")
Back to Journals » Clinical Epidemiology » Volume 12
Low Incidence of Maternal Near-Miss in Zhejiang, a Developed Chinese Province: A Cross-Sectional Study Using the WHO Approach
Authors Ma Y, Zhang L , Wang X, Qiu L, Hesketh T, Wang X
Received 23 December 2019
Accepted for publication 1 April 2020
Published 29 April 2020 Volume 2020:12 Pages 405—414
DOI https://doi.org/10.2147/CLEP.S243414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
YuanYing Ma,1 LiSan Zhang,2 Xian Wang,3 Liqian Qiu,1 Therese Hesketh,4,5 Xinyu Wang6
1Department of Women’s Healthcare, Women’s Hospital, Zhejiang University School of Medicine, Zhejiang Province, People’s Republic of China; 2Department of Neurology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Zhejiang Province, People’s Republic of China; 3Department of Big Data Analysis, Hangzhou Maicim Medical Technology Co., Ltd, Zhejiang Province, People’s Republic of China; 4Centre for Global Health, Zhejiang University, Zhejiang Province, People’s Republic of China; 5Institute for Global Health, University College London; London, UK; 6Department of Obstetrics and Gynaecology, Women’s Hospital, Zhejiang University School of Medicine, People’s Republic of China
Correspondence: Xinyu Wang; Therese Hesketh Email [email protected]; [email protected]
Background and Aim: Maternal near-miss (MNM) surveillance has been developed to identify severe complications in pregnancy since 2011 in China. However, very little is known about MNM in China. This study aims to explore the prevalence of MNM, the risk factors, and perinatal outcomes using the WHO near-miss approach in a developed Chinese province.
Materials and Methods: We used data from China’s National Maternity Near Miss Obstetrics Surveillance System for the period 2012 to 2017, which included 18 hospitals in Zhejiang Province. Chi-squared tests were used to compare the socio-demographic factors, obstetric complications and perinatal outcomes between women with and without MNM. Logistic regression was used to examine the independent risk factors for MNM.
Results: A total of 612,264 pregnant women were recruited. There were 3208 MNM cases and 34 maternal deaths. The MNM incidence ratio was low at 5.9 per 1,000 live births, with an MNM mortality ratio of 98:1 and mortality index of 1.1%. Among 3208 women with MNM, postpartum hemorrhage was the commonest cause at 76.3% followed by severe anemia at 23.7% and placenta previa at 23.0%. Embolism was identified as having the highest risk for MNM (AOR 46.0; 95% CI 19.1– 110.7), followed by postpartum hemorrhage (AOR 41.0; 95% CI 35.7– 47.0), and severe anemia (AOR 36.6; 95% CI 16.0– 84.1). MNM cases were significantly associated with severe perinatal outcome, including premature birth, low birth weight, multiple fetuses, stillbirth rates and neonatal mortality.
Conclusion: Overall near-miss indicators suggested a relatively high quality of maternal health care in a developed province of China. The identified risk factors may be helpful in developing targeted interventions for improving maternal safety.
Keywords: maternal near-miss, adverse perinatal outcomes, clinical audit, high-risk pregnancy, pregnancy complication
Introduction
Maternal mortality in China has decreased dramatically over the past 20 years, and China is one of the few countries to have achieved Millennium Development Goal 5.1,2 The maternal mortality ratio decreased from 66 to 19.9 deaths per 100, 000 live births between 1996 and 2016. The reasons are multi-factorial, and include improvements in overall socio-economic conditions, expansion of rural health services, an effective referral system increases in overall health expenditure, universal health insurance coverage, and improvements in the maternal health workforce.3 In 1988, Zhejiang Province started to audit all maternal deaths through a maternal mortality surveillance system, to inform policy to reduce maternal mortality.4,5
Zhejiang Province is a prosperous province located on the east coast of China with a population of 54 million in 2016.6 The maternal mortality ratio decreased from 48.50 in 1988 to 5.73 per 100,000 in 2016 and is now lower than in the USA.7,8 Because maternal mortality is now rare it can no longer serve as a sensitive marker of the quality of services. Over the past decade the use of maternal near-miss studies, which examine cases of women who survived a severe complication in pregnancy, childbirth, or the postpartum period, are increasingly being recognized as more useful than studying maternal mortality in terms of assessing healthcare needs.9,10 Near-miss cases represent most of the characteristics of maternal deaths, but occur more often.11,12 In addition, auditing near-miss cases may be less threatening for the involved healthcare workers.13 WHO defined the concept of maternal near-miss (MNM) in 2009, as a means of monitoring and improving the quality of obstetric care. The WHO near-miss approach for maternal health was further developed in 201114 and validated for the evaluation of the quality of care for severe pregnancy complications. By monitoring the implementation of critical interventions in maternal health care, it provides a systematic mechanism for assessing the quality of care.15,16
The aims of this study are to explore the prevalence of MNM, examine the risk factors for MNM and explore the relationship between MNM and perinatal outcomes, in Zhejiang Province using WHO near-miss indicators.
Materials and Methods
We used the data for Zhejiang Province from China’s National Maternal Near-Miss Surveillance System (NMNMSS) for the period between Jan 1, 2012, and Dec 31, 2017. This system was established in October, 201017,18 using the WHO near-miss approach in 326 health facilities across all provinces in urban districts and rural counties.14 In Zhejiang 18 health facilities with more than 1000 deliveries per year, (out of a total of 85 eligible hospitals) were randomly sampled, stratified by region and urban or rural characteristics to ensure proportional representation of Zhejiang Province. They included 11 tertiary and 7 secondary hospitals, with 12 at county level, 4 municipal level, and 2 at provincial level. Detailed information about the data collection process has been reported elsewhere.17 In all 18 facilities, data were collected for all pregnant and post-partum women, who were admitted to obstetric departments with postpartum complications. Doctors and nurses in each facility were trained to collect data prospectively from admission to discharge using an especially designed data collection form for each woman. Data were collected for socio-demographic characteristics, obstetric history, place and method of delivery, pregnancy outcome, and complications during pregnancy, delivery, or postpartum. Definitions were those outlined in the surveillance manual and the definition of MNM complied with WHO standards.14,18 Data were entered into a web-based data management system, which was centralized at the National Office for Maternal and Child Health (MCH) Surveillance of China. Quality assurance was ensured by county-level, municipal, and provincial MCH hospital staff who visited all of the selected facilities at least once a year. The National Office for Maternal and Child Health Surveillance also visited a random sample of six to eight hospitals in each province once a year to verify the quality of the records. Hospitals were asked to re-examine all of the data if errors exceeded a predefined standard (eg, obstetric complications if underreported by more than 5%, maternal deaths if under-reported by more than 1%, and MNM if underreported by more than 5%). No hospitals in Zhejiang exceeded the predefined standard. MNM were underreported by 2% in Beijing, 6% in Hubei, and 4% in Shanxi which all were asked to re-examine all of the data for 2014.17 Chi-squared tests were used to compare the socio-demographic factors, obstetric complications and perinatal outcomes between women with and without MNM. Logistic regression was used to examine the independent risk factors for MNM. R version 3.4.1 was used for statistical analysis.
Definitions
Maternal Death (MD)
A woman died during pregnancy, childbirth or within 42 days of termination of pregnancy.
MNM
A woman who nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy. WHO defined the criteria by identifying markers for organ system dysfunction.14
Maternal Complication19
Maternal complications were divided into two categories: direct obstetric complications and medical diseases. Direct obstetric complications included uterine rupture, placenta praevia, abruptio placentae, unspecified antepartum hemorrhage, pre-eclampsia, eclampsia, HELLP syndrome, or any fetal malpresentation. Medical diseases included heart disease, embolism/thrombophlebitis, liver disease, anaemia (haemoglobin <110 g/l), renal disease (including urinary tract infection), lung disease (including respiratory tract infection), HIV/AIDS, connective tissue disorders, gestational diabetes and cancer.
Severe Maternal Outcome Ratio (SMOR)
The number of women with life-threatening conditions (MNM + MD) per 1000 live births (LB).
Mortality Index
Mortality index refers to the number of maternal deaths divided by the number of women with life-threatening conditions expressed as a percentage [MI = MD/(MNM + MD)]. The higher the index the more women with life-threatening conditions die (low quality of care), whereas the lower the index the fewer women with life-threatening conditions die (better quality of care).
Results
There were 612,264 pregnant women recruited by the MNM surveillance system across the 18 health facilities in Zhejiang Province from 2012 to 2017. There were 543,109 live births which represented 19.7% of the total live births in Zhejiang Province. Of these 45.9% delivered in provincial and municipal hospitals, with 47.4% delivering in county hospital. A very small number of 689 (0.2%) delivered in a township hospital (where there are very limited or no obstetric services) or at home, and were recruited in county or higher level hospitals after delivery. Of the total 388, 667 (63.5%) women had some kind of obstetrics complication (mostly anemia). Of these 42,501 (6.9%) had potentially life-threatening disorders, 3208 (0.5%) MNM and there were 34 maternal deaths (maternal mortality 5.6/105) (See Figure 1). The near-miss indicator showed an SMO ratio of 6.0 per 1000 live births, an MNM incidence ratio of 5.9 per 1000 live births and a mortality index of 1.1%.
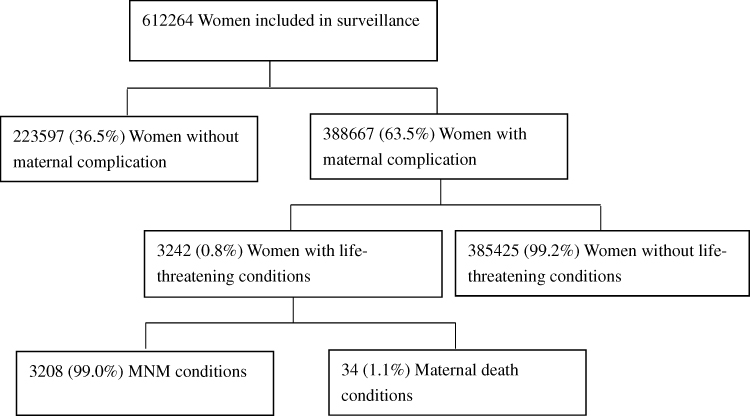 |
Figure 1 Flow chart of survey participants and maternal safety outcome. Abbreviation: MNM, maternal near-miss. |
The breakdown of MNM conditions, according to the MNM approach is shown in Table 1. The commonest cause was coagulation/hematological dysfunction, n=2480 (77.3%) cases, including 1769 (55.1%) requiring five or more units of blood, followed by of acute thrombocytopenia (less than 50,000 platelets) n=756 (23.6%) and of clotting failure n=479 (14.9%). From 2012 to 2017, coagulation/hematological dysfunction showed an increased trend from 68.8% in 2012 to 85.2% in 2017. The next most common cause of MNM was cardiovascular dysfunction n=717 (22.4%), followed by uterine dysfunction n=469 (14.6%) (See Table 1).
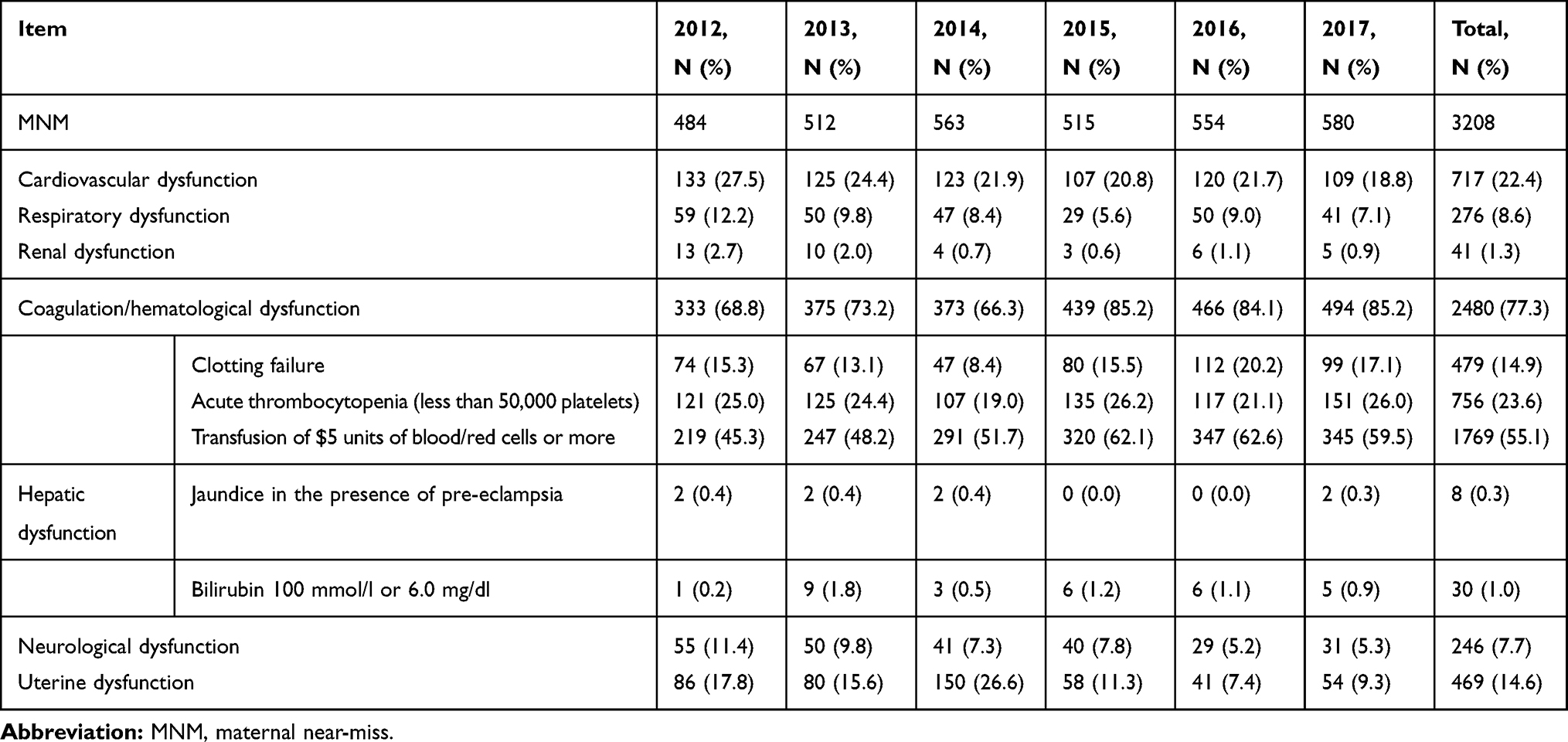 |
Table 1 Frequency of Organ Dysfunction Related to Pregnancy Among 3208 MNM During 2012–2017 |
Women aged older than 35 or younger than 19, primary school or no education, multipara, C-section history, no prenatal examination, abortion history over 2, delivery in township hospital or home are more likely to be MNM (see Table 2). The prevalence of obstetric hemorrhage, hypertensive disorders of pregnancy, anemia, hepatopathy, infection are significantly higher among MNM than others (see Table 3).
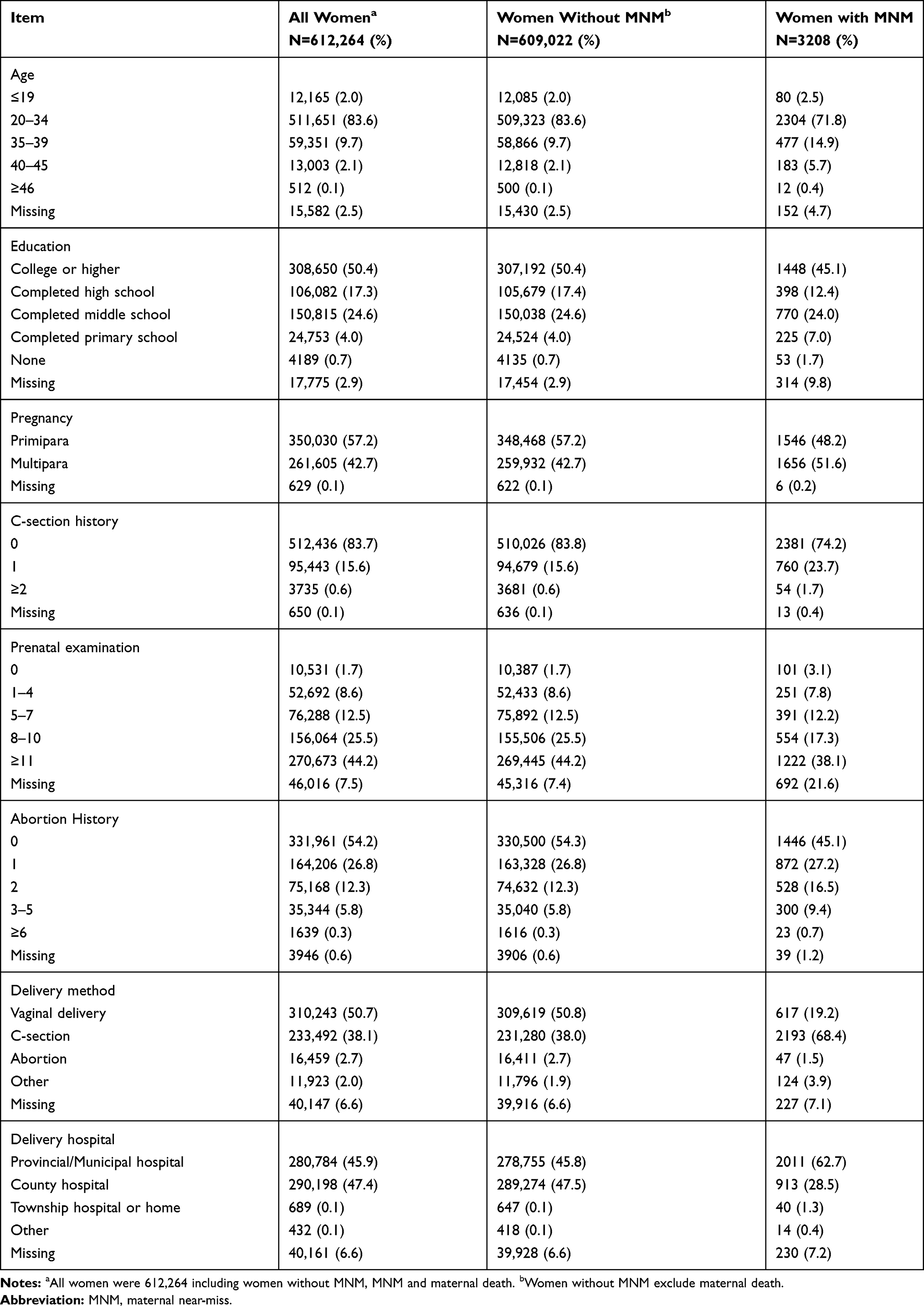 |
Table 2 The Difference of Demographic and Obstetric History and Delivery Mode Characteristics of Women with and Without MNM |
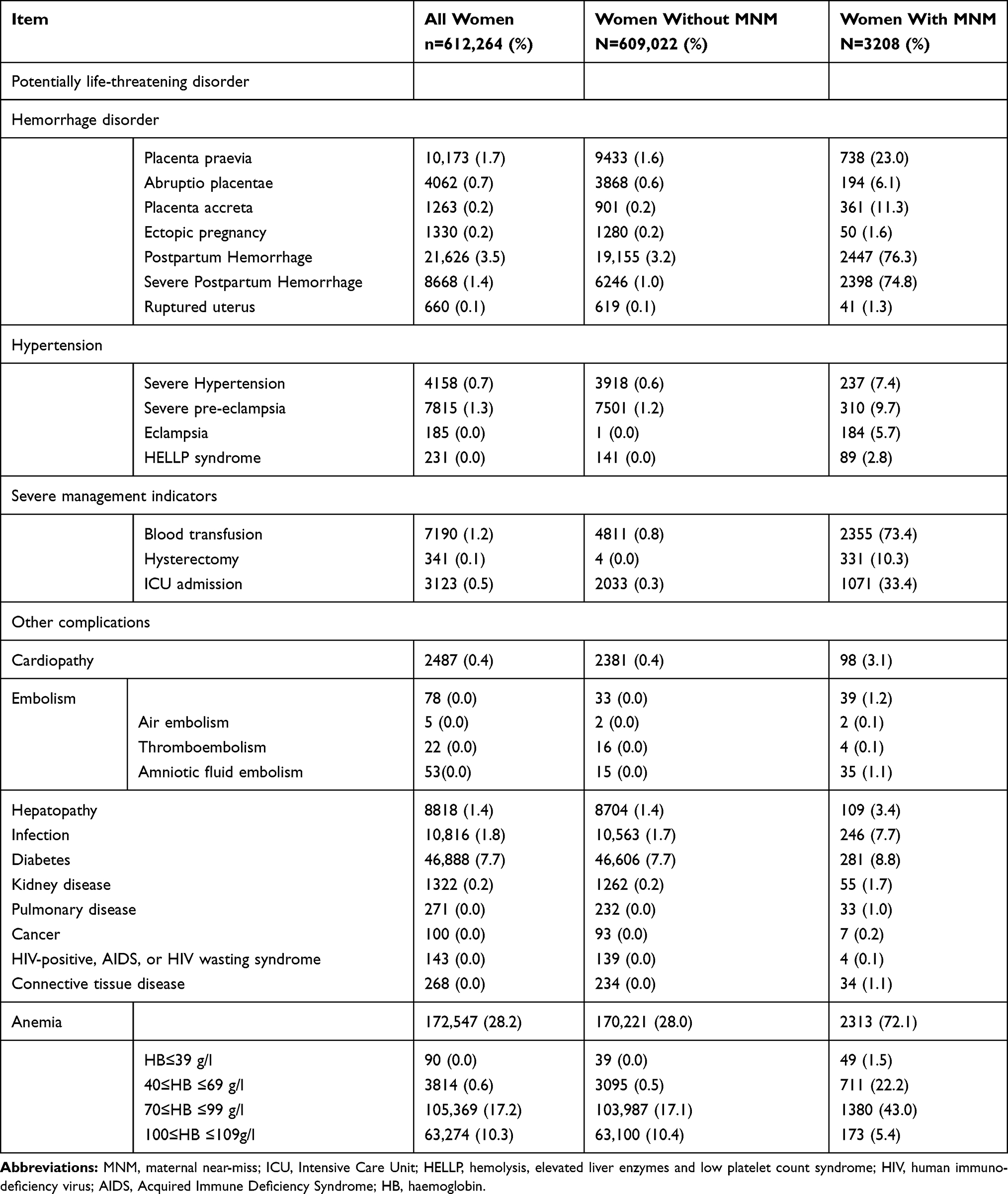 |
Table 3 Comparison of the Frequency of Potentially Life-Threatening Disorder and Other Complications Between Women with MNM and Without |
Among 3208 women with MNM, postpartum hemorrhage was the commonest cause at 76.3%, severe anemia at 23.7%, followed by placenta praevia at 23.0%, and placenta accreta at 11.3%. Uterine atony was the leading cause for postpartum hemorrhage of MNM at 895 (27.6%), followed by retained placenta at 101 (3.1%), soft birth canal laceration 58 (1.8%) and combined two or more of the above three diseases at 993 (30.7%). In fact, among all the women enrolled in the study, anemia was by far the commonest complication, n=172,547 (28.2%) followed by gestational diabetes at 46,888 (7.7%). Other common obstetrics diseases were postpartum hemorrhage with 21,626 (3.5%) and severe pre-eclampsia at 7815 (1.3%) (see Table 3).
MNM was highly significantly associated with premature birth (ORs 7.0; 95% CI 6.5–7.6), low birth weight (ORs 6.9; 95% CI 6.4–7.5), multiple fetuses (ORs 4.4; 95% CI 3.8–5.0), stillbirth (ORs 5.7; 95% CI 4.9–6.5) and neonatal mortality (ORs 10.2; 95% CI 7.2–14.5) (see Table 4).
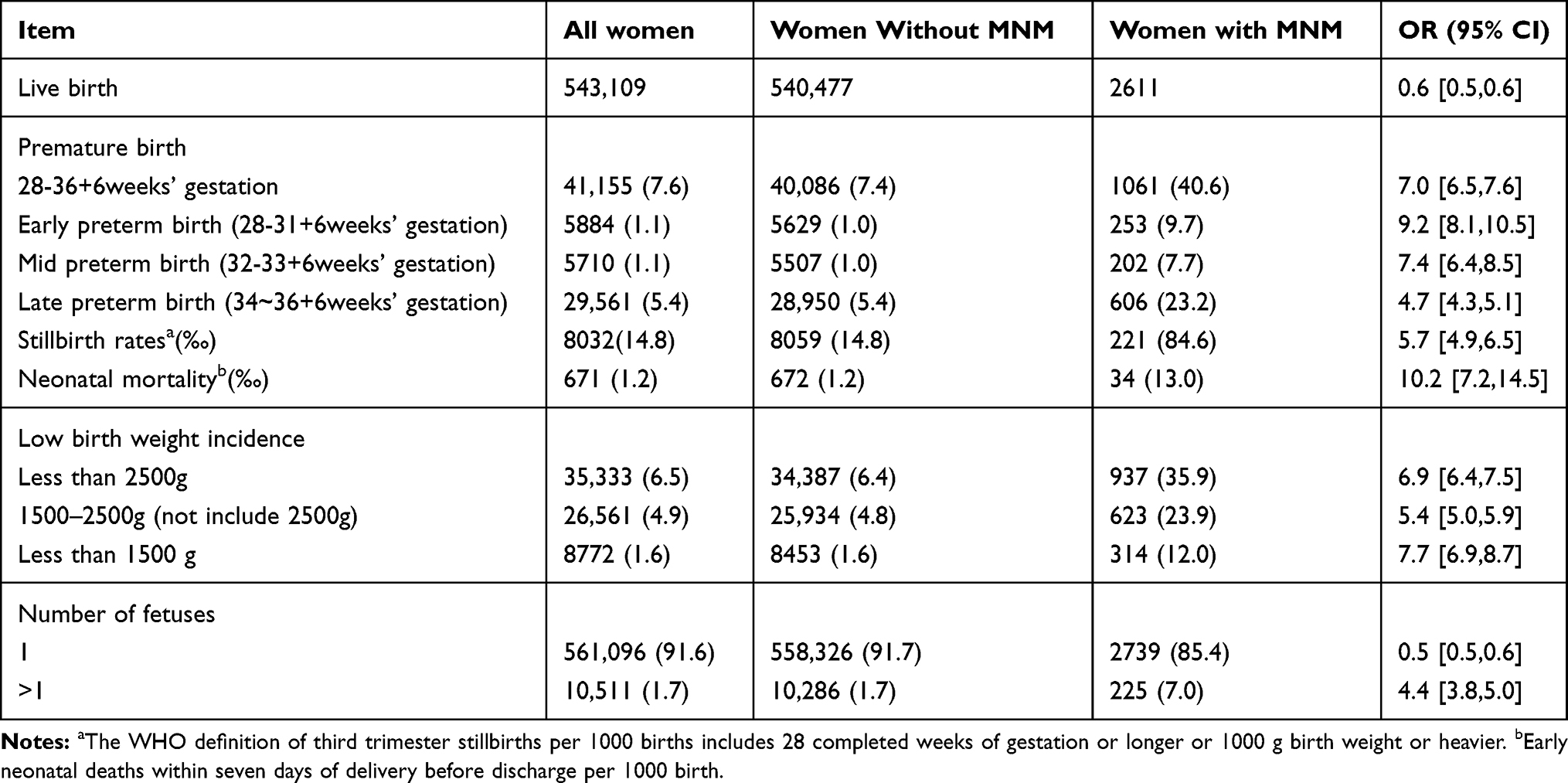 |
Table 4 Comparison of Perinatal Outcome Between Women with MNM and Without During 2012–2017 |
Embolism had the highest risk for causing MNM (AOR 46.0; 95% CI 19.1–110.7). Embolism was diagnosed in 78 of the women including 53 with amniotic fluid embolism, 22 thromboembolism and 5 air embolism. Postpartum hemorrhage has the second-highest likelihood for MNM (AOR 41.0; 95% CI 35.7–47.0) followed by HB≤39g/l (AOR 36.6; 95% CI 16.0–84.1), delivery in township hospital and at home (AOR 12.4; 95% CI 3.9–39.7), HELLP syndrome (AOR 8.4; 95% CI 5.0–14.2) and C-section (AOR 3.1; 95% CI 2.8–3.6) (see Table 5).
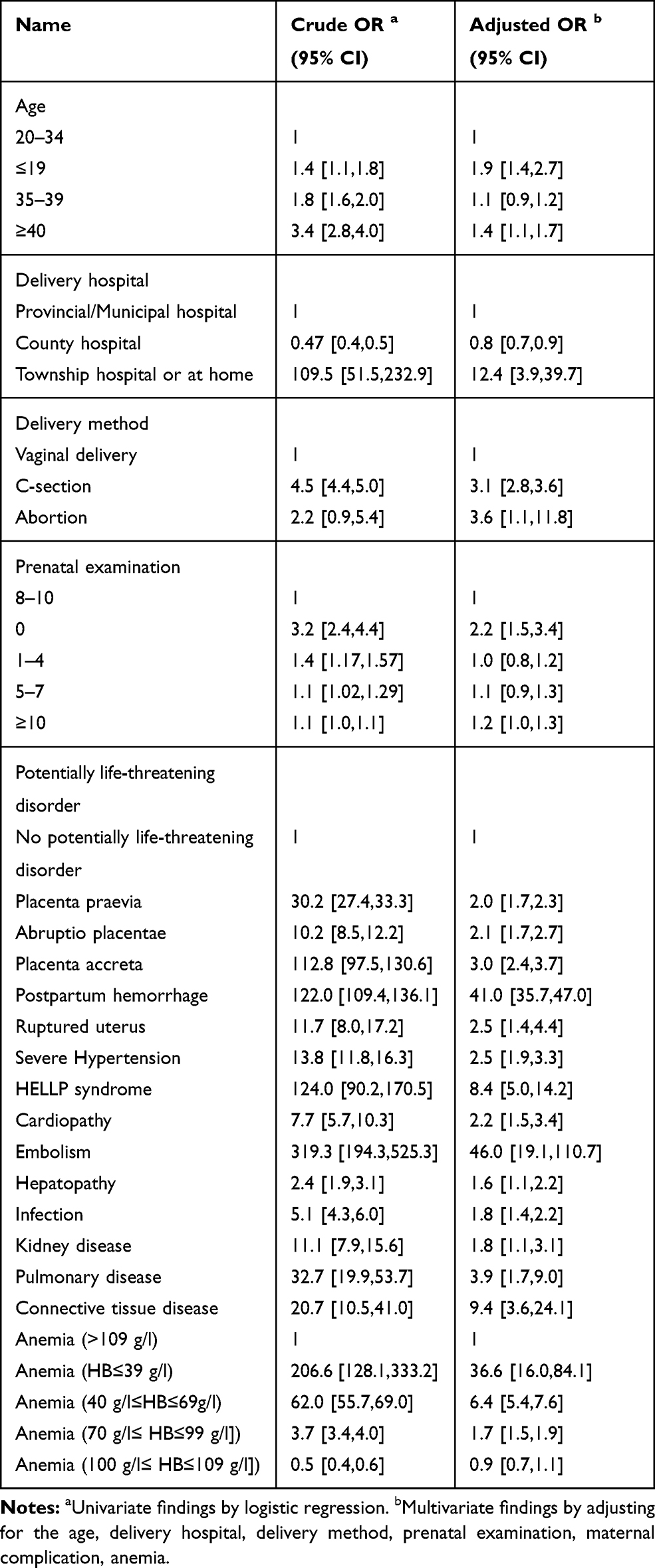 |
Table 5 Risk Factors for MNM in Zhejiang Province During 2012–2017 |
Discussion
This is the first provincial level, systematic study about MNM in China. Maternal near-miss indicators for Zhejiang Province show a low maternal mortality, low severe maternal outcome and low mortality index. This indicates a relatively high quality of maternal health care in a developed province of China. Only two previous Chinese papers have reported the MNM ratio, both covering just one hospital, and reporting ratios of 3.8/1000 live births in Suzhou city20 and 12.4/1000 in Hefei city.21 Maternal healthcare has been improving for over 30 years in Zhejiang Province along with socio-economic development. Maternal mortality is very low, thus highlighting the importance of MNM surveillance to assess the quality of health in more developed areas of China.
This research highlights several points. Firstly, unsurprisingly, hospital level was significantly associated with MNM. Women delivering at home and township hospital had high risk (OR:12.4) of MNM. Although home births have not been permitted since 1990 in Zhejiang, as shown here, there are still a small number. However, MNM was less common in county hospitals, probably because high-risk pregnancies are transferred to higher level hospitals for the management of severe complications. In Zhejiang Province, there is an effective referral system for high-risk pregnancy, providing access to obstetric emergency centers. In addition, free basic antenatal and postpartum care service is provided by medical practitioners at primary level community services.22 Therefore, many women in the study achieved more than five prenatal examinations allowing for early identification of complications.
Secondly, the identified socio-demographic risk factors are similar to those found in the WHO Multi-country Survey (WHOMCS) which included 314,623 women in 29 countries.23 These risk factors included young and older age, and low education level. In Zhejiang Province, education levels are now relatively high, contributing to the low MNM ratio and maternal mortality ratio.
Thirdly, the study indicated that C-section was an independent risk factor for MNM. This is very important because of the high rate in China, although it is one of the few countries to have reversed the rising caesarean section rates over the past ten years.19,24-26 The C-section rate of 38.1% in this study is still twice the recommended rate of 19% recently recommended by WHO.27
Fourthly, MNM was significantly associated with obstetrics complications and medical diseases, such as postpartum hemorrhage, pre-eclampsia and embolism. We showed postpartum hemorrhage was the most common cause of MNM, which is higher than the 26% reported by WHOMCS.23 We showed that postpartum hemorrhage increased over the six years period, partly because of increases in birth canal laceration. But uterine atony was the leading cause of postpartum hemorrhage overall, in line with findings of the WHO study in 28 countries.28 We showed that severe pre-eclampsia was a major cause of MNM. Hypertensive disorders were among the three leading causes for maternal mortality in Zhejiang Province.29 Our findings also showed low frequency of embolism but with the highest likelihood of leading to MNM. In many developed country settings, embolism is the major cause of maternal death.30
Importantly, this study indicated that MNM was significantly associated with adverse perinatal outcomes for the fetus and newborn, including intrauterine growth restriction, low birth weight, and stillbirth, consistent with findings from elsewhere.11 This is largely caused by the need for early induction of labor or cesarean delivery and subsequent preterm birth.
There are several limitations in our study. Firstly, the data were collected from the electronic medical record system, which in itself has limitations. For example, the economic situation of the mother, and her health insurance cover were unavailable in the system and these may be associated with MNM. There was a high incidence of abortion and as a cause of MNM, but the dataset could not differentiate between induced and natural abortion. Secondly, the neonatal mortality and maternal mortality may be underestimated due to data collection before hospital discharge and no follow-up within the system. Thirdly, the level of included hospitals is the county hospitals or above, with township hospitals and private hospitals excluded, except when women are transferred to higher level hospitals. In addition, the results represent a developed area of China. And we were unable to obtain data for poorer regions of China for comparison purposes.
Conclusions
Overall near-miss indicators suggested a relatively high quality of maternal health care in a developed province of China and highlight the importance of MNM surveillance. Incorporating the MNM approach into routine hospital information systems could contribute to improvement of the quality of maternal health care in many settings with resulting reductions on mortality and in obstetric complications. The identified risk factors may be helpful in developing targeted interventions and early prevention on MNM for improving maternal safety. In particular, strategies need to be reinforced to reduce unnecessary Caesarean section. Targeted interventions for decreasing the incidence of anemia and postpartum hemorrhage should be implemented delivery technology.
Abbreviations
MNM, maternal near-miss; NMNMSS, National Maternal Near-Miss Surveillance System; MCH, Maternal and Child Health; MD, Maternal death; SMOR, Severe maternal outcome ratio; WHOMCS, WHO Multi-country Survey.
Ethics and Consent Statement
The study achieved 18 hospital’s authorization. There was no direct interaction with patients and no information was obtained direct from patients. Therefore, it was unnecessary to get informed consent from individual patients. All needed data are extracted from hospital’s electric medicine records without any patient identification.
Acknowledgments
YuanYing Ma and LiSan Zhang are joint first authors. Xinyu Wang and Therese Hesketh contributed equally to the correspondence work. We thank the professionals and managers in the study sites for their help in data collection and creating a data set.
Funding
This study was supported by grants from the National Science Foundation of China (No. 71804162) and Public Technology Application Research Project of Science and Technology Department of Zhejiang Province (Nos. 2016C33132 and 2017c33059).
Disclosure
The authors report no conflicts of interest in this works.
References
1. Liang J, Li X, Kang C, et al. Maternal mortality ratios in 2852 Chinese counties, 1996-2015, and achievement of millennium development goal 5 in China: a subnational analysis of the global burden of disease study 2016. Lancet. 2019;393(10168):241–252. doi:10.1016/S0140-6736(18)31712-4
2. Powell Jackson TP, Gao YP, Ronsmans CP, Zhou HP, Wang YD, Fang HP. Health-system determinants of declines in maternal mortality in China between 1996 and 2013: a provincial econometric analysis. Lancet. 2015;386:S15–S15. doi:10.1016/S0140-6736(15)00593-0
3. Yanqiu G, Ronsmans C, Lin A. Time trends and regional differences in maternal mortality in China from 2000 to 2005. Bull World Health Organ. 2009;87(12):913–920. doi:10.2471/BLT.08.060426
4. Qiu L, Lin J, Ma Y, et al. Improving the maternal mortality ratio in Zhejiang Province, China, 1988–2008. Midwifery. 2010;26(5):544–548. doi:10.1016/j.midw.2010.06.003
5. Gan X, Hao C, Dong X, et al. Provincial maternal mortality surveillance systems in China. Biomed Res Int. 2014;3(2014):187896. doi:10.1155/2014/187896
6. China Statistics Bureau. Total population of Zhejiang Province China. Available from: http://www.stats.gov.cn/.
7. Zhejiang Provincial People’s Government. 公共卫生服务惠民生. Public health services benefit people’s livelihood; 2017. Available from: http://www.zj.gov.cn/art/2017/7/24/art_7406_2241477.html.
8. Agrawal P. Maternal mortality and morbidity in the United States of America. Bull World Health Organ. 2015;93(3):135. doi:10.2471/BLT.14.148627
9. Pattinson R, Say L, Souza JP, van den Broek N, Rooney C. WHO maternal death and near-miss classifications. Bull World Health Organ. 2009;87(10):734. doi:10.2471/BLT.09.071001
10. Pattinson R. Near miss audit in obstetrics. Best Prac Res Clin Obstet Gynaecol. 2009;23(3):285–286. doi:10.1016/j.bpobgyn
11. Souza JP, Cecatti JG, Faundes A, et al. Maternal near miss and maternal death in the World Health Organization’s 2005 global survey on maternal and perinatal health. Bull World Health Organ. 2010;88(2):113–119. doi:10.2471/BLT.08.057828
12. Pattinson RC, Buchmann E, Mantel G, Schoon M, Rees H. Can enquiries into severe acute maternal morbidity act as a surrogate for maternal death enquiries? BJOG. 2003;110(10):889–893. doi:10.1111/j.1471-0528.2003.03044.x
13. Nelissen E, Mduma E, Broerse J, et al. Applicability of the WHO maternal near miss criteria in a low-resource setting. PLoS One. 2013;8(4):e61248. doi:10.1371/journal
14. Souza JP, Bartlett L. Evaluating the quality of care for severe pregnancy complications: the WHO near-miss approach for maternal health. World Health Organization. 2011.
15. Witteveen T, de Koning I, Bezstarosti H, van den Akker T, van Roosmalen J, Bloemenkamp KW. Validating the WHO maternal near miss tool in a high-income country. Acta Obstet Gynecol Scand. 2016;95(1):106–111. doi:10.1111/aogs.12793
16. Souza JP, Cecatti JG, Haddad SM, et al. The WHO maternal near-miss approach and the maternal severity index model (MSI): tools for assessing the management of severe maternal morbidity. PLoS One. 2012;7(8):e44129. doi:10.1371/journal.pone.0044129
17. Zhu J, Liang J, Mu Y, et al. Sociodemographic and obstetric characteristics of stillbirths in China: a census of nearly 4 million health facility births between 2012 and 2014. Lancet Global Heal. 2016;4(2):e109–18. doi:10.1016/S2214-109X(15)00271-5
18. China Ministry of Health. 危重孕产妇监测手册. [National maternal near miss surveillance working manual. 2015]; 2015. Available from: http://www.mchscn.org/Article_Show.asp?ArticleID=609.
19. Liang J, Mu Y, Li X, et al. Relaxation of the one child policy and trends in caesarean section rates and birth outcomes in China between 2012 and 2016: observational study of nearly seven million health facility births. BMJ. 2018;5(360):k817. doi:10.1136/bmj.k817
20. Shen FR, Liu M, Zhang X, Yang W, Chen YG. Factors associated with maternal near-miss morbidity and mortality in Kowloon Hospital, Suzhou, China. Int J Gynaecol Obstet. 2013;123(1):64–67. doi:10.1016/j.ijgo.2013.06.011
21. Yang Y, Fang Y, Wang X, Zhang Y, Liu X, Yin Z. A retrospective cohort study of risk factors and pregnancy outcomes in 14,014 Chinese pregnant women. Medicine. 2018;97(33):e11748. doi:10.1097/MD.0000000000011748
22. National Health Commission of China. 国家基本公共卫生服务项目. [National basic public health service in 2015. 2015]; 2015. Available from: http://www.nhc.gov.cn/jws/zcwj/201506/61340494c00e4ae4bca0ad8411a724a9.shtml.
23. Souza JP, Gülmezoglu AM, Vogel J, et al. Moving beyond essential interventions for reduction of maternal mortality (the WHO multicountry survey on maternal and newborn health): a cross-sectional study. Lancet. 2013;381(9879):1747–1755. doi:10.1016/S0140-6736(13)60686-8
24. Li H, Luo S, Trasande L, et al. Geographic variations and temporal trends in cesarean delivery rates in China, 2008-2014. JAMA. 2017;3;317(1):69–76. doi:10.1001/jama.2016.18663
25. Liu X, Lynch CD, Cheng WW, Landon MB. Lowering the high rate of caesarean delivery in China: an experience from Shanghai. BJOG. 2016;123(10):1620–1628. doi:10.1111/1471-0528.14057
26. Ma R, Lao TT, Sun Y, et al. Practice audits to reduce caesareans in a tertiary referral hospital in south-western China. Bull World Health Organ. 2012;90(7):488–494. doi:10.2471/BLT.11.093369
27. Molina G, Weiser TG, Lipsitz SR, et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015;314(21):2263–2270. doi:10.1001/jama.2015.15553
28. Sheldon WR, Blum J, Vogel JP, Souza JP, Gulmezoglu AM, Winikoff B. Postpartum haemorrhage management, risks, and maternal outcomes: findings from the world health organization multicountry survey on maternal and newborn health. BJOG. 2014;121(Suppl 1):5–13. doi:10.1111/1471-0528.12636
29. Kayem G, Kurinczuk J, Lewis G, Golightly S, Brocklehurst P, Knight M. Risk factors for progression from severe maternal morbidity to death: a national cohort study. PLoS One. 2011;6(12):e29077. doi:10.1371/journal.pone.0029077
30. Benson MD. Amniotic fluid embolism mortality rate. J Obstet Gynaecol Res. 2017;43(11):1714–1718. doi:10.1111/jog.13445
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.