")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Long-term follow-up on health-related quality of life in major depressive disorder: a 2-year European cohort study
Authors Saragoussi D, Christensen MC, Hammer-Helmich L , Rive B, Touya M, Haro JM
Received 8 December 2017
Accepted for publication 9 April 2018
Published 22 May 2018 Volume 2018:14 Pages 1339—1350
DOI https://doi.org/10.2147/NDT.S159276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Delphine Saragoussi,1 Michael Cronquist Christensen,2 Lene Hammer-Helmich,3 Benoît Rive,4 Maëlys Touya,5 Josep Maria Haro6
1Real-World Evidence and Epidemiology, Lundbeck SAS, Issy-les-Moulineaux, France; 2Medical Affairs Vortioxetine, H. Lundbeck A/S, Valby, Denmark; 3Real-World Evidence and Epidemiology, H. Lundbeck A/S, Valby, Denmark; 4Global Analytics, Lundbeck SAS, Issy-les-Moulineaux, France; 5Health Economics and Outcomes Research, Lundbeck, Deerfield, IL, USA; 6Research and Teaching Unit, Parc Sanitari Sant Joan de Deu, CIBERSAM, University of Barcelona, Sant Boi de Llobregat, Barcelona, Spain
Background: Major depressive disorder (MDD) is associated with significant impairments in health-related quality of life (HRQoL) and everyday functioning. This cohort study investigated the long-term development of HRQoL in patients with MDD and its association with patient characteristics, including depressive symptom severity and cognitive symptoms.
Methods: The Prospective Epidemiological Research on Functioning Outcomes Related to Major depressive disorder (PERFORM) study was a longitudinal cohort study conducted in 1,159 outpatients aged 18–65 years with MDD in France, Germany, Spain, Sweden, and the UK. The patients were either initiating antidepressant monotherapy or undergoing their first switch of antidepressant. HRQoL was assessed using the Medical Outcomes Study Short-Form 12-item Health Survey (SF-12) up to month 12 and the EuroQol Five Dimensions questionnaire up to month 24 (UK only). Depressive symptom severity was assessed up to month 24 by the patient-reported Patient Health Questionnaire and cognitive symptoms by the Perceived Deficit Questionnaire. Multivariate analyses were performed to identify patient characteristics associated with HRQoL.
Results: Mental HRQoL was severely impaired at baseline versus normative data (mean [SD] SF-12 mental component summary [MCS], 26.5 [9.2]); mean (SD) physical component summary (PCS) total score was 45.2 (12.1). SF-12 MCS improved over 12 months of follow-up (38.7 [11.6] at month 12), while SF-12 PCS remained stable (45.3 [11.1]). At each assessment time point, there was a clear pattern of lower SF-12 MCS and PCS total score in patients experiencing greater cognitive problems. The mean EuroQol Five Dimensions questionnaire utility index score generally decreased (i.e., worsened) with increasing severity of cognitive and depressive symptoms at all time points up to 24 months. Multivariate analyses identified both depression severity and cognitive symptoms as strongly and significantly associated with poor HRQoL.
Conclusion: These findings highlight the importance of recognizing and managing residual symptoms in patients with MDD, including the cognitive symptoms, to restore long-term psychosocial functioning.
Keywords: major depressive disorder, health-related quality of life, depression, cognitive symptoms
Introduction
Major depressive disorder (MDD) affects more than 300 million people worldwide and is the leading cause of disability.1 By 2030, MDD is expected to be the leading cause of disability-adjusted life-years in high-income countries.2 A critical element to the disabling aspect of depression is the adverse impact of the disorder on patients’ health-related quality of life (HRQoL). HRQoL can be defined as “how well a person functions in their life and his or her perceived wellbeing in physical, mental, and social domains of health.”3 In the Sequence Treatment Alternative to Relieve Depression (STAR*D) study – a large US study designed to assess the efficacy of sequential acute treatments for MDD – <3% of patients with MDD reported normal quality of life before initiation of antidepressant therapy.4 Studies on HRQoL in depression document impairments in interpersonal, psychological, and even physical functioning.5–8 Given both the personal and societal consequences of such functional deficits, improving and ultimately restoring HRQoL has been identified as an important treatment target in patients with MDD.9–12
Although numerous studies have shown MDD to have a significant detrimental impact on HRQoL,4,8,13–18 these studies have typically been cross-sectional or with a short-term follow-up. Few studies have considered HRQoL beyond the acute or short-term maintenance phase of treatment. With full functional recovery as the ultimate treatment goal for MDD,19 it is clearly important to also consider HRQoL after acute symptom relief. However, the severity of depressive symptoms only partially accounts for the impairment in HRQoL observed in patients with MDD.4,10,13,20 Indeed, impairment of HRQoL has been shown to persist in patients with MDD after remission of depressive symptoms,4,10,15,20 suggesting that other patient characteristics play an important role in full recovery from the disease. Cognitive symptoms are a core feature of MDD that make a major contribution to disease burden due to their impact on social and professional functioning.11,21–24 While a growing body of literature continues to uncover the clinical importance of cognitive symptoms in MDD in terms of understanding disease severity and progression, and a number of recent updates of treatment guidelines for MDD specifically point to cognitive symptoms as an important therapeutic target,19,22,24–28 little is known about the association between cognitive symptoms and HRQoL during the different stages of MDD progression and treatment.
A strong association between concentration difficulties assessed using the specific item 6 on the Montgomery–Åsberg Depression Rating Scale and HRQoL, independent of the severity of other symptoms, was observed in a recent 6-month study in patients with unipolar depressive disorders.29 However, to our knowledge, no study to date has fully explored the long-term development of both cognitive symptoms and HRQoL in MDD from a patient perspective or the patient demographic and clinical characteristics that may be associated with HRQoL impairment.30,31 As cognitive symptoms have also been shown to persist in patients with MDD after the remission of depressive symptoms,24,28 detailed exploration of the relationship between HRQoL and cognition seems to be warranted.
The Prospective Epidemiological Research on Functioning Outcomes Related to Major depressive disorder (PERFORM) study was a longitudinal observational cohort study undertaken to better understand the course of MDD and its impact on functioning and HRQoL over a 2-year period in outpatients with MDD who were either initiating or undergoing their first switch of antidepressant monotherapy in routine clinical practice in five European countries.24 This manuscript presents the findings on the development of HRQoL over the 2 years of follow-up and investigates its association with other patient characteristics, including depressive symptom severity and cognitive symptoms.
Methods
Study design
PERFORM was a 2-year multicenter, prospective, non-interventional cohort study in outpatients with MDD enrolled by either a general practitioner (GP) or a psychiatrist at 194 sites in France, Germany, Spain, Sweden, and the UK (ClinicalTrials.gov NCT01427439). The study design has been reported in detail previously.24 Briefly, eligible patients were aged 18–65 years, had a current diagnosis of MDD according to the Diagnostic and Statistical Manual of Mental Disorders (4th Edition, Text Revision criteria; confirmed by the Mini International Psychiatric Interview questionnaire [depression module]), and were either initiating antidepressant monotherapy or undergoing their first switch of antidepressant. The choice of antidepressant prescribed was determined by the treating physician and was independent of study participation. Patients receiving antidepressant combination therapy at the time of the initial consultation and patients with schizophrenia or other non-affective psychosis, bipolar disorder, substance dependence, mood disorders due to a general medical condition or substances, or dementia or other neurodegenerative diseases that might significantly impact cognitive functioning were excluded from study entry. Pregnant women and women ≤6 months postpartum were also excluded.
Ethics approval and consent to participate
Ethical approval was obtained for each study site before the initiation of the study following country regulations regarding observational studies. National approvals were obtained as follows: France: French National Agency for Medicines and Health Products Safety (Agence Nationale de Sécurité du Médicament et des Produits de Santé, previously called Agence Française de Sécurité Sanitaire des Produits de Santé), Advisory Committee on Information Processing in Material Research in the Field of Health (Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé), French data protection agency (Commission Nationale de l’Informatique et des Libertés), French National Medical Council (Conseil National de l’Ordre des Médecins), Ethics Committee (CPP Ile de France II); 102 physicians/sites; Germany: Munich Ethics Committee, local Ethics Committees including Hamburg, Rheinland-Pfalz, Sachsen, and Westfalen-Lippe Ethics Committees and others; 47 physicians/sites; Spain: Agencia Española del Medicamento y Productos Sanitarios, Comités Eticos de Investigaciones Clinicas, Comunidades Autónomas of 14 regions; 46 physicians/sites; Sweden: Uméå Ethics Committee; 22 physicians/sites; UK: Medical Research and Ethics Committee, National Institute for Health Research, and local submissions; 65 physicians/sites. All patients provided written informed consent to participate in the study.
Study assessments and data collection
Study assessments and data collection occurred during routine visits within the normal course of care at baseline and 2, 6, 12, 18, and 24 months thereafter. Data collected included sociodemographic data, physical characteristics, history of MDD, characteristics of the current episode of depression, MDD management and resource use, and the presence of any other mental disorder or functional syndrome.
HRQoL was assessed up to month 12 in all patients by the Medical Outcomes Study Short-Form 12-item Health Survey (SF-12).32 The SF-12 assesses both physical and mental health and specifically enquires about physical functioning, emotional functioning (at work and with activities of daily living), energy, and social functioning. It is a widely used patient-reported outcome measure that is validated for use in many diseases and has been identified as one of the most appropriate measures to assess quality of life in clinical trials of MDD.33 It measures the patient’s perception of their own mental and physical health across eight domains: physical functioning, role limitations due to physical health, bodily pain, general health, vitality (energy/fatigue), social functioning, role limitations due to emotional health, and mental health (psychological distress and psychological wellbeing).32 The SF-12 generates two main scores ranging from 1 to 100, the mental component summary (MCS) and the physical component summary (PCS); higher scores indicate better quality of life. Patients reporting MCS and PCS scores <42.0 and <43.85, respectively, are considered significantly impaired.32 In this study, the same calculations for standardization and transformation of SF-12 dimension scores were used for all countries; norms applied were those of the US general population.32
In the UK, HRQoL was also assessed up to month 24 by the EuroQol Five Dimensions questionnaire (EQ-5D).34 The EQ-5D is a widely used self-report instrument covering five health dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, each with three levels (no problem, some problems, or extreme problems). A utility index score can be derived, with a value of 1 indicating perfect health, 0 indicating a state equivalent to being dead, and <0 indicating a state considered worse than being dead. Patients also assessed their health state on a visual analog scale ranging from 0 (worst imaginable health state) to 100 (best imaginable health state). The more comprehensive EQ-5D utility index score was used for the analyses in this study. Utility scores were derived from the EQ-5D scales by applying UK tariffs.35
Depression severity was assessed by patients by the 9-item Patient Health Questionnaire (PHQ-9).36 The PHQ-9 assesses the severity of depressive symptoms over the previous 2 weeks on a scale from 0 (absence of depression) to 27 (severe depression); scores of 5–9, 10–14, 15–19, and >20 represent mild, moderate, moderately severe, and severe depression, respectively. Depression severity was also assessed by all participating investigators by the Clinical Global Impression–Severity of illness scale (CGI-S). CGI-S is a widely used assessment tool in a range of psychiatric diseases for rating the severity of illness on a 7-point scale; scores range from 1 (normal, not at all ill) to 7 (among the most extremely ill patients).37
Cognitive functioning was assessed by the Perceived Deficit Questionnaire 5-item (PDQ-5), which assesses the cognitive symptoms (e.g., memory, concentration, and executive function) experienced by the patient over the past 4 weeks.38,39 PDQ-5 total score ranges from 0 to 20, with higher scores reflecting greater severity of cognitive symptoms.
Statistical analysis
The population for analysis comprised all patients who met study inclusion criteria and who completed a baseline and at least one post-baseline assessment. All assessment data were summarized at each time point by descriptive statistics; continuous variables are presented as the number of observations and mean ± standard deviation (SD), and categorical and binary variables are presented as counts and percentages. Mean PHQ-9, PDQ-5, SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores were plotted with standard errors over time from baseline (up to month 12 for SF-12 MCS and PCS and up to month 24 for other outcomes). SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores were described according to severity of cognitive symptoms (i.e., by PDQ-5 score quartile) and PHQ-9 total score categories at all available time points.
To determine patient characteristics associated with HRQoL, a multi-step statistical analysis was performed at four time points: baseline, month 2, months 6 and 12 combined, and months 18 and 24 combined. SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores were analyzed separately. Each of these outcomes was compared between patient groups by univariate analysis of variance. The patient characteristics included in the univariate analyses were selected based on literature review and clinical experience (Supplementary materials). Patient characteristics with P<0.20 in the univariate analyses were then selected for the multivariate analysis of covariance model to which backwards stepwise variable selection was applied (i.e., sequential removal of the least significant variable from the model and recomputation of the model until all remaining variables had P<0.05). Four patient characteristics were forced into the model because they were identified as potential confounders (country, sex, and age at baseline for analyses at all time points, PHQ-9 total score at baseline for the baseline analyses and at month 2 for analyses at the other time points). As data from two visits were included in the month 6/month 12 and month 18/month 24 analyses, a mixed model for repeated measurements including a random effect for patients was used for these analyses. Missing data were not replaced in any of the analyses (i.e., all data included in the analyses were observed cases). Analyses were performed using SAS® statistical software (SAS Institute, Cary, NC, USA), version 9.2.
Results
Study population
A total of 1,159 patients completed the baseline visit and at least one follow-up visit without any violation of inclusion or exclusion criteria and were therefore included in the analysis. A total of 862 patients (74.4% of total) completed the full 2 years of follow-up. The demographic and baseline clinical characteristics of the study population are summarized in Table S1. Briefly, most patients were enrolled and followed up by GPs (83.6%), 56.6% had experienced a previous depressive episode, 78.7% were initiating antidepressant therapy, and 21.3% were switching antidepressant therapy for the first time. Mean (SD) age was 44.3 (12.0) years, and 73.2% of patients were female.
Evolution of HRQoL, depression severity, and perceived cognitive symptoms
Figure 1 shows mean SF-12 MCS, SF-12 PCS, EQ-5D utility index, PHQ-9, and PDQ-5 scores, with standard errors, over time. Mental HRQoL was impaired at baseline (mean [SD] SF-12 MCS total score, 26.5 [9.2]); the mean (SD) SF-12 PCS total score was 45.2 (12.1). SF-12 MCS score improved over the 12 months of follow-up (38.7 [11.6] at month 12), while SF-12 PCS score remained stable (45.3 [11.1] at month 12). The mean (SD) EQ-5D utility index score was 0.5 (0.3) at baseline, increasing to 0.7 (0.3) at month 2 and remaining stable at each subsequent visit (months 6, 12, 18, and 24).
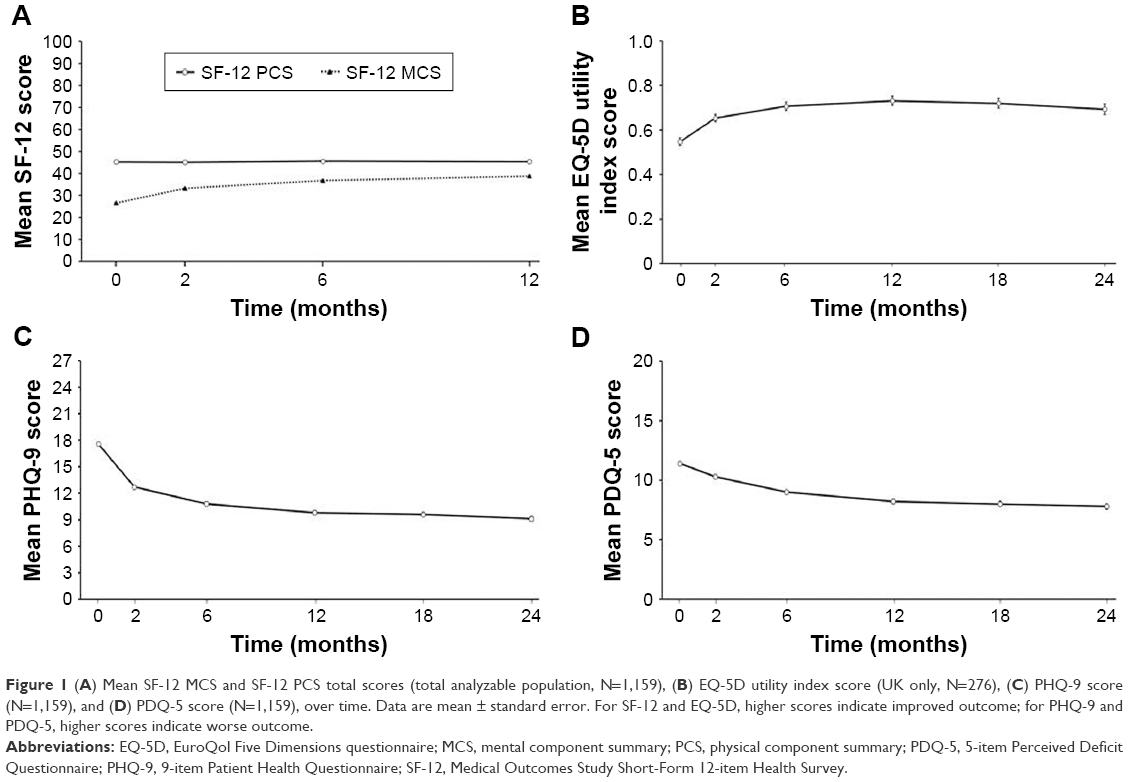 | Figure 1 (A) Mean SF-12 MCS and SF-12 PCS total scores (total analyzable population, N=1,159), (B) EQ-5D utility index score (UK only, N=276), (C) PHQ-9 score (N=1,159), and (D) PDQ-5 score (N=1,159), over time. Data are mean ± standard error. For SF-12 and EQ-5D, higher scores indicate improved outcome; for PHQ-9 and PDQ-5, higher scores indicate worse outcome. |
Patient-reported depression severity at baseline was moderate to severe (mean [SD] PHQ-9 score, 17.6 [5.3]). Marked improvement in depression severity was seen during the acute treatment phase (PHQ-9 score, 12.7 [6.2] at month 2 and 10.8 [6.6] at month 6), and this was sustained over the period of follow-up (PHQ-9 score, 9.1 [6.6] at month 24). With regard to cognitive symptoms, mean (SD) PDQ-5 score at baseline was 11.4 (4.6). Improvement in cognitive symptoms during the first 6 months after treatment initiation or switch was less marked than for depressive symptoms (mean PDQ-5 score, 10.3 [4.8] at month 2 and 9.0 [5.1] at month 6); mean PDQ-5 score at month 24 was 7.8 (5.2).
HRQoL according to severity of cognitive symptoms and depression over time
Figure 2 shows SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores by PDQ-5 total score quartiles over time. Figure 3 shows SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores by PHQ-9 total score categories over time. SF-12 MCS scores decreased (i.e., worsened) with increasing severity of cognitive symptoms at all time points up to 12 months, but increased (i.e., improved) over time for each quartile of cognitive symptom severity. A similar trend of worsened HRQoL with increasing severity of cognitive symptoms was seen for SF-12 PCS and EQ-5D utility index scores; however, for these outcomes, no overall improvement was seen for each quartile of cognitive symptom severity over time. Mean SF-12 MCS, SF-12 PCS, and EQ-5D utility index scores decreased (i.e., worsened) with increasing severity of depressive symptoms at all time points assessed.
 | Figure 2 Scores for (A) SF-12 MCS, (B) SF-12 PCS, and (C) EQ-5D utility index, categorized by PDQ-5 total score quartile at baseline, month 2, month 6/month 12, and month 18/month 24. |
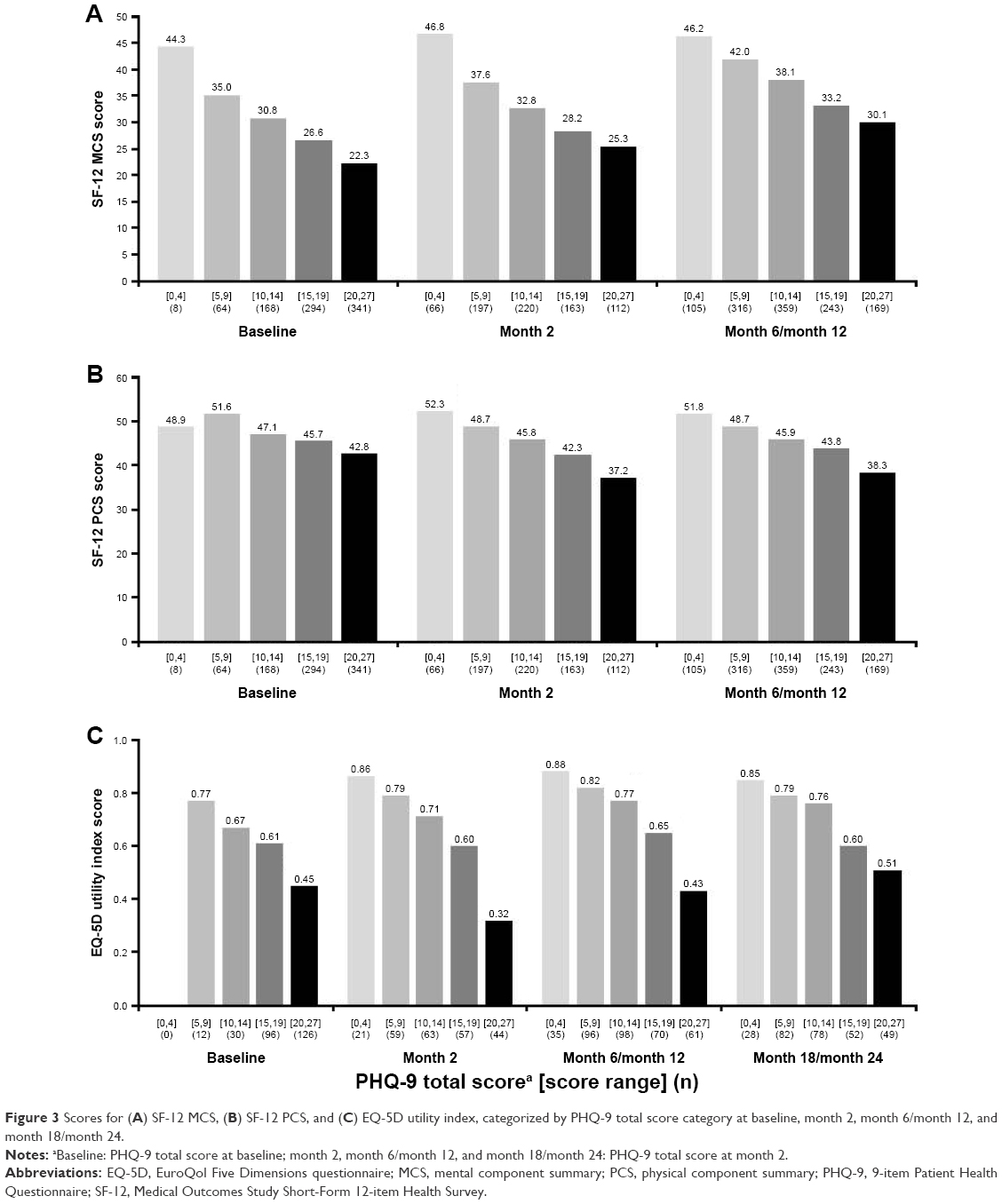 | Figure 3 Scores for (A) SF-12 MCS, (B) SF-12 PCS, and (C) EQ-5D utility index, categorized by PHQ-9 total score category at baseline, month 2, month 6/month 12, and month 18/month 24. |
Patient characteristics associated with HRQoL
Results of the univariate analyses of patient demographic and clinical characteristics associated with HRQoL are shown in Table S2 and Table S3. Results of the multivariate analysis of patient demographic and clinical characteristics associated with HRQoL are shown in Tables 1 and 2.
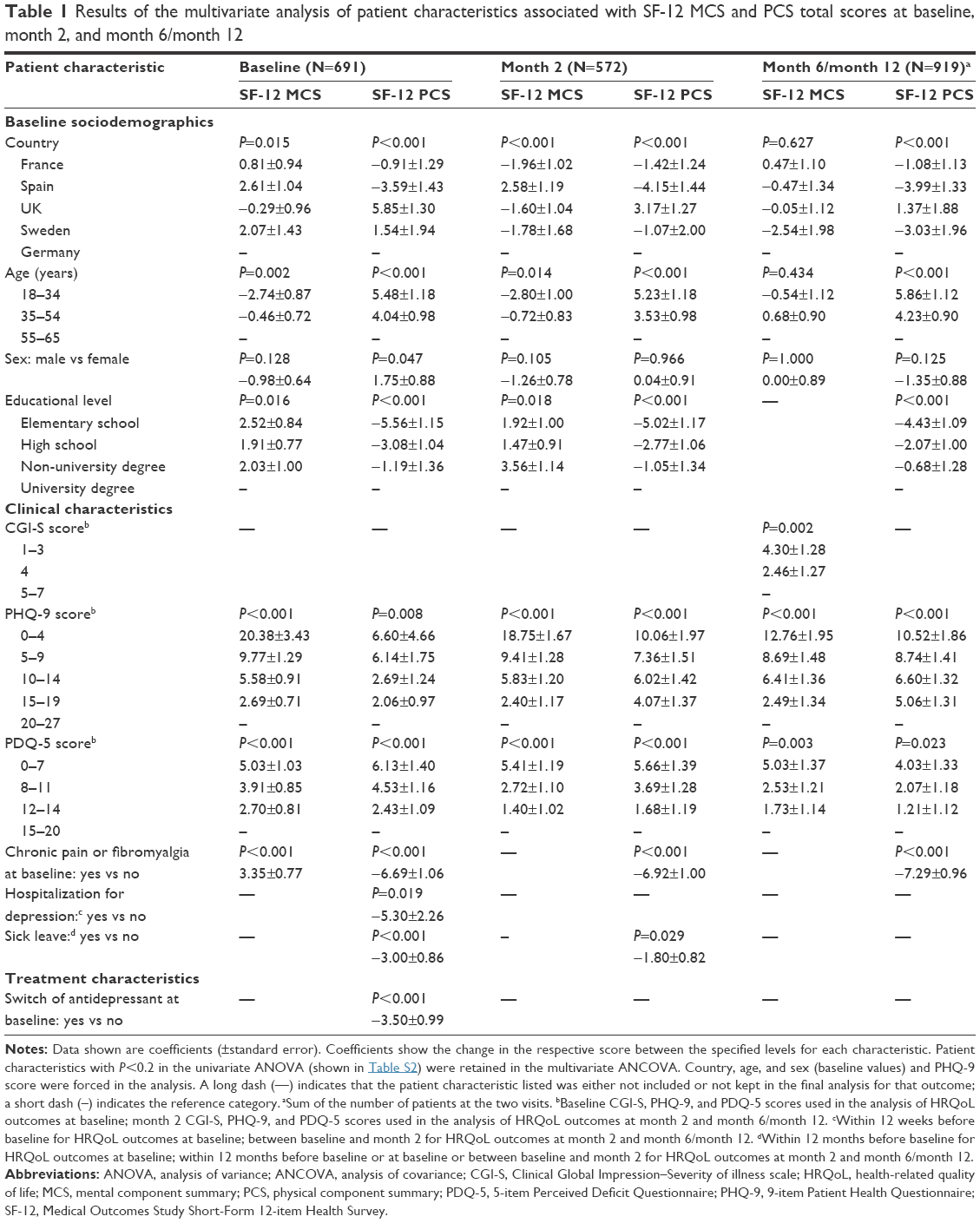 | Table 1 Results of the multivariate analysis of patient characteristics associated with SF-12 MCS and PCS total scores at baseline, month 2, and month 6/month 12 |
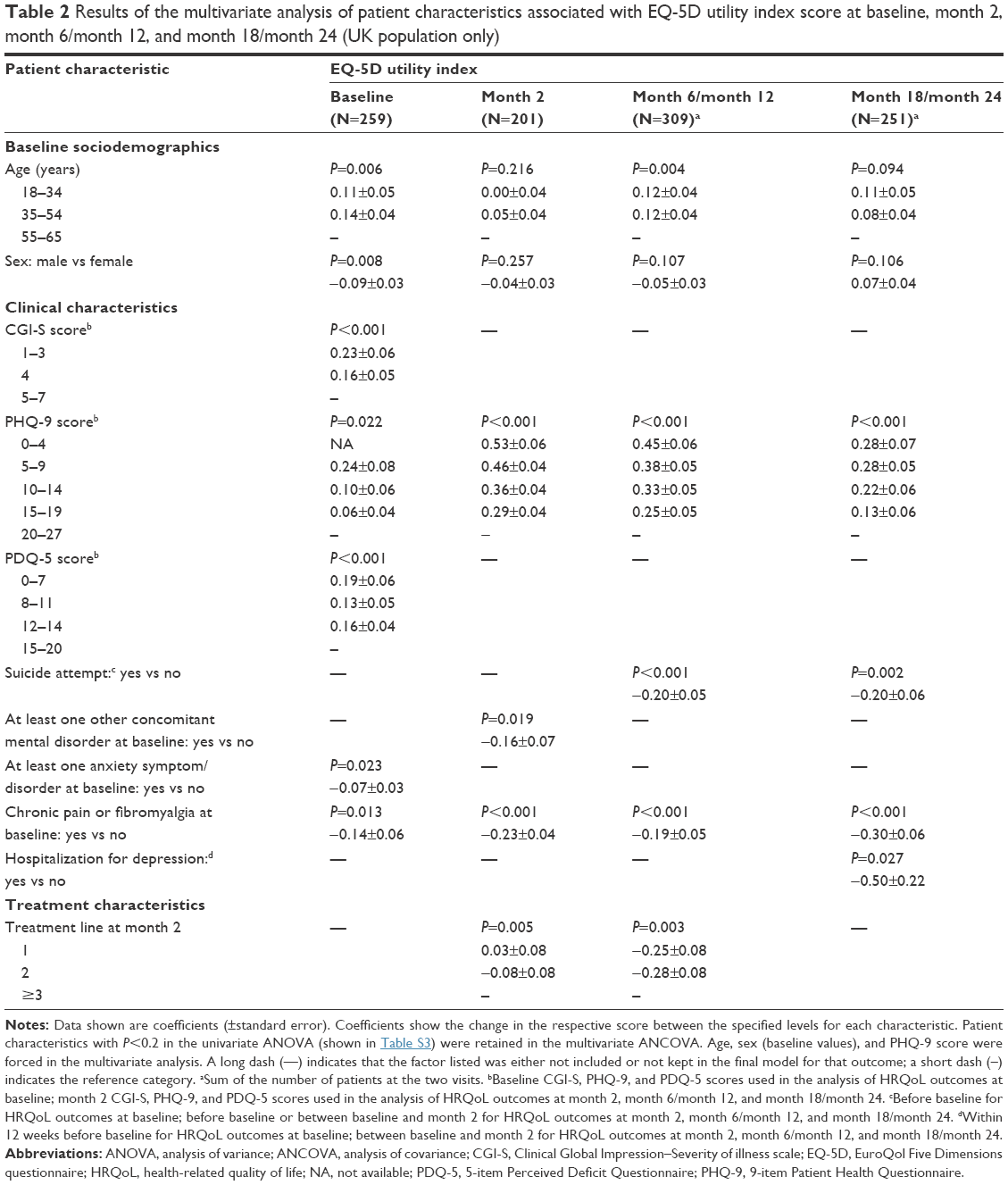 | Table 2 Results of the multivariate analysis of patient characteristics associated with EQ-5D utility index score at baseline, month 2, month 6/month 12, and month 18/month 24 (UK population only) |
Depression severity
Severity of depression at baseline, as assessed by patient-reported PHQ-9 total score, was significantly associated with HRQoL impairment at baseline (P<0.001 for SF-12 MCS, P=0.008 for SF-12 PCS, and P=0.022 for EQ-5D utility index score). Similarly, PHQ-9 total score at month 2 was significantly associated with HRQoL impairment at all post-baseline time points assessed (month 2 and month 6/month 12 for all three outcomes, as well as month 18/month 24 for EQ-5D; all P<0.001). Severity of depression as assessed by physicians using the CGI-S did not show consistent association with HRQoL; associations were seen between CGI-S and EQ-5D utility index scores at baseline (P<0.001), and between CGI-S score at month 2 and SF-12 MCS score at month 6/month 12 (P=0.002).
Cognitive symptoms
Severity of cognitive symptoms (PDQ-5 total score) at baseline was found to be significantly associated with impairment of HRQoL at baseline (P<0.001 for all three HRQoL outcomes). Severity of cognitive symptoms at month 2 was also significantly associated with HRQoL impairment at month 2 (P<0.001 for both SF-12 MCS and SF-12 PCS) and at month 6/month 12 (P=0.003 for SF-12 MCS; P=0.023 for SF-12 PCS).
Other patient characteristics
All baseline sociodemographic characteristics (country, age, sex, and educational level) were found to be significantly associated with at least two of the three HRQoL outcomes at various time points. Age at baseline demonstrated a significant association with HRQoL outcomes at baseline, month 2 and month 6/month 12 (all P<0.05). An association with sex was seen only for baseline HRQoL outcomes (P=0.047 for SF-12 PCS score; P=0.008 for EQ-5D utility index score). Educational level at baseline was significantly associated with both SF-12 outcomes at baseline and month 2 (all P<0.05). Experiencing chronic pain or fibromyalgia at baseline was significantly associated with at least two of the three HRQoL outcomes at baseline, month 2, and month 6/month 12 and with EQ-5D utility index score at month 18/month 24. Suicide attempt before month 2 (P=0.002) and hospitalization for depression between baseline and month 2 (P=0.027) were significantly associated with poorer EQ-5D utility index score at month 18/month 24.
Discussion
Results of this large, longitudinal, international cohort study of MDD show HRQoL to be severely impaired at the time of initiating or undergoing first switch of antidepressant monotherapy. While the magnitude of impairment observed at baseline was comparable with that seen in other observational studies in patients with depression,29,40,41 the baseline SF-12 MCS score was considerably lower (26.5 compared with ~50) than that reported for other common chronic diseases including cardiovascular disease, diabetes, respiratory diseases, and cancer42,43 or even that reported in patients a few months after surviving severe trauma injury.44 Consistent with the findings of other studies,10,45 the greatest improvement in HRQoL was observed during the acute phase of treatment (i.e., within 2 months of antidepressant initiation or switch), followed by more gradual improvement or stabilization during the maintenance phase (2–6 months). However, the long-term follow-up in this study allowed for a continued assessment of HRQoL progression and clearly demonstrates that a patient’s self-perceived health status is not fully restored after the acute and short-term maintenance phases of treatment, but in fact continues to be impaired long after. The mean SF-12 MCS score at month 12 was 38.7 (SD 11.6), which is still below the threshold considered indicative of significant impairment (42.0),32 indicating substantial room for improving outcomes in patients with MDD and achieving full recovery.
A novel finding in our study is the clear association between HRQoL impairment and the severity of cognitive symptoms during the first year of follow-up when HRQoL was assessed using the SF-12. This finding was independent of the severity of depression experienced by the patients. These findings are particularly important in light of previously published data from the PERFORM study demonstrating that the severity of cognitive symptoms is also independently associated with functional impairment, as assessed by the Sheehan Disability Scale, in patients with MDD.24 In addition, the PERFORM study has demonstrated how residual patient-reported cognitive symptoms in patients who achieve remission of depressive symptoms are significantly associated with an increased likelihood of relapse at 6 months.28 The findings by Saragoussi et al28 add to the existing literature documenting how the more typically studied residual symptoms of MDD, namely, mood and physical symptoms, pose a significant risk for relapse.46–48
Impairment of HRQoL was also found to be significantly associated with patient-reported depression severity for up to 2 years after initiating or undergoing first switch of antidepressant monotherapy. This is an important finding considering the numerous studies demonstrating how depression severity is inversely related to HRQoL during much shorter periods of observation.14,29,40,45,49–51 Similarly, the significant association of HRQoL with patient demographic characteristics (country, age, sex, and educational level) over the long term highlights the importance of considering these factors when planning long-term multinational clinical investigations, as the relevance of these factors has so far only been investigated in the short term.14,40,45,49,50
Interestingly, we found the presence of chronic pain or fibromyalgia at baseline to be consistently associated with impairment of the physical aspects of HRQoL as indicated by lower SF-12 PCS and EQ-5D utility index scores at all time points assessed over the 2-year follow-up period. This important finding adds to the vast existing literature on the prevalence and importance of the physical symptoms of depression, including pain, in both acute and remitted MDD patients, and the associated impairment of daily activities and reduction in many patients’ perceptions of the overall quality of life.52 The fact that chronic pain was still a predictor of poor quality of life 2 years after the patients in our study started antidepressant medication or switched antidepressant for the first time clearly highlights a very important unmet medical need in addressing this serious symptom of depression.
A major strength of this study is that it was performed in a real-world setting with long-term longitudinal follow-up of a large cohort of patients, the majority of whom were enrolled and followed up by GPs. Study sites were balanced according to the national proportions of GPs treating patients with depression to ensure that findings were applicable to routine practice. Sociodemographic and clinical characteristics of enrolled patients were as expected for an MDD population.53 Further strengths include the low attrition rate (74.4% of patients completed the 24-month visit) and the long duration of follow-up, particularly with regard to the assessment of HRQoL, which is usually only evaluated for ≤6 months in observational studies (e.g., the European FINDER study) in patients with depression.29,40,54–56 The use of patient-reported outcomes to gather information on the impact of MDD from the patient’s own perspective is another notable advantage as such data represent an important complement to the examinations of health status of patients with physical or mental illness. This has been suggested to be particularly relevant in patients with mental health disorders such as MDD.57 Analysis of the association between cognitive symptoms and HRQoL assessed using the EQ-5D specifically was limited by the fact that this questionnaire was only used in the UK, thereby reducing the statistical power of the analysis. This may at least in part explain why the observed association between severity of cognitive symptoms and EQ-5D utility index score at baseline was not seen at subsequent time points as was observed for the SF-12 MCS and PCS, although this could also be due to the greater association of EQ-5D utility index score with other factors, such as depression severity. A further limitation is that the study only recruited outpatients who were initiating antidepressant monotherapy or switching antidepressant monotherapy for the first time; this means that the study results cannot be generalized to the entire MDD population in Europe, particularly those at a later disease stage or those receiving psychotherapy only.
Conclusion
Results of this large, 2-year European cohort study show that the mental component of HRQoL is markedly impaired in patients with MDD below the level of impairment reported for other common chronic diseases. Importantly, from a clinical perspective, the impairment of HRQoL was not only driven by the severity of depressive symptoms but also independently associated with the severity of cognitive symptoms when adjusted for depression severity. These findings suggest that cognitive functioning is an important treatment target for patients with MDD.
Acknowledgments
The authors would like to express their gratitude to all the patients and physicians who participated in the study. The authors also thank Professor Bengt Jönsson (Department of Economics, Stockholm School of Economics, Stockholm, Sweden) and Professor Martin Knapp (Personal Social Services Research Unit, London School of Economics and Political Science, London, UK) for their advice regarding the PERFORM study design and interpretation of the study findings, Mapi for logistical management of the study, and Inferential for assistance with statistical analyses. Editorial assistance was provided by Jennifer Coward of Anthemis Consulting Ltd, funded by H Lundbeck A/S. This study was funded by Lundbeck SAS.
Disclosure
JMH has received honoraria for being an advisor or providing educational talks for Lundbeck, Otsuka, Roche, and Eli Lilly and Company. MCC and LHH are full-time employees of H Lundbeck A/S. MT is a full-time employee of Lundbeck LLC. At the time the study was conducted, DS and BR were full-time employees of Lundbeck SAS. The authors report no other conflicts of interest in this work.
References
World Health Organization [webpage on the Internet]. Fact sheet: depression. Updated February 2017. Available from: http://www.who.int/mediacentre/factsheets/fs369/en/. Accessed November 30, 2017. | ||
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. | ||
Karimi M, Brazier J. Health, health-related quality of life, and quality of life: what is the difference? Pharmacoeconomics. 2016;34(7):645–649. | ||
IsHak WW, Mirocha J, James D, et al. Quality of life in major depressive disorder before/after multiple steps of treatment and one-year follow-up. Acta Psychiatr Scand. 2015;131(1):51–60. | ||
Kennedy SH, Eisfeld BS, Cooke RG. Quality of life: an important dimension in assessing the treatment of depression? J Psychiatry Neurosci. 2001;26(Suppl):S23–S28. | ||
Demyttenaere K, De Fruyt J, Huygens R. Measuring quality of life in depression. Curr Opin Psychiatry. 2002;15(1):89–92. | ||
Berlim MT, Fleck MP. “Quality of life”: a brand new concept for research and practice in psychiatry. Rev Bras Psiquiatr. 2003;25(4):249–252. | ||
Papakostas GI, Petersen T, Mahal Y, Mischoulon D, Nierenberg AA, Fava M. Quality of life assessments in major depressive disorder: a review of the literature. Gen Hosp Psychiatry. 2004;26(1):13–17. | ||
Langlieb AM, Guico-Pabia CJ. Beyond symptomatic improvement: assessing real-world outcomes in patients with major depressive disorder. Prim Care Companion J Clin Psychiatry. 2010;12(2):PCC.09r00826. | ||
IsHak WW, Greenberg JM, Balayan K, et al. Quality of life: the ultimate outcome measure of interventions in major depressive disorder. Harv Rev Psychiatry. 2011;19(5):229–239. | ||
McIntyre RS, Cha DS, Soczynska JK, et al. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depress Anxiety. 2013;30(6):515–527. | ||
Demyttenaere K, Donneau AF, Albert A, Ansseau M, Constant E, van Heeringen K. What is important in being cured from depression? Discordance between physicians and patients. J Affect Disord. 2015;174:390–396. | ||
Rapaport MH, Clary C, Fayyad R, Endicott J. Quality-of-life impairment in depressive and anxiety disorders. Am J Psychiatry. 2005;162(6):1171–1178. | ||
Daly EJ, Trivedi MH, Wisniewski SR, et al. Health-related quality of life in depression: a STAR*D report. Ann Clin Psychiatry. 2010;22(1):43–55. | ||
ten Doesschate MC, Koeter MW, Bockting CL, Schene AH; DELTA Study Group. Health related quality of life in recurrent depression: a comparison with a general population sample. J Affect Disord. 2010;120(1–3):126–132. | ||
IsHak WW, Balayan K, Bresee C, et al. A descriptive analysis of quality of life using patient-reported measures in major depressive disorder in a naturalistic outpatient setting. Qual Life Res. 2013;22(3):585–596. | ||
Roberts J, Lenton P, Keetharuth AD, Brazier J. Quality of life impact of mental health conditions in England: results from the adult psychiatric morbidity surveys. Health Qual Life Outcomes. 2014;12:6. | ||
Kim JM, Chalem Y, di Nicola S, Hong JP, Won SH, Milea D. A cross-sectional study of functional disabilities and perceived cognitive dysfunction in patients with major depressive disorder in South Korea: the PERFORM-K study. Psychiatry Res. 2016;239:353–361. | ||
Lam RW, McIntosh D, Wang J, et al; CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 1. Disease Burden and Principles of Care. Can J Psychiatry. 2016;61(9):510–523. | ||
Angermeyer MC, Holzinger A, Matschinger H, Stengler-Wenzke K. Depression and quality of life: results of a follow-up study. Int J Soc Psychiatry. 2002;48(3):189–199. | ||
Baune BT, Miller R, McAfoose J, Johnson M, Quirk F, Mitchell D. The role of cognitive impairment in general functioning in major depression. Psychiatry Res. 2010;176(2–3):183–189. | ||
Gonda X, Pompili M, Serafini G, Carvalho AF, Rihmer Z, Dome P. The role of cognitive dysfunction in the symptoms and remission from depression. Ann Gen Psychiatry. 2015;14:27. | ||
Clark M, DiBenedetti D, Perez V. Cognitive dysfunction and work productivity in major depressive disorder. Expert Rev Pharmacoecon Outcomes Res. 2016;16(4):455–463. | ||
Hammer-Helmich L, Haro JM, Jönsson B, et al. Functional impairment in patients with major depressive disorder: the 2-year PERFORM study. Neuropsychiatr Dis Treat. 2018;14:239–249. | ||
Lam RW, Kennedy SH, Mclntyre RS, Khullar A. Cognitive dysfunction in major depressive disorder: effects on psychosocial functioning and implications for treatment. Can J Psychiatry. 2014;59(12):649–654. | ||
Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2015;49(12):1087–1206. | ||
McIntyre RS, Suppes T, Tandon R, Ostacher M. Florida best practice psychotherapeutic medication guidelines for adults with major depressive disorder. J Clin Psychiatry. 2017;78(6):703–713. | ||
Saragoussi D, Touya M, Haro JM, et al. Factors associated with failure to achieve remission and with relapse after remission in patients with major depressive disorder in the PERFORM study. Neuropsychiatr Dis Treat. 2017;13:2151–2165. | ||
Fattori A, Neri L, Bellomo A, Vaggi M, Mencacci C; ILDE Study Group. Depression severity and concentration difficulties are independently associated with HRQOL in patients with unipolar depressive disorders. Qual Life Res. 2017;26(9):2459–2469. | ||
Shimizu Y, Kitagawa N, Mitsui N, et al. Neurocognitive impairments and quality of life in unemployed patients with remitted major depressive disorder. Psychiatry Res. 2013;210(3):913–918. | ||
Cotrena C, Branco LD, Shansis FM, Fonseca RP. Executive function impairments in depression and bipolar disorder: association with functional impairment and quality of life. J Affect Disord. 2016;190:744–753. | ||
Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. | ||
Wisniewski SR, Rush AJ, Bryan C, et al. Comparison of quality of life measures in a depressed population. J Nerv Ment Dis. 2007;195(3):219–225. | ||
EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. | ||
Dolan P, Gudex C, Kind P, Williams A. A social tariff for EuroQol: results from a UK population survey. Discussion paper 138. York: University of York; September 1995. http://www.york.ac.uk/che/pdf/DP138.pdf. Accessed April 23, 2018. | ||
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. | ||
Guy W. Clinical Global Impressions. ECDEU Assessment Manual for Psychopharmacology. Rockville, USA: National Institute of Mental Health; 1976. | ||
Sullivan MJ, Edgley K, Dehoux E. A survey of multiple sclerosis. Part 1. Perceived cognitive problems and compensatory strategy use. Can J Rehabil. 1990;4:99–105. | ||
National Multiple Sclerosis Society. Multiple Sclerosis Quality of Life Inventory: A User’s Manual. New York: The Consortium of Multiple Sclerosis Centers Health Services Research Subcommittee, The National Multiple Sclerosis Society; 1997. | ||
Lenox-Smith A, Macdonald MT, Reed C, et al. Quality of life in depressed patients in UK primary care: the FINDER study. Neurol Ther. 2013;2(1–2):25–42. | ||
Kolovos S, Bosmans JE, van Dongen JM, et al. Utility scores for different health states related to depression: individual participant data analysis. Qual Life Res. 2017;26(7):1649–1658. | ||
Putrik P, Ramiro S, Chorus AM, Keszei AP, Boonen A. Socioeconomic inequities in perceived health among patients with musculoskeletal disorders compared with other chronic disorders: results from a cross-sectional Dutch study. RMD Open. 2015;1(1):e000045. | ||
Thiel DM, Al Sayah F, Vallance JK, Johnson ST, Johnson JA. Association between physical activity and health-related quality of life in adults with type 2 diabetes. Can J Diabetes. 2017;41(1):58–63. | ||
Christensen MC, Banner C, Lefering R, Vallejo-Torres L, Morris S. Quality of life after severe trauma: results from the global trauma trial with recombinant factor VII. J Trauma. 2011;70(6):1524–1531. | ||
Reed C, Monz BU, Perahia DG, et al. Quality of life outcomes among patients with depression after 6 months of starting treatment: results from FINDER. J Affect Disord. 2009;113(3):296–302. | ||
Paykel ES, Ramana R, Cooper Z, Hayhurst H, Kerr J, Barocka A. Residual symptoms after partial remission: an important outcome in depression. Psychol Med. 1995;25(6):1171–1180. | ||
Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as predictor of rapid relapse. J Affect Disord. 1998;50(2–3):97–108. | ||
Kanai T, Takeuchi H, Furukawa TA, et al. Time to recurrence after recovery from major depressive episodes and its predictors. Psychol Med. 2003;33(5):839–845. | ||
Trivedi MH, Rush AJ, Wisniewski SR, et al. Factors associated with health-related quality of life among outpatients with major depressive disorder: a STAR*D report. J Clin Psychiatry. 2006;67(2):185–195. | ||
Lin CH, Yen YC, Chen MC, Chen CC. Depression and pain impair daily functioning and quality of life in patients with major depressive disorder. J Affect Disord. 2014;166:173–178. | ||
Köhler S, Unger T, Hoffmann S, Mackert A, Ross B, Fydrich T. The relationship of health-related quality of life and treatment outcome during inpatient treatment of depression. Qual Life Res. 2015;24(3):641–649. | ||
Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl 1):12–16. | ||
Martín-Merino E, Ruigómez A, Johansson S, Wallander MA, García-Rodriguez LA. Study of a cohort of patients newly diagnosed with depression in general practice: prevalence, incidence, comorbidity, and treatment patterns. Prim Care Companion J Clin Psychiatry. 2010;12(1):PCC.08m00764. | ||
Sobocki P, Ekman M, Agren H, et al. Health-related quality of life measured with EQ-5D in patients treated for depression in primary care. Value Health. 2007;10(2):153–160. | ||
Shelton RC, Sloan Manning J, Barrentine LW, Tipa EV. Assessing effects of l-methylfolate in depression management: results of a real-world patient experience trial. Prim Care Companion CNS Disord. 2013;15(4):PCC.13m01520. | ||
Montoya A, Lebrec J, Keane KM, et al. Broader conceptualization of remission assessed by the remission from depression questionnaire and its association with symptomatic remission: a prospective, multicenter, observational study. BMC Psychiatry. 2016;16(1):352. | ||
Andresen R, Caputi P, Oades LG. Do clinical outcome measures assess consumer-defined recovery? Psychiatry Res. 2010;177(3):309–317. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.