")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Long QT and death in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease is not related to electrolyte disorders
Authors Zilberman-Itskovich S, Rahamim E, Tsiporin-Havatinsky F, Ziv-Baran T, Golik A, Zaidenstein R
Received 6 December 2018
Accepted for publication 16 April 2019
Published 20 May 2019 Volume 2019:14 Pages 1053—1061
DOI https://doi.org/10.2147/COPD.S196428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Shani Zilberman-Itskovich,1 Eldad Rahamim,1 Faina Tsiporin-Havatinsky,1 Tomer Ziv-Baran,2 Ahuva Golik,1 Ronit Zaidenstein1
1Internal Medicine Department A, Assaf-Harofeh Medical Center, Zerifin, Israel; 2School of Public Health, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Objectives: COPD is the fourth-leading cause of mortality worldwide. Prolonged QTc has been found to be a long-term negative prognostic factor in ambulatory COPD patients. The aim of this study was to evaluate the extent of prolonged-QTc syndrome in COPD patients upon admission to an internal medicine department, its relationship to hypomagnesemia, hypokalemia, and hypocalcemia, and the effect of COPD treatment on mortality during hospital stay.
Methods: This prospective cohort study evaluated COPD patients hospitalized in an internal medicine department. The study evaluated QTc, electrolyte levels, and known risk factors during hospitalization of COPD patients.
Results: A total of 67 patients were recruited. The median QTc interval was 0.441 seconds and 0.434 seconds on days 0 and 3, respectively. Prolonged QTc was noted in 35.8% of patients on admission and 37.3% on day 3 of hospitalization. The median QTc in the prolonged-QTc group on admission was 0.471 seconds and in the normal-QTc group 0.430 seconds. There was no significant difference in age, sex, electrolyte levels, renal function tests, or blood gases on admission between the two groups. Mortality during the hospital stay was significantly higher in the prolonged-QTc group (3 deaths, 12%) than in the normal QTc group (no deaths) (P=0.04). A subanalysis was performed, removing known causes for prolonged QTc. We found no differences in age, electrolytes, or renal functions. There was a small but significant difference in bicarbonate levels.
Conclusion: Our findings demonstrated that there was no correlation between QTc prolongation in hospitalized COPD patients and electrolyte levels, comorbidities, or relevant medications. A higher rate of mortality was noted in patients with prolonged QTc in comparison to normal QTc. As such, it is suggested that prolonged QTc could serve as a negative prognostic factor for mortality during hospitalization in COPD patients.
Keywords: COPD, QT prolongation, hypomagnesemia, hypokalemia, hypocalcemia
Plain language summary
In this study, we examined electrocardiographic (ECG) changes and prolonged QTc, in patients with COPD admitted to an internal department. ECG abnormality is related to cardiac arrhythmia and death, and is usually caused by drug treatment and electrolyte imbalance. In this study, we found 36% long QTc in hospitalized COPD patients, but without any relationship to known risk factors. All mortality during hospitalization was in the prolonged-QTc group. The authors suggest prolonged QTc as a negative prognostic factor for mortality in COPD patients and advise drug therapy that does not cause prolonged QTc for this group.
Introduction
COPD is a common reason for morbidity and hospitalizations and is the fourth-leading cause of mortality worldwide.1,2 Treatment is aimed at prevention of acute exacerbations (AEs).1,2 Chronic management of COPD is composed of behavioral and medication treatments, with the most widely used being bronchodilator and corticosteroid inhalers. Treatment for AE in COPD (AE-COPD) includes administration of systemic corticosteroids, antibiotics, and bronchodilators.1–4 Both chronic and AE medications have the potential of causing electrolyte disorders.5–9
Evidence has accumulated in the past few years demonstrating a relationship between COPD patients and cardiovascular morbidity and mortality.10 In an outpatient COPD population, prolonged QTc was detected in a third of the patients, and the only independent factor related to this finding was hypoxia.11 In patients with COPD and no major comorbidities, prolonged QTc was found to be related to long-term mortality without correlation with degree of COPD severity.12 Repolarization abnormalities on electrocardiography (ECG), reflected as prolonged QTc segment and QT variations, were observed in COPD patients.12 These repolarization abnormalities are related to ventricular arrhythmias and mortality.13
Hypomagnesemia has been demonstrated to increase the risk of cardiovascular events, including long-QT syndrome and ventricular arrhythmias.14 Magnesium is the second-most abundant intracellular divalent cation in the human body. It is an obligatory element in many mandatory intracellular signaling processes and serves as a cofactor in enzymatic reactions.15 Hypomagnesemia, defined as magnesium serum levels <1.7 mEq/L, is a common observation in hospitalized patients and related to morbidity and mortality during hospitalization.16 Etiology for hypomagnesemia is diverse: related to reduced intake, intracellular shift, and renal and gastrointestinal losses.14,17 Gourgoulianis et al suggested that magnesium has a bronchodilatory effect on smooth-muscle cells in the respiratory tree.18 The bronchoconstriction observed in hospitalized AE-COPD patients can be a result of hypomagnesemia, frequently observed in these patients.19
Medical treatment is considered one of the most prevalent causes of hypomagnesemia nowadays. Many medications increase renal loss of magnesium, thereby exposing patients to hypomagnesemia’s consequences. Drugs that carry an increased risk of hypomagnesemia are antibiotics,6 diuretics, and proton-pump inhibitors (PPIs),20,21 all potential causes of prolonged QTc.13 Some of the influences of hypomagnesemia are increased risk of hypokalemia and hypocalcemia, thereby augmenting the risk of QT-segment prolongation.14,22
The aim of this study was to evaluate the extent of prolonged QT segments in COPD patients upon admission to an internal medicine department (IMD), its relation to hypomagnesemia, hypokalemia, and hypocalcemia, and the effect of AE-COPD treatment during hospitalization on these variables and mortality.
Methods
In this prospective, noninterventional, cohort clinical trial, COPD patients admitted to the Department of Internal Medicine A, Assaf-Harofeh Medical Center, Israel from September 2016 until December 2017 were enrolled. The study was approved by the institutional ethics committee, and written informed consent was obtained from all patients. The study was conducted in accordance with the Declaration of Helsinki.
Patients were recruited on admission. They were eligible to participate in the study if they were ≥18 years old, capable of signing informed consent, and had been diagnosed with COPD according to the standard criteria of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines: symptoms of chronic (minimum 3 months) dyspnea, cough, or sputum in combination with spirometry test demonstrating irreversible obstructive disease.2,23 Exclusion criteria were pulmonary congestion, severe pleural effusion, pneumothorax, diagnosis of restrictive disease according to a pulmonologist, or spirometry demonstrating FEV1/FVC>0.7, dementia, unconscious at admission, and pregnancy. Patients with known cardiac diseases were not excluded from the study. AE-COPD was defined as worsening of respiratory symptoms (increased dyspnea, cough, or sputum) beyond the normal day-to-day variation in symptoms, as per GOLD guidelines.2,23
Patients’ medical history was recorded upon admission and during the hospital stay. Venous blood samples were withdrawn for magnesium, potassium, calcium (corrected to albumin), CO2, and parathyroid hormone (PTH) on the day of admission and day 3 of hospitalization. Electrolyte levels were measured from plasma. A “spot“ urine test for creatinine and magnesium was performed at hospitalization. Urinary fraction excretion of magnesium was calculated as (urinary Mg × plasma creatinine)/0.7 × (plasma Mg × urinary creatinine). No intervention was done for correcting electrolyte disturbances or the choice of antibiotic therapy by the authors, and treatment was done according to physician decisions.
ECG was conducted on the day of admission and day 3 of hospitalization. ECG analysis was performed using a Fukuda FX-8222 on all patients. QT was measured manually by two physicians. The longest QTc interval was calculated using Bazett’s formula for each patient. Maximal heart rate for the measurement was 120 bpm. Prolonged QTc was defined as >450 milliseconds for men and >460 milliseconds for women.24
The primary outcomes of the study were prolonged QTc, serum levels of magnesium, calcium, potassium, and CO2, and the relationship between them. The second outcome was the effect of drug administration before and during hospitalization on electrolytes and QT-segment changes.
Statistical analysis was performed using SPSS version 25. Categorical variables are reported as frequency and percentage, and continuous variables as median and IQR or mean and SD, according to distribution. For descriptive statistics during hospitalization, McNemar’s test and Wilcoxon's signed-rank test was used. In subgroup analysis, for categorical variables, Fisher’s exact test and χ2 were used based on sample size and distribution of variables, and for continuous variables the Mann–Whitney U test was used. All statistical tests were two sided. P<0.05 was considered statistically significant.
Results
A total of 67 patients were recruited during the study. Baseline characteristics of the patients are presented in Table 1. Mean age was 70±11 years, 48% were female, and 75% were being treated chronically with bronchodilator inhalers, 66% with corticosteroid inhalers, 42% with home oxygen therapy, and 24% with bilevel positive airway pressure. AE-COPD was the main diagnosis on admission to hospital.
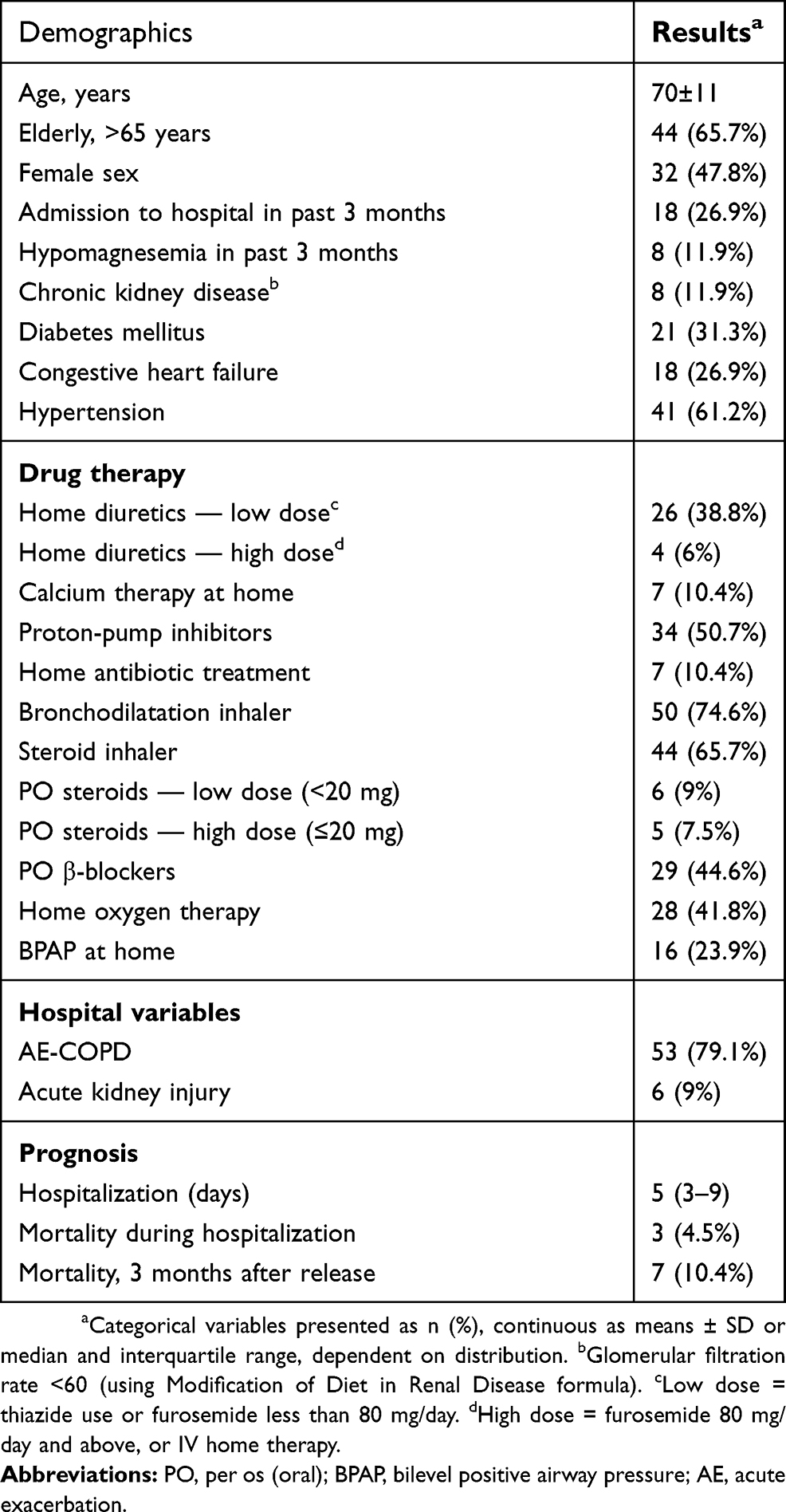 | Table 1 Patient demographics and clinical characteristics (n=67) |
Upon admission, median potassium level was 4.1(IQR 3.8–4.5) mmol/L and 4.0 (IQR 3.62–4.4) mmol/L at day 3 of hospitalization. Two patients (3%) had hypokalemia upon admission and seven patients (10.4%) on day 3. Only one patient had both hypomagnesemia and hypokalemia. Median magnesium level upon admission was 1.87 (IQR 1.77–2.04) mg/dL and 2.04 (IQR 1.84–2.18) mg/dL on day 3. Seven patients (10.4%) had hypomagnesemia upon admission and five patients (8.9%) on day 3. Median calcium level (corrected for albumin) upon admission was 9.12 (IQR 8.8–9.5) mg/dL and 9.15 (IQR 8.85–9.36) mg/dL on day 3. Four patients (6%) had hypocalcemia upon admission and three patients (5%) on day 3. Median PTH level upon admission was 5.7 pmol/L. Median QTc interval upon admission was 0.441 (IQR 0.424–0.467) seconds and 0.434 (IQR 0.410–0.465) seconds at 3 days. Prolonged QTc upon admission was noted in 24 patients (35.8%), and 19 patients (37.3%) had prolonged QTc at day 3 (Table 2).
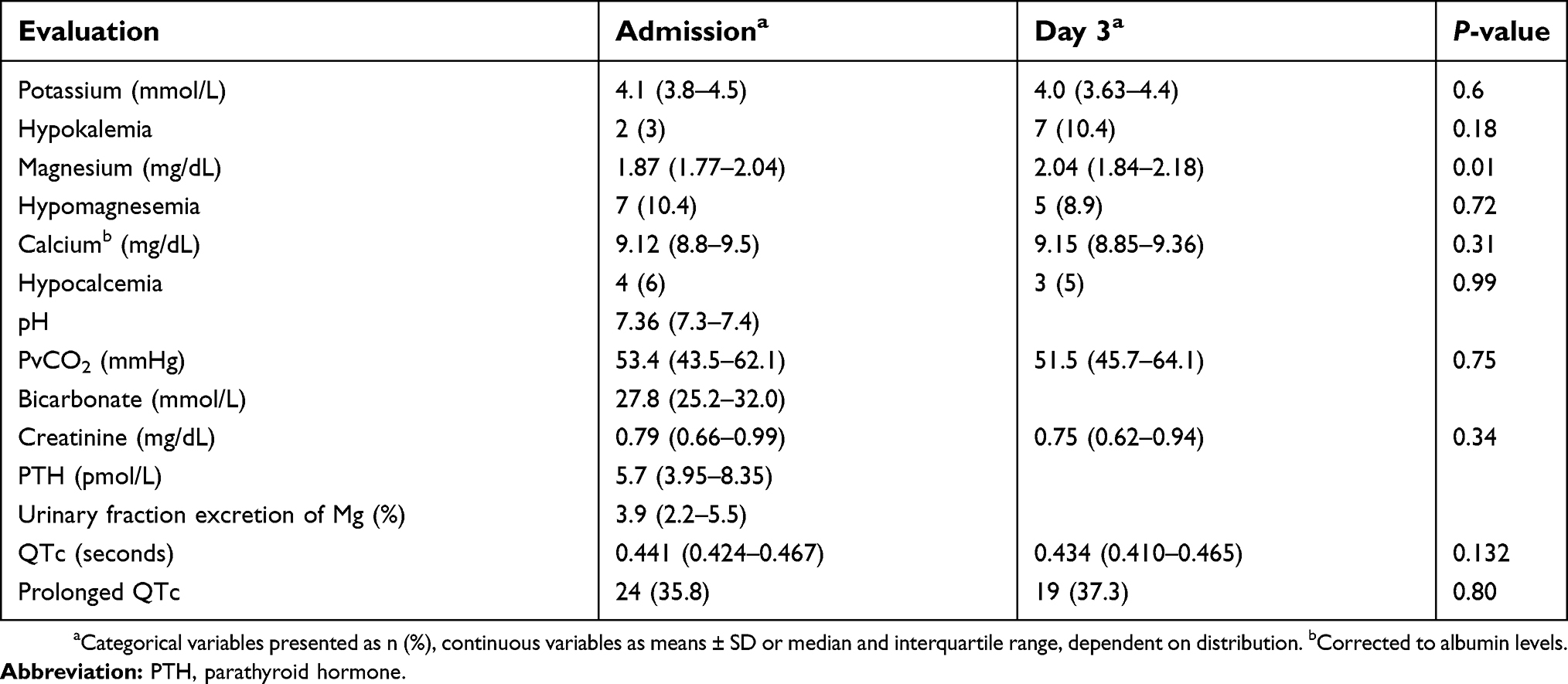 | Table 2 Laboratory evaluation and QTc at admission and after 3 days |
Comparison of patients with prolonged QTc upon admission and those with normal QTc showed that median QTc was 0.471 (IQR 0.465–0.500) vs 0.430 (IQR 0.410–0.440) seconds, respectively. There were no significant differences in age, sex, electrolyte levels, creatinine, or blood gases on admission between the two groups. Median PTH levels were higher in the prolonged-QTc group than the normal group (7.55 vs 5.2 pmol/L, P=0.04). Chronic kidney–disease prevalence was higher in the prolonged-QTc group with six patients (25%) vs two patients (4.7%) from the normal-QTc group (P=0.02). There was no significant difference between the groups in prevalence of diabetes mellitus, congestive heart failure, hypertension, hypothyroidism, home treatment with diuretics of any dosage, use of PPIs, antibiotic treatment prior to hospitalization, β-blocker treatment, use of glucocorticoids (inhaled or oral), or bronchodilator treatment (Table 3).
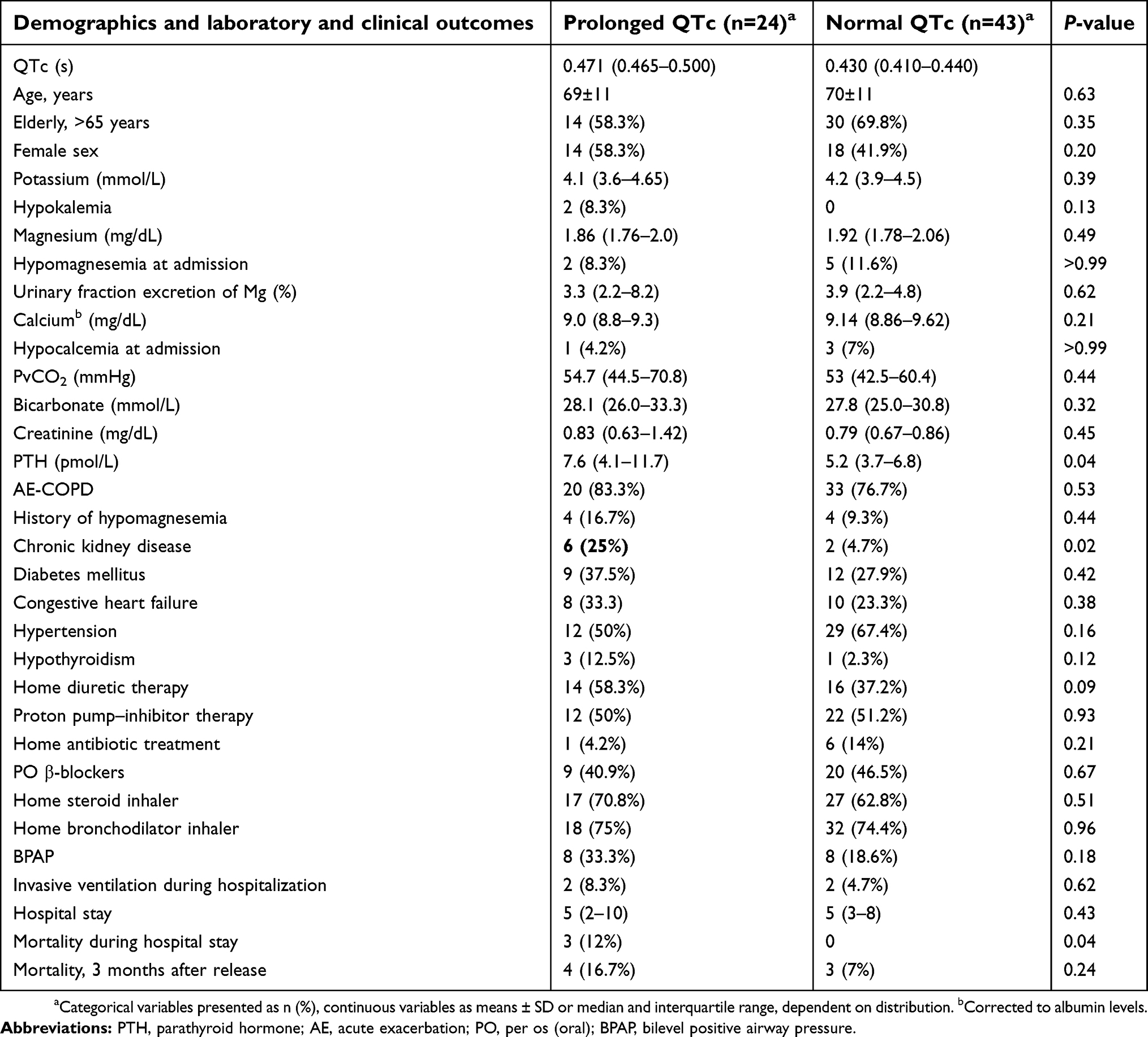 | Table 3 Comparison between patients with normal-range QTc to those with prolonged QTc upon admission: demographics, laboratory, and clinical outcomes |
Mortality during hospitalization was significantly higher in the prolonged-QTc group (three deaths, 12%), with no deaths in the normal-QTc group (P=0.04). No significant difference in mortality was observed at 3 months posthospitalization (Table 3). Mortality reasons during hospitalization were respiratory failure (two patients) and septic shock (one patient).
Very prolonged QTc of >0.5 seconds was observed in six patients (9% of total cohort). None of these patients died during hospitalization, and only one died in the 3 months following the index hospitalization.
Spearman’s correlation coefficient was used to evaluate the association between QTc-interval length and the three major electrolyte deficiencies known to affect it: potassium, magnesium, and calcium. Correlations revealed P-values of 0.132, 0.428, and 0.551 and coefficients of −0.186, −0.099, and −0.074 for potassium, magnesium, and calcium respectively.
Subanalysis was performed omitting known causes for prolonged QTc: β-blockers, PPIs, home antibiotic therapy prior to hospitalization, amiodarone, and chemotherapy. In the remaining patients, median QTc was 0.471 seconds in the prolonged-QTc group (IQR 0.466–0.484 seconds) and 0.419 seconds in the normal-QTc group (IQR 0.397–0.441 seconds). There were significantly more females in the prolonged-QTc group (76.9% in the prolonged-QTc vs 36.4% in the normal group, P=0.02). No difference was observed in age, electrolytes, or renal function tests.
However, upon subanalysis a significant difference in the of bicarbonate levels was noted: 29 (IQR 26.8–35.3) mmol/L in the prolonged-QTc group compared with 25.9 (IQR 23.8–30.1) mmol/L in the normal-QTc group (P=0.04). There was no significant difference in the rate of acute exacerbation between the two groups. In addition, no significant differences between the normal- and prolonged-QTc groups regarding PTH, comorbidities, or drug therapy were observed (Table 4).
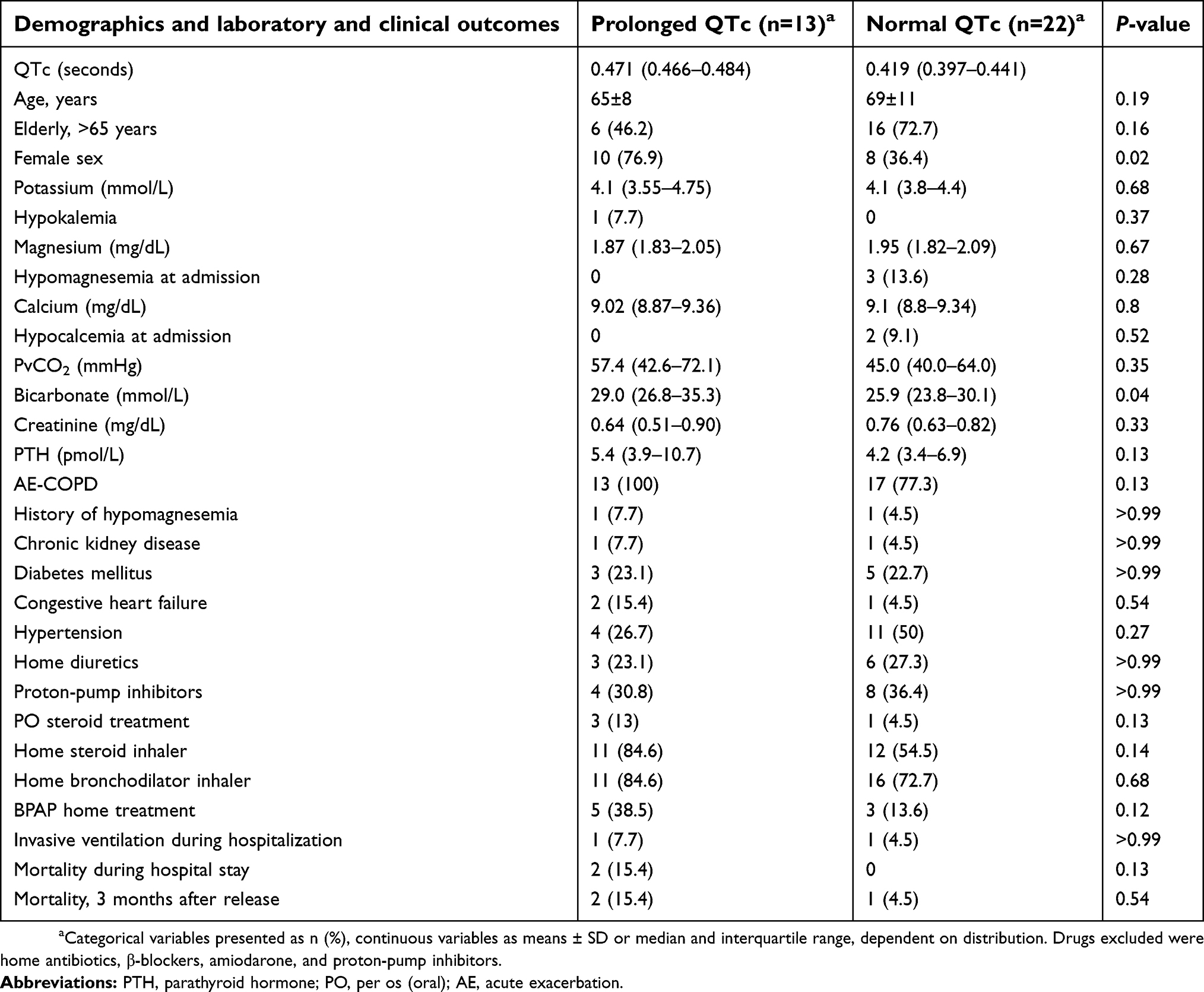 | Table 4 Subanalysis of patients with no known medication related to prolonged QTc: patients with prolonged vs normal QTc |
Discussion
In this study, we examined the ECG and electrolytes of COPD patients upon admission to an IMD and 3 days after hospitalization. Patients were mainly elderly and suffered from comorbidities, including hypertension, diabetes, and congestive heart failure. Prolonged QTc was observed in 35% of patients. No correlation was found between QTc interval and any electrolyte disturbance. Hospital stay was 5 days and mortality during hospitalization 4.5%, which occurred only in patients with prolonged QTc.
Our findings demonstrated that QTc prolongation was an independent risk factor of morbidity unrelated to electrolyte disorders. These findings are consistent with previous studies, which demonstrated the prevalence of prolonged-QTc syndrome in COPD patients. Armsrtong et al examined ambulatory patients free of cardiovascular disease who had undergone spirometry and pulmonary function tests. The data revealed that COPD patients had longer QT segments compared with no-COPD patients and that long QT was associated with severity of disease only in patients with severe COPD (FEV1 <50%).25
Moreover, in previous studies11,12,24–26 QTc abnormalities were found to be a negative prognostic factor for long-term mortality among ambulatory COPD patients. Zulli et al examined 246 COPD patients without any significant comorbidities, and concluded that prolonged QTc interval was a predictor of long-term mortality in COPD patients, independently of respiratory illness.12 These results illustrate the need to monitor data regarding QT segments of COPD patients during hospitalization.
In our study, an attempt was made to find a correlation between the etiology of prolonged QTc and electrolyte levels in COPD. However, our findings demonstrated that QTc prolongation was independent of electrolyte disorders. In previous reports, high prevalence of hypomagnesemia was reported in COPD patients, correlating with poor outcomes in chronic asthmatic and COPD patients.26–28 In our study, no connection was found between magnesium levels and prolonged QTc or secretion of urinary magnesium. Nonetheless, the measurement of serum magnesium can be falsely normal, despite low total-body magnesium levels. It has already been shown that intracellular levels of electrolytes, such as magnesium, are poorly represented in serum and that clinical significance is correlated more with intracellular measurements.29 There are individuals, particularly those with a subtle chronic magnesium deficiency, whose serum-magnesium levels are within the reference range, but still may have a deficit in total-body magnesium.29 For example, Emelyanov et al evaluated magnesium levels in airway hyperreactivity in asthma patients and found low levels only intracellularly and not in the serum.30
In our study there were higher PTH levels in patients with prolonged QTc, which might represent a change in total-body calcium. Intracellular hypocalcemia, which is not reflected in blood-level measurements, might induce cardiac repolarization abnormalities that will present as prolonged QTc. The prevalence of chronic kidney disease was also higher in the group with prolonged QTc, an observation that is also related to electrolyte disturbances and secondary hyperparathyroidism.31 These data might lead to the assumption that the intracellular electrolyte disturbances found in COPD patients might contribute to prolonged QTc.32 Previous studies has demonstrated a change in PTH in COPD patients. Park et al demonstrated increased PTH in ambulatory patients with severe COPD (GOLD 4 criteria), with no correlation with vitamin D levels.33 Dimai et al found bone loss in COPD patients related to hypercapnia. In these patients calcium and phosphorus levels were not different, but PTH was higher in COPD patients than controls. They concluded that higher PTH levels can be secondary to higher bone turnover in these patiens.34
However, due to the lack of published evidence to support the observation that cytosolic electrolyte disturbance is involved in the prolongation of QTc, we hypothesized that other mechanisms might contribute to this observation. Cardiovascular autonomic neuropathy has been found to be common among COPD patients. Chhabra et al measured heart-rate response followed by autonomic stimulation, and discovered a lack of response to the stimuli, mainly in moderate–severe COPD patients.35 Rasheedy et al examined elderly outpatients with COPD and measured heart-rate and blood-pressure response to different stimuli. It was found that among patients with cardiac autonomic dysfunction, a higher baseline heart rate and higher CO2 levels represented severity of the disease.36 The data from our study revealed higher bicarbonate levels in the prolonged-QTc group, which might represent the chronic compensation of CO2 retention found in severe COPD patients. Therefore, prolonged QTc could be related to a chronic response to respiratory acidosis.37
Strengths and limitations
The study was prospective and included all COPD patients eligible to participate in the study in the time period. Patients with known cardiac diseases were included, consistently with internal department patients with multiple medical problems. The initial assumption for the study estimated that QTc interval would correlate with electrolyte changes. After initial statistical evaluation, it was clear that serum magnesium level is not related to prolonged QTc. The sample of the study was smaller than expected in the study period. This study did not reveal electrolyte changes as the cause of QTc prolongation. A study with a larger sample of patients might reveal small changes that could not be estimated here. These changes are not necessarily clinically significant. Intracellular electrolyte levels were not routinely measured.
Conclusion
Our findings demonstrated that QTc prolongation in hospitalized COPD patients was not correlated to electrolyte levels, comorbidities, or relevant medications. A higher rate of mortality was found in the prolonged-QTc group than the normal-QTc group. Therefore, it is suggested that prolonged QTc could serve as a negative prognostic factor for mortality during hospitalization in COPD patients. Nevertheless, in the latest edition of the GOLD guidelines, released in 2018, there was no recommendation to include QTc as part of the routine assessment of COPD patients.38 Therefore, we suggest adding QTc measurements as routine follow-up, regardless of electrolyte levels, and to administer appropriate care, including avoidance of medical therapy that causes QTc prolongation. Further investigations are needed concerning intracellular electrolyte levels and their relationship to QTc prolongation, as well as the correlation between prolonged QTc and mortality in hospitalized COPD patients.
Abbreviation list
COPD, chronic obstructive pulmonary disease; IMD, internal medicine department; ECG, electrocardiography; AE-COPD, acute exacerbation of COPD; PPIs, proton-pump inhibitors; GOLD, Global Initiative for Chronic Obstructive Lung Disease; CO2, carbon dioxide; PTH, parathyroid hormone; BPAP, bilevel positive airway pressure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aaron SD. Management and prevention of exacerbations of COPD. BMJ. 2014;349:g5237. doi:10.1136/bmj.g5237
2. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
3. Woods JA, Wheeler JS, Finch CK, Pinner NA. Corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:421–430. doi:10.2147/COPD.S51012
4. Taylor SP, Sellers E, Taylor BT. Azithromycin for the prevention of COPD exacerbations: the good, bad, and ugly. Am J Med. 2015;128(12):1362e1361–1366. doi:10.1016/j.amjmed.2015.07.032
5. Liamis G, Milionis HJ, Elisaf M. A review of drug-induced hypocalcemia. J Bone Miner Metab. 2009;27(6):635–642. doi:10.1007/s00774-009-0119-x
6. Zaloga GP, Chernow B, Pock A, Wood B, Zaritsky A, Zucker A. Hypomagnesemia is a common complication of aminoglycoside therapy. Surg Gynecol Obstet. 1984;158(6):561–565.
7. Rolla G, Bucca C, Bugiani M, Oliva A, Branciforte L. Hypomagnesemia in chronic obstructive lung disease: effect of therapy. Magnes Trace Elem. 1990;9(3):132–136.
8. Ben Salem C, Hmouda H, Bouraoui K. Drug-induced hypokalaemia. Curr Drug Saf. 2009;4(1):55–61.
9. Keller GA, Alvarez PA, Ponte ML, et al. Drug-induced QTc interval prolongation: a multicenter study to detect drugs and clinical factors involved in every day practice. Curr Drug Saf. 2016;11(1):86–98.
10. Sin DD, Man SF. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality. Proc Am Thorac Soc. 2005;2(1):8–11. doi:10.1513/pats.200404-032MS
11. Sievi NA, Clarenbach CF, Camen G, Rossi VA, van Gestel AJ, Kohler M. High prevalence of altered cardiac repolarization in patients with COPD. BMC Pulm Med. 2014;14:55. doi:10.1186/1471-2466-14-55
12. Zulli R, Donati P, Nicosia F, et al. Increased QT dispersion: a negative prognostic finding in chronic obstructive pulmonary disease. Intern Emerg Med. 2006;1(4):279–286.
13. Kaye AD, Volpi-Abadie J, Bensler JM, Kaye AM, Diaz JH. QT interval abnormalities: risk factors and perioperative management in long QT syndromes and Torsades de Pointes. J Anesth. 2013;27(4):575–587. doi:10.1007/s00540-013-1564-1
14. Martin KJ, Gonzalez EA, Slatopolsky E. Clinical consequences and management of hypomagnesemia. J Am Soc Nephrol. 2009;20(11):2291–2295. doi:10.1681/ASN.2007111194
15. Blaine J, Chonchol M, Levi M. Renal control of calcium, phosphate, and magnesium homeostasis. Clin J Am Soc Nephrol. 2015;10(7):1257–1272. doi:10.2215/CJN.09750913
16. Cheungpasitporn W, Thongprayoon C, Qian Q. Dysmagnesemia in hospitalized patients: prevalence and prognostic importance. Mayo Clin Proc. 2015;90(8):1001–1010. doi:10.1016/j.mayocp.2015.04.023
17. Agus ZS. Mechanisms and causes of hypomagnesemia. Curr Opin Nephrol Hypertens. 2016;25(4):301–307. doi:10.1097/MNH.0000000000000238
18. Gourgoulianis KI, Chatziparasidis G, Chatziefthimiou A, Molyvdas PA. Magnesium as a relaxing factor of airway smooth muscles. J Aerosol Med. 2001;14(3):301–307. doi:10.1089/089426801316970259
19. Bhatt SP, Khandelwal P, Nanda S, Stoltzfus JC, Fioravanti GT. Serum magnesium is an independent predictor of frequent readmissions due to acute exacerbation of chronic obstructive pulmonary disease. Respir Med. 2008;102(7):999–1003. doi:10.1016/j.rmed.2008.02.010
20. Wile D. Diuretics: a review. Ann Clin Biochem. 2012;49(Pt 5):419–431. doi:10.1258/acb.2011.011281
21. Park CH, Kim EH, Roh YH, Kim HY, Lee SK. The association between the use of proton pump inhibitors and the risk of hypomagnesemia: a systematic review and meta-analysis. PLoS One. 2014;9(11):e112558. doi:10.1371/journal.pone.0112558
22. Kallergis EM, Goudis CA, Simantirakis EN, Kochiadakis GE, Vardas PE. Mechanisms, risk factors, and management of acquired long QT syndrome: a comprehensive review. Sci World J. 2012;2012:212178. doi:10.1100/2012/212178
23. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
24. Rautaharju PM, Surawicz B, Gettes LS, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009;53(11):982–991. doi:10.1016/j.jacc.2008.12.014
25. Armstrong HF, Lovasi GS, Soliman EZ, et al. Lung function, percent emphysema, and QT duration: the Multi-Ethnic Study of Atherosclerosis (MESA) lung study. Respir Med. 2017;123:1–7. doi:10.1016/j.rmed.2016.12.003
26. Aziz HS, Blamoun AI, Shubair MK, Ismail MM, DeBari VA, Khan MA. Serum magnesium levels and acute exacerbation of chronic obstructive pulmonary disease: a retrospective study. Ann Clin Lab Sci. 2005;35(4):423–427.
27. Gumus A, Haziroglu M, Gunes Y. Association of serum magnesium levels with frequency of acute exacerbations in chronic obstructive pulmonary disease: a prospective study. Pulm Med. 2014;2014:329476. doi:10.1155/2014/329476
28. Alamoudi OS. Hypomagnesaemia in chronic, stable asthmatics: prevalence, correlation with severity and hospitalization. Eur Respir J. 2000;16(3):427–431.
29. Jahnen-Dechent W, Ketteler M. Magnesium basics. Clin Kidney J. 2012;5(Suppl 1):i3–i14. doi:10.1093/ckj/sfs139
30. Emelyanov A, Fedoseev G, Barnes PJ. Reduced intracellular magnesium concentrations in asthmatic patients. Eur Respir J. 1999;13(1):38–40.
31. Hanley DA, Sherwood LM. Secondary hyperparathyroidism in chronic renal failure. Pathophysiology and treatment. Med Clin North Am. 1978;62(6):1319–1339.
32. Larbig R, Reda S, Paar V, et al. Through modulation of cardiac Ca(2+) handling, UCP2 affects cardiac electrophysiology and influences the susceptibility for Ca(2+) -mediated arrhythmias. Exp Physiol. 2017;102(6):650–662. doi:10.1113/EP086209
33. Park JH, Park HK, Jung H, Lee SS, Koo HK. Parathyroid hormone as a novel biomarker for chronic obstructive pulmonary disease: Korean national health and nutrition examination survey. PLoS One. 2015;10(9):e0138482. doi:10.1371/journal.pone.0120491
34. Dimai HP, Domej W, Leb G, Lau KH. Bone loss in patients with untreated chronic obstructive pulmonary disease is mediated by an increase in bone resorption associated with hypercapnia. J Bone Miner Res. 2001;16(11):2132–2141. doi:10.1359/jbmr.2001.16.11.2132
35. Chhabra SK, De S. Cardiovascular autonomic neuropathy in chronic obstructive pulmonary disease. Respir Med. 2005;99(1):126–133.
36. Rasheedy D, Taha HM. Cardiac autonomic neuropathy: the hidden cardiovascular comorbidity in elderly patients with chronic obstructive pulmonary disease attending primary care settings. Geriatr Gerontol Int. 2016;16(3):329–335. doi:10.1111/ggi.12473
37. Martinu T, Menzies D, Dial S. Re-evaluation of acid-base prediction rules in patients with chronic respiratory acidosis. Can Respir J. 2003;10(6):311–315. doi:10.1155/2003/818404
38. Burkes RM, Donohue JF. An update on the global initiative for chronic obstructive lung disease 2017 guidelines with a focus on classification and management of stable COPD. Respir Care. 2018;63(6):749–758. doi:10.4187/respcare.06174
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.