")
Back to Journals » International Journal of Women's Health » Volume 14
Low Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening Increases the Subsequent Risk of Preterm Birth in Uncomplicated Singleton Pregnancy
Authors Yuan X, Han X, Jia C, Zhou W , Yu B
Received 1 March 2022
Accepted for publication 7 July 2022
Published 13 July 2022 Volume 2022:14 Pages 889—897
DOI https://doi.org/10.2147/IJWH.S364554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Xiaosong Yuan, Xiaoya Han, Chenbo Jia, Wenbo Zhou, Bin Yu
Department of Medical Genetics, Changzhou Maternal and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, People’s Republic of China
Correspondence: Bin Yu, Email [email protected]
Objective: To examine the association between low fetal fraction (FF) of cell free DNA determined at non-invasive prenatal screening (NIPS) and the subsequent risk of preterm birth in uncomplicated singleton pregnancy.
Methods: We retrospectively interrogated NIPS System and hospitalization records from April 2018 to August 2019 and obtained results from 1521 consecutive and uncomplicated women with singleton pregnancy in which plasma FF of cell free DNA at NIPS had been investigated together with birth outcomes. We examined the association between FF and preterm birth (PTB) by regression analysis.
Results: The incidence of preterm birth, low birthweight, and macrosomia in the study population was 5.06%, 2.89%, and 7.17%, respectively. FF at NIPS in the second to fourth quartiles (8.40– 11.07, 11.08– 13.70, and > 13.70%, respectively) was associated with higher gestational age at delivery relative to the lowest quartile (< 8.40%), with estimated mean increases of 0.27 weeks (95% CI: 0.05– 0.49), 0.29 weeks (95% CI: 0.06– 0.51), and 0.28 weeks (95% CI: 0.05– 0.51), respectively (P for trend = 0.027). Low FF (< the 5th percentile) was associated with an increased risk of PTB (adjusted OR: 2.23, 95% CI: 1.01– 4.98, P = 0.047) compared to normal FF (≥ the 5th and ≤ the 95th percentiles). In addition, when compared to women with normal FF and body mass index (BMI) < 25 at NIPS, the risk of early PTB (< 34 weeks gestation) was remarkably significantly higher among those with low FF and BMI ≥ 25 (adjusted OR: 6.29, 95% CI: 1.71– 23.15, P = 0.006).
Conclusion: Our study supports the association of low FF at NIPS with PTB (especially early PTB) for uncomplicated singleton pregnancy.
Keywords: preterm birth, cell-free fetal DNA, fetal fraction, non-invasive prenatal screening, birth outcomes
Introduction
The incidence of preterm birth (PTB) is about 6.1% in China, 8.7% in Europe, and 11.3% in the USA.1,2 Globally, PTB ranks first among the causes of neonatal death and is associated with adverse health sequelae in adulthood.3,4 Consequently, better identification of pregnant women at high risk of PTB is a prerequisite for reducing its incidence.
The discovery of circulating cell-free fetal DNA (cffDNA) in maternal plasma has been profoundly and rapidly transformed into clinical application – noninvasive prenatal screening (NIPS) detecting fetal aneuploidies with high sensitivity and specificity.5 Fetal fraction (FF) of cell free DNA represents a ratio of cffDNA to total cell-free DNA in maternal circulation and is an important parameter for assessing analytical results of NIPS. During the past decade, the association of abnormal FF at NIPS with adverse pregnancy outcomes has attracted increasing attention in the scientific community, but the clinical implications of abnormal FF remain unclear. For example, a limited number of observational studies have examined the relationship between abnormal FF and PTB, and have yielded conflicting results. Dugoff et al found that a high FF (≥ the 95th percentile) at 14–20 weeks gestation is related to PTB, whereas other studies found no association between high FF (≥ the 95th percentile) in the second trimester and high risk of PTB.6–9 In contrast, evidence from two studies showed that PTB frequently occurs among pregnant women with low FF (<4%) and a low FF (< the 10th percentile) is associated with an increased risk of early PTB (< 34 weeks gestation).9,10 This discrepancy could be attributed to the failure of most studies to control for pregnancy complications leading to PTB.
We conducted an observational cohort study in Changzhou Maternity and Child Health Care Hospital to investigate the association between low FF measured at NIPS and PTB for uncomplicated singleton pregnancies. We hypothesized that the independent or combined effect of low FF and maternal characteristics can be established for PTB.
Methods
Study Population and Data Collection
This observational cohort study was conducted in Changzhou Maternal and Child Health Care Hospital, Jiangsu Province, China. Between April 2018 to August 2019, consecutive pregnant women presenting for NIPS and delivery in the hospital were included in the present study. The protocol was approved by the ethics committee of the hospital (No. ZD201803) and informed consent was obtained from each participant. Women were included if they had a singleton pregnancy, complete medical records and NIPS data. Women were not eligible if they met one of the following conditions: positive NIPS results (Z-scores ≥3 or ≤-3, high risk for fetal aneuploidy in T21/T18/T13); abortion; fetal death, termination and birth defects; pre-pregnancy disease (chronic hypertension, diabetes mellitus, heart, liver, or kidney disease, thyroid disease, immune rheumatic disease, syphilis); major pregnancy complications [gestational diabetes mellitus (GDM), intrahepatic cholestasis of pregnancy (ICP), preeclampsia (PE), pregnancy induced hypertension (PIH)]. 1521 consecutive pregnant women and their singleton pregnancies were included in the present study (Figure 1). None of the participants in this study smoked or consumed alcohol and drugs during pregnancy. As described previously, NIPS was performed on the sequence platform of Illumina NextSeq 500 in the Second-trimester (Illumina China, China).11 In brief, maternal whole blood (8 mL) was collected, and the plasma was obtained by centrifugation at 1600 g for 10 min at 4 °C. Cell freeDNA was extracted from 1.2 mL of plasma using an automatic magnetic bead extraction and purification system (KingFisher Flex, Thermo Scientific & Co. USA). The extracted DNA was then constructed library and massively parallel sequencing. After sequence data were analyzed, the z-scores and FF were obtained. After reporting NIPS results, all NIPS-positive women (Z-scores ≥3 or ≤-3) were recalled for genetic counseling. FF is the key quantity to detect the aneuploidy status of a fetus in NIPS. Its measurement using sequence read counts was determined by a multivariable model.12 We retrospectively collected and interrogated NIPS data and hospitalization records for this observational study. Data on maternal age, gravidity, parity, assisted reproduction, medical history, pregnancy complications, delivery mode, gestational age at delivery, and fetal birth weight were obtained from the hospitalization records. Maternal height, weight, and FF at NIPS were collected from NIPS system.
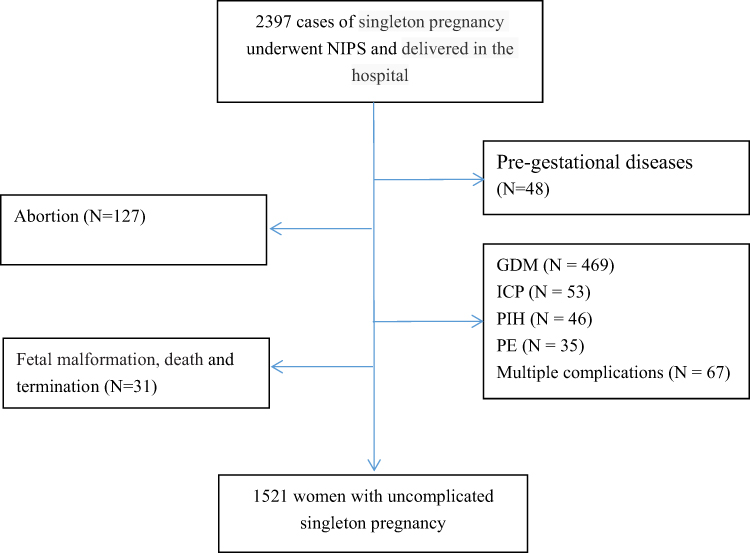 |
Figure 1 Flow chart of study population. |
Outcome Definitions and Statistical Analysis
Our primary outcome was gestational age at delivery; secondary outcome was birthweight. According to the gestational age at delivery, PTB was classified as early PTB (< 34 weeks), late PTB (34 to 36 weeks), and total PTB (< 37 weeks), respectively.13 Based on the birthweight, neonates were stratified into low birthweight (LBW) (<2500 g), normal birthweight (2500–4000 g), and macrosomia (>4000 g), respectively.14 In addition, the diagnosis of major pregnancy complications including GDM, PE, PIH and ICP, was based on a previous study.15 Continuous variables with or without normal distribution were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). Categorical variables were presented as N (%). To be consistent with previous studies, FF was defined as three categories: low FF (<5th percentile), normal FF (5–95th percentile), and high FF (>95th percentiles), respectively.6,7,9,16,17 Parametric and non-parametric methods, as appropriate, were used to describe the differences in the basic characteristics between normal and low/high FF mother–neonate pairs. General linear analysis was used to examine the association of different FF quartiles with fetal gestational age at delivery and birthweight.
After the gestational age at delivery and birthweight were defined as categorical variables (PTB/LBW/macrosomia), logistic regression analysis was applied to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to assess the association of low FF with outcomes. In addition, an effect of low FF combined high BMI (≥25) at NIPS on different PTB was evaluated by the regression models. The statistical analyses in this study were performed using R (http://www.R-project.org) and Empower Stats software (X&Y solutions, Boston, MA, USA). A P-value < 0.05 was considered as statistical significance.
Results
After excluding 876 cases of major pregnancy complications, medical abortion, pre-gestational diseases, fetal malformation, death and termination, 1521 pregnant women and their singleton pregnancies were eligible for this study. The incidence of preterm birth, low birthweight, and macrosomia in the study population was 5.06%, 2.89%, and 7.17%, respectively. Tables 1 and S1 showed the demographic characteristics of the study population according to the different FF categories, respectively. Significant differences were observed for maternal BMI at NIPS, assisted reproduction, fetal birthweight, gestational age at delivery, and the incidence of cesarean section and PTB between women with low FF and those with normal FF (for BMI at NIPS: 24.36 vs 22.35, P <0.001; for assisted reproduction: 11.84% vs 5.56%, P <0.05; for gestational age at delivery: 38.16 vs 38.76 week, P <0.01; for fetal birthweight: 3205 vs 3370 g, P <0.05; for cesarean section: 60.53% vs 48.43%, P <0.05; for PTB: 10.53% vs 4.75%, P <0.05) (Table 1). In addition, gestational age at NIPS was significantly increased between FF categories (121.62 vs 123.61 vs 126.25 day, P <0.05) (Table S1).
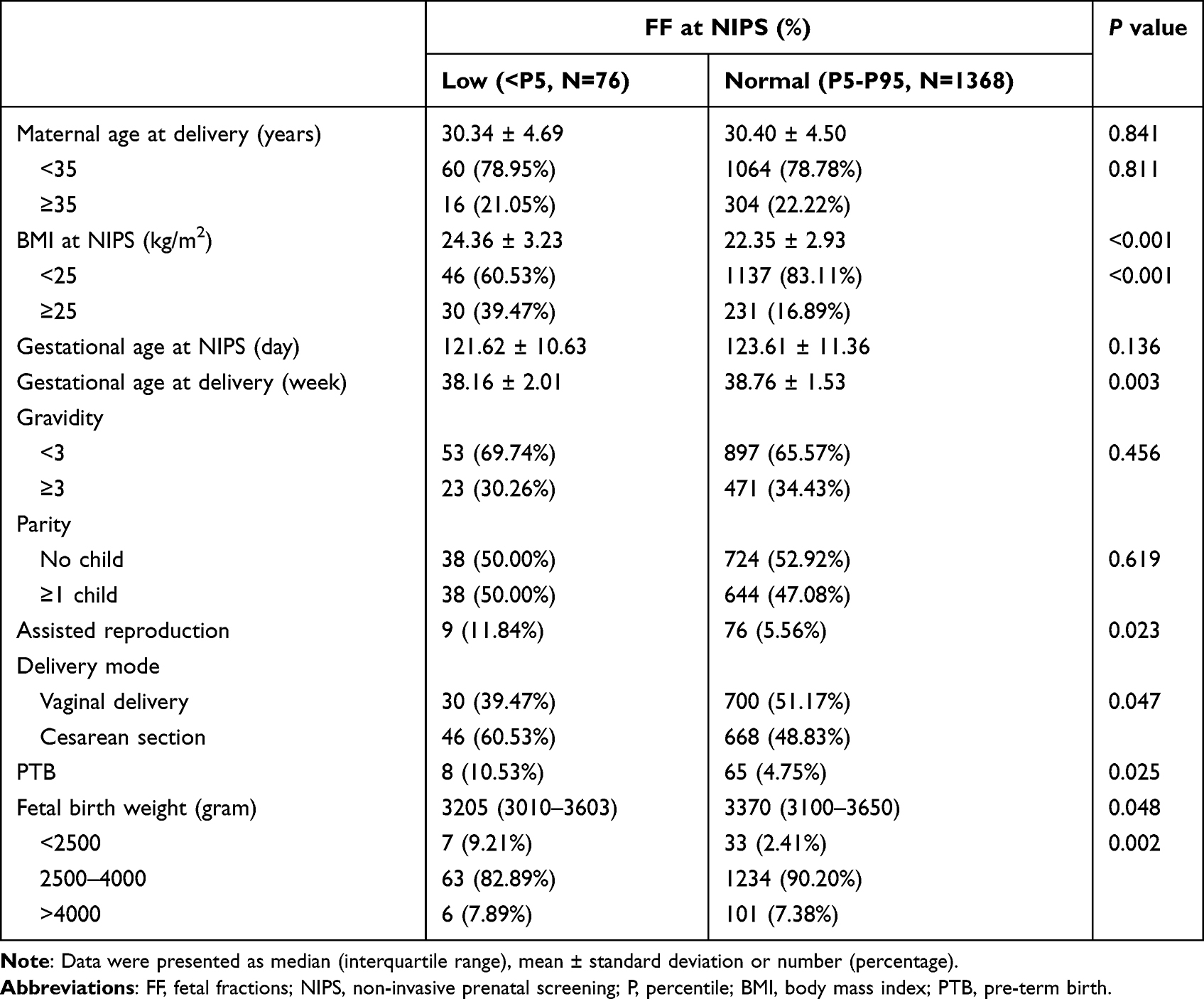 |
Table 1 The Difference in Maternal Characteristics and Neonatal Outcomes Between Low and Normal Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening |
The distribution of maternal plasma FF at NIPS grouped by PTB and full-term birth (FTB) was presented in Table 2. Compared to FTB women, PTB women had lower plasma FF at NIPS (median FF: 10.09% vs 11.12%, P < 0.05). With increasing quartile of FF at NIPS, the gestational age at delivery increased by 0.27, 0.29, and 0.28 weeks (Table 3). Compared to women with normal FF (≥ the 5th and ≤ the 95th percentiles), the risk of PTB in those with low FF (< 5th percentile) significantly increased by 2.23-fold (95% CI: 1.01–4.98; P < 0.05) (Table 4). In addition, low FF increased the LBW risk in the crude models (OR: 4.15, 95% CI: 1.77, 9.76, P < 0.01), but the increase was not significant in the adjusted models (OR: 3.31, 95% CI: 0.73, 14.93, P = 0.120). For the combined effect of FF and BMI at NIPS on PTB, when compared to women with normal FF and BMI <25 at NIPS, the risk of PTB and early PTB (<34 week) was remarkably significantly higher among those with low FF and BMI ≥25 (for PTB: adjusted OR: 3.2, 95% CI: 1.06–9.64, P < 0.05; for early PTB: adjusted OR: 6.29, 95% CI: 1.71–23.15, P < 0.01) (Table 5). No significant association of low FF at NIPS with late PTB (34–36 week) was observed in both the crude and adjusted models.
 |
Table 2 The Distribution of Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening According to the Subsequent Preterm Birth and Full-Term Birth |
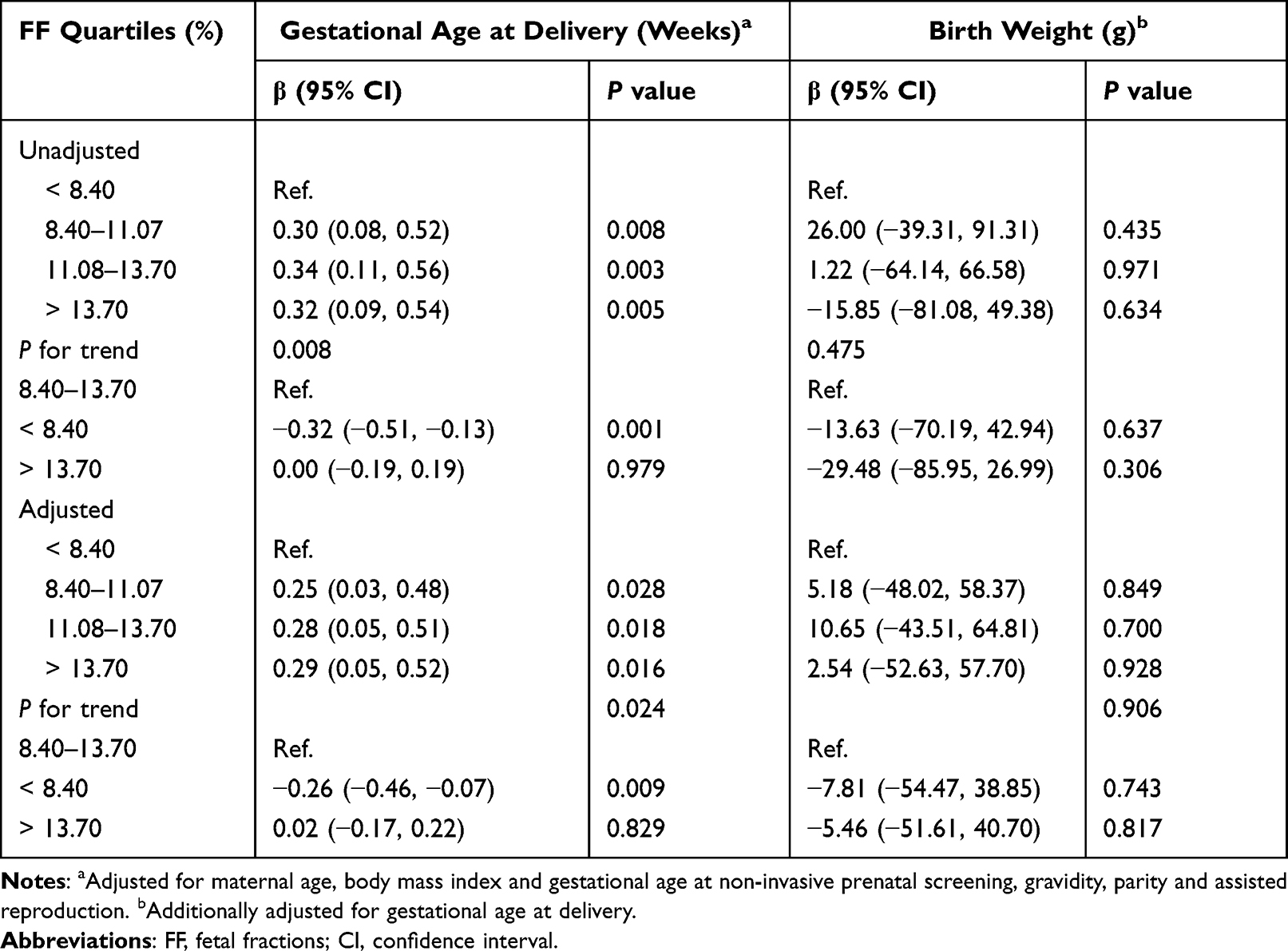 |
Table 3 Regression Coefficients for Fetal Birthweight and Gestational Age Associated with the Quartiles of Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening |
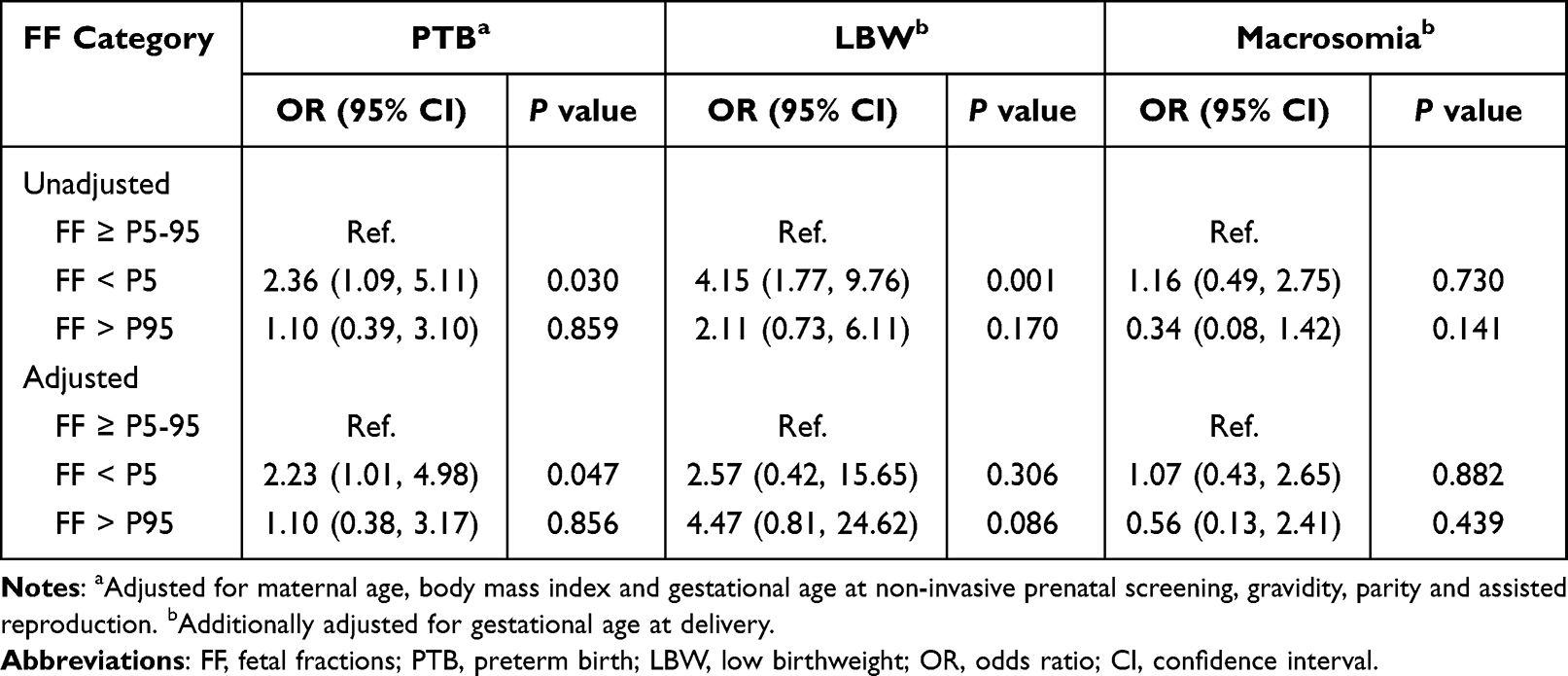 |
Table 4 Association Between Low Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening and Adverse Birth Outcomes |
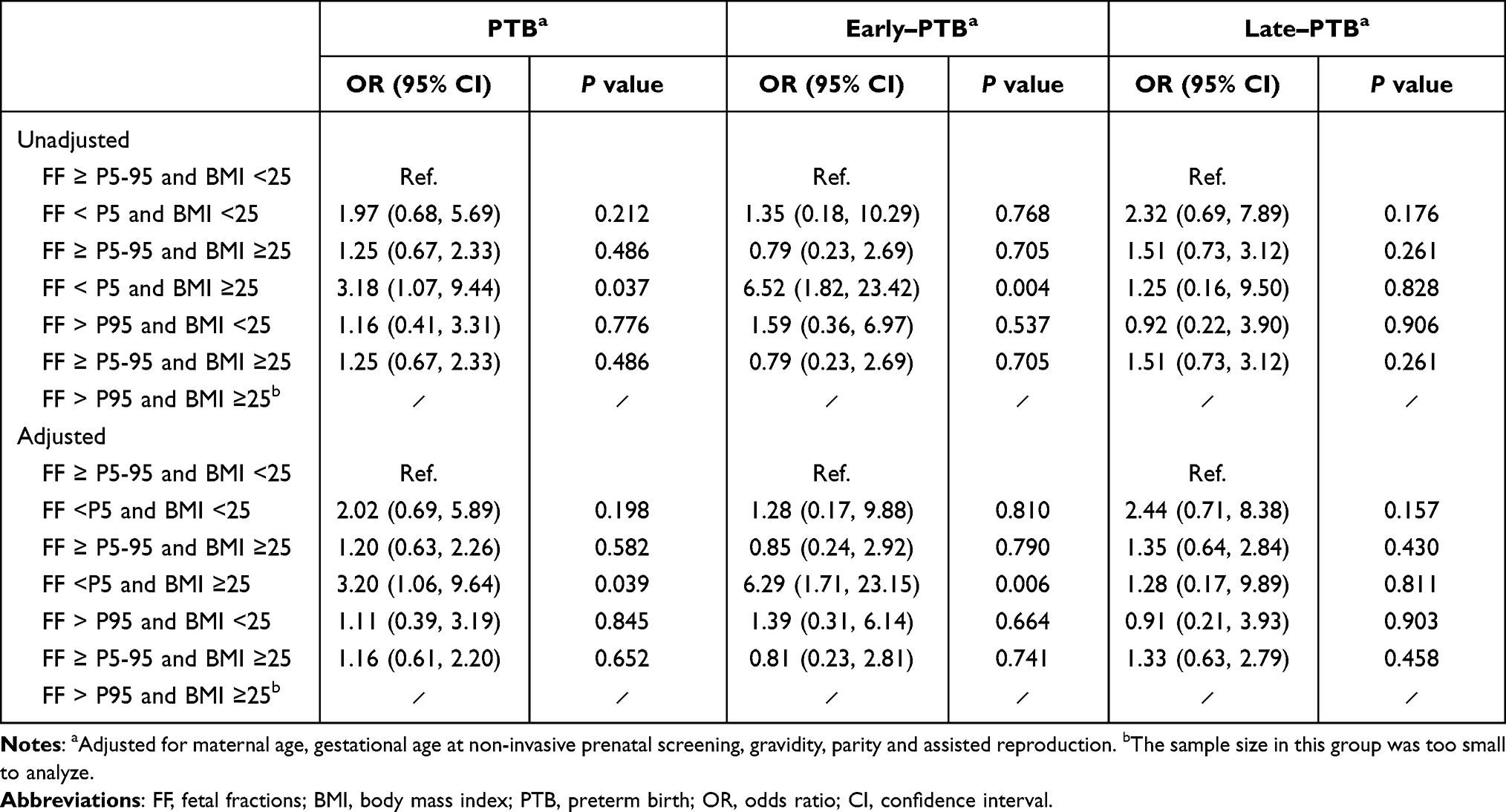 |
Table 5 Combined Effect of Low Fetal Fraction of Cell Free DNA and High BMI at Non-Invasive Prenatal Screening on Subsequent Preterm Birth |
Discussion
There were several interesting findings from this observational cohort study of uncomplicated pregnant women. First, with increasing FF quartile at NIPS from Q2 to Q4, the gestational age at delivery increased by 0.27 weeks, 0.29 weeks, and 0.28 weeks. Second, when compared to women with normal FF (≥ the 5th and ≤ the 95th percentiles) in the second trimester, women with low FF (< the 5th percentile) had a 2.25-fold increased risk of PTB. Third, women with low FF and high BMI (≥25) at NIPS had a 6.29-fold greater risk of early PTB compared to those with normal FF and BMI <25.
PTB is a common perinatal complication affecting a large number of pregnancies. Jing et al conducted a meta-analysis of 24,039,084 births from China and noted that the incidence of PTB has steadily risen from 5.36% in 1990–1994 to 7.04% in 2015–2016.1 The rate of PTB in this study was 5.06%, and lower than their report. The decline was possibly due to excluding a significant number of complicated pregnancies (670 cases). Women with pregnancy complications have a high likelihood of PTB. For example, ICP and PE are associated with increased rate of PTB.18,19 Previous studies demonstrated that the incidence of PTB in study populations who underwent serum screening for Down’s syndrome or NIPS is significantly higher in women with ICP or PE compared to those with non-pregnancy complications (NPC) (for serum screening: PE/ICP vs NPC, 20.6% /7.0% vs 3.1%; for NIPS: PE/ICP vs NPC, 15.4% /7.7% vs 3.3%). In addition, as suggested by a recent cohort study on the association between maternal thyroid hormone in late pregnancy and adverse birth outcomes, the rate of PTB in 11,564 Chinese pregnant women including those with major pregnancy complications was 6.9%, close to 7.0%.20 Furthermore, PTB rate differs by regions in China, among which East China shows a lower PTB rate.1 A low PTB rate in the East may be related to a higher socioeconomic status.21 The present study was conducted in Changzhou City, one of the developed areas in East China.
Over the past ten years, the importance of FF at NIPS has been highlighted by clinical practice. Sufficient FF (>%4) is an important threshold to avoid a non-reportable result in NIPS. Some reports have demonstrated that FF is related to maternal and fetal characteristics and indirectly reflects early placental status.22–29 Others have suggested that low FF at NIPS may provide early information on placental dysfunction and is therefore associated with unfavorable pregnancy outcomes, specifically with hypertensive disease of pregnancy and fetal growth restriction.9,10,17,30–34 An association with PTB is unclear, as limited studies reported conflicting results. A retrospective cohort study from Philadelphia indicated that among NIPS women, a high FF level (>95th percentile) at 14–20 weeks gestation but not at 10–14 weeks, is related to an increased risk of PTB.6 Shook et al in Boston reported a similar finding, confirming that high FF at <14 weeks gestation is not associated with PTB.16 In addition, results from three other cohort studies from China and France indicated that high FF levels (>95th percentile and/or >90th percentile) at the second trimester of pregnancy are not associated with an increased risk of PTB.7–9 Several recent studies have examined potential low FF-associated alterations in PTB.9,10,33 In Atlanta, Krishna et al suggested that PTB is more frequent in pregnancy with a low FF result (<4%) on NIPS.10 A recent study from China demonstrated that a low FF (< the 10th percentile) is associated with an increased risk of early PTB (< 34 weeks gestation).9 Conversely, data obtained by Gerson et al in Boston suggest that low FF (< the 25th percentile) in the first or second trimester is not associated with PTB.33 Our results suggest that higher FF levels at NIPS increase the gestational age at delivery and lower FF levels (< the 5th percentile) are positively associated with the risk of PTB for uncomplicated pregnancy (adjusted OR: 2.23, 95% CI: 1.01–4.98). This discrepancy might be due to sample sizes, racial origin, the timing of NIPS, and cut-off criteria for defining low FF. A significantly negative association has been demonstrated of FF at NIPS with South Asian racial and Afro-Caribbean origin; the prevalence of PTB varies by maternal race/ethnicity.24,35,36 Gestational age of the participants at NIPS has been shown to be a key factor affecting FF.37 In our study, FF was positively correlated with gestational age at NIPS. A previous study indicated that measurement of FF in maternal plasma at 11–13 weeks gestation is not predictive of PTB.35
Increased BMI is correlated to adverse obstetric outcomes, although the underlying mechanism of this correlation has not been fully clarified.38 In the present study, we found that maternal BMI at NIPS significantly decreases with the elevation of FF categories (24.36 vs 22.35 vs 20.66). It is compatible with the findings of previous NIPS studies in Chinese Han Populations.7,9,29 Obese women often have various alterations in metabolic profile (turnover of adipocytes, increased blood volume, and vascular apoptosis), which will lead to an increased release of maternal derived cfDNA into the circulation and result in a dilution for the fixed amount of FF.39,40 Our findings indicated that women with low FF and high BMI at NIPS had a 6.29-fold greater risk of early PTB compared to those with normal FF and BMI. Therefore, for pregnant women with elevated BMI at NIPS, medical staff should pay more attention to the FF at NIPS, and provide better perinatal care for those with low FF due to the high risk of early PTB.
Several strengths of this observational study included the following: 1) the exclusion of participants with major pregnancy complications or pre-existing disease, which were the main confounding factors affecting birth outcomes, 2) the same diagnostic criteria for various pregnancy complications and birth outcomes, and minimal variation in prenatal care because of the cohort from a single institution, 3) the determination of FF in a single laboratory using the same platform and settings to minimize the differences caused by NIPS, and 4) adjusting for the available confounders including maternal age, BMI and gestational age at NIPS, gravidity, parity, and assisted reproduction. This cohort study’s limitations should also be taken into consideration. One was the lack of data on other maternal demographic characteristics (maternal socioeconomic, educational status, and history of PTB) contributing to a high risk of PTB; because of the retrospective observational design, we have no data on whether the pregnant women at high risk of PTB received glucocorticoids medication, which may affect gestational age at delivery. Another was that the relationship between the FF in early, late pregnancy and PTB risk was not investigated due to the retrospective design.
Conclusion
Our study demonstrates that a low FF in the second trimester of pregnancy significantly increases a risk of PTB, especially in women with high BMI at NIPS for uncomplicated singleton pregnancy. It is necessary to conduct a longitudinal prospective cohort study to explore the fluctuation of low FF during normal pregnancy and complicated pregnancies and its association with PTB.
Abbreviations
FF, fetal fraction; NIPS, non-invasive prenatal screening; PTB, preterm birth; BMI, body mass index; cffDNA, cell-free fetal DNA; GDM, gestational diabetes mellitus; ICP, intrahepatic cholestasis of pregnancy; PE, preeclampsia; PIH, pregnancy induced hypertension; LBW, low birthweight; SD, standard deviation; IQR, interquartile range; OR, odds ratio; CI, confidence interval; FTB, full-term birth; NPC, non-pregnancy complication.
Data Sharing Statement
The data used and/or analyzed in the present study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We confirm that our study complies with the Declaration of Helsinki. The study protocol was approved by the ethics committee of Changzhou Maternity and Child Health Care Hospital (No. ZD201803). Informed consent in our study was waived because of retrospective and anonymous analysis.
Acknowledgment
We thank all participants of this study and the staff of laboratory and medical record section from Changzhou maternity and child health care hospital for their help with technical assistance and information service.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Changzhou science and technology support project (Social Development: CE20205028), Science and technology project for young talents of Changzhou Health Commission (QN202048), Jiangsu Maternal and Child Health Research Projects (F201842), and General project of Jiangsu Provincial Health Commission (M2021079).
Disclosure
The authors declare that they have no competing interests.
References
1. Jing S, Chen C, Gan Y, Vogel J, Zhang J. Incidence and trend of preterm birth in China, 1990-2016: a systematic review and meta-analysis. BMJ Open. 2020;10(12):e039303.
2. Chawanpaiboon S, Vogel JP, Moller AB, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(1):e37–e46.
3. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–3035.
4. Crump C, Sundquist J, Winkleby MA, Sundquist K. Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study. Lancet Child Adolesc Health. 2019;3(6):408–417.
5. Norton ME, Jacobsson B, Swamy GK, et al. Cell-free DNA analysis for noninvasive examination of trisomy. N Engl J Med. 2015;372(17):1589–1597.
6. Dugoff L, Barberio A, Whittaker PG, Schwartz N, Sehdev H, Bastek JA. Cell-free DNA fetal fraction and preterm birth. Am J Obstet Gynecol. 2016;215(2):
7. Guo FF, Yang JX, Huang YL, et al. Association between fetal fraction at the second trimester and subsequent spontaneous preterm birth. Prenat Diagn. 2019;39(13):1191–1197.
8. Duvillier C, Quibel T, Felsenheld C, Hupin-Genty L, Cohen C, Vialard F. Cell-free DNA fraction: can it be used to evaluate the risk of obstetrical issues? Gynecol Obstet Fertil Senol. 2019;47(11):790–796.
9. Yuan X, Zhou L, Zhang B, Wang H, Yu B, Xu J. Association between low fetal fraction of cell free DNA at the early second-trimester and adverse pregnancy outcomes. Pregnancy Hypertens. 2020;22:101–108.
10. Krishna I, Badell M, Loucks TL, Lindsay M, Samuel A. Adverse perinatal outcomes are more frequent in pregnancies with a low fetal fraction result on noninvasive prenatal testing. Prenat Diagn. 2016;36(3):210–215.
11. Yuan X, Zhou L, Zhang B, Wang H, Jiang J, Yu B. Early second-trimester plasma cell free DNA levels with subsequent risk of pregnancy complications. Clin Biochem. 2019;71:46–51.
12. Kim SK, Hannum G, Geis J, et al. Determination of fetal DNA fraction from the plasma of pregnant women using sequence read counts. Prenat Diagn. 2015;35(8):810–815.
13. Crump C, Sundquist J, Winkleby MA, Sundquist K. Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study. Lancet Child Adolesc Health. 2019;3(6):408–417.
14. Araujo Júnior E, Peixoto AB, Zamarian AC, Elito Júnior J, Tonni G. Macrosomia. Best Pract Res Clin Obstet Gynaecol. 2017;38:83–96.
15. Yuan X, Hu H, Zhang M, et al. Iron deficiency in late pregnancy and its associations with birth outcomes in Chinese pregnant women: a retrospective cohort study. Nutr Metab (Lond). 2019;16:30.
16. Shook LL, Clapp MA, Roberts PS, Bernstein SN, Goldfarb IT. High Fetal Fraction on First Trimester Cell-Free DNA Aneuploidy Screening and Adverse Pregnancy Outcomes. Am J Perinatol. 2020;37(1):8–13.
17. Clapp MA, Berry M, Shook LL, Roberts PS, Goldfarb IT, Bernstein SN. Low Fetal Fraction and Birth Weight in Women with Negative First-Trimester Cell-Free DNA Screening. Am J Perinatol. 2020;37(1):86–91.
18. Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. Lancet. 2019;393(10174):899–909.
19. Barros FC, Papageorghiou AT, Victora CG, et al. International Fetal and Newborn Growth Consortium for the 21st Century. The distribution of clinical phenotypes of preterm birth syndrome: implications for prevention. JAMA Pediatr. 2015;169(3):220–229.
20. Yuan X, Wang J, Gao Y, Wang H, Yu B. Impact of maternal thyroid hormone in late pregnancy on adverse birth outcomes: a retrospective cohort study in China. Endocr J. 2021;68(3):317–328.
21. Bilgin A, Mendonca M, Wolke D. Preterm Birth/Low Birth Weight and Markers Reflective of Wealth in Adulthood: a Meta-analysis. Pediatrics. 2018;142(1):e20173625.
22. Ashoor G, Poon L, Syngelaki A, Mosimann B, Nicolaides KH. Fetal fraction in maternal plasma cell-free DNA at 11-13 weeks’ gestation: effect of maternal and fetal factors. Fetal Diagn Ther. 2012;31(4):237–243.
23. Samuel A, Bonanno C, Oliphant A, Batey A, Wright JD. Fraction of cell-free fetal DNA in the maternal serum as a predictor of abnormal placental invasion-a pilot study. Prenat Diagn. 2013;33(11):1050–1053.
24. Ashoor G, Syngelaki A, Poon LC, Rezende JC, Nicolaides KH. Fetal fraction in maternal plasma cell-free DNA at 11-13 weeks’ gestation: relation to maternal and fetal characteristics. Ultrasound Obstet Gynecol. 2013;41(1):26–32.
25. Canick JA, Palomaki GE, Kloza EM, Lambert-Messerlian GM, Haddow JE. The impact of maternal plasma DNA fetal fraction on next generation sequencing tests for common fetal aneuploidies. Prenat Diagn. 2013;33(7):667–674.
26. Kinnings SL, Geis JA, Almasri E, et al. Factors affecting levels of circulating cell-free fetal DNA in maternal plasma and their implications for noninvasive prenatal testing. Prenat Diagn. 2015;35(8):816–822.
27. Zhou Y, Zhu Z, Gao Y, et al. Effects of Maternal and Fetal Characteristics on Cell-Free Fetal DNA Fraction in Maternal Plasma. Reprod Sci. 2015;22(11):1429–1435.
28. Scott FP, Menezes M, Palma-Dias R, et al. Factors affecting cell-free DNA fetal fraction and the consequences for test accuracy. J Matern Fetal Neonatal Med. 2018;31(14):1865–1872.
29. Hou Y, Yang J, Qi Y, et al. Factors affecting cell-free DNA fetal fraction: statistical analysis of 13,661 maternal plasmas for non-invasive prenatal screening. Hum Genomics. 2019;13(1):62.
30. Chan N, Smet ME, Sandow R, da Silva Costa F, McLennan A. Implications of failure to achieve a result from prenatal maternal serum cell-free DNA testing: a historical cohort study. BJOG. 2018;125(7):848–855.
31. Suzumori N, Sekizawa A, Ebara T, et al. Fetal cell-free DNA fraction in maternal plasma for the prediction of hypertensive disorders of pregnancy. Eur J Obstet Gynecol Reprod Biol. 2018;224:165–169.
32. Rolnik DL, da Silva Costa F, Lee TJ, Schmid M, McLennan AC. Association between fetal fraction on cell-free DNA testing and first-trimester markers for pre-eclampsia. Ultrasound Obstet Gynecol. 2018;52(6):722–727.
33. Gerson KD, Truong S, Haviland MJ, O’Brien BM, Hacker MR, Spiel MH. Low fetal fraction of cell-free DNA predicts placental dysfunction and hypertensive disease in pregnancy. Pregnancy Hypertens. 2019;16:148–153.
34. Scheffer PG, Wirjosoekarto SAM, Becking EC, et al. Association between low fetal fraction in cell-free DNA testing and adverse pregnancy outcome: a systematic review. Prenat Diagn. 2021;41(10):1287–1295.
35. Quezada MS, Francisco C, Dumitrascu-Biris D, Nicolaides KH, Poon LC. Fetal fraction of cell-free DNA in maternal plasma in the prediction of spontaneous preterm delivery. Ultrasound Obstet Gynecol. 2015;45(1):101–105.
36. Bryant AS, Worjoloh A, Caughey AB, Washington AE. Racial/ethnic disparities in obstetric outcomes and care: prevalence and determinants. Am J Obstet Gynecol. 2010;202(4):335–343.
37. Shi X, Zhang Z, Cram DS, Liu C. Feasibility of noninvasive prenatal testing for common fetal aneuploidies in an early gestational window. Clin Chim Acta. 2015;439:24–28.
38. Goldstein RF, Abell SK, Ranasinha S, et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: a Systematic Review and Meta-analysis. JAMA. 2017;317(21):2207–2225.
39. Haghiac M, Vora NL, Basu S, et al. Increased death of adipose cells, a path to release cell-free DNA into systemic circulation of obese women. Obesity. 2012;20:2213–2219.
40. Rava RP, Srinivasan A, Sehnert AJ, Bianchi DW. Circulating fetal cell-free DNA fractions differ in autosomal aneuploidies and monosomy X. Clin Chem. 2014;60:243–250.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.