")
Back to Journals » International Journal of Women's Health » Volume 12
Level of Happiness and Its Associated Factors Among Pregnant Women in South Gondar Zone Hospitals, North Central Ethiopia
Authors Tesfa D , Aleminew W, Tadege M , Digssie A , Abebe B, Abebaw S , Kefale B
Received 16 August 2020
Accepted for publication 29 October 2020
Published 5 November 2020 Volume 2020:12 Pages 983—991
DOI https://doi.org/10.2147/IJWH.S275709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Desalegn Tesfa,1 Wallelign Aleminew,2 Melaku Tadege,1 Alemayehu Digssie,1 Bedilu Abebe,1 Sofonyas Abebaw,1 Belayneh Kefale3
1Department of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Health Education, University of Gondar, Gondar, Ethiopia; 3Department of Pharmacy, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Desalegn Tesfa Department of Public Health
College of Health Sciences, Debre Tabor University, P.O. Box 031, Debre Tabor, Ethiopia
Tel +251-918027124
Email [email protected]
Background: Happiness is the most indicator of good quality of life particularly for pregnant women. Reduced happiness of pregnant women can result in reduced maternal health services utilization and can result in adverse newborn and maternal outcomes. Assessing the level of happiness and its factors are important for pregnant women and the next generation. Hence, the current research paper aimed to assess the level of happiness and its associated factors among pregnant women who attended antenatal care follow-up in South Gondar Zone Hospitals.
Methods: Institution-based cross-sectional study was carried out from September 2018 to February 2019 among 1606 expectant pregnant women in the last 6 months. The Oxford Happiness Questionnaire (OHQ) was used as a measure of the degree of happiness and used four as average person score. Besides, bivariate, multivariable logistic analyses were deployed to identify associations.
Results: A total of 1606 pregnant women were participating in this study. The prevalence of low level of pregnancy happiness in this study was 24% (95% CI: 20.7 − 26.6). Mothers who exposed to unintended pregnancy (AOR; 1.94, CI 95% 1.86– 4.52), reported intimate partner violence (AOR; 2.42, 95% CI 1.67– 3.54) and being in the third trimester (AOR; 1.89 95% CI 1.19– 3.01) were the most predictor variables with the low level of happiness.
Conclusion: Approximately one-fourth of the pregnant women had a low level of pregnancy happiness. Mothers who were exposed to unintended pregnancy encountered intimate partner violence, who were in the third trimester were the most significant variables associated with a low level of happiness. Governmental and non-governmental organizations work on women’s reproduction rights and the zonal health department with local health offices should educate on the prevention of intimate partner violence and unintended pregnancy and its consequences and also empower women to cope with changes and challenges of pregnancy and childbirth.
Keywords: happiness, pregnancy, women, level, associated factors
Background
Happiness is a psychological thought with several ideologies and dimensions of well-being.1,2 It is one of the most important concepts in the field of mental health.3,4 Scholars in various disciplines have been involved in the exploration of the pursuit and achievement of a good life and many psychologists argued that happiness has fundamental elements.2,5 Hence, the word “happiness” is used in various ways and it is an umbrella term for all that is good.5 In this meaning, it is often used interchangeably with terms like “well-being” or “quality of life” and denotes both individual and social welfare.5,6 Happiness has been the most important indicator of the quality of life (QoL) because, together with physical and mental health, it shows how people live and thrive.6 The world-well-known philosopher Aristotle believed that happiness depends on ourselves and the cultivation of virtue, though his virtue is somewhat more individualized than the essentially social virtues7 and the concept eudaimonia primarily considered in its subjective and psychological dimensions, rather than in its objective aspects.7,8 It comprises meanings, self-actualization, and personal growth at the individual level and commitment to socially shard goals and values at the social level.2,9
Happiness does no resulting from outside and momentary pleasures alone but an internal pleasure. Optimistic psychology concerns three desires: the pleasant life (positive emotions), the good life (intelligence and athleticism), and the meaning full life (positive institution such as democracy, strong families, and free inquiry).10 Happiness was the key predictor of quality of life since positive life expectancy rises dramatically in both absolute terms and relative terms at all adult ages. Furthermore, it increases the average life expectancy.6 However, in pregnant women, there is tremendous individual difference in the response to inherent emotional, psychological, and cognitive changes during pregnancy, particularly in first-time mothers.11
For women, the pregnancy experience including planning to meet the physical requirements of the baby prepared themselves for labor, control over their experience had a better connection with their partner, and greater contribution in child care with their partner.12 The nine months of gestation can be seen as the substitution for parenthood,10 and feminine identity.13,14 But it is not only a period of exceptional enjoyment but also causes a woman physically, mentally, and social variations. Even in healthy women, pregnancy may lead to many anxieties because of anticipated uncertainty linked to pregnancy.15 Happiness delivers a positive attitude towards life, a healthy mental state creates self-confidence, emotional balance, better sleep, hope for the future, and being visionary.16 However, low levels of happiness among pregnant women have a strong association between prenatal care service utilization and adverse pregnancy outcome including neonatal and infant death.17 A low level of happiness remains a global problem among pregnant women. Thus, even though no further studies have been found in the world, few reports have shown that 59.5% of black Colombians, 42.7% Asians, and 31.5% of Iranians had a low level of happiness. The impact of maternal stress not only on mothers but also harms birth outcomes, including LBW, preterm, SGA, and IUGR.18 Because as maternal stress increases, the level of corticotrophin-releasing hormone (CRH)19 which results in different adverse prenatal and neonatal outcomes.
Nevertheless, optimistic-minded pregnant women had less harmful effects than cynical thinkers.18 Thus, anxiety and life stress were independently significant contributors to an abnormality of pregnancy and are serious at different periods.20 A positive appraisal is the only way associated with less distress and a high level of stability in coping throughout pregnancy.21 Furthermore, in healthy pregnant women, pleasure-time physical activity may be a potentially effective low-cost method of psychological well –being.22 Happiness was significantly affected by the inhabitant, employment status, physical activity,23 dual/single career families,24 age, family type, parity, marital status, religion,25,26 lack of social support, unintended pregnancy, domestic violence, and no stillbirth.27,28
The majority of studies conducted in this field are about fears, anxiety, distress, and discomforts during child delivery, and there is little evidence regarding happiness/unhappiness during pregnancy using happiness measurement standardized questionnaire. Therefore, this study assessed the level of happiness and its associated factors among pregnant women who attended antenatal care follow-up in South Gondar Zone Hospitals, North West Ethiopia.
Methods
Since we cannot address all of the eight hospitals that are found in the South Gondar Zone, 50% (four of them) such as Nefas- Mewicha, Mekane Eyesus, Addis Zemene, and Debre Tabor hospitals were selected randomly. Based on the 2007 Census, this Zone has a total population of 2,051,738 and an increase of 16% over the 1994 census, of which 1,041,061 are men and 1,010,677 women. As the 2019 south Gondar zone report, around 87, 955 pregnant, and 527,967 reproductive-age women are found in the zone. The zone has eight hospitals, 94 health centers, and 378 health posts. The socioeconomic status of the population attending these four hospitals is almost identical, except those which are not similar in form of crop production and altitudes. Except for Debre Tabor General Hospital, which acts as a referral center for public and governmental health institutions, all of them offer similar services. The study was hospital-based and cross-sectional in design. The study took place for six months from September 1st, 2018 to February 30, 2019.
All pregnant women who attended antenatal care in south Gondar zone hospitals and selected hospitals were the source and study population respectively. All women who attended antenatal care in the specified period (six months) were included in the study. Whereas women could not answer the intended questions because of illness and mental problems and referred to higher institutions were excluded. Besides, pregnant women who had unhealthy information such as abortion or miscarriage, intrauterine fetal death, eclampsia, severe bleeding, congenital abnormality, placental problems like placenta previa, and mothers with any other complications that need admission during the visit were excluded. However pregnant women with simple pregnancy-related complications such as infection, dyspepsia, nausea, and vomiting were not excluded. The sample is composed of 1606 eligible women for the current study. All women who met the eligibility criteria in 6 months (September 1st, 2018 to February 30th, 2019) were included.
Concepts such as self-satisfaction, life satisfaction, quality of life, and well-being are interest criteria of the World Health Organizations´ in the definition of mental health. However, the word “happiness” is used in various ways. In the widest sense, it is an umbrella term for all that is good. Oxford Happiness Questionnaire (OHQ) was used as a measure of the degree of happiness. It is a highly standardized, inclusive, improved version and has precise measurement compared with other measurements.5 So for this study, the level of happiness was assessed using the Oxford Happiness Questionnaire (OHQ).29 The OHQ comprises 29 statements, which can be endorsed on a uniform 6 point Likert scale ranging from strongly agrees to strongly disagree. From 29 statements, 12 of them were negative presentations and we considered by reverse scoring. For each statement, the respondents expected to achieve a score of one to six. The overall score of the questionnaire is calculated as the total of all the 29 items divided by 29. The average score in the original version of the Oxford questionnaire is four (somewhat happy or moderately happier or satisfied) even though a score of 3.5 would be an exact numerical average of happy and unhappy responses. The Oxford Happiness Questionnaire is a highly rigorous research assessment instrument conducted cross-culturally through a wide variety of countries and participants from various ethnicities, socio cultures, and socio-economic backgrounds for women, and the alternate form reliability score was in the range of 0.73 and 0.94.30–35 For this analysis, we also evaluated the reliability score and its Cronbach’s alpha was 0.79.
Intimate partner violence: was assessed as exposure to physical violence (6 items) such as slapping, hitting, kicking, beating, sexual violence (3 items) including forced sexual intercourse and other forms of sexual coercion, emotional (psychological) abuse (6 items) such as insults, belittling, intimidation and controlling behaviors (7 items) including isolating a person from family and friends; monitoring their movement; restricting accesses to financial resources Women were asked to indicate whether they had been an experienced to any of the violent acts during pregnancy or in the year before the current pregnancy and/or after childbirth. However, to assess the seriousness, trend, and time frame women were also asked whether they were exposed to the same acts of violence ever in life. For each of the forms of violence, women who reported any of the violent acts were considered as exposed.36
Household wealth status: is computed by principal component analysis from different variables such as the presence of own farmland, own toilet facility, bank account, mobile phone, electricity, the roof of the house with corrugated iron sheet, number of cows/oxen, horses/mules/donkeys goats/sheep and chicken.37
After reviewing the relevant literature, questionnaires were designed to include all possible variables that address the intent of this study. Firstly, all relevant questionnaires including the OHQ were developed in English translated into the local language (Amharic), finally, retranslated into English by a language expert. The data were collected by face-to-face interviews For each hospital 4 BSc and 2 MSc holder psychiatric health professionals have participated as a data collector and supervisor respectively.
Data Quality Assurance
To ensure the quality of data, training was given for all data collectors and supervisors at each hospital for one day on the over-all procedure of data collection by the principal investigator and local language expert. The questionnaire was pre-tested one week before the actual data collection time on 81 participants (5% of the sample) on other hospitals that are not included in the actual study and we evaluated the reliability score and its Cronbach’s alpha.
This was an important chance for the investigator to assess its completeness, clarity, length, and to make changes to questions that were ambiguous to understand during the interview. The investigator and supervisors closely followed the day-to-day data collection process and ensured the completeness and consistency of the questionnaire administered each day. The investigator and supervisor supervising the data collectors randomly while interviewing the mothers. The collected data reviewed and checked for completeness before data entry.
Data Processing and Analysis
Cleaning and cross-checking of data were done before analyzing and coding, entering and cleaning data using EPI INFO windows -version 7 statistical software; and analyzing using SPSS version-20. Both descriptive and analytical statistical methods were utilized. Only Variables in binary screening found at p-value less than 0.2 are considered into multivariate logistic regression.
Logistic regression analysis was applied to describe the functional independent predictors. Odds ratio (OR) with 95% confidence interval (CI) determined to assess the strength of association between independent and dependent variables. For all statistical significant tests p-value < 0.05 was used as a cut-off point.
Ethical Considerations
Ethical clearance was obtained from Debre Tabor University research and ethical review committee (approval number: DTU/5012/August 24/2018). A formal letter from the College of health science was written to four hospitals, and then the permission and support letter was obtained from each hospital. The data was collected from each participant after obtaining informed, voluntary, written, and signed consent before the start of data collection. Respondents’ names were not written on the questionnaire for anonymity and confidentiality of their information. Assent was obtained from participants under the age of 18 years and was approved by the research and an ethical review committee of Debre Tabor University to provide informed consent on their behalf. Individuals were informed that it was fully voluntary, they could withdraw from the study at any time or refuse to answer, could ask anything about the study and that would not affect them. This study was conducted following the declaration of the Helsinki.
Results
Socio-Demographic Characteristic of the Respondents
For this study, a total of 1606 pregnant women have participated. About two-thirds of the mothers 1036 (64.5%) were found in the age category of 20–29 and only 616 (38.4%) of them were attended their education primary and above. Almost all 1574 (98%) of the mothers lived in union with their husbands and half of the mothers lived with a family size of less than three 906 (56.4%), but only one out of six 262 (16.3%) lived in the highest wealth quintile (Table 1).
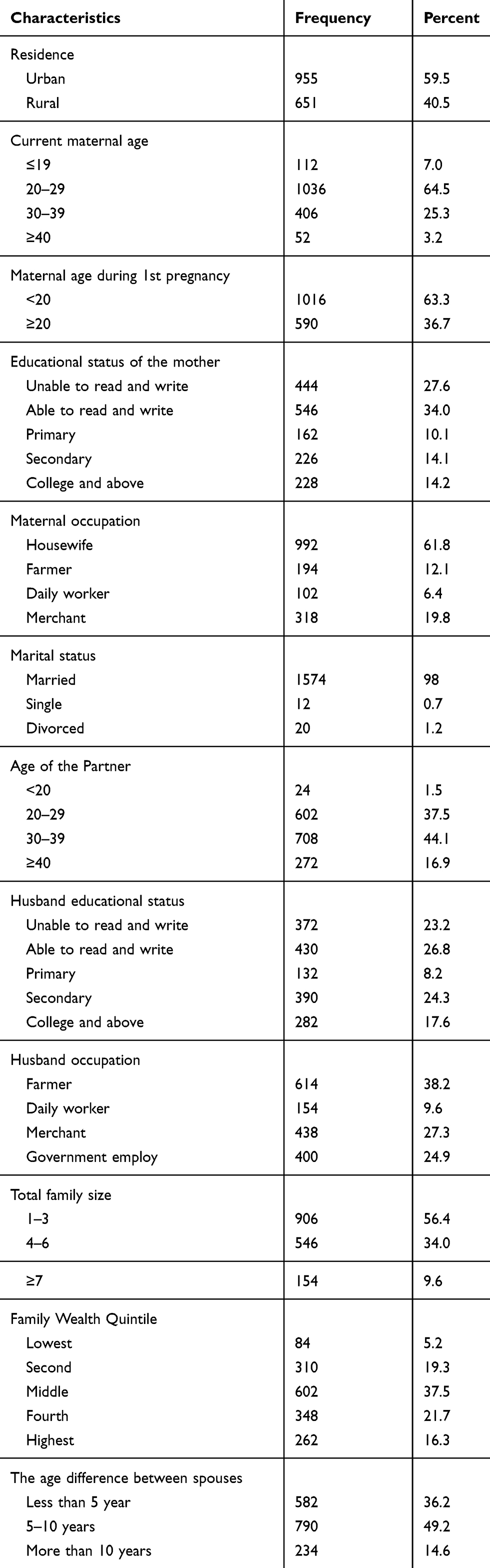 |
Table 1 Socio-Demographic Characteristics of the Respondents in South Gondar Zone Hospitals, North Central Ethiopia 2018/2019 (n=1606) |
Habitual and Abusive Factors
About one fourth 422 (26.3%) of mothers were married by the enforcement of their family and around two-fifth 620 (38.6%) of the pregnant women had encountered intimate partner violence (Table 2)
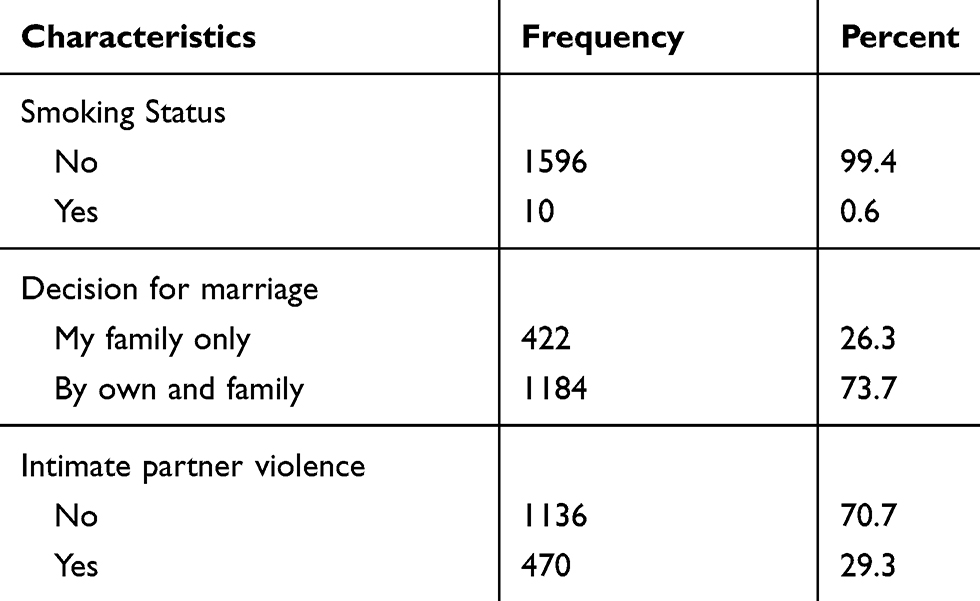 |
Table 2 Habitual and Abusive Characteristics of the Respondents in South Gondar Zone Hospitals, Northcentral, Ethiopia, 2018/2019 (n=1606) |
Obstetric Factors
Spousal accompany during ANC follow-up was 1112 (69.2%) and greater than one out of 6 pregnant women were exposed to unintended pregnancy. Greater than half 886 (55.2%) of the pregnant mothers were interviewed during the 3rd trimester and 34 (2.1%) of the respondents had a history of stillbirth (Table 3).
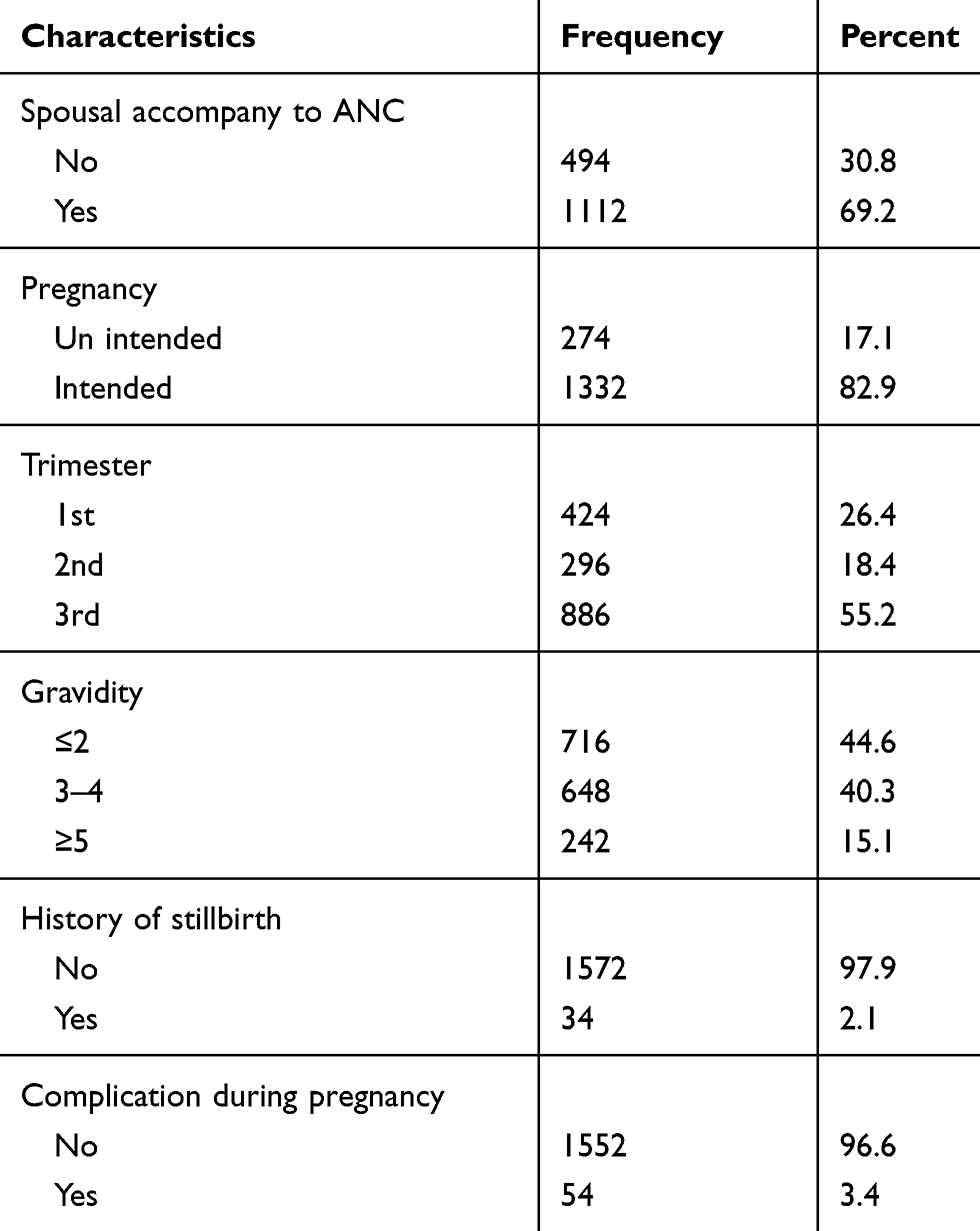 |
Table 3 Obstetric Factors of the Mothers in the South Gondar Zone, Hospitals, North Central Ethiopia, 2018/2019 (n=1606) |
Factors Associated with a Low Level of Happiness Among Pregnant Women
To avoid an excessive number of variables and unstable estimates, only variables with p-value ≤ 0.2 were kept in multivariate logistic analysis using the backward stepwise LR method. Because of confounding effects, not all variables that are significantly associated with bivariate analysis also associated with multivariate analysis. From 5 variables that are significantly associated with the bivariate result, only 3 variables were significantly associated with multivariate results. Since risk factors for happiness are interrelated, multivariable logistic regression analysis gives more meaningful results. The multivariate logistic regression analysis showed that exposure to unintended pregnancy, faced intimate partner violence, and found in the third trimester were significant determinants of the low level of happiness. Mothers who exposed to unintended pregnancy, faced intimate partner violence, and found in the third trimester were 2 times more likely to experience a low level of happiness than women becomes pregnant intentionally (planned and wanted) (AOR; 1.94, 95% CI: 1.86–4.52), had no intimate partner violence (AOR; 2.42, 95% CI: 1.67–3.54) and found on the first trimester (AOR; 1.89 95% CI: 1.19–3.01) (Table 4).
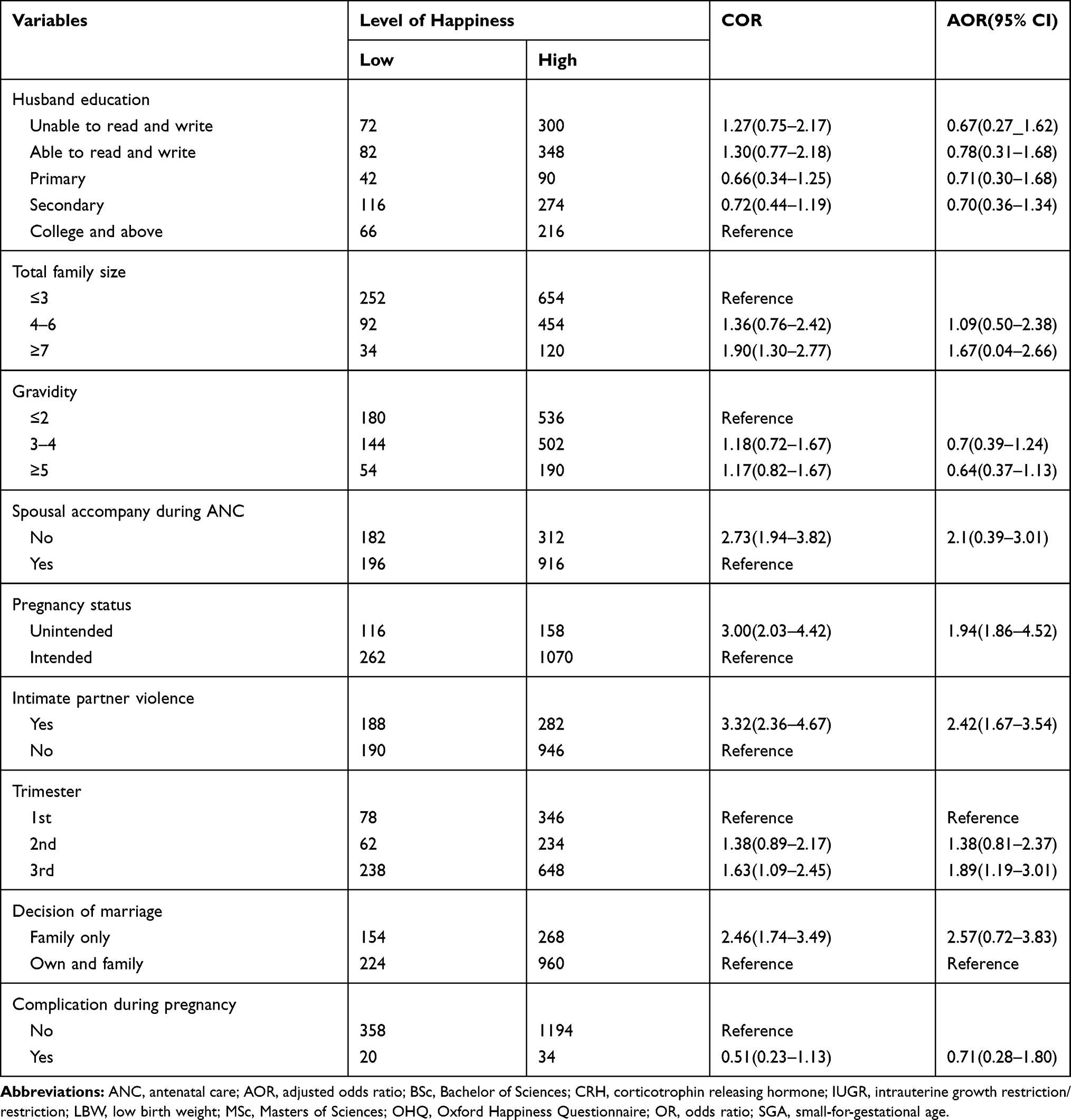 |
Table 4 Factors Associated with a Low Level of Happiness in South Gondar Zone, Hospitals, North Central Ethiopia, 2018/2019 (n=1606) |
Discussions
Happiness has numerous effects on the human’s lifecycle, including a constructive approach that is deeper than a temporary good towards living, the self-concept, the advancement of vitality,38 and enhancing the physical and psychological prosperity.39 Measuring happiness about being pregnant or partner happiness may yield a strong association with prenatal and postnatal care utilization and adverse pregnancy outcome such as IUGR, SGA, LBW, prematurity, high neonatal and infant death.40–42 During pregnancy, unhappiness is a common circumstance;1,3,11,12,14,43 so that differentiating, diagnosing, and taking an instantaneous action is essential.44 Hence, in developing countries like Ethiopia, assessing happiness during pregnancy is important. Considering a wide range of childbirth in Ethiopia, a study regarding the level of happiness among pregnant women is lacking. In this study, therefore, basically determined the level of happiness and its associated factors among pregnant women who attended antenatal care follow-up in South Gondar Zone Hospitals.
In our study, the prevalence of low level of happiness among pregnant women was 24% 95% CI: 20.7 −26.6 and it was close to a study conducted among Indian pregnant women 26%. The similarities between these studies may be the happiness measurement instruments (both of them used the Oxford Happiness Questionnaire) and the same point break. The prevalence of happiness in the pregnancy process was low (11.3%), moderate (72.5%), and high (16.2%) among 300 pregnant women who referred to Mashhad specialized medical centers for further pregnancy care45 and the prevalence of happiness in another study (Iran) was 18.3%, 64.5% and 16.3% low, moderate, and high level, respectively. On the other hand, the prevalence of happiness/unhappiness varies from country to country and from area to area: 42.3% of Asian pregnant women had a low level of happiness17 and 40.7% of polish pregnant women had a low level of life satisfaction in their third trimester pregnancy period.46 Around one third (31.5%) of Iranian pregnant women were categorized under a low level of happiness47 and 59.5% of black Columbian women became unhappy during their pregnancy time. Likewise, in a cohort study of Brazil,48 67.8% of the women were unhappy in their pregnancy process. One of the reasons behind the discrepancy between the prevalence of happiness in our study and the above other investigations could be the specific approaches they used for categorizing methods for assessing satisfaction and happiness. Because as we have seen in the above, we did not distinguish the moderate level from the high level of happiness and then divided the entire case into two categories (low and high level of happiness). The difference on the other hand may be attributed to socio-demographic and socio-cultural factors. Based upon the results of this study, unintended pregnancy was one of the predictor variables of a low level of happiness during pregnancy, therefore, mothers who were exposed to unintended pregnancies were 2 times (AOR; 1.94, 95% CI: 1.86, 4.52) more likely to have a low level of happiness than those women who had intended to have a pregnancy. This study was supported by previous studies.45,49–52 Women with a history of intimate partner violence were two times (AOR; 2.42, 95% CI: 1.67, 3.54) more likely to experience a low level of happiness compared to those who had never experienced intimate partner violence and were confirmed by the study carried out in Iranian women.47,53 Besides, it was also surprising that domestic violence is not only a significant factor of unhappiness; it is also the most predictor of depression, anxiety, mental disorder, and other adverse maternal and newborn outcomes.53–55
The odds of being unhappy (low level of happiness) were elevated among pregnant women who were in their third trimesters (AOR; 1.89, 95% CI; 1.19, 3.01) than women who found in the first trimesters and this was supported with a systematic review.43 That shows pregnant women during the 3rd trimester had significantly lower quality of life scores. And also it was congruent in Iran52 and India25 displayed that a high level of pregnancy-specific anxiety occurred during the third trimesters of the pregnancy process. The reduced amount of happiness in the third trimesters of pregnancy may be due to many women encountered sleep disturbance, concerned about childbirth, becoming fatigued, fear of losing the new baby, concerned about the birthplace, type of birth, breastfeeding, newborn care, and some of the women worried about becoming a parent.
Conclusions
In this cross-sectional study, happiness among pregnant women was a public health concern. The most predictor variables have been pregnancy status (being intended or not), intimate partner violence, and trimesters. We recommended that numerous governmental (like gender office) and non-governmental organizations are concerned about this great issue to improve the right of women to decide on reproductions. The zonal health department and district health offices with other health actors of the area should deliver health information on the prevention of unintended pregnancy and intimate partner violence. Health care workers are expected to encourage spousal to accompany during maternal health service utilization and thereafter. During antenatal care, health care workers should give special attention to pregnant mothers. Finally, in the third-trimester health care’s workers better shall be ready her for childbirth or empower women to cope with changes and challenges of pregnancy and childbirth.
Limitations
The finding lacks comparison from other happiness assessment methods.
There was no more literature for comparison of the result.
The questionnaire is difficult to understand for respondents and took more time.
Acknowledgments
Our deepest gratitude goes to study participants, data collectors, supervisors, and Debre Tabor University.
Author Contributions
DT, WA, AD, and MT conceptualized the idea, and DT, MT, BK, SA, and BA analyzed and wrote the original draft. DT and SA supervised the overall study. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was obtained from any external organization for this research; it was supported by Debre Tabor University.
Disclosure
The authors declared that they have no conflicts of interest in this work.
References
1. Delle Fave A, Brdar I, Freire T, Vella-Brodrick D, Wissing M. The eudaimonic and hedonic components of happiness: qualitative and quantitative findings. Soc Indic Res. 2010;100(2):185–207. doi:10.1007/s11205-010-9632-5
2. Massimini F, Delle Fave DA. Individual development in a bio-cultural perspective. Am Psychol. 2000;55(1):24–33. doi:10.1037/0003-066X.55.1.24
3. Arthur MS. The lost meaning of ‘the pursuit of happiness. William Mary Q. 1964;326–327.
4. McMahon DM. From the happiness of virtue to the virtue of happiness: 400 BC-AD 1780. Daedalus. 2004;133(2):5–17. doi:10.1162/001152604323049343
5. Honkanen HK, Honkanen R, Viinamki H, Heikkilä K, Kaprio J, Koskenvuo M. Life satisfaction and suicide: azo-year follow-up study. Am J Psychiatry. 2001;158(3):433–439. doi:10.1176/appi.ajp.158.3.433
6. Yang Y. Long and happy living: trends and patterns of happy life expectancy in the US, 1970–2000. Soc Sci Res. 2008;37(4):1235–1252. doi:10.1016/j.ssresearch.2007.07.004
7. Pursuit of Happiness. Aristotle [Internet]; 2014 [
8. Diener E. Subjective well-being: the science of happiness and a proposal for a national index. Am Psychol. 2000;55(1):34–43. doi:10.1037/0003-066X.55.1.34
9. Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological wellbeing. J Pers Soc Psychol. 1989;57(6):1069–1081.
10. Seligman M. Can happiness be taught? Daedalus. 2004;133(2):80–87. doi:10.1162/001152604323049424
11. Oates M. Normal’s emotional changes in pregnancy and the puerperium. Baillíeres Clin Obstet Gynaecol. 1989;3(4):791–804. doi:10.1016/S0950-3552(89)80065-3
12. Kiehl E, White M. Maternal adaptation during childbearing in Norway, Sweden, and the United States. Scand J Caring Sci. 2003;17(2):96–103. doi:10.1046/j.1471-6712.2003.00116.x
13. Hagstrom P, Wu S. Are pregnant women happier? Racial differences in the relationship between pregnancy and life satisfaction; 2010. Available from: http://mpra.ub.uni-muenchen.de/24853.
14. Sable MR, Libbus MK. Pregnancy intention and pregnancy happiness: are they different? Matern Child Health J. 2000;4(3):191–197.
15. Direkvand-Moghadam A, Delpisheh A, Direkvand-Moghadam A. Effect of infertility on the quality of life, a cross-sectional study. J Clin Diagn Res. 2014;8(10):OC13–15.
16. Sabatini F. The relationship between happiness and health: evidence from Italy. Soc Sci Med. 2014;114:178–187. doi:10.1016/j.socscimed.2014.05.024
17. Blake SM, Kiely M, Gard CC, El-Mohandes AA, El-Khorazaty MN, Initiative ND. Pregnancy intentions and happiness among pregnant black women at high risk for adverse infant health outcomes. Perspect Sex Reprod Health. 2007;39(4):194–205. doi:10.1363/3919407.
18. Lobel M, DeVincent C, Kaminer A, Meyer B. The impact of prenatal maternal stress and optimistic disposition on birth outcomes in medically high-risk women. Health Psychol. 2000;19(6):544. doi:10.1037/0278-6133.19.6.544
19. Sandman C, Glynn L, Schetter C, et al. Elevated maternal cortisol early in pregnancy predicts third-trimester levels of placental corticotropin-releasing hormone (CRH): priming the placental clock. Peptides. 2006;27(6):1457–1463. doi:10.1016/j.peptides.2005.10.002
20. Gorsuch R, Key M. Abnormalities of pregnancy as a function of anxiety and life stress. Psychosom Med. 1974;36(4):352–362. doi:10.1097/00006842-197407000-00009
21. Yali A, Lobel M. Stress-resistance resources and coping in pregnancy. Anxiety Stress Coping. 2002;15(3):289–309. doi:10.1080/1061580021000020743
22. Costa D, Rippen N, Drita M, Ring A. Self-reported leisure-time physical activity during pregnancy and relationship to psychological well-being. J Psychosom Obstet Gynaecol. 2003;24(2):111–119. doi:10.3109/01674820309042808
23. Mehrdad A. Factors affecting happiness: a cross-sectional study in the Iranian youth. J Clin Diagn Res. 2016;10(5):VC01–VC03.
24. Patra A, Suar D. Factors influencing happiness & satisfaction in single & dual-career families. Indian J Ind Relat. 2009;44(4):
25. Madhavanprabhakaran GK, D’Souza MS, Nairy KS. Prevalence of pregnancy anxiety and associated factors. Int J Africa Nurs Sci. 2015;3:1–7. doi:10.1016/j.ijans.2015.06.002
26. Cordero JM, Salinas-Jiménez J, Salinas-Jiménez MM. Exploring factors affecting the level of happiness across countries: a conditional robust nonparametric frontier analysis. Eur J Oper Res. 2016. doi:10.1016/j.ejor.2016.07.025.
27. Lancaster C, Gold K, Flynn H, Yoo H, Marcus S, Davis M. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5–14. doi:10.1016/j.ajog.2009.09.007
28. Steinecker NLM, Magnier AKAM, Robert JCS, Ibanez NGG. Factors influencing the quality of life of pregnant women: a systematic review. BMC Pregnancy Childbirth. 2018;18(1):455. doi:10.1186/s12884-018-2087-4
29. Hills P, Argyle M. The Oxford happiness questionnaire: a compact scale for the measurement of psychological well‐being. Pers Individ Dif. 2002;33(7):1073–1082. doi:10.1016/S0191-8869(01)00213-6
30. Jayasvasti K, Kanchanatawan B. Happiness and related factors in pregnant women. J Med Assoc Thai. 2005;88:220–225.
31. Singh N, Khan I. Self acceptance and happiness: a study on gender differences among school Teachers. Int J Educ Soc Dev. 2013;4(1):55–60.
32. Hasnain N, Wazid S, Hasan Z. Optimism, hope, and happiness as correlates of psychological well-being among young adult Assamese males and females. IOSR J Humanit Soc Sci. 2014;14(2, Ver. II):44–51. doi:10.9790/0837-19224452
33. Joseph J, Joseph M. Emotional competency and happiness among teacher trainees. Guru J Behav Suc Sci. 2013.
34. Asl S, Bakhtiari M, Raufi A, Yousefi V, Poursalman M, Ahmadi S. Happiness and related factors in infertile women. Int J Adv Stud Humanit Soc Sci. 2013;1(8):1166–1173.
35. Abdullah H, Li L, Yee O. Happiness quotient of upper secondary school students. Int J Phys Soc Sci. 2011;1(4):37–57.
36. WHO. Intimate partner and sexual violence against women: factsheets. Available from: http://www.who.int/mediacentre/factsheets/fs239/en/.
37. Worku AG, Yalew AW, Afework MF. Factors affecting the utilization of skilled maternal care in Northwest Ethiopia: a multilevel analysis. BMC Int Health Hum Rights. 2013;13(20). doi:10.1186/1472-698X-13-20
38. Lyubomirsky S, King L, Diener E. The benefits of frequent positive affect: does happiness lead to success? Psychol Bull. 2005;131(6):803–855. doi:10.1037/0033-2909.131.6.803
39. Steptoe A, Wardle J, Marmot M. Positive affect and health-related neuroendocrine, cardiovascular, and inflammatory processes. Proc Natl Acad Sci U S A. 2005;102(18):6508–6512. doi:10.1073/pnas.0409174102
40. Sable MR, Stockbauer JW, Schramm WF, Land GH. Differentiating the barriers to adequate prenatal care in Missouri, 1987–88. Public Health Rep. 1990;105(6):549–555.
41. Sable MR, Wilkinson DS. Pregnancy intentions, pregnancy attitudes, and the use of prenatal care in Missouri. Matern Child Health J. 1998;2(3):155–165. doi:10.1023/A:1021827110206
42. Sable MR, Spencer JC, Stockbauer JW, et al. Pregnancy wantedness and adverse pregnancy outcomes: differences by race and medicaid status. Fam Plann Perspect. 1997;29(2):76–81. doi:10.2307/2953366
43. Lagadec N, Steinecker M, Kapassi A, et al. Factors influencing the quality of life of pregnant women: a systematic review. BMC Pregnancy Childbirth. 2018;18(1):55.
44. Maulik DEV. Fetal growth restriction: the etiology. Clin Obstet Gynecol. 2006;49(2):228–235. doi:10.1097/00003081-200606000-00006
45. Hashemi Asl BM, Golmakani N, Shakeri MT, Sadjadi A. The level of happiness in pregnancy and its related factors in pregnant women of Mashhad city in 2013. Iran J Obstet Gynecol Infertil. 2015;17(137):19–27.
46. Gebuza G, Kaźmierczak M, Mieczkowska E, Gierszewska M, Kotzbach R. Life satisfaction and social support received by women in the perinatal period. Adv Clin Exp Med. 2014;23(4):611–619. doi:10.17219/acem/37239
47. Pishgar F, Soleyman-Jahi S, Pishgar F, Ardebili HE, Jamal A, Arab A. Level of happiness and its determining factors in pregnant women: a cross-sectional study. J Reprod Infant Psychol. 2016;34(5):431–441. doi:10.1080/02646838.2016.1222071
48. Hallal FC, Murray J, László M. Happiness and depression in adolescence after maternal smoking during pregnancy: birth cohort study. PLoS One. 2013;8(11):e80370. doi:10.1371/journal.pone.0080370.
49. Piccinino LJ, Peterson LS. Ambivalent attitudes and unintended pregnancy. In: Miller WR, Severy LJ, editors. Advances in Population: Psychosocial Perspectives. Vol. 3. London: Jessica Kingsley Publishers; 1999:227–249.
50. Able MR, Libbus MK. Pregnancy intention and pregnancy happiness: are they different? Matern Child Health J. 2000;4(3):191–196. doi:10.1023/A:1009527631043
51. Trussell J, Vaughan B, Stanford J. Are all contraceptive failures unintended pregnancies? Evidence from the 1995 national survey of family growth. Fam Plann Perspect. 1999;31(5):
52. Pakseresht S, Nejad TM, Khalesi ZB, Roshan ZA, Soleimani R. Predictors of happiness among pregnant women: a regression analysis Sedigheh Pakseresht. Electron Physician. 2019;11(4):7629–7635. doi:10.19082/7629
53. Pico-Alfonso MA, Garcia-Linares MI, Celda-Navarro N, et al. The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. J Womens Health (Larchmt). 2006;15(5):599–611. doi:10.1089/jwh.2006.15.599
54. Scheffer Lindgren M, Renck B. ‘It is still so deep-seated, the fear’: psychological stress reactions as consequences of intimate partner violence. J Psychiatr Ment Health Nurs. 2008;15(3):219–228. doi:10.1111/j.1365-2850.2007.01215.x
55. Nixon RD, Resick PA, Nishith P. An exploration of comorbid depression among female victims of intimate partner violence with posttraumatic stress disorder. J Affect Disord. 2004;82(2):315–320. doi:10.1016/j.jad.2004.01.008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.