")
Back to Journals » Nature and Science of Sleep » Volume 12
Longitudinal Association Between Sleep Duration and Depressive Symptoms in Chinese Elderly
Authors Jing R , Xu T, Rong H, Lai X, Fang H
Received 30 June 2020
Accepted for publication 14 September 2020
Published 13 October 2020 Volume 2020:12 Pages 737—747
DOI https://doi.org/10.2147/NSS.S269992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Steven A Shea
Rize Jing,1,2 Tingting Xu,1,3 Hongguo Rong,2 Xiaozhen Lai,1 Hai Fang2,4,5
1School of Public Health, Peking University, Beijing 100083, People’s Republic of China; 2China Center for Health Development Studies, Peking University, Beijing 100083, People’s Republic of China; 3Department of Social and Behavioral Science, Harvard TH Chan School of Public Health, Harvard University, Boston, Massachusetts 02115, USA; 4Peking University Health Science Center- Chinese Center for Disease Control and Prevention Joint Center for Vaccine Economics, Peking University, Beijing 100083, People’s Republic of China; 5Key Laboratory of Reproductive Health, National Health Commission of the People’s Republic of China, Peking University, Beijing 10083, People’s Republic of China
Correspondence: Hai Fang
China Center for Health Development Studies, Peking University, Xueyuan Road 38, Mailbox 505, Haidian District, Beijing 100083, People’s Republic of China
Tel +86-108-280-5702
Fax +86-108-280-5695
Email [email protected]
Aim: This study aimed to evaluate the longitudinal association between sleep duration and depressive symptoms among the elderly in China.
Methods: A data set from China Health and Retirement Longitudinal Study (CHARLS) in 2011, 2013 and 2015 was adopted with a total of 22,847 respondents aged ≥ 60-years-old. A linear regression analysis with generalized estimating equations was employed to examine the longitudinal associations between duration of total sleep, nighttime sleep and daytime nap, and depressive symptoms.
Results: An extra hour of total sleep including nighttime sleep and daytime nap was associated with lower incidence of depressive symptoms among the elderly after adjusting all confounders (OR=0.83, 95% CI: 0.82– 0.84). In addition, an extra hour of nighttime sleep (OR=0.82, 95% CI: 0.80– 0.83) or daytime nap (OR=0.93, 95% CI: 0.89– 0.97) was also negatively associated with depressive symptoms among the elderly. After controlling the total sleep time, an extra hour of nighttime sleep was negatively associated with depressive symptoms (OR=0.88, 95% CI: 0.84 to 0.92), while an extra hour of daytime nap displayed a positive association with depressive symptoms (OR=0.88, 95% CI: 0.84 to 0.92). Compared with the moderate nappers, only extended nappers had significantly higher incidence of depressive symptoms (OR=1.32, 95% CI: 1.19 to 1.45).
Conclusion: For the elderly in China, increasing their total sleep, nighttime sleep, and/or daytime nap duration would reduce the incidence of depressive symptoms. Moreover, after fixing the total sleep time, increasing nighttime sleep was more beneficial to the decrease of the incidence of depressive symptoms than daytime nap.
Keywords: sleep duration, daytime nap, depressive symptoms, China, the elderly
Introduction
Depression is a common cause of substantial disability and morbidity in the general population. An estimation from the World Health Organization (WHO) showed that more than 300 million people are now suffering from depression, with an increase of over 18% from 2005 to 2015.1 The WHO study on global burden of diseases predicated that depression would be the second largest burden of diseases by 2020, ranking after cardiovascular diseases.2 Depression is also prevalent among older adults all over the world, with an estimated prevalence of 8–16%,3,4 and it can lead to increased risk of functional impairment,5 disability,6 suicide,7 all-cause mortality8 and increased health services utilization.9 Around a third of global DALYs attributable to metal disorders were found in China and India, greater than those found in developed countries, and depressive disorder was the leading cause of mental disorder burden.10 Till the 1990s, studies on depressive symptoms among the elderly reported much lower prevalence of depression in developing countries compared with Western countries.11 In recent years, as developing countries are experiencing rapid health and demographic transitions,12 the protection of traditional lifestyle or family structure against geriatric depression has been weakened in China, giving rise to the development and presence of depression.13 According to baseline survey of 2011 China Health and Retirement Longitudinal Study (CHARLS), about 40% of older adults aged 60 and above (74.0 million) reported depressive symptoms.14 Therefore, the prevention and treatment of depression among older adults has become a serious public health issue in developing countries.
Sleep duration is an important health-related factor which plays a role in the development of many diseases, and thus can serve as a contributor to mortality,15 especially for the elderly. A review indicated that restricted sleep duration was a risk factor for depressive symptoms.16 Besides, there were some studies exploring the association between sleep duration and depression among the elderly in developed countries, but the results were inconsistent. A long-term prospective study in the USA demonstrated that sleep duration of 7 hours or less was associated with clinical depression compared with > 7 hours sleep duration.17 The Wisconsin Sleep Cohort Study found a positive association between short sleep duration (< 5.57 hours) and depression for people aged 33–71 years.18 A Northern Manhattan study found that short sleep (< 6 hours) instead of long sleep (≥ 9 hours) was associated with higher risk of depressive symptoms among older adults.19 The English Longitudinal Study of Ageing also showed that in comparison with optimal sleep duration (7–8 hours), people with shorter sleep (< 5 hours) had higher odds of depressive symptoms.20 However, some other studies did not indicate significant relationship between sleep duration and depression among the elderly.21,22 To our best knowledge, there was very limited evidence on the longitudinal association between sleep duration and depressive symptoms in developing countries, especially in China.
Additionally, a daytime nap (afternoon nap) is a traditional practice commonly seen in the Mediterranean, Latin America, and China,23 while in Western countries, napping is less common and often prompted by unplanned sleepiness due to aging or nighttime complaints.24 A nap after lunch is very common in China,23–25 and more than half of older Chinese adults habitually have a daytime nap.26 Daytime napping among older adults may compensate for insufficient nighttime sleep, so as to reduce fatigue and improve cognitive function.27,28 Although a few studies in China have revealed the relationship between nighttime sleep duration and depression,29 there was currently no longitudinal study evaluating the association between a daytime nap and depressive symptoms among the elderly in China. Therefore, this study used nationally representative longitudinal data in China to examine the association between the duration of total sleep, nighttime sleep and daytime naps, and depressive symptoms, with a special focus on the role of daytime napping.
Methods
Sample and Survey
This study used data from CHARLS, a nationally representative survey of Chinese residents aged 45 and above.30 The baseline survey started in 2011, and two follow-up waves were conducted in 2013 and 2015. The CHARLS questionnaire included information on demographics, family structure/transfer, health status and functioning, biomarkers, health care and insurance, work, retirement and pension, income and consumption, assets (individual and household) and community.30
The present study used all three CHARLS waves from 2011, 2013 and 2015 with 17,596, 18,455 and 20,967 respondents in the raw data respectively. CHARLS longitudinally followed respondents since wave 1 (2011) with some new respondents enrolled in wave 2 (2013) and wave 3 (2015). Most variables in the present study were collected from the harmonized CHARLS data, while the sleep and nap variables were from CHARLS raw data, as they are detailed variables which are unavailable from the harmonized CHARLS data. The present study focused on Chinese older adults, so we dropped 31,111 respondents aged between 45 and 59. A total of 2,310 respondents were excluded for missing CES-D scores, 619 were excluded for missing nighttime sleep or daytime nap measures, and 61 were excluded because their nighttime sleep was less than 1 hour. We further excluded 27 respondents with missing age measures and 43 respondents over 90-years-old. The final study sample included a total of 22,847 respondents: 6,698 respondents in 2011, 7,330 respondents in 2013, and 8819 respondents in 2015 (Figure 1). Among the 6,698 respondents recruited in 2011, 5,108 were successfully re-interviewed in wave 2 (2013), and they were included in later sensitive analysis.
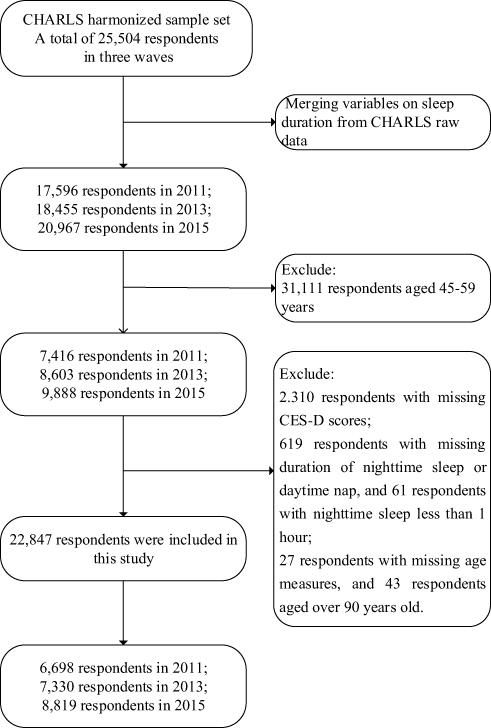 |
Figure 1 Flow chart of sample selection. |
Outcome Variables
Depressive symptoms were identified using the 10-item Chinese version of the Center for Epidemiological Studies Depression scale (CES-D-10) provided at the CES website. The CES-D-10 contains 10 items with 4 response options, including rarely, some days (1–2 days), occasionally (3–4 days) and most of the time (5–7 days).12 The scales for each of the 10 items were adjusted to 0, 1, 2 and 3, so the CES-D-10 score ranged from 0 to 30, with higher scores indicating more negative feelings during the past week. The cut-off CES-D score of depressive symptoms was 10, so a respondent with total score ≥ 10 was defined as having clinically significant depressive symptoms.31,32
Main Predictor Variable
The present study employed three measures of sleep duration. The first measure is total sleep duration at night obtained from the question
During the past month, how many hours of actual sleep did you get at night (average hours for one night)? This may be shorter than the number of hours you spend on bed.
Respondents were further asked “During the past month, how long did you take a nap after lunch?” to measure the daytime nap duration as the second variable. These two questions had high validity and reliability for measuring the length of night-time sleep and afternoon naps in Chinese studies.29,33 Consistent with existing literature,26,33,34 respondents were categorized into four daytime nap groups: non-nappers, short nappers (< 0.5 hour), moderate nappers (0.5–1.5 hours), and extended nappers (> 1.5 hours). The third measure added both nighttime sleep and daytime nap together as the total sleep time per day.35 According to other studies in developed countries,21,22,35 respondents’ total sleep duration was classified into five categories in the present study: < 6 hours, 6 to < 7 hours, 7 to < 8 hours, 8 to < 9 hours, and ≥ 9 hours.
Covariates
In previous studies, depressive symptoms were found to be strongly correlated with health status,36 smoking status,31 and drinking status,31 which might also affect sleep habits. Demographic characteristics, health habits and self-reported comorbidities were controlled as covariates in this study. Demographic characteristics included age, gender (male as the reference group), marital status (unmarried or single as the reference group), residency (urban as the reference group), and education (illiterate as the reference group).37,38 Health habits included body mass index (BMI; kg/m2), smoking (non-smoking as the reference group) and drinking (non-drinking as the reference group). Health comorbidities included self-reported health status (fair or poor as the reference group) and self-reported chronic diseases (no chronic diseases as the reference group). Due to the fact that BMI and smoking status were missing for a large number of respondents, we constructed dummy variables of BMI missing and smoking missing to avoid sample bias by keeping those respondents in the study sample.
Statistical Analysis
Analyses were conducted using the Stata 13 software (Stata Corporation LLC, College Station, Texas). Descriptive statistics covered all respondents without missing variables surveyed in 2011, 2013 and 2015. Continuous variables were described in mean and standard deviation, and categorical variables were described in percentage. Univariate analysis of T test and Chi-squared test were used to explore the association between sleep duration (total sleep, nighttime sleep, and daytime nap) and depressive symptoms.
Linear regression analyses with generalized estimating equations were adopted to estimate the longitudinal association between total sleep duration (as a continuous variable and category variable, respectively) and depressive symptoms among Chinese elderly. Factors known to be associated with depressive symptoms were adjusted for in the regression including age, gender, marital status, education, residency, BMI, drinking, smoking, self-reported health status, and self-reported chronic diseases. The longitudinal association between nighttime sleep or daytime nap (as a continuous variable and category variable, respectively) and depressive symptoms were further analyzed after controlling confounding variables. Moreover, to estimate the association between sleep duration of wave 2 and the incidence or persistence of depressive symptoms, the binary logistic regression model was adopted after adjusting for the same confounding variables.
Results
Descriptive Statistics
The descriptive statistics of the overall population (three waves) and study population in each wave are shown in Table 1. Among the overall population, the mean (SD) CES-D score was 8.46 (6.28), and the incidence of depressive symptoms was 36%. Overall speaking, 49% of the respondents were female, 80% were married, and 60% lived in rural areas. As for education, 34%, 21%, 25%, and 20% of the overall population were categorized as illiterate, primary school (unfinished), primary school (finished) and junior high and above, respectively. In 2011, the study population had a mean (SD) age of 68.00 (6.58) years, with only 19% reporting good health status and 78% having at least one chronic diseases. From 2011 to 2015, no significant change was observed in demographic characteristics except for an increasingly higher likelihood to report overweight, drinking, smoking, and chronic diseases.
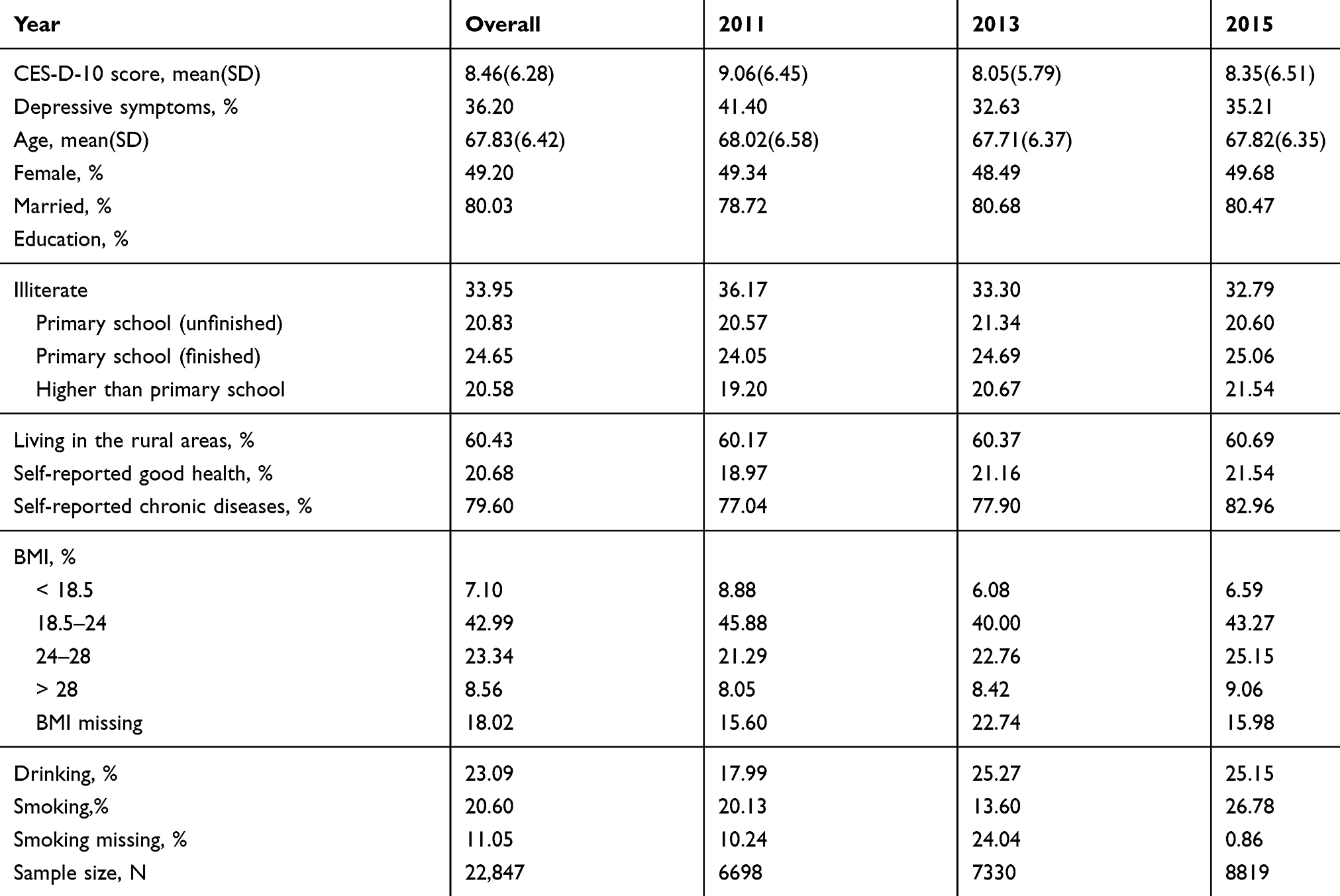 |
Table 1 Descriptive Statistics for Population Characteristics in Three Waves |
Association Between Sleep Duration and Depressive Symptoms in Three Waves
Table 2 compared the sleep duration of by depressive status in three waves. In total, there were 8,270 (36.20%) and 14,577 (63.80%) respondents with and without depressive symptoms, respectively. The mean (SD) total sleep time of those with and without depressive symptoms was 6.16 (2.40) hours and 7.22 (2.07) hours, respectively. The mean (SD) nighttime sleep duration with and without depressive symptoms were 5.59 (2.27) hours and 6.54 (1.85) hours, respectively. The mean (SD) daytime nap duration with and without depressive symptoms were 0.58 (0.74) hours and 0.68 (0.77) hours. Thirty-three percent and 38% of the study population with and without depressive symptoms had a moderate daytime nap. All the above differences are statistically significant at the 1% level by T tests and Chi-Square tests.
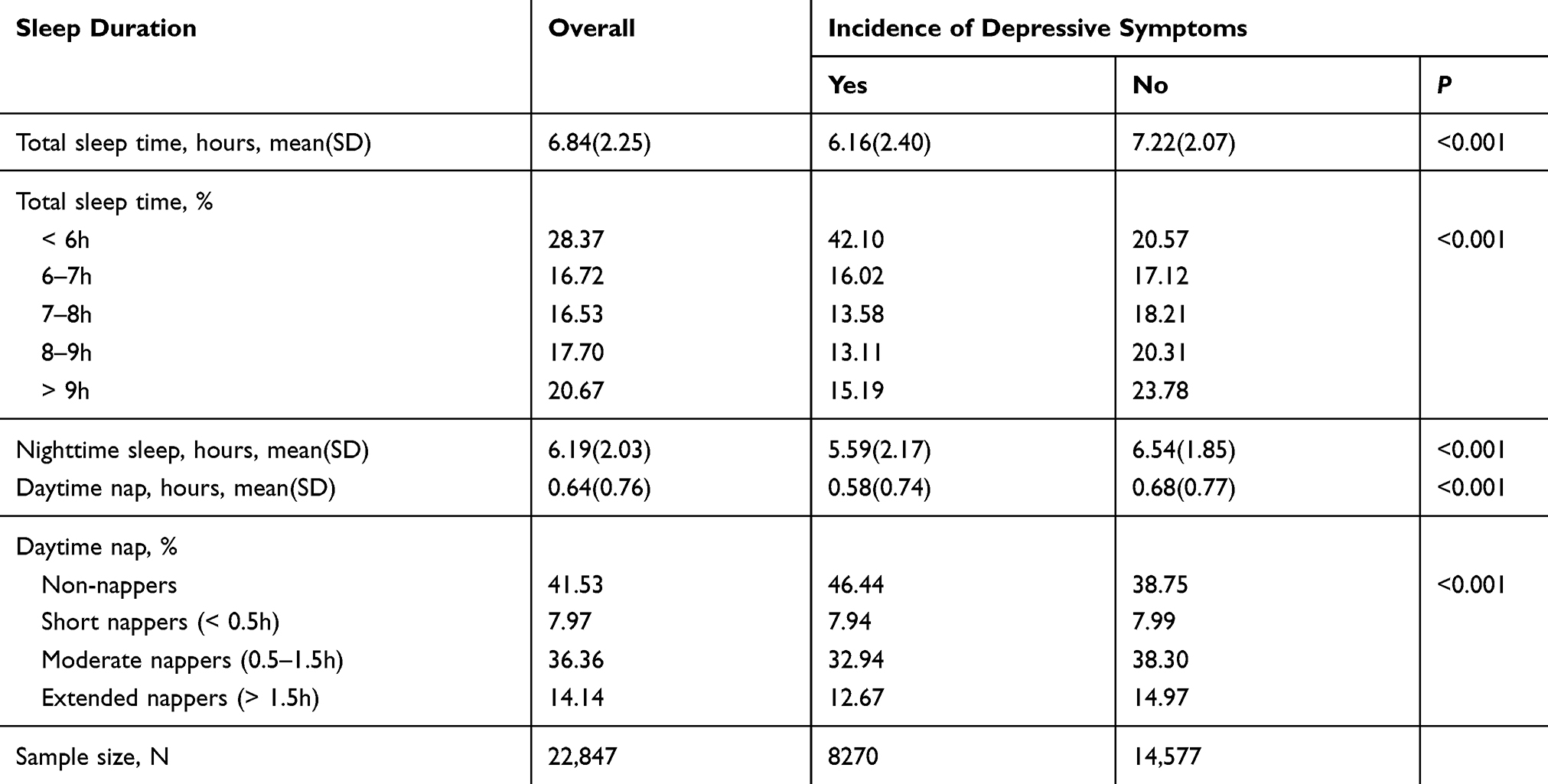 |
Table 2 Association Between Sleep Duration and Depressive Symptoms in Three Waves |
Longitudinal Association Between Total Sleep Time and Depressive Symptoms
Tables 3 and 4 demonstrated the results of linear regression analysis with generalized estimating equations using the longitudinal data in 2011, 2013 and 2015. Table 3 showed that an extra hour of total sleep was associated with lower incidence of depressive symptoms in the elderly after adjusting for all confounders (OR=0.83, 95% confidence interval (CI): 0.82 to 0.84), indicating that the incidence of depressive symptoms would decrease by 17% for every additional one hour of total sleep time for the elderly.
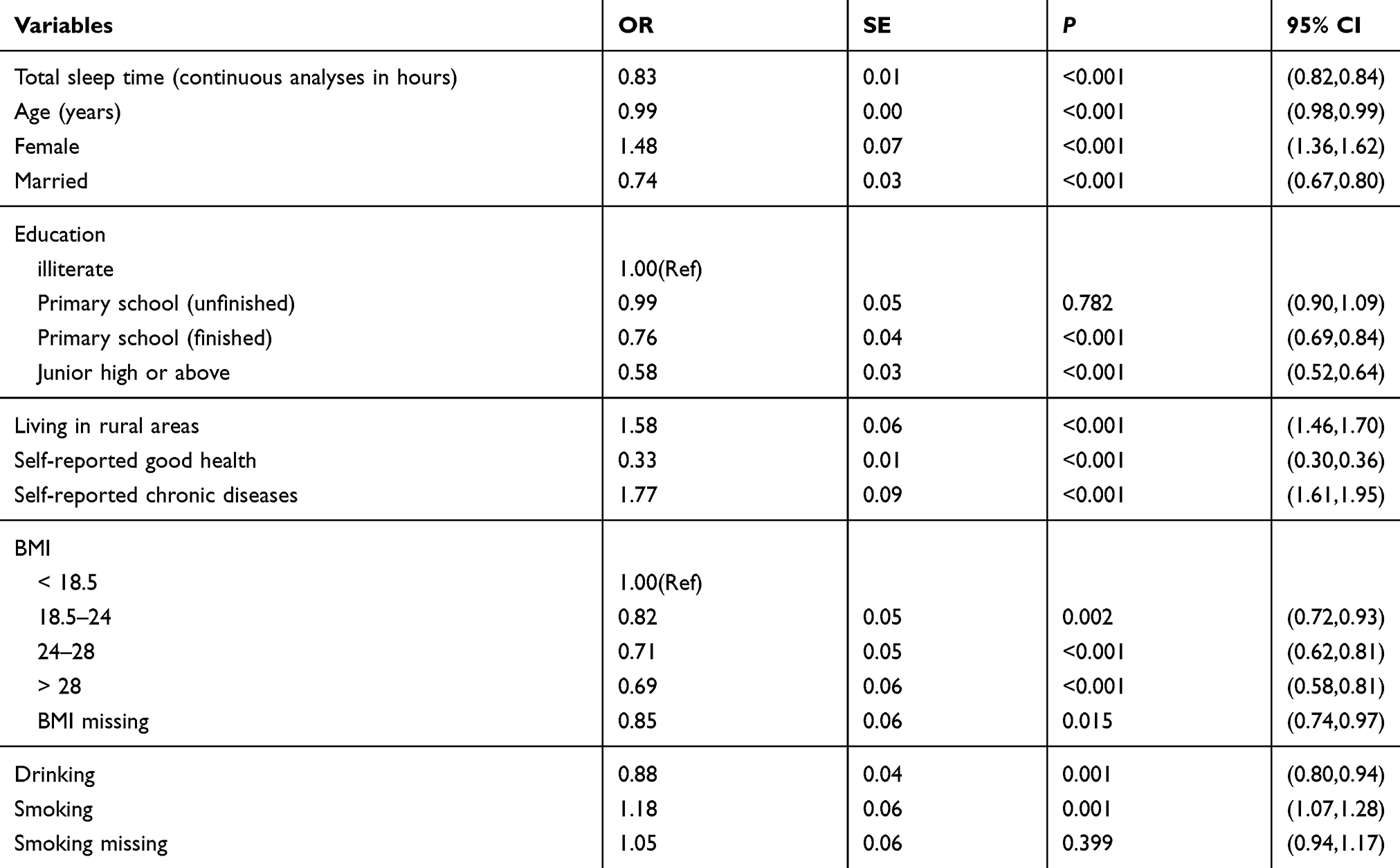 |
Table 3 Longitudinal Association Between Total Sleep Time (Hours) and Depressive Symptoms |
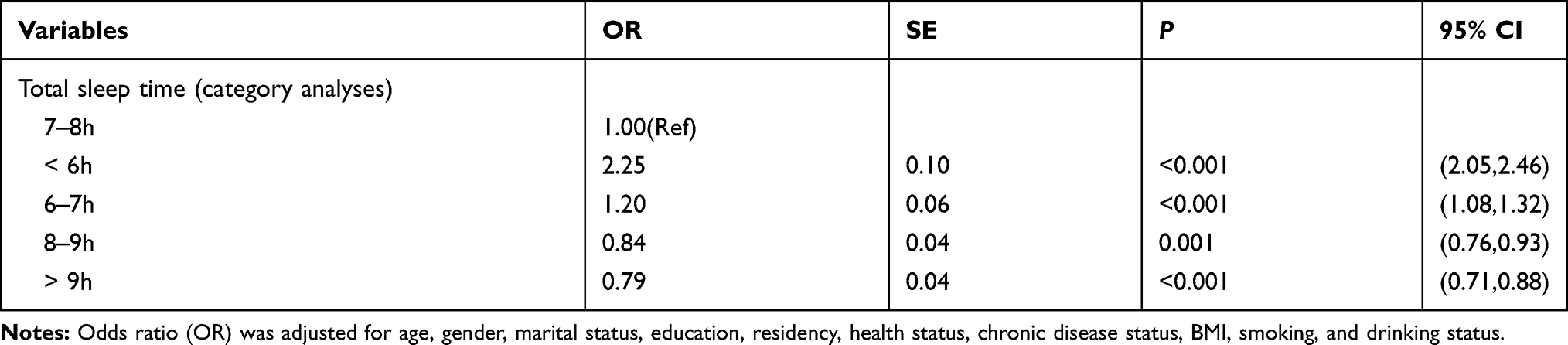 |
Table 4 Longitudinal Association Between Total Sleep Time (Category Variable) and Depressive Symptoms |
Table 4 further presented the association between different total sleep time groups and the incidence of depressive symptoms after adjusting all confounders. Compared with the reference group with 7–8 hours’ total sleep time, the fully adjusted ORs of total sleep time < 6 hours, 6–7 hours, 8–9h and > 9 hours were 2.25 (95% CI: 2.05 to 2.46), 1.20 (95% CI: 1.08 to 1.32), 0.84 (95% CI: 0.76 to 0.93), and 0.79 (95% CI: 0.71 to 0.88), respectively.
Longitudinal Association Between Nighttime Sleep and Daytime Nap and Depressive Symptoms
Tables 5 and 6 reported the associations between nighttime sleep and daytime nap and the depressive symptoms. Longer nighttime sleep and daytime naps would significantly reduce the incidence of depressive symptoms after adjusting for all confounders. According to Table 5, an extra hour of nighttime sleep (OR=0.82, 95% CI: 0.80 to 0.83) or daytime nap (OR=0.93, 95% CI: 0.89 to 0.97) was associated with lower incidence of depressive symptoms in the elderly, indicating that the incidence of depressive symptoms would decline by 18% for one additional hour of nighttime sleep and 7% for one additional hour of daytime nap. We further analyzed the effects of different daytime nap groups on depressive symptoms, and found that moderate nappers had significantly lower incidence of depressive symptoms than non-nappers (OR=1.17, 95% CI: 1.09 to 1.26) and short nappers (OR=1.18, 95% CI: 1.05 to 1.32).
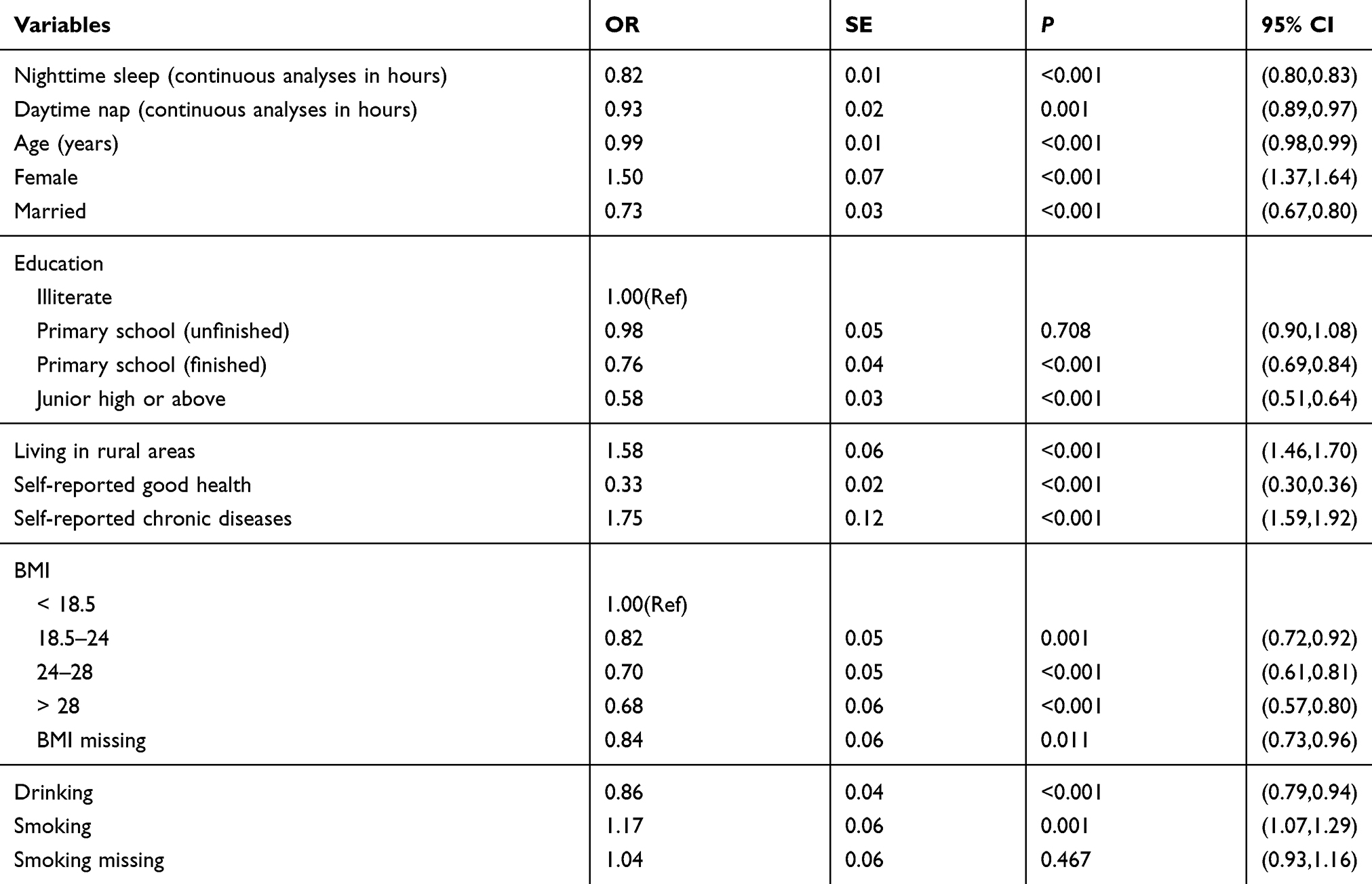 |
Table 5 Longitudinal Association Between Nighttime Sleep and Daytime Nap and Depressive Symptoms |
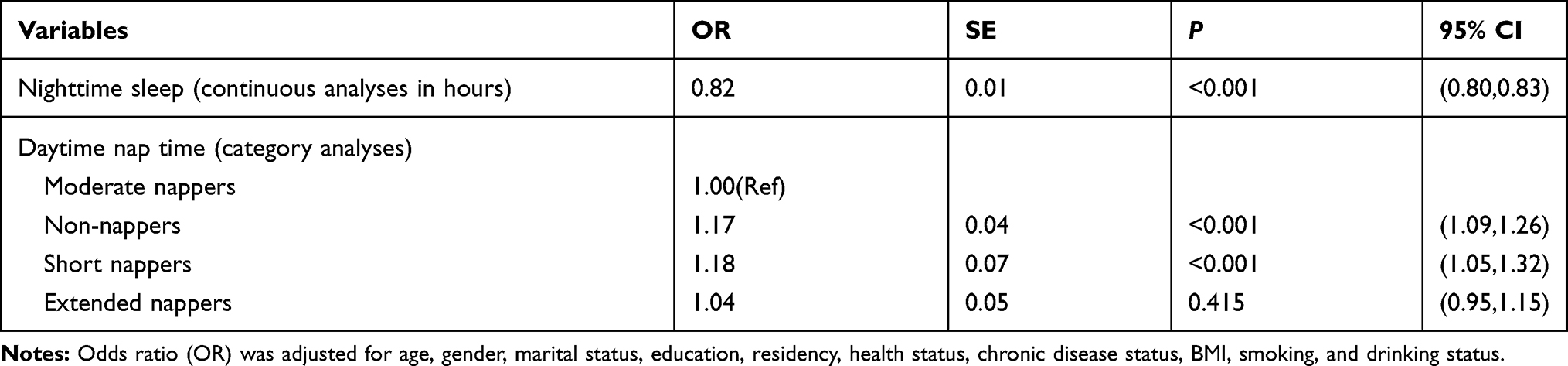 |
Table 6 Longitudinal Association Between Nighttime Sleep and Daytime Nap (Category Variable) and Depressive Symptom |
After controlling the confounders and total sleep time (hours), we found that an extra hour of nighttime sleep was negatively associated with the incidence of depressive symptoms (OR=0.88, 95% CI: 0.84 to 0.92) (See Supplementary Table 1). However, an extra hour of daytime nap displayed a positive association with depressive symptoms (OR=0.88, 95% CI: 0.84 to 0.92), and compared with moderate nappers, only extended nappers had significantly higher incidence of depressive symptoms (OR=1.32, 95% CI: 1.19 to 1.45) (See Supplementary Table 2).
Sensitive Analysis: Association Between Sleep Duration and Persistent Depressive Symptoms
We further analyzed the sleep duration of respondents with or without depressive symptoms at follow-up period (wave 2, 2013). A total of 5,108 respondents aged 60-years-old and over were included in this section who were interviewed at wave 1 and followed up at wave 2. At wave 1, there were 2,072 respondents (40.56%) suffering from depressive symptoms. As shown in Supplementary Table 3-1, 967 respondents (46.67%) reported reversion of depressive symptoms, while the rest showed persistent depression. The mean (SD) total sleep time of those with persistent and reversed depressive symptoms was 5.84 (2.31) and 6.73 (2.29) hours at wave 2, respectively. Compared with the reference group with total sleep time of 7–8 hours, those with total sleep time of < 6 hours had a prospective higher incidence of persistent depressive symptoms (OR=1.77, 95% CI: 1.34 to 2.32) (See Supplementary Table 3-2).
At wave 1, there were 3,036 respondents not suffering from depressive symptoms. During the follow-up period, 547 new cases with depressive symptoms were observed in the 2-year follow-up. Compared with respondents without depressive symptoms at wave 2, respondents with depressive symptoms had shorter total sleep time and nighttime sleep (P<0.001) (See Supplementary Table 4-1). Furthermore, Supplementary Table 4-2 indicated short total sleep time (<6 hours) was prospectively associated with new onsets of depressive symptoms (OR=1.97, 95% CI: 1.47 to 2.65).
Discussion
The duration of total sleep time, nighttime sleep and daytime nap was found to be closely associated with depressive symptoms. Our results indicated a significant association between total sleep time and depressive symptoms, in which shorter total sleep time (less than 7 hours) would increase the incidence of depressive symptoms. In addition, increasing either nighttime sleep or daytime nap was negatively associated with depressive symptoms. After controlling total sleep time, the negative association still persist between nighttime sleep and the incidence of depressive symptoms, while the association turned to be positive between daytime nap and the incidence of depressive symptoms. Sensitive analysis also showed that those with shorter total sleep time still had a prospective higher incidence of persistent or newly-appeared depressive symptoms in 2-year follow-up if older adults with or without depressive symptoms in wave 1 were analyzed separately.
Many previous studies from developed countries have identified short sleep duration as a risk factor for depression among the elderly,18–20,39 and other studies also considered it as a risk factor for depression or depressive symptoms in other age groups.17,40 In contrast to the protective effect of long sleep duration proved in previous studies,40 our study also concluded that short sleep duration was positively associated with depressive symptoms, and was prospectively associated with persistent depressive symptoms across two waves, consistent with the findings of the Northern Manhattan Study18 which indicated that short sleep duration had a prospective association with depressive symptoms in an urban multi-ethnic cohort of older adults. Therefore, the present study prompted that prolonging sleep duration could help avoid persistent depressive symptoms for individuals with depression. As far as we know, most of these studies were conducted in developed countries, despite the fact that the disease burden of depressive symptoms was much higher in developing countries.10 With the industrialization and modernization process of developing countries, they have been experiencing rapid health and demographic transitions,12 resulting in reduced protection of traditional culture against geriatric depression.13 There are few studies on the association between sleep duration and depression in developing countries, and the present study reported interesting results for developing countries: longer total sleep time would reduce the incidence of depressive symptoms among the elderly. Therefore, it is important to take sleep duration into consideration when identifying individuals at higher risk of developing depression in the choice of appropriate interventions and monitor of depression treatments in developing countries.
Few studies have focused on the longitudinal association between daytime nap and depressive symptoms. In Western countries, a daytime nap is less common and often prompted by unplanned sleepiness,24 while a nap after lunch is very common in China. Previous studies have shown that moderate daytime nap (30–90 minutes) was the best for cognition and diabetes mellitus among Chinese elderly.26,33,34 The present study demonstrated that non-nappers, short nappers and extended nappers were more prone to depressive symptoms than those with moderate naps (30–90 minutes) for Chinese elderly. Furthermore, after controlling the total sleep time, increasing the daytime nap turned to be associated with higher incidence of depressive symptoms, which was consistent with a previous study which reported a positive association between daytime nap and depression among people aged 45–65 years.41 By comparison, increasing nighttime sleep was persistently related to lower incidence of depressive symptoms. Therefore, the present study indicated that longer nighttime sleep and daytime nap was helpful in reducing depressive symptoms, but after controlling the total sleep time, increasing nighttime sleep was more beneficial to the control of depressive symptoms. As for the trade-off of nighttime sleep and daytime nap, daytime nap could benefit cognitive functions, but it was linked with a number of subsequent negative outcomes, including higher levels of depressive symptoms, and poorer nocturnal sleep quality (i.e., sleep latency and wake after sleep onset).28,42 This study reported that longer daytime nap could not replace the role of nighttime sleep for reducing the incidence of depressive symptoms.
Depression is often accompanied by comorbid sleep disturbances like insomnia, restless sleep, and restricted sleep duration.43 However, the nature of the association between depression and these sleep disturbances remains unclear,16 and most depressive disorders are characterized by subjective sleep disturbances.44 Several potential mechanisms were discussed to help analyze the observed association between sleep duration and depressive symptoms in this study. Firstly, given that sleep difficulty (either insomnia or hypersomnia) is one of the diagnostic criteria for depressive disorder, it is not surprising that sleep problems are common among up to 90% depressive disorder patients.45 Some researchers also reported that sleep disturbance and short sleep duration could be considered as prodromal depressive symptoms.46 Secondly, depressive disorder has been associated with a particular set of alterations in sleep that are evident in the polysomnogram (PSG), such as alterations in sleep timing, sleep characteristics, and the number of sleep stages.47 Thirdly, systemic inflammation (CRP, TNFa, and IL6) has emerged as a potential pathway linking depressive and anxiety disorders with disease risks. Short and long sleep duration has previously been related to increased inflammation, and is common among psychiatric patients.48,49
This study has several strengths. First, we used sizable longitudinal sample of older participants to examine the association between sleep duration (total sleep time, nighttime sleep and daytime nap) and depressive symptoms for the elderly in a large developing country. Second, the present study revealed the associations between nighttime sleep or daytime nap and the incidence of depressive symptoms, and acknowledged that nighttime sleep played a more important role than daytime nap. There are also some limitations worth consideration. First, we evaluated depressive symptoms using only CES-D score, as its reliability and validity have been established. Nevertheless, the DSM-IV and ICD-10 were also employed in clinically diagnosis.21 Other diagnostic methods should be considered in the future research. Second, there were some studies evaluating the longitudinal association between depressive symptoms and sleep disturbance or insomnia included sleep quality, sleep efficiency, difficulty initiating sleep (DIS), early morning awakening (EMA), and difficulty maintaining sleep (DMS) in developed countries.19,21,22,31,40 CHARLS data used in the present study can only provide information on sleep duration, so currently we are not able to examine the effects of sleep disturbance or insomnia. Third, the sleep duration of both nighttime sleep and daytime nap was self-reported, and some other covariates, for example, chronic diseases, smoking and drinking conditions were also self-reported, resulting in recalling bias. Therefore, more objective sleep test like actigraphy and epidemiological research techniques can be adopted in future studies to obtain precise information.
Conclusion
Sleep duration was associated with depressive symptoms among Chinese elderly. Increasing the total sleep time would decrease the incidence of depressive symptoms, and short total sleep time (less than 6 hours) was positively associated with persistent depressive symptoms. In addition, both nighttime sleep and daytime nap were negatively associated with depressive symptoms, but increasing nighttime sleep played a more important role in reducing the incidence of depressive symptoms than daytime nap after controlling the total sleep time.
Data Sharing Statement
All data in CHARLS are maintained at Peking University and will be accessible publicly. The dataset are available at http://charls.pku.edu.cn/pages/data/111/zh-cn.html. We confirmed that all data accessed of this study complied with relevant data protection and privacy regulations.
Ethics Approval
The data collection in CHARLS was ethically approved by the Biomedical Ethics Review Committee of Peking University (approval number: IRB00001052–11015). Ethics approval for the use of CHARLS data was obtained from the University of Newcastle Human Research Ethics Committee (H-2015-0290).
Acknowledgments
The authors would like to thank the China Center for Economic Research and the National School of Development of Peking University for providing the data of China Health and Retirement Longitudinal Study (CHARLS).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from National Natural Science Foundation of China (71774006) and China Postdoctoral Science Foundation (2019M650392). The funders had no role in the design, analysis, or writing of the manuscript.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. World Health Organization (WHO) 2017: mental health-Depression: let’s talk. Available at: https://www.who.int/mental_health/management/depression/en/. Accessed on 24 July 2019.
2. Murray CJL, Lopez AD, World Health Organization, World Bank & Harvard School of Public Health. (1996). The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary/Edited by Christopher J. L. Murray, Alan D. Lopez. World Health Organization:Available at: https://apps.who.int/iris/handle/10665/41864. Accessed on 24 July 2019.
3. Cole MG, Dendukuri N. Risk factors for depression among elderly community subjects: a systematic review and meta-analysis. Am J Psychiatry. 2003;160(6):1147–1156. doi:10.1176/appi.ajp.160.6.1147
4. Lebowitz BD, Pearson JL, Schneider LS, et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA. 1997;278(14):1186–1190.
5. Lyness JM, Kim J, Tang W, et al. The clinical significance of subsyndromal depression in older primary care patients. Am J Geriatr Psychiatry. 2007;15(3):214–223. doi:10.1097/01.JGP.0000235763.50230.83
6. Cronin-Stubbs D, de Leon CF, Beckett LA, Field TS, Glynn RJ, Evans DA. Six-year effect of depressive symptoms on the course of physical disability in community-living older adults. Arch Intern Med. 2000;160(20):3074–3080. doi:10.1001/archinte.160.20.3074
7. Blazer DG, Bachar JR, Manton KG. Suicide in late life. Review and commentary. J Am Geriatr Soc. 1986;34(7):519–525. doi:10.1111/j.1532-5415.1986.tb04244.x
8. Sun W, Schooling CM, Chan WM, Ho KS, Lam TH. The association between depressive symptoms and mortality among Chinese elderly: a Hong Kong cohort study. J Gerontol a Biol Sci Med Sci. 2011;66(4):459–466. doi:10.1093/gerona/glq206
9. Unützer J, Patrick DL, Simon G, et al. Depressive symptoms and the cost of health services in HMO patients aged 65 years and older. A 4-year prospective study. JAMA. 1997;277(20):1618–1623. doi:10.1001/jama.1997.03540440052032
10. Charlson FJ, Baxter AJ, Cheng HG, et al. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. The Lancet. 2016;388(10042):376–389. doi:10.1016/s0140-6736(16)30590-6
11. Chen R, Copeland JR, Wei L. A meta-analysis of epidemiological studies in depression of older people in the People’s Republic of China. Int J Geriatr Psychiatry. 1999;14(10):821–830. doi:10.1002/(SICI)1099-1166(199910)14:10<821::AID-GPS21>3.0.CO;2-0
12. Lei X, Sun X, Strauss J, et al. Depressive symptoms and SES among the mid-aged and elderly in China: evidence from the China Health and Retirement Longitudinal Study national baseline. Soc Sci Med. 2014;120:224–232. doi:10.1016/j.socscimed.2014.09.028
13. Li D, Zhang DJ, Shao JJ, et al. A meta-analysis of the prevalence of depressive symptoms in Chinese older adults. Arch Gerontol Geriatr. 2014;58(1):1–9. doi:10.1016/j.archger.2013.07.016
14. CHARLS Research Team 2013. Challenges of population aging in China: evidence from the national baseline survey of the China Health and Retirement Longitudinal Study (CHARLS).Available at: http://online.wsj.com/public/resources/documents/charls0530.
15. Gallicchio L, Kalesan B. Sleep duration and mortality: a systematic review and meta-analysis. J Sleep Res. 2009;18(2):148–158. doi:10.1111/j.1365-2869.2008.00732.x
16. Wiebe ST, Cassoff J, Gruber R. Sleep patterns and the risk for unipolar depression: a review. Nat Sci Sleep. 2012;4:63–71. doi:10.2147/NSS.S23490
17. Chang PP, Ford DE, Mead LA, et al. Insomnia in young men and subsequent depression: the johns hopkins precursors study. Am J Epidemiol. 1997;146(2):105–114. doi:10.1093/oxfordjournals.aje.a009241
18. Lippman S, Gardener H, Rundek T, et al. Short sleep is associated with more depressive symptoms in a multi-ethnic cohort of older adults. Sleep Med. 2017;40:58–62. doi:10.1016/j.sleep.2017.09.019
19. Szklo-Coxe M, Young T, Peppard PE, et al. Prospective associations of insomnia markers and symptoms with depression. Am J Epidemiol. 2010;171(6):709–720. doi:10.1093/aje/kwp454
20. Jackowska M, Poole L. Sleep problems, short sleep and a combination of both increase the risk of depressive symptoms in older people: a 6-year follow-up investigation from the English Longitudinal Study of Ageing. Sleep Med. 2017;37:60–65. doi:10.1016/j.sleep.2017.02.004
21. Yokoyama E, Kaneita Y, Saito Y, et al. Association between depression and insomnia subtypes: a longitudinal study on the elderly in Japan. Sleep. 2010;33(12):1693–1702. doi:10.1093/sleep/33.12.1693
22. Paudel M, Taylor BC, Ancoli-Israel S, et al. Sleep disturbances and risk of depression in older men. Sleep. 2013;36(7):1033–1040. doi:10.5665/sleep.2804
23. Lan TY, Lan TH, Wen CP, Lin YH, Chuang YL. Nighttime sleep, Chinese afternoon nap, and mortality in the elderly. Sleep. 2007;30(9):1105–1110. doi:10.1093/sleep/30.9.1105
24. Lam KB, Jiang CQ, Thomas GN, et al. Napping is associated with increased risk of type 2 diabetes: the Guangzhou Biobank Cohort Study. Sleep. 2010;33(3):402–407. doi:10.1093/sleep/33.3.402
25. Yang L, Yang H, He M, et al. Longer sleep duration and midday napping are associated with a higher risk of CHD incidence in middle-aged and older Chinese: the Dongfeng-Tongji cohort study. Sleep. 2016;39(3):645–652. doi:10.5665/sleep.5544
26. Fang W, Li Z, Wu L, et al. Longer habitual afternoon napping is associated with a higher risk for impaired fasting plasma glucose and diabetes mellitus in older adults: results from the Dongfeng-Tongji cohort of retired workers. Sleep Med. 2013;14(10):950–954. doi:10.1016/j.sleep.2013.04.015
27. Garside P, Arizpe J, Lau CI, et al. Cross-hemispheric alternating current Stimulation during a nap disrupts slow wave activity and associated memory consolidation. Brain Stimul. 2015;8(3):520–527. doi:10.1016/j.brs.2014.12.010
28. Mantua J, Spencer RMC. Exploring the nap paradox: are mid-day sleep bouts a friend or foe? Sleep Med. 2017;37:88–97. doi:10.1016/j.sleep.2017.01.019
29. Li Y, Wu Y, Zhai L, et al. Longitudinal association of sleep duration with depressive symptoms among middle-aged and older Chinese. Sci Rep. 2017;7(1):11794. doi:10.1038/s41598-017-12182-0
30. Zhao Y, Hu Y, Smith JP, et al. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
31. Cheng HG, Chen S, McBride O, et al. Prospective relationship of depressive symptoms, drinking, and tobacco smoking among middle-aged and elderly community-dwelling adults: results from the China Health and Retirement Longitudinal Study (CHARLS). J Affect Disord. 2016;195:136–143. doi:10.1016/j.jad.2016.02.023
32. Jin Y, Luo Y, He P. Hypertension, socioeconomic status and depressive symptoms in Chinese middle-aged and older adults: findings from the China health and retirement longitudinal study. J Affect Disord. 2019;252:237–244. doi:10.1016/j.jad.2019.04.002
33. Li J, Cacchione PZ, Hodgson N, et al. Afternoon napping and cognition in Chinese older adults: findings from the China Health and Retirement Longitudinal Study baseline assessment. J Am Geriatr Soc. 2017;65(2):373–380. doi:10.1111/jgs.14368
34. Li J, Chang YP, Riegel B, et al. Intermediate, but not extended, afternoon naps may preserve cognition in Chinese older adults. J Gerontol a Biol Sci Med Sci. 2018;73(3):360–366. doi:10.1093/gerona/glx069
35. Arora T, Jiang CQ, Thomas GN, et al. Self-reported long total sleep duration is associated with metabolic syndrome: the Guangzhou Biobank Cohort Study. Diabetes Care. 2011;34(10):2317–2319. doi:10.2337/dc11-0647
36. Covinsky KE, Fortinsky RH, Palmer RM, Kresevic DM, Landefeld CS. Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons. Ann Intern Med. 1997;126(6):417–425. doi:10.7326/0003-4819-126-6-199703150-00001
37. Huang W, Zhou Y. Effects of education on cognition at older ages: evidence from China’s Great Famine. Soc Sci Med. 2013;98:54–62. doi:10.1016/j.socscimed.2013.08.021
38. Lei X, Sun X, Strauss J, et al. Health outcomes and socio-economic status among the mid-aged and elderly in China: evidence from the CHARLS national baseline data. J Econ Ageing. 2014;4:59–73. doi:10.1016/j.jeoa.2014.10.001
39. Maglione JE, Ancoli-Israel S, Peters K, et al. Subjective and objective sleep disturbance and longitudinal risk of depression in a cohort of older women. Sleep. 2014;37(7):1179–1187. doi:10.5665/sleep.3834
40. Gehrman P, Seelig AD, Jacobson IG, et al. Predeployment sleep duration and insomnia symptoms as risk factors for new-onset mental health disorders following military deployment. Sleep. 2013;36(7):1009–1018. doi:10.5665/sleep.2798
41. Liu Y, Peng T, Zhang S, Tang K. The relationship between depression, daytime napping, daytime dysfunction, and snoring in 0.5 million Chinese populations: exploring the effects of socio-economic status and age. BMC Public Health. 2018;18(1):759. doi:10.1186/s12889-018-5629-9
42. Cross N, Terpening Z, Rogers NL, et al. Napping in older people ‘at risk’ of dementia: relationships with depression, cognition, medical burden and sleep quality. J Sleep Res. 2015;24(5):494–502. doi:10.1111/jsr.12313
43. Krahn LE. Psychiatric disorders associated with disturbed sleep. Semin Neurol. 2005;25(1):90–96. doi:10.1055/s-2005-867077
44. Thase ME. Depression and sleep: pathophysiology and treatment. Dialogues Clin Neurosci. 2006;8(2):217–226.
45. Thase ME. Antidepressant treatment of the depressed patient with insomnia. J Clin Psychiatry. 1999;60(Suppl 17):28–48.
46. Perlman CA, Johnson SL, Mellman TA. The prospective impact of sleep duration on depression and mania. Bipolar Disord. 2006;8(3):271–274. doi:10.1111/j.1399-5618.2006.00330.x
47. Gillin JC, Duncan W, Pettigrew KD, Frankel BL, Snyder F. Successful separation of depressed, normal, and insomniac subjects by EEG sleep data. Arch Gen Psychiatry. 1979;36(1):85–90. doi:10.1001/archpsyc.1979.01780010091010
48. Prather AA, Vogelzangs N, Penninx BW. Sleep duration, insomnia, and markers of systemic inflammation: results from the Netherlands Study of Depression and Anxiety (NESDA). J Psychiatr Res. 2015;60:95–102. doi:10.1016/j.jpsychires.2014.09.018
49. Jeon SW, Kim YK. Neuroinflammation and cytokine abnormality in major depression: cause or consequence in that illness? World J Psychiatry. 2016;6(3):283–293. doi:10.5498/wjp.v6.i3.283
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.