")
Back to Journals » International Journal of Women's Health » Volume 15
Listeriosis During Pregnancy: Maternal and Neonatal Consequences—A Case Report
Authors Rovas L, Razbadauskas A, Slauzgalvyte G
Received 1 December 2022
Accepted for publication 8 April 2023
Published 6 May 2023 Volume 2023:15 Pages 695—699
DOI https://doi.org/10.2147/IJWH.S399542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Marleen van Gelder
Linas Rovas,1,2 Arturas Razbadauskas,1 Gabriele Slauzgalvyte2
1Klaipeda University, Klaipeda, Lithuania; 2Department of Obstetrics and Gynecology, Klaipeda University Hospital, Klaipeda, Lithuania
Correspondence: Linas Rovas, Klaipeda University Hospital, Klaipeda University, H. Manto g. 84, Klaipeda, 92294, Lithuania, Tel +37069843875, Email [email protected]
Abstract: Listeriosis is a rare but extremely dangerous infection for both mother and fetus. This pathogen can spread in humans’ bodies by consumption of contaminated food. The main high-risk groups of people for being infected are immunosuppressed and especially pregnant women. We present a case of materno-neonatal listeriosis illustrating that empiric antimicrobial therapy of chorioamnionitis during labor and neonate postpartum can also cover listeriosis which was not diagnosed prior to obtaining cultures.
Keywords: listeriosis, chorioamnionitis, pregnancy, neonatal infection, antimicrobial treatment
Introduction
Listeriosis has an incidence estimated at 36 cases per million per year.1 In Lithuania, it is reported that between 2010–2016 47 listeriosis patients were diagnosed, including 9 (19%) deaths.2 This pathogen can spread in humans’ bodies by consumption of contaminated food.
Listeria monocytogenes has approximately 13 serotypes, but only a few of them are involved in the majority of human listeriosis outbreaks and sporadic cases.3 The ability to resist external environmental factors allows the bacteria to multiply at different temperatures (0.4–45 °C) in raw milk/vegetables, frozen corn, French-style cheese, poultry, or fish products.4,5 Listeria can be inactivated by chlorine-containing disinfectants or direct sunlight. There are two forms of listeriosis: invasive and noninvasive. Noninvasive listeriosis does not cross the gastrointestinal barrier.6 Outbreaks are increasingly recognized, predominantly in upper-income countries where infection is more readily diagnosed, where strain typing is performed by whole-genome sequencing, and where existing surveillance programs facilitate early recognition, which allows for identification of outbreak-linked cases and definitive attribution of the source.5
Although listeriosis is rare, it is a serious condition for pregnant women.7 The pregnancy risk of being infected by listeriosis is more than 18 times higher than in the general population.3 An infectious dose of 104–106 organisms/gram of ingested product causes the disease.4 Incubation period is from 24 hours to 70 days.4 Listeria can spread via the bloodstream and result in febrile bacteremia. The infection is usually asymptomatic, but it can occur as influenza, gastroenteritis, neurolisteriosis, sepsis, or even meningitis with brain abscesses. In immunocompromised people, such as pregnant women, listeria may cause endocarditis, cerebritis or rhombencephalitis.7,8 Infection can affect both the mother and fetus. Vertical transmission can occur transplacentally to the fetus or via birth through an infected vaginal canal.4 Pregnant women mostly get sick in the second or third trimester, but it can be diagnosed in the first trimester as well.9 Infection is considered a high risk for the fetus and can lead to abortion, stillbirth, or delivery of an ill infant with damage of the central nervous system.4,7 Perinatal outcome depends on the point in pregnancy when the infection occurs. Perinatal fatality rate of listeriosis is around 20–30%.10 Most common symptoms of maternal listeriosis are fever, cough, pain in the abdomen or pelvic area, myalgias, and arthralgias.10
The recommended therapeutic agents of choice for suspected or diagnosed listeria monocytogene infection in pregnancy include ampicillin, penicillin and amoxicillin.1 Timely recognition and appropriate antibiotic therapy can prevent poor outcomes.
Case Report
A 26-year-old nulligravida woman at 36 weeks and 6 days gestation presented to Obstetrics and Gynecology emergency department at Klaipeda University Hospital, Lithuania with irregular uterine contractions and fever of 37.7 °C. On the day before arrival at the hospital, the patient complained of chills, cough, and fever up to 37.9 °C; she was administered paracetamol. Her prenatal period was complicated by gestational diabetes mellitus and obesity; 3 months before arrival the patient had asymptomatic SARS-CoV-2 infection. Fetal movements were felt normally.
On arrival, she was noted to have a heart rate of 92 beats per minute (bpm). CTG (fetal cardio-toco registration) was recorded. Exam showed a normal variability with a fetal tachycardia of 175 bpm. After assessment of the patient’s objective and subjective symptoms, paracetamol and natrium chloride infusion therapy were prescribed. Laboratory analysis consisting of complete blood count, C-reactive protein (CRP) count and group B streptococcus bacteria (GBS) test were conducted. Test results of blood count presented leukocytosis (16.81 x 109 /L) and thrombocytopenia (116 x 109 /L); CRP was 102.7 mg/L; GBS was not found. Based on laboratory test results and clinical symptoms, the patient was diagnosed with chorioamnionitis and initiated on empiric triple antibiotic therapy with ampicillin, gentamicin and metronidazole.
Five hours after arrival, she went into labor spontaneously. During birth, the patient was noted to have a fever up to 38.4 °C and the run-off amniotic fluid was contaminated with meconium. After 4 hours of labor, the patient delivered a female premature infant by natural vaginal delivery, weighing 2850 g, with Apgar scores of 8 and 8 at 1 and 5 minutes, respectively. Umbilical artery blood gas pH was 7.37, BE was 13 and blood lactate concentration was 1.25. The placenta delivered spontaneously without any complications and was taken for pathohistological examination. The surface of the placenta was covered with micro abscesses. Placental cultures were taken as well. Macroscopic histologic placenta examination of the placenta showed yellow-coloured, up to 1.5 cm diameter micro infarcts. Immunohistochemical examination revealed intervillous abscess, diffuse intensive inflammation with microabscesses in the chorionic decidua, placental chorionic plate and umbilical cord. Results of analysis are shown in Figures 1 and 2.
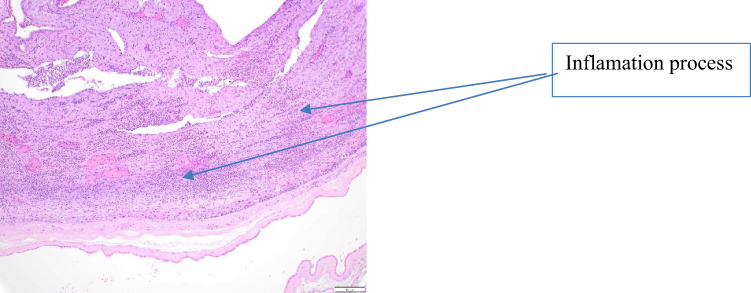 |
Figure 1 Diffuse intense inflammation with microabscesses in placental chorionic plate. HE x200. Small foci of purulent villitis in which groups of acutely inflamed villi are surrounded by fibrin and an acute peri-villous and intervillous inflammatory exudate. |
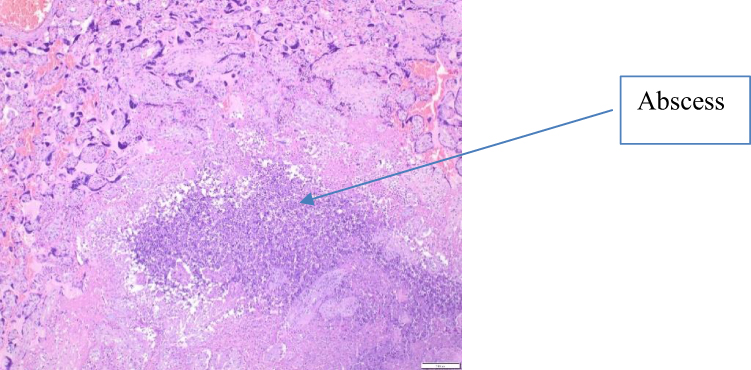 |
Figure 2 Intervillous abscess. HE x200. The abscess is surrounded by a rim of giant cells and palisaded histiocytes. |
The placental cultures were positive for listeria monocytogenes, escherichia coli and bacteroides vulgatus. No microorganism grown from the patient’s blood culture was detected.
During the postpartum period, the patient was treated with intravenous ampicillin 8 g per day, gentamicin 240 mg per day and peroral metronidazole 1500 mg per day for 6 days.
After delivery the fever continued for 24 hours, meanwhile leucocytosis and CRP steadily declined and reached normal levels on day 5. The patient was discharged home the sixth day after delivery based on her stable state, decreased fever and normal repeated laboratory evaluations.
After the delivery, the neonate was taken to the neonate intensive care Unit (NICU) because of her complicated state. The infant had crepitation while breathing, her skin was cyanotic and her muscle tone was low. Continuous positive airway pressure (CPAP) was initiated. Blood cultures were positive for listeria monocytogenes, sensitive to ampicillin, therefore antibiotic therapy was intended for the baby. Radiological neonate examination showed decreased pulmonary airiness. A lumbar puncture was performed. Cerebrospinal fluid (CSF) test was negative for any bacterial cultures. Blood tests revealed: CRP 239 mg/L, ALT/GPT 375 U/L and AST/GOT 413 U/L.
Neonate was diagnosed with sepsis, congenital anemia, respiratory insufficiency, and preterm birth. She was treated with intravenous ampicillin 220 mg two times a day, gentamicin 12 mg for 5 days, curosurf 480 mg and intravenous midazolam. In the beginning of treatment the infant’s condition was severe; lactate concentration in neonate’s blood rose to 5.5 mmol/L, blood artery gas pH was 7.25. Erythrocyte transfusion was performed (45 mL), infusion with 8.2% glucose, and vaminolact, calcium gluconate 10%, dobutamine and intravenous metoclopramide 1 mL for one day were prescribed. Neonate presented with edema of the throat, therefore DiGeorge syndrome was suspected, but genetic examination denied this assumption. During the treatment, newborn’s condition stabilized and edema of the throat decreased. The newborn was taken home in good condition without adverse consequences after 15 days of hospitalization.
Discussion
The diagnosis of listeria in pregnancy is often problematic, as approximately 30% of women are asymptomatic.4 Due to nonspecific clinical symptoms, it is hard to diagnose listeriosis. The gold standard for the diagnosis of maternal/fetal listeriosis is via placental or blood culture.4 In our case, the diagnosis of listeriosis was approved after taking the culture from the placenta.
Inflammatory changes in the placental tissue are common in listeriosis. In the case discussed,pathological examination of the placenta revealed an inflammatory process in the umbilical cord, chorionic plate, chorion, and decidua. With adequate treatment, listeriosis infection is not a major problem for the mother and usually outcomes are positive. Our patient received empirical treatment of chorioamnionitis with ampicillin, which stabilized listeriosis infection and the maternal condition improved rapidly.
According to the literature, neonatal listeriosis manifests commonly in the first 24–72 hours after delivery.11 This infection usually leads to sepsis or meningitis by vertical transmission from the mother.10 Neonatal listeriosis is a major cause of mortality in the newborn, but fetal demise is more common than neonatal death.12 In utero infections it can occur as inhalation or ingestion of an amniotic fluid as well as in the hematogenous transplacental way. Infected infants may have pustular lesions of the skin and pharynx, can be lethargic or hypothermic.4 It can also include respiratory distress, shock, and abnormal laboratory results.1 The outcomes of neonatal listeriosis might be worse in mothers who are not treated or inadequately treated.1
In the case described, the newborn was already born with clinical signs of infection, but the origin of the infection was unclear in the early hours. However, since empirical treatment with ampicillin and gentamicin has been applied to neonates with suspected sepsis (according to approved sepsis treatment protocols), this algorithm was successful for listeriosis infection as well.
Many experts recommend 6 g or more per day of ampicillin for treatment during pregnancy and in the postpartum period. This antibiotic regimen allows adequate intracellular penetration and maintains an adequate dose for traversing the placenta. Dosage of 2 g every 6 or 8 hours is generally given.1 A few antibiotics have been demonstrated to be active against L. monocytogenes; overall, penicillin, amoxicillin, and ampicillin are those used with the highest frequency and suggested based on guidelines or expert opinions.1 In our case, treatment with ampicillin was fast and effective for the mother, who left the hospital after 6 days in fine condition. Based on the protocols approved in our hospital, we begin empirical treatment with ampicillin, gentamicin, and metronidazole when suspecting of chorioamnionitis. This treatment is also effective for listeriosis-induced infection. We think that antibiotic therapy with ampicillin started during childbirth might have improved the outcome for the newborn.
Listeriosis infection commonly cause clinic similar to chorioamnionitis (fever, frequent pulse, uterine tenderness), therefore empirical treatment applied in case of chorioamnionitis may save both the mother and the fetus, even though the causative agent is unknown.
Conclusions
Our case demonstrates that listeriosis may appear in the third trimester of pregnancy and manifest with no obvious symptoms. It is still not clear which clinical indicators should be assessed for a possible infection. However, our study shows that the gold diagnostic standard is pathohistological analysis of the placenta, whose macroscopic examination may indicate possible listeriosis infection. Blood or placental culture have to be performed as soon as this infection is suspected. In the case analysed, the empirical treatment with ampicillin, which was started in the presence of signs of chorioamnionitis (even though the cause of the infection was unknown at the beginning), protected both the mother and the newborn from adverse outcomes. Nevertheless, the main way to protect against listeriosis infection and possible complications is prevention of the disease. Disease prevention is the key to success for decreasing listeria indices during pregnancy and regularly updated information on proper food preparation to prevent contamination and routes of infection must be available for moms-to-be.
Ethics Committee Approval and Consent for Publication
Klaipeda University Hospital, Lithuania ethics committee waived approval for this case report. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Disclosure
The authors declare that they have no competing interests.
References
1. Pagliano P, Arslan F, Ascione T. Epidemiology and treatment of the commonest form of listeriosis: meningitis and bacteraemia. Le infezioni Medicina. 2017;25(3):210–216.
2. Communicable diseases in Lithuania in 2017. Available from: http://www.ulac.lt.
3. Madjunkov M, Chaudhry S, Ito S. Listeriosis during pregnancy. Arch Gynecol Obstet. 2017;296(2):143–152. doi:10.1007/s00404-017-4401-1
4. Serventi L, Curi B, Johns R, Silva J, Bainbridge R, Gaither K. Pregnancy complicated by listeria monocytogenes: a case report and review of the literature. J Natl Med Assoc. 2022;112(4):428–432. doi:10.1016/j.jnma.2020.05.002
5. Juno T, Nevashan G, McCarthy M, et al. Outbreak of listeriosis in South Africa associated with processed meat. N Engl J Med. 2020;382:632–643. doi:10.1056/NEJMoa1907462
6. Wadhwa Desai R, Smith MA. Pregnancy-related listeriosis. Birth Defects Res. 2017;109(5):324–335. doi:10.1002/bdr2.1012
7. Colomba C, Rubino R, Anastasia A, et al. Postpartum listeria meningitis. IDCases. 2020;21:e00896. doi:10.1016/j.idcr.2020.e00896
8. Duport-Percier M, Aya A, de Tayrac R, Letouzey V, Mousty E. Meningite à listeria au troisième trimestre de la grossesse. À propos d’un cas [Listeria meningitis in the third trimester of pregnancy. Case report]. Gynecol Obstetr Fertil Senologie. 2017;45(7–8):444–446. doi:10.1016/j.gofs.2017.06.014
9. Charlier C, Disson O, Lecuit M. Maternal-neonatal listeriosis. Virulence. 2020;11(1):391–397. doi:10.1080/21505594.2020.1759287
10. Luo L, Chen X, Payne M, et al. Case report: whole genome sequencing based investigation of maternal-neonatal listeriosis in Sichuan, China. BMC Infect Dis. 2019;19(1):893–894. doi:10.1186/s12879-019-4551-9
11. Sapuan S, Kortsalioudaki C, Anthony M, et al. Neonatal listeriosis in the UK 2004–2014. J Infect. 2017;74(3):236–242. doi:10.1016/j.jinf.2016.11.007
12. Tai Y, Chi H, Chiu N, et al. Clinical features of neonatal listeriosis in Taiwan: a hospital-based study. J Microbiol Immunol Infect. 2019;53(6):866–874. doi:10.1016/j.jmii.2019.08.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.