")
Back to Journals » International Journal of Women's Health » Volume 13
Lived Experience of Women Who Underwent Early Removal of Long-Acting Family Planning Methods in Bedesa Town, Wolaita Zone, Southern Ethiopia: A Phenomenological Study
Authors Obsa MS , Takiso KT, Ayele TT, Chare Koyra H , Tafesse Hidoto K , Getahun Molla Shanka G, Kelbiso Hanfore L, Arba MA , Anjulo AA , Worku Kercho M, Zema Z
Received 18 February 2021
Accepted for publication 23 June 2021
Published 2 July 2021 Volume 2021:13 Pages 645—652
DOI https://doi.org/10.2147/IJWH.S307142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Mohammed Suleiman Obsa,1 Kassahun Tekle Takiso,2 Tamiru Tilahun Ayele,1 Hailu Chare Koyra,3 Kassahun Tafesse Hidoto,4 Getahun Getahun Molla Shanka,2 Lolemo Kelbiso Hanfore,5 Mihiretu Alemayehu Arba,4 Antehun Alemayehu Anjulo,6 Melkamu Worku Kercho,7 Zewde Zema3
1Department of Anesthesia, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 2School of Medicine, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 3Department of Pharmacy, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 4School of Public Health, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 5Department of Nursing, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 6Department of Medical Laboratory Science, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 7Department of Midwifery, Wolaita Soddo University, Wolaita Soddo, Ethiopia
Correspondence: Mohammed Suleiman Obsa
Department of Anesthesia, Wolaita Soddo University, P.O. Box: 138, Wolaita Soddo, Ethiopia
Tel +251 924333199
Email [email protected]
Background: Long-acting family planning method (LAFP) is a low-cost yet effective method of reducing maternal mortality, limiting and spacing childbirth. In Ethiopia, the family planning prevalence rate rises from 15% in 2005 to 36% in 2016. However, the discontinuation rate of LAFP is still high in the region. Therefore, the aim of this study was to explore the lived experiences of women who underwent early removal of long-acting family planning methods in Bedesa town, Southern Ethiopia.
Methods: An interpretative phenomenological study design was employed. Women aged 15– 49 years who removed LAFP therapy in the past 12 months were our sampled population. Data were collected through in-depth interviews (IDIs) by using open-ended structured interview guide. Purposive sampling technique was used to select 10 participants from the family planning logbook registration of Bedesa health center. The interview continued until information saturation was reached. Open code version 4.03 was used to code and facilitate analysis. Transcripts were read and re-read separately to identify emerging themes. A thematic analysis technique was used.
Results: This study revealed that the side effects, seeking more children and the husband’s opposition were the main reason for early removal of LAFP. Amongst side effects, heavy and irregular menses were occurred most frequently. Besides, there were various myths and misconceptions about family planning methods. It also noted that the counseling services provided by health professionals were not adequate.
Conclusion: Side effects, desired to have more children, and the husband’s opposition are the most important reason of early removal of LAFP methods. Furthermore, there were misunderstanding, fear and rumors raised by women about each method. Hence, greater public awareness on family planning should be delivered to change community perception on LAFP methods.
Keywords: long-acting family planning method, early removal, phenomenology, Bedesa
Plain Language Summary
Family planning is a process which usually involves a discussion between a woman, a man, and a trained service provider by focusing on family health and the desires of the couple to either space birth interval or limit their family size. Intentions among women found in the childbearing age are usually classified into those who desired to have more children, those who wanted to space a birth interval and those who wanted to limit their family size. Although prevalence rate family planning use is increasing, the discontinuation rate of long-acting family planning methods still high in Ethiopia. Hence, this study was aimed to explore lived experiences of women who underwent early removal of long-acting contraceptives methods.
In this study, we used interpretative phenomenological approach which helped us know a detailed in-depth experience and perceptions of women who discontinued long-acting methods before the recommended time. We conducted 10 in-depth interviews on women who underwent early removal of long-acting family planning methods in Bedessa town. We used open-ended structured interview guide that permitted the participants to talk freely so that a well versed interviewer could gather rich data from participants. The interview guide consisted of basic sociodemographic characteristics, experiences and perceptions about family planning methods, and future suggestion on family planning use.
This study found that fear of side effects, desired to have large family size, husband’s opposition, wrong myths and misconceptions about long-acting planning family methods were the main reasons of removal. The main barriers of male involvement in family planning methods are lack of appropriate information, inaccessibility of family planning services, attitudes of men towards family planning, perceived fear of side-effects, cultural or religious oppositions and desire for more children.
In conclusion, health professionals and other stakeholders should create community awareness to modify community views about long-acting family planning methods.
Introduction
Long-acting family planning method is a low-cost yet effective method of preventing maternal health problems.1,2 It can play a key role in reducing maternal mortality and number of unintended births.3 These can result in substantial cost savings for families, governments; as a result, it can contribute directly to achieve the national and international health goals by providing long-lasting contraceptive protection.4 Moreover, avoiding barriers to the use of contraceptives and enhancing the demand for family planning could prevent 54 million unintended pregnancies. In addition, it could prevent more than 79,000 maternal and one million infant deaths per year.5
In Ethiopia, the prevalence rate of family planning use rises from 15% in 2005 to 36% in 2016. However, the unmet need for family planning is still high in the region (22%). This high unmet demand and other factors such as lack of awareness, fear of social rejection, resistance to spouses, religious or cultural values, and concern for side-effects lead to a high fertility rate (average 4.6 children).6 On the other hand, this rapid population growth is not in line with the weak economic growth of the country. Such an imbalance between population size and economic growth will certainly have a negative impact on the wellbeing of the nation.7
According to the 2016 EDHS report, the discontinuation rate of the Implant and IUD were 35% and 11%, respectively. Another mixed method study conducted by FMOH showed that 17% of the women removed their Implanon before the expected removal date.8 The most common reasons for early removal are the desire to become pregnant, side effects, wanting a more effective method, husband’s opposition, and inconvenience of use.9
Wolaita Zone is characterized by a crude population density of 385 people/square kilometer.7 Providing the most effective family planning methods is a vital strategy for the improvement of balancing population growth with local economic growth. Thus, this study aimed to explore the lived experience of women who underwent early removal of LAFP methods Bedessa town, Wolaita zone.
Methods and Materials
The study was conducted in Bedesa town which is the administrative capital of Damot Weyde district of Wolaita Zone, Ethiopia. The town got its name because it was located near Bedessa river. Bedessa is located about 373 KM away from Addis Ababa to the south direction on the way of sodo to Dimtu or Sodo to Hawassa road, and 21 KM away from sodo, the capital city of Wolaita Zone. An interpretative phenomenological (IPA) study design was used. We chose this method because it is very good at bringing out what is usually hidden in human experience and human relations.10 The use of IPA helped us understand how individuals make sense of their experience about LAFP.11 We selected participants for the in-depth interviews from the Bedesa health center, which were providing family planning services. The head of the health center assisted in the recruitment of participants to obtain rich information about the phenomenon. Women aged 15–49 years who removed LAFP therapy in the past 12 months were our sampled population. Finally, 10 participants were purposively selected from the family planning logbook registration of Bedesa health center. The interview continued until information saturation was reached. Data were collected through IDI using open-ended structured interview guide. It was uploaded as Supplementary File 1. The interview guide consisted of basic sociodemographic characteristics, experiences about LAFP methods, perceptions about FP, and future suggestion on family planning use. All interviews were conducted in a separate quiet room to avoid interruption from outside and to maintain privacy. Each IDI lasted for approximately 30 to 38 min. Interviews were conducted in the Amharic language. The free flow of information was encouraged through probing. All interviews were tape-recorded with the consent of interviewees. A unique identification number was assigned to all the recorded files. Audio data were transcribed verbatim and translated to English. The data were first saved in plain text format and imported into open code software version 4.03 to facilitate coding and categorizing. The coding process began with reading each transcript multiple times and their respective translations to ensure a degree of standardization. The coded data were compared and organized into groups. Finally, the thematic approach was used to classify and organize data according to key categories. The findings encompass direct quotes of women and narrated as without editing the grammar to avoid loss of its meaning.
Results
Sociodemographic Characteristics of the Participants
We carried out ten in-depth interviews among women who underwent early removal of LAFP methods. All study participants were married. The majority of participants were protestant in religion. In terms of age, the participants were between 25 and 32 years old, and the mean age was 29.10± (3.01). Four-fifth (8 out of 10) of the participants were government employees, and 2 out of 10 were housewives. Half of all study participants were diploma holders (5 out of 10) (Table 1).
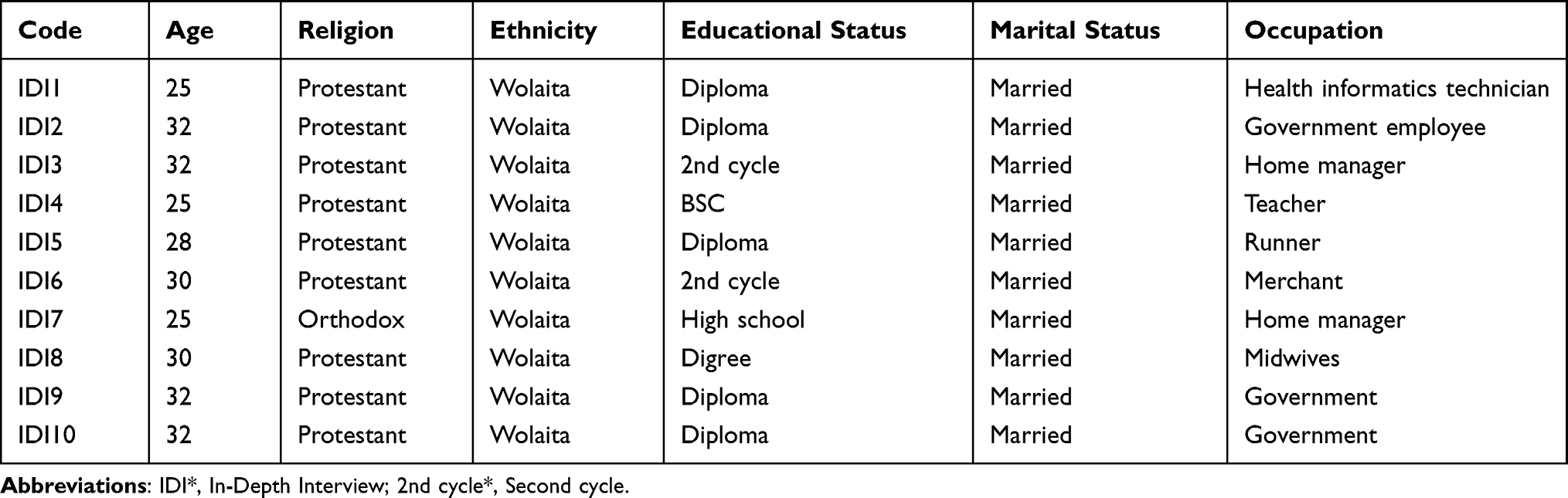 |
Table 1 Sociodemographic Characteristics of Women Who Underwent Early Removal of Long-Acting Family Planning Methods in Bedesa Town, Wolaita Zone, 2020 |
Women Experience About Long-Acting Family Planning Methods
Women have different experiences concerning the use of various family planning methods. Most women said that they regained their health immediately after removal of the LAFP method while some women have a similar complaint even after its removal. Most participants changed their use of LAFP methods to short-acting family planning methods, mainly to Depo-Provera.
One participant explained the condition while using family planning as:
Before I gave my first birth, I had been using depo. I used Jadelle after the second child. But Jadelle was removed because of side effects, and then I switched Jadelle to depo. (IDI2)
Another participants also explained the condition while using family planning as:
“ … After removal of Implanon, I regained my health and peaceful life. I have changed to Depo Provera, and I have been comfortable with depo. ” (IDI10)
After removal of Implanon, the bleeding was not improved, and I went to the health center, and they removed it. However, the bleeding remained without showing any improvement. (IDI7)
There are different side effects mentioned for early removal of LAFP, of which the frequently mentioned side effects were heavy and irregular menses, weight loss, and dizziness. The other mentioned side effects were crampy abdominal pain, skin discoloration, itching, behavioral change, numbness, burning sensation on micturition, melasma, headache, sleep disturbance, amenorrhea, delayed fertility, dysmenorrhea, frequent hunger, thirst, weakness, difficulty walking, and activity intolerance.
One of the participants pointed out side effects as the reason for early removal as follows:
I decided to discontinue early because of heavy and irregular menses and weight loss. The bleeding stayed for one to two months. I also had skin discoloration and itchy skin (IDI10)
The other participant also mentioned side effects as the reason for early removal as follows:
Implanon was inserted for 3 years, but it was kept only for 7 months. Because I was not comfortable, my facial skin color was changed, and black patches such as melasma appeared on my face. In addition, there was a movement in my abdomen like baby kicking during pregnancy, persistent neck pain, and absence of menses. (IDI1)
Appropriate utilization of family planning methods requires clear and concise counseling services by health workers. Although women received counseling services by the health care provider. Most of them explained that the counseling services were not adequate.
“Health workers gave me a counseling service before inserting Implanon. However, they didn’t inform me in detail about the benefits and risks of Implanon.” (IDI3)
The health care providers informed me that an implant is more advantageous than injectable Injectables do have an effect on bone damage, cause weight gain and contain additives. Pills are also full of additives, which may lead to gastritis. (IDI5)
Husband involvement in family planning methods and sharing responsibilities in reproductive life is essential. However, there was no consensus about the role of husbands in family planning decision-making. Some women got good support from their husbands while most of them did not get support. Some participants said that husband consider use family planning methods as women’s responsibility only while some of merely participate in discussion. The main barriers of husband involvement in family planning include attitudes of men towards family planning, cultural or religious oppositions, social norms, and desire for more children.
Some women pointed out the husband’s opposition as one of the reasons for the early removal of LAFP methods as here below:
I stopped the injectable to get pregnant due to the influence made by my husband and few neighbors. Following the cessation of the injectable, I was on normal menstrual period for one year and half. Finally, I got pregnant and faced no problem during the whole pregnancy period until I gave birth at the health center. (IDI7)
Another woman also pointed out that the husband’s disapproval was one of the reasons for the early removal of Implanon as:
“ … My intention is to use Implanon for 3 years; however, my husband was against my intention. He even fought with me and bitten my hands.” (IDI10)
Seeking more children was also found to be the other reason for the early removal of long-acting family planning methods. The majority of women desired two to three children while some of them desired more than five children.
One of the participant mentioned seeking more children as a reason for early removal as:
“ …. Even though I took Implanon according to my personal choice and voluntary base, I have removed it because of seeking more children.” (IDI2)
Women Perception About Long-Acting Family Planning Methods
Although majority of participants had information about different types of family planning method, they have various perception or fear on its use. Delayed fertility after removal was one of the most frequently stated fear by the clients. On the other hand, some others perceived as it could affect their health status. Some other participants also perceived that these family planning methods require eating special food and drinks. There were also a number of participants who had fear of procedures, paralysis, death, medical illness, and discomfort during sex. Some participants mentioned that there were resistance to early remove LAFP by health workers even when requested to remove.
Participant who had fear to use LAFP explained as:
I feared using loop because of the information that was circulating in the community … women who used loop as birth control developed paralysis …. which refrained me from using it. (IDI 1)
Another participants who had fear to use LAFP also explained as:
“IUD is not good during sex. It can be lost in the body and may cause foul smelling vaginal discharge”. (IDI 6)
Implant can move in your body from arm to leg, it can stab you, and you ’can’t work while the implant is in your arm. It is painful on insertion and removal and challenging to do hard works such as cooking food and washing clothes. Health workers are not interested in removal within six months after insertion. (IDI 10)
Participant Suggestion and Future Plan
Most women identified different sorts of opinion regarding their future plan on family methods. The most frequently mentioned suggestions were to choose family planning methods without the influence of health professionals and to delay contraceptive use until the first child delivery.
One participant has the following suggestion:
Information regarding family planning needs adequate counseling. However, health professionals do not provide adequate information. Most of the time, women obtain information from neighbours and become worried. (IDI10)
Other participants had further suggestions; for example,
one interviewee said:
I visited health facility three months after Implanon insertion to take Implanon off, but the health professional did not agree to remove it before six months. (IDI8)
Discussion
Family planning is a process which usually involves a discussion between a woman, a man, and a trained service provider by focusing on family health and the desires of the couple to either space birth interval or limit their family.12 There are two types of family planning methods: short acting and long-acting and permanent methods. Long-acting methods can be used for both limiting and spacing childbirth, while permanent methods are used only for limiting childbirths. Short-acting methods are suitable for women who want to space childbirths.13
This study found that there were misunderstanding, fear and rumors raised by women about each method, and mistrust towards the providers on removal. They had also expressed their concern on the return of fertility after using long-acting family planning methods. However, most of the participants had information about different types of family planning methods, which is consistent with similar research conducted in Arba Minch town.7 Our findings were also substantiated by another study from Adigrat town14 and Nekemte town.15 But, the findings of demographic and health surveys of Ethiopia showed that women of reproductive age know less information on family planning methods.16,17 The possible reason for these differences could be the frequent promotion or advertisement of the methods by various stakeholders.
Some participants believed that the implant could move freely in the body and get lost, and they also thought that implant and IUCD cause illness. The result of this study is consistent with the study conducted in the Wolaita Zone, Southern Ethiopia.18 This might be due to the presence of rumors circulating in the community regarding long-acting family planning methods.
This study identified side effects as the main reason for the early removal of LAFP, which is consistent with other similar studies.9,19–26 The most frequently mentioned side effects were heavy and irregular menses, weight change, and dizziness. This finding is similar to studies conducted in Ethiopia and other low-income countries.19,21,24 The reason for discontinuation may be due to inadequate counseling by health care providers and lack of family support.
In this study, desiring more children was recognized as one of the common reasons for the early removal of LAFP methods which agrees with other similar studies.27–30 Similarly, another study conducted in southern Nigeria showed that looking for more children causes a high rate of early removal of Implanon.31 However, according to a study conducted on fertility, family size preference and contraceptive use in Sub-Saharan Africa from 1990 to 2014, fertility levels and family size preference declined while contraceptive use increased particularly in the Southern and Eastern Africa. In this context, increased female labour force participation, modernization, and urbanization might be major potential causes of fertility decline in some region of Sub-Saharan Africa.32
According to the finding of this study, although husband involvement in the decision making process of family planning use is essential in reproductive life, most of them rarely participate in the family planning decision-making process and use. Another study also showed that there was no relationship between contraceptive use continuation and husband support.33 In contrast, a study conducted in Indonesia showed that husbands support the utilization of long-acting contraceptive methods.34,35 In Ethiopia, the main barriers of husband’s involvement in family planning methods are lack of appropriate information, inaccessibility of family planning services, the attitudes of men towards family planning, perceived fear of side-effects, cultural or religious oppositions and desire for more children.36–39
This study explored problems with a health care provider counseling process. Women informed that they did not discuss their concerns freely with health care provider which agrees with other similar study.7 Moreover, another study found that poor adherence to the existing family planning guideline, providers’ religious beliefs, and desire among providers to deliver services based on prior knowledge rather than protocols and guideline are some of the barriers of effective family planning utilization.40 This might also be a reason for the early removal of long-acting family planning methods.
Limitation of the Study
Participant responses may have been influenced by the interviewers’ own biases and the presence of the interviewer may have in turn affected the participant response. The results represent only the experiences of those interviewed; hence, are not generalizable and transferable. Translation and interpretation errors may exist in these data, even though every effort was made to assure fidelity to the context during translation, analysis and interpretation. There may have also been an issue of recall bias among participants. However, efforts were made to hire and train interviewers who were well versed in qualitative research methods, knowledgeable in how to probe for more accurate recall, comfortable with the sensitivities of the subject matter, and cultural norms.
Strengths of the Study
In this study, we used IPA design which helped us know a detailed in-depth experience and perceptions of women who discontinued LAFP methods before the expected time. We also used open-ended structured interview guide that permitted the participants to talk freely so that a well versed interviewer could gather rich data from participants. As a result, our research found a number of previously unidentified myths and misconceptions about LAFP methods that had been largely circulating in the community. And, these could be a basis for future implementation of intervention by health professionals and other stakeholders.
Conclusion
Side effects, desired to have more children, and the husband’s opposition are the most important reason of early removal of LAFP methods. Furthermore, there are misunderstanding, fear and rumors raised by women about each method. Hence, greater public awareness on family planning methods should be delivered to change community perception on LAFP methods. Further mixed method research with a large sample size is required to better understand why women discontinue LAFP in this particular context.
Abbreviation
EDHS, Ethiopian Demographic Health Survey; FMOH, Federal Ministry of Health.
Data Sharing Statement
Data translated to English and coded were uploaded as Supplementary File 2.
Before conducting the study, ethical approval was obtained from the ethical review committee of the College of Health Science and Medicine, Wolaita Sodo University, under the Ref No: CHSM/ERC/113 (01, February, 2020). Moreover, the official permission letter was obtained from Bedesa health center. Informed written consent was obtained from every participant. This study was conducted in accordance with the Declaration of Helsinki. The purpose of the study was explained to all participants. The information obtained was kept confidential. The name of any participant was not written so that the collected data remained anonymous. We interviewed women in a private room to maintain participants’ privacy. The participants had the right to interrupt their participation at any time without any cost.
Consent for Publication
Not applicable
Acknowledgment
We would like to acknowledge Health Education Partnership Initiative (HEPI) project office of Addis Ababa University and Wolaita Sodo University for providing materials support.
Author Contributions
MS, AA, LK, MW, HC, and KT were involved in the conception, study design, execution, acquisition of data, analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content. TT, KT, MA, GM, and ZZ were involved in study design, execution, acquisition of data, analysis, interpretation, drafted and final manuscript writing. All authors reviewed and agreed on all versions of the manuscript before submission, agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Not available.
Disclosure
The authors declared that we have no conflicts of interest.
References
1. Royston E, Armstrong S. Organization WH: preventing maternal deaths: world Health Organization; 1989.
2. Kesetebirhan A. National Guideline for Family Planning Services in Ethiopia. Federal Democratic Republic Ethiopia, Ministry Health. 2011.
3. Hancock NL, Stuart GS, Tang JH, Chibwesha CJ, Stringer JS. Renewing focus on family planning service quality globally. Contraception Reprod Med. 2016;1(1):10. doi:10.1186/s40834-016-0021-6
4. Gebremariam A, Addissie A. Intention to use long acting and permanent contraceptive methods and factors affecting it among married women in Adigrat town, Tigray, Northern Ethiopia. Reprod Health. 2014;11(1):1–9.
5. Bongaarts J, Cleland J, Townsend JW, Bertrand JT, Gupta MD. Family planning programs for the 21st century. New York: Population Council. 2012;21.
6. Kebede A, Abaya SG, Merdassa E, Bekuma TT. Factors affecting demand for modern contraceptives among currently married reproductive age women in rural Kebeles of Nunu Kumba district, Oromia, Ethiopia. Contraception Reprod Med. 2019;4(1):1–15. doi:10.1186/s40834-019-0103-3
7. Utaile MM, Debere MK, Nida ET, Boneya DJ, Ergano AT. A qualitative study on reasons for early removal of Implanon among users in Arba Minch town, Gamo Goffa zone, South Ethiopia: a phenomenological approach. BMC Women’s Health. 2020;20(1):1–7.
8. MCdowel M. A mixed-methods study of factors associated with implanon removal in ethiopia; 2017.
9. Ethiopia Csao: EFDRE. ETHIOPIA Demographic and Health Survey 2016 Key Indicators Report. In. Edited by CSAE; 2016.
10. Creswell JW, Creswell JD. Research design: qualitative, quantitative, and mixed methods approaches: sage publications; 2017.
11. Pietkiewicz I, Smith JA. A practical guide to using interpretative phenomenological analysis in qualitative research psychology. Psychol j. 2014;20(1):7–14.
12. Bekele D, Fantahun M, Gutema K, Getachew H, Lambiyo T. Family Planning Module. Ethiopian Health Center Team Hawassa Univ USAID. 2003.
13. Creanga AA, Gillespie D, Karklins S, Tsui AO. Low use of contraception among poor women in Africa: an equity issue. Bull World Health Organ. 2011;89:258–266. doi:10.2471/BLT.10.083329
14. Gebremariam A, Addissie A. Intention to use long acting and permanent contraceptive methods and factors affecting it among married women in Adigrat town, Tigray, Northern Ethiopia. Reprod Health. 2014;11(1):24. doi:10.1186/1742-4755-11-24
15. Hambissa G, Sena L, Hiko D, Merga H. Intention to Use Long Acting and Permanent Contraceptives Methods and Associated Factors among Family Planning Clients in West Ethiopia. Fam Med Med Sci Res. 2018;7(228):2. doi:10.4172/2327-4972.1000228
16. Gebremedhin AY, Kebede Y, Gelagay AA, Habitu YA. Family planning use and its associated factors among women in the extended postpartum period in Addis Ababa, Ethiopia. Contraception Reprod Med. 2018;3(1):1. doi:10.1186/s40834-017-0054-5
17. Tarekegn SM, Lieberman LS, Giedraitis V. Determinants of maternal health service utilization in Ethiopia: analysis of the 2011 Ethiopian Demographic and Health Survey. BMC Pregnancy Childbirth. 2014;14(1):161. doi:10.1186/1471-2393-14-161
18. Meskele M, Mekonnen W. Factors affecting women’s intention to use long acting and permanent contraceptive methods in Wolaita Zone, Southern Ethiopia: a cross-sectional study. BMC Women’s Health. 2014;14(1):109. doi:10.1186/1472-6874-14-109
19. Utaile MM, Debere MK, Nida ET, Boneya DJ, Ergano AT. A qualitative study on reasons for early removal of Implanon among users in Arba Minch town, Gamo Goffa zone, South Ethiopia: a phenomenological approach. BMC Womens Health. 2020;20(1):2. doi:10.1186/s12905-019-0876-1
20. Aminu MB, Dattijo LM, Shehu AM, Kadas SA. Factors responsible for discontinuation of long-term reversible contraceptives in a tertiary facility in Northeastern Nigeria. Port Harcourt Med J. 2019;13(2):67.
21. Nageso A, Gebretsadik A. Discontinuation rate of Implanon and its associated factors among women who ever used Implanon in Dale District, Southern Ethiopia. BMC Womens Health. 2018;18(1):189. doi:10.1186/s12905-018-0678-x
22. Tadesse A, Kondale M, Agedew E, Gebremeskel F, Boti N, Oumer B. Determinant of Implanon discontinuation among women who ever used Implanon in Diguna Fango District, Wolayita zone, southern Ethiopia: a community based case control study. Int j Reprod Med. 2017;2017. doi:10.1155/2017/2861207
23. Adeagbo O, Mullick S, Pillay D, et al. Uptake and early removals of Implanon NXT in South Africa: perceptions and attitudes of healthcare workers. South African Med J. 2017;107:10. doi:10.7196/SAMJ.2017.v107i10.12821
24. Staveteig S, Mallick L, Winter R. Uptake and discontinuation of long-acting reversible contraceptives (LARCs) in low-income countries.In:DHS Analytical studies No 54. Rockville, Maryland, USA: ICF Internation; 2015.
25. Burusie A. Reasons for Premature Removal of Implanon among Users in Arsi Zone, Oromia Region, Ethiopia, 2013. Reprod System Sexual Disorders. 2015;04:01.
26. Birhane K, Hagos S, Fantahun M. Early discontinuation of implanon and its associated factors among women who ever used implanon in Ofla District, Tigray, Northern Ethiopia. Int J Pharma Sci Res. 2015;6(3):8.
27. Mesfin Mamo Utaile MKD, Etsehiwot Tilahun N, Dube Jara B, Amsale Tekle E. A qualitative study on reasons for early removal of Implanon among users in Arba Minch town, Gamo Goffa zone, South Ethiopia: a phenomenological approach. BMC Women’s Health. 2020;20(2):4–7. doi:10.1186/s12905-019-0874-3
28. Kalayu birhane SG. Early discontinuation of implanon and its associated factors among women who ever used implanon in Ofla District, Tigray, Northern Ethiopia. Int J Pharma Sci Res. 2015;6(3):544–551.
29. Alem Gebremariam AA. intention to use long acting and permanent contraceptive methods and factors affecting it among married women in Adigrat town, Tigray, Notrhen Ethiopia. BMC Reprod Health. 2014;11:24.
30. Hbtamu Zerihun AB, Worku A, Desta E. HailemariamTafesse, Hika Dinssa, Ashenafi Asmelash. Implanon removal experience of women in Butajira, ethiopia. EthipJhealth Dev. 2015;29(3):177–180.
31. Ojule JDOE, Enyindah CE. Experience with Implanon in southern Nigeria. J Med Med Sci. 2012;3(11):710–714.
32. Odimegwu CO, Akinyemi JO, Banjo OO, Olamijuwon E, Amoo EO. Fertility, family size preference and contraceptive use in sub-Saharan Africa: 1990-2014. Afr J Reprod Health. 2018;22(4):44–53. doi:10.29063/ajrh2018/v22i4.5
33. Harzif AK, Mariana A, Malik DM, Silvia M, Lovita BT. Factors associated with the utilization of long-acting reversible contraceptives among family planning clients at the Pameungpeuk Rural Hospital, Indonesia. F1000Research. 2018;7:1891. doi:10.12688/f1000research.15755.1
34. Bewket Zeleke L, Gella MM, Almaw Derseh H, Alemu AA, Abebe Kassahun E, Gelaw KA. Utilization of Long-Acting Contraceptive Methods and Associated Factors among Female Health Care Providers in East Gojjam Zone, Northwest Ethiopia, in 2018. Biomed Res Int. 2019;2019:5850629. doi:10.1155/2019/5850629
35. Mukamuyango J, Ingabire R, Parker R, et al. Motivational interviewing to promote long-acting reversible contraception among Rwandan couples wishing to prevent or delay pregnancy. Am J Obstet Gynecol. 2019. doi:10.1016/j.ajog.2019.11.1280
36. Nuzzo JB, Meyer D, Snyder M, et al. What makes health systems resilient against infectious disease outbreaks and natural hazards? Results from a scoping review. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-7707-z
37. Kassa M, Abajobir AA, Gedefaw M. Level of male involvement and associated factors in family planning services utilization among married men in Debre markos town, Northwest Ethiopia. BMC Int Health Hum Rights. 2014;14(1):1–8. doi:10.1186/s12914-014-0033-8
38. Walle Y, Alamrew Z. The current states of male involvement on family planning and factors correlated with among male factory workers in Bahir Dar City. Am J Public Health Res. 2014;2(5):188–197. doi:10.12691/ajphr-2-5-2
39. Gizaw A, Regassa N. Family planning service utilization in Mojo town, Ethiopia: a population based study. J Geography Regional Planning. 2011;4(6):355–363.
40. Abate A. The Regulation and Supervision of Interest-Free Banking in Ethiopia. Addis Ababa University; 2015.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.