")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Level of Physical Activity and Its Associated Factors Among Type II Diabetes Patients in Dessie Referral Hospital, Northeast Ethiopia
Authors Edmealem A , Ademe S , Tegegne B
Received 31 August 2020
Accepted for publication 2 October 2020
Published 29 October 2020 Volume 2020:13 Pages 4067—4075
DOI https://doi.org/10.2147/DMSO.S279772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Afework Edmealem, Sewunet Ademe, Belachew Tegegne
Department of Nursing, School of Nursing and Midwifery, Wollo University, Dessie, Ethiopia
Correspondence: Afework Edmealem Tel +251921287207
Email [email protected]
Background: Overweight and obesity results in poor control of chronic illnesses such as diabetes mellitus. The main reason for being overweight and obese among patients with chronic illness is low level of physical activity. Thus, this study aimed to assess level of physical activity and its associated factors among type II diabetes patients at Dessie Referral Hospital, Northeast Ethiopia.
Methods: A hospital-based cross-sectional study was employed from October 1 to November 25 2019 in Dessie Referral Hospital. The study utilized systematic sampling technique to recruit the sample population of 364 diabetic patients. Face-to-face exit interview was used to collect the data. The data were presented with text and tables. Bivariable and multivariable binary logistic regression was employed to identify independent predictors of low level of physical activity at a P-value of < 0.05.
Results: From the total study participants, 110 (33.1%) of them did not perform health enhancing physical activity. Patients whose body mass index was below 18.5 kg/m2 did not perform health enhancing physical activity twice more likely compared with patients whose weight was normal (AOR=2.36, 95%CI: 0.02– 5.42). Patients who were depressed did not perform health enhancing physical activity five times more likely compared with their counterparts (AOR=4.83, 95%CI: 1.46– 15.96). In addition, being widowed (P=0.037), living in an urban area (P=0.028) and duration of disease (P=0.020) were statistically associated with low level of physical activity.
Conclusion and Recommendations: The level of physical activity among patients with type II diabetes was low. Being widowed, living in an urban area, being underweight, duration of disease and being depressed were independent predictors of low level of physical activity. Health education should be given in every visit to patients with type II diabetes. Promotion of physical activity through campaign should be done.
Keywords: physical activity, factors, Ethiopia
Background
Physical activity is any bodily movement produced by skeletal muscle that require energy expenditure.1 World Health Organization (WHO) recommends at least 150 minutes of moderate intensity aerobic physical activity throughout the week or at least 75 minutes of vigorous intensity aerobic physical activity or a combination of moderate and vigorous intensity physical activity for adults 18–64 years old for the prevention of chronic illness. On the other hand, similar dose of physical activity with low intensity activities such as leisure activities was recommended for adults aged 65 years and above.2
Physical activity functionally alters and improves all body systems.3 As a result, it is essential to preserve the health and physical functioning of healthy individuals and those with chronic diseases. Physical activity helps to increase daily functions of patients with chronic illness. This in turn improves quality of life.4 It also helps to manage fatigue.5 Physical activity is viewed as medication and currently it is included in medical management plan of different chronic illnesses.3 A recent systematic review and meta analysis reported that physical activity helps to alleviate depression in patients with chronic illness such as cardiac diseases.6
Being inactive in physical activity is the main reason for being overweight and obese among patients with chronic illness.7 Overweight and obesity are the major factors that hinder the control of chronic illnesses such as diabetes.8 This is true for middle to low income countries including Ethiopia.9 Physical activity and chronic illness have bidirectional relationship that low level of physical activity causes chronic illness and chronic illness leads to inactive in physical activity.7,10 In addition to morbidity and premature mortality, physical inactivity is responsible to substantial economical burden. In 2013, Physical inactivity related death contribute to 13.8 billion dollar worldwide.11
Early physical activity lowers the prevalence of chronic illnesses such as diabetes and hypertension in adulthood.12 Health Enhancing Physical Activity (HEAP) has numerous positive effects to patients with diabetes and cardiovascular disease. It is associated with reduced risk of all causes of mortality in hypertensive adults and a reduced incidence of both macro vascular and micro vascular complications of diabetes.13,14 Moreover, physical activity has a benefit for patients with heart failure and hypertension by increasing their oxygen supply and increasing myocardial electrical stability.3
Physical inactivity is associated with different factors. According to different studies, physical activity is associated with age,15 residence,15,16 sex, body mass index,16,17 drinking alcohol, smoking cigarette, educational status and economical status.17
Determining the level of physical activity among patients with diabetes is helpful to understand patient’s adherence to lifestyle modification (physical activity). Recognizing patients’ low level of physical activity is also important for the prevention of adverse prognosis of diabetes. Nevertheless, the level of physical activity and factors associated with low level of physical activity in patients with diabetes is not assessed in Ethiopia. Therefore, this study was initiated to assess level of physical activity and factors associated with physical activity among patients with type II diabetes in Dessie Referral Hospital, Northeast Ethiopia. Health care providers and policy makers can use the finding of this study as evidence for factors that decrease exercise performance of patients with type II diabetes.
Methods
Study Area and Period
The study was conducted at Dessie Referral Hospital which is found in Dessie town. Dessie town is found 401km far from Addis Ababa. The only referral hospital in Dessie town is Dessie Referral Hospital which serves more than 3.5 million. Dessie Referral Hospital has a total of 749 workers. Among these, 548 are health professionals and 201 are administrative staffs. Out of those health professionals, 363are nurses.18 The study was conducted from October 1st till November 25 2019.
Study Design
Hospital-based cross-sectional study design was employed.
Population
The source populations were all patients with type II diabetes who are on follow up in Dessie Referral Hospital. All patients with type II diabetes who are on follow up in Dessie Referral Hospital during data collection period were study populations.
Inclusion and Exclusion Criteria
Type II diabetes patients who are on follow up and who are 18 years and above were include in the study. On the other hand, patients who are pregnant, patients who are unable to communicate and seriously ill were excluded.
Sample Size Determination
Sample size was calculated by using single population proportion formula with 95% confidence level, 5% margin of error and adherence to recommended physical activity among hypertensive patients. The proportion, which is 31.4%, was taken from study conducted in Addis Ababa.19 It was calculated as follows.

d2
N: Sample size,
Z a/2 =1.96 (standardized normal distribution curve value for the 95%CI),
P = 0.314 (proportion of adherence to physical activity among hypertensive patients) and
D = 0.05 (degree of margin of error)
= (1.96)2 (0.314) (0.686)
(0.05)2
= 330.8
= ~331
There for, by adding 10% non response rate of 331, the total sample size was 364.
Sampling Technique and Procedure
Systematic random sampling technique was utilized to recruit study participants. Study participants were selected in every kth value which is 7. K value was calculated from the proportion of sample to the total diabetes population. The first patient was selected by simple random sampling from patients who are coming for follow up during data collection period.
Variables
Dependent variables was level of physical activity and independent variables were socio demographic variables (sex, age, educational level, marital status, resident, occupation, monthly income, body mass index), disease characteristics (duration of disease since diagnosis, number of medication, medication adherence), perception towards prognosis of illness, substance use (smoking, chat chewing and uses of hashish and shisha and alcohol use).
Data Collection Tool and Procedures
Data Collection Tool
The data were collected by structured standardized tool. It has three parts. The first part asked about sociodemographic status of study participants. The second part measured level of physical activity. Physical activity was measured by International Physical Activity Questionnaire (IPAQ-7) which is standardized tool for measurement of physical activity for patients with chronic illnesses. In this study, internal reliability for IPAQ-7 was 0.84. The third part focused on factors such as substance use, alcohol use, anxiety and depression. Anxiety and depression were assessed by Generalized Anxiety Disorder (GAD-7) and Patient Health Questionnaire (PHQ-2) respectively. In this study, the internal reliability of GAD-7 and PHQ-2 were 0.76 and 0.8 respectively. Medication adherence is measured by a four item tool whose response categories were “yes” and “no”. For each item, 0 points was given for “yes” response and 1 point was given for “no” response. All questionnaires were prepared in English version and translated into Amharic then back to English to check its consistency. The weight and height of nonpregnant and edematous patients were measured in kilograms and in meters respectively.
Data Collection Procedures
Four data collectors and a supervisor who was holder of degree in nursing were recruited. After recruiting them, training was given for two days duration. The training was given on the meaning of every item of the questionnaire and the techniques of data collection such as ways of greeting, ways of taking consent, ways of data quality monitoring during height and weight measurement and ways of addressing ambiguous items. Face-to-face exit interview was used to collect the data. Height and weight were measured for nonpregnant and edematous patients during data collection period by data collectors. The data collectors asked and verified whether the patient had been interviewed or not before data collection in order to avoid repeated interviews for patients with repeated visits. The data collection process was monitored closely by the principal investigator and the supervisor.
Data Quality Assurance
Designing the questionnaire carefully, training data collectors and supervisor, monitoring the data collection process and checking completeness of data during data collection time were used to assure the quality of data. In addition to these, to address confusing items and to increase the quality of data, all parts of the questionnaire were pretested on 10% of the sample size (36 respondents) at Hidar 11 Primary Hospital.
Data Processing and Analysis Procedure
After data collection, completely collected data were entered in to EpiData version 3.1 and exported to Statistical Package and Service Product (SPSS) version 25 for analysis. During analysis, the total score of physical activity was categorized into two levels: inactive and health enhancing physical activity (HEPA). Inactive: score which do not meet criteria of HEPA or less than three days of vigorous activity of at least 20 min per day or less than five days of moderate-intensity activity or walking of at least 30 min per day or less than five days of any combination of walking, moderate-intensity or vigorous intensity activities achieving less than 1500 metabolic equivalent (MET)-min/week. HEPA: vigorous-intensity activity on at least three days achieving a minimum of at least 1500 MET-min/week or seven or more days of any combination of walking, moderate-intensity or vigorous intensity activities achieving a minimum of at least 3000 MET-minutes/week. Study participants who scored 9 and above in Generalized Anxiety Disorder Item 7 (GAD-7) questionnaire were categorized as having anxiety and study participants who scored three and above in atient Health Questionnaire item 2 (PHQ-2) questionnaire were categorized as positive for depression disorder. Study participants who scored ≥3 from medication adherence scale were grouped as adherent and less than three were nonadherent. The results of the study were presented using text, tables, and a binary logistic regression model was enrolled by considering 95% confidence level and P-value of 0.05. Initially, the association between variables and physical activity was seen in bivariable binary logistic regression. Then, multivariable binary logistic regression was done by taking variables that have a P-value of ≤0.2 from bivariable logistic regression to control the confounding variables.
Results
Sociodemographic and Economic Characteristics
From a total of 364 respondents, 332 respondents participated with a 91.2% response rate. Among these, 157 (47.3%) were female; 131 (39.5%) were illiterate (unable to read and write); 207 (62.3%) were married and 117 (35.2%) were farmers. The median age of respondents was 45 (IQR=30) and 44 (13.3%) of the respondents were 65 years of age and above. From the total respondents, 128 (38.6%) of them lived in rural areas. Over one fifth of the total respondents 73 (22%) did not get any support from others. BMI was calculated for 320 nonpregnant and edematous respondents and among these, over one fifth (21.6%) of them were overweight (BMI ≥25 kg/m2) (Table 1).
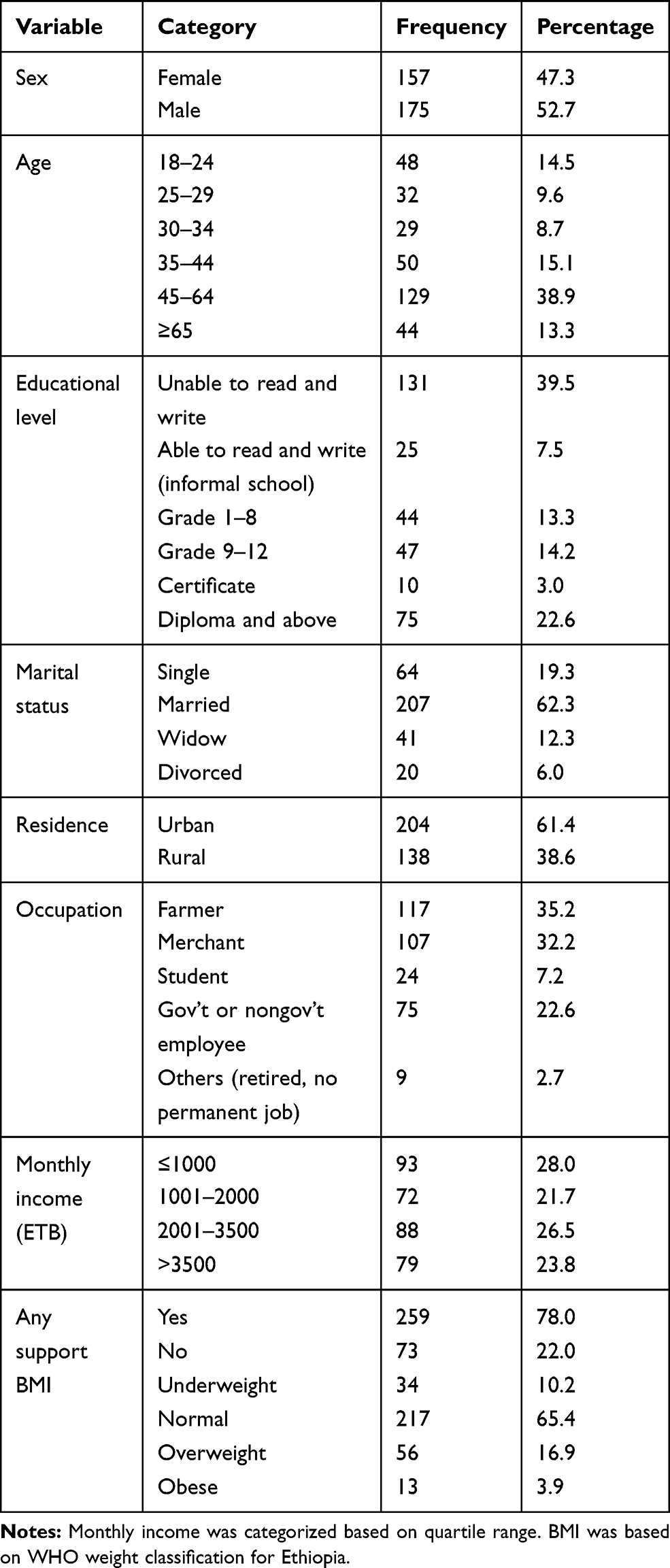 |
Table 1 Sociodemographic Status of Patients with Type II Diabetes at Dessie Referral Hospital, Northeast Ethiopia, 2020 (N=332) |
Overall Level of Physical Activity
From the total study participants, 110 (33.1%) of them were inactive in physical activity or did not perform health enhancing physical activity.
Description of Physical Activity by Sociodemographic Characteristics
From the total 155 female study participants, 55 of them were inactive in physical activity. Forty-one study participants were widowed and among these, 22 of them were inactive or did not perform health enhancing physical activity. From the 204 study participants who resided in an urban area, more than half of them were inactive. Sixty-nine respondents were overweight and obese. Among these, 18 of them were inactive or did not perform health enhancing physical activity (Table 2).
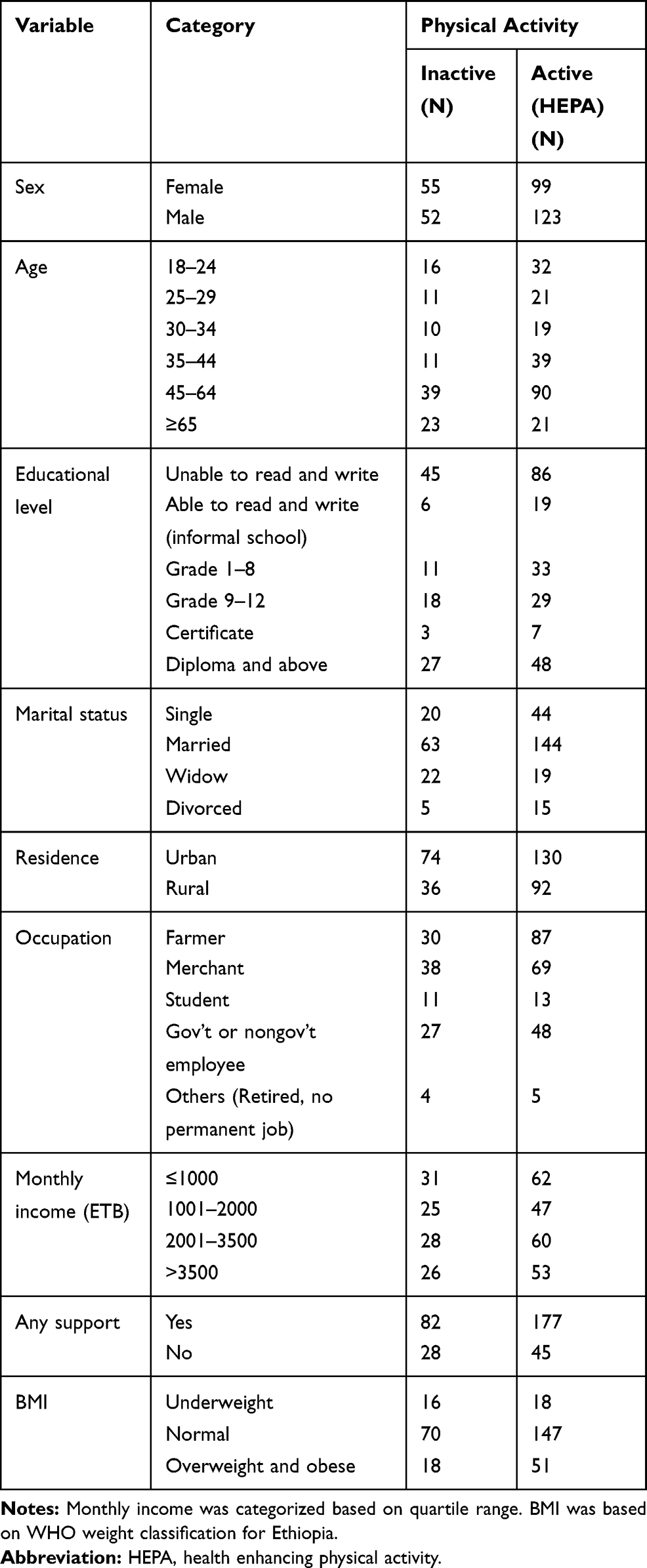 |
Table 2 Description of Physical Activity by Sociodemographic Characteristics Among Patients with Type II Diabetes at Dessie Referral Hospital, Northeast Ethiopia, 2020 (N=332) |
Disease Characteristics and Physical Activity
From the total study participants, 36 (10.8%) of them had poor perception toward the prognosis of their illness. From 36 study participants who had poor perception, 14 of them were inactive in physical activity. Over one fifth (21.4%) of the respondents were not adherent to their medication. From the total of 71 nonadherent respondents, 42 of them were inactive in physical activity. For 54 (16.3%) study participants, the duration of disease since diagnosis was over six years. From the total study participants, 26 (7.8%) of them took five and above drugs daily in the past one month (Table 3).
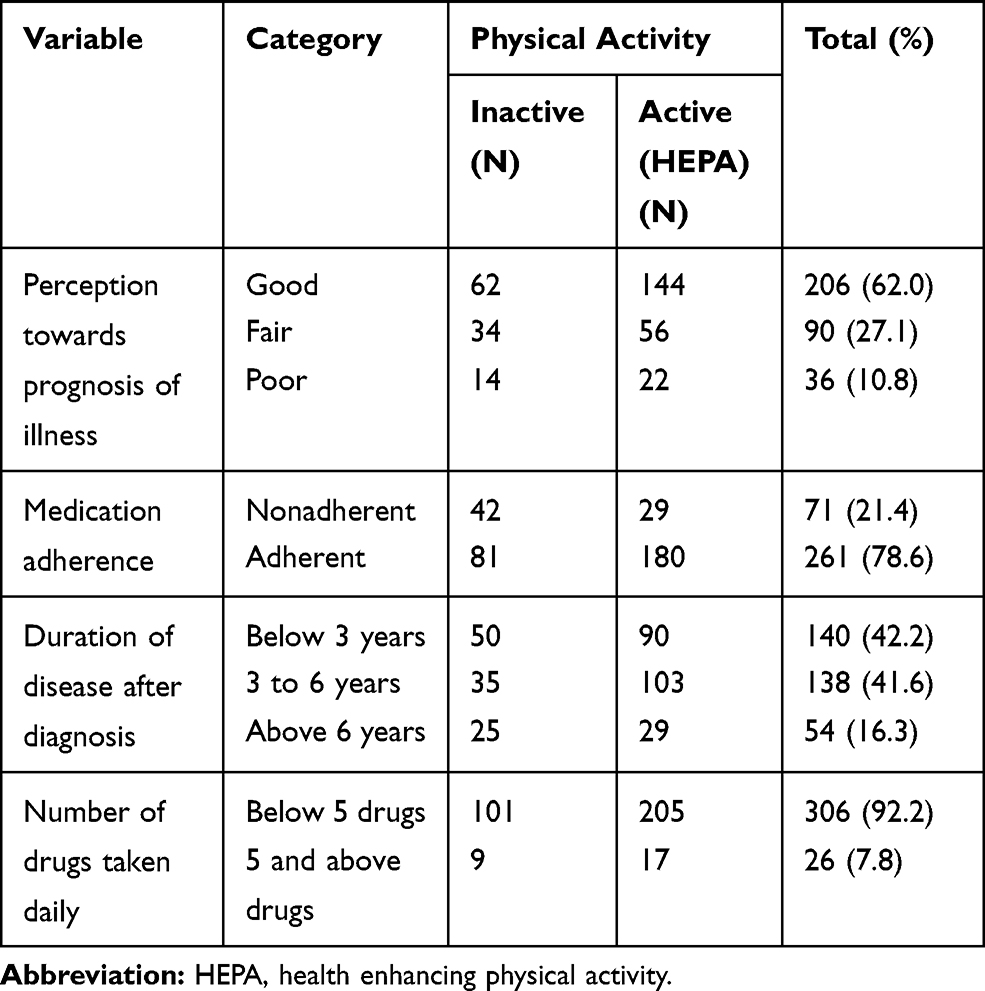 |
Table 3 Disease Characteristics and Physical Activity Among Patients with Type II Diabetes at Dessie Referral Hospital, Northeast Ethiopia, 2020 (N=332) |
Anxiety, Depression, Substance Use and Physical Activity
From the total respondents, 113 (34%) had anxiety. From 113 study participants who had anxiety, 36 of them were inactive in physical activity or did not perform health enhancing physical activity. Eighteen respondents had depression and from this 13 of them were inactive in physical activity. Furthermore, 30 (9%) of the respondents drank alcohol or smoked cigarettes or chewed chat (Table 4).
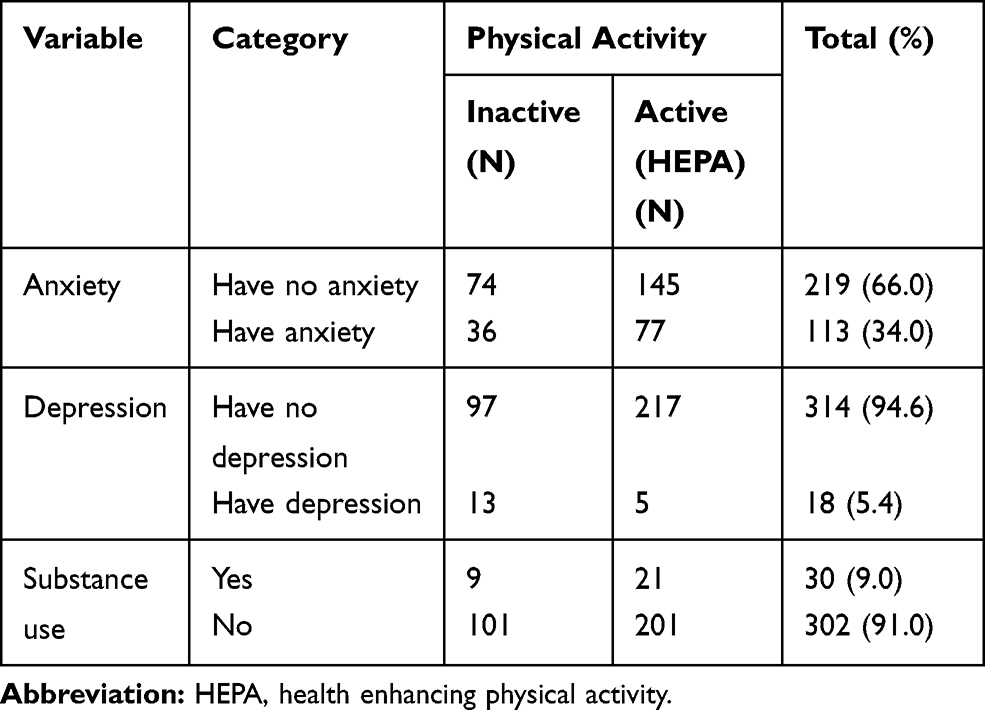 |
Table 4 Anxiety, Depression, Substance Use and Physical Activity Among Patients with Type II Diabetes at Dessie Referral Hospital, Northeast Ethiopia, 2020 (N=332) |
Factors Associated with Physical Activity
Variables which have an association with physical activity at P-value ≤0.2 in bivariable logistic regression were sex, age, marital status, residence, body mass index, duration of disease, depression and medication adherence. These were entered in multivariable logistic regression to identify factors associated with physical activity. However, in multivariable logistic regression, only marital status, residence, duration of disease, body mass index and depression were associated with physical activity at P-value <0.05. According to the results, patients who were widowed did not perform health enhancing physical activity five times more likelycompared to patients who were single (AOR=5.02, 95%CI: 1.19–21.16).Patients whose body mass index was <18.5 kg/m2 did not perform health enhancing physical activity twice more likely compared with patients whose weight was normal (AOR=2.36, 95%CI: 0.02–5.42). In addition, patients who were depressed did not perform health enhancing physical activity five times more likely compared with their counterparts (AOR=4.83, 95%CI: 1.46–15.96) (Table 5).
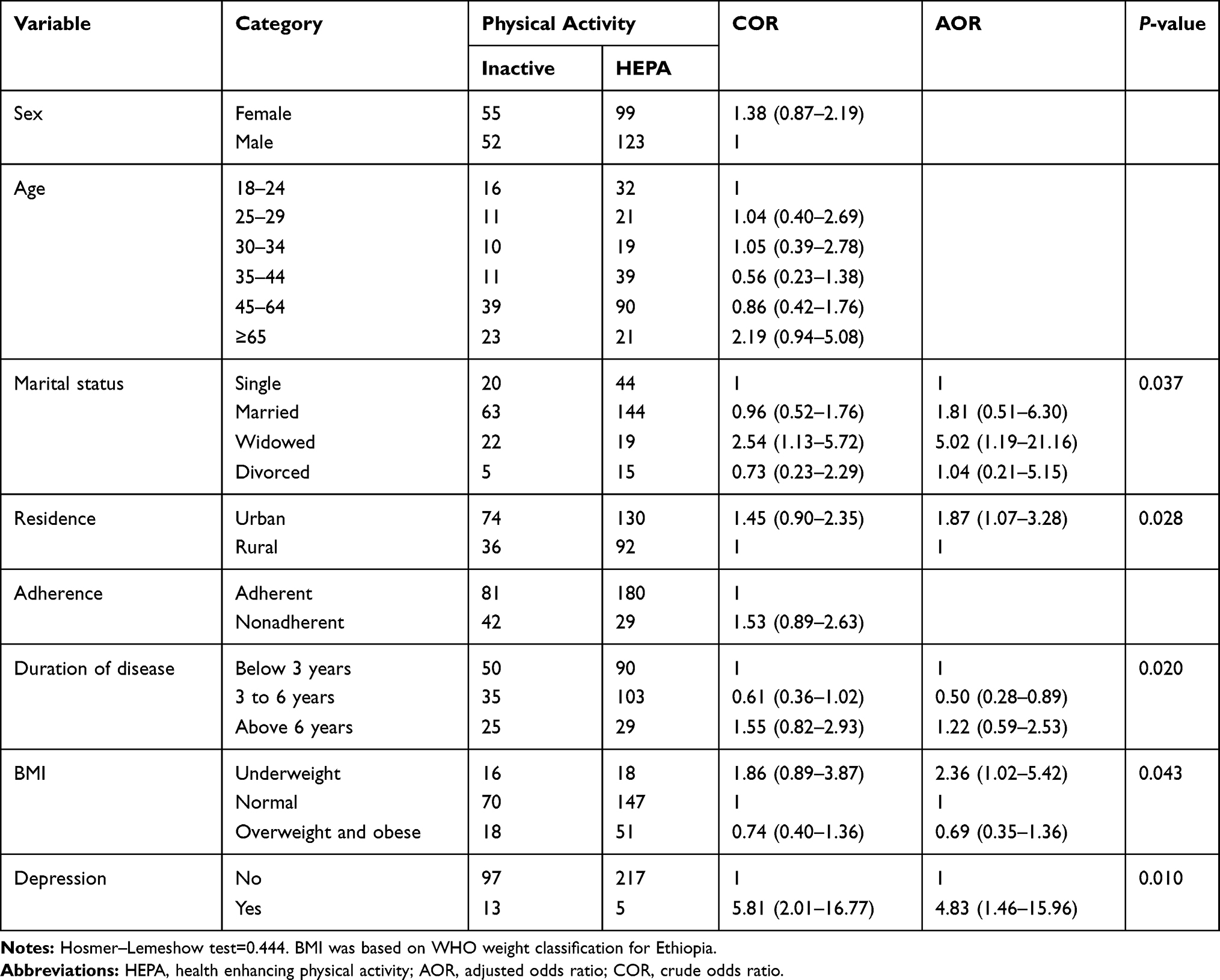 |
Table 5 Logistic Regression Output on the Association Between Level of Physical Activity and Factors, 2020 (N=332) |
Discussion
Low level of physical activity is the main predisposing factor for different chronic illnesses. This study assesses the level of physical activity and its associated factors among patients with type II diabetes mellitus in Dessie Referral Hospital. This study revealed that the level of physical activity among patients with type II diabetes mellitus was 33.1% (95%CI: 28.0–38.6). This finding is in line with the findings of studies conducted in Jimma University Specialized Hospital (36.3%) among hypertensive patients,20 Addis Ababa (31.4%)19 and KwaZulu-Natal (28.4%).21 However, the finding of this study is lower than in the studies conducted in Northwest Ethiopia (78%),22 West Ethiopia (63.4%),23, China (63.1%),17 and Brazil among elderly residents (45.3%).16 The possible justification for this discrepancy might be the difference in source population and tool. Studies conducted in Northwest and West Ethiopia only include patients with hypertension, however this study includes patients with type II diabetes. Furthermore, the categorization of physical activity in a study conducted in Brazil is different from the categorization of this study. Unlike this study, the source population included in a study conducted in China comprised middle and older aged community-dwelling adults. Moreover, the finding of this study is higher than the study conducted in Brazil among hypertensive patients (17%) and diabetes patients (15.1%).24 The possible justification for this difference might be the difference in lifestyle and sociodemographic characteristics.
This study revealed that residence was statistically associated with level of physical activity. According to the finding, patients who were living in an urban area were inactive in their physical activity twice more likely compared with patients who were living in a rural area (AOR=1.87, 95%CI: 1.07–3.28). The possible justification for this might be due to patients living in an urban area used transportation service in their daily activity. In contrast patients who are living in a rural area might perform vigorous physical activity due to their daily activity and farming. The finding of this study is in line with studies conducted in Mozambique25 and Brazil.16
Patients who were widowed were five times more likely inactive in their physical activity when compared with patients who were single (AOR=5.02; 95%CI: 1.19–21.16). This is consistent with the finding of study conducted in KwaZulu-Natal.21 Moreover, patients who were depressed were five times more likely inactivite in physical activity compared with their counterparts (AOR=4.83, 95%CI: 1.46–15.96). The possible justification for this might be hopelessness and decreased attention to the importance of physical activity to chronic illness.
Patients who were underweight were inactive in physical activity twice more likely compared with patients with normal weight (AOR=2.36, 95%CI: 1.02–5.42). Physical activity is seen as an important lifestyle activity to lower the body weight.26 Due to this, patients who are underweight may associate physical activity with being overweight and this could be the possible justification for this finding. This finding is in line with those found in studies conducted in Brazil24 and Wuhan, China.17
This finding also revealed the association between duration of disease and physical inactivity. Patients with type II diabetes mellitus for three-to-six years had lower risk of physical inactivity compared with those with T2DM below three years (OR= 0.50, 95%CI: 0.28–0.89)
Limitations of Study
This study has limitations although it has different methodological strengths. Being a cross-sectional study design is one limitation of this study. Recall bias may be the other limitation of this study. This study assessed level of physical activity for only type II diabetes patients. It cannot be generalized for other types of diabetes.
Conclusion and Recommendations
The level of physical activity among patients with type II diabetes was low. Being widowed, living in an urban area, duration of disease, being underweight and being depressed were factors that affect the level of physical activity. Every patient with type II diabetes should be screened for physical activity in every visit. Health-care providers should give advice to patients with type II diabetes about the importance of physical activity. Promotion of physical activity should be done through campaign. Researchers should investigate further regarding the factors affecting physical activity among patients with type II diabetes with strong study design.
Data Sharing Statement
The data set will not be shared in order to protect the participants’ identities but is available from the corresponding author on reasonable request.
Ethical Consideration
The study was conducted in accordance with the Declaration of Helsinki. Prior to the data collection period, ethical clearance and approval was obtained from Wollo University College of Health Science Research and Ethical Committee (Com/Nurs/152/11). Since the study was conducted by interview, the research and ethical committee of Wollo University College of Medicine and Health Sciences waived written consent and approved and accepted verbal informed consent. A supportive letter was given to the Dessie Referral Hospital and permission was obtained from hospital managers to implement the study. Prior to interviewing the respondents, the aim and objectives of the study were clearly explained to the participants and oral informed consent was obtained. In addition, participants were informed about the right to ask questions and stop response anywhere.
Consent for Publication
Not applicable.
Acknowledgments
We want to forward our heartfelt thanks to the study participants and data collectors for their commitment and cooperation during the data collection period. We would also like to thank Dessie Referral Hospital and Wollo University for their support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflict of interest in this work.
References
1. World Health Organization. Physical activity; 2020. Available from: http://www.who.int.health_topic/physical.activity
2. World Health Organization. Global recommendation on physical activity for health. Global strategy on diet, physical activity and health; 2020. Available from: http://www.who.int.health-topics/factsheet_adults.
3. Larry J, Durstine A, Benjamin Gordon A, Luo X. Chronic disease and the link to physical activity. J Sport Health Science. 2013;2:3–11. doi:10.1016/j.jshs.2012.07.009
4. Schmidt N, et al. Daily activity and functional performance in people with chronic disease: A cross-sectional study. Cogent Med. 2020;7.
5. Abonie US, MarelleHeesterbeek& GRHS, Hettinga FJ. Effects of activity pacing in patients with chronic conditions associated with fatigue complaints: a meta-analysis. Disabil Rehabil. 2018. doi:10.1080/09638288.2018.1504994
6. Béland M, Briand LK, et al. Aerobic exercise alleviates depressive symptoms in patients with a major non-communicable chronic disease: a systematic review and meta-analysis. BMJ Sports Med. 2019;1–9.
7. Booth FW, C.K R, Matthew J. Laye., Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2014;2(2):1143–1211.
8. Pharr JR, Bungum TJ CC. An Assessement of the relationship of physical activity, obesity, and chronic disease/conditions between active/obese and sedentary/normal weight American women in national sample. Public Health. 2018;156:117–123. doi:10.1016/j.puhe.2017.12.013
9. Elizabeth Anderson JLD. Physical activity, exercise and chronic diseases: A brief review. Sports Med Health Sci. 2019;1(1):10–13.
10. Zhou P, Hughes AK, Grady SC, et al. Physical activity and chronic disease among older people in a mid size city in China: a longitudinal of bipolar effects. BMC Public Health. 2018;18:486. doi:10.1186/s12889-018-5408-7
11. Kolbe Alexander TL, E.A F, Peter TK, et al. The economic burden of physical inactivity: a global analysis of major nob communicable diseases. Physical Activity 2016: progress and Challenge. Lancet. 2016;388(10051):1311–1324.
12. Zanesco RAFAA. Early physical activity promotes lower prevalence of chronic disease on adulthood. Hypertension Res. 2010;33:926–931. doi:10.1038/hr.2010.106
13. Loprinzi PD, SNG E, ADDOH O. Physical activity and residual -specific mortality among adults in the United States. Med Sci Sports Exercise. 2016;48(9):1730–1736. doi:10.1249/MSS.0000000000000952
14. Blomster JI, Zoungas S CC, Woodward M, et al. The influence of physical activity on vascular complications and mortality in patients with type 2 diabets mellitus. Diab Obesity Metabolism. 2013;15(11):1008–1012. doi:10.1111/dom.12122
15. Gaskin CJ. Factors associated with physical activity and sedentary behaviour in older adults from six low and middle income countries. Int J Environmental Res Public Health. 2018;15:5. doi:10.3390/ijerph15050908
16. Renato Campos Freire Junior, D.C.C.d.A. Factors associated with low levels of physical activity among elderly residents in a small urban area in the interior of the Brazilian Amazon. Arch Gerontol Geriatr. 2017;75:37–43.
17. Yanfen Zhou JW, Zhang S, Yan S, et al. Prevalence and risk factors of physical inactivity among middle aged and older Chinese in Shenzhen: a cross sectional study. BMJ Open. 2018;8:10.
18. Edmealem A, Olis. CS. Factors associated with anxiety and depression among diabetes, hypertension, and heart failure patients at dessie referral hospital, Northeast Ethiopia. Behav Neurol. 2020;2020:1–10. doi:10.1155/2020/3609873
19. Tibebu A, Mengistu D, Bulto LN. Adherence to prescribed antihypertensive medications and associated factors for hypertensive patients attending chronic follow-up units of selected public hospitals in Addis Ababa, Ethiopia. Int J Health Sci. 2017;11:4.
20. Girma F, et al. Compliance with anti-hypertensive treatment and associated factors among hypertensive patients on follow-up in Jimma University specialized hospital, Jimma, south west Ethiopia: a quantitative cross-sectional study. J Hypertens. 2014;3(5):174.
21. Mbambo SW, Dlungwane TP. Factors associated with physical activity amongest patients with hypertension in two communities health centers in uMgungundlovu health district, KwaZulu-Natal, 2018. South African Family Practice. 2019;61:6. doi:10.4102/safp.v61i6.5074
22. Teshome DF, Demssie AF, Zeleke BM. Determinants of blood pressure control amongst hypertensive patients in Northwest Ethiopia. PLoS One. 2018;13:5. doi:10.1371/journal.pone.0196535
23. Berisa HDAMGD. Non-adherence related factors to antihypertensive medications among hypertensive patients on follow up at Nedjo General Hospital in West Ethiopia. Open Public Health J. 2018;11:1.
24. Forechi L, et al. Adherence to physical activity in adults with chronic diseases: ELSA-Brasil. Revista de Saude Publica 2018;52:31.
25. Padro P, Damasceno A, Silva-Matos C, Prista A, Lunet N. Physical activity Patterns in Mozambique: urban/rural differences during epidemiological transition. Prev Med. 2012;55:444–449. doi:10.1016/j.ypmed.2012.08.006
26. World Health Organization. Chronic disease and thier common risk factors; 2020. Available from: http://who/int/chp/chronic-disease.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.