1093/annonc/mdx790
42. Fukui T, Hosotani S, Soda I, et al. Current status and progress of concurrent chemoradiotherapy in patients with locally advanced non-small cell lung cancer prior to the approval of durvalumab. Thorac Cancer. 2020. doi:10.1111/1759-7714.13357
43. Sacdalan DB, Lucero JA, Sacdalan DL. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: a review and meta-analysis. Onco Targets Ther. 2018;11:955–965. doi:10.2147/OTT
44. Dusselier M, Deluche E, Delacourt N, et al. Neutrophil-to-lymphocyte ratio evolution is an independent predictor of early progression of second-line nivolumab-treated patients with advanced non-small-cell lung cancers. PLoS One. 2019;14(7):e0219060. doi:10.1371/journal.pone.0219060
45. Russo A, Franchina T, Ricciardi GRR, et al. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with Nivolumab or Docetaxel. J Cell Physiol. 2018;233:6337–6343. doi:10.1002/jcp.26609
46. Jiang T, Qiao M, Zhao C, et al. Pretreatment neutrophil-to-lymphocyte ratio is associated with outcome of advanced-stage cancer patients treated with immunotherapy: a meta-analysis. Cancer Immunol Immunother. 2018;67(5):713–727. doi:10.1007/s00262-018-2126-z
47. Lee YJ, Kim WR, Han J, et al. Prognostic impact of immunonutritional status changes during preoperative chemoradiation in patients with rectal cancer. Ann Coloproctol. 2016;32(6):208–214. doi:10.3393/ac.2016.32.6.208
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.