")
Back to Journals » Patient Preference and Adherence » Volume 12
Living with cystic fibrosis – a qualitative study of a life coaching intervention
Authors Knudsen KB , Boisen KA , Katzenstein TL , Mortensen LH , Pressler T, Skov M, Jarden M
Received 8 December 2017
Accepted for publication 23 February 2018
Published 19 April 2018 Volume 2018:12 Pages 585—594
DOI https://doi.org/10.2147/PPA.S159306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Karin Bæk Knudsen,1 Kirsten Arntz Boisen,2 Terese Lea Katzenstein,1,3 Laust Hvas Mortensen,4 Tacjana Pressler,5 Marianne Skov,5 Mary Jarden1,4
1Department of Infectious Diseases, Copenhagen University Hospital, Copenhagen, Denmark; 2Department of Pediatric and Adolescent Medicine, Center of Adolescent Medicine, Copenhagen University Hospital, Copenhagen, Denmark; 3Department of Clinical Medicine, Faculty of Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 4Department of Public Health, University of Copenhagen, Copenhagen, Denmark; 5Department of Pediatric and Adolescent Medicine, Cystic Fibrosis Center Copenhagen, Copenhagen University Hospital, Copenhagen, Denmark
Background: Cystic fibrosis (CF) is a chronic, life-shortening disease with a significant treatment burden. To support young adults with CF in their everyday life, we previously conducted a life coaching feasibility trial (published elsewhere). The aim of the current study was to explore how life coaching was experienced by study participants within the context of their lives with CF.
Methods: A qualitative study using individual interviews. Respondents (n=14) were recruited from the intervention group after participation in life coaching. Data were analyzed from a phenomenologic-hermeneutical perspective, inspired by Ricoeur’s theory.
Findings: Periodic exacerbations of CF led to worry about disease progression, and interrupted the respondents’ ability to fulfill daily life roles satisfactory. The treatment burden demanded self-discipline and this was sometimes at the expense of social life or career. The young adults rarely spoke to others about their situation; therefore, they valued opening up to a professional coach about life and concerns. We identified three themes: 1) living an unpredictable life; 2) the conflict between freedom and the constraints of illness; and 3) the value of telling one’s story. In relation to all three themes, coaching promoted reflection over life situations, reframed thoughts, and facilitated finding new ways to manage everyday life.
Conclusion: Life coaching is an intervention that is valued for those who feel challenged by their CF disease. Coaching programs should be designed to include the participants, when they feel a need for coaching and are open for change. Screening parameters to identify persons who will most likely benefit from life coaching are needed.
Keywords: phenomenological-hermeneutic methods, adherence, self-determination theory, dialogue, young adults, chronic diseases
Introduction
Cystic fibrosis (CF) is a genetic, chronic, and life-shortening multisystemic disease associated with numerous health problems, the most significant being recurring or chronic lung infections, gastrointestinal problems, and CF-related diabetes.1 Enhanced treatment options have improved physical health among patients with CF. Life expectancy is steadily rising and is estimated as >50 years for newborns from 2010.2 Most young adults with CF live independently, taking on responsibilities with education, careers, and family.3 However, the treatment burden is substantial and people with CF spend on average 2 hours per day with treatment regimen activities.4 Several studies have found that people with CF have low adherence to treatment and an increased prevalence of anxiety and depression.3,5,6 Psychological health problems are burdensome in themselves; besides, they may negatively affect quality of life, and furthermore reduce adherence to treatment.3,7 Low adherence to the CF medical regimen has been shown to increase risk of pulmonary exacerbations.8 Qualitative studies have explored individual life experiences with CF to give a more comprehensive understanding of the challenges that patients face while living with CF.9–14 People with CF wish to engage in the same life activities as their healthy peers, including social activities, education, and careers. However, participation in everyday activities demands additional effort while mastering the complexity of the CF disease.13 Many adolescents and young adults choose not to disclose their disease, which may lead to strained social relationships and an unhealthy lifestyle.11 The lifelong need for treatment is challenging; competing priorities between social life and adherence to medical care may result in nonadherence,12,14 which subsequently may trigger feelings of guilt.10
New approaches (eg, motivational interviewing, psychosocial support, cognitive-behavioral therapy) have been recommended to support people with CF in coping with their complex health and life situation.12,15–17 Current evidence for psychological and behavioral interventions among patients with CF is insufficient, but according to a recent Cochrane review, cognitive-behavioral therapy has shown promising results.18 Health coaching has demonstrated positive effects on physiologic, behavioral, and psychological conditions and the management of chronic diseases,19 but due to scarcity of studies, more research is needed. Life coaching is an approach that has the potential to empower individuals to identify and successfully pursue personal goals.20 Life coaching builds on the skills and capabilities of individuals, as well as allowing for their optimal utilization.21 At the CF clinic at the Department of Infectious Diseases, Copenhagen University Hospital, Rigshospitalet, we found a life coaching intervention among young adults aged 18–30 with CF to be feasible.22
The aim of this qualitative study was to explore the experiences of young adults with CF participating in a life coaching intervention. Further, the objective of this study was to gain a greater understanding of the relevancy and usefulness of life coaching within the context of participants’ social and emotional well-being.
Methods
Settings and participants
The present qualitative study was part of a randomized controlled feasibility trial “Coach to Cope” (ID: NCT02110914), conducted at the CF clinic at the Department of Infectious Diseases at Copenhagen University Hospital, Rigshospitalet. Participants aged 18–30 years with CF (n=38), all fluent in Danish and without cognitive impairments, were randomized to either an intervention group receiving life coaching, or a control group receiving standard care. The sample was representative for the group of young adults with CF; however, there was an overrepresentation of females in the study sample compared to the entire CF population (71% versus 50%). Participants, who were allocated to the intervention group (n=18), were recruited for the qualitative study by the co-author investigator (KAB) or the coach after the final life coaching session. The intervention group was asked to participate in an interview regarding their experience with the life coaching intervention in the context of their life with CF. Our recruitment strategy and criterion for selecting participants were to collect a wide range of experiences from CF participants who had completed from a few to the maximum number of sessions offered. The interviews were carried out either in person at the department or by telephone and lasted on average 25 minutes (range 10–55 minutes). Of the 18 participants from the intervention group, 16 were approached and 14 agreed to participate. Two were not approached; one was unavailable because of family circumstances, and one had passed away. The remaining two, who chose not to participate, were too busy or abroad. Seven respondents were interviewed in person, and seven were interviewed by telephone. Characteristics of the respondents are shown in Table 1.
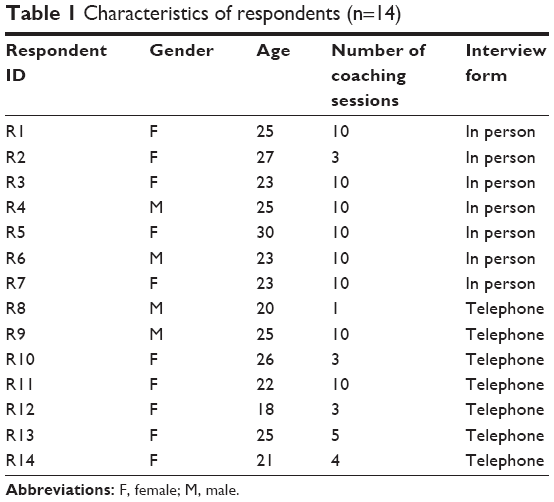 | Table 1 Characteristics of respondents (n=14) |
Life coaching intervention
The participants in the life coaching intervention were offered up to 10 individual face-to-face or telephone coaching sessions.22 The average length of the coaching sessions was ~1 hour for face-to-face coaching and half an hour for telephone coaching. All coaching sessions were delivered by the principal investigator and nurse specialist (KBK) experienced with CF and certified by an Accredited Coaching Training Program, which included 125 student contact hours, 10 hours of mentor coaching, and a performance evaluation.23 The life coaching intervention was underpinned by the co-active coaching model,21 and the specific objectives in the coaching sessions were decided upon by the participants in collaboration with the coach. The coaching method was based on the principles of client-centeredness, collaboration and client preferences, reflective dialogue, empathy and use of positive language, and promotion of capacity and self-determination.21,24
Interview procedures
A semistructured interview guide with open-ended questions was developed and utilized during the individual interviews (Table 2). The questions focused on how they experienced the life coaching intervention in the context of life with CF. The interviews were conducted in Danish by the co-author investigator (KAB) who was not involved in the life coaching intervention. The interviews took place in an undisturbed room at the Center of Adolescent Medicine, Rigshospitalet or by telephone. The interviews were digitally recorded and transcribed verbatim.
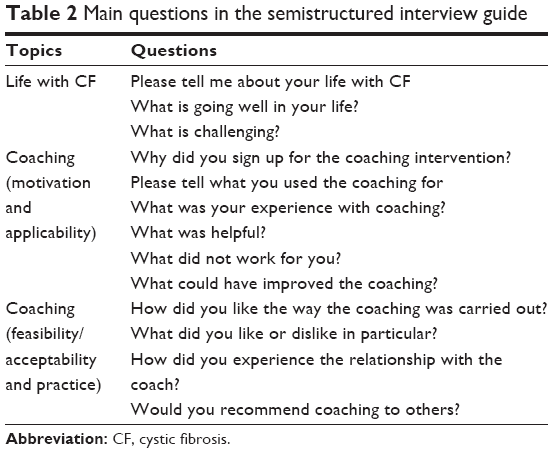 | Table 2 Main questions in the semistructured interview guide |
Methodology and data analysis
The analysis was carried out based on Lindseth and Norberg’s25 modification of the French philosopher Paul Ricoeur’s phenomenologic-hermeneutical method. Ricoeur states that to truly understand the essence of a phenomenon, the essential meaning must be studied and revealed in the interpretation of a text. In the interpretation, there is an interaction between understanding and explanation, and in that process a new way of seeing the world is disclosed.26
The analysis consisted of three steps: a naïve reading, a structural analysis, and a critical analysis. The naïve reading was the first reading of the transcribed text as a whole to achieve an immediate understanding. The naïve understanding was formulated as a short text, which provided a foundation for further analyses. The structural analysis was carried out as a thematic structural analysis, breaking the text into meaning units, which were further condensed into themes. The themes were reflected upon in relation to the naïve reading. The thematic analysis was performed using NVivo data analysis Software; QSR International Pty Ltd. Version 11, 2015. Credibility in the analysis process was strengthened by engaging three researchers (KBK, KAB, and MJ). The researchers acknowledged their professional and scientific roles, attitudes, and biases in the process. Coding was undertaken individually and the themes were discussed until consensus was reached. The final part of the structural analysis was the comprehensive understanding, where themes were summarized in relation to the research aim. The last step, critical analysis, was carried out based on literature and theory.
Ethical consideration
The study was reviewed by the regional ethics committee of the Capital Region of Denmark and according to Danish regulations, the committee exempted this project from formal evaluation because it did not involve human biologic material (H-2-2013-FSP01). The study was registered at the Danish Data Protection Agency (j.nr. 30-0918) and at ClinicalTrials.gov (ID: NCT02110914). Written informed consent was obtained. All participants were informed that their participation in the current substudy was voluntary, and assured of anonymity and confidentiality.
Findings
Naive reading
Life coaching was described as a positive and recommendable experience. The life coach was a health professional that had an open-minded and accepting approach. Conversations about life and disease concerns were constructive. Some felt that life coaching was useful; others did not feel that coaching was relevant for them in their present situation. CF was experienced as an unstable disease, with a continuous ebb and flow of unknown medical events affecting daily life. In acute phases or worsening of CF, the demands of the disease increased, while everyday life was constricted to manage the disease properly. The threat of chronic lung infections, declining lung function, and early death was lurking. But for the most part, the informants felt fortunate that they were still physically well, independent, and alive. Striving for being independent and living a “normal life” was a mindset, which was characteristic for all participants. However, a “normal life” for a person with CF required integrating a time-consuming treatment regimen, which often felt constricted. Life coaching facilitated new ways of talking about and coping with everyday life challenges. Life coaching was preferred, when the disease or life in general was more challenging, allowing for relief of stress and worry. However, as soon as life was going well, life coaching was given a low priority.
Structural analysis
Three overarching themes were identified from the structural analysis: 1) living an unpredictable life; 2) the conflict between freedom and the constraints of illness; and 3) the value of telling one’s story.
Living an unpredictable life
Even though CF is a multisystemic disease, participants generally described feeling physically well, and being able to live a life comparable to their healthy peers. They expressed that they felt fortunate in their present situation, indicating that their health was better than expected, yet with a concern that it may not continue to last. Challenges related to life with CF were described as more emotional and social than physical.
CF in itself doesn’t restrict me much; it restricts me more mentally than physically. But I’m also quite lucky, I’m still quite well. [R3]
Some described life as a “rollercoaster”, expressing how they experienced fluctuations of their disease. They expressed that their lung function was for the most part good. However, respondents described periodic declines in lung function because of pulmonary exacerbations, with increasing difficulty in returning to the same functional level afterward. They were apprehensive about how their health would evolve, and feared decline in lung function, loss of independence, and “ending up” on the transplant waiting list. Some were concerned about whether to become a parent or if their job opportunities might be compromised compared to healthy peers. Their thoughts about the future varied. Some distanced themselves and avoided thinking too much about goals and plans for the future, while others were energetic and hoped to start a family while it was still possible:
[…] I don’t think that I consciously avoid thinking about the future, I just don’t do it […]. [R3]
I have a girlfriend and we are getting married now, and we have started the fertility process. [R6]
An accumulation of worries was stressful for the respondents, and, therefore, it was helpful to have the opportunity via coaching to reflect, articulate, and air their concerns and fears with someone knowledgeable about CF, yet neutral and uninvolved in their everyday CF management. Most importantly, it was beneficial for the respondents to work with someone they trusted.
But I discovered fairly quickly that coaching could give me something, especially give me structure in my life, and help me to put things in order, so that it wasn’t a big mess, where I at the same time should manage to find time for my disease. The coaching was capable of that. I wasn’t aware of the chaos I was in, before we started. It [my life] was just a big mess, which I couldn’t handle on my own right then. [R5]
The conflict between freedom and the constraints of illness
Living with CF demands great responsibility and self-discipline. A significant part of daily life is taking medication; some reported that they managed to make it a routine, while others struggled to schedule it into their daily schedules. They were aware of having to make many decisions throughout the day, and some of the decisions were made in favor of the needs related to their disease (eg, taking medication as prescribed), while others chose to live like their healthy peers. In general, respondents feared that their physical health only would get worse in the future, and therefore they embraced life, which sometimes created a conflict with spending time managing their treatment. Taking stock of their everyday situation on occasion made them to prioritize friends or work higher than their treatment regimen, disclosing that they were often intentionally nonadherent:
I never forget to take my medication, I opt out my medication. If I don’t take it, it’s because I have consciously chosen not to take it today. [R6]
Some had come to terms with their decisions, and described that they had decided to live with their disease, but not a life of illness. Others never really felt comfortable with their choices and when they followed desires that conflicted with recommended health behavior, their decisions made them feel guilty, especially if they experienced an exacerbation of CF. Guilt was a central emotional burden found among the interviewed young adults living with CF, strongly connected with feeling personally responsible for their health. In this context, responsibility meant following a strict treatment regimen, exercising, sleeping well, eating healthy, and avoiding too much alcohol. The strict treatment regimen in particular conflicted with their need to feel free. They reported discontent with the same daily treatment routines, and as a result, they dropped some of their treatment routines to live a life similar to their healthy peers:
Bad conscience is nagging me, there is always more you could do. But I have made a choice, I don’t know if it is the right one, but I have chosen that it (the disease) should not restrict me, meaning that if I must choose between taking my treatment or doing something with my friends, then I will without doubt choose my friends. [R3]
In general, young people with CF were striving to be on an equal level to their healthy peers. They fought against being categorized as ill, and wanted to be able to manage their own life.
When I moved away from home, I had a new boyfriend and a new apartment, and I was just living my life and that happened completely at the expense of my medication. [R3]
The respondents felt that the treatment burden made it highly difficult to adhere to the treatment plan with consistency. The treatment regimen was followed to the letter for periods of time, but became so demanding that a point of exhaustion or frustration was reached because they did not feel that their efforts were fruitful, and, therefore, they gave up.
You can do your exercises, you can take your medication and then it [the lung function] just goes down and you think: What the hell do you want from me? Forget it, I don’t care anymore, it can go to blazes for all I care. [R2]
Life coaching, which is based on building a trusting and respectful relationship that facilitates reflective dialogue with the participant as a coactive equal partner, enabled the respondents to open up and be honest about the struggles they had faced with adhering to daily treatments. In the life coaching process, some found it useful to set milestones together with the coach, and wanted to be held accountable. For others, the answer was to reframe their thoughts about the treatment regimen and change daily routines so that treatment was more easily and naturally integrated.
The disease gave the informants resilience, which was mentioned as the only positive aspect of having CF. The downside was that they sometimes felt the burden of the disease, making it too difficult to be strong all the time. Because life coaching conversations focused on autonomy or individual values and on how to prioritize them, it helped the respondents to set limits in relation to work tasks or friends; it also helped them in accepting their situation.
Taking care of my diabetes and my cystic fibrosis comes first, because if it doesn’t I can’t function […]. I don’t have the same strength, so the priorities, where you learn to say “no” and “stop” has helped a lot, and putting things into words […] You have a lot on your mind every day, and it helped, just to say the most important things in a few words, yes. [R1]
We did it more times during the coaching, and actually there came more priorities on places, where it actually was important; not what I just wanted, but what I wished. You can want to do a lot of things, but not wish it deep inside. [R7]
The value of telling one’s story
The respondents valued talking to the coach about their life. Having contact with other young people with CF was sparse or nonexistent because of the risk of cross-infections, and many rarely disclosed CF life issues with their healthy peers or at work.
It is very seldom, that I talk to other people about it (CF), that is, except for my family. [R2]
Most often, respondents were selective with what information they shared and with whom, and often needed to get to know people before they told them about their CF disease. They wanted to protect themselves from being stigmatized or discriminated against, and/or they simply wanted to avoid pity or questions.
Nowadays I can tell a little bit about it, but I don’t feel like doing it too much, I always have a kind of fear, since the day I told one of my first boyfriends about it and he looked it up on Google and got all these worst-case scenarios, right? [R3]
Close, trustful, supportive relationships were important for them, especially with people who were understanding and tolerant toward the challenges respondents had to deal with. In the life coaching intervention, the participants were encouraged to verbalize thoughts and worries about their lives. Some of them needed to build a trusting relationship before they opened up and shared their concerns. It was important that they felt trust in the coach, and they generally preferred to meet the coach in person in order to read the reactions of the coach when they told their story. Opening up was linked to vulnerability and courage, especially for the participants who normally were cautious with sharing their concerns and emotions with others.
In the beginning I was a bit evasive because I didn’t know the coach very well and I didn’t feel like spreading my weaknesses or anything, but after a couple of times everything poured out. Because I have to know a person a bit more before I tell all sorts of stuff. [R4]
The respondents found that there was a good match between the type and severity of their concerns, and the support they received from life coaching. They expressed that their problems were not so severe that they needed a psychologist, and they perceived the more action-oriented life coaching as a relevant solution.
A psychologist sounds so extreme, but with coaching I think I just get better at doing the things I do every day. [R7]
A psychologist […], it’s more like, well, you are sick or a bit crazy. [R2]
However, opening up was described as hard work because the reflective dialogues made them aware of values, convictions, or bad habits, any of which could affect their thoughts or emotions. Therefore, the life coaching method triggered ambivalence among some of the respondents; they found it helpful but also a bit exhausting. Some found it tempting to stop coaching when they were in control of their situation once again.
Sometimes when I looked at my calendar, I thought: “Do I really have to go to coaching today, I can hardly cope with that.” But nevertheless, I did it and it turned out to be quite good. [R4]
The respondents valued being seen and met as the person they are, and the ability to verbalize their thoughts, which helped them to view their life from a new perspective. The dialogue with the coach, which always began by clarifying what the participants preferred to talk about, facilitated a way for the participants to reflect upon how they normally thought or behaved.
An eye opener, I think […] yes, I’m not putting up with other people’s opinion anymore and I have learned to say “No” […]. It was a great, great help to get; also that we could talk about how I felt and I could allow myself to talk about everything, that was quite fantastic. [R1]
I went through a personal development and got new ways of thinking. Mentally, it was quite well. [R14]
The respondents, who found coaching helpful, pointed out that certain aspects of coaching were important for a successful and meaningful outcome. First, there needed to be an issue or problem identified which they were both willing and ready to work with, especially ready to make a change. Second, there should be a willingness to open up for conversations about their lives, receive feedback, and be personally involved. Finally, there should be a good match between the coach and the coachee, where a trusting relationship was able to develop. To accommodate these points, some suggested incorporating screening of needs before coaching. They also emphasized that meeting face-to-face was important to build a trustful relationship, but telephone coaching was a nice alternative later on after rapport had been established. The respondents, who did not find life coaching useful, made it clear that one approach does not fit all. Some disliked the method, and found life coaching to be too vague or slow, and would have preferred a more straightforward approach; at the same time they were all very positive about the initiative and were aware that an active cooperation of both parties was needed if life coaching was to be successful.
Perhaps it was unnecessary, maybe I wasn’t the right one. I didn’t really get anything I could work with, because where I am in my life right now, I’m resolved with many things, I do what I have to do and I know what is going on. [R6]
Even though I stopped, it wasn’t negative, only positive. I think it was fine to give it a try and if I had had some issues, I think it would have been rewarding, or more rewarding. I would definitely recommend it to others, but I will not go home and make a giant advertising for it [laughing]. [R2]
The coaching started at a very turbulent time in my life […] The situation I was in when it [the coaching] started and the entire period, – it was just so good for me that she [the coach] was there. [R5]
Comprehensive understanding
The respondents perceived coaching to be helpful when they went through demanding phases of their disease or difficult times in their life. They valued the possibility to air their concerns, reframe their thoughts, and get support for the chaotic state they were in. Living with an unpredictable disease influenced the respondents’ everyday life, and led them to worry about the future. There was a preference to live in the moment, and they experienced difficulty in making choices between taking good care of their health and living a life similar to healthy peers. They took responsibility for their actions, but often the choices they made resulted in guilt for not focusing on their health and treatment. Thus, an unpredictable disease, concerns about the future, and feelings of guilt made life with CF a mental and emotional burden. Life coaching was a process that enabled some young adults with CF to come up with what they needed to change and to take more control over their lives.
Critical interpretation and discussion
We aimed at exploring the world of young adults with CF, and gaining a greater understanding of how they experienced life coaching in the context of CF disease. The comprehensive understanding revealed that there was an interactional play of both promotional and inhibitory factors present in the readiness to engage in a life coaching intervention, including decision making regarding which problems to work with, readiness to work with a challenge that is complex, and taking action to manage the problem. It has been suggested that self-determination theory (SDT) presents a theoretical framework for coaching.27 In light of this, we will critically interpret our findings applying the SDT.28 SDT is a theory of human motivation, based on the underlying idea that people are born with three fundamental psychological needs: autonomy, competence, and relatedness. Autonomy refers to the freedom to make independent choices. Competence involves an inherent desire to contribute to community and successfully manage or influence the outcome of one’s life. Finally, relatedness includes belonging with peers, family, and/or community and a need to feel connected to and valued by others. According to SDT, fulfillment of these needs will enhance motivation, whereas motivation will be diminished when these needs are not met successfully. Furthermore, motivation is defined as intrinsic and extrinsic motivation; intrinsic motivation refers to activities undertaken to satisfy a person’s core values or interests, while extrinsic motivation refers to a motivation to gain external reinforcement, for example, the desire to please others or avoid punishment.28
Autonomy
The young adults with CF in our study clearly stated that it was important to them to make their own autonomous decisions, even when their decisions conflicted with the recommended guidelines for optimizing their health. They followed their own quality-of-life values and prioritized their job or friends higher than their treatment regimen if that seemed like the most valuable decision. Sometimes, respondents prioritized differently; they put their ambitions or friendships on hold and prioritized their health highest. Heaton et al29 described that most young adults with chronic diseases perceived being in medical control and having autonomy as independent and potentially conflicting goals. To combat this, they adopted the strategy of being partially adherent to the medical regimen in order to balance conflicting goals. Life coaching facilitates autonomy. Coachees are considered naturally creative and resourceful, and strategies to obtain desired outcomes are based on the coachee’s unique needs.21 A part of life coaching is evoking the coachee’s discovery of personal values, and help them to base their decisions on these values.21 Thus, in life coaching, the coachee may have the goal of being in control of the treatment regimen, but the goal may also include achieving a satisfying balance in life, and/or to make peace with their decisions instead of feeling guilty.
Competence
Our findings showed that our respondents described themselves as physically well and that they lived lives similar to healthy peers. Despite their time-consuming treatments, they were employed or enrolled in college or university, and they strived to be on equal footing with their peers. They wanted to influence or master their environment, to live independent lives, to contribute to their communities, and to manage and control their disease. Similar findings have been described in other studies.10,29 However, the unpredictable nature of CF challenged these young adults in achieving control of the disease and feeling competent. They experienced recurrent exacerbations even during periods of high treatment adherence. When basic needs like competence are being thwarted, this may lead to diminished motivation,28 explaining low rates of adherence. Furthermore, successfully managing school or jobs with a time-consuming treatment regimen led to the development of tight schedules. Some of the young adults felt drained of their resources and experienced stress as a result, which is in line with the findings of Gjengedal et al.13 Life coaching can be used to enhance competence through developing achievable goals, and brainstorming and choosing alternative appealing options. Furthermore, being supported and believed in by the coach and being held accountable to a self-chosen action can help the process.21,30 The young adults in our study valued being seen and met as the persons they are, getting support to prioritize daily tasks and to structure their schedules, setting milestones, and being held accountable for their actions.
Relatedness
During the interviews the respondents repeatedly talked normality. Despite their extraordinary life conditions, they expressed that they lived normal lives. Human beings have a psychological need to belong and will strive to avoid social exclusion and rejection. Therefore, identifying with peers through similar behavior is an easier strategy to become part of a group.31,32 Even though it seemed that the young adults with CF succeeded in satisfying their need for relationships, they still feared stigmatization, and many of them were cautious about sharing their inner concerns with others. In coaching, the coachees were invited to a relationship built on trust and openness; thus, coaching provided a safe place in which the coachees could work with the important issues of their lives.21
Life coaching and SDT
According to SDT, individuals are driven by an inner motivation to achieve a healthy balance between autonomy, competence, and relatedness. Life coaching is an approach that supports autonomy, for example, by placing the coachee in the center of the decision-making process. The coachee is free to choose what to accomplish and, moreover, the choice will be respected.27 Life coaching supports competence with the core assumption that people are resourceful and capable and the coachees are encouraged to utilize the capacities they have. Furthermore, life coaching supports relatedness by the development of a trusting relationship. Our respondents appreciated verbalizing their concerns and being listened to. According to Bohart and Tallman,33,34 people actively make changes when they are ready, but the change process is best supported when a person feels understood, accepted, and listened to. A systematic review conducted by Ammentorp et al in 201335 showed that the term “life coaching” was rarely used in coaching intervention studies. Due to the limited number (n=5) of studies, the effect of life coaching on health outcomes is not known. However, it was pointed out that the alternative way of communicating and meeting patients during life coaching sessions seemed to be beneficial for some patients, especially disadvantaged patients. Our respondents found that coaching was most helpful during stressful phases of life and they emphasized the importance of having an issue or concern to be discussed that they were ready to address, and that the relationship with the coach should be one of trust. Mutual trust, and feeling respected and understood have been highlighted as core elements in the interrelationship in a therapeutic alliance.36 The respondents valued the possibility to air their concerns, reframe their thoughts, and receive support to prevent and restructure potential chaos so that they may better handle future challenges in their lives. This is in line with the findings of a pilot coaching intervention in which boundary setting and prioritization were used to improve well-being and reduce stress and burnout.37 Central elements of life coaching are to set goals and develop action plans, and our participants viewed those components as less important; instead, they emphasized the communication and relationship they had with the coach. This supports the research of Stelter38 who argues that a central perspective of coaching is the reflections and the exploration of values and meaning-making, and that new stories created in collaboration between the coach and the coachee will help the coachee to see things from a new perspective.
Methodologic considerations
The study complies with relevant criteria for COREQ39 and meets the demands of trustworthiness. Credibility was assured by triangulation, having three researches analyzing data and discussing themes until agreement and by peer debriefing with the physicians treating CF patients. A limitation of this study is that there was not consistency across all interviews in terms of setting and length of the interviews. However, the interview data were considered complete, nuanced, and rich in information. The primary investigator conducted the coaching intervention, and to avoid a risk of allegiance bias, the interviews were conducted by a co-author who did not take part in the intervention. During the interview, the informants were consistently asked to affirm or correct what the interviewer understood. Three researchers were engaged in the three-step analysis process, contributing to the credibility and trustworthiness of the study.40
Conclusion and clinical implication
Life coaching was appreciated by young adults with CF for being a safe environment to explore feelings and thoughts, but also for facilitating new behaviors. Life coaching was especially valued by those who were going through a difficult period of life. Our study adds important insight into the worldview of young adults with CF, and provides us with a greater understanding of their inner struggles and driving forces. The need to be heard should be given greater attention, especially among a group of patients who are isolated from others with the same disease and who withhold concerns to avoid stigmatization. As most participants were most motivated for a life coaching intervention in stressful phases of their lives, it can be noted that patients, screened for a high level of stress, could benefit from life coaching. Future research should explore screening parameters that can identify persons who will most likely benefit from life coaching.
Acknowledgments
The authors thank the participants for their contribution to the study. This research was supported by unconditional grants from Gilead Sciences Inc. and from Finsen Centre, Copenhagen University Hospital, Rigshospitalet.
Disclosure
The authors report no conflicts of interest in this work.
References
Spoonhower KA, Davis PB. Epidemiology of cystic fibrosis. Clin Chest Med. 2016;37(1):1–8. | ||
MacKenzie T, Gifford AH, Sabadosa KA, et al. Longevity of patients with cystic fibrosis in 2000 to 2010 and beyond: survival analysis of the Cystic Fibrosis Foundation Patient Registry. Ann Intern Med. 2014;161(4):233–241. | ||
Knudsen KB, Pressler T, Mortensen LH, et al. Associations between adherence, depressive symptoms and health-related quality of life in young adults with cystic fibrosis. Springerplus. 2016;5(1):1216. | ||
Sawicki GS, Sellers DE, Robinson WM. High treatment burden in adults with cystic fibrosis: challenges to disease self-management. J Cyst Fibros. 2009;8(2):91–96. | ||
Quittner AL, Goldbeck L, Abbott J, et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers: results of The International Depression Epidemiological Study across nine countries. Thorax. 2014;69(12):1090–1097. | ||
Quittner AL, Zhang J, Marynchenko M, et al. Pulmonary medication adherence and health-care use in cystic fibrosis. Chest. 2014;146(1):142–151. | ||
Smith BA, Modi AC, Quittner AL, Wood BL. Depressive symptoms in children with cystic fibrosis and parents and its effects on adherence to airway clearance. Pediatr Pulmonol. 2010;45(8):756–763. | ||
Eakin MN, Riekert KA. The impact of medication adherence on lung health outcomes in cystic fibrosis. Curr Opin Pulm Med. 2013;19(6):687–691. | ||
Waldboth V, Patch C, Mahrer-Imhof R, Metcalfe A. Living a normal life in an extraordinary way: a systematic review investigating experiences of families of young people’s transition into adulthood when affected by a genetic and chronic childhood condition. Int J Nurs Stud. 2016;62:44–59. | ||
Badlan K. Young people living with cystic fibrosis: an insight into their subjective experience. Health Soc Care Community. 2006;14(3):264–270. | ||
Kaushansky D, Cox J, Dodson C, McNeeley M, Kumar S, Iverson E. Living a secret: disclosure among adolescents and young adults with chronic illnesses. Chronic Illn. 2017;13(1):49–61. | ||
George M, Rand-Giovannetti D, Eakin MN, Borrelli B, Zettler M, Riekert KA. Perceptions of barriers and facilitators: self-management decisions by older adolescents and adults with CF. J Cyst Fibros. 2010;9(6):425–432. | ||
Gjengedal E, Rustøen T, Wahl AK, Hansen BR. Growing up and living with cystic fibrosis. Adv Nurs Sci. 2003;26(2):149–159. | ||
Oddleifson DA, Sawicki GS. Adherence and recursive perception among young adults with cystic fibrosis. Anthropol Med. 2017;24(1):65–80. | ||
Higham L, Ahmed S, Ahmed M. Hoping to live a “normal” life whilst living with unpredictable health and fear of death: Impact of cystic fibrosis on young adults. J Genet Couns. 2013;22(3):374–383. | ||
Quittner AL, Abbott J, Georgiopoulos AM, et al. International Committee on Mental Health in Cystic Fibrosis: Cystic Fibrosis Foundation and European Cystic Fibrosis Society consensus statements for screening and treating depression and anxiety. Thorax. 2016;71(1):26–34. | ||
Mogayzel PJ, Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680–689. | ||
Goldbeck L, Fidika A, Herle M, Quittner AL. Psychological interventions for individuals with cystic fibrosis and their families. Thorax. 2015;70:1089–1091. | ||
Kivelä K, Elo S, Kyngäs H, Kääriäinen M. The effects of health coaching on adult patients with chronic diseases: a systematic review. Patient Educ Couns. 2014;97(2):147–157. | ||
Spence GB, Grant AM. Professional and peer life coaching and the enhancement of goal striving and well-being: an exploratory study. J Posit Psychol. 2007;2(3):185–194. | ||
Whitworth L, Kimsey-House K, Kimsey-House H, Sandahl P. Co-active Coaching: New Skills for Coaching People Toward Success in Work and Life. Palo Alto, CA: Davies-Black Pub; 2007:312. | ||
Knudsen KB, Pressler T, Mortensen LH, et al. Coach to cope: feasibility of a coaching intervention for young adults with cystic fibrosis. Patient Prefer Adherence. 2017;11:1613–1623. | ||
ACTP Accreditation–Program Accreditation–ICF [Internet]. Available from: http://coachfederation.org/program/landing.cfm?ItemNumber=2151. Accessed September 21, 2017. | ||
Schwellnus H, King G, Thompson L. Client-centred coaching in the paediatric health professions: a critical scoping review. Disabil Rehabil. 2015;37(15):1305–1315. | ||
Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18(2):145–153. | ||
Ricoeur P. The hermenuetic function of distanciation. Philos Today. 1973;17(2):129–141. | ||
Oades LG, Spence GB. Coaching with self-determination in mind: using theory to advance evidence-based coaching practice. Int J Evid Based Coach Mentor. 2011;9(2):37–55. | ||
Ryan R, Deci E. Self-determination theory and the facilitation of intrinsic motivation. Am Psychol. 2000;55(1):68–78. | ||
Heaton J, Räisänen U, Salinas M. “Rule your condition, don”t let it rule you’: young adults’ sense of mastery in their accounts of growing up with a chronic illness. Sociol Health Illn. 2016;38(1):3–20. | ||
Pearson ES. The “how-to” of health behaviour change brought to life: a theoretical analysis of the co-active coaching model and its underpinnings in self-determination theory. Coach An Int J Theory Res Pract. 2011;4(2):89–103. | ||
Baumeister RF, Leary MR. The need to belong: desire for interpersonal attachments as a fundamental human motivation. Psychol Bull. 1995;117(3):497–529. | ||
Williams KD. Ostracism. Annu Rev Psychol. 2007;58(1):425–452. | ||
Bohart AC. From there and back again. J Clin Psychol Sess. 2015;71(11):1060–1069. | ||
Bohart AC, Tallman K. Clients: the neglected common factor in psychotherapy. Hear Soul Chang Deliv What Work Ther. 2010;83–111. | ||
Ammentorp J, Uhrenfeldt L, Angel F, Ehrensvärd M, Carlsen EB, Kofoed P-E. Can life coaching improve health outcomes? A systematic review of intervention studies. BMC Health Serv Res. 2013;13:428. | ||
Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301. | ||
Schneider S, Kingsolver K, Rosdahl J. Physician coaching to enhance well-being: a qualitative analysis of a pilot intervention. Explore (NY). 2014;10(6):372–379. | ||
Stelter R. Third generation coaching: reconstructing dialogues through collaborative practice and a focus on values. Int Coach Psychol Rev. 2014;9(1):51–66. | ||
Tong A, Sainsbury P, Craig J. Consolidated criterio for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus group. Int J Qual Heal Care. 2007;19(6):349–357. | ||
Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res. 1999;34(5 Pt 2):1189–1208. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.