")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 9 » Issue 1
Living in negotiation: patients’experiences of being in the diagnostic process of COPD
Authors Lindgren S, Storli SL, Wiklund-Gustin L
Received 7 January 2014
Accepted for publication 20 February 2014
Published 6 May 2014 Volume 2014:9(1) Pages 441—451
DOI https://doi.org/10.2147/COPD.S60182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Sari Lindgren,1,2 Sissel Lisa Storli,3 Lena Wiklund-Gustin4,5
1Department of Health and Care Sciences, Faculty of Health Sciences, UiT Arctic University of Norway, Tromsø, Norway; 2Faculty of Health and Society, Narvik University College, Narvik, Norway; 3Department of Health and Care Sciences, Faculty of Health Sciences, UiT Arctic University of Norway, Tromsø, Norway; 4Faculty of Health and Society, Narvik University College, Narvik, Norway; 5School of Health, Care and Social Welfare, Mälardalen University, Västerås, Sweden
Purpose: To illuminate patients’ lived experiences of going through the process of being diagnosed with chronic obstructive pulmonary disease (COPD).
Patients and methods: A phenomenological-hermeneutic analysis was applied in the interpretation of interviews with eight persons diagnosed with mild or moderate COPD.
Results: One main theme ‘living in negotiation’, and three themes ‘living with a body out of step with the diagnosis’, ‘dealing with the past’, and ‘being challenged by the future’ reflected the process participants were living through in their quest for acceptance and a new balance in life. Participants found that the diagnostic processes were confusing, and that the diagnosis itself was ‘a slap in the face’. Unclear messages gave rise to fluctuating between an understanding of the condition as ‘not too severe’, insecurity, and fear. Shame and guilt related to the diagnosis had origins in the past, and in combination with the idea of ‘chronic’ the COPD diagnosis interfered with the present moment and gave rise to uncertainty for the future. The understanding of the present is related to negotiations not only with the past, but also with the future. Thus temporal aspects of the diagnosis are of great significance for the process of finding acceptance.
Conclusion: Regardless of disease severity, the diagnosis seems to be a breakdown of life, which puts life itself at stake. Medical professionals should be aware that the way the diagnosis is disclosed and communicated has considerable significance for how individuals understand and deal with their illness. The diagnosis should be communicated face-to-face, clearly and with empathy, and followed by information about COPD. Physicians should allow time and listen to the patients’ stories, and thus develop a shared understanding of the temporal aspect of the illness and patients’ needs and concerns. Thus, good communication is essential in determining whether the patient remains in negotiation, or enters a process toward acceptance and new understanding.
Keywords: Chronic obstructive pulmonary disease, phenomenological hermeneutics, lived experience, temporality
Introduction
The global burden of chronic obstructive pulmonary disease (COPD) remains a major public health problem; in 2020 it is projected to rank fifth worldwide in burden of disease, and it represents a huge economic challenge for the health care system.1 The strategy of the Global Initiative for chronic Obstructive Lung Disease (GOLD) strongly encourages early detection and prompt diagnosis; this will increase the possibility of smoking cessation, which is the most effective intervention to reduce the risk of developing COPD, stop its progression1,2 and improve long-term prognosis.3 COPD is both under-diagnosed and diagnosed late in primary care.4–6 An exacerbation emergency is often the first presentation of previously undiagnosed but symptomatic COPD and frequently severe at presentation.7 However, one study shows that nearly every second patient presents at early stages of the disease, thus opening a window for behavioral and therapeutic intervention.8 A large number of general practitioners (GPs), especially outside of Europe and North America, have very limited knowledge of COPD and its management.9 It has been found that GPs intentionally avoid early diagnosis as a result of misperception of patients’ unwillingness to be given a diagnosis and their own pessimistic attitude to prognosis.4 To achieve ‘optimal’ COPD care, holistic management is proposed based on the concept that immediate goals should be integrated with goals to improve long-term outcomes.10 COPD has been described as ‘a story with no beginning’,11 as early symptoms are seen as a normal way of life.3,11–13 A common way of coping with symptoms is avoiding or giving up physical activity.13–15 The shame of a self-inflicted disease is a reason for delaying taking the initiative to seek medical advice.14 The diagnostic phase is experienced as a prolonged process,14 where the COPD diagnosis is not clearly communicated.4,12,14 Diagnostic information is lacking, or given insensitively, and patients do not receive enough information regarding their prognosis or future management.16 Patients express uncertainty about the difference between asthma and COPD,14 and they do not understand the terminology used by their doctors nor its implications.16 Patients themselves use terms such as asthma, emphysema or bronchitis,4,17,18 or are not able to provide a name for their chest condition.19 At the time of diagnosis the person experiences a sense of loss and also hopelessness which is difficult to come to terms with, perceiving that ‘nothing can be done’.20 COPD is an invisible disability that affects individuals negatively and is a source of suffering related to a need to justify or explain one’s behavior.21 Patients feel guilty for smoking17,18,22,23 and are exposed to stigmatizing attitudes in society as well as in the health care system,22,23 and some conceal their impairments to avoid stigmatization.21 Patients have poor understanding of their condition and express frustration when not given a diagnosis4 or sufficient information or education about COPD.16,17,19,20,24 Some patients express a need of information at the point of diagnosis, including prognosis and management strategies, while others prefer less prognostic information and may avoid information that might lead to worries for the future.12,16 Experiences of self-blame and helplessness undermine patients’ sense of control and contribute to poor self-management.23 A good relationship and communication with the patient is fundamental when discussing diagnosis and prognosis25,26 and the poor long-term prognosis of COPD is best communicated with compassion and empathy.12 In order to meet patients’ needs, sufficient chronic care programs and robust self-management support are required. Primary care needs to transform its approach to chronic disease, including COPD.3,27 Research on the early stages of COPD has mainly been conducted from a pathophysiological and medical view, with a focus on diagnostic criteria and management of symptoms.1,2 Previous research leads to the conclusion that the COPD diagnosis has a great impact on people’s lives, and is a source of suffering for the individual.20,21,24 To date, qualitative COPD research has been focused on challenges met in severe stages of COPD.28–31 Surprisingly few studies with a qualitative approach focus on patients’ experiences of the diagnostic process or early stages of the disease. To be able to meet patients’ needs, knowledge about patients’ perspectives is essential. A phenomenological lifeworld perspective32–34 emphasizes the everyday world as it is experienced by a subject, and attempts to explicate the meanings of phenomena as we live them in our everyday existence. Thus a lifeworld approach in research can provide understanding of how the COPD diagnosis influences life, and how the person can be supported during the diagnostic process.
The aim of this study is to illuminate the meaning of being in the diagnostic process of COPD.
Method
The process of understanding the meaning of patients’ lived experiences of being in the diagnostic process of COPD was guided by a phenomenological-hermeneutic method.33 The aim of a phenomenological approach is not to describe objective facts; it is based on people’s everyday experiences32–34 and is suitable for studying the uniqueness in human situations.
Perspectives and methodological approach
According to Merleau-Ponty,35 we exist as lived bodies inseparable from our world and it is through the body we direct our intentionality to our projects in life and add meaning to the world while our experiences intersect with others. In contrast to the physiological body, the lived body is experienced immediately in a pre-reflective and non-objective way, and there is no perceived separation between body and self.35 Toombs, drawing on these perspectives, states that a disruption of bodily capacity, which illness represents, has a significance that far exceeds that of simple mechanical dysfunction, and when one’s body breaks down, so does life.36,37 A distinctive characteristic of chronic illness is its temporal dimension. Chronic illness persists over time; it is not a discrete episode in the course of a person’s life narrative, but a permanent feature of that narrative.38 Thus, access to participants’ experiences cannot be achieved without narration.33 By exploring people’s lived experiences, the present study can provide insights into nuances and variations of the meaning of being diagnosed with COPD. For research purposes, lived experience has to be fixed in texts and essential meaning must be revealed in the interpretation of the texts.33 Within the tradition of phenomenological hermeneutics, it is acknowledged that researchers are also part of the same world as the investigated phenomena. Thus objective interpretations are impossible, as the interpretations are always related to the researcher’s pre-understanding.33,39 Therefore distanciation from pre-understanding is necessary in order to not jump to conclusions. This requires an open, reflective attitude, ‘actively waiting’ for the phenomena and their meaning to be revealed, and a deliberate effort to restrain one’s pre-understanding by following certain methodological procedures. In this reflective process parts are understood in relation to the whole, and vice versa, as different phenomena are reflected on at different levels of interpretation, in the light of each other and also in relation to theory. This could also be described as a movement between understanding and explanation.39,40
Ethical considerations
The study was approved by the North Norwegian Regional Committee for Medical and Health Research Ethics. Participants were informed about the study and gave written consent to participate. People with serious illness and reduced functional capacity are considered a vulnerable group. This requires the interviewer to be open and sensitive and to respect participants’ integrity. As an interview may evoke painful memories and emotions, the participants could at any time stop the interview, and also contact their GP if needed after the interview.
Participants
The aim was to obtain data extensive enough to provide nuances and variations of participants’ experiences and thus provide descriptions that were rich and yet manageable in terms of the method.41,42 Purposive sampling was used to recruit persons diagnosed at least 2 months previously, with mild or moderate COPD, willing to tell about their experiences of being in the diagnostic process of COPD. Participants were recruited by three GPs in three practices and by one pulmonologist from an outpatient pulmonary rehabilitation clinic. Eleven potential participants were given prior written information. Those who gave written consent were contacted by telephone by the first author and an arrangement for an interview was made. There were no details about those not willing to participate in the study.
Participants’ characteristics are described in Table 1.
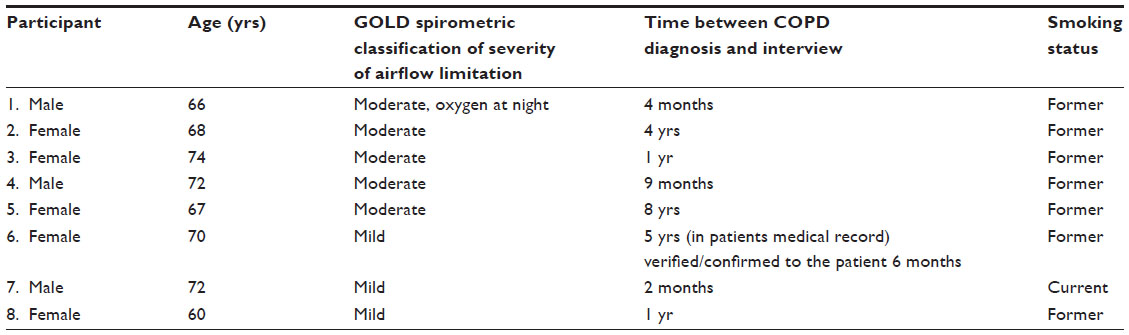 | Table 1 Descriptions of participants |
Interviews
All individual interviews were conducted during February to April 2010 by the first author in the participants’ homes. The study was introduced as aiming to highlight patients’ experiences of being diagnosed with COPD. The interviews were carried out in a relaxed atmosphere as a dialogue allowing participants to talk about any topic they found relevant in connection with COPD. However, participants were encouraged to narrate freely33 about their experiences of being diagnosed with COPD, and in what way the diagnosis had impacted their lives. New questions arose during the conversation based on the participant’s narrative. Follow-up questions such as: ‘How did you feel about that?’ and ‘Can you give an example?’ were used to gain a deeper understanding and to confirm shared understanding. The interviews lasted for 60–110 minutes, and were recorded digitally and transcribed verbatim by the first author.
Analysis
A phenomenological-hermeneutic analysis33 was applied in the interpretation of transcripts from the narrative qualitative interviews. The analysis aimed at interpreting the meaning of these texts through three steps: Naïve understanding, structural analysis, and comprehensive understanding.33 The naïve understanding aimed at grasping a first impression of the meaning of the text by repeated readings of the text as a whole. This first interpretation is however immature and conjectural. Thus further analysis is needed in order to obtain a valid interpretation.43 This is accomplished by structural analysis (explanation) aiming at distanciation.40 The text was divided into meaning units and condensed into everyday words. By going back and forth between the naïve understanding and meaning units, similarities and differences were clustered and abstracted into subthemes and themes (Table 2). In the comprehensive understanding the text was re-read and interpreted as a whole, with previous interpretations in mind, and further reflected upon in relation to theory. Thus different interpretations were confronted in a heterogeneous synthesis, ie, a synthesis able to include even seemingly different perspectives.40 This phase is a re-contextualization of the text, linking it to the context of the study and to a theoretical framework. This process provides contextual and theoretical support for the interpretations in a way that promotes further understanding.43
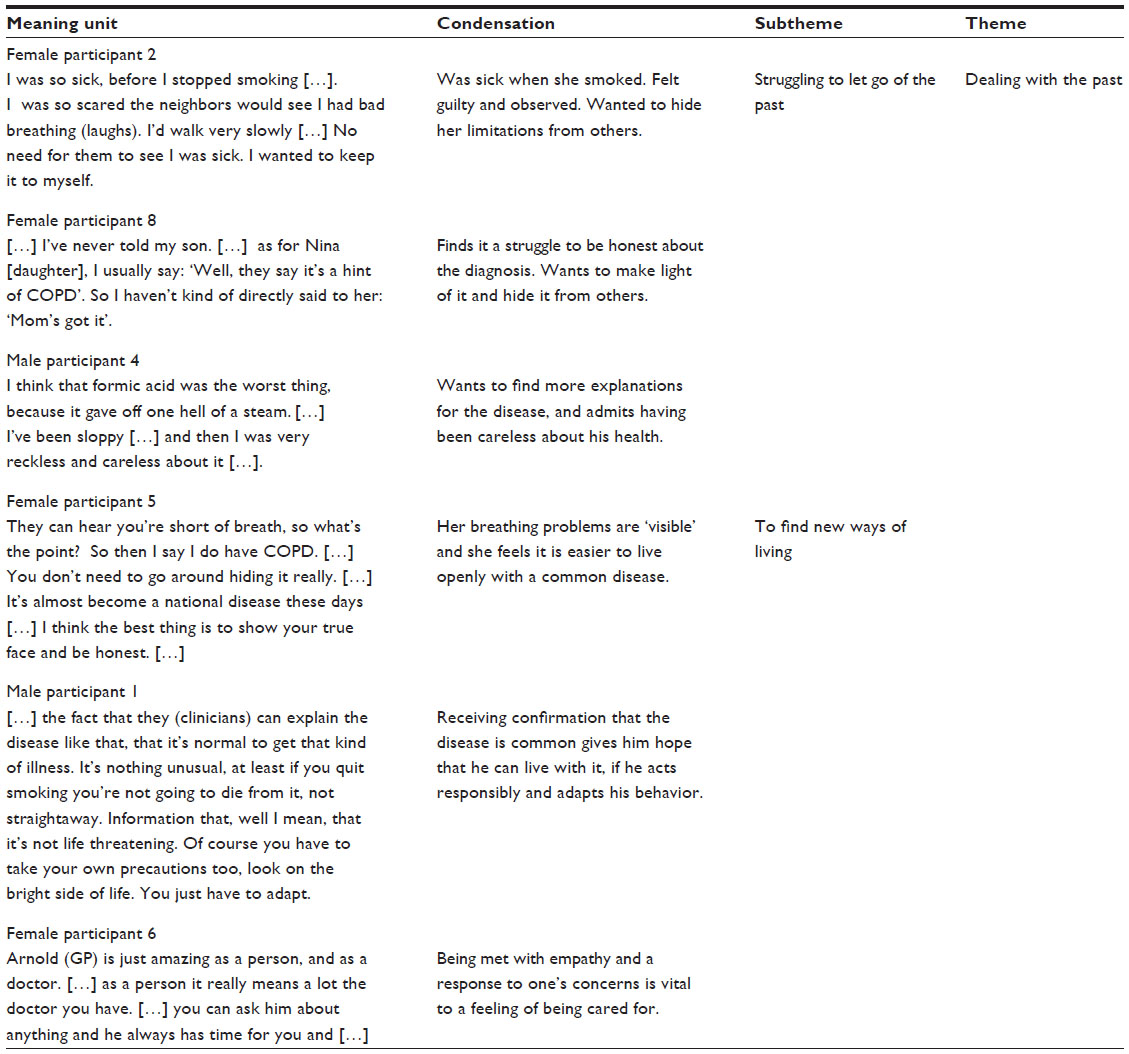 | Table 2 Examples from the structural analysis |
Findings
In order to create transparency in relation to the interpretation process, the presentation of the findings follows the three-step procedure;33 naïve understanding, structural analysis (with themes and subthemes) and comprehensive understanding.
Naïve understanding
Being diagnosed with COPD was interpreted as an experience intertwining both past and future life. The diagnostic process was experienced as prolonged and unclear, and when the COPD diagnosis was made, it was experienced as overwhelming and alien. Loss of bodily control restricted life and the diagnosis triggered uncertainty and fear for the future, but the fear also induced motivation and hope to be able to stop the decline. There was an ongoing struggle to find answers and support which could reduce symptoms and limitations. Having a self-inflicted disease gave rise to self-judgment, guilt and shame and participants struggled against being labeled as a COPD patient, partly through hiding and isolating themselves from the outside world. To accept the diagnosis, participants had an ongoing process of dealing with the past and finding different ways to release some of their guilt. Brief meetings and the way the diagnosis was delivered and portrayed contributed to feelings of uncertainty, and left participants alone with unanswered questions. The experience of being taken seriously and seen as an individual enhanced the possibility to take control of one’s own life, and the awareness of not being alone raised feelings of self-worth, which helped to enable participants to live with an open attitude toward their own illness and in relations with others.
Structural analysis
In the following, three themes and subthemes are presented.
Living with a body out of step with the diagnosis. Subthemes; ‘the struggle to find answers’ and ‘distance between the body and the diagnosis’.
Dealing with the past. Subthemes; ‘struggling to let go of the past’ and ‘to find new ways of living’.
Being challenged by the future. Subthemes; ‘being torn between fear and hope’ and striving to establish a new balance’.
The main theme, ‘living in negotiation’, emerged when the themes and subthemes in the structural analysis were related to each other. This is further elaborated in the comprehensive understanding.
Living with a body out of step with the diagnosis
The diagnostic process was initiated when physical limitations gave rise to a sense of losing control of life. Previously bodily impairments had been understood as harmless and related to eg, smoker’s cough or aging. Acknowledging that ‘there must be something wrong’ started ‘the struggle to find answers’ in order to synchronize with life again. As no immediate and clear answers were provided, the diagnostic process was experienced as a long journey of diagnostic tests giving rise to frustration and mistrust. When the diagnosis was made, participants struggled to make sense of it. Unclear messages such as ‘a hint of COPD’ or ‘a slight form of asthma’ made them feel insecure and doubtful, and left on their own with their questions unanswered.
[…] what I’ve been told is that I had a bit of […] ‘some spots on my lungs’. But not kind of how much and so on. Not what the reason was or anything like that? [Male participant 7]
These doubts lead to a striving to obtain a second opinion to ascertain the significance of such a diagnosis. Thus participants were continuously searching for information in order to regain control in life. However, the struggle to find answers was impeded by the ‘distance between the body and the diagnosis’, which also challenged the process of synchronizing and harmonizing with life again. Participants denied and distanced themselves from symptoms associated with COPD, and the diagnosis was perceived as alien and not as belonging to the body. Thus it was difficult to accept COPD as a reliable explanation of their health deterioration. Even when symptoms had a major impact on everyday life, the gap between the body and the diagnosis was evident.
I don’t have any problems connected to, well, to the COPD thing. Unless this pneumonia could be part of it? Because I don’t know that, do I? [Female participant 3]
By minimizing and negotiating the importance of symptoms, the diagnosis could partly be denied and kept at a distance, often in the shadow of a more ‘important’ or familiar diagnosis. Being introduced to the COPD diagnosis in written form when unprepared for it was overwhelming and evoked a sense of loss of control and feelings of distress and anxiety.
[…] well, it was a slap in the face getting it on a sick note. Instead of sitting down and talking about it normally […] maybe we’re lucky after all in this bad luck, by finding it out early on, so maybe you can do something about it? But when you just get it on a sick note, you start to wonder, ‘what is going on?’ Because as I said, I thought this was asthma.
[Female participant 8]
This kind of experience gave rise to feelings of not being taken seriously and being left alone in a vulnerable situation. By adapting to a life with a failing body, partly by doubting the symptoms and diagnosis, participants maintained a sense of normality in life and postponed dealing with the new diagnosis.
Dealing with the past
Getting the diagnosis was described as being ‘labeled’ as a smoker, a visible testimony of bad choices made in past life. Being exposed as a person with a self-inflicted disease was humiliating. ‘Struggling to let go of the past’ was a question of releasing some life-restricting guilt, in order to live with the condition as a part of oneself. By denying and negotiating the label, distressing feelings such as shame and guilt could be reduced, and dignity and identity could be maintained. Thus it was easier to reconcile with the diagnosis of asthma than with COPD.
[…] my God, have I got COPD? […]. I had a hard time believing it. […] ‘I haven’t got any COPD, you must just write asthma’, I said. ‘Cause I felt it was really terribly degrading’. [Female participant 8]
Participants expressed ambiguous attitudes toward smoking as the main causal factor, as non-smokers can also get COPD. They also pointed out that attitudes in society were different when they grew up than today. It was a moment of great disappointment when it became clear that they had failed, even though they took responsibility for it themselves.
After such a long time, is it really possible? […] nobody said then that smoking was dangerous. But that’s no excuse for me waiting so long before I gave it up. […] I get so annoyed with myself, to think I was so stupid. [Female participant 3]
It was also hard to let go of past norms such as staying healthy. A self-judgmental attitude hindered the process of acceptance of the diagnosis, and compliance with doctors’ advice to stop smoking.
[…] if I’d believed what the doctor said, that it’s COPD, well then I might have stopped smoking […]. Got scared enough to drop it […] It was pounded into me (from my childhood) that being ill, that’s something that doesn’t exist […] That’s the story of my life. [Male participant 7]
Feeling judged by oneself and others maintained a sense of guilt and shame, obstructing the process of letting go of the past and resulting in a concerted effort to hide the diagnosis. Thus, thoughts about not being entitled to health care and fear of being identified as a ‘COPD patient’ made participants prepared to forgo further information and treatment.
[…] at the same time I don’t know, do I dare go there (pulmonary rehabilitation)? Cause then they’ll know […] Then I’d actually get the diagnosis, and then it might come out, other people might get to know. ‘Yeah, she’s got COPD’! [Female participant 8]
For the participants, hiding their condition was intended to keep guilt at a distance and to preserve their own identity and dignity. However, having the prognosis explained in positive terms helped them to realize that they still had a chance to make changes and ‘to find new ways of living’. Experiences of having taken control and having made good choices made participants feel happy and proud of themselves, making it easier to let go of the past and to face the future in a new way.
[…] if you quit smoking, you’re not going to die from it, not straightaway. […] you have to take your own precautions too, look on the bright side of life. [Male participant 1]
When the participants realized that COPD was a common disease and that they were not alone, a more open attitude toward their own illness arose. Sharing experiences with understanding others raised participants’ self-esteem and made it easier to let go of self-criticism.
[…] from feeling you’re all alone with your illness to being able to share your thoughts with other people (in the same situation). Yes, I thought that was good. You know, because you get a bit kind of […] self-centered […] ‘poor me, what a pity’. Then you realize there are other people with the same fate. [Female participant 5]
Awareness of their own self-worth and needs led to further questions and also demands regarding treatment, such as physiotherapy, and general information, such as social welfare benefits, which increased their ability to live in the best possible way. Further, being seen as an individual and met with empathy eased some of the burden of guilt and self-imposed restrictions in life and facilitated reconciliation and letting go of the past. This thus enhanced their ability to live with the condition as a part of themselves.
Being challenged by the future
During the diagnostic process, the future is constantly intertwined with the here and now, raising questions about how one’s life will evolve. Thus, being challenged by the future is a question about ‘being torn between fear and hope’, and striving to establish a new balance. When participants finally acknowledge their symptoms or their diagnosis as serious, worries and expectations about the future soon follow. Questions about life and death arise in conjunction with experiences of losing control not only of one’s body but also of life itself.
[…] I’m hardly ever out and about with other people. […] now my physical strength’s beginning to go downhill […] and I can’t manage to do anything to get it back up again […] [Male participant 7]
The severity of one’s own situation was assessed by comparing COPD with other diagnoses, and this led to both fear and hope. It was a relief to know it was not cancer, and in spite of fear about how the future might be, there was hope of finding ways to manage problems as they became explicable. Experiences of losing oneself and one’s previous plans and dreams for the future made it difficult to accept the diagnosis. The threat of getting worse and becoming oxygen dependent was frightening but also led to motivation and hope to be able to stop the decline.
[…] that’s what I was afraid of […] that I’d be starting on oxygen … because I’d seen them walking around town with their oxygen bottle on their backs […] that (sighs) was quite something to make me quit smoking like that.
[Female participant 2]
Thus the fear of what the future might bring about also challenged participants in ‘striving to establish a new balance’. This meant making changes in life aimed at regaining control, and thus being able to let go of some fear. Experiences of learning to live with the problems also contributed to hope. Regaining control and hope therefore contributed to balance, and facilitated adjustment to the circumstances.
[…] I have to kind of hang over like this (supports herself on a table with outstretched arms) so I can get my breath back. […] When you get these kinds of breathing problems, it’s almost like it gets worse if you get a bit kind of panicky. When you can’t breathe properly […] But […] I’ve actually learnt to live with it so […]. If I get scared or […] like this, you get short of breath. […] The way it is now, I can live with it. [Female participant 5]
When participants were able to accept the diagnosis and adjust to the limitations imposed by the symptoms, they could reconcile with life becoming different from what they had hoped for. Acceptance and striving to make the best of life were described as crucial in receiving and living with the diagnosis.
Comprehensive understanding
This last interpretive step takes the process to another level of abstraction, by reflecting on previous steps in relation to the literature and linking with the broader context. The meaning of patients’ experiences of being in the diagnostic process was understood as ‘living in negotiation’. The diagnostic process was experienced as a journey of continuous back and forth movement embracing one’s whole life, in a quest for answers to preserve oneself and to find acceptance and a new balance in life. This negotiation process has been described by Toombs44 as ‘living through’, taking inspiration from Husserl’s45 radical distinction between objective clock time and subjective time. It is a process of lived time, interrelated as a whole, spanning past, present and future. Living through the diagnostic process means being involved over time in a struggle to negotiate and find explanations for bodily impairments. Adapting to symptoms maintains a sense of normality in life and dealing with a new situation can be postponed. Maintaining a sense of normality could be understood in the light of Leder’s46 view of the healthy body. Taking inspiration from Merleau-Ponty,35 he states that the healthy body performs without any need to reflect, and thus ‘disappears from consciousness’. In contrast, a sick, disabled and painful body will dys-appear in our consciousness and disturb and interfere with our plans and actions. However, maintaining a sense of normality fails when everyday life is disturbed too much by breathing problems and fatigue, leading to a need for answers. Being then diagnosed with COPD could metaphorically be described as ‘a slap in one’s face’. The diagnosis strikes suddenly and brutally, putting life itself at stake, and is hard to assimilate as a reality. This gives rise to fluctuating between an understanding of the condition as ‘not too severe’, and insecurity and fear.
Physical impairments and the experience of being labeled with a disease considered self-inflicted challenge identity and dignity. Shame and guilt related to the diagnosis with origins in the past interfere with the present moment and lead to uncertainty about the future. The understanding of the present is related to negotiations not only with the past, but also with the future. A temporal perception of ‘chronicity’ entails the creation of ‘chronic’ patients and can impede the patient’s view of the possibilities for change.47 Such a view of ‘chronic’ limits opportunities in the patient’s anticipated future life. This can be understood as contributing to hindering the individual’s effort to focus ahead to find a form of acceptance and balance in life and also to take responsibility to change life to prevent it deteriorating. Thus, everyday life is not only challenged in terms of physical interaction, but also by emotions such as anger, grief, shame and fear. According to Toombs, such unavoidable emotions are a principal source of suffering.38 Thus doubt and negotiation with the diagnosis may be understood as means to keep guilt and fear at a distance, and find balance in the present moment.
Being in the diagnostic process of COPD can be understood as a disruption of bodily capacity, as illness has a significance that far exceeds that of simple mechanical dysfunction36,37 and when one’s body breaks down, so does life.36 Shame is also an element contributing to the disruption.48 Past life and the future converge on the present, affecting the patients’ perceptions of the here and now and of their possibilities when living with a ‘new’ diagnosis. According to Toombs, being diagnosed with chronic illness incorporates a changed relation to one’s body, to the surrounding world and to others.38 A serious illness such as COPD becomes a profound threat to the self and represents a fundamental loss of wholeness, related not only to physical state, but to personhood. The disease disrupts who we are in terms of personal and professional roles and our goals and dreams in life.38 This can reduce a person’s feeling of self-worth and self-esteem, and evoke feelings of guilt, when lacking the energy to maintain social activities.38 By hiding the ‘COPD label’ one’s own identity and dignity are protected, but simultaneously difficulties arise in living honestly toward oneself and others. This calls for negotiations between protecting the vulnerable person associated with the diagnosis, and relating to others as the person one is.
Discussion of findings
The process of being diagnosed with COPD embraced and invaded all aspects of life and participants had ongoing negotiations with themselves and others to find reliable answers to help overcome obstacles in order to achieve a form of acceptance and to proceed with life with the new diagnosis. The process of negotiation that the participants are living through is characterized by a continuous back and forth movement embracing their entire lives. This movement toward acceptance is described by Delmar et al as getting in harmony with oneself.49 According to Delmar et al,49 acceptance of a chronic disease is both a learning process and an effort to acknowledge suffering, illness and disease as a part of life. As seen in other studies, participants narrated a story with ‘no beginning’,11 and made their undiagnosed illness a part of normal life.11,13–15 As other studies4,14 have concluded, being diagnosed in vague terms was a source of frustration and fear. In contrast to a sense of loss and a struggling with hopelessness described previously,20 this study also reveals that vague messages sometimes gave rise to experiences of hope about the diagnosis being incorrect or not too severe. Being diagnosed with a self-inflicted disease challenged identity and dignity, and participants often blamed themselves and felt judged by others. Participants’ efforts to hide the diagnosis made some of them also prepared to forgo both further information and treatment for fear of being identified as a ‘COPD patient’. As reported in previous studies, feelings of shame related to smoking can delay the help-seeking process14 and contribute to helplessness and poor self-management.23 Further, patients feel exposed to stigmatizing attitudes,22,23 including negative attitudes in the health care system if they failed to stop smoking. In the present study, vague messages followed by questions about smoking habits and general information about the lungs gave rise in some cases to feelings of mistrust and of not being taken seriously. The findings are in accordance with a review27 that shows that in dealing with a new COPD diagnosis, patients often experience stages of grief, denial, anger, bargaining and depression, on their way to acceptance. Decisions about smoking cessation and other self-care strategies may be complicated by these phenomena, and they may also contribute to non-adherence with therapy and poor respiratory and functional coping.50 A patient’s illness is usually defined in terms of objective and quantifiable data representing pathological and physiological conditions with specific locations in the body. But considering a diagnosis as a disease state in objective time regardless of past and future is to ignore the temporal structure of lived experience.44 For many participants, an objective early stage of the disease did not mean fewer worries and emotions regarding the diagnosis. It can thus be acknowledged that the significance of the diagnosis far exceeds what one can anticipate when terms such as ‘spots on the lungs’ are used. It is appropriate to conclude that the COPD diagnosis has a great impact on people’s lives; it is often a source of suffering for people who are constantly negotiating their lives in the tough dilemma of simultaneously trying to escape and justifying their way of behaving.20,21
Methodological considerations
In accordance with the phenomenological-hermeneutic approach, the aim was not to describe and generalize objective facts but to provide insights into participants’ lived experiences. The sample has limitations concerning the cultural setting as only ethnic Norwegians participated, but the age range of 60–74 is representative of the nature of the COPD trajectory. The number of participants was small (eight) but in terms of the aim of the study, the sample was representative and large enough to provide extensive data to enable an understanding of the meaning of being in the diagnostic process. This is consistent with the recommendations (15±10) in qualitative research51 and phenomenological studies to allow for in-depth analysis of the phenomena under investigation.42 Over the course of the interviews participants narrated similar experiences and no more new themes emerged after eight interviews. This point is comparable to data saturation and replication.41 Similar estimates for sample size are also found in grounded theory.52 But it must be borne in mind that the experiences of those willing to discuss their experiences may well differ from the experiences of those unwilling to discuss. The interviews express participants’ recollections of being in the diagnostic process. Time since diagnosis varied and some participants were diagnosed some time ago which may have affected their memory of the ‘point’ of diagnosis. Life changing events, such as being diagnosed, are structured by lived processes and embodied. In the interviews participants came close to experiences and narrated as if they were in the situation, but an element of reflection and contemplation may have changed experiences in retrospect. But as Husserl states,45 there is a radical distinction between objective clock time and subjective time. A diagnosis will not be experienced as an isolated now-point along a given timeline, but as a continuum which incorporates the present now-point but also past now-points as well as anticipations of future now-points. In this subjective experience of duration Husserl identifies a particular type of memory called ‘retention’ or primary memory, which differs from recollecting or secondary memory.44 Thus, narrative truth differs from empirical facts; it is endowed with meaning, not corresponding to empirical facts, but also not opposed to factual ‘truth’.43 Trustworthiness depends on truthful, detailed narratives of lived experiences,33 thus the interviews were carried out in a relaxed atmosphere as a dialogue allowing participants to talk freely, resulting in rich data. It is acknowledged that the participant’s narrative is directly influenced by and co-created with the researcher.32,43 A text can be interpreted in different ways, but the chosen interpretation has been validated by argumentation as plausible.40 Through the whole interpretation process it was important that the researchers were aware of their own pre-understanding and had as open a mind as possible. The structural analysis where interpretations were validated aimed at creating distance to the text and handling pre-understandings.40 All the authors (three) were involved in different parts of the interpretation process. The first author conducted all interviews and an initial interpretation. The co-authors made individual interpretations, followed by discussions within the team to ensure the validity of interpretations. Within the method the analysis of data and the presentation of the findings belong together.32,33 Thus to achieve trustworthiness, the interpretation process has been presented to allow the reader to follow it step by step. The findings show that the participants’ detailed narratives are not only restricted to the ‘point’ of diagnosis, but apply to the entire diagnostic process spanning past, present and future, interrelated as a whole. Thus a lifeworld approach was appropriate in this study.
Conclusion
This study reveals the burden and challenges of being diagnosed with COPD. Regardless of disease severity, the diagnosis is a breakdown of life which puts life itself at stake. Being diagnosed with a disease often termed both self-inflicted and ‘chronic’ sometimes interfered negatively with the present moment, and also partly impeded participants’ efforts to prevent health deteriorating. Living through the diagnostic process means being involved over time in a struggle to negotiate and find explanations for bodily impairments and to find acceptance and a new balance in life. Professionals should be aware that the way the diagnosis is disclosed and communicated has considerable significance on how individuals understand and deal with their illness. If the physician’s diagnosis focuses on the ‘here and now’ disease stage, temporal aspects of the illness and participants’ experiences and concerns may be disregarded. Rather than sharing a reality, patients and physicians then represent two different incommensurable time dimensions which can lead to a decisive gap in communication and understanding.44 This research suggests that the diagnosis should be communicated face-to-face, clearly and with empathy, and followed by information about COPD. But to be able to support patients, physicians should allow time and listen to the patient’s story/narrative and thus develop a shared understanding of the temporal aspect of the illness and patients’ needs and concerns.
Thus, good communication is essential in determining whether the patient remains in negotiation or enters a process toward acceptance and new understanding.
Further research on physicians’ perspectives of early stages of COPD can illuminate professionals’ experiences and attitudes, and research on patients’ experiences of how early stages of COPD affect life to come and how they adjust to the limitations can help clinicians to better understand patients’ needs and provide them with optimal support.
Disclosure
The authors report no conflicts of interest in this work.
References
Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2013. Available from: http://www.goldcopd.org/. Accessed November 12, 2013. | |
Vestbo J, Hurd SS, Rodriguez-Roisin R. The 2011 revision of the global strategy for the diagnosis, management and prevention of COPD (GOLD) – why and what? Clin Respir J. 2012;6(4):208–214. | |
Fromer L. Diagnosing and treating COPD: understanding the challenges and finding solutions. Int J Gen Med. 2011;4:729–739. | |
Walters JA, Hansen EC, Walters EH, Wood-Baker R. Under-diagnosis of chronic obstructive pulmonary disease: A qualitative study in primary care. Respir Med CME. 2008;102(5):738–743. | |
Schayck CPv, Loozen JMC, Wagena E, Akkermans RP, Wesseling GJ. Detecting patients at a high risk of developing chronic obstructive pulmonary disease in general practice: cross sectional case finding study. BMJ. 2002;324(7350):1370. | |
Lindström M, Jonsson E, Larsson K, Lundbäck B. Underdiagnosis of chronic obstructive pulmonary disease in Northern Sweden. Int J Tuberc Lung Dis. 2002;6(1):76–84. | |
Bastin A, Starling L, Ahmed R, et al. High prevalence of undiagnosed and severe chronic obstructive pulmonary disease at first hospital admission with acute exacerbation. Chron Respir Dis. 2010;7(2):91–97. | |
Kornmann O, Beeh KM, Beier J, Geis UP, Ksoll M, Buhl R. Newly diagnosed chronic obstructive pulmonary disease. Clinical features and distribution of the novel stages of the Global Initiative for Obstructive Lung Disease. Respiration. 2003;70(1):67–75. | |
Aisanov Z, Bai C, Bauerle O, et al. Primary care physician perceptions on the diagnosis and management of chronic obstructive pulmonary disease in diverse regions of the world. Int J Chron Obstruct Pulmon Dis. 2012;7:271–282. | |
Postma D, Anzueto A, Calverley P, et al. A new perspective on optimal care for patients with COPD. Prim Care Respir J. 2011;20(2):205–209. | |
Pinnock H, Kendall M, Murray SA, et al. Living and dying with severe chronic obstructive pulmonary disease: multi-perspective longitudinal qualitative study. BMJ. 2011;342. | |
Giacomini M, Dejean D, Simeonov D, Smith A. Experiences of Living and Dying With COPD: A Systematic Review and Synthesis of the Qualitative Empirical Literature. Ont Health Technol Assess Ser. 2012;12(13):1–47. | |
Habraken JM, Pols J, Bindels PJE, Willems DL. The silence of patients with end-stage COPD: a qualitative study. Br J Gen Prac. 2008;58(557):844–849. | |
Arne M, Emtner M, Janson S, Wilde-Larsson B. COPD patients perspectives at the time of diagnosis: a qualitative study. Prim Care Respir J. 2007;16(4):215–221. | |
Chan SC. Chronic obstructive pulmonary disease and engagement in occupation. Am J Occup Ther. 2004;58(4):408–415. | |
Gore JM, Brophy CJ, Greenstone MA. How well do we care for patients with end stage chronic obstructive pulmonary disease (COPD)? A comparison of palliative care and quality of life in COPD and lung cancer. Thorax. 2000;55(12):1000–1006. | |
Rodgers S, Dyas J, Molyneux AWP, Ward MJ, Revill SM. Evaluation of the information needs of patients with chronic obstructive pulmonary disease following pulmonary rehabilitation: a focus group study. Chron Respir Dis. 2007;4(4):195–203. | |
Hansen EC, Walters J, Wood Baker R. Explaining chronic obstructive pulmonary disease (COPD): perceptions of the role played by smoking. Sociol Health Illn. 2007;29(5):730–749. | |
Gardiner C, Gott M, Small N, et al. Living with advanced chronic obstructive pulmonary disease: patients concerns regarding death and dying. Palliat Med. 2009;23(8):691–697. | |
Oliver SM. Living with failing lungs: the doctor–patient relationship. Fam Pract. 2001;18(4):430–439. | |
McMillan Boyles C, Hill Bailey P, Mossey S. Chronic Obstructive Pulmonary Disease as Disability: Dilemma Stories. Qual Health Res. 2011;21(2):187–198. | |
Lindqvist G, Hallberg LR-M. ‘Feelings of Guilt due to Self-inflicted Disease’: A Grounded Theory of Suffering from Chronic Obstructive Pulmonary Disease (COPD). J Health Psychol. 2010;15(3):456–466. | |
Sheridan N, Kenealy T, Salmon E, Rea H, Raphael D, Schmidt-Busby J. Helplessness, self blame and faith may impact on self management in COPD: a qualitative study. Prim Care Respir J. 2011;20(3):307–314. | |
Gysels M, Higginson IJ. The Experience of Breathlessness: The Social Course of Chronic Obstructive Pulmonary Disease. J Pain Symptom Manage. 2010;39(3):555–563. | |
Halliwell J, Mulcahy P, Buetow S, Bray Y, Coster G, Osman LM. GP discussion of prognosis with patients with severe chronic obstructive pulmonary disease: a qualitative study. Br J Gen Pract. 2004;54(509):904–908. | |
Kennedy S. Caring for a patient newly diagnosed with COPD: a reflective account. Nurs Stand. 2011;25(49):43–48. | |
Fromer L. Implementing chronic care for COPD: planned visits, care coordination, and patient empowerment for improved outcomes. Int J Chron Obstruct Pulmon Dis. 2011;6:605–614. | |
Barnett M. Chronic obstructive pulmonary disease: a phenomenological study of patients’ experiences. J Clin Nurs. 2005;14(7):805–812. | |
Fraser DD, Kee CC, Minick P. Living with chronic obstructive pulmonary disease: insiders’ perspectives. J Adv Nurs. 2006;55(5):550–558. | |
Seamark DA, Blake SD, Seamark CJ, Halpin DM. Living with severe chronic obstructive pulmonary disease (COPD): perceptions of patients and their carers. Palliat Med. 2004;18(7):619–625. | |
Williams V, Bruton A, Ellis-Hill C, McPherson K. What really matters to patients living with chronic obstructive pulmonary disease? An exploratory study. Chron Respir Dis. 2007;4(2):77–85. | |
Dahlberg K, Dahlberg H, Nyström M. Reflective Lifeworld Research. [Lund]: Studentlitteratur; 2008. | |
Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18(2):145–153. | |
Van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. London, Ont: Althouse Press; 1997. | |
Merleau-Ponty M. Phenomenology of Perception. London: Routledge; 2002. | |
Toombs SK. The Meaning of Illness: A Phenomenological Account of the Different Perspectives of Physician And Patient. Dordrecht: Kluwer Academic Publishers; 1993. | |
Toombs SK. Handbook of Phenomenology and Medicine. Dordrecht: Kluwer Academic; 2001. | |
Toombs SK, Barnard D, Carson RA. Chronic Illness: From Experience to Policy. Bloomington: Indiana University Press; 1995. | |
Dahlberg K. The essence of essences – the search for meaning structures in phenomenological analysis of lifeworld phenomena. Int J Qual Stud Health Well-being. 2006;1(1):11–19. | |
RicŒur P. Interpretation Theory: Discourse and the Surplus of Meaning. Fort Worth, Tex: Texas Christian University Press; 1976. | |
Morse JM, Barrett M, Mayan M, Olson K, Spiers J. Verification Strategies for Establishing Reliability and Validity in Qualitative Research. Int J Qual Methods. 2002;1(2):1–19. | |
Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183. | |
Wiklund L, Lindholm L, Lindström UÅ. Hermeneutics and narration: a way to deal with qualitative data. Nursing Inquiry. 2002;9(2):114–125. | |
Toombs SK. The temporality of illness: four levels of experience. Theoretical Medicine. 1990;11(3):227–241. | |
Husserl E. The Phenomenology of Internal Time-Consciousness. Bloomington: Indiana university press; 1964. | |
Leder D. The Absent Body. Chicago: University of Chicago Press; 1990. | |
von Peter S. The Temporality of “Chronic” Mental Illness. Culture, Medicine and Psychiatry. 2010;34(1):13–28. | |
Toombs SK. The lived experience of disability. Hum Stud. 1995;18(1):9–23. | |
Delmar C, Bøje T, Dylmer D, et al. Achieving harmony with oneself: life with a chronic illness. Scandinavian Journal of Caring Sciences. 2005;19(3):204–212. | |
Post L, Collins C. The poorly coping COPD patient: a psychotherapeutic perspective. International Journal of Psychiatry in Medicine. 1981;11(2):173–182. | |
Kvale S. Interviews: An Introduction to Qualitative Research Interviewing. Thousand Oaks, Calif: Sage; 1996. | |
Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago: Aldine; 1967. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.