")
Back to Journals » Patient Preference and Adherence » Volume 16
Level of Patient Health Literacy and Associated Factors Among Adult Admitted Patients at Public Hospitals of West Shoa Oromia, Ethiopia
Authors Gurmu Dugasa Y
Received 25 January 2022
Accepted for publication 23 March 2022
Published 30 March 2022 Volume 2022:16 Pages 853—859
DOI https://doi.org/10.2147/PPA.S357741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yonas Gurmu Dugasa
Department of Nursing, College of Medicine & Health Sciences, Ambo University, Ambo, Ethiopia
Correspondence: Yonas Gurmu Dugasa, Department of Nursing, College of Medicine & Health Sciences, Ambo University, P. O. Box: 19, Ambo, Ethiopia, Email [email protected]
Background: Health literacy is a capacity of individual to gain knowledge that helps to use health information in different levels as needed for self-management and to communicate with health providers. Health literacy has a significant impact on patient health outcomes. The aim of this study was to assess level of patient health literacy and associated factors among adult admitted patients at public hospitals of West Shoa zone, Oromia, Ethiopia.
Methods: A cross-sectional, quantitative study was carried out among adult admitted patients at public hospitals of West Shoa Oromia, Ethiopia. An interviewer-administered Health Literacy Questionnaire (HLQ) instrument tool was used to assess patients’ health literacy. All statistical analysis were performed using SPSS for windows program version 21.
Results: A total of 403 patients participated in this study. Majority of the participants were males 235 (58.3%) and aged 40– 59 years (n = 164, 40.7%). Overall, 59.1% (n = 238) of the participants have high health literacy. Those respondents who are above grade 12 (tertiary) were 2.45 times more likely to have high health literacy (AOR = 2.45, 95% CI: 1.21, 4.98) compared to those respondents not able to read and write . Participants who had age greater or equal to sixty were 65% less likely to have high health literacy (AOR: 0.35, 95% CI: 0.18, 0.70).
Conclusion and Recommendation: Forty percent of the participants have low health literacy. Age and education are significant factors in health literacy. Ethiopian ministry of health, Oromia regional health bureau, West shoa zonal office and healthcare professionals have to provide an intervention in enhancing the level of health literacy by mass media and written material.
Keywords: patient, health literacy, admitted patients
Introduction
Health literacy is a capacity of individuals to obtain and use health information in different level as needed for self-management and to communicate with health care providers.1–4 The term health literacy was first suggested in the 1970s.1 It is a comprehensive skill that contains reading, writing, listening, and speaking skills.5 Health literacy means more than being able to read pamphlets; it is the achievement of a level of knowledge, skills and confidence to take action by improving people’s access to health information, and their capacity to use it effectively; this benefits for improving people’s empowerment within the areas of healthcare, disease prevention and health promotion.6,7
Patients admitted to hospitals come with different levels of health information. So, the healthcare providers have to know the level of health literacy of their patients as low health literacy is associated with poorer health outcomes, increased healthcare costs,8,9 increased mortality,10–12 increased hospitalizations,13 poorer use of preventive healthcare services,14,15 difficulty in communicating with health professionals,14,16 absence of engagement with health care providers,10 and inadequate in medical decision making.17
Level of literacy of individual has an effect on health literacy. Poor literacy can affect health directly by limiting personal, social and cultural development of individuals, as well as hindering the development of health literacy.6 Higher educational qualification cannot guarantee health literacy as an individual’s health literacy level may be lower than his or her general literacy, meaning that even highly educated adults may have limited health literacy.18
Some research findings showed that the levels of health literacy vary according to socio demographic and disease characteristics of patients. Thus, different patient empowerment programs and approaches aimed at raising patients’ health literacy would be essential to improve medication adherence; therefore, healthcare professionals should assess patients’ health literacy level and tailor information and support to the health literacy skills and personal context of their patients.19,20
Approaches to improve health literacy may include easy access to information and services, more effective healthcare provider–patient communication, better patient education materials, individualized self-care support for those with health literacy challenges, relevant postgraduate professional training, and more efficient collaboration across healthcare providers in communicating information and targeting services to individual needs.21–23
Due to the fact that, the limited studies conducted in our context and their disparities in their findings, raise the drive to conduct this study in our study area. The aim of this study was to find the level of patient health literacy and associated factors among adult admitted patients at public hospitals of West Shoa Oromia, Ethiopia.
Methods
Study Design and Participants
An institutional-based cross-sectional study was conducted from February 1–30, 2020 in four public hospitals located in the West Shoa zone: Ambo University Referral Hospital, Ambo General Hospital, Gedo Hospital and Tikur Inchini Hospital were included. All adult (18 years or older) admitted patients were included except those who were critically ill at the time of data collection. The net sample of 422 was recruited using a proportionate sampling method. Accordingly, we have selected 148 patients from Ambo University Referral Hospital, 127 from Ambo General Hospital, 84 from Gedo Hospital, and 63 from Tikur Inchini Hospital.
Instruments (Measures) and Data Collection
Before data collection, the questionnaire was translated from English to Afaan Oromo and Amharic languages by a multilingual translator and then back translated to English by another multilingual translator. The equivalence between the original English version of the questionnaire and the versions in the two local languages were checked.
Interviewer administered, pre-tested, standardized questionnaire was used. During the pretest the internal consistency of the question was evaluated and the Cronbach`s alpha value was 0.8. The instrument comprised sections: namely socio demographic and Health Literacy Questionnaire (HLQ).24 The content was contextualized to Ethiopian patients. Having sufficient information to manage my health, ability to good health information, understanding health information well enough to know what to do considered as functional health literacy; ability to actively engage with health care providers considered as communicative or interactive health literacy; and appraisal of health information considered as critical health literacy. The patients were asked to what extent they agree with the statements: understanding health information well enough to know what to do and having sufficient information to manage my health. Accordingly, responded as 1= strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. Participants responded for ability to actively engage with health care providers, appraisal of health information, and ability to good health information as 1 = cannot do, 2 = very difficult, 3 = quite difficult, 4 = quite easy, and 5 = very easy.24 As it was normal data distribution, the cut-offs to define “high health literacy” was determined considering those patients who scored mean and above mean and otherwise as “low health literacy”.
Continuous follow up was made by principal investigator throughout the data collection period. The data collectors were trained BSc health care providers who were assigned at each of the four hospitals. The purpose of the training is to ensure that all the data collectors have the same information about the study instrument and followed the same interview procedures. The training deal with the purpose of the study, confidentiality and how to approach and forward questions to patients.
Statistical Analysis
The analysis was done using SPSS statistical software version 21.0. The independent variables which have statistically significant association with the patient health literacy, and bivariate, multivariate analysis using logistic regression were computed. For each variable, frequencies, odds ratios (OR), 95% CI and p-value at 5% was computed. The data was described and presented using narrative text, and tables.
Results
Socio‑demographic Characteristics of Respondents
Out of the total patients who were adult admitted patients at public hospitals in government hospitals of West Shoa Zone during the study period, 403 patients participated in the interview making a response rate of 95.5%. Among the total of respondents, 235 (58.3%) were males. About 164 (40.7%) of the respondents were belonging to the age group 40–59 years, and 253 (62.8%) were married (Table 1 below).
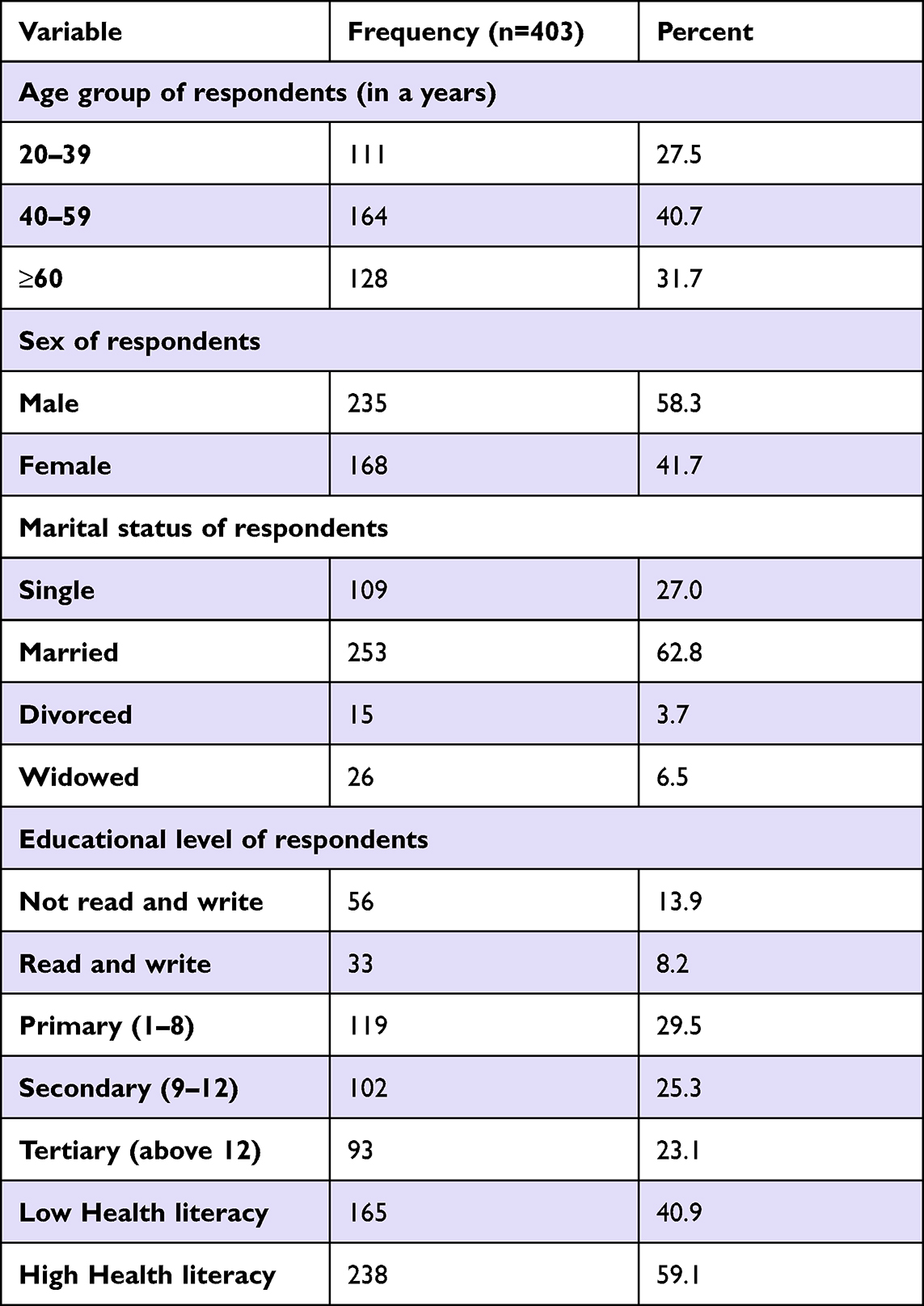 |
Table 1 Socio Demographic Characteristics of Respondents in Selected Public Hospitals of West Shoa, East-West Shoa, Oromia, Ethiopia, 2020 |
Health Literacy of Respondents
More than half of the participants had high health literacy. Mostly low health literacy was the case for the appraisal of health information (Table 2).
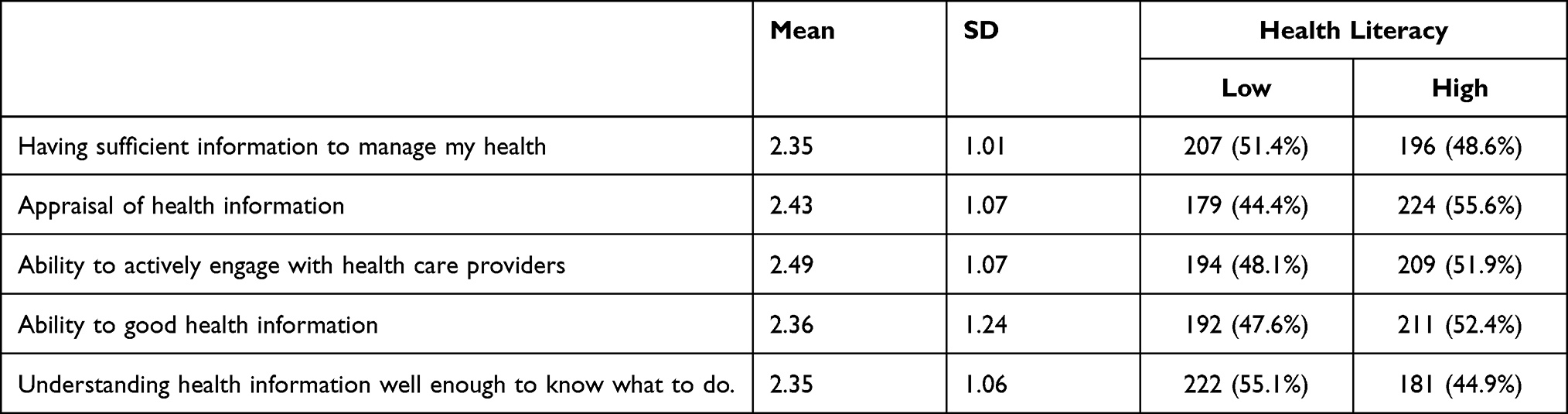 |
Table 2 Health Literacy of Respondents in Selected Public Hospitals of West Shoa, East-West Shoa Oromia, Ethiopia, 2020 (n=403) |
Factors Associated with Health Literacy
In order to explore factors that have association with health literacy both simple and multiple logistic regression analysis were used. Variables that had association with health literacy at significant level (p-value) less than 0.2 in the simple logistic regression analysis were taken as candidates for multiple logistic regression analysis.
Those respondents who are above grade 12 (tertiary) were 2.45 times more likely to have high health literacy (AOR=2.45, 95% CI: 1.21, 4.98) compared to those respondents who could not read and write . Participants who had age greater or equal to sixty were 65% less likely to have high health literacy (AOR: 0.35, 95% CI: 0.18, 0.70) (Table 3).
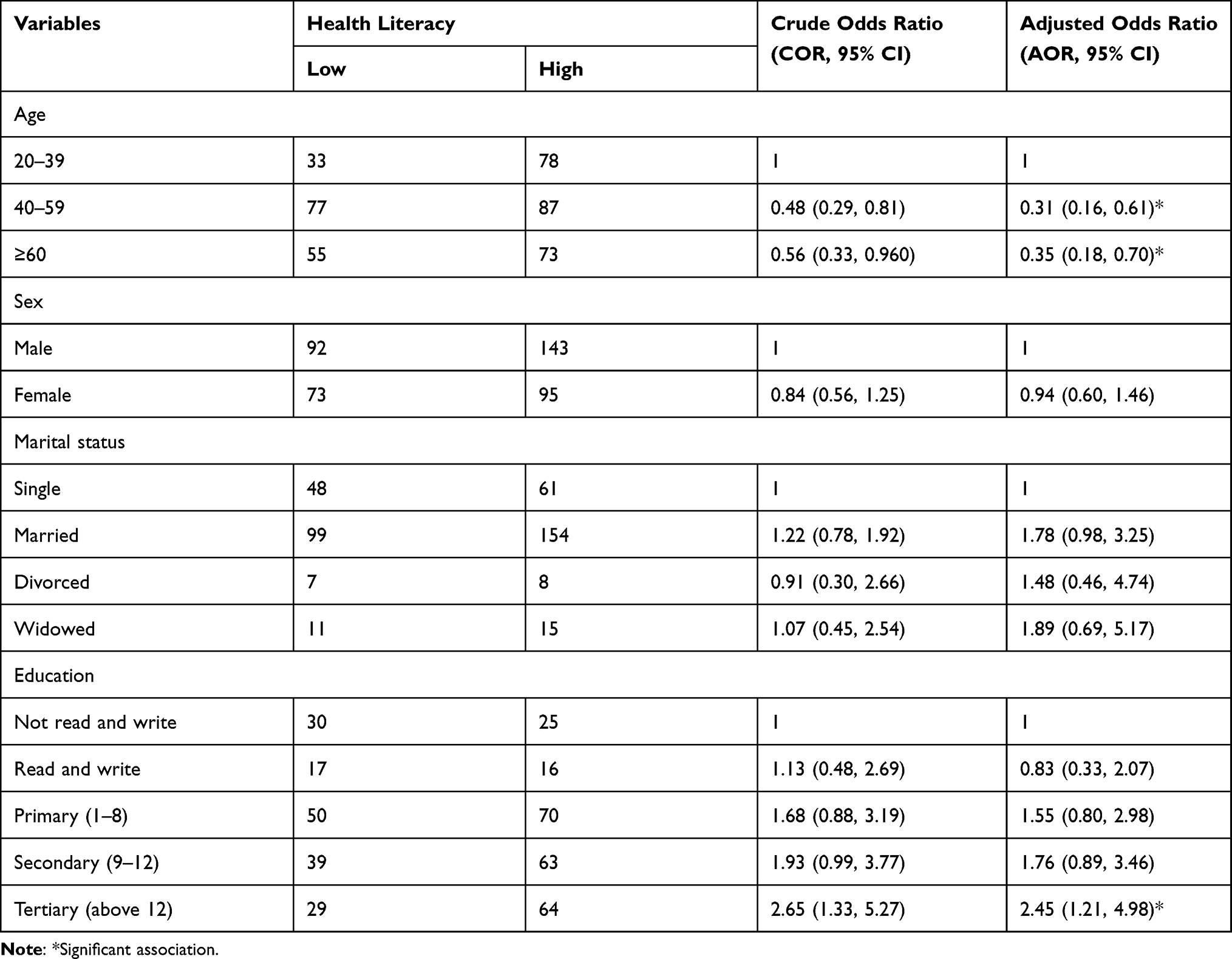 |
Table 3 Factors Associated with Health Literacy of Admitted Patients in Government Hospitals of West Shoa Zone, East-West Shoa Oromia, Ethiopia, 2020 (n= 403) |
Discussion
A patient’s health literacy is an important component of high-quality care that can influence on clinical decisions and actions of patients and providers.25 Adequate health literacy and a better understanding of health education are highly correlated.20 Those patients having low health literacy reported less participation in their care with the clinician, which in turn results in poorer health outcomes. Health Literacy is an important indicator which can guide health providers in tailoring their communication for patients with limited health literacy skills.26
There is a limited data on health literacy among adult admitted patients in government hospitals of West Shoa Zone, Ethiopia. In this study, more than half of the participants had high health literacy. These findings were similar to a study done in Jimma Medical Center, Ethiopia;19,27 even though the patients on follow up may be enhanced health literacy with the health education provided from the health care provider about their treatments. Where as in this study the level of health literacy may be increased due to the information they may get during their stay in hospital.
This study showed aged (≥60 years) participants were 65% less likely to have high health literacy. This is similar with a study done in an acute public hospital in Victoria, Australia on the title health literacy of recently hospitalized patients’ survey; that is being increased age (≥65 years) associated with having the most health literacy challenges.28 Another study done in the University of Gondar Comprehensive Specialized Hospital, Ethiopia 56.5% of patients were considered to have high diabetic-related health literacy being in the age group of less than 40 years old is 6.23 times more likely to achieve the target glycemic control as compared with those older than 60 years with 95% CI AOR 6.23 (1.99–9.11).20
In this study, the health literacy of patients with education of those can read was significantly higher than that of patients who cannot read. Education can upturn patient knowledge, which is inconsistent with another study in Nigeria.29 According to the study done in Saudi Arabia have shown that health education not only can improve knowledge, but also can improve attitude and practice; even though in this study we did not address it.30
This study has strength being used structured, standardized questionnaire and has high response rate. A study contributes baseline information for future studies of that area. In addition to strength; the study has limitation on social desirability bias and cross-sectional study design (cannot provide any information about causal relationships).
Conclusion and Recommendation
Forty percent of the participants have low health literacy. Age and education are significant factors in health literacy. Ethiopian ministry of health, Oromia regional health bureau, West shoa zonal office and healthcare professionals have to provide an intervention in enhancing the level of health literacy by mass media and written material. Future work that is expected from researcher is an interventional study in which, this study didn`t address it.
Abbreviations
SD, Standard deviation; SPSS, Statistical Package for the Social Sciences.
Data Sharing Statement
Datasets used and /or analyzed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The research project was reviewed by an Institutional Review Board of Ambo University. Permission to conduct the research was obtained from the authorities in the study settings and written informed consents were secured from each participant.
Acknowledgments
I am grateful to Ambo University, College of Medicine and Health Science for all their priceless supports. Finally, I would like to thank supervisors, data collectors and all study participants.
Funding
The study was funded by Ambo University. This funding source had role in the design of this study and have role during its execution, analyses, interpretation of the data.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Liu C, Wang D, Liu C, et al. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam Med Commun Health. 2020;8(2):e000351. doi:10.1136/fmch-2020-000351
2. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(Suppl 2):9–15, 19. doi:10.1080/10810730.2010.499985
3. Dickens C, Piano MR. Health literacy and nursing: an update. Am J Nurs. 2013;113(6):52–58. doi:10.1097/01.NAJ.0000431271.83277.2f
4. Gurmu Y, Gela D, Aga F. Factors associated with self-care practice among adult diabetes patients in West Shoa Zone, Oromia Regional State, Ethiopia. BMC Health Serv Res. 2018;18:732. doi:10.1186/s12913-018-3448-4
5. Coleman C, Kurtz-Rossi S, McKinney J, Pleasant A, Rootman I, Shohet L. The Calgary Charter on Health Literacy: Rationale and Core Principles for the Development of Health Literacy Curricula. Centre for Literacy; 2011.
6. Sørensen K, Van den Broucke S, Fullam J. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. doi:10.1186/1471-2458-12-80
7. Bourne A, Peerbux S, Jessup R, Staples M, Beauchamp A, Buchbinder R. Health literacy profile of recently hospitalised patients in the private hospital setting: a cross sectional survey using the Health Literacy Questionnaire (HLQ). BMC Health Serv Res. 2018;18:877. doi:10.1186/s12913-018-3697-2
8. Weiss BD, Palmer R. Relationship between health care costs and very low literacy skills in a -medically needy and indigent Medicaid population. J Am Board Fam Pract. 2004;17(1):44–47. doi:10.3122/jabfm.17.1.44
9. Easton P, Entwistle VA, Williams B. How the stigma of low literacy can impair patient-professional spoken interactions and affect health: insights from a qualitative investigation. BMC Health Serv Res. 2013;13(1):319. doi:10.1186/1472-6963-13-319
10. DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004;19(12):1228–1239. doi:10.1111/j.1525-1497.2004.40153.x
11. Peterson PN, Shetterly SM, Clarke CL, et al. Low health literacy is associated with increased risk of mortality in patients with heart failure. Circulation. 2009;120(18):S749–S749.
12. Baker DW, Gazmararian JA, Williams MV, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–1283. doi:10.2105/AJPH.92.8.1278
13. Song L, Mishel M, Bensen JT, et al. How does health literacy affect quality of life among men with newly diagnosed clinically localized prostate cancer?: findings from the North CarolinaLouisiana Prostate Cancer Project (PCaP). Cancer. 2012;118(15):3842–3851. doi:10.1002/cncr.26713
14. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. doi:10.7326/0003-4819-155-2-201107190-00005
15. Ramandeep G, Arshdeep S, Vinod K, Parampreet P. Oral health literacy among clients visiting a Rural Dental College in north India-A cross-sectional study. Ethiop J Health Sci. 2014;24(3):261–268. doi:10.4314/ejhs.v24i3.10
16. Brabers AEM, Rademakers JJ, Groenewegen PP, van Dijk L, de Jong JD. What role does health literacy play in patients’ involvement in medical decision-making? PLoS One. 2017;12(3):e0173316. doi:10.1371/journal.pone.0173316
17. Jayasinghe UW, Harris MF, Parker SM. The impact of health literacy and life style risk factors on health-related quality of life of Australian patients. Health Qual Life Outcomes. 2016;14:68. doi:10.1186/s12955-016-0471-1
18. Cawthon C, Mion LC, Willens DE, Roumie CL, Kripalani S. Implementing routine health literacy assessment in hospital and primary care patients. Joint Commission J Qual Patient Safety. 2014;40(2):68–AP1. doi:10.1016/S1553-7250(14)40008-4
19. Tilahun D, Abera A, Nemera G. Communicative health literacy in patients with non-communicable diseases in Ethiopia: a cross-sectional study. Trop Med Health. 2021;49(1):1–9.0. doi:10.1186/s41182-021-00345-9
20. Tefera YG, Gebresillassie BM, Emiru YK, et al. Diabetic health literacy and its association with glycemic control among adult patients with type 2 diabetes mellitus attending the outpatient clinic of a university hospital in Ethiopia. PLoS One. 2020;15(4):e0231291. doi:10.1371/journal.pone.0231291
21. Friis K, Aaby A, Lasgaard M, Pedersen MH, Osborne RH, Maindal HT. Low health literacy and mortality in individuals with cardiovascular disease, chronic obstructive pulmonary disease, diabetes, and mental illness: a 6-year population-based follow-up study. Int J Environ Res Public Health. 2020;17(24):9399. doi:10.3390/ijerph17249399
22. Lloyd JE, Song HJ, Dennis SM, Dunbar N, Harris E, Harris MF. A paucity of strategies for developing health literate organisations: a systematic review. PLoS One. 2018;13:e0195018. doi:10.1371/journal.pone.0195018
23. Willis CD, Saul JE, Bitz J, Pompu K, Best A, Jackson B. Improving organizational capacity to address health literacy in public health: a rapid realist review. Public Health. 2014;128:515–524. doi:10.1016/j.puhe.2014.01.014
24. Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health. 2013;13. doi:10.1186/1471-2458-13-658
25. Burks AC, Keim-Malpass J. Health literacy and informed consent for clinical trials: a systematic review and implications for nurses. Nurs Res Rev. 2019;9:31–40.
26. Sim D, Yuan S, Yun J. Health literacy and physician-patient communication: a review of the literature. Int J Commun Health. 2016;10:101–114.
27. Tilahun D, Gezahegn A, Tegenu K, Fenta B. Functional health literacy in patients with cardiovascular diseases: cross-sectional study in Ethiopia. Int J Gen Med. 2021;14:1967. doi:10.2147/IJGM.S304007
28. Jessup RL, Osborne RH, Beauchamp A, Bourne A, Buchbinder R. Health literacy of recently hospitalised patients: a cross-sectional survey using the Health Literacy Questionnaire (HLQ). BMC Health Serv Res. 2017;17(1):1–2. doi:10.1186/s12913-016-1973-6
29. Adeomi AA, Adeoye OA, Asekun-Olarinmoye EO, Abodunrin OL, Olugbenga-Bello AI, Sabageh AO. Evaluation of the effectiveness of peer education in improving HIV knowledge, attitude, and sexual behaviours among in-school adolescents in Osun State. Nigeria Aids Res Treat. 2014;14:131756. doi:10.1155/2014/131756
30. Hanaf MI, Hamid Shalaby SA, Falatah N, El-Ammari H. Impact of health education on knowledge of, attitude to and practice of breastfeeding among women attending primary health care centres in Almadinah Almunawwarah, Kingdom of Saudi Arabia: controlled pre–post study. J Taibah Univ Med Sci. 2014;9(3):187–193. doi:10.1016/j.jtumed.2013.11.011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.