")
Back to Journals » International Medical Case Reports Journal » Volume 12
Longitudinal follow-up of two patients with isolated paracentral acute middle maculopathy
Authors Nakamura M, Katagiri S , Hayashi T, Aoyagi R, Hasegawa T, Kogure A, Iida T, Nakano T
Received 26 November 2018
Accepted for publication 15 March 2019
Published 6 May 2019 Volume 2019:12 Pages 143—149
DOI https://doi.org/10.2147/IMCRJ.S196047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Masaki Nakamura,1 Satoshi Katagiri,1 Takaaki Hayashi,1,2 Ranko Aoyagi,1 Taiji Hasegawa,3 Akiko Kogure,3 Tomohiro Iida,3 Tadashi Nakano1
1Department of Ophthalmology, The Jikei University School of Medicine, Tokyo, Japan; 2Department of Ophthalmology, Katsushika Medical Center, The Jikei University School of Medicine, Tokyo, Japan; 3Department of Ophthalmology, Tokyo Women’s Medical University, Tokyo, Japan
Objective: To describe longitudinal retinal changes in two cases of isolated paracentral acute middle maculopathy (PAMM).
Case series: We reported two cases (64 and 67-year-old men) with isolated PAMM, who were followed-up for over 5 and 2.5 years, respectively. Both cases exhibited similar clinical natural histories. The first examinations took place several days after onset, with funduscopy showing that both cases exhibited paracentral scotoma with good visual acuity and small gray lesions, while optical coherence tomography (OCT) showed the presence of a hyperreflective band that ranged from the inner plexiform layer to the outer plexiform layer (OPL). The lesions became unremarkable within 1 month. The hyperreflective band also became unremarkable and was limited to the inner nuclear layer (INL) within 1 month, with the band disappearing within several months. Subsequently, OCT showed there was a thin and irregular INL and OPL, an excavated change of the inner retinal surface, along with outer nuclear layer (ONL) thickening. After several years, OCT angiography demonstrated normal flow of macular capillaries in the superficial capillary plexus, and decreased flow in the lesion with dilation of the capillaries around the area in the deep capillary plexus (DCP). Focal serous retinal detachment (SRD) occurred in one case after 4–5 years.
Conclusion: Our findings indicated that long-term retinal changes in PAMM resulted in excavation of the inner retinal surface, INL thinning, ONL thickening and abnormal vasculature, especially in the DCP. Focal SRD may be a rare complication that can present at 4 years after onset.
Keywords: paracentral acute middle maculopathy, optical coherence tomography angiography, serous retinal detachment
Introduction
Paracentral acute middle maculopathy (PAMM), which was originally described in the literature in 2013, is a retinal disease with characteristic optical coherence tomography (OCT) findings of a hyperreflective band mainly in the inner nuclear layer (INL).1,2 Intermediate and deep capillary plexuses (DCP) are found throughout the INL, with ischemia of these plexuses considered to be a cause of PAMM.1,2 Recent developments in OCT angiography (OCTA) have allowed ophthalmologists to separately visualize the superficial capillary plexus (SCP) and the DCP. As a result, this has made it possible to demonstrate that ischemia in the DCP is the mechanism responsible for causing PAMM.3,4
Both OCT and OCTA have been used to study retinal structural changes and the vasculature in PAMM.1,2 These studies have clarified that the lesions of isolated PAMM develop a normal retinal appearance within several weeks, with the hyperreflective band in the INL becoming inconspicuous within several months.1,2 To date, however, little is known about the long-term prognosis of the retinal structure and vasculature in patients with isolated PAMM.
Here, we described the longitudinal retinal changes of two cases with isolated PAMM lesions. The purpose of this report was to clarify the long-term prognosis of the retinal structure and vasculature in isolated PAMM.
Case series
Case 1
A 64-year-old man with no history of ophthalmic disease reported paracentral scotoma in his left eye 4 days before his first visit. The patient’s medical history included hypertension and hyperuricemia. At his first visit, decimal best-corrected visual acuity (BCVA) was 1.5 in both eyes (with −7.00 diopter (D), cylinder (cyl) −1.00 D axis (Ax) 40° in the right and −7.00 D cyl. −1.00 D Ax 150° in the left eye). No remarkable findings were observed in the anterior segment and media in either eye. Funduscopy showed a small dark gray lesion supero-nasal to the fovea in the left eye (Figure 1A). B-scan OCT (Cirrus HD-OCT; Carl Zeiss Meditec AG, Dublin, CA, USA) showed a hyperreflective band ranging from the inner plexiform layer (IPL) to the outer plexiform layer (OPL), which corresponded to the fundus lesion (Figure 1A). Fluorescein angiography (FA) showed no remarkable findings in either of his eyes, while indocyanine green angiography (ICGA) in the late phase showed a transmission defect that corresponded to the fundus lesion (data not shown). Visual field testing using a Humphrey Visual Field Analyzer (HFA) (Carl Zeiss Meditec AG) showed decreased sensitivities in the infero-temporal area of the left eye (data not shown).
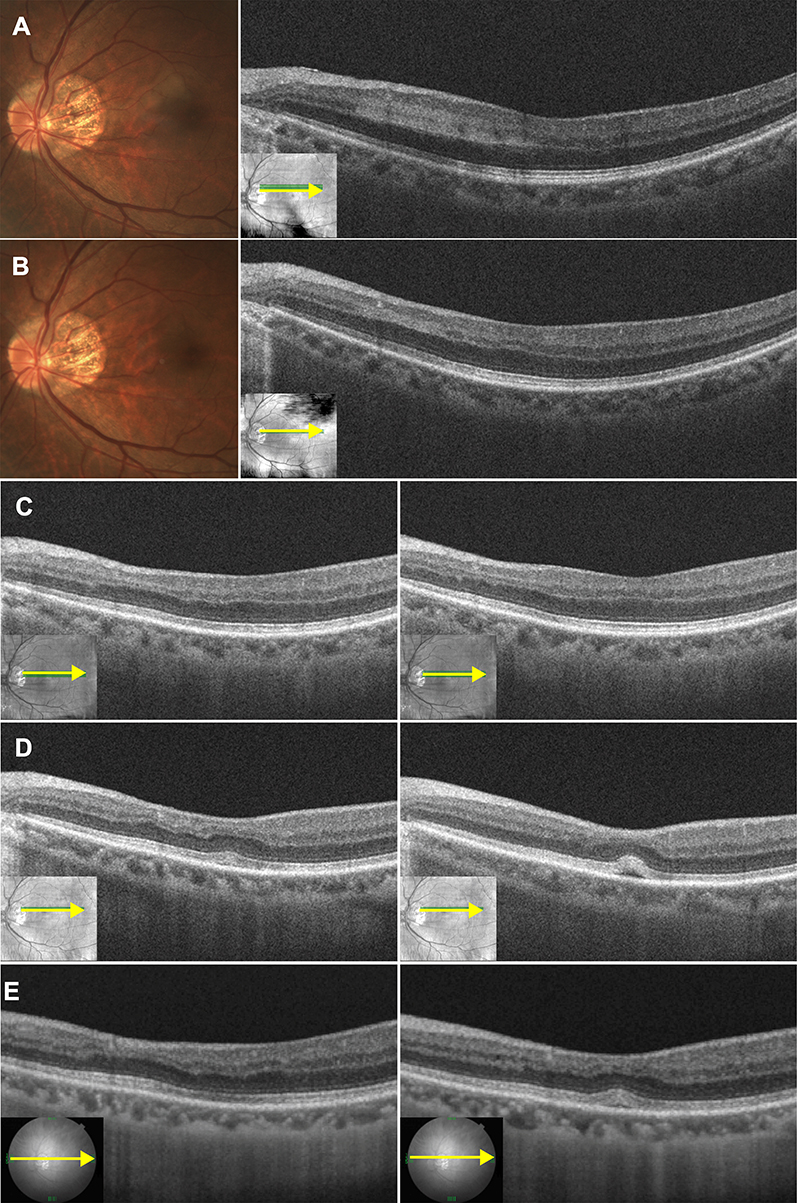 | Figure 1 Fundus photographs and B-scan OCT images of the left eye in case 1. Images were obtained at the first examination (4 days after the onset) (A), and then at 1 month (B), 6 months (C), 4 years (D), and 5 years (E). (A) Fundus photograph shows a small dark gray lesion supero-nasal to the fovea. OCT shows a hyperreflective band ranging from the inner plexiform layer to the OPL, which corresponded to the fundus lesion. (B) Fundus photograph shows there was a gradual disappearance of the lesion. OCT showed that the hyperreflective band was limited to the thinned inner nuclear layer. (C) OCT revealed there was a thin and irregular inner nuclear layer and OPL with the hyperreflective change no longer present. (D and E) Additional OCT images show the presence of focal serous retinal detachment, with an excavated change of the inner retinal surface and thickening of the outer nuclear layer. Abbreviations: OCT, optical coherence tomography; OPL, outer plexiform layer. |
The patient was followed-up at 1 month (Figure 1B), 6 months (Figure 1C), 4 years (Figure 1D) and 5 years (Figure 1E) after the onset. Funduscopy showed that the lesion gradually disappeared after 1 month. OCT showed that the hyperreflective band was limited to the thinned INL. After 6 months, however, OCT revealed that the thin and irregular INL and OPL no longer exhibited the hyperreflective change. After 4 years, OCT showed that there was focal serous retinal detachment (SRD) in addition to the thin and irregular INL and OPL, an excavated change of the inner retinal surface, and ONL thickening. At 5 years after the onset, OCT showed that these retinal changes still remained. Evaluation by OCTA (DRI OCT-1 Atlantis, Topcon Corporation, Tokyo, Japan) after 5 years showed there was normal flow of the macular capillaries in the SCP, and a decreased flow in the area of the lesion, with a slight dilation of the capillaries around the lesion in the DCP (Figure 2A). In addition, the patient’s subjective symptom of paracentral scotoma remained after 5 years.
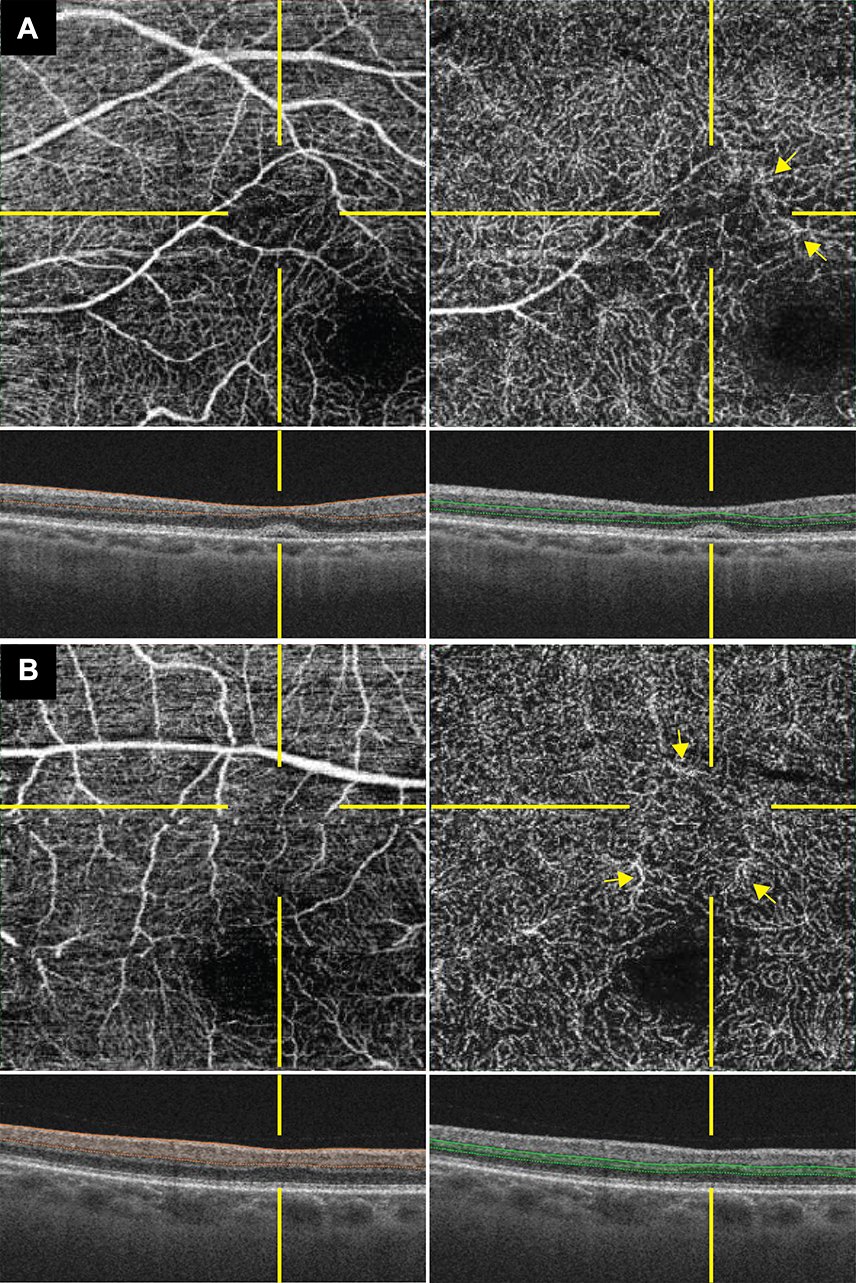 | Figure 2 OCTA images during the chronic phase in cases 1 and 2. The OCTA images were obtained at 5 years after the onset in case 1 (A) and at 2.5 years after the onset in case 2 (B). The left column shows the superficial capillary plexus (SCP) images while the right column shows the DCP images. OCTA images of both cases revealed there was normal flow of the macular capillaries in the SCP, and a decreased flow in the PAMM lesion, with dilation of the capillaries (yellow arrows) around the lesion in the DCP. Abbreviations: OCTA, optical coherence tomography angiography; SCP, superficial capillary plexus; DCP, deep capillary plexus; PAMM, paracentral acute middle maculopathy. |
Case 2
A 67-year-old man with no history of ophthalmic disease reported inferior paracentral scotoma in his right eye at 5 days prior to his first visit. The patient’s medical history included hypertension and hyperlipidemia. At his first visit, BCVA was 1.5 in both eyes (with −11.00 D cyl. −0.50 D Ax 110° in the right and −8.00 D cyl. −1.00 D Ax 115° in the left eye). No remarkable findings were observed in the anterior segment and media in either of his eyes. Funduscopy showed there was a small dark gray lesion just superior to the fovea in his right eye (Figure 3A). B-scan OCT showed a hyperreflective band ranging from the IPL to OPL, which corresponded to the fundus lesion (Figure 3A). FA showed no remarkable findings in either eye, while ICGA in the late phase showed there was a transmission defect that corresponded to the lesion (data not shown).
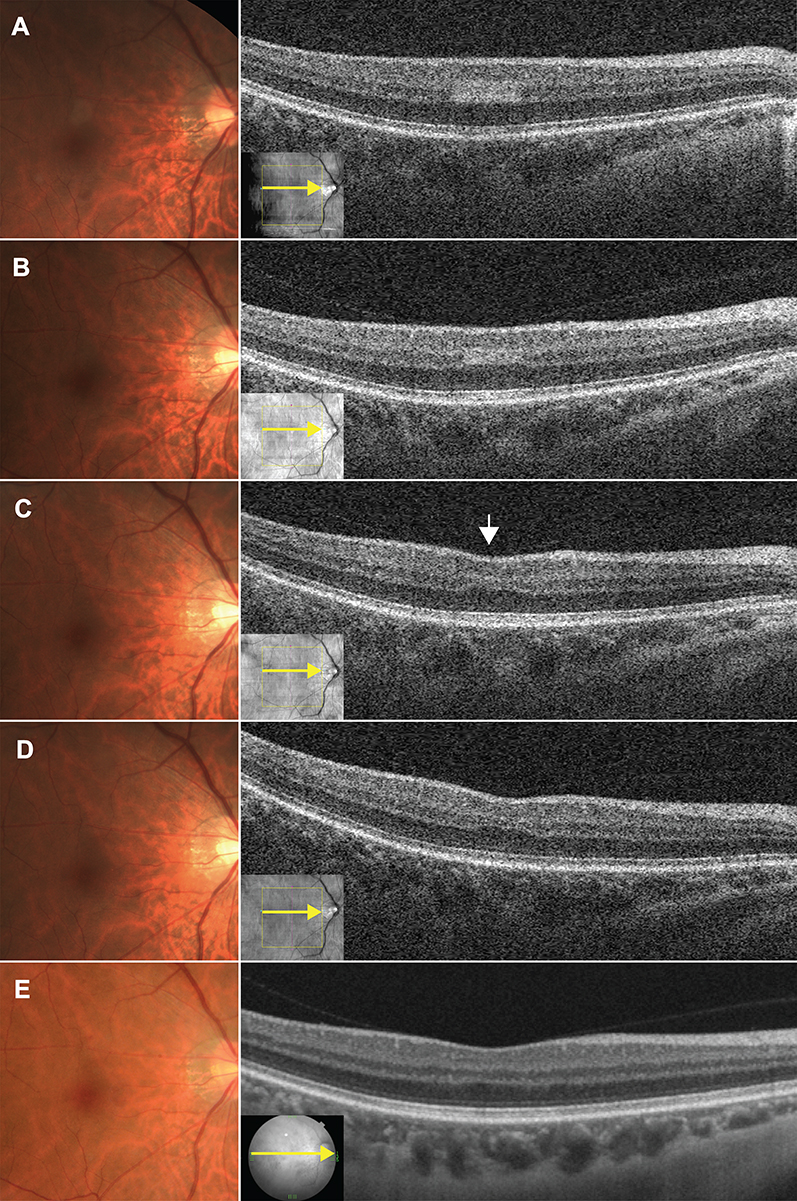 | Figure 3 Fundus photographs and OCT B-scan images of the right eye in case 2. The images were obtained at the first examination (5 days after the onset) (A), and at 3 weeks (B), 4 months (C), 1.5 years (D), and 2.5 years (E). (A) Fundus photograph shows a small dark gray lesion just superior to the fovea. OCT shows a hyperreflective band that ranges from the inner plexiform layer to the OPL, and which corresponded to the fundus lesion. (B) Funduscopy shows there was a gradual disappearance of the lesion. OCT revealed that the hyperreflective band was limited to the INL with slight thinning. (C) OCT also showed there was a thin and irregular INL and OPL that no longer exhibited a hyperreflective change, an excavated change of the inner retinal surface (arrow), and thickening of the outer nuclear layer. (D and E) The images remain unchanged. Abbreviations: OCT, optical coherence tomography; OPL, outer plexiform layer; INL, inner nuclear layer. |
The patient was subsequently followed-up at 3 weeks (Figure 3B), 4 months (Figure 3C), 1.5 years (Figure 3D) and 2.5 years (Figure 3E) after the onset. Funduscopy showed that the lesion gradually disappeared after 3 weeks. OCT showed that the hyperreflective band was limited to the INL with slight thinning. After 4 months, OCT revealed that the thin and irregular INL and OPL no longer exhibited the hyperreflective change. In addition, OCT demonstrated that there was an excavated change of the inner retinal surface and ONL thickening, which occurred in the same region as the INL and OPL thinning. OCT showed that these retinal changes remained after 1.5 and 2.5 years. At 2.5 years after onset, OCTA images showed there was a normal flow of the macular capillaries in the SCP, and a decreased flow in the lesion, with dilation of the capillaries around the lesion observed in the DCP (Figure 2B). In addition, the patient’s subjective symptom of paracentral scotoma remained after 2.5 years.
Discussion
In this current study, we used OCT and OCTA to examine the longitudinal prognosis of the retinal structure and vasculature in two cases with isolated PAMM over follow-up periods of 2.5–5 years. To the best of our knowledge, this is the longest longitudinal follow-up report of isolated PAMM.
During the acute phase of PAMM, funduscopy generally shows faint white lesions, while OCT shows hyperreflective bands that are mainly present in the INL (but that can sometimes spread to other layers such as the IPL and OPL), and OCTA reveals vascular abnormalities in the SCP and/or DCP.1,2,4 Although the white lesions usually disappear within several weeks, it has been reported that OCT and OCTA images continue to show abnormal findings over a long period of time.3–6 However, it was also reported that the hyperreflective bands seen in OCT images disappeared within several months, and that during this period, there was INL thinning, an excavated change of the inner retinal surface, and ONL thickening.3–6 Dansingani et al also reported on these retinal changes, which they referred to as “focal retinal lamellar ectopia”.4 Based on their findings, they suggested three possible theories for the mechanism of “focal retinal lamellar ectopia”. These hypotheses included, 1) the change is the primary result of focal ONL thickening, 2) the change is the secondary result of the inward micro-forces due to INL thinning, and 3) the artifactual result is caused by a change in the reflectivity of each retinal layer.4 As our present findings demonstrated there was an excavated change of the inner retinal surface in both cases and focal SRD in case 1, both of which were observed in conjunction with INL thinning and ONL thickening, these results support the second theory of inward micro-forces. Therefore, if that SRD occurred by the inward micro-forces, focal vitreomacular traction might be involved.
The mechanism of PAMM has been reported to be primarily due to ischemia of the DCP, and in some cases, is accompanied by ischemia of the SCP. These changes have been well visualized by OCTA.1,2,4 However, while OCTA showed there were no abnormalities in the SPC in both of our cases, our results did show there was decreased flow in conjunction with dilation of the capillaries around the lesion in DCP even at 2.5 and 5 years after the onset (Figure 2). Previous studies using OCTA to examine PAMM have reported finding retinal vascular changes in the DCP, which include flow abnormalities and dilation of the capillaries during the acute phase of PAMM.3,4,7,8 Follow-up OCTA images have shown that these vascular changes remain for about 1 month.4,8 Although mild phenotypes of PAMM exhibit complete recovery of the retinal vasculature in only a few months,7 our data demonstrated that the abnormalities of the retinal vasculature and structure were present for years.
To date, most studies that have examined cases with isolated PAMM lesions have followed the clinical course for a half to a full year, and reported that the retinal changes appear to become stable within several months.1,2 Furthermore, ophthalmic follow-ups are usually completed within 1 year, as the retinal changes associated with PAMM are limited to an extremely narrow area and have only a few risk factors of severe ischemic complications such as neovascular glaucoma. However, our case 1 showed SRD, even though no complications were reported during the examination at 4 years after the onset. Thus, this finding suggests that other unreported events in the outer retina may occur during the chronic phase. Therefore, further cases will need to be examined in order to clarify whether or not severe retinal events occur during the chronic phase of PAMM.
Conclusion
In this study, we reported on the longitudinal retinal changes of two cases with isolated PAMM who were followed-up for 2.5 and 5 years. Our results indicated that long-term retinal changes in PAMM resulted in the excavation of the inner retinal surface, INL thinning, ONL thickening and the presence of abnormal vasculature, especially in the DCP. In addition, one case exhibited a rare complication of focal SRD at 4 years after the onset.
Ethics statement
Written informed consent has been provided by the patients for publication of these case details and any accompanying images. Institutional approval was not required for this case report.
Acknowledgments
This study was supported in part by JSPS KAKENHI Grant Number 17K11434.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sarraf D, Rahimy E, Fawzi AA, et al. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary ischemia. JAMA Ophthalmol. 2013;131(10):1275–1287. doi:10.1001/jamaophthalmol.2013.4056
2. Rahimy E, Kuehlewein L, Sadda SR, Sarraf D. Paracentral acute middle maculopathy: what we knew then and what we know now. Retina (Philadelphia, Pa). 2015;35(10):1921–1930. doi:10.1097/IAE.0000000000000785
3. Trese MG, Thanos A, Yonekawa Y, Randhawa S. Optical coherence tomography angiography of paracentral acute middle maculopathy associated with primary antiphospholipid syndrome. Ophthalmic Surg Lasers Imaging Retina. 2017;48(2):175–178. doi:10.3928/23258160-20170130-13
4. Dansingani KK, Inoue M, Engelbert M, Freund KB. Optical coherence tomographic angiography shows reduced deep capillary flow in paracentral acute middle maculopathy. Eye (London, England). 2015;29(12):1620–1624. doi:10.1038/eye.2015.28
5. Carey A, Cohen S. Paracentral acute middle maculopathy in birdshot chorioretinopathy: a novel association. Retin Cases Brief Rep. 2016;10(2):151–153. doi:10.1097/ICB.0000000000000212
6. Nemiroff J, Phasukkijwatana N, Sarraf D. Optical coherence tomography angiography of deep capillary ischemia. Dev Ophthalmol. 2016;56:139–145.
7. Khan MA, Rahimy E, Shahlaee A, Hsu J, Ho AC. En face optical coherence tomography imaging of deep capillary plexus abnormalities in paracentral acute middle maculopathy. Ophthalmic Surg Lasers Imaging Retina. 2015;46(9):972–975. doi:10.3928/23258160-20151008-12
8. Zhao Z, Faith P, Pakzad-Vaezi K, et al. Paracentral acute middle maculopathy associated with bilateral optic disk swelling and meningitis. Retin Cases Brief Rep. 2017. doi:10.1097/ICB.0000000000000671
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.