")
Back to Journals » Patient Related Outcome Measures » Volume 11
Life After Myocardial Infarction: A Qualitative Study on Experiences of Kurdish Patients Affected by Iran–Iraq War
Authors Sepehrian E, Pooralmasi M, Abdi A , Rajati M, Mohebi S, Tavakol K , Rajati F
Received 29 May 2020
Accepted for publication 15 September 2020
Published 15 October 2020 Volume 2020:11 Pages 209—219
DOI https://doi.org/10.2147/PROM.S265124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Lynne Nemeth
Elahe Sepehrian, 1 Maryam Pooralmasi, 1 Alireza Abdi, 2 Mojgan Rajati, 3 Siamak Mohebi, 4 Kamran Tavakol, 5 Fatemeh Rajati 6
1Student Research Committee, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Critical Care and Emergency Department, Nursing and Midwifery School, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Department of Obstetrics and Gynecology, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran; 4Department of Health Education and Health Promotion, Faculty of Public Health, Qom University of Medical Sciences, Qom, Iran; 5School of Medicine, Howard University, Washington, DC, USA; 6Research Center for Environmental Determinants of Health, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Fatemeh Rajati Email [email protected]
Background: Coronary artery disease (CAD) is a major cause of death globally. Myocardial infarction (MI) secondary to CAD affects patients’ quality of life and their lifestyle. The experience of war can affect people’s perception of phenomena. Given the scarcity of information in Kurdish patients with MI, the current study was designed to explore the lived experiences of individuals after MI in Kurdish patients affected by Iran–Iraq war.
Methods: This interpretive-phenomenological study was conducted on eleven patients with MI (9 men, 2 women) at Imam Ali Hospital, Center for Heart Diseases, in Kermanshah, Iran, considering MI as a phenomenon. Data was collected by a semi-structured interview and analyzed using the Van Mannen method. We employed the Lincoln and Guba criteria to examine the credibility, confirmability, dependability, and transferability of data. MAXQDA software was used for data management. We followed the COREQ checklist to ensure rigor in our study.
Results: Four themes and ten sub-themes were emerged as (1) “changes in the quality of life” including (a) negative physical outcomes, (b) mental effects, (c) social support, (d) adopting healthy behaviors, (e) increase or decrease in self-efficiency, (f) previous experience, and (g) developing future behaviors; (2) “bodily perceptions and medical care” including (a) medical care: saving or terminating life?, (b) a new message from the heart; (3) “returning to spirituality against death” including (a) spirituality as a guiding principle, (b) accepting death as an eventual destiny; and (4) denial.
Conclusion: The results suggest that MI could change the quality of physical and mental health of the person, anywhere from deterioration to full recovery. Furthermore, the influence of spirituality and previous experience of war to overcome the complications of MI has been discussed, leading to either acceptance or denial of MI, and the consequences.
Keywords: myocardial infarction, qualitative research, phenomenology quality of life
Background
Cardiovascular disease (CVD) is the leading cause of morbidity, mortality, and disability, worldwide1 and accounts for the deaths of 7.3 million people (>30%) annually.1,2 Nowadays, CVD is becoming an epidemic because of the growing risk factors, which include obesity and diabetes.3 Over 75% of the associated death occurs in low and middle-income countries.4 In the high-income nations, the rate is much lower due to the availability of many preventive measures.5,6 In Iran, it is estimated that the disability-adjusted life years (DALY) caused by CVD will be doubled by 2025 compared to that in 2005.7
Myocardial infarction (MI), a consequence of CVD, occurs due to cardiac ischemia induced by poor or lack of blood perfusion.8 The causes of MI include a) dislodged blood clots, and embolism, b) imbalance between the demand and supply of blood to the heart tissue, c) percutaneous interventions, d) atherosclerosis induced by stents, and e) following coronary artery bypass surgery. However, the primary cause of MI is ischemic cardiac disorders.9 The severity of MI varies depending on the extent of the infarcted lesion, length of coronary artery occlusion, and the number of collateral arteries.8 Moreover, the impact of MI on patients’ life includes decreased physical activity secondary to low cardiac output, medication side effects (e.g., headache and dizziness), unemployment, stress, anxiety, and various socioeconomic issues.10–12
Despite the cardiovascular risk factors in the developed countries, the burden of the disease on patients is three times greater in low-income nations. The disparity is directly associated with the quality of healthcare services, diagnostic equipment, and treatment followed by appropriate cardiac rehabilitation programs.8 Therefore, the complications and consequences of MI are dependent on various contextual and socioeconomic factors.12 Therefore, researchers have proposed using qualitative studies to support policy making in the care of cardiac patients.13,14 The data derived from such studies will uncover new facts including the true experiences of patients with MI.15 In this context, a study conducted in 2017 examined the experiences of young men with MI within three to six months after the incident. The results uncovered three main themes: “Being less than a man”, “Facing a bleak future”, and “Life has lost its meaning”.16 Other qualitative studies in Iran have assessed the experiences of male and female elderly with CAD from which the following themes emerged: “ Having lost peace”, “Finding peace in spirituality” and “Having lost ones health and sexuality”.17–20
War as a social determinant affects the mental health among war survivors. Previous studies demonstrated the long-term effects of war and the original experience of war-trauma on post-war life. War causes the persistence of certain symptoms in some individuals, such as anxiety, depression, alcohol and drug abuse, and post-traumatic stress disorder (PTSD). In the phenomenological context, these mental health states are the normal aspects of cognitive functioning and response to a conflict situation.21
Despite the wealth of published literature, the experiences of patients post-MI have not been evaluated at all in Kermanshah, Iran, where the largest Kurdish Iranians reside who carry the bitter memories of the 8-year, Iraq-Iran war. We assumed that the Kurdish people’s memories and experience with that war may have influenced their perception of MI differently. Thus, the aim of this study was to explore the lived experiences of patients post-MI in Kermanshah, Iran.
Methods
Study Design
This qualitative study used an interpretive phenomenology to discover the patients’ experiences about a specific issue, ie, personal experience from MI. Phenomenology explores the essence of individuals’ experiences with specific issues.22,23 For the purpose of this study, we employed hermeneutic phenomenology of Van Mennen, adapted from Heidegger, with a focus on the interpretation of the participants expressed views and experiences after having suffered an MI.24,25
Participants
The research community included patients who had a heart attack. Participants were eleven MI patients (2 women and 9 men) referred to the Cardiovascular Clinic of Imam Ali Hospital (a major cardiac center in western Iran) during the prior four months in 2018. The inclusion criteria were consent to participate in the study, being physically and mentally stable, aged 30 years or older, having at least a 6-month history of post-MI, and lack of other chronic conditions including neurological disorder and musculoskeletal disease. Also, we provided anonymous written informed consent forms to the participants. The informed consent specified in advance that the data collected would be used and how they would be applied. The informed consent also included consent to publish quotes from the participants’ interviews. They reviewed the form and signed it before we enrolled them in the study. The participants were assured of the confidentiality of their information. All of the study documents were kept under lock and key and were only accessible to the authors. The face-to-face semi-structured in-depth interviews were held in a previously agreed upon place between patients and researchers. We recorded the interviews by a tape-recorder and wrote down the non-verbal gestures. The interviews lasted between 30 to 45 minutes. Both the first and second authors, who were trained in in-depth interviewing method and were graduate with a B.Sc. in public health, performed the interviews at Imam Ali Hospital in the cardiovascular meeting room and away from patients care rooms over a 2 or 3-day period. Each participant was interviewed individually, without other participants being present. Four authors coded the data. The medical and some socio-demographic variables including age, sex, ejection fraction of the heart, marital status, educational level, occupational status were extracted from patients’ medical records.
The fourth author selected the interviewees using a purposeful sampling method. Purposeful sampling allows in-depth interviews with patients that are assumed to be rich sources of information. Before the interviews, the study aim was described to the participants. So, the participants knew the researcher’s role and the reasons for the study were disclosed during the informed consent process. In the first session, both interviewers were introduced to the patients by the fourth authors to explain the reasons for the research. However, no relationship with the participants was made before the study began.
The participants did not belong to specific political or social parties and were interested in the research topic. Of the 13 primary selected patients, two of them refused to participate in the study due to having no time to interview.
The researchers were graduates of medical sciences including medicine, nursing, public health, and rehabilitation. Specific characteristics of the researchers may have an influence on data and analysis. Nevertheless, we established strict protocols to carry out the interviews and analysis of the data to reduce bias. Except for the first and second authors, other authors were faculty members. Three of them were male, and the other was female. As the main aim of researchers in the phenomenological studies was the transformation of data to the lived experience, interviewers tried to bring individual experiences into phrases and attempted to understand those experiences based on the participants’ statements. The interviews continued until it was clear that no additional concepts or themes were emerging. The sampling proceeded until data saturation.26 Disagreements were discussed by the two interviewers until consensus was reached. In addition, Boyd et al (2001) consider two to 10 participants as adequate to reach saturation27 and Creswell et al (1998) suggest “long interviews with up to 10 people” to conduct a phenomenological study.28 Therefore, the selection of the 11 patients to perform this study was adequate. MAXQDA software was used for data management. We followed the COREQ checklist to ensure the rigor in our study (Supplementary Table 1).29 Data was collected by semi-structured interviews. The interview is one of the common methods, which is conducted in structured, semi-structured, or unstructured style.30 We asked some open questions such as: “What will be in your mind when you hear the myocardial infarction?”, “What are the effects of cardiac disease on your life?”, “Compare your situation now to what you were before your MI”, and “Describe your feelings about heart disease”. We also asked “How old were you during the war?” “How did the Iran-Iraq war affect your life?” “How has your illness affected your past experiences?” This type of interview made it possible for personal experiences to be broadly and freely expressed. Essential skills for conducting interviews are paraphrasing, clarification, summarizing, and reflecting the feelings freely.30 Limited probing questions were raised during the interviews for clarification, for instance “What do you mean by this statement?”, “Please give an example”, “Why?” or “Please elaborate or explain”.
Data were analyzed using the Hermeneutic approach developed by Van Mannen (1990), under seven categories as follows:
- Narration: The data were written as narrative texts.
- Interpretation: The texts were reviewed several times to enable interpretation.
- Coding: Each statement was coded after a thorough interpretation.
- Sub-themes: Similar coded statements were categorized into sub-themes.
- Themes: Relevant sub-themes were used to form distinct themes.
- Stories: Groups of themes were combined to develop Stories.
- Assessment: We critically assessed the rigor of the stories by both the authors and an external reviewer.31
The story rigor, was assessed by Lincoln and Guba’s criteria,32 for being credible, dependable, confirmable, and transferable. We also held regular meetings to interview and consult the patients, asking them to read and check the subthemes and themes derived from the deliberations. Finally, the patients had the opportunity to confirm, clarify or reject the stated themes and concepts.
Also, additional contacts made between the story authors and patients over the subsequent four months enhanced the credibility of the statements. The dependability of the statements was checked after recording, transcribing, and analyzing the interview contents. Further, the data were analyzed for consistency following the interviews. The confirmability was established based on the objectivity level of the data. To enhance this process, we developed an audit system to record the deliberations at each session throughout the study. The transferability was addressed by carefully recording the descriptions of the patients’ lived experiences. At the end of the study we provided feedback on the findings to the participants.
Results
This study examined the lived experiences of MI patients, for which we recruited 12 voluntary participants into the study. One participant who could not continue with the study was excluded. Of the 11 participants, most of them were married (2 women and 9 men) at the ages of 47 to 74 years old (mean 52±4.5;), with the mean of 33.7±6.7 ejection fraction. (Table 1)
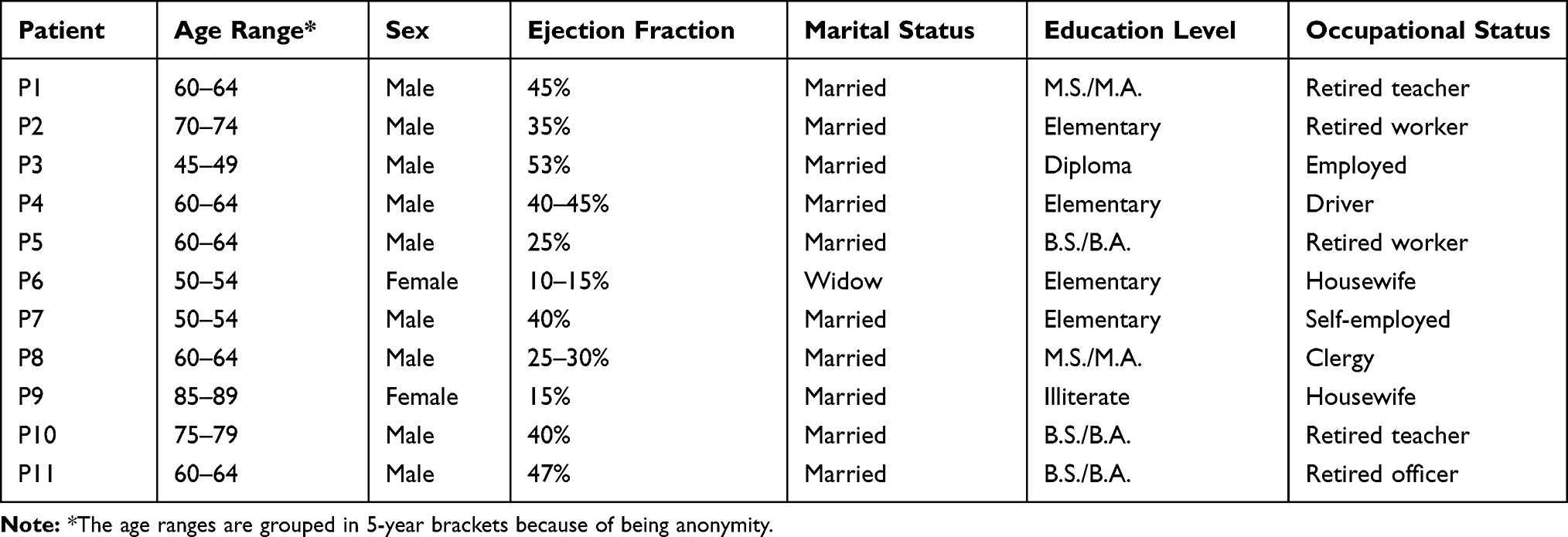 |
Table 1 Demographic Characteristics of the Participants |
Since two researchers who performed the interweaving codes of the transcripts, they were mutually compared and interpreted. Upon the completion of data analysis four themes and 10 subthemes were extracted, which were written up in details as represented in Table 2:
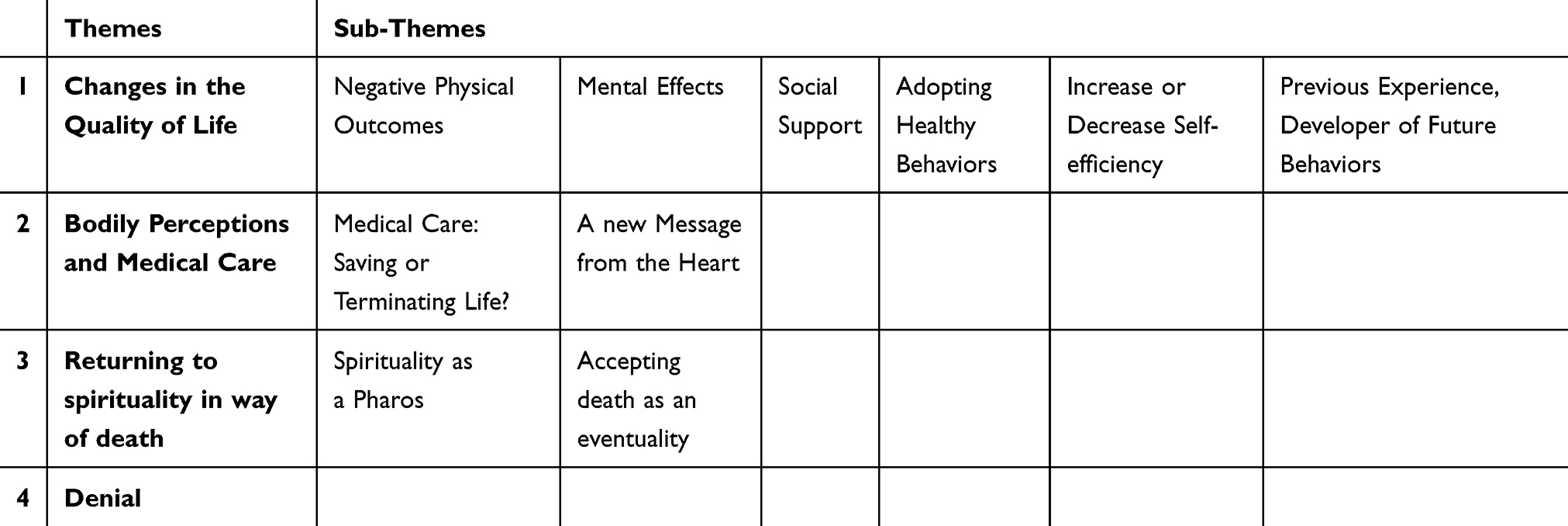 |
Table 2 Themes and Subthemes Emerged from the Interviews |
Changes in the Quality of Life
Three of the participants shared their post-MI experiences of physical, psychological, and social outcomes spanning two different perspectives. At one end of the spectrum, the experiences were linked to physical functioning, feeling of dependence, low tolerance threshold, inability to manage social relationships, aggression, need for social support, feeling of sadness, and slow the healing process. On the other end, positive changes occurred in lifestyle and healthy behaviors, resulting in improved social relationships, stress, a healthy diet, appropriate physical activity, and quitting smoking. Within the changes in the quality of life theme, the following seven sub-themes emerged:
Negative Physical Outcomes
Five participants referred to MI as a debilitating condition and stated that it restricted their ordinary physical activities. Participant 1, a 60-year-old man with a 4-year history of heart disease, stated: “I should stay away from some of the activities I wish to do, for example, being careful when doing exercises”. This participant stated that he could not walk steadily on uphill roads. Physical limitations, such as shortness of breath, choking feeling while asleep, and inability to lift and carry heavy objects were his major physical concerns. This patient also discussed some of the consequences of his physical illness. Participant 3, a 47-year old man stated: “I retired because I couldn’t earn income”. He also complained of financial hardship due to a lack of income and was concerned about becoming physically weak. Participants 4 and 5 expressed concern about their physical strength to do ordinary, daily work. They believed people with disabilities would be frustrated or saddened at the realization of losing power to work, especially heavy exercises. Another participant compared himself, physically to what he could do prior to his MI and said: “I used to go mountain climbing and had fun, but now I don’t have the power to do any of that” (Participant 8).
Mental Effects
Some participants compared themselves to their pre-MI and complained about their low tolerance for handling difficulties, mood changes, anger, depression, and the feeling of hopelessness. Participant 2 stated: When I encounter clients at work, I feel I am not the same person I was before; I am becoming more aggressive. When I reflect on my heart attack, I feel sad and wonder why I had a stroke; I get upset with myself for getting into this condition; my voice sounds sick, and my temperament with my family has deteriorated; my mood is unstable, and I cannot laugh at all. (Participant 2)
Participant 6 stated: I get into a lot of thoughts about my life; I get depressed and irritated with people around me; I would get angry quickly, and each spoken word makes my heart ache. (Participant 6)
Participant 8 shared this with us: “I get angry quickly, I feel I am more isolated than before due to my MI; I believe the disease has had a negative effect on me, with no positive outcome”. Participant 11 indicated: I get upset, depressed, very frustrated, and I always say to myself I wish I could have died then; I haven’t had a pleasant night sleep since I had my MI; I am seeing a psychologist because I feel my spirit has broken. (Participant 11)
Social Support
Participants believed that MI had impacted their social relationships and expectations of others. Some had no specific expectations of the family, but most relied on the family presence for peace, comfort, and strength in the spirit. Participant 7 said: “I am very dependent; I do not like my daughter to be away from me. When I was in the hospital, I did not even let her go as far as the hospital exit door. Participant 6 said: “I expected those around me to be nice to me”. Similarly, participant 8 said: “I expected people around me to do my job for me; while Participant 9 stated: “I would complain to them if they did not come to visit me at the hospital, bringing fruit juice for me.” In this context, Participant 5 indicated: “My social relationships have become overly hectic. This allows me not to think of problems; my surroundings have become kinder, their affection to me has increased, and my commute is longer now. For one thing, it is OK because I have ample time, which allows me to participate in my family gatherings. Unlike others, Participant 4 said: “I have neither expectation of myself nor of my wife or children.”
Adopting Healthy Behaviors
A number of participants attributed the positive changes in their diet, and physical activity as a result of MI and stated that it had persuaded them to adopt healthy diets Participant 1 said: “The stroke effects on my diet have helped me to stay away from salt, fatty foods, and unhealthy stuff. In this context, Participant 8 said” I used to eat everything before I got sick, but now I eat low-fat foods and watch my diet carefully.” Participant 3 said: “I try to avoid high-fat foods and do not do the heavy exercises, because my doctor advised me so.” Participant 5 said: Now, I have increased my hiking schedule, trying to exercise and get involved in light sports activities, but no heavy ones. I eat much less fat and red meat; rather, but I have white meat more often now than before and watch my eating habits carefully too.
Increase or Decrease in Self-Efficiency
Some participants mentioned that MI had enabled them to have better control over their thoughts, emotions, and daily behaviors. For instance, Participant 1 said: If I die of hunger, I won’t go for sausage or bologna at all. He further indicated that everyone must be their own doctor, and know what is good or bad for them. Now, I know better what my problems are; sometimes I get nervous or angry; of course, MI has had its effects on me, but I try to tolerate comments from others without getting angry quickly.
Similarly, Participant 3 said: “I try to stay as calm as I can. I try to have more peace in my life because I have no other choices.” Participant 5 said: I was involved in stressful administrative work before, but now, I wouldn’t accept them even if I am still offered similar jobs. And if a bitter thought comes to my mind, I won’t pay attention to it. Also, I am careful about taking my medications regularly and on time.
Influence of Previous Experiences on Future Behaviors
Among the participants, there were individuals who had gone through difficult and tragic life events. These experiences included the Iran–Iraq War, and the related stresses on themselves, families, and relatives. We founded that war experience affects the patients’ coping strategies. These experiences had various effects on the participants, some of which led them to be more self-dependent than before. In fact, they used war experiences as a pattern to deal with their MI. An example of this was a participant who had first-hand involvement in the war and took the opportunity as a source of developing resistance against hardships and illnesses later in life. In this context, Participant 1 shared the following views: Emotionally, a person who is ready will take it easy with any disease. But if the person is mentally weak, he may feel he is dying with a simple illness. I experienced the Iran–Iraq war, so this disease didn’t have much impact on me because I was in Halabja (an Iraqi town on the Iranian border) and I went through those painful times. The situation I am going through now is not very important to me. You have to be resilient; otherwise, you will lose the battle in life.
One participant believed that his resistance had increased as a result of his heart condition He believed he could fight the illness by following a simple plan in life. Participant 5 said: I try to stop the disease to impact my life; I am now able to fight the disease and am not afraid, despite the eventual consequences. Everyone must have a plan to resist the disease otherwise one cannot fight back. We must overcome the disease, and don’t let the disease take over us.
Bodily Perceptions and Medical Care
Medical Care
Saving or Terminating Life? In this study, the Participants believed that physicians could play a key role in promoting or diminishing health in people with cardiovascular disease. In their opinions, doctors played a key role in patients’ survival by diagnosing the heart attack and preventing death from MI and other serious illnesses. Some patients went even further and considered medical advancements and equipment facilitated the recovery from the heart attack. They commented that unlike the old times, no one should be afraid of cardiovascular disease now with the available medical knowledge and technology. “It’s not like the old times, managing heart disease is now as simple as extracting a tooth (Participant 1).”If I had not been diagnosed correctly by the emergency physician in the first place, I would not be in great trouble today (Participant 5).” “Doctors can do miracles.”
When I had a stroke, I had a cold sweat and he grabbed my hands, I supposed, he gave me fresh spirit when he prescribed the right medication for me; Otherwise, I would have been dead now. (Participant 9)
A New Message from the Heart
Unlike most ordinary people who have positive thoughts about the word “heart”, patients with heart disease have conceptualized the word “heart” as a new term, calling it a heavy, stressful, and distressing word that is reminiscent of the hard days they had in their lives. “When I hear the word ‘heart’, I subconsciously experience a strange stress in me.” (Participant 1) ”I also feel very sad when I hear the word stroke.” (Participant 2). “Similarly, a heart attack has become a heavy stressful word to me” (Participant 7).
Returning to Spirituality
Spiritual Guidance
Some of the participants used certain words and phrases in describing their relationship with God before and after their heart attack, such as “God willing”, “thanks to God”, “trust and leave it to God”, “divine experimentation”, “submission to divine judgment”, “trust in God”, “rely on the sacred faith”, “God forgives”, “miracles happen”, and “essence of life”. Many of the participants believed in God and resorted to Him under difficult circumstances, and regarded God as the ultimate source of support. Participant 1 stated: “we must leave everything to God because if one believes in God, He will save that individual from all perils. We have to trust God and leave the rest of our health affairs to physicians. “After the illness, I am very thankful to God” (Participant 1).
Thank God I didn’t need anything else for my heart attack; it was a miracle that I didn’t need a balloon or stent. I believe whatever God wishes, that will happen. I trusted God’s will and I called upon the Imams (holy persons in Islam), asking them to save me. After the stroke, I was thankful to God, because He is our Creator, and all our body parts are given to us by Him. I feel like it was a divine test for me and I came out of it successfully. (Participant 3)
Accepting Death as an Eventual Destiny
After a stroke, most participants felt they were closer to death than ever before. Some tried to think about death more than before their MI, and dreamed of life after death. They thought of death as a reality that would eventually happen to everybody. “When I had my chest pain, I thought I was going to die right away” (Participant 2).
I believe everyone goes through the experience of death. One day we are born and another day we will die; so, we are in God’s grace. I only prayed to God when I was sick and prepared myself for death, but thank God I was allowed to survive. I didn’t think death was really that close, but now I say that death is very close and will happen to everyone. Death is so much easier to fit into our mind, and the moment that a cup is filled (Persian proverb: when the path of life is over), be rest assured that there is no escape from death. After the stroke, my belief of death as a reality strengthened and I prayed to God to grant me the opportunity to serve the people honestly and enjoy life after death. (Participant 3)
“I am now thinking more about the next life hereafter because I know it’s our destiny, which is the same for everyone” (Participant 8). “I am afraid of death; I always say I will die soon” (Participant 7).
Denial
While most participants accepted their illness by changing their lifestyle and tried to live a healthy life, some denied their illness and did not cope with the resultant psychological stress they experienced. “My wife says you had a stroke; you have to be careful; you don’t have to do heavy work; do not eat most foods; try to do exercise” (Participant 10). I do not feel anything unusual other than a little shortness of breath, so it is unlikely that I have a heart problem; I do not see myself as being sick” (Participant 10). “Where’s the heart? What is heart disease anyway? The family wanted to take me back to the hospital some time ago, but I don’t have any problem” (Participant 9). Others commented on the unexpected or expected heart attack: “I had no high blood pressure or fat in my blood, and I always went for a walk; so, I don’t know why I had a stroke (Participant 5).” After my husband died, I was very sad, depressed and I was expecting it to happen to me too” (Participant 6).
Discussion
This study explored the lived experiences of 11 Iranian patients after a heart attack. To our knowledge, this is the first study to evaluate the effects of the Iran–Iraq war on post-MI patients One of the most important results we observed was “changes in the quality of life (QoL) of the participants”, that happened for many reasons. The changes included: physical disorders, mental effects of the disease, and changes in social life and interactions with others. Most patients explained diets low in fat, low in salt, and high in vegetable. Heo et al33 offered multiple definitions for QoL in the opinion of people with heart disease. The definition covers the capability of getting engaged in physical and social activities, feeling happy, and continued relationships with others. A meta-analysis of 30 qualitative studies, entitled “Lived experiences of people with heart failure” “A narrative review showed” showed that cardiovascular disease caused various life issues including social isolation, living with the fear of death and pain, and losing control on various personal aspects of life. All of these side effects collectively reduce the QoL in patients with heart disease.34 Changing in lifestyle and adopting a range of coping strategies were emerged in previous studies conducted among patients affected by MI.35 Coping strategies define as specific behavioral and psychological efforts, that individuals employ to master, tolerate, reduce stressful events. In our study, patients adopted some strategies to deal with their new lifestyle such as trying to avoid stressful situations and to keep calm.
The mental effect was another issue that emerged from our analysis. It took the form of sadness, anxiety, depression, and despair. Staniute et al36 confirmed that some mental symptoms, such as depression and anxiety are the determinants of decreased QoL in patients with CAD. Studies showed that anxiety is an important determinant of each non-adherence in myocardial infarction.37 In contrast to our study, some patients after MI had reported that they found positive consequences, new life values, and hopes in the future.38
Relying on others, ie, “social support” was one of the main consequences of the current study. The participants were often in the spotlight of their families and were supported by them; so they tend to be dependent on their care more than before. A meta-analysis shows in Post-MI patients, lack of social support are more likely to increase mortality and morbidity, with an odds ratio of 2.0 to 3.0. This impact was marked by depressing, indicating an inverse interaction between social support and mental issues.39 This could hypothesize for future qualitative studies whether the lack of perceived social support in post-MI patients could be the result of depression that disables patients to accept support. However, some post- MI patients could not carry out self-care because of the disease severity, and patients receiving a low level of support are characterized by a lower level of self-care than patients who had a high level of support.40 Our result regarding seeking social support was in line with the study conducted by Jones et al (2019) among African American women patients with MI.41 In contrast, women in another study experienced only tangible support and a lack of emotion after MI.42 Further, it appears that in Kurdish family-centered culture, people are used to paying more attention to their sick family members, and the care is known to be effective for patients with chronic than those with acute conditions.43 So, such results are not surprising in previous studies in Iran, given that good family support always is available in Iranian culture. Further studies are needed to evaluate this assumption.
In this study, the participants learned about the consequences of a heart attack, which led them to adopt healthy behaviors and positive changes in lifestyle. They remarked that they had gained on self-efficacy compared to what they knew of themselves before. Other qualitative studies also show that patients take responsibility for lifestyle changes after MI.44 For adaptation, lifestyle changes are required, which are associated with both mental fascinators and physical barriers. The fascinators include positive physical feedback, interpretation of the disease in patients’ viewpoint (opportunity to heal or not), identifying the risk factors, and developing self-management of the symptoms. Lack of knowledge, and considering low or no value in changes have been noted as the barriers.45 Other important factors accounting for positive changes in patients are their relationships and communication skills with healthcare providers.46 However, initiating adaptation and smooth lifestyle changes in socioeconomic, demographic, and cultural perspectives require careful planning and learning preventive measures from healthcare providers that fit the uniqueness of each individual patient.4748 In the current study, we concluded that previous experience would impact on coping strategies, including exploration and initial strategies through strategy refinement. Our results confirm that post-MI patients used coping strategies such as keeping calm, which is in turn affected by previous experience regarding the Iran–Iraq war.
The findings of this study demonstrated that the participants regarded the healthcare providers as their life savers and were pleased that the cardiovascular facilities were generously available to them. In contrast with our results, patients with heart disease are distressed and fearful when the healthcare facilities and medications are not available.49 This notion may arise from the confidence and trust that patients have in their healthcare providers, which is an essential aspect of convincing patients to adhere to the treatment and follow-up plan.49 In Iran, public health services are available, such as general hospitals, outpatient clinics, and private practice medical offices for many patients including those with cardiac conditions. However, there are problems with the distribution or with inadequate healthcare equipment in certain regions.50 Further, there is evidence to suggest that the private healthcare system is steadily growing in Iran.51,52 However, some patients are not satisfied with the services, depending on their location and/or economic status.
In our study patients found a new concept from the heart. Hutton et al (2007) showed that patients had an experience of changing in self-image after MI.35 According to the illness perception model, these changes can be interpreted that cardiovascular disease categorized as a chronic condition, mostly needed long-term medical care.53
Lastly, spirituality is an important factor in Iran for patients with MI, which helps them cope better with the condition. In this respect, a qualitative study was conducted in Iran by Shahrbabaki et al in 2017, investigating patients’ spirituality and coping.53 In that study, the patients’ ideas were categorized as “religious beliefs” with such the sub-categories of “inner faith” and “search for meaning” and “connection to God as a supreme power” (with subcategories of seeking healing through supplication and rituals”, “worship as a barrier to the flood of problems”, and “submission to and trust in God”).54 Additional studies have also documented the role of spirituality in dealing with chronic diseases in Some communities.55 However, spirituality positively contributed to better QoL in post-MI patients in studies conducted outside Iran.17 Patients with MI need to have a peaceful and calm living environment to be able to live without symptoms. In this context, spirituality is a practical approach to achieve this goal,56 because it provides strengths to the patients to strive and overcome the negative aspects of the disease.57
Study Limitations
This study had certain limitations. First, interviewing patients with comorbidities, such as cancer was not easy. Second, some patients had forgotten their experiences about the Iran–Iraq war due to the passage of time. Despite the limitations, this study is the first of its kind to report on patients with MI in the Kurdish population that had also experienced the Iran–Iraq war.
Conclusions
This study provided qualitative evidence that patients’ lived experience post MI could impact their lifestyle, perceptions about their body and the health care system. War as a previous experience played an important role in illness perception in post-MI patients. The study demonstrated that the illness leads the patients to seek spiritual motivation to overcome their stressors. Denial to overcome stresses also observed in some patents. It is important that healthcare practitioners have a realistic idea about the patient’s perceptions and experiences with their disease in order to adopt their health behavior when they are away from the healthcare institutions. We also recommend that further qualitative and quantitative studies be conducted to explore and develop creative approaches to enhance the quality of life in patients with prior heart conditions, such as heart failure and MI.
Abbreviation
MI, myocardial infarction.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The study was approved by research ethics committee of Kermanshah University of medical sciences, Kermanshah, Iran ID #: KUMS.REC.1395.32.
Consent for Publication
All the authors and the Kermanshah University of Medical Sciences consented to publish the study in your journal.
Acknowledgments
The authors express their sincere gratitude for the cooperation of the patients and staffs of Imam Ali Hospital, Kermanshah, Iran. The authors wish to appreciate Kermanshah University of Medical Sciences for funding this study. This study reports the results of an approved thesis project conducted at Kermanshah University of Medical Sciences (ID #: KUMS.REC.1395.32). For data collection, we received permission from the office of Research Deputy of Kermanshah University of Medical Sciences and the administration of Imam Ali Hospital. The authors declare that they have no competing interests. This study was funded by the Office of Deputy of Research and Technology, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Kermanshah University of Medical Sciences.
Disclosure
The authors declare that there were no competing interests while conducting this study.
References
1. Aljefree N, Ahmed F. Prevalence of cardiovascular disease and associated risk factors among adult population in the Gulf region: a systematic review. Adv Public Health. 2015;2015:1–23. doi:10.1155/2015/235101
2. Gaziano TA, Bitton A, Anand S, Brahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low-and middle-income countries. Curr Prob Cardiol. 2010;35(2):72–115. doi:10.1016/j.cpcardiol.2009.10.002
3. Lavie CJ, De Schutter A, Parto P, et al. Obesity and prevalence of cardiovascular diseases and prognosisGÇöthe obesity paradox updated. Prog Cardiovasc Dis. 2016;58(5):537–547. doi:10.1016/j.pcad.2016.01.008
4. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
5. Roth GA, Johnson CO, Abate KH, et al. The burden of cardiovascular diseases among US states, 1990–2016. JAMA Cardiol. 2018;3(5):375–389. doi:10.1001/jamacardio.2018.0385
6. Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and cost of chronic diseases in low-income and middle-income countries. Lancet. 2007;370(9603):1929–1938. doi:10.1016/S0140-6736(07)61696-1
7. Sadeghi M, Haghdoost AA, Bahrampour A, Dehghani M. Modeling the burden of cardiovascular diseases in Iran from 2005 to 2025: the impact of demographic changes. Iran J Public Health. 2017;46(4):506.
8. Heusch G, Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J. 2016;38(11):774–784. doi:10.1093/eurheartj/ehw224
9. Anderson JL, Morrow DA, Campion EW. Acute myocardial infarction. N Engl J Med. 2017;376(21):2053–2064. doi:10.1056/NEJMra1606915
10. Pahan C, Demiral Y, Kilic B, Aslan O. Changes in employment status after myocardial infarction among men. Balk Med J. 2016;33(4):419. doi:10.5152/balkanmedj.2016.150611
11. Jenkins CD, Stanton BA, Savageau JA, Denlinger P, Klein MD. Coronary artery bypass surgery: physical, psychological, social, and economic outcomes six months later. JAMA. 1983;250(6):782–788. doi:10.1001/jama.1983.03340060060027
12. Lazarewicz MA, Wlodarczyk D, Espnes GA. Quality of life in survivors of myocardial infarction. Handb Psychocardiol. 2015;1–18. doi:10.1007/978-981-4560-53-5_63-1
13. Glogowska M, Simmonds R, McLachlan S, et al. Managing patients with heart failure: a qualitative study of multidisciplinary teams with specialist heart failure nurses. Ann Fam Med. 2015;13(5):466–471. doi:10.1370/afm.1845
14. Nordfonn OK, Morken IM, Bru LE, Huseb AML. Patients experience with heart failure treatment and selfcare qualitative study exploring the burden of treatment. J Clin Nurs. 2019;28(9–10):1782–1793. doi:10.1111/jocn.14799
15. Huffman JC, DuBois CM, Mastromauro CA, Moore SV, Suarez L, Park ER. Positive psychological states and health behaviors in acute coronary syndrome patients: a qualitative study. J Health Psychol. 2016;21(6):1026–1036. doi:10.1177/1359105314544135
16. Merritt CJ, de Zoysa N, Hutton JM. A qualitative study of younger men’s experience of heart attack (myocardial infarction). Br J Health Psychol. 2017;22(3):589–608. doi:10.1111/bjhp.12249
17. Heravi-Karimooi M, Rejeh N, Abbasi M. Lived experiences of elderly patients with coronary artery disease: a hermeneutic phenomenological study. Elder Health J. 2017;3(1):28–34.
18. Moshki M, Khajavi A, Hashemizadeh H, Vakilian F, Minaee S, Martin SS. Dark or bright half of the moon: a qualitative study exploring the experience of Iranian heart failure patients regarding their quality of life. Open Access Maced J Med Sci. 2019;7(5):824–830. doi:10.3889/oamjms.2019.189
19. Naseri N, Moeeni M. The lived experiences of symptoms in women with coronary heart disease: a phenomenology study. J Healthc Qual. 2017;18(4):326–335.
20. Lopez-Medina IM, Gil-Garca E, Sínchez-Criado V, Pancorbo-Hidalgo PL. Patients experiences of sexual activity following myocardial ischemia. Clin Nurs Res. 2016;25(1):45–66. doi:10.1177/1054773814534440
21. Pedersen D. Political violence, ethnic conflict, and contemporary wars: broad implications for health and social well-being. Soc Sci Med. 2002;55(2):175–190. doi:10.1016/S0277-9536(01)00261-1
22. Tracy SJ. Qualitative Research Methods: Collecting Evidence, Crafting Analysis, Communicating Impact. John Wiley & Sons; 2012.
23. Finlay L. Debating Phenomenological Methods. Hermeneutic Phenomenology in Education. Springer; 2012:17–37.
24. Kafle NP. Hermeneutic phenomenological research method simplified. Bodhi: Interdiscip J. 2011;5(1):181–200.
25. Van Manen M.Phenomenology of practice: Meaning-giving methods in phenomenological research and writing. Routledge; 2016.
26. Walker JL. Research column. The use of saturation in qualitative research. Eur J Cardiovasc Nurs. 2012;22(2).
27. Boyd C. Phenomenology the method in nursing research: a qualitative perspective. 2001.
28. Creswell JW, Poth CN. Qualitative Inquiry & Research Design; Choosing among Five Approach. Sage Publications; 2018.
29. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
30. Ajjawi R, Higgs J. Using hermeneutic phenomenology to investigate how experienced practitioners learn to communicate clinical reasoning. Qual Rep. 2007;12(4):612–638.
31. Loh J. Inquiry into issues of trustworthiness and quality in narrative studies: a perspective. Qual Rep. 2013;18(33):1–15.
32. Lincoln YS, Guba EG. Naturalistic inquiry. Newberry Park. In: CA: Sage; 1985
33. Heo S, Lennie TA, Okoli C, Moser DK. Quality of life in patients with heart failure: ask the patients. Heart Lung. 2009;38(2):100–108. doi:10.1016/j.hrtlng.2008.04.002
34. Jeon YH, Kraus SG, Jowsey T, Glasgow NJ. The experience of living with chronic heart failure: a narrative review of qualitative studies. BMC Health Serv Res. 2010;10(1):77. doi:10.1186/1472-6963-10-77
35. Hutton JM, Perkins SJ. A qualitative study of men’s experience of myocardial infarction. Psychol Health Med. 2008;13(1):87–97. doi:10.1080/13548500701294549
36. Staniute M, Brozaitiene J, Burkauskas J, Kazukauskiene N, Mickuviene N, Bunevicius R. Type D personality, mental distress, social support and health-related quality of life in coronary artery disease patients with heart failure: a longitudinal observational study. Health and Quality of Life Outcomes. 2015;13(1):1. doi:10.1186/s12955-014-0204-2
37. Park Y, Park Y-H, Park K-S. Determinants of non-adherences to long-term medical therapy after myocardial infarction: a cross-sectional study. Int J Environ Res Public Health. 2020;17:10. doi:10.3390/ijerph17103585
38. Kristofferzon M-L, Löfmark R, Carlsson M. Managing consequences and finding hope – experiences of Swedish women and men 4–6 months after myocardial infarction. Scand J Caring Sci. 2008;22(3):367–375. doi:10.1111/j.1471-6712.2007.00538.x
39. Mookadam F, Arthur HM. Social support and its relationship to morbidity and mortality after acute myocardial infarction: systematic overview. Arch Intern Med. 2004;164(14):1514. doi:10.1001/archinte.164.14.1514
40. Wilski M, Sienkiewicz Wilowska JA. Social support as a regulator of self-care attitude in persons with myocardial infarction. Polish Psychol Bull. 2014;45(4). doi:10.2478/ppb-2014-0062
41. Jones L, Williams S, Bydalek K, Elkins C, Fruh S. African American Women’s perceptions of cardiovascular disease after myocardial infarction: a phenomenological inquiry. J Cardiovasc Nurs. 2019;34(6):503–510. doi:10.1097/JCN.0000000000000614
42. McSweeney JC, Rosenfeld AG, Abel WM, et al. Preventing and experiencing ischemic heart disease as a woman: state of the science: a scientific statement from the American Heart Association. Circulation. 2016;133(13):1302–1331. doi:10.1161/CIR.0000000000000381
43. Borhani F, Najafi MK, Rabori ED, Sabzevari S. The effect of family-centered empowerment model on quality of life of schoolGÇôaged children with thalassemia major. Iran J Nurs Midwifery Res. 2011;16(4):292.
44. Condon C, McCarthy G. Lifestyle changes following acute myocardial infarction: patients perspectives. Eur J Cardiovasc Nurs. 2006;5(1):37–44. doi:10.1016/j.ejcnurse.2005.06.005
45. Finlun N, Fridlund B, Schaufel MA, Schei E, Norekv TM. Patients, goals, resources, and barriers to future change: a qualitative study of patient reflections at hospital discharge after myocardial infarction. Eur J Cardiovasc Nurs. 2016;15(7):495–503. doi:10.1177/1474515115614712
46. Farmer SA, Magasi S, Block P, et al. Patient, Caregiver, and Physician Work in Heart Failure Disease Management: A Qualitative Study of Issues That Undermine Wellness. Elsevier; 2016. doi:10.1016/j.mayocp.2016.05.016
47. Bhattacharyya M, Stevenson F, Walters K. Exploration of the psychological impact and adaptation to cardiac events in South Asians in the UK: a qualitative study. BMJ Open. 2016;6(7):e010195. doi:10.1136/bmjopen-2015-010195
48. Busza J, Dauya E, Makamba M, Ferrand RA. GÇ£I will not stop visiting!GÇ¥ a qualitative study of community health workersGÇÖ reluctance to withdraw household support following the end of a community-based intervention in Zimbabwe. BMC Health Serv Res. 2018;18(1):718. doi:10.1186/s12913-018-3531-x
49. Currie K, Strachan PH, Spaling M, Harkness K, Barber D, Clark AM. The importance of interactions between patients and healthcare professionals for heart failure self-care: a systematic review of qualitative research into patient perspectives. Eur J Cardiovasc Nurs. 2015;14(6):525–535. doi:10.1177/1474515114547648
50. Farahbakhsh M, Bazargani HS, Saadati M, Tabrizi JS, Golestani M, Zakery A. Health services utilisation and responsiveness profiles in Iran: a provincial household study. J Family Med Prim Care. 2019;7(1):e000007. doi:10.1136/fmch-2018-000007
51. Kebriaeezadeh A, Koopaei NN, Abdollahiasl A, Nikfar S, Mohamadi N. Trend analysis of the pharmaceutical market in Iran; 1997–2010; policy implications for developing countries. Daru. 2013;21(1):52. doi:10.1186/2008-2231-21-52
52. Ditto PH. Perceptions of health and illness: current research and applications. In: Petrie KJ, Weinman JA, editors. Psychological Medicine. New York: Harwood Academic Publishers; 1998:1999. doi:10.1017/s0033291799218806
53. Shahrbabaki PM, Nouhi E, Kazemi M, Ahmadi F. Spirituality: a panacea for patients coping with heart failure. Int J Commun Based Nurs Midwifery. 2017;5(1):38.
54. Choumanova I, Wanat S, Barrett R, Koopman C. Religion and spirituality in coping with breast cancer: perspectives of Chilean women. Breast J. 2006;12(4):349–352. doi:10.1111/j.1075-122X.2006.00274.x
55. Ebadi A, Ahmadi F, Ghanei M, Kazemnejad A. Spirituality: a key factor in coping among Iranians chronically affected by mustard gas in the disaster of war. Nurs Health Sci. 2009;11(4):344–350. doi:10.1111/j.1442-2018.2009.00498.x
56. Janssen-Niemeijer AJ, Visse M, Van Leeuwen R, Leget C, Cusveller BS. The role of spirituality in lifestyle changing among patients with chronic cardiovascular diseases: a literature review of qualitative studies. J Relig Health. 2017;56(4):1460–1477. doi:10.1007/s10943-017-0384-2
57. Padilla-D¡az M. Phenomenology in educational qualitative research: philosophy as science or philosophical science. IJEE. 2015;1(2):101–110. doi:10.18562/IJEE.2015.0009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.