")
Back to Journals » OncoTargets and Therapy » Volume 10
Long-term outcomes of neoadjuvant chemotherapy followed by concurrent chemoradiotherapy (CCRT) vs CCRT alone for nasopharyngeal carcinoma in the era of intensity-modulated radiation therapy using propensity score matching method
Authors Chen X, Zhu X , Liang Z, Li L, Qu S, Chen K, Pan X
Received 25 February 2017
Accepted for publication 27 April 2017
Published 9 June 2017 Volume 2017:10 Pages 2909—2921
DOI https://doi.org/10.2147/OTT.S135590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Carlos E Vigil
Xueling Chen,1 Xiaodong Zhu,1–3 Zhongguo Liang,1 Ling Li,1–3 Song Qu,1–3 Kaihua Chen,1 Xinbin Pan1
1Department of Radiation Oncology, Affiliated Tumor Hospital, Guangxi Medical University, Cancer Institute of Guangxi Zhuang Autonomous Region, 2Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education, 3Guangxi Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Guangxi Medical University, Nanning, Guangxi, People’s Republic of China
Purpose: Whether neoadjuvant chemotherapy (NCT) followed by concurrent chemoradiotherapy (CCRT) could improve survival in nasopharyngeal carcinoma (NPC) remains controversial especially in the era of intensity-modulated radiation therapy (IMRT), and we explored the role of NCT for NPC patients.
Patients and methods: A retrospective review was conducted of 255 NPC patients treated with NCT+CCRT (n=67) or CCRT alone (n=188) based on IMRT between December 2006 and December 2012. To control the imbalance, a 1:2 match was performed using propensity score matching (PSM) method based on patient’s heterogeneity and regimens of concurrent chemotherapy (CCT). The long-term treatment outcomes and toxicity between NCT group (n=67) and concurrent chemoradiotherapy (CRT) group (n=134) after PSM were compared.
Results: The 5-year overall survival (OS), progression-free survival (PFS), recurrence-free survival (RFS), local recurrence-free survival (LRFS), regional recurrence-free survival (RRFS) and distant failure-free survival (DFFS) were 78.8%, 69.1%, 90.0%, 90.0%, 100% and 78.3% for NCT group, while 79.5%, 75.7%, 92.7%, 94.2%, 96.1% and 82.7% for CRT group (P=0.305, 0.448, 0.790, 0.512, 0.104 and 0.671). It indicated that the treatment method (NCT+CCRT vs CCRT) was not the independent prognostic factor for the survival in NPC patients, and only patients who had completed at least two cycles of CCT got better OS, RFS and DFFS (P=0.009, 0.016 and 0.043), whether to receive NCT or not. No difference in the incidences of any acute and most late toxicity between the two groups was shown.
Conclusion: Our study did not show the exact advantage of NCT followed by CCRT compared with CCRT alone or higher incidences of toxicity in NCT group. It suggests that NCT might not be necessary if two or more cycles of CCT are finished well in the era of IMRT, and when NCT is finished well, less than two cycles of CCT with IMRT could be enough. However, in the era of IMRT, the role of NCT still needs to be further explored.
Keywords: propensity score matching, PSM, nasopharyngeal carcinoma, concurrent chemotherapy, IMRT
Introduction
Nasopharyngeal carcinoma (NPC) is common in southern China, and the only curative treatment modality for non-metastatic NPC is radiation therapy. Intensity-modulated radiation therapy (IMRT) gradually becomes the primary treatment of NPC because of its unique advantage and really achieves excellent locoregional control.1–3 It has offered the potential of improved target conformation and sparing of critical structures. Concurrent chemoradiotherapy (CCRT) has been the current standard treatment strategy for locally advanced NPC.4–8 However, in the era of IMRT, a major failure pattern of distant metastasis still occurs.9 Actually, NPC patients have benefited from neoadjuvant chemotherapy (NCT) followed by CCRT that may be associated with the reduced distant failure and significantly improved progression-free survival (PFS) compared with CCRT alone.10,11 Given the lack of studies, the efficacy of NCT followed by CCRT remains unclear in the era of IMRT. Long-term efficacy and toxicities of the NCT followed by CCRT for NPC still need to be further investigated.12 Long-term outcomes of 255 patients receiving NCT followed by CCRT or CCRT alone using IMRT were retrospectively analyzed, and propensity score matching (PSM) method was used to reduce the bias and mimic randomized trials based on patient’s heterogeneity and chemotherapy regimens of CCRT.
Patients and methods
Patient selection using the PSM method
A total of 255 NPC patients primary pathologically confirmed without distant metastases and treated by NCT followed by CCRT (NCT group, n=67) or CCRT alone (concurrent chemoradiotherapy [CRT] group, n=188) at Guangxi Medical University (GXMU) Assistant Tumor Hospital from December 2006 to December 2012 were eligible for our study. Auxiliary examination included hematology and biochemistry profiles, fiberoptic nasopharyngoscopy with biopsy, magnetic resonance imaging (MRI) of nasopharynx and neck, chest radiography or computed tomography (CT), abdominal sonography or CT and technetium-99m-methylene diphosphonate whole-body bone scan. All the cases were staged according to American Joint Cancer Committee (AJCC) 2010 staging classification. In order to control the imbalance, a 1:2 match between the NCT and CRT groups was performed using PSM based on the patients’ heterogeneity and chemotherapy regimens of CCRT. Eight covariates were entered in the propensity model, including age, sex, Karnofsky performance status (KPS), pathology type of World Health Organization (WHO), T, N and clinical classification and chemotherapy regimens of CCRT. After PSM, 201 patients (NCT:CCRT =67:134) were included for analysis successfully. The ethics committee of the Affiliated Tumor Hospital of GXMU approved the study protocol, and all patients provided signed informed consent for the use of their data for future research.
Treatment
IMRT
A description of IMRT was detailed in our study published previously.13 Target volume and organs at risk (OARs) were contoured according to the International Commission on Radiation Units and Measurements Report 50 and 62 (ICRU50 and 62) guidelines. Patient’s head and neck were immobilized using a thermoplastic mask in the supine position. Planning CT simulation-enhanced scanning of the head and neck area at 2.5 or 5 mm thickness was performed. The gross tumor volume (GTV) and cervical lymph node tumor volume (GTVnd) were defined as the gross extent of the tumor shown by CT/MRI and physical examinations. The clinical target volume (CTV) was delineated, which included the GTV with a 0.5–1.0 cm margin. When GTV was adjacent to critical OARs, such as the spinal cord or brainstem, the margin of CTV was adjusted to no >3 mm depending on the proximity of critical structures. Planning target volume (PTV) was defined as CTV plus a margin of 3 mm depending on the proximity of critical structures. The radiotherapy prescription dose is as follows: PGTVnx 68.0–74.0 Gy/30–32f, PGTVnd 60.0–71.0 Gy/30–32f, PCTV1 60.0–70.4 Gy/30–32f and PCTV2 54.0–60.0 Gy/30–32f. Radiation doses were delivered at five frequencies per week.
Chemotherapy
The regimens of NCT include TPF, PF, TP and others. 1) PF: two or three cycles of cisplatin 80 mg/m2 on day 1 and 5-fluorouracil (5-FU) 750 mg/m2/day by continuous intravenous infusion on 96 h every 3 weeks. 2) TP: docetaxel (DOC) at 75 mg/m2 on day 1 and cisplatin at 80 mg/m2 on day 1 every 3 weeks. 3) TPF: two or three cycles of cisplatin 60 mg/m2 on day 1, DOC 60 mg/m2 on day 1 and 5-FU 600 mg/m2/day by continuous intravenous infusion on 120 h every 3 weeks. Other NCT comprised two or three cycles of DOC at 75 mg/m2 on day 1 and nedaplatin (NDP) at 80 mg/m2 on day 1, repeated every 3 weeks.
Concurrent chemotherapy consisted of cisplatin alone (100 mg/m2) every 3 weeks or cisplatin 80 mg/m2 on day 1 and 5-FU 750 mg/m2/day by continuous intravenous infusion on 96 h every 4 weeks.
Study end points
The survival time was calculated from the date of pathologic diagnosis of NPC. Overall survival (OS), PFS, recurrence-free survival (RFS) and distant failure-free survival (DFFS) were treated as the end points that referred to the duration from the date of pathologic diagnosis to the date of any cause of death, any progression including death, nasopharyngeal or regional lymph node relapse and distant metastasis, respectively. Treatment-related toxicities were assessed according to the Common Terminology Criteria for Adverse Events (CTCAE, v4.0).14
Follow-up
The cohort was followed up after the completion of IMRT every 3 months in the first 2 years, every 6 months for 3 additional years and annually thereafter according to our institutional protocol of NPC management. Inspection methods include MRI or CT scanning for nasopharynx and neck, fiber optic endoscopy and biopsy if necessary, bone scan, abdominal ultrasonography and chest X-ray. The follow-up rate was ~93.0% for 201 patients selected from PSM method.
Statistics
Survival analysis was estimated with the Kaplan–Meier method. The log-rank test was applied for univariate analysis. Cox regression was used for multivariate analysis. Statistical analyses were carried out by SPSS 19.0 statistical software. The level of significance was set at a two-tailed P-value of <0.05.
PSM
PSM was completed by Stata 14.0 statistical software. A 1:2 match between the NCT and CRT groups was performed using the nearest available neighbor matching. Eight covariates were entered in the propensity model, including age, sex, KPS, type of WHO, T, N and clinical stage and chemotherapy regimens of CCRT.
Results
Patients, treatment characteristics and compliance
Baseline patient and treatment characteristics in the pre- and post-PSM cohort are shown in Table 1. After PSM, patients were evenly distributed, and there were no statistically significant differences of the age, sex, KPS, type of WHO, T, N and clinical stage and chemotherapy regimens of CCRT after PSM (all P>0.05). Of the 201 patients selected by the PSM method, there were 67 patients in NCT group with a median age of 43 years (24–71 years) and 134 in CRT group with a median age of 44.5 years (18–70 years). WHO type I (keratinizing carcinoma) tumors were not found after PSM. In NCT group, 13 patients (19.4%) were with the AJCC tumor stage II, 26 (38.8%) with stage III, 22 (32.8%) with stage IVa and six (9.0%) with stage IVb, while 30 (22.4%) with stage II, 56 (41.8%) with stage III, 43 (32.1%) with stage IVa and five (3.7%) with stage IVb in CRT group. The most commonly used chemotherapy regimen during the NCT was 5-FU combined with cisplatin for 33 patients (49.3%). During the CCRT, cisplatin alone was most frequently used for 55 patients (82.1%) in NCT group and 113 (84.3%) in CRT group. For NCT group, there were 45 patients (67.2%) who completed only one cycle of NCT perhaps because of physical, economic, individual aspiration or other reasons, seven patients (10.4%) who completed two cycles and 15 patients (22.4%) who completed three cycles. In addition, during CCRT, 41 patients (61.2%) had completed at least two cycles of concurrent chemotherapy in NCT group, while 112 patients (83.6%) in CRT group (P=0.000). The reasons of incomplete concurrent chemotherapy cycles might also include physical, economic, individual aspiration or other reasons. Durations of IMRT were similar between the two groups, with an average of 45.3 days for NCT group and 45.1 days for CRT group for the PSM cohort (P=0.760).
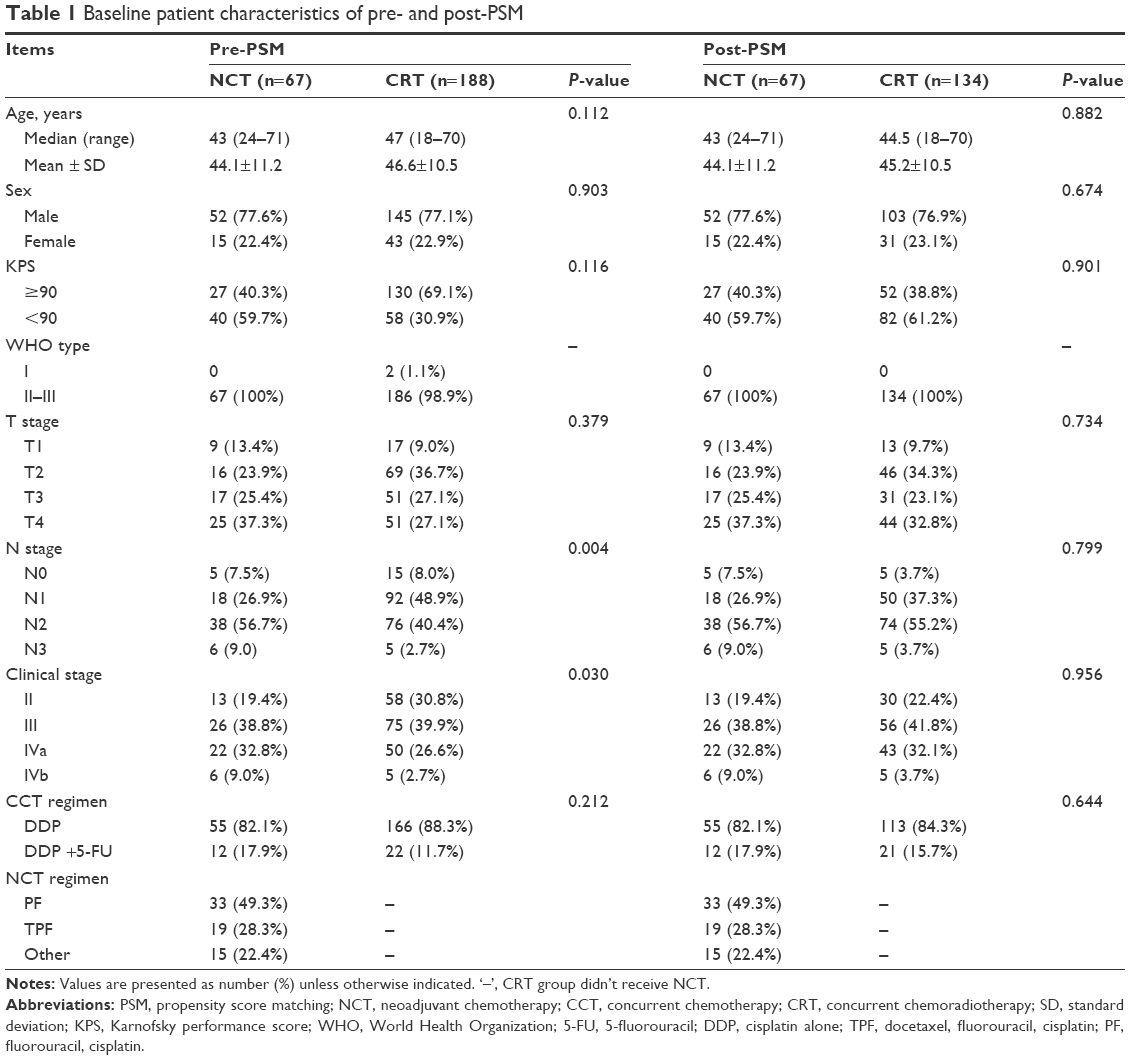 | Table 1 Baseline patient characteristics of pre- and post-PSM |
Long-term survival outcomes
The median follow-up time was 49 months (11–105 months) for NCT group, while 48 months (8–109 months) for CRT group. By the end of follow-up, there were 18 patients with death, 21 with progression, six with local recurrence, none with regional recurrence and 13 with distant metastasis in NCT group, while 24 with death, 33 with progression, eight with local recurrence, five with regional recurrence and 22 with distant metastasis in CRT group. No obvious difference in incidence of the events was found between the two groups (all P>0.05). For NCT group, 1-, 3- and 5-year OS was 98.5%, 86.4% and 78.8%, while 97.7%, 88.6% and 79.5% for CRT group, respectively (P=0.305). For NCT group, 1-, 3- and 5-year PFS was 95.5%, 80.4% and 69.1%, while 92.5%, 80.3% and 75.7% for CRT group, respectively (P=0.448). For NCT group, 1-, 3- and 5-year RFS was 98.5%, 95.2% and 90.0%, while 98.5%, 96.1% and 92.7% for CRT group, respectively (P=0.790). For NCT group, 1-, 3- and 5-year local recurrence-free survival (LRFS) was 98.5%, 95.2% and 90.0%, while 99.2%, 96.9% and 94.2% for CRT group, respectively (P=0.512). For NCT group, 1-, 3- and 5-year regional recurrence-free survival (RRFS) was all 100%, while 99.2%, 98.5% and 96.1% for CRT group, respectively (P=0.104). For NCT group, 1-, 3- and 5-year DFFS was 97.0%, 86.3% and 78.3%, while 94.8%, 84.6% and 82.7% for CRT group, respectively (P=0.671). However, OS, PFS, RFS, LRFS, RRFS and DFFS were with no statistically significant difference in pairwise comparison among NCT and CRT groups (Figure 1).
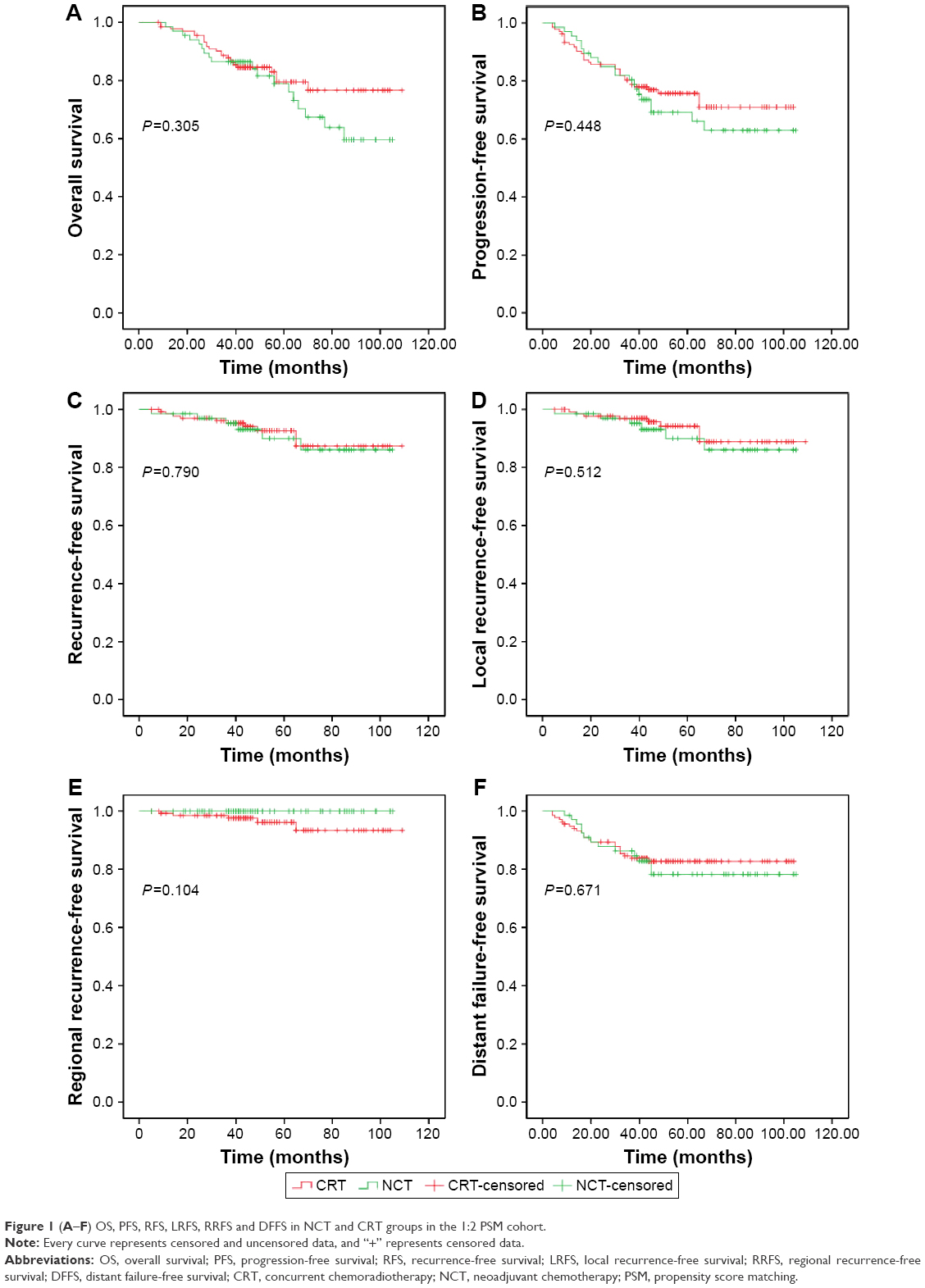 | Figure 1 (A–F) OS, PFS, RFS, LRFS, RRFS and DFFS in NCT and CRT groups in the 1:2 PSM cohort. |
Prognostic factors affecting survival in the whole PSM cohort
The multivariate analysis of the whole propensity-matched cohort by the adjusted Cox proportional hazards model is shown in Table 2, and the hazard radio (HR) was adjusted for all variables in the table including treatment effects, age, sex, KPS, regimens and cycles of concurrent chemotherapy and T, N and clinical stage. It indicated that the effects of treatment (NCT+CCRT vs CCRT) on patients’ OS, PFS, RFS, LRFS, RRFS and DFFS were not statistically significant (P=0.627, 0.879, 0.760, 0.847, 0.969 and 0.774, respectively). It also demonstrated that OS and RFS tended to decrease with the increase in age (P=0.021 and 0.044, respectively), while higher KPS improved DFFS (P=0.039). It showed worse results on OS, PFS, RFS and LRFS in advanced cases of stage IV (P=0.002, 0.022, 0.003 and 0.004, respectively). Results showed that no matter whether NCT was adopted or not, patients who had completed at least two cycles of concurrent chemotherapy got better OS, RFS and DFFS (P=0.009, 0.016 and 0.043, respectively). Other factors including sex, T stage, N stage and regimens of CCRT were not significant factors affecting the survival.
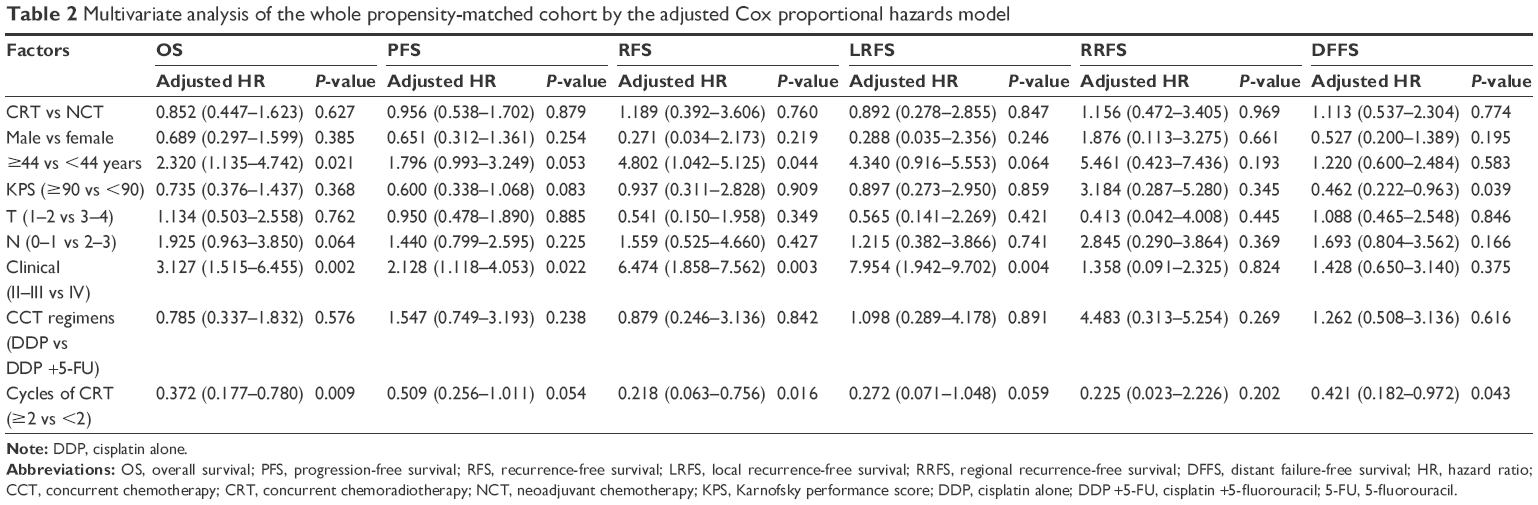 | Table 2 Multivariate analysis of the whole propensity-matched cohort by the adjusted Cox proportional hazards model |
Subset analysis between NCT and CRT groups
In subset analysis by sex, age, KPS, T, N and clinical stage and regimens and cycles of concurrent chemotherapy, the results of most survival outcome between the NCT and CRT groups were similar (Table 3). Therefore, in patients with locally advanced NPC disease (staged T3–4), the DFFS did not favor NCT group with no significance (P=0.764). However, there was no one growing into regional failure in NCT group by the end of follow-up, and only the results for RRFS were different in patients who received less than two cycles of concurrent chemotherapy between the CCRT and NCT groups (P=0.044). The survival outcome of subset between the NCT and CRT groups after PSM was illustrated in Figure 2.
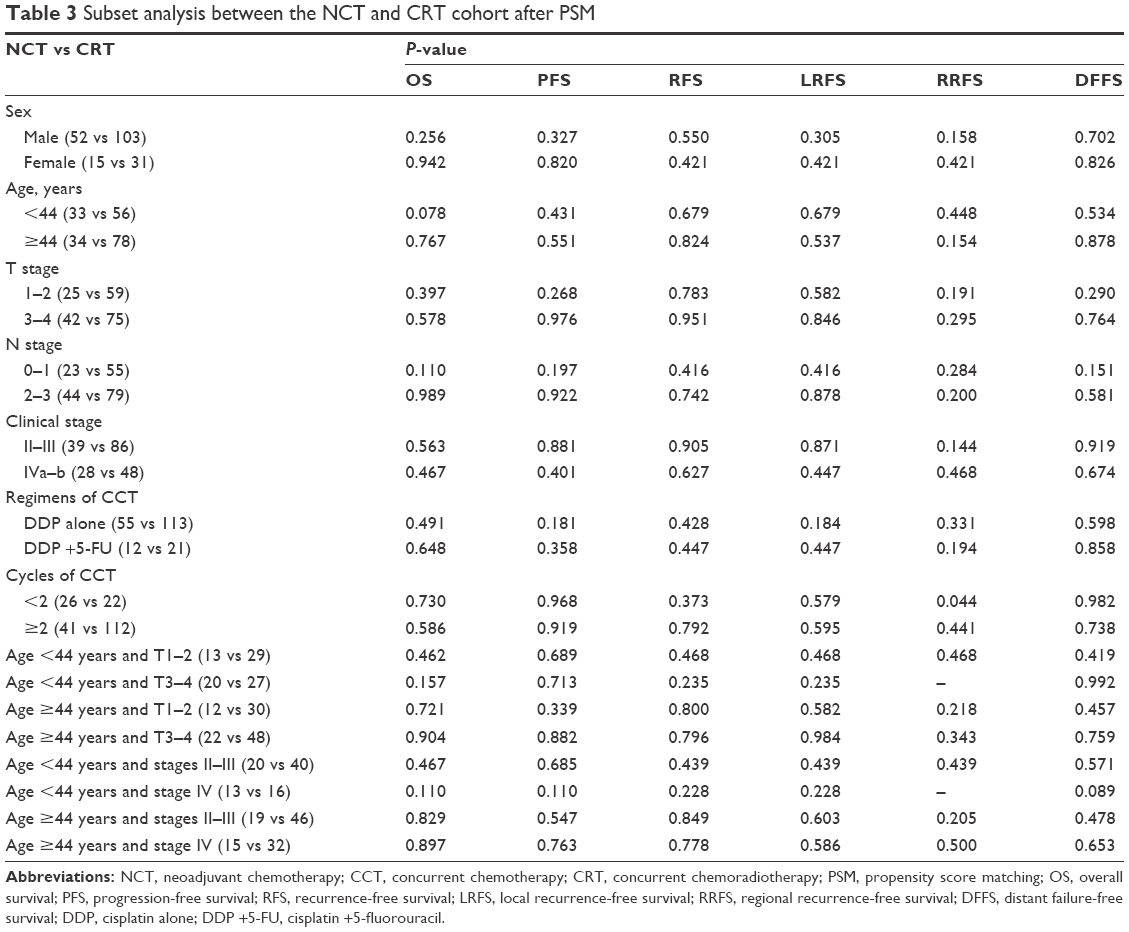 | Table 3 Subset analysis between the NCT and CRT cohort after PSM |
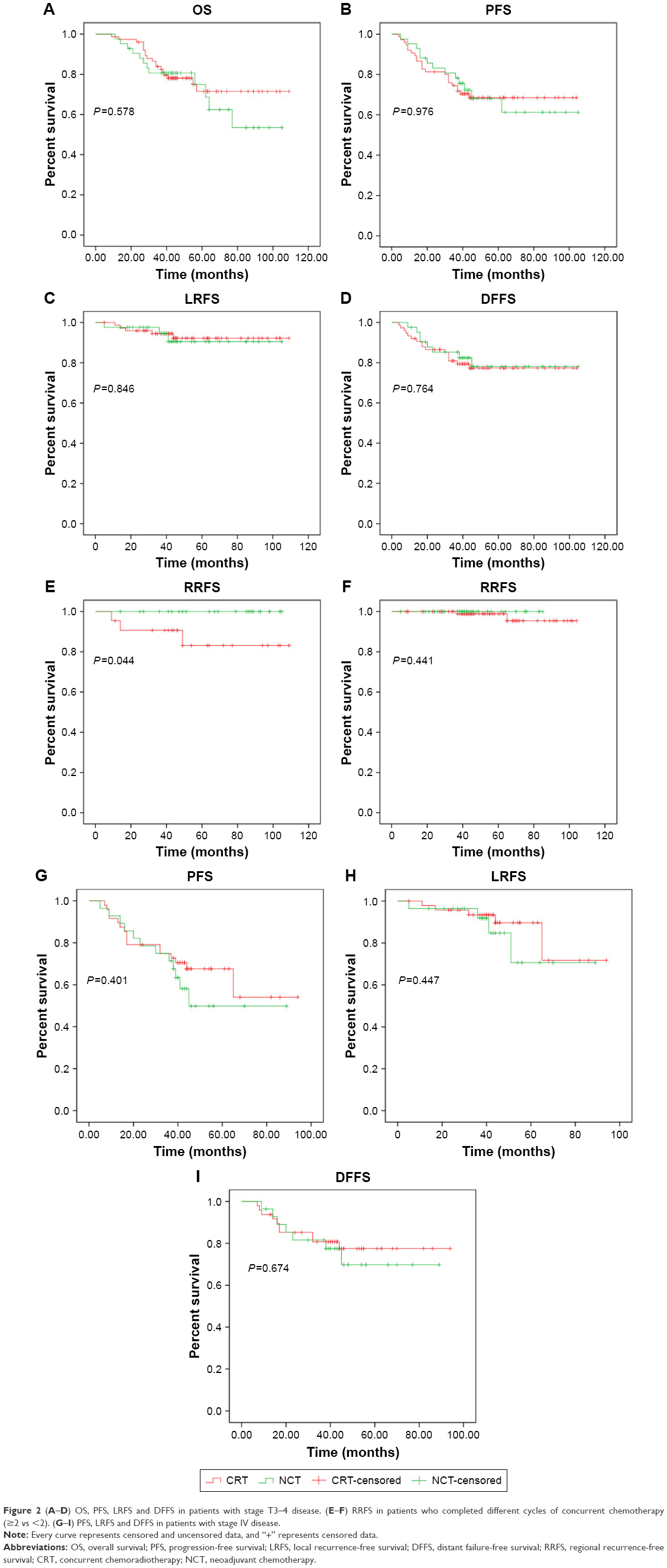 | Figure 2 (A–D) OS, PFS, LRFS and DFFS in patients with stage T3–4 disease. (E–F) RRFS in patients who completed different cycles of concurrent chemotherapy (≥2 vs <2). (G–I) PFS, LRFS and DFFS in patients with stage IV disease. |
Neochemotherapy regimens affecting survival in the NCT cohort
In NCT cohort, the impact of neochemotherapy regimens was also analyzed (PF vs TPF vs other), and the results showed that there was no statistically significant difference (P=0.321, 0.254, 0.380 and 0.304 for OS, PFS, LRFS and DFFS, respectively). There was no advantage of PF or TPF regimens compared to other neochemotherapy regimens such as DOC and NDP (Figure 3).
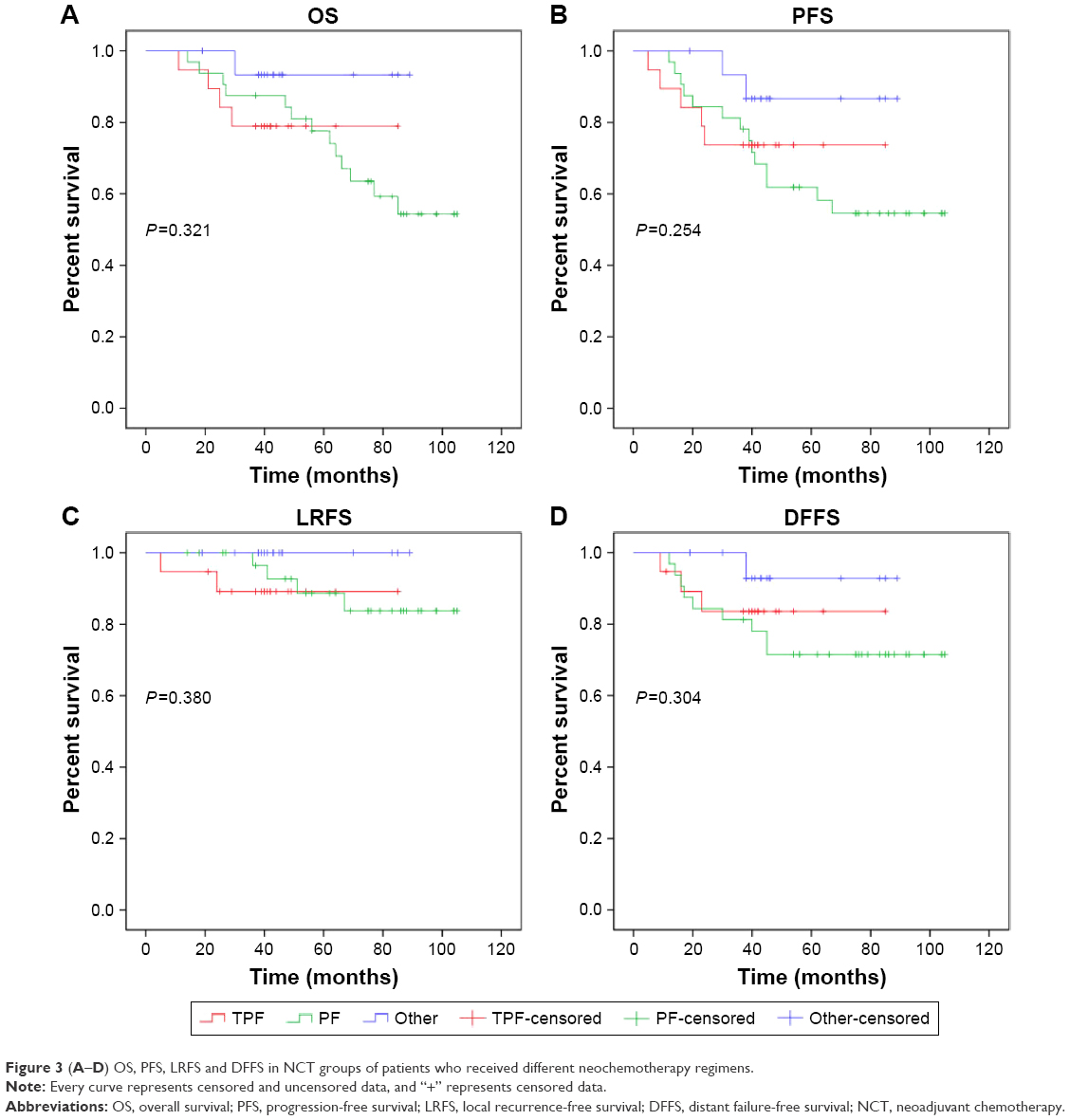 | Figure 3 (A–D) OS, PFS, LRFS and DFFS in NCT groups of patients who received different neochemotherapy regimens. |
Toxicity
Acute and late toxicities are shown in Table 4. It showed no difference of incidences of any acute and most late toxicity between the NCT and CRT groups. Leukopenia, neutropenia and mucositis were the most frequent grade 2 acute toxicities in the two groups. Grade 4 toxicity of anemia and thrombocytopenia were just observed in the NCT group. However, one patient in CRT group achieved percutaneous endoscopic gastrostomy (PEG) due to dysphagia. What is more, grade 3–4 toxicity was not common in our study.
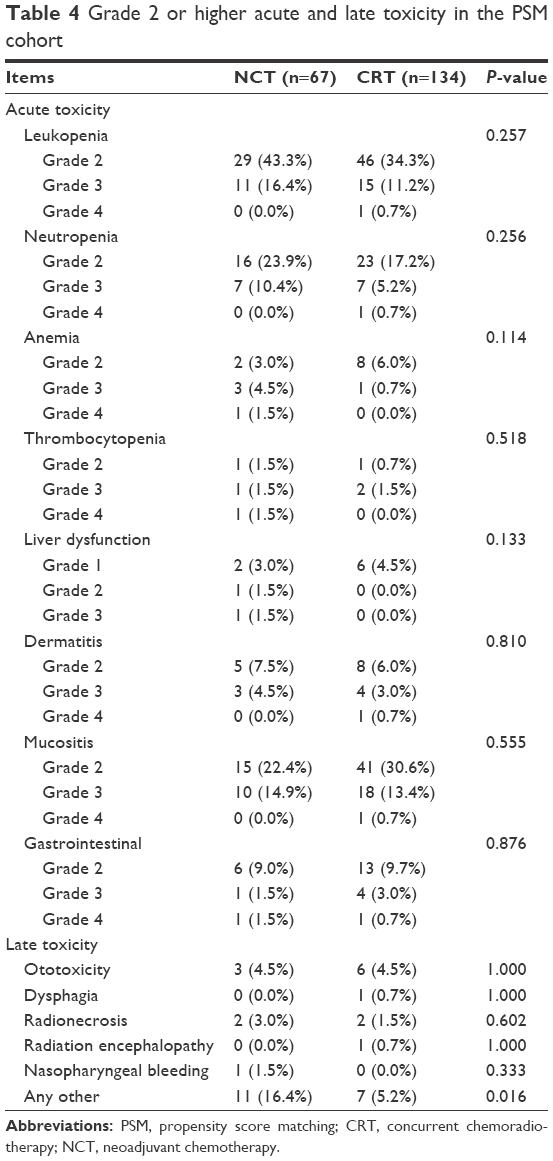 | Table 4 Grade 2 or higher acute and late toxicity in the PSM cohort |
Discussion
IMRT is really an appropriate treatment for NPC because of the irregular target volume and proximity of critical structures, and it really achieves excellent results. However, there still exist failure patterns for NPC including distant metastasis in the era of IMRT. Whether the addition of NCT to CCRT could improve the treatment outcomes of NPC in the era of IMRT needs further research. In our study, the cases of newly diagnosed NPC were all from GXMU Assistant Tumor Hospital from December 2006 to December 2012 and had strong homogeneity. To control the imbalance and bias, we used PSM method. In this series of 201 patients all treated with IMRT after PSM, our results show no difference in long-term survival outcomes between NCT and CRT groups by Kaplan–Meier method including OS, PFS, RFS, LRFS, RRFS and DFFS (P=0.305, 0.448, 0.790, 0.512, 0.104 and 0.671, respectively). The multivariate analysis indicated that the effects of treatment (NCT+CCRT vs CCRT) on patients’ OS, PFS, RFS, LRFS, RRFS and DFFS were not statistically significant in the whole cohort (P=0.627, 0.879, 0.760, 0.847, 0.969 and 0.774, respectively).
In the era of IMRT, the studies about the additional NCT to CCRT is uncommon today, most of which were not entirely based on patients treated with IMRT. Previous data revealed that in 65 eligible patients with stages III–IVB NPC (a part of patients received IMRT), the 3-year PFS and OS for NCT with DOC and cisplatin (TP) followed by CCRT vs CCRT alone were 88.2% and 59.5% (P=0.12) and 94.1% and 67.7% (P=0.012), respectively.12 Induction chemotherapy (IC) with three cycles of CEP (cisplatin, epirubicin and paclitaxel) when followed by CCRT did not significantly improve response rates and/or survival compared with CCRT alone in patients staged IIB–IVB according to the American Joint Committee on Staging of Cancer classification (AJCC 2002), a few of whom were treated with two-dimensional radiotherapy.15 It was also showed that NCT followed by CCRT did not significantly improve OS, LRFS or DFFS by a meta-analysis on 11 studies included 1096 NPC patients, some of whom received IMRT.16 Another meta-analysis in which IMRT and three-dimensional conformal radiotherapy were adopted for partial patients indicated that NCT+CCRT is associated with reduced distant failure compared with CCRT alone, and whether the additional NCT can improve survival for locoregionally advanced NPC should be further explored.11 For 83 locoregionally advanced NPC patients all treated with IMRT who underwent NCT followed by CCRT (49%) or CCRT with/without adjuvant chemotherapy (51%), NCT demonstrated no benefit and an increased risk of severe hematologic toxicity, but potential of improving distant metastasis-free survival in stage IV patients compared to patients treated with CCRT alone.17
However, our study failed to observe a better long-term outcome for the addition of NCT to CCRT in the era of IMRT, which revealed that NCT+CCRT was equivalent to CCRT in patients treated with IMRT. It can be interpreted as that IMRT improves locoregional control and decreases the disparity of survival benefit from the addition of NCT to CCRT. NCT may destroy the sensitive tumor stem cells before IMRT, and the remaining tumor cells may present radiation resistance during IMRT, which may be one of the causes resulting in no advantage for survival in addition of NCT to CCRT compared to CCRT alone. Another reason might be the limit of the relatively small sample and insufficient cycles of NCT in our research. A total of 45 patients (67.2%) completed only one cycle of NCT perhaps because of physical, economic, individual aspiration or other reasons. According to the situation, we advised to optimize the allocation of medical resources and provide psychological support for patients. However, preliminary results indicated that the benefit of changing to an induction-concurrent sequence remains uncertain.18
In our study, during CCRT, 41 patients (61.2%) had completed at least two cycles of concurrent chemotherapy in NCT group, while 112 patients (83.6%) in CRT group. It showed even worse compliance during CCRT in NCT group. Recent study showed that chemotherapy tolerance during CCRT was similar in the NCT and CCRT arms for any chemotherapy regimen.19 We found that there was no one growing into regional failure in NCT group by the end of follow-up, and the results in multivariate analysis indicated that no matter whether NCT was adopted or not, the patients who had completed at least two cycles of concurrent chemotherapy got better OS, RFS and DFFS (P=0.009, 0.016 and 0.043, respectively). This could reveal that NCT will be not necessary if concurrent is finished well (two cycles of concurrent chemotherapy or more). RRFS was different in patients who received less than two cycles of concurrent chemotherapy (P=0.044) between NCT and CRT groups by subset analysis, which also might reveal that when NPC patients accomplished less than two cycles of concurrent chemotherapy, the addition of NCT may account for the better regional control compared to CCRT alone. But there was a limitation of the small sample in NCT group and the insufficient cycles of NCT. This could affect the results. More patients and longer term follow-up were warranted to evaluate late toxicity and treatment outcome.
Our study demonstrated that OS and RFS tended to decrease with the increase in age (P=0.021 and 0.044, respectively) and higher KPS improved DFFS (P=0.039). It was easy to understand why they affected the survival. What is more, OS, PFS, RFS and LRFS were worse in advanced cases of stage IV compared to stages II–III (P=0.002, 0.022, 0.003 and 0.004, respectively). Regarding T stage, N stage and regimens of concurrent chemotherapy, they were not significant factors affecting the survival by multivariate analysis in our research. Therefore, in patients with locally advanced NPC disease (staged T3–4), the DFFS did not favor NCT group with no significance (P=0.764). A study indicated that the NCT arm showed superior DFFS and disease-free survival (DFS) in stage IV patients younger than 60 years.19 A Phase III randomized trials indicated that 3-year failure-free survival was 80% in the NCT+CRT group and 72% in the CCRT alone group (P=0.034) in patients with previously untreated, stages III–IVB (except T3–4N0) NPC.10 It indicated that in the ascending type (T4 and N0–1) of NPC, distant metastasis-free survival rate and PFS rate were improved significantly by NACT+RT compared with CCRT.20 Another research revealed that 5-year DFFS was significantly improved by induction chemotherapy in stage IVa (86.8% vs 77.3%, P=0.008) but not stage IVb.21 With evidence of survival benefit from Phase III randomized trials in the era of IMRT, NCT should be carefully administered in locoregionally advanced NPC patients at high risk of developing distant metastasis and radiotherapy-related mucositis. More results of ongoing trials are awaited in the era of IMRT.
In our NCT cohort, there was no advantage of PF or TPF regimens compared to other neochemotherapy regimens such as DOC and NDP. What is more, it showed no difference of incidences of any acute and most late toxicity between the NCT and CRT groups in our study. The optimal chemotherapeutic regimen of NCT has not been determined completely. The 5-year OS and PFS were not significantly different between NCT with DOC, cisplatin and fluorouracil (TPF) followed by CCRT and CRT groups (OS: 78.3% vs 82.7%, P=0.77; PFS: 72.5% vs 68.2%, P=0.81, respectively) but less grade 3–4 late toxicities were observed.22 In the multicenter prospective study, there was no statistically significant difference for the 3-year OS, LRFS, RRFS, DFFS and PFS in experimental group adopted NCT with DOC plus NDP followed by concomitant NDP and IMRT compared to control group where NDP was replaced by cisplatin, and patients showed good tolerance and compliance with a manageable toxicity profile to the regimen of NCT with DOC plus NDP followed by concomitant NDP and IMRT.23 A PFS benefit for NCT with DOC, cisplatin and fluorouracil (TPF) compared to PF (84.5% vs 77.9%, P=0.380) with a minimum of 2 years follow-up was observed, and the treatment efficacy of PF is not superior to TPF in patients with locoregionally advanced NPC.24 This study showed the similar efficacy for NCT with DOC plus carboplatin (TC) or 5-FU plus carboplatin (FC) in treating locally advanced NPC.25 Recently, a Phase III, multicenter, randomized controlled trial indicated that failure-free survival was improved significantly by the addition of NCT with cisplatin, fluorouracil and DOC (TPF) to CCRT in locoregionally advanced NPC with acceptable toxicity.10
It might be a reasonable approach with the addition of NCT to CCRT, and we need more work to confirm the effects. There were several limitations in our study. Due to the relatively small sample in NCT group and the insufficient cycles of NCT, the current findings could only be taken as preliminary. We will try our best to continue this work in future.
Conclusion
Our study did not show the exact advantage of NCT followed by CCRT compared with CCRT alone or higher incidences of toxicity in NCT group. It suggests that NCT might not be necessary if two or more cycles of concurrent chemotherapy are finished well in the era of IMRT, and when NCT is finished well, less than two cycles of concurrent chemotherapy with IMRT could be enough. However, in the era of IMRT, the role of NCT still needs to be further explored.
Acknowledgments
We highly appreciate Ying Chen from the Department of Administration, Office of Disease Process, for helping us to finish follow-up. We are very grateful to the editor and reviewers. This study was sponsored by Guangxi Planning Project of Scientific Research and Technological Development (No 1598012-22) and the fund of Guangxi Natural Science (No 0575090).
Disclosure
The authors report no conflicts of interest in this work.
References
Co J, Mejia MB, Dizon JM. Evidence on effectiveness of intensity-modulated radiotherapy versus 2-dimensional radiotherapy in the treatment of nasopharyngeal carcinoma: meta-analysis and a systematic review of the literature. Head Neck. 2016;38(suppl 1):E2130–E2142. | ||
Su SF, Han F, Zhao C, et al. Long-term outcomes of early-stage nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy alone. Int J Radiat Oncol Biol Phys. 2012;82(1):327–333. | ||
Takiar V, Ma D, Garden AS, et al. Disease control and toxicity outcomes for T4 carcinoma of the nasopharynx treated with intensity-modulated radiotherapy. Head Neck. 2016;38(suppl 1):E925–E933. | ||
Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J Clin Oncol. 1998;16(4):1310–1317. | ||
Lee AW, Tung SY, Ngan RK, et al. Factors contributing to the efficacy of concurrent-adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: combined analyses of NPC-9901 and NPC-9902 Trials. Eur J Cancer. 2011;47(5):656–666. | ||
Lin JC, Jan JS, Hsu CY, Liang WM, Jiang RS, Wang WY. Phase III study of concurrent chemoradiotherapy versus radiotherapy alone for advanced nasopharyngeal carcinoma: positive effect on overall and progression-free survival. J Clin Oncol. 2003;21(4):631–637. | ||
Chua DT, Sham JS, Au GK, Choy D. Concomitant chemoirradiation for stage III–IV nasopharyngeal carcinoma in Chinese patients: results of a matched cohort analysis. Int J Radiat Oncol Biol Phys. 2002;53(2):334–343. | ||
Chen Y, Liu MZ, Liang SB, et al. Preliminary results of a prospective randomized trial comparing concurrent chemoradiotherapy plus adjuvant chemotherapy with radiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma in endemic regions of china. Int J Radiat Oncol Biol Phys. 2008;71(5):1356–1364. | ||
Chen X, Lei H, Liang Z, Li L, Qu S, Zhu X. Intensity-modulated radiotherapy controls nasopharyngeal carcinoma distant metastasis and improves survival of patients. Springerplus. 2016;5(1):1459. | ||
Sun Y, Li WF, Chen NY, et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016;17(11):1509–1520. | ||
Chen YP, Guo R, Liu N, et al. Efficacy of the additional neoadjuvant chemotherapy to concurrent chemoradiotherapy for patients with locoregionally advanced nasopharyngeal carcinoma: a Bayesian Network Meta-analysis of Randomized Controlled Trials. J Cancer. 2015;6(9):883–892. | ||
Hui EP, Ma BB, Leung SF, et al. Randomized phase II trial of concurrent cisplatin-radiotherapy with or without neoadjuvant docetaxel and cisplatin in advanced nasopharyngeal carcinoma. J Clin Oncol. 2009;27(2):242–249. | ||
Liang Z, Zhu X, Li L, et al. Concurrent chemoradiotherapy followed by adjuvant chemotherapy compared with concurrent chemoradiotherapy alone for the treatment of locally advanced nasopharyngeal carcinoma: a retrospective controlled study. Curr Oncol. 2014;21(3):e408–e417. | ||
National Library of Medicine, National Institutes of Health. Common terminology criteria for adverse events v4.0. [webpage on the Internet] Available from: http://evs.nci.nih.gov/ftp1/CTCAE/About.html. Accessed May 22, 2017. | ||
Fountzilas G, Ciuleanu E, Bobos M, et al. Induction chemotherapy followed by concomitant radiotherapy and weekly cisplatin versus the same concomitant chemoradiotherapy in patients with nasopharyngeal carcinoma: a randomized phase II study conducted by the Hellenic Cooperative Oncology Group (HeCOG) with biomarker evaluation. Ann Oncol. 2012;23(2):427–435. | ||
Liang ZG, Zhu XD, Tan AH, et al. Induction chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy with or without adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: meta-analysis of 1,096 patients from 11 randomized controlled trials. Asian Pac J Cancer Prev. 2013;14(1):515–521. | ||
Wee CW, Keam B, Heo DS, Sung MW, Won TB, Wu HG. Locoregionally advanced nasopharyngeal carcinoma treated with intensity-modulated radiotherapy plus concurrent weekly cisplatin with or without neoadjuvant chemotherapy. Radiat Oncol J. 2015;33(2):98–108. | ||
Lee AW, Ngan RK, Tung SY, et al. Preliminary results of trial NPC-0501 evaluating the therapeutic gain by changing from concurrent-adjuvant to induction-concurrent chemoradiotherapy, changing from fluorouracil to capecitabine, and changing from conventional to accelerated radiotherapy fractionation in patients with locoregionally advanced nasopharyngeal carcinoma. Cancer. 2015;121(8):1328–1338. | ||
Song JH, Wu HG, Keam BS, et al. The role of neoadjuvant chemotherapy in the treatment of nasopharyngeal carcinoma: a multi-institutional retrospective study (KROG 11-06) using propensity score matching analysis. Cancer Res Treat. 2016;48(3):917–927. | ||
Yao JJ, Zhou GQ, Zhang F, et al. Neoadjuvant and concurrent chemotherapy have varied impacts on the prognosis of patients with the ascending and descending types of nasopharyngeal carcinoma treated with intensity-modulated radiotherapy. PLoS One. 2016;11(10):e0161878. | ||
Lan XW, Zou XB, Xiao Y, et al. Retrospective analysis of the survival benefit of induction chemotherapy in stage IVa-b nasopharyngeal carcinoma. PLoS One. 2016;11(8):e0160758. | ||
Ou D, Blanchard P, El Khoury C, et al. Induction chemotherapy with docetaxel, cisplatin and fluorouracil followed by concurrent chemoradiotherapy or chemoradiotherapy alone in locally advanced non-endemic nasopharyngeal carcinoma. Oral Oncol. 2016;62:114–121. | ||
Tang C, Wu F, Wang R, et al. Comparison between nedaplatin and cisplatin plus docetaxel combined with intensity-modulated radiotherapy for locoregionally advanced nasopharyngeal carcinoma: a multicenter randomized phase II clinical trial. Am J Cancer Res. 2016;6(9):2064–2075. | ||
Jin T, Qin WF, Jiang F, et al. Interim analysis of a prospective randomized non-inferiority trial of cisplatin and fluorouracil induction chemotherapy with or without docetaxel in nasopharyngeal carcinoma. Oncotarget. Epub 2016 Jul 28. | ||
Lv X, Xia WX, Ke LR, et al. Comparison of the short-term efficacy between docetaxel plus carboplatin and 5-fluorouracil plus carboplatin in locoregionally advanced nasopharyngeal carcinoma. Onco Targets Ther. 2016;9:5123–5131. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.