")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Living with a sibling who suffers from an eating disorder: a pilot interview study
Authors Callio C, Gustafsson SA
Received 27 June 2016
Accepted for publication 24 August 2016
Published 9 November 2016 Volume 2016:9 Pages 615—622
DOI https://doi.org/10.2147/JMDH.S115934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Carina Callio, Sanna Aila Gustafsson
Faculty of Medicine and Health, University Health Care Research Center, Region Örebro County, Örebro University, Örebro, Sweden
Background and objective: Having a sibling who suffers from an eating disorder (ED) has a profound effect on healthy siblings’ own health, quality of life and family relationships, yet siblings have been an excluded group within health care, and there is a lack of knowledge regarding healthy siblings’ needs and wishes for information and support. Thus, the aim of this study was to examine adolescents’ experiences of living with a sibling who suffers from an ED.
Method: In this small-scale pilot study, three boys and two girls aged 15–20 years were interviewed, and the interviews were analyzed by qualitative content analysis.
Results: This study confirms prior knowledge of adolescents’ experiences of living with a sibling who is suffering from an ED. The adolescents were concerned about their siblings and lacked information about their siblings’ illness and treatment progress. The girls described that their everyday life had been heavily influenced by their sisters’ illness, while the boys described that their everyday life with friends and activities were not affected to such a great extent. One new result that emerged as something positive was that some informants described that although the ED was a source of conflict in the family, it had led to greater awareness of the importance of gaining sufficient energy and had contributed to better meal situations in the family.
Conclusion: Having a sibling with an ED had a profound and negative effect on family relationships, and was often a source of conflict, especially around mealtime. However, it appeared that if parents were able to organize family meals and create an open and supportive climate, the negative effects for the family could be reduced. The health care professionals need to acknowledge the siblings’ need for information and support, and support parents in their important role of caring for well siblings.
Keywords: eating disorders, adolescents, siblings, family
Introduction
Eating disorders (EDs) often start during adolescence, thus many of those who suffer from ED live with their parents and siblings. Sibling relationships have a profound impact on development,1 are often the longest relationships in a person’s life, give children the opportunity to learn about themselves and others2 and impact our personality and coping abilities.3
Having a family member who suffers from an ED has a profound effect on family relationships and causes conflicts in the family.4–8 Siblings report worrying in silence and fear that the ill sibling might die,4–7 and they may feel uncomfortable to express feelings that would bring attention to themselves and adopt a role as an undemanding child7 or take on a role as a mediator between the ill sibling and the parents.9
Siblings of ED patients report higher levels of depression and negative sibling relationship compared to a control group10 and express that the illness has a negative impact on their quality of life.4,7 The healthy siblings often have a great sense of responsibility and when the previous equal relationship between the siblings changes, the healthy sibling can assume a more parent-like role.1,5–7,9,11,12 The healthy siblings are often engaged in caregiving activities9,11 and have been suggested to have a beneficial influence on the ill sibling’s recovery.13 Despite this, few studies have explored the role of siblings and how the ill and the healthy siblings influence each other.4,8
Parents try to protect their healthy children by, for example, withholding information about the serious nature of the sibling’s disease.14 Meanwhile, the healthy sibling often feels left out and neglected by parents5,6 and lacks information about the sibling’s disorder.1,4–7,9 Siblings have also often been neglected by mental health care systems.1 However, in family-based treatment for EDs, siblings are considered an integral part of the treatment.15 In this approach, siblings are encouraged to take part in family sessions, and the role of the siblings is to support the patient, without taking on a parental role. The goal is to reinforce healthy intergenerational boundaries in the family, and counterproductive cross-generational alliances are confronted in therapy.15
However, growing up with an ill sibling may also have some positive effects. For example, young adults who had grown up with a chronically ill sibling reported that the illness had positive effects on their life, such as cautiousness about their own health, acceptance of others, feeling empathy and compassion for others, maturity and appreciation of life.16 Family solidarity and stronger family relationships have been reported by healthy siblings as positive outcomes of having a sibling who suffers from an ED.4,7,9
Thus, having a sibling who suffers from an ED affects the everyday life of adolescents in many ways. Yet, we lack knowledge about how the healthy siblings experience their situation, and their need for guidance and support. Against this background, the aim of the present study was to examine adolescents’ experiences of living with a sibling who suffers from an ED.
Methods
All informants and their parents provided informed written consent. Before the inclusion started, the study was ethically approved by the review board at St Lukas institution of psychotherapy at Ersta Sköndal college. Recruitment of participants took place in a specialist treatment unit, where both authors are employed. Approximately 20 families were asked by care staff at the unit to distribute an information letter to healthy siblings aged 13–20 years living at home. The therapists informed both the parents and the sick adolescents during a family session, and gave them a letter to pass on to the sibling. Siblings who wished to take part contacted the interviewer to arrange a time and place for the interview. Patients were excluded if they were treated by one of the researchers. Some of the patients did not want their siblings to receive information about the study, and some parents stated that the healthy sibling was unaware of the ED or that they did not talk about it and that the siblings’ life was not affected. These families did not want to ask the healthy sibling to participate, as they believed that it would only give rise to worry. Some 8–10 families took the letter home to share with the healthy sibling; and five adolescents (two girls and three boys) contacted the researcher to arrange for an interview.
An interview guide was developed to capture knowledge gaps in previous research in the area and included the following topics:
- How has the ED affected the family and the relations in the family
- Reflections on the healthy siblings’ need or wish for information, support or involvement in the treatment
- Consequences for the healthy sibling
The interview guide was sent to the adolescents two weeks before the interview to make it possible for them to prepare themselves. They were also informed that they were free to contact the researcher should they have any questions.
The interviews were carried out during February and March 2013. Five interviews were conducted with adolescents aged 15–20 years, three boys and two girls, all of whom had a sister undergoing treatment for ED. Four of the interviews took place at the ED unit, while one adolescent wished to be interviewed over the telephone. The interviews lasted for 40–50 minutes, were audiotaped and transcribed verbatim. The adolescents were given the opportunity to narrate freely around each topic, and the interviewer posed follow-up questions in order to obtain more in-depth information.
The interviews were analyzed by conventional content analysis.17 The interview texts were first read several times in order to obtain a general impression of the whole material. Then important statements were marked in order to capture the meaning of thoughts and impressions. Both researchers independently read and marked important statements, and these were then discussed in a process of negotiated consensus until an agreement was reached. Since the aim of the study was descriptive, the analysis was conducted on a manifest level. Data with the same meaning were then grouped into codes and domains based on the aim of the study. The two researchers undertook this step together.
Results
Six main categories emerged based on 16 subcategories. The subcategories are presented within quotes in the text. The names used in the “Results” section are fictitious (Table 1).
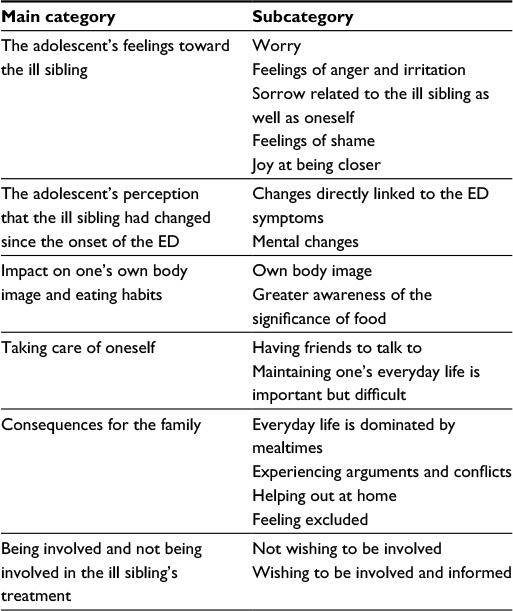 | Table 1 Overview of the results Abbreviation: ED, eating disorder. |
The adolescent’s feelings toward the ill sibling
The adolescent’s feelings toward the ill sibling were mainly characterized by “worry”.
You worry about it more or less all the time and I have also thought about whether she might take her life, you sort of never know. [Carl, 16]
The adolescents also described “feelings of anger and irritation” about their sisters’ behavior, and that they did not perceive that she wanted or tried to recover. While some adolescents contained their anger within themselves, others reported expressing their anger directly toward their sister.
In the beginning she denied it …”I don’t do anything wrong, nothing that isn’t right” and things like that …, then I could become really angry, go to her room and say that it’s not just difficult for her but for the whole family, and I sometimes started to cry or yell at her. [Eva, 16]
“Sorrow related to the ill sibling as well as oneself” was also evident. Also here, the extent to which the siblings revealed their sorrow to their ill sister differed. One adolescent described that she was able to talk to her sister about feeling sad and that they shared their sorrow.
I went to [sister] and told her my feelings, that I felt sad … and she became sad too, I think she realized after that how it affected the whole family. [Anna, 16]
Sorrow could also be about feelings of sadness and disappointment for oneself, for example, due to perceiving being disregarded, as the sister’s needs and wishes were paramount.
She is the one who decides where we will go for lunch, things like that, so I have no say in the matter or … it makes you feel a bit sad, disappointed but of course I realized that it was because of her problems. [Eva, 16]
“Feelings of shame” emerged in two interviews. The adolescents described finding it embarrassing and shameful that others knew about it or could see that their sister is suffering from ED. They did not want others to know about or notice it.
It’s sometimes embarrassing to explain it, if we go somewhere or are in a friend’s house, I have to put food on her plate… because she will not do it herself. … It was the same thing when she started school. For a while I had to put food on her plate and our teacher told the class that she had an eating disorder … so they knew about it but it still felt a bit odd putting food on her plate for her. [Anna, 16]
“Joy at being closer” emerged in two of the interviews. One of the participants described that due to the illness she and her sister took greater care of each other and spent more time together.
I believe that this may have led us to take greater care of each other. I think we are more aware of each other and notice if something is wrong and try to deal with it immediately to avoid the same situation happening again … we immediately ask “What is the matter?” … I suppose we have become closer, we do more things together, previously we did nothing. [Eva, 16]
The adolescent’s perception that the ill sibling had changed since the onset of the ED
All five participants reported noticing that their ill sister’s behavior had changed after the onset of ED.
One subcategory comprises “changes directly linked to ED symptoms,” such as reduced food intake and vomiting after meals. Sometimes, the sibling was the first to notice these changes, after which she/he told the parents, while in other cases it was the parents who informed the sibling.
I noticed that she ate very little in school … and she didn’t eat when she came home either … so I told mum. [Anna, 16]
I think it was mum who told me that she vomited in the shower, that is she went to the shower to vomit there, I think that was how it started. [Erik, 15]
The adolescents also narrated that “mental changes” such as anger, sadness and lack of energy became apparent to them in connection with their sister becoming ill with ED.
She can’t do things, can’t hang out with her pals and such, so I noticed, she may go there for one, two or three hours and then she comes home again, doesn’t want to stay … feels that she can’t cope. [Oliver, 20]
She spent a lot of time in her room by herself so she didn’t see her friends as much as before. She became more and more angry and bad-tempered. [Carl, 16]
She always looked tired, thin and haggard and never seemed happy … as soon as you said something she reacted aggressively and felt attacked. [Eva, 16]
One sibling also mentioned self-harm.
I think we were sitting at the dinner table and mum had found out and told me about it … I think it was that she cut herself … and vomited or something like that. [Carl, 16]
Impact on one’s own body image and eating habits
None of the siblings perceived that their sister’s illness had affected their “own body image.” Two of the brothers who participated did not consider that their sister’s illness had influenced their perception of their own body, while the other three adolescents stated that their body image was not affected, although admitting that they compared themselves with their sister.
Of course I was aware that she had become thinner and when walking beside her I appeared a bit fat but it doesn’t affect me because I like myself too much. [Eva, 16]
Three of the adolescents stated that their sister’s illness had led to “greater awareness of the significance of food” as well as the importance of food for gaining sufficient energy to do things. Two adolescents revealed that the family’s eating habits had improved and become more regular due to their sister’s illness, resulting in being able to do more at school.
Mealtimes are more regular now […], because they were a bit haphazard before […] I can do more at school now, I used to be constantly tired at school, but I have become more alert. [Erik, 15]
Taking care of oneself
The adolescents described the importance of “having friends to talk to.” Four of them described having talked to their friends about their sister’s illness. One adolescent narrated that a way of taking care of herself was by talking with her parents about things that she experienced as difficult. However, the others avoided talking to their parents about their worries, and none of them had sought support from student care, the youth center or similar, although some of them felt that it might be beneficial.
I talked to my friends … it helped me a lot … I had intended to go and talk to someone … but didn’t do it … never did. I don’t know why I didn’t go and talk to somebody. I have sometimes thought that it might have been much better for me had I done so … I don’t tell my mum or dad or my sister what I think, because I want to be sort of strong and support her. [Eva, 16]
The other subcategory was “maintaining one’s everyday life is important but difficult.” The adolescents wanted to have an ordinary life, do things that they enjoyed and spend time with their friends. They wished to continue their everyday life as before, although some of them found it difficult to maintain an ordinary life:
She doesn’t like me going out without her, so I don’t see my friends very much either … because she stays at home more or less all the time and I know that she gets sad, angry with me and sulks. [Anna, 16]
Both sisters described finding it difficult to bring their friends home due to their ill sister’s behavior.
One gets irritated, when watching TV for example, suddenly someone is standing beside you … I could see that my pals also became irritated with her. [Eva, 16]
Consequences for the family
All five adolescents were of the opinion that their families were constantly affected and restricted by their sister’s ED. A common thread in their narratives was that “everyday life is dominated by mealtimes” and that both mealtimes and the food served had changed.
We have like a schedule about who is to do the cooking and then we have to plan one week in advance what to cook, and I think it’s bloody frustrating and childish sort of … I don’t understand why mum doesn’t just say that today we prepare this and tomorrow we prepare that, but we have a schedule for everything and every little detail is planned and can’t be changed. [Carl, 16]
This limited the family’s possibility to travel and have a nice time doing pleasant things together.
We can never be away for very long … due to her frequent mealtimes … she has to eat six times a day… so we can only stay away for a certain number of hours. [Anna, 16]
The adolescents also reported that “experiencing arguments and conflicts” at mealtimes was a strain.
It was a bit difficult when we were going for a meal … because then she started like, I can have a child’s portion ... and Dad becomes so sad that he gets angry and then there’s a bad atmosphere as she feels that she doesn’t want to eat, she doesn’t allow herself to indulge in anything. [Eva, 16]
Two of the adolescents (both girls) perceived that they took greater responsibility for their parents by “helping out at home” more than previously.
As I’ve had to help out quite a lot with food and such, it’s only mum and I who have to do it … I’ve had to start helping more by fixing her meals. [Anna, 16]
Two of the adolescents described “feeling excluded” by their family.
I have felt excluded from time to time, at first I didn’t understand that mum and dad worried all the time, all the focus was on her … but then when it became more serious I understood that she needed attention, so it didn’t make me angry because … well, I was happy sometimes because I had been successful at school … and that was good but then the focus reverted to her. [Eva, 16]
Being involved and not being involved in the ill sibling’s treatment
Two of the brothers who were interviewed reported “not wishing to be involved” in the care of their sister.
I’m not all that interested … actually. [Erik, 15]
The remaining three adolescents expressed “wishing to be involved and informed.” One of them described how the staff did not want her to be involved in her sister’s care.
At first I accompanied her when she went for meetings … but then they didn’t think that I should be so involved so I didn’t go … I wanted to go, thought that she would lie there for ages, not allowed to come home … as she was worse she had to be admitted, she was in such a bad state ... so we knew that she was worse than before … she wasn’t able to eat at home any longer. [Anna, 16]
One sister stated that in her view, the care unit should provide an opportunity for siblings to attend support meetings and leave it up to them to decide whether or not they wanted to go.
Ask if one wants to talk to somebody … I think that would be good, I suppose everyone doesn’t want to … but they could ask so that one could have the opportunity. [Eva, 16]
Discussion
The aim of this small-scale pilot study was to examine adolescents’ experiences of living with a sibling who suffers from ED. Five adolescents, three boys and two girls, aged between 15 and 20 years were interviewed. It would have been desirable to interview a greater number of adolescents. However, parents and patients were somewhat reluctant to raise the issue with the healthy siblings. Some parents did not want to burden or worry the sibling. This is in line with previous findings that parents try to shield the healthy sibling out of consideration for her/him.14 Some parents considered that the healthy sibling did not know about the ED or was not involved, and therefore would not be able to contribute. Of course, we do not know what the situation was like in those families who declined to participate, but all the adolescents that took part in the study described that changes in their sibling’s behavior and mental health heavily affected them and the whole family. In several cases, the healthy sibling was the family member who first noticed the ill sibling’s disorder. Yet, several adolescents described not wishing to worry their parents and thus avoiding revealing feelings of worry, anger and sadness. Thus, it could be that the parents tend to underestimate how much the healthy sibling knows, notices or how much she/he worries and therefore do not include her/him. Excluding the siblings from treatment or withholding information might be counterproductive14 and may lead to a family atmosphere where conversations about the illness are avoided, which may rather increase the healthy siblings’ worries and resentment.1
Our results support previous findings that adolescents experience worry, anger, sadness and shame in relation to their sibling’s disorder. A previous study found that although siblings of adolescents with an ED reported higher scores on negative sibling relationship such as antagonism and jealousy compared to a control group, they did not differ in positive factors of sibling relationship, such as love and intimacy.10 Thus, it seems that although the ED evokes negative feelings toward the ill sibling, the positive aspects of the sibling bond remain. Previous research describes intense and conflicted emotions among siblings were due to the siblings experiencing feelings of injustice, hurtfulness, frustration and resentment, although also expressing a strong need to care for their sister.4,6 Two adolescents in our study also reported having become closer to their siblings, a result also reported in previous research.4,6,7,9 Although positive, it is important that siblings are encouraged to maintain their normal activities. Previous research has shown that siblings may feel obligated to exercise tolerance and understanding and be sensitive to the ill siblings’ needs.6 It may be hypothesized that a closer relationship between the siblings is associated with a stronger feeling of personal responsibility and conflicts of loyalty for the healthy sibling, and the healthy sibling may need help to express and cope with conflicting emotions. Otherwise, the healthy sibling may later on feel resentment against the sibling for having occupied much of the family’s attention. This may also cause feelings of guilt in the ill sibling. A recent study found that adolescents who recovered from ED have a strong sense of guilt about having become the focus of the parents’ attention at the expense of the healthy siblings during their illness.18 In family-based treatment for ED, restoring healthy boundaries between siblings and their parents is considered an important objective. This may help the siblings to maintain a close relationship in the long term.15
We believe that it is important for the siblings to be allowed to express these conflicting emotions, and to have some guidance on how to cope with them. The parents’ way of dealing with the situation may be important in addition to an open atmosphere that allows the family members to express their feelings, and an important role for the health care is to assist parents in this important task.14
There were differences in the way that sisters and brothers were affected by having a sibling who suffered from ED. Owing to the small number of participants in this study, no conclusions can be drawn, but an interesting observation is that sisters appeared to be more emotionally and practically involved in their sister’s ED than brothers. This was also found in the study by Garley and Johnson.6 The sisters described that their everyday life was affected by the fact that they helped out more at home. They also assumed responsibility for supporting their ill sister by abstaining from seeing their friends in order to stay at home with her. The girls wished for greater involvement in their sister’s treatment and to receive more information about the illness. Neither of the boys felt that their everyday life had been affected, nor did they wish to be involved in their sister’s treatment to any great extent. Garley and Johnson6 suggest that cultural norms may place a heavier carrying burden on sisters since women have traditionally assumed caretaking roles.
Some studies have suggested that having a sibling with an ED might be a risk factor for developing an ED, but the findings are contradictory.13 In a study that investigated disturbed eating behavior and associated psychological characteristics in ED patients, their healthy siblings and a control group, the siblings did not differ from healthy controls.19 In another study of female ED patients and their siblings, there was no evidence of any body image disturbances among the siblings. In a study that compared body image in female ED patients and their siblings, there was no evidence of any body image disturbances among the siblings.20 None of the adolescents in our study perceived that their sister’s illness had negatively influenced their body image. As a matter of fact, three of the adolescents described that although the ED was a source of conflict in the family, their sister’s illness had led to greater awareness of the importance of eating to gain sufficient energy to do things, and two brothers reported that the family mealtime routines had improved, in turn leading to positive effects for them. This is a finding not previously reported. Previous research has shown that participation in family meals is protective against dieting and unhealthy weight control behaviors even after controlling for atmosphere at family meals.21 Thus, family meals seem to have a supportive effect, even though there may be some conflicts. This highlights the importance of supporting parents in dealing with mealtimes as well as making them aware that structured mealtimes will benefit all family members. The sibling’s frustration can be reduced by creating awareness that these changes can be positive for all the family members. In a previous interview study, younger sisters of adolescents with anorexia expressed a negative attitude toward dieting.5 These results might indicate that growing up with a sibling who suffers from an ED might actually provide an opportunity for health literacy. This has previously been reported among siblings of patients with chronic illness.16 A better understanding of how the ED affects the healthy sibling may decrease parents’ feelings of guilt and fear that the healthy siblings will be affected.
The interviewed adolescents exhibited different views of whether or not they wished to be involved in the treatment. Several studies have emphasized the importance of involving healthy siblings in treatment of adolescent ED,7,8,11,14 and in family-based treatment, siblings are an important and integral part of the treatment.15 However, siblings have often been described as being reluctant to take part in family therapy.11 Perhaps this aversion is based on a fear that involvement in the treatment will increase siblings’ caretaking responsibilities. It is therefore important that siblings as well as parents are clearly informed about the rationale for sibling participation and that the siblings are not supposed to take on a parental role.
It has previously been suggested that the relationship between the siblings before the onset of the illness is important to take into account when involving healthy siblings in the treatment, and that there is insufficient knowledge of how the healthy sibling is affected by being involved in the treatment.11 A close relationship between the siblings enhances the healthy sibling’s wish and need to be more involved in what is happening to her/his ill sibling. It is essential that involvement in treatment is based on the sibling’s own wish to participate. This makes it important to raise the question with the family in order to understand what the relationship between the siblings is likely to be and how it was previously. For example, a way of ensuring that siblings have the opportunity to express their wishes is routinely inviting them when a family member is starting treatment for ED in order to provide them with information and ask whether they need some support.
A limitation of the study is the small number of participants and that saturation of the data was not reached. Thus, it is likely that more interviews would have added to the results, and allowed for a deeper interpretation of some results. For example, the two sisters seemed to be more affected by their sister’s ED compared to the three brothers. However, the two sisters also elaborated more on their answers in general, compared to the three brothers and the overrepresentation of the voices of Anna and Eva may bias the results. More interviews may have made it possible to get a deeper understanding of the gender differences. Another limitation is the inclusion procedure, where the healthy siblings were invited to participate in the study by their family members who took part in the treatment. In this way, the selection procedure favored those families in which there was a certain openness in relation to ED. Despite these limitations, we believe the results of this study confirm those reported by previous research in the field, as well as present some new findings to explore further in quantitative studies. Especially, the findings that the sisters seemed more emotionally affected by their sister’s ED and that the ED affected their everyday life more compared to the brothers need to be explored in a larger quantitative study including sisters and brothers of female and male patients. The finding that some of the adolescents described that the ED had led to greater awareness of the importance of gaining sufficient energy and had contributed to better meal situations in the family is also important to investigate further.
Disclosure
The authors report no conflicts of interest in this work.
References
Abrams MS. The well sibling: challenges and possibilities. Am J Psychother. 2009;63(4):305–317. | ||
Dunn J. State of the art: siblings. The Psychologist. 2000;13(5):244–249. | ||
White L. Sibling relationships over the life course: a panel analysis. J Marriage Fam. 2001;63(2):555–568. | ||
Halvorsen I, Ro O, Heyerdahl S. Nine-year follow-up of girls with anorexia nervosa and their siblings: retrospective perceptions of parental bonding and the influence of illness on their everyday life. Eur Eat Disord Rev. 2013;21(1):20–27. | ||
Latzer Y, Ben-Ari A, Galimidi N. Anorexia nervosa and the family: effects on younger sisters to anorexia nervosa patients. Int J Adolesc Med Health. 2002;14(4):275–281. | ||
Garley D, Johnson B. Siblings and eating disorders: a phenomenological perspective. J Psychiatr Ment Health Nurs. 1994;1(3):157–164. | ||
Areemit RS, Katzman DK, Pinhas L, Kaufman ME. The experience of siblings of adolescents with eating disorders. J Adolesc Health. 2010;46(6):569–576. | ||
Dimitropoulos G, Freeman VE, Bellai K, Olmsted M. Inpatients with severe anorexia nervosa and their siblings: non-shared experiences and family functioning. Eur Eat Disord Rev. 2013;21(4):284293. | ||
Dimitropoulos G, Klopfer K, Lazar L, Schacter R. Caring for a sibling with anorexia nervosa: a qualitative study. Eur Eat Disord Rev. 2009;17(5):350–365. | ||
Latzer Y, Katz R, Berger K. Psychological distress among sisters of young females with eating disorders: the role of negative sibling relationships and sense of coherence. J Fam Issues. 2015;36(5):626–646. | ||
Honey A, Clarke S, Halse C, Kohn M, Madden S. The influence of siblings on the experience of anorexia nervosa for adolescent girls. Eur Eat Disord Rev. 2006;14(5):315–322. | ||
Whitney J, Murray J, Gavan K, Todd G, Whitaker W, Treasure J. Experience of caring for someone with anorexia nervosa: qualitative study. Br J Psychiatry. 2005;187:444–449. | ||
Vandereycken W, Van Vreckem E. Siblings of patients with an eating disorder. Int J Eat Disord. 1992;12(3):273–280. | ||
Honey A, Halse C. Looking after well siblings of adolescent girls with anorexia: an important parental role. Child Care Health Dev. 2007;33(1):52–58. | ||
Lock J, Le Grange D. Treatment Manual for Anorexia Nervosa. A Family Based Approach. 2nd ed. The Guilford Press: London; 2012. | ||
Fleary SA, Heffer RW. Impact of growing up with a chronically ill sibling on well siblings’ late adolescent functioning. ISRN Family Med. 2013;2013:737356. | ||
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. | ||
Lindstedt K, Neander K, Kjellin L, Gustafsson SA. Being me and being us – adolescents’ experiences of treatment for eating disorders. J Eat Disord. 2015;3:9. | ||
Wunderlich U, Gerlinghoff M, Backmund H. Eating disturbances in siblings of patients with eating disorders. Eat Weight Disord. 2004;9(4):258–263. | ||
Benninghoven D, Tetsch N, Jantschek G. Patients with eating disorders and their siblings. An investigation of body image perceptions. Eur Child Adolesc Psychiatry. 2008;17(2):118–126. | ||
Loth K, Wall M, Choi CW, et al. Family meals and disordered eating in adolescents: are the benefits the same for everyone? Int J Eat Disord. 2015;48(1):100–110. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.