")
Back to Journals » Open Access Emergency Medicine » Volume 12
Long−Distance Aeromedical Transport of Patients with COVID−19 in Fixed−Wing Air Ambulance Using a Portable Isolation Unit: Opportunities, Limitations and Mitigation Strategies
Authors Schwabe D, Kellner B, Henkel D , Pilligrath HJ , Krummer S, Zach S , Rohrbeck C, Diefenbach M, Veldman A
Received 11 September 2020
Accepted for publication 24 October 2020
Published 24 November 2020 Volume 2020:12 Pages 411—419
DOI https://doi.org/10.2147/OAEM.S277678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Dirk Schwabe,1 Bernhard Kellner,1 Dirk Henkel,1 Heinz Jürgen Pilligrath,1 Stefanie Krummer,1,2 Sascha Zach,1 Cornelia Rohrbeck,1 Michael Diefenbach,1 Alex Veldman1– 3
1Jetcall GmbH&CoKG, Idstein, Germany; 2Department of Pediatrics, St. Vincenz Hospital, Limburg, Germany; 3Hudson Institute of Medical Research, Monash University, Melbourne, Australia
Correspondence: Alex Veldman
Jetcall GmbH&CoKG, Walramstr. 21, Idstein 65510, Germany
Email [email protected]
Introduction: Aeromedical transport of patients with highly−infectious diseases, particularly over long distances with extended transport times, is a logistical, medical and organizational challenge. Following the 2014– 2016 Ebola Crisis, sophisticated transport solutions have been developed, mostly utilizing large civilian and military airframes and the patient treated in a large isolation chamber. In the present COVID− 19 pandemic, however, many services offer aeromedical transport of patients with highly−infectious diseases in much smaller portable medical isolation units (PMIU), with the medical team on the outside, delivering care through portholes.
Methods: We conducted a retrospective review of all transports of patients with proven or suspected COVID− 19 disease, transported by Jetcall, Idstein, Germany, between April 1 and August 1, 2020, using a PMIU (EpiShuttle, EpiGuard AS, Oslo, Norway). Demographics and medical data were analyzed using the services’ standardized transport protocols. Transport−associated challenges and optimization strategies were identified by interviewing and debriefing all transport teams after each transport.
Results: Thirteen patients with COVID− 19 have been transported in a PMIU over distances up to 7,400 kilometers (km), with flight times ranging from 02:15 hours to 11:10 hours. We identified the main limitations of PMIU transports as limited access to the patient and reduced manual dexterity when delivering care through the porthole gloves and disconnection of lines and tubes during loading and unloading procedures. Technical solutions such as bluetooth−enabled stethoscopes, cordless ultrasound scanners and communication devices, meticulous preparation of the PMIU and the patient following standardized protocols and scenario−based training of crew members can reduce some of the risks.
Discussion: Transporting a patient with COVID− 19 or any other highly infectious disease in a PMIU is a feasible option even over long distances, but adding a significant layer of additional risk, thus requiring a careful and individualized risk−benefit analysis for each patient prior to transport.
Keywords: highly infectious diseases, COVID− 19, transportation, portable medical isolation unit, aircraft
Introduction
During the present global COVID−19 pandemic, and also during previous Public Health Emergencies of International Concern like the 2014–2016 West African Ebola Crisis, safe transport of patients affected by highly infectious diseases has become a unique challenge for which a wide array of solutions has been developed.
Transport of a COVID−19 infected patient in the confined environment of an ambulance, helicopter or aircraft might be a particularly difficult task, especially over long distances with prolonged transport times. Experimental studies in a laboratory−controlled environment demonstrated that aerosolized SARS−CoV−2 particles (<5 µm) remained suspended in the air for at least 3 hours, viable in air for at least 1 hour, and on surfaces for up to days.1
In this retrospective study, we report on our experience using a portable medical isolation unit (PMIU) for long−distance fixed−wing air ambulance repatriation of 13 patients with COVID−19 and briefly review alternative options. Risks of a PMIU transport are identified and mitigation strategies proposed.
Methods
- Retrospective review of all transports of patients with proven or suspected COVID−19 disease, transported by Jetcall, Idstein, Germany, a EURAMI (European Aeromedical Institute) accredited Air Ambulance company, between April 1 and August 1, 2020; using a PMIU (EpiShuttle; EpiGuard AS, Oslo, Norway).
- Retrospective analysis of demographics (age, sex), transport specific data (point of origin, destination, flight time, number of fuel stops, cabin pressure) and medical data using the services’ standardized transport protocols.
- Analysis of transport−associated challenges and optimization strategies by interviewing and debriefing all transport teams after each transport.
Transport System
All patients were transported using a Bombardier Challenger 604 long distance air ambulance aircraft and the EpiShuttle PMIU (EpiGuard AS, Oslo, Norway). Patients were loaded head−first into the aircraft and transported with the head towards the rear of the fuselage to guarantee best access to the head portholes (see Figure 1). The PMIU was fixed on a Spectrum Aeromed 20/2200 Stretcher Base Module during the transport (Spectrum Aeromed, Fargo, ND, USA). Standard Air Ambulance equipment, including advanced monitoring (oxygen saturation (SaO2), heart rate (HR), invasive and non−invasive blood pressure (BP), temperature), ventilator, suction pump, infusion pumps and syringe drivers, portable blood gas analyzer and portable ultrasound, a wide array of intravenous and oral medications was available on board.
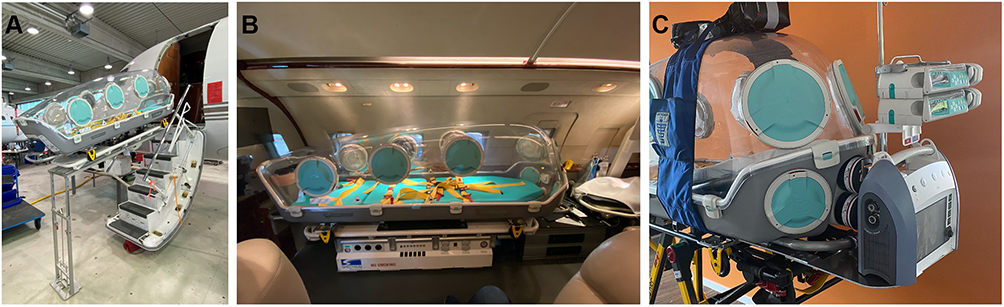 |
Figure 1 EpiShuttle PMIU in a Bombardier Challenger 604 Air Ambulance Jet. Panel (A) Loading/Unloading of the EpiShuttle PMIU. Panel (B) The EpiShuttle PMIU in the Cabin of the Challenger 604. Panel (C) Equipment “Rack” at the Head End of the EpiShuttle PMIU and “Saddle” to prevent disconnection of lines, ventilation tubes and monitoring during loading and unloading. |
Transport Teams
Transport teams consisted of three medical team members (1 physician and 2 nurses or 2 physicians and 1 nurse) and two or three pilots (number of pilots depending on distance and transport times). Physicians and nurses were critical care experienced and qualified and underwent theoretical and practical training on the PMIU according to the instructions by the manufacturer.
Preparation of the PMIU
The PMIU was leak−tested according to the instructions by the manufacturer prior to each deployment. During the outbound sector of the flight towards the takeover point, the PMIU was prepared with all lines, cables, tubes and cables threaded through the wireport, blocked and secured, using a standardized checklist (Box 1). Prior to loading the patient, a “contaminated” and a “clean” side of the PMIU were defined and the contaminated side covered with a large, adhesive single use blanket. The medical crew in full personal protective equipment (PPE) loaded the patient from this side and after securing all lines, tubes and monitoring cables, the blanket was removed and discarded. The PMIU was closed and the outside thoroughly disinfected, the medical crew then discarded their PPE. After unloading the patient at the destination (process reverse to the above), the PMIU was again closed, the outside thoroughly disinfected, and transported to the Operations Base to be cleaned, disinfected and prepared for the next transport by trained personnel according to the instructions supplied by the manufacturer. The aircraft was disinfected after each transport with peroxide swipes and nebulizer.2
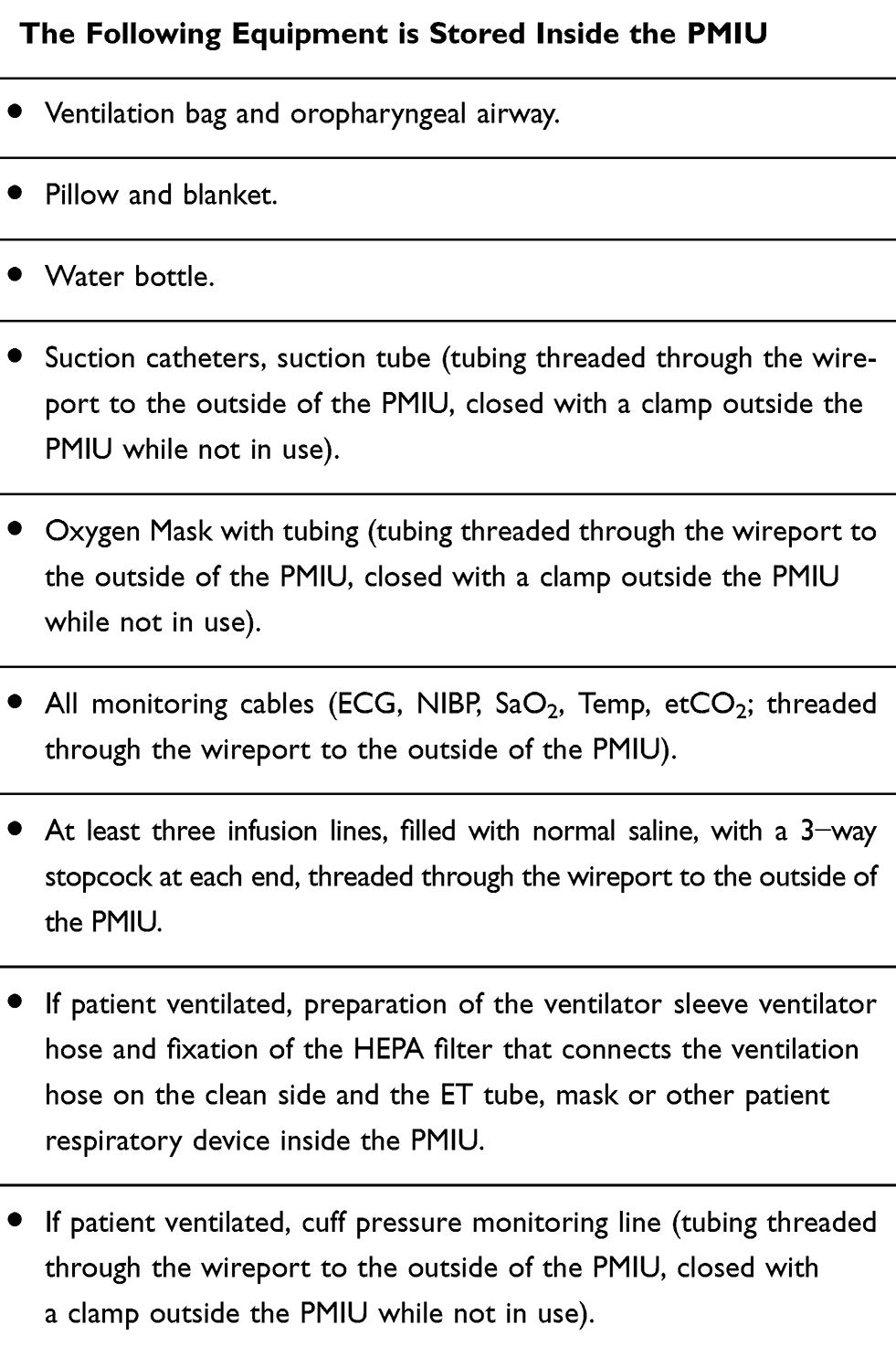 |
Box 1 Checklist PMIU Preparation Prior to Patient Loading |
Preparation of the Patient
Optimal preparation of the patient prior to loading into and closing of the PMIU was communicated with the treating hospital/via the assistance company following a standardized checklist on the day before the transport (Box 2). All personal belongings and luggage of the patient, as well as the medical report were placed in large plastic bags and sealed prior to transport.
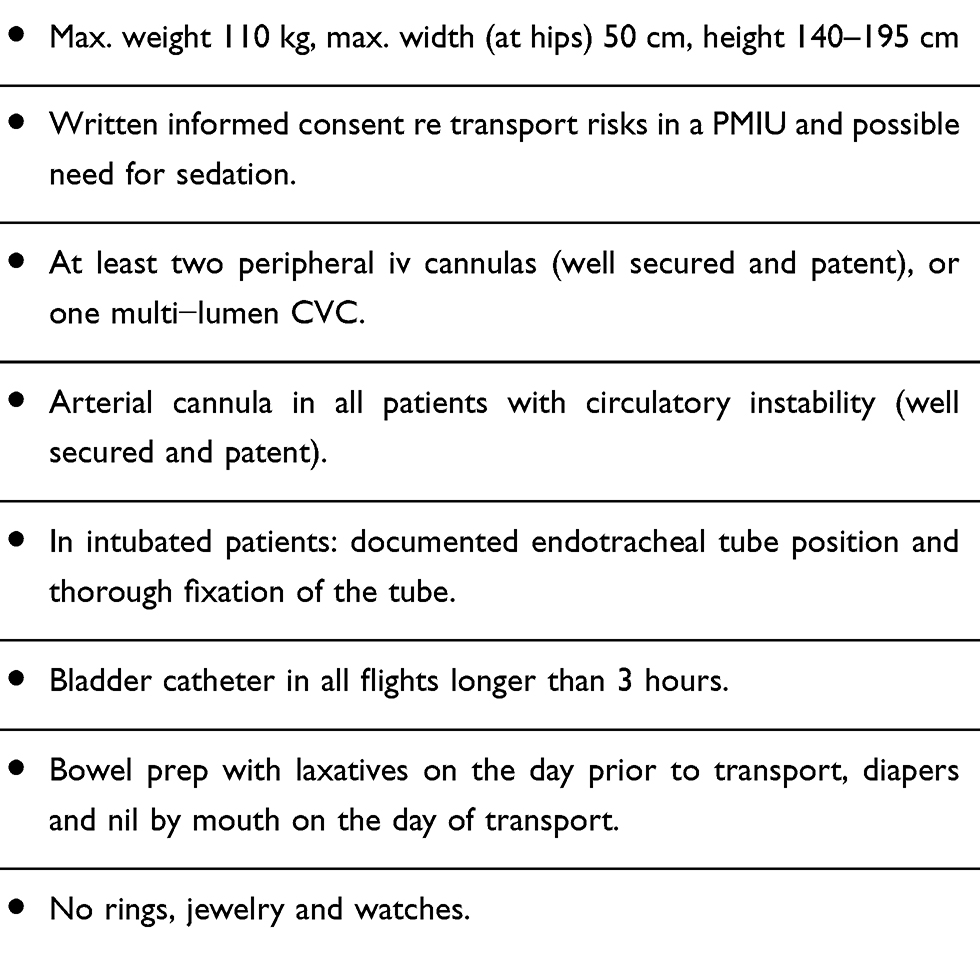 |
Box 2 Checklist PMIU Patient Preparation |
Institutional Review Board
The project plan was presented to the Ethics Review Board of the German (Hessen) Chamber of Physicians in Frankfurt/Germany, who granted an exemption of formal Ethics Board Review and a waiver of patient informed consent due to the retrospective nature of the analysis without any interventions imposed on the patient by the analysis. The principles of the Declaration of Helsinki and data confidentiality were followed throughout the conduct of this retrospective analysis.
Results
A total of 13 patients have been scheduled for aeromedical transport with one of those not being released from the hospital after arrival of the air ambulance at the pick−up point, resulting in an aborted mission. This patient subsequently died in the referring hospital. All 12 patients who boarded the aircraft survived the transport, with major adverse events (AEs) occurring in one patient (inadvertent inward movement of the endotracheal tube despite fixation of the tube with a Thomas Tube Holder, with subsequent one−sided intubation, hypercapnia and respiratory acidosis).
Median flight time was 08:00 hours (range 02:15–11:00 hours), with a median distance of 5,110 km covered (range 1563 km to 7412 km). Table 1 depicts patient and transport characteristics of all transports, including the aborted mission. No crewmember (medical crew or flight crew) developed signs and symptoms of COVID−19 disease within 14 days after each transport.
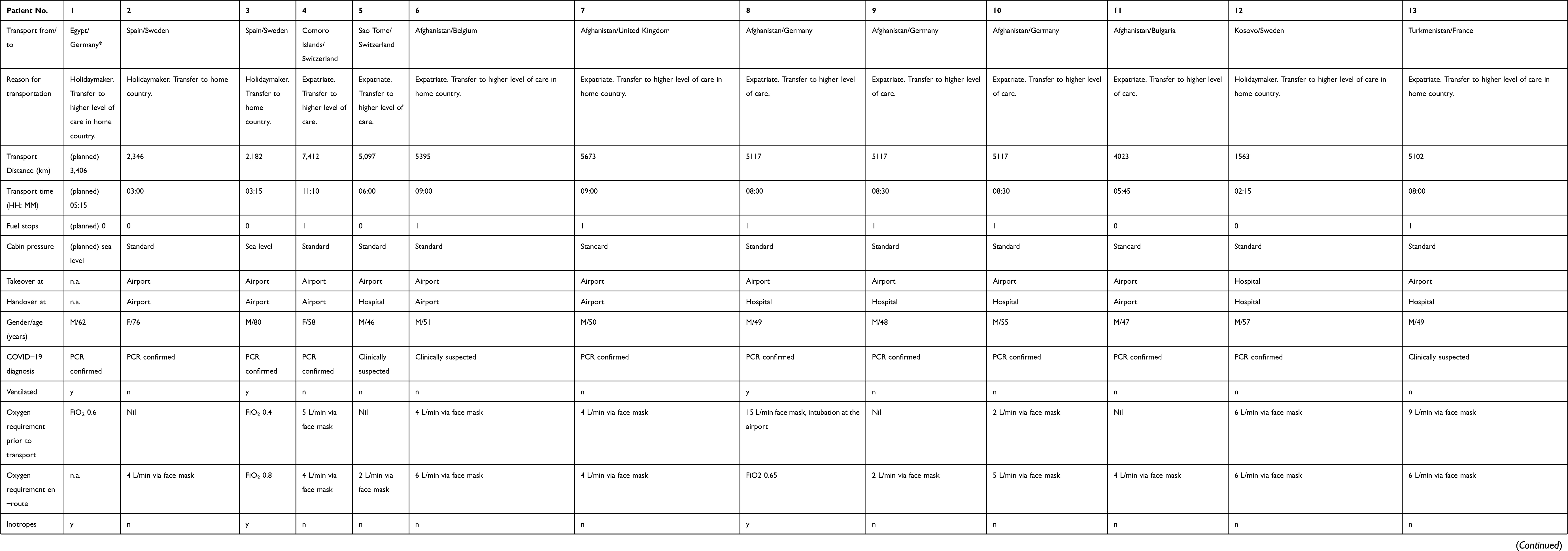 |
Table 1 Patient and Transport Characteristics |
Debriefing sessions revealed a couple of challenges for which subsequently mitigation strategies have been developed; these are listed in Table 2. Checklists for preparing the PMIU and a checklist for preparing the patient for transport in the PMIU have been created in this process, see Boxes 1 and 2.
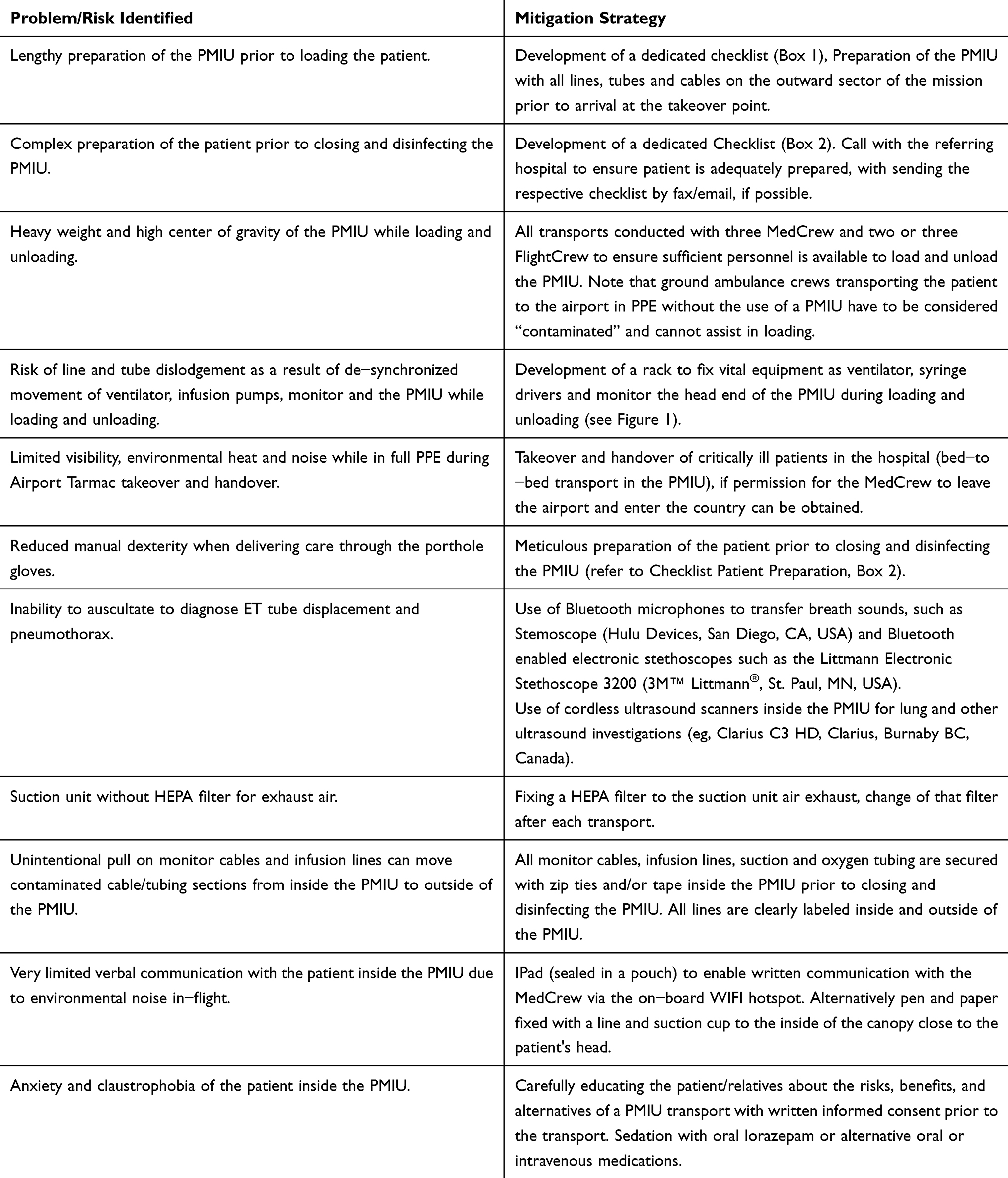 |
Table 2 Main Challenges Identified During PMIU Transports and Mitigation Strategies |
Discussion
Movement of patients with highly infectious diseases between hospitals is a technical, logistical and medical challenge with significant risks for the safety of the patient, the crew, and the public. The safety of such transports, specifically during the present COVID−19 pandemic, is an area of growing interest and concern and has prompted calls for standardized guidelines in the past.3,4 In response to previous Public Health Emergencies of International Concern, mostly hemorrhagic fevers such as Ebola and Lassa, a multitude of transport solutions have been developed, many of those with the military or government/public health agencies involved.5–11
Aeromedical transport solutions for highly infectious patients are available as open and closed systems. In open systems, the medical crew is entering a negative pressure isolation unit (container) via an air lock wearing full PPE, sometimes including a positive pressure suit, while inside the unit. Such concepts have been developed for the use in road ambulances and aircraft.12,13 The large volume of the unit requires unique engineering solutions for the use in pressurized aircraft – such as large equalizing tanks to store the explosively expanding air in the case of rapid cabin decompression. The size and weight of open systems are prohibitive for the use in rotary wing aircraft and require large civilian or military fixed wing aircraft as transport platforms.13,14
In closed systems, the patient is isolated in a smaller negative pressure isolation chamber, with the medical crew outside that chamber. Patients can be treated/manipulated with gloves that are fixed to several portholes in the wall of the isolation chamber. Lines for infusions and cables for monitoring, as well as ventilation and oxygen tubes are threaded through specifically designed ports. A small air lock with a disinfection port allows the movement of small equipment in and out of the chamber. Several soft−shell (eg. IsoArk, BethEl Group, Zikhron Yaaqov, Israel; Portable Isolator (IZO.04), LAMSYSTEMS CC, Miass, Russia; CAPSULS™, ISOVAC Products LLC, Romeoville, IL USA; Portable Isolation Bed CIB−2000S, NK Systems, Osaka, Japan; Adult Pic – Portable Isolation Chamber, Securotec, Tarare, France) and hard−shell chambers (EpiShuttle, EpiGuard AS, Oslo, Norway; Portable Isolation Chamber, ATA Medical, Orvault, France) are available today. The hard−shell PMIU used in the case series reported here has been tested and approved for the use in fixed− and rotary−wing air ambulances, including testing for integrity during rapid decompression and flotation in case of emergency landings on water, while some soft−shell PMIUs have been reported to leak internal air in the event of a rapid decompression, which prompted individual design solutions such as air bags for air volume expansion.9,15
One may speculate that open systems allow easier access to the patient and thus enable safer care for critically ill patients, however, prohibitive high costs of open systems due to the need of a larger airframe compared to a PMIU may be a limiting factor, specifically in large scale global pandemics such as the current COVID−19 situation. In our experience, the majority of transfers of moderately to severely ill patients in the present COVID−19 pandemic are carried out by private air ambulance providers, rather than military and government bodies, with the focus shifting from open transport systems towards more cost−effective closed PMIU based solutions for the majority of these transports.9,16–19 However, transport of COVID−19 patients in a container−based open system that is loaded in a Boeing 747 and capable of transporting multiple patients in a single mission has also been described recently.20 On the other end of the spectrum, Cornelius et al20 described a mass evacuation of COVID−19 patients who were asymptomatic or showed only mild symptoms in the regular cabin of chartered airliners with the crew wearing PPE.21 This highlights the need for careful consideration of the patient’s individual condition, number of patients to be transported, transport distance and available options to find the safest and most cost−effective option. While the older CDC’s Guidance for Air Medical Transport of Severe Acute Respiratory Syndrome Patients and the Guidance on Air Medical Transport for Middle East Respiratory Syndrome Patients as well as the regional guidelines such as the AirMed guideline published on the Association of Air Medical Services (AAMS) website and others might offer some advice, there is currently no specific guideline on the use of (or the need to use) a PMIU for a COVID−19 infected air ambulance patient. Regardless of the transport system employed (aeromedical or ground ambulance based), transportation in a PMIU is costly. PMIUs are available from approximately 4,500.− USD onwards for a very simple soft−shell model to more than 40,000.− USD for an advanced hard−shell PMIU. In addition to the purchase, consumables such as air filters and seals, as well as complicated disinfection procedures further contribute to high operating costs. As a result, such systems might not be available for the majority of COVID−19 patients in the developing world, highlighting the need to better understand the risk of transporting – and attending to – a COVID−19−infected patient in a resource−limited environment.22
Indeed, there are several risks in transporting a moderately to severely ill patient in a PMIU. Not surprisingly, we identified the main challenges around limited access to the patient and reduced manual dexterity when delivering care through the porthole gloves. In our case series, we experienced a serious adverse event of endo−tracheal (ET) tube mal−positioning in one ventilated patient. While the medical crew noted the hypercapnia and respiratory acidosis and discussed a one−sided intubation as the root cause, the inability to auscultate the patient made an at−risk manipulation of the ET tube a highly unsafe procedure. While some authors report that emergency airway management, including cricothyrotomy, is achievable inside a closed PMIU at least in simulations, we would challenge the ability to handle possible complications of intubation and cricothyrotomy and strongly believe that such maneuvers are best to be avoided by meticulous preparation of the patient before closing the unit.23 In the follow−up we developed technical solutions such as Bluetooth−equipped electronic stethoscopes and cordless ultrasound scanners, which can overcome some but not all of these problems. Disconnection of ventilation circuits, intravenous and arterial lines and monitoring cables due to un−synchronized movement of the very heavy PMIU (approx. 80 kg plus patient body weight) and ventilator, infusion pumps, and monitor are other hazards, particularly during loading and un−loading of the patient in and off the aircraft. We developed a “rack and saddle” solution (Figure 1), that, at least on our limited experience, effectively prevented disconnection in this critical phase of the transport. Positioning of a patient in a PMIU is limited (with a risk of pressure sores on long transports) and prone positioning of ventilated patients is impossible. Finally, spending prolonged periods of time in the close confinement of a PMIU is unpleasant for the patient and did require some sedation in almost all cases – a fact that we integrated in a procedural informed consent describing the nature, procedures and risks of transportation in an PMIU that patients/relatives signed on the day before the transport. Relatives are not permitted on board, however, in special circumstances accompanying relatives might be considered when tested negative for COVID−19 within 48 hours prior to transport.
This case series has some obvious limitations. Most importantly, we report only on the use of one single type of PMIU, while several models are available on the market today. However, the two main risks around challenges delivering care though porthole gloves and preventing disconnection of critical equipment while moving the PMIU are likely independent of manufacturer and type. Also, we cannot directly compare patient safety in open and closed systems – although it is reasonable to believe that the much greater access to the patient in an open system would translate to more procedural ability in managing acute deterioration of a critically ill patient. A prospective study could have integrated a more detailed assessment of illness severity prior to transport and protocolized assessments of physiological parameters of the patient and also the transport team during the transport. This should be addressed in future studies.
Whatever system is used, training of crew on delivering care in the PMIU is essential. The lack of training of medical personnel in working in full PPE and with various isolation systems has been identified as an area of concern previously and requires scenario−based training exercises.24,25 In 2019, Gibbs et al26 conducted a comprehensive review of the literature on High−Level Containment Aeromedical Transport, mostly in open systems utilizing large military transport airframes, such a Boeing C−17 or Lockheed C−130.26 In their excellent paper, the authors perform a detailed analysis of the published operational aspects and protocols on highly infectious disease transports published mainly in the wake of the Ebola outbreak, with a focus on many important pre− and post−transport aspects that go beyond the scope of this paper.
In conclusion, transporting a patient with COVID−19 in a PMIU is a feasible and, compared to open systems, cost−effective option even over long distances; however, such transportation adds significant additional risk which could proportionally increase with the complexity and seriousness of a patient’s condition and, to some extent, the length of air−transportation. Meticulous preparation of equipment and patient using standardized protocols and checklists, the use of wireless technology to transmit as much physiologic data from the inside of the PMIU to the outside and training and simulation sessions with transport teams can mitigate some, but not all of the transport−specific risks. Therefore, the risk− benefit balance of transporting a patient versus local care needs to be carefully considered. The most critically ill patients, who despite a foreseeable high frequency of interventions during the transport still need to be moved over great distances, may be better suited for interhospital transfer in open than in closed transport systems.
Acknowledgments
We gratefully acknowledge the sound technical support and excellent training on the EpiShuttle PMIU provided by Thomas Hissin, Hissin Medizintechnik, Oberursel, Germany.
Disclosure
All authors are shareholders of and/or employed full− or part−time by Jetcall GmbH&CoKG and as such receive an honorarium or salary. Specifically, Dirk Schwabe, Bernhard Kellner, Heinz Jürgen Pilligrath, Stefanie Krummer, Cornelia Rohrbeck and Alex Veldman report salary from Jetcall, outside the submitted work and Michael Diefenbach reports salary from and is a shareholder of Jetcall, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Chirico F, Sacco A, Bragazzi NL, Magnavita N. Can air−conditioning systems contribute to the spread of SARS/MERS/COVID−19 infection? Insights from a rapid review of the literature. Int J Environ Res Public Health. 2020;17(17):6052. doi:10.3390/ijerph17176052
2. Klaus J, Gnirs P, Holterhoff S, et al. Disinfection of aircraft: appropriate disinfectants and standard operating procedures for highly infectious diseases. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2016;59(12):1544–1548. doi:10.1007/s00103−016−2460−2
3. Liew MF, Siow WT, Yau YW, See KC. Safe patient transport for COVID−19. Crit Care. 2020;24(1):94. doi:10.1186/s13054−020−2828−4
4. Gibbs SG, Herstein JJ, Le AB, et al. Need for aeromedical evacuation high−level containment transport guidelines. Emerg Infect Dis. 2019;25(5):1033–1034. doi:10.3201/eid2505.181948
5. Ewington I, Nicol E, Adam M, Cox AT, Green AD. Transferring patients with ebola by land and air: the British military experience. J R Army Med Corps. 2016;162(3):217–221. doi:10.1136/jramc−2016−000623
6. Christopher GW, Eitzen EM. Air evacuation under high−level biosafety containment: the aeromedical isolation team. Emerg Infect Dis. 1999;5(2):241–246. doi:10.3201/eid0502.990208
7. Lotz E, Raffin H. Aeromedical evacuation using an aircraft transit isolator of a patient with lassa fever. Aviat Space Environ Med. 2012;83(5):527–530. doi:10.3357/ASEM.3094.2012
8. Nicol ED, Mepham S, Naylor J, et al. Aeromedical transfer of patients with viral hemorrhagic fever. Emerg Infect Dis. 2019;25(1):5–14. doi:10.3201/eid2501.180662
9. Albrecht R, Knapp J, Theiler L, Eder M, Pietsch U. Transport of COVID−19 and other highly contagious patients by helicopter and fixed−wing air ambulance: a narrative review and experience of the swiss air rescue rega. Scand J Trauma Resusc Emerg Med. 2020;28(1):40. doi:10.1186/s13049−020−00734−9
10. Tsai SH, Chen WL, Chiu WT. International aeromedical evacuation. N Engl J Med. 2007;356(16):1685–1687.
11. Biselli R. Aeromedical evacuation of pateints with hemorrhagic fevers: the experience of Italian air force aeromedical isolation team. J Hum Virol Retrovirol. 2015;2(5):0058. doi:10.15406/jhvrv.2015.02.00058
12. Schilling S, Follin P, Jarhall B, et al. European concepts for the domestic transport of highly infectious patients. Clin Microbiol Infect. 2009;15(8):727–733. doi:10.1111/j.1469−0691.2009.02871.x
13. MRI Global. Coronavirus evacuees return safely to U.S. via innovative, MRIGlobal−designed biocontainment system; 2020. Available from: https://www.ptcommunity.com/wire/coronavirus−evacuees−return−safely−us−innovative−mriglobal−designed−biocontainment−system.
14. Phoenix Air Group. Contagious disease transport; 2020. Available from: https://phoenixair.com/air−ambulance/contagious−disease−transport/.
15. Albrecht R, Kunz A, Voelckel WG. Airplane transport isolators may loose leak tightness after rapid cabin decompression. Scand J Trauma Resusc Emerg Med. 2015;23(1):16. doi:10.1186/s13049−015−0090−6
16. BBC. Capital air: the isolation bag for coronavirus patients; 2020. Available from: https://www.bbc.com/news/av/uk−england−devon−52337069/capital−air−the−isolation−bag−for−coronavirus−patients.
17. Jetflite. Air ambulance service during the COVID−19 outbreak; 2020. Available from: https://www.jetflite.fi/en/air-ambulance/corona/.
18. FAI. Transportation options for coronavirus patients; 2020. Available from: https://www.fai.ag/air−ambulance/transportation−option−for−coronavirus−patients/.
19. Luxembourg Air Rescue. COVID−19: weekend update: LAR transports five more patients; 2020. https://www.lar.lu/en/media/lar−media−presence/media−details/2020/04/covid−19−bilan−du−week−end−lar−a−transporte−5−autres−patients−covid−19.
20. The Drive. 747 carrying Americans exposed to Coronavirus used new quarantine box for infected flyers; 2020. Available from: https://www.thedrive.com/the−war−zone/32248/747s−carrying−americans−exposed−to−coronavirus−used−new−quarantine−box−for−infected−flyers.
21. Cornelius B, Cornelius A, Crisafi L, et al. Mass air medical repatriation of Coronavirus disease 2019 patients. Air Med J. 2020;39(4):251–256. doi:10.1016/j.amj.2020.04.005
22. Magnavita N, Sacco A, Nucera G, Chirico F. First aid during the COVID−19 pandemic. Occup Med (Lond). 2020;70(7):458–460. doi:10.1093/occmed/kqaa148
23. Plazikowski E, Greif R, Marschall J, et al. Emergency airway management in a simulation of highly contagious isolated patients: both isolation strategy and device type matter. Infect Control Hosp Epidemiol. 2018;39(2):145–151. doi:10.1017/ice.2017.287
24. Le AB, Buehler SA, Maniscalco PM, et al. Determining training and education needs pertaining to highly infectious disease preparedness and response: a gap analysis survey of US emergency medical services practitioners. Am J Infect Control. 2018;46(3):246–252. doi:10.1016/j.ajic.2017.09.024
25. Coignard−Biehler H, Isakov A, Stephenson J. Pre−hospital transportation in Western countries for ebola patients, comparison of guidelines. Intensive Care Med. 2015;41(8):1472–1476. doi:10.1007/s00134−015−3734−0
26. Gibbs SG, Herstein JJ, Le AB, et al. Review of literature for air medical evacuation high−level containment transport. Air Med J. 2019;38(5):359–365. doi:10.1016/j.amj.2019.06.006
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.