")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Level of Good Adherence on Option B+ PMTCT and Associated Factors Among HIV Positive Pregnant and Lactating Mothers in Public Health Facilities of Ilu Abba Bor and Buno Bedele Zones, Oromia Regional State, Southwestern Ethiopia, 2018
Authors Yeshialem Asefa E , Edosa Dirirsa D
Received 29 September 2020
Accepted for publication 18 November 2020
Published 27 November 2020 Volume 2020:12 Pages 789—798
DOI https://doi.org/10.2147/HIV.S283184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Eyosiyas Yeshialem Asefa,1 Dejene Edosa Dirirsa2
1Department of Midwifery, College of Health Science, Debre Birhan University, Debre Birhan, Ethiopia; 2Department of Midwifery, Public Health, and Medical Science Faculty, Mettu University, Mettu, Ethiopia
Correspondence: Eyosiyas Yeshialem Asefa Email [email protected]
Background: PMTCT programs help safe delivery practices and recommended infant feeding, as well as providing ART for infants exposed to HIV after birth for prevention and effective treatment. PMTCT service helps to reduce about 1.4 million HIV infections among children between 2010 and 2018. This study aimed to assess the good adherence level and associated factors of option B+ PMTCT among HIV-positive pregnant and lactating women in public health facilities of Ilu Abba Bor and Buno Bedele zones, Oromia regional state, Southwestern Ethiopia 2018.
Methodology: Institutional-based cross-sectional study design was implemented to investigate the level of good adherence to option B+ PMTCT and possible predictors. A simple random sampling technique was used to interview a total of 180 mothers using the interviewer-guided questionnaire for data collection. Data were entered into EpiData version 3.1 and analyzed by SPSS version 23.0 statistical software. Descriptive statistics and logistic regression were computed to identify and see the relative effect of predictors on the outcome variable.
Results: In this study, 146 (81.1%) of the study participants had good adherence to PMTCT option B+. Women who received social and financial support from friends, family members, and partners had good adherence to PMTCT option B+ than their counterparts. Similarly, women who disclosed their HIV status to others had good adherence than those who did not expose their status to their friends and parents.
Conclusion and Recommendation: This study identified the overall level of PMTCT option B+ adherence level in the study area to be good compared to the national and some other findings. Providing support and encouraging a woman for disclosing their HV status for partners and families are very important to increase the adherence level of option B+.
Keywords: adherence, HIV, lactating women, social support, disclosure
Introduction
Background
Despite the significant changes, 740,000 women of reproductive age acquire HIV in 2016. About 73% of these women reside in 23 countries, where the vast majority are in sub-Saharan Africa.1 Even though the main mode of HIV transmission is through unsafe sexual practice, a significant number of HIV infections occurred by vertical transmission i.e. From mother to child (MTCT). MTCT is when a baby acquired HIV from a mother during pregnancy, childbirth, or breastfeeding.2
Although new HIV infections among children declined by 60% in the 21 Global Plan priority countries, 110,000 new HIV infections occurred in the 21 there 2015 and 150,000 globally.3 The rate of vertical transmission at 6 weeks was 5% among 21 global plan countries, but this rose to 14% at the end of breastfeeding. So, reduced adherence and retention during the period of breastfeeding results in twice as many new pediatrics HIV infections as during pregnancy, labor, and delivery.4
PMTCT programs help safe delivery practices and recommended infant feeding, as well as providing ART for infants exposed to HIV after birth for prevention and effective treatment. PMTCT service helps to reduce about 1.4 million HIV infections among children between 2010 and 2018.5
In 2017, about 80% of HIV positive pregnant women were receiving ART which was a significant increase from 51% during 2010.5 In low- and middle-income countries, there is very limited access for receiving HIV prevention and treatment services for women to prevent their children and themselves even though, the life of a mother and a child has the same value, irrespective of where she or he is born and lives.6 Half (52%) of 1.8 million children having HIV were getting ART by 2017. Of those who did not access effective ART treatment, 110,000 lost their life because of AIDS-related illnesses.7
World health organization’s 2013 policy calls for universal use of ART during pregnancy, regardless of HIV disease stage or degree of immunodeficiency (WHO) called “Option B+”8 PMTCT (Option B+) providing not only similar triple ARV medications to every HIV-reactive pregnant women but also it is lifetime care for all women. Option B+ helps as a simplification of drug regimen and service delivery and harmonization with ART programs, PMTCT in future pregnancies, helps to prevent transmission to serodiscordant partners and avoiding stopping and starting of ARV drugs.9
Women living with HIV have had to repress poor health and systemic discrimination while trying to overcome different challenges related to HIV. Many HIV positive women refused to use prevention of mother to child transmission (PMTCT) of HIV services because of different barriers like long-distance from service facilities, poor quality and integration of services to prevent vertical transmission within MCH services, and fear of stigma and discrimination.10
The level of retention to option B+ PMTCT in Africa was reported to be 72.9% for a woman on the follow-up of <12 months and 76.4% at 12 months for studies reporting ≥12 months of follow up. Younger age, starting PMTCT on the same day as diagnosis, initiating during pregnancy versus breastfeeding, and initiating late in the pregnancy were identified factors. Adherence was also affected by stigma, fear of disclosure, and lack of social support.11
In Ethiopia, vertical transmission accounts for more than 95% of pediatrics HIV infections. Despite PMTCT programs in Ethiopia, attrition, and loss to follow-up (LTF) are continued to be high, threatening the effectiveness of PMTCT intervention.12
Different studies from different part of our country showed a different level of Good PMTCT option B+ adherence; East Showa (82.6%), Hadiya zones (83.7%) east Wollega (84.6%), northeast Ethiopia (83.5%), Mekelle (87.1%) and south Wollo zone (87.9%).13–17
Unlike other parts of Ethiopia, there is no available data about the level of good adherence to PMTCT option B+ and related predictors in our study area. Therefore; this study aimed to assess good adherence and associated factors of PMTCT option B+ among HIV positive pregnant and lactating women in public health facilities of Ilu Abba Bor and Buno Bedele zones, Oromia regional state, southwestern Ethiopia 2018.
Methods
Study Design and Period
Institutional based cross-sectional study design was implemented from February 1 to March 30, 2018.
Study Setting
The study was conducted in Ilu Abba Bor and Buno Bedelle zones, two of the twenty- zones of Oromia regional state, southwestern Ethiopia. The capital towns of Ilu Aba Bor and Buno Bedelle zones are Mettu and Bedele which are located in southwestern Ethiopia at 600 KM and 483KM from the capital city of Ethiopia, Addis Ababa respectively. There are three public hospitals (Metu Karl Referral Hospital, Darimu, and Bedele Primary hospitals) and 37 health centers) in the two zones. All of the public hospitals and health centers in these zones provide PMTCT services. The study was conducted in randomly selected 2 public hospitals and 11 health centers.
All selected pregnant and lactating women on PMTCT option B+ follow up for at least one month at public health facilities of Illu Abba Bor and Buno Bedelle zones were our study population. Pregnant or lactating women who were on PMTCT follow up critically ill or those who could not communicate during the data collection period were excluded from this study.
Sample Size Determination and Sampling Technique
Sample size (n) was determined based on a single population proportion formula using the proportion of good adherence of option B+ PMTCT of 87.1% from a study conducted Mekelle, Tigray regional state18 With consideration of the level of confidence (α) 0.05, (Z (1 -α/2) = 1.96); and the margin of error was taken as 0.05. Accordingly, the final sample size was 190 after adding 10% for the non-response rate.
Public health care facilities in Ilu Abba Bor and Buno Bedelle zones were stratified as public hospitals and health centers. By taking at least 30% of the facilities to be representative, two of the public hospitals and 11 health centers in zones were randomly selected by a simple random sampling technique. The calculated sample was distributed to each selected health facility proportionally. The participants from each facility were selected using a simple random sampling technique using the available registration logbook as a frame.
Data Collection Tools and Procedures
Data was collected by interviewer-administered questionnaire prepared in the local language afaan Oromo after being translated from the English version questionnaire. The tool included questions to address; Socio-demographic characteristics, Knowledge about HIV/AIDS, MTCT and PMTCT, Health care provider and health service characteristics, HIV and ART history of pregnant mothers, Adherence level measuring questions, Clinical condition, and Reasons for Adherence and non-adherence. The tool was pretested on 5% of the total sample at non-selected health facilities.
We used 13 data collectors and 5 supervisors after providing one-day Training on the objective of the research and content of data collection tool. Data collectors oriented about the objective of the study for eligible individuals and requested them informed written consent. Witnessed verbal consent was used for participants who cannot read and write. An exit interview was conducted after their PMTCT schedule visit using the above-mentioned data collection tool at a separate area prepared for this purpose around the waiting hall of each health facility.
Measurement
Good Adherence
We used self-reporting from A women regarding their experience with the ART medication using the following 4 questions. A woman was considered as having good adherence if she responded “No” to all (four) questions prepared to assess the adherence level. These questions were;
- Do you sometimes find it difficult to remember to take your medication?
- When you feel better, do you sometimes take a break from your medication?
- Many patients have trouble taking their ARV doses as prescribed; did you miss any ARV doses in the last 3 days?
- Sometimes if you feel worse when you take the medicine, do you stop taking it?
Poor Adherence
A woman was considered as having poor adherence if she responded “Yes” to at least one of the above questions.14
Data Processing and Analysis
Collected Data was entered into EpiData version 3.1 and exported to SPSS version 23.0 for analysis. Frequencies were used to see the overall distribution of the study subjects concerning the variables under the study. Bivariate logistic regressions were used to select important variables candidate for the multivariate logistic regression. Finally, multivariable Logistic regressions were used to assess the relative effect of independent variables on dependent variables and to select important predictors of the level of PMTCT option B+ adherence included in the model. Odds Ratio (OR) and their 95% Confidence Interval (CI) were used to measure the association. A significance level of 0.05 was used to decide the significance of statistical tests. Finally, the results are presented in text and tables.
Ethical Consideration
A letter of Ethical clearance was secured from the Research Ethics Committee (REC) of Mettu University. A letter of permission was obtained from the Zonal Health Bureau and each facility administrations. Informed written consent were obtained from study subjects and from their parents for those with age below 18. Participants had the right to self-determination regarding participation in research, both initially and during the research. For confidentiality purposes, the names of the participant were not included in the questionnaire. The collected data were kept confidential and used only for the study. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of Respondents
A total of 190 respondents were planned to be interviewed. However, about 180 pregnant women on option B+ PMTCT drugs were interviewed regarding their good ART level of adherence with an overall response rate was 95%. Concerning the age category of respondents 58 (32.2%) of them belong to the age group of 20–24 while 48 (26.7%) of them belong to the age group 30–34. The mean age of the participants was 27.2 years with SD ± 6.2. One hundred fifteen (78.8%) of the respondents were urban residents. More than half of the participants 96 (53.3%) were Muslim religious followers and 66 (36.7%) of study participants cannot write and read. Regarding their occupation, more than half of 100 (55.6%) of the respondents were housewives and the majority of the 118 (65.6%) were living with their husbands/partners at the time of the study period (See Table 1).
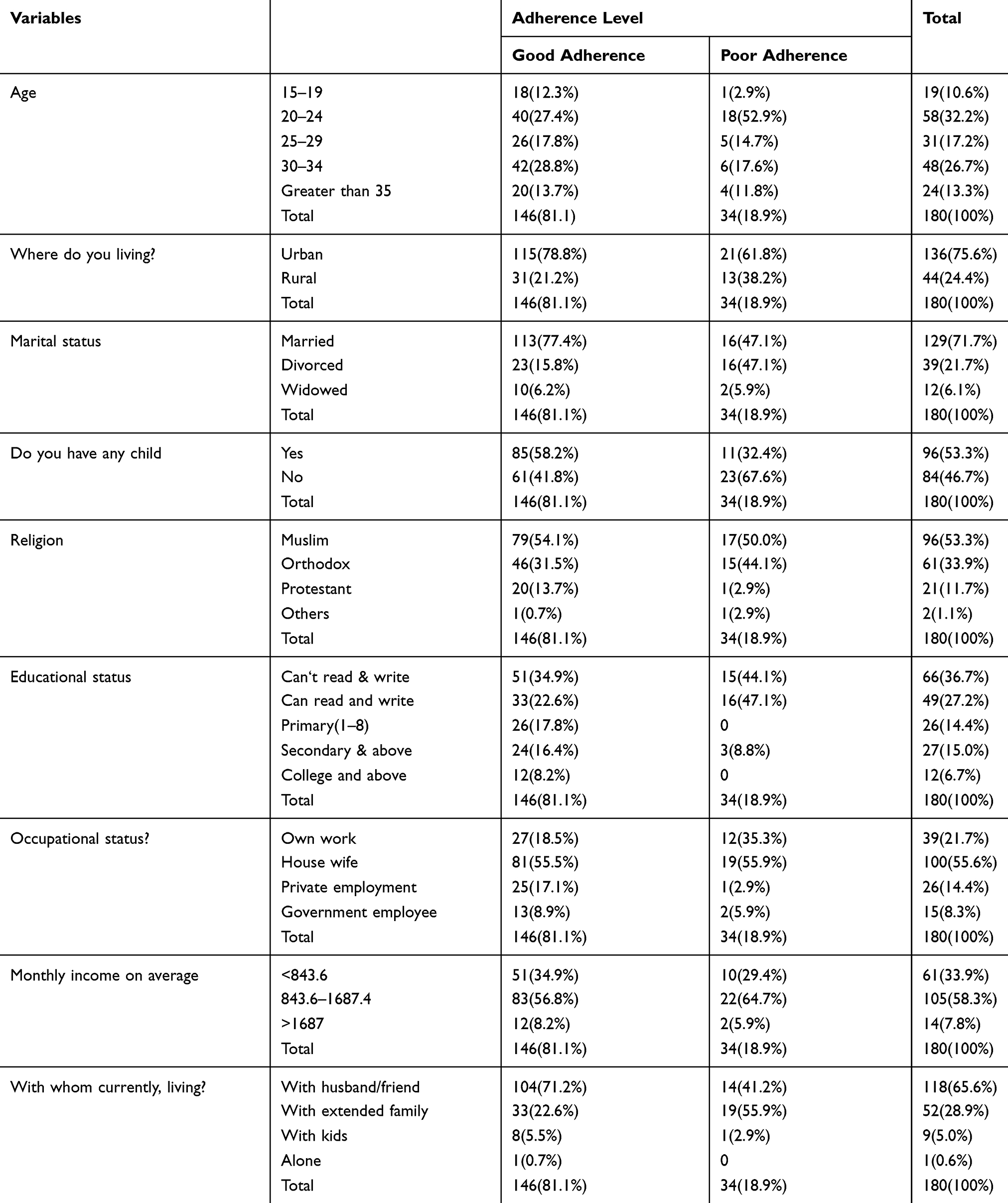 |
Table 1 Socio-Demographic Characteristics of Pregnant and Lactating Women on Option B+ PMTCT in Ilu Abba Bor and Buno Bedelle Zones, Oromia, Ethiopia, 2018 |
Knowledge About HIV/AIDS, MTCT, and PMTCT
The majority of the respondents, 145 (80.6%), perceived that HIV-infected pregnant women can transmit HIV to her unborn baby. Additionally, 113 (77.4%) of respondents with Good adherence and 13 (38.2%) of participants with poor-adherence believed that PMTCT drugs used by mothers can decrease transmission of HIV from or to their partner (See Table 2).
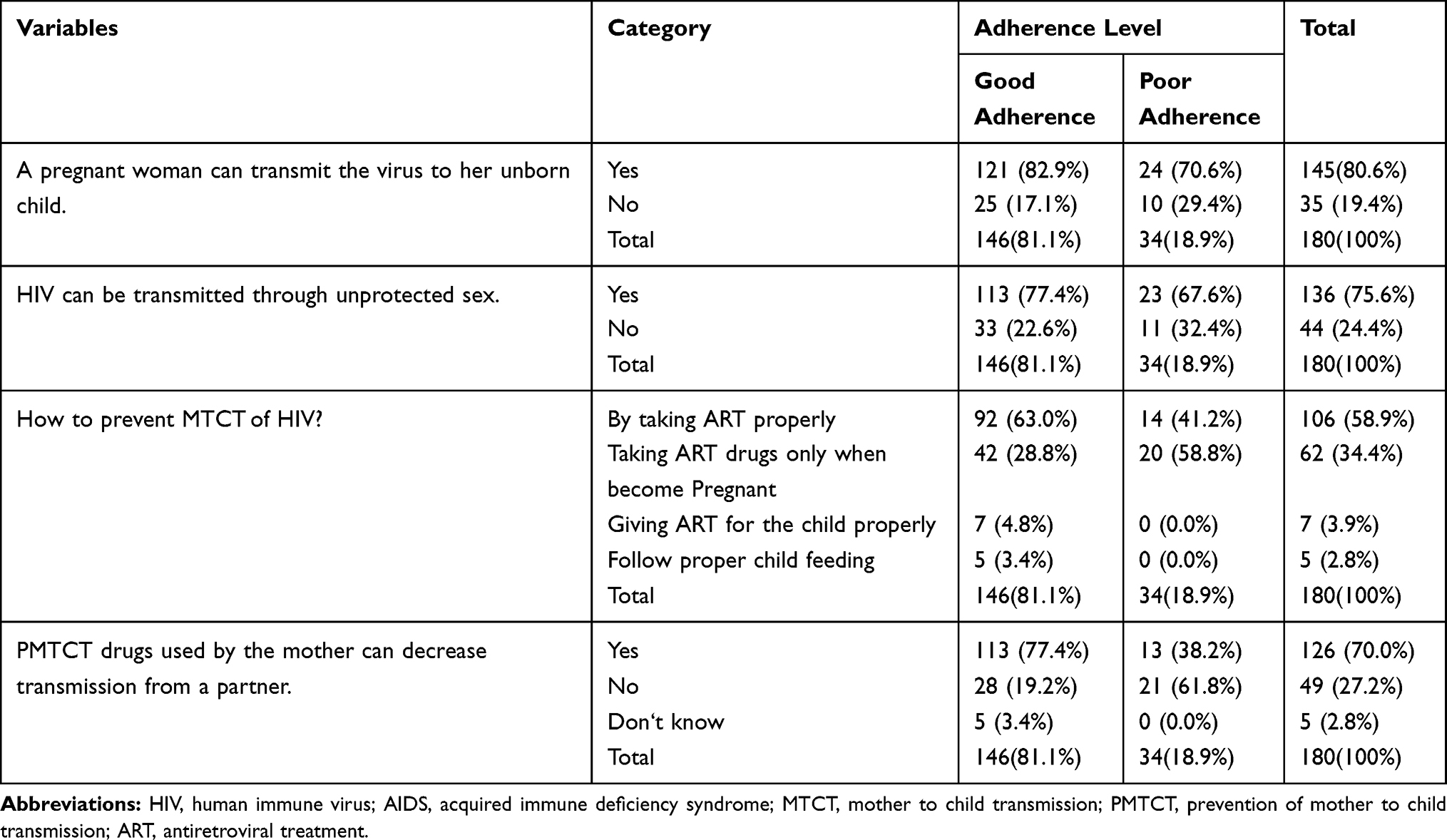 |
Table 2 Knowledge About HIV/AIDS, MTCT, and PMTCT Among Pregnant and Lactating Women on Option B+ at Ilu Abba Bor and Buno Bedelle Zones, Oromia, Ethiopia, 2018 |
HIV, ART and Health Care System-Related Characteristics
One hundred twenty-seven (70.6%) of study participants believe that the health care providers were trustable and 129 (71.7%) of them describe their care provider as sociable. The majority of the respondents, 125 (69.4%) started their ART drugs by an informed decision from health care providers while 103 (57.2%) of the study participants spent less than an hour walking on foot to reach health care facilities for their follow up. Regarding the time of their HIV status diagnosis, the majority of the study participants 93 (51.7%) knew their HIV status before being pregnant. More than half of the respondents, 118 (65.6%), started their ART drugs during the second trimester (13–28 weeks) of their pregnancy. About 84 (57.5%) of adherent and 15 (44.1%) of non-adherent women received financial and social support from partners (See Table 3).
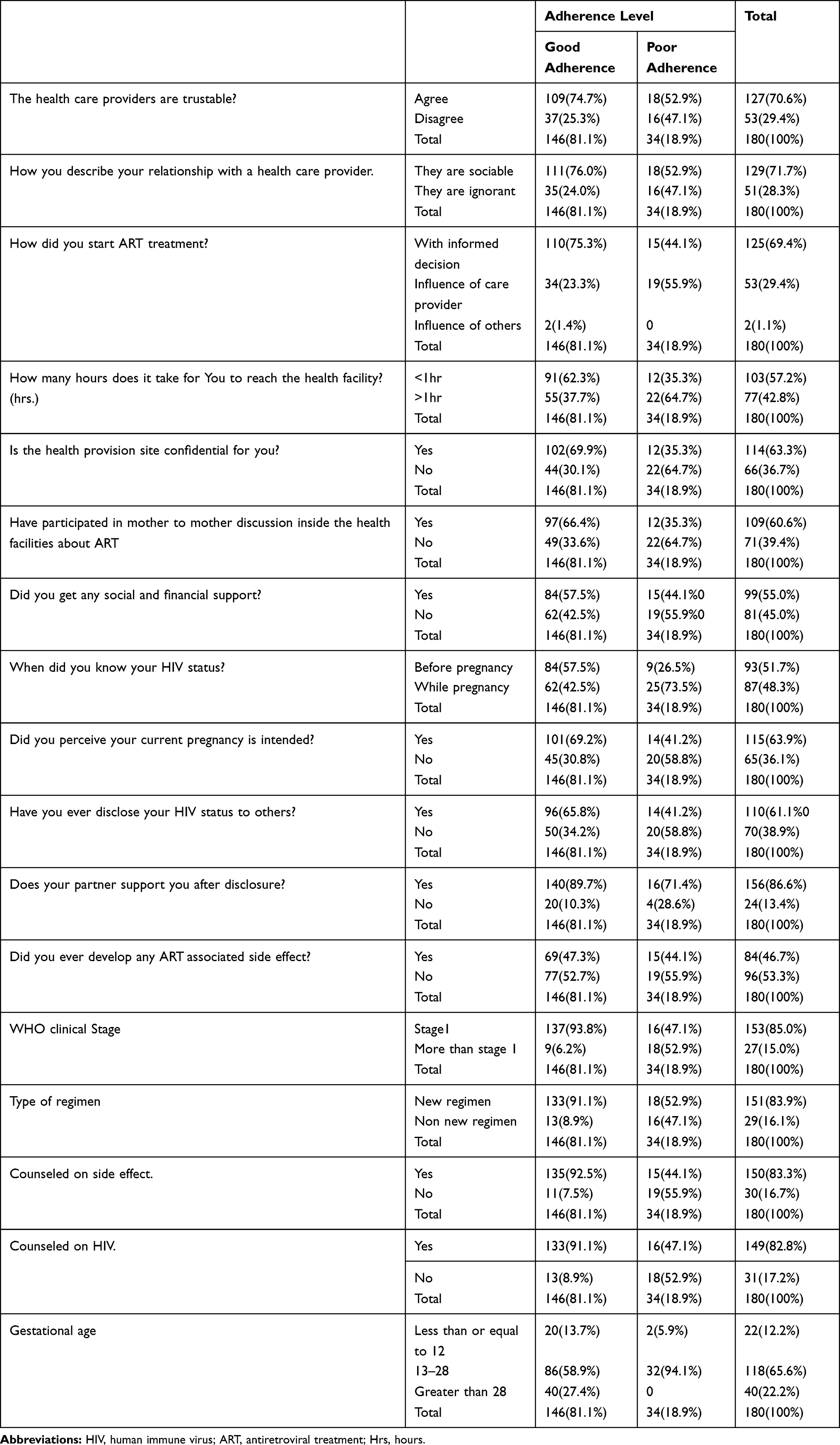 |
Table 3 HIV, ART, and Health Care System-Related Characteristics Among Pregnant and Lactating Women on Option B+ at Ilu Abba Bor and Buno Bedelle Zones, Oromia, Ethiopia, 2018 |
Level of Adherence to Option B+ PMTCT Drugs
The total level of good adherence on PMTCT option B+ measured using the four questions as described on method section was 146 (81.1%) while 34 (18.9%) of participants found to have poor adherence.
Self-reporting from participants indicate that, 96.11% answered “No” to the question “Do you sometimes find it difficult to remember to take your medication?” while 93.33% of them gave negative response for the question “When you feel better, do you sometimes take a break from your medication?”. Additionally, 95% and 96.66% of the respondents replay “No” for questions “Many patients have trouble taking their ARV doses as prescribed; did you miss any ARV doses in the last 3 days?” and “Sometimes if you feel worse when you take the medicine, do you stop taking it?” respectively.
Predictors of Option B+ PMTCT Adherences
To identify the significant predictors, initially, all independent variables were analyzed with the dependent variable. Then, a variable with a p-value less than 0.25 were included in multivariate logistic regression analysis to control the effect of other covariates. Accordingly, about nine variables were entered into multivariate logistic regression analysis. Finally, women who received Social and financial support were 5 times more likely to be adherent with PMTCT option B+ than their counterparts with AOR= 5 [95% CI; 1.8–17]. The study also revealed that respondents who disclosed their HIV status to others (partner, family, friends) have good adherence than those who did not disclose their HIV status, [AOR= 2 (95% CI; 1.8, 2.5)] (See Table 4).
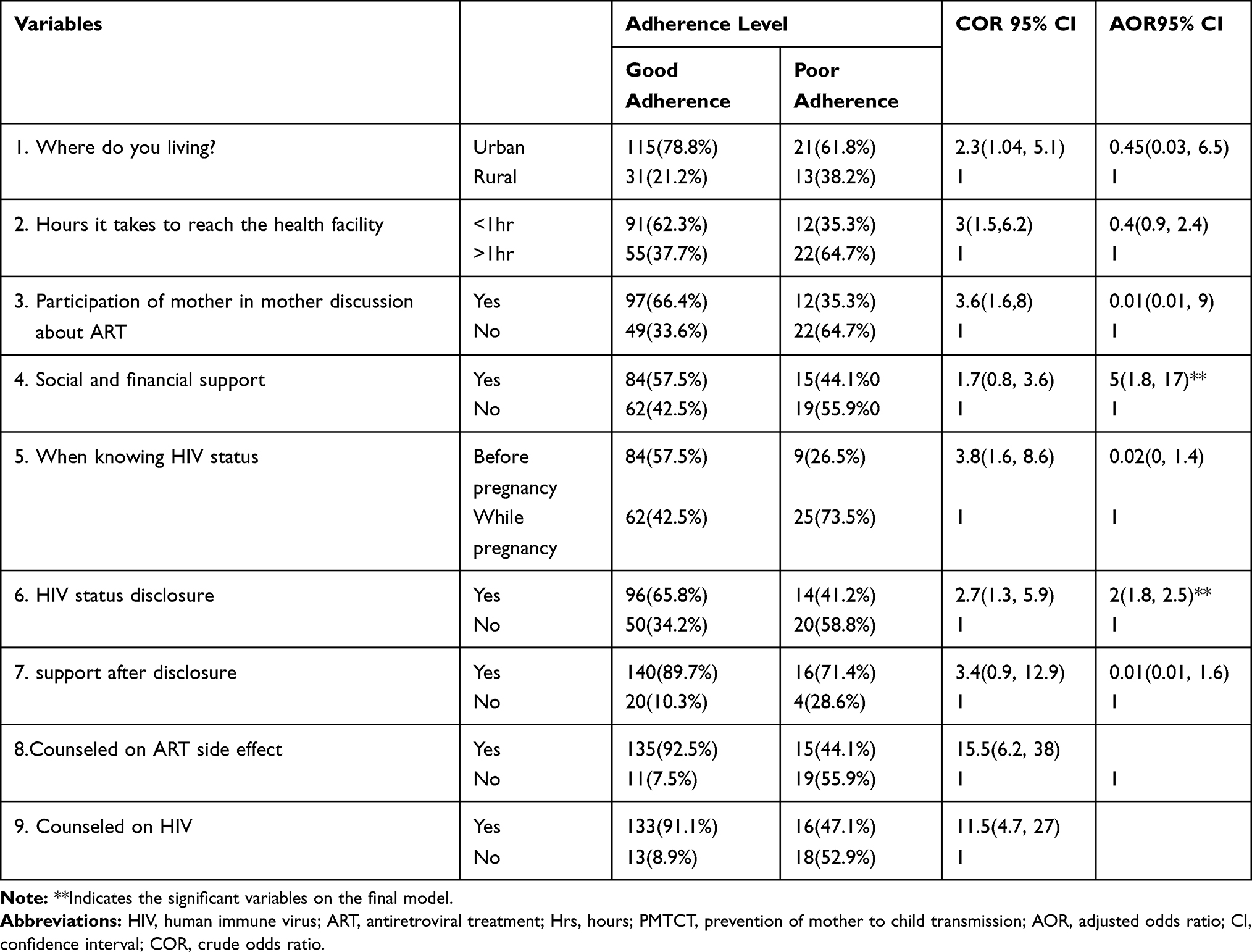 |
Table 4 Predictors of Option B+ PMTCT Adherence Among Pregnant and Lactating Women on Option B+ at Ilu Abba Bor and Buno Bedelle Zones, Oromia, Ethiopia, 2018 |
Discussion
In this study, the level of good adherence was found among 146 respondents (81.1%) of the study participants. This level of adherence is similar to the study conducted in East Showa and Hadiya zones which account for 82.6% and 83.7% respectively.13,14 The finding was also consistent with a study done in the east Wollega zone and northeast Ethiopia, where the level of loss to follow up of option B+ is 15.4% and 16.5% respectively.15,16
The finding is higher than the level of adherence from systemic review and meta-analysis showing the pooled adherence of patients with a good adherence rate of (76.1%) in low income and middle-income countries and (62.0%) in high-income countries.19 This variation might be from the difference in the study setting. Similarly, this finding was higher than a study done in Tanzania, East Gojjam zone, and western Uganda showing Good adherence to option B+ PMTCT drugs of 26.3%, 75%, and 51% respectively.20–22 This difference might be, because of the difference in study setting like a study done in western Uganda measures the adherence level only for postpartum women.
On the other hand, the overall adherence level of this study is less than the result reported by the study conducted in Mekelle and south Wollo zone which was; 87.1 and 87.9%.17 This discrepancy might be due to; the study conducted in Mekelle town used data from public hospitals only, while our study used hospitals and health centers. There is evidence that women on a follow up at primary health care facilities such as health centers are less adherent to ART medications than those on a follow up at hospitals,23 probably because of better counseling services in the hospitals. This finding also lesser than a study conducted in western Uganda where the median adherence of Option B+ during pregnancy was 95.7% pill intake.24 The reason for this discrepancy might be because the study in Uganda indicates only among pregnant women.
Women who received Social and financial support from partner, family, and others were 5 more likely to have good adherence than those who had no social and financial support. This study finding is in line with the result reported by the two studies conducted in East Shewa,13 Indonesia,25 and Tanzania,20 which shows having treatment supporters from partner, family, friends, relatives, government or non-governmental organizations enhances ART drug adherence. This might be due to the usual benefit of financial supports for moral encouragement and health care assistance through transportation and reminders.26
The study also showed that respondents who disclosed their HIV status to others (partner, family, friends) were 2 times more likely to have good adherence than those who did not disclose their HIV status, [AOR 2 (95% CI; 1.8, 2.5)]. This finding is consistent with studies done in rural Uganda,27 Malawi,28 Kenya,29 Tigray,18 east Shewa zone,13 east Wollega,15 Amhara region,30 western Ethiopia31 and Hadya zone14 indicating that HIV status disclosure to partner, family, friend, and significant others had a statistically significant association with ART adherence.
Limitation of This Study
We used self-reporting to measure the adherence level. It is important to state that self-reporting used to measure adherence level might be prone to bias.
Conclusion and Recommendation
This study identified the overall level of PMTCT option B+ adherence level in the study area to be good compared to the national and some other findings. But this should not take an acceptable level by the stakeholders where their target to be 100% based on the consequences of defaulting from the care.
The health professionals and other stakeholders should periodically assess the client’s PMTCT option B+ adherence at every visit and intervene accordingly. Encouraging the women to disclose their HIV status to their parents, inform and come along with a treatment supporter (partners, family, or others) for the counseling sessions would help in educating the treatment supporters appropriately and improving adherence in the long run.
Families, community leaders, non-governmental organizations, health administration, and other government organizations should identify HIV positive women who require social and financial support and facilitate it.
We recommend researchers to do a further study using advanced study design and multiple methods of adherence measurement.
Abbreviations
AOR, adjusted odds ratio; BSc, Bachelor of Science; CI, confidence interval; COR, crude odds ratio; SD, standard deviation; WHO, World Health Organization; SPSS, statistical package for social science; PMTCT, prevention of mother to child transmission; HIV, human immune virus; AIDS, acquired immune deficiency syndrome.
Data Sharing Statement
The data utilized for this study are available from the corresponding author upon reasonable request.
Acknowledgment
First of all, we would like to thank God for giving us the courage and wisdom to do our work. Then, we would like to mention and pass our thanks to Mettu University, faculty of public health and medical science & the department of Midwifery for giving this chance. We extend our deepest gratitude to our friends and colleagues for giving us materials, their guidance in our overall work, and also for their irreplaceable support and sharing their experience. We finally thank zonal health departments and respective health facility officials for permitting us to do so as well as involved data collectors and supervisors for their commitment during the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The whole required (material and humanitarian) cost for this research work was covered by Mettu University.
Disclosure
The authors report no conflicts of interest for this work.
References
1. HIV/AIDS JUNPo. Start Free Stay Free AIDS Free–2017 Progress Report. Geneva: UNAIDS; 2018.
2. Shaw GM, Hunter E. HIV transmission. Cold Spring Harb Perspect Med. 2012;2(11):a006965. doi:10.1101/cshperspect.a006965
3. Haroz D, von Zinkernagel D, Kiragu K. Development and impact of the global plan. J Acquir Immune Defic Syndr. 2017;75(1):S2. doi:10.1097/QAI.0000000000001318
4. HIV/AIDS UNPo. Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping Their Mothers Alive. Joint United Nations Programme on HIV/AIDS (UNAIDS); 2011.
5. UNAIDS. Miles to Go. Global AIDS Update 2018. Geneva: UNAIDS; 2018.
6. HIV/AIDS JUNPo. Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping Their Mothers Alive: 2011–2015. Geneva, Switzerland: UNAIDS; 2011:2016.
7. AIDSinfo U. Country Fact Sheet. Lao PDR UNAIDS; 2017.
8. Organization WH. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. World Health Organization; 2016.
9. World Health Organization (WHO). Update WP. Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants. Geneva, Switzerland; 2012.
10. Ababa A. Ethiopia. 2013. Available from: https://wfphaconfexcom/wfpha/2012/webprogram/Paper10587html.
11. Knettel BA, Cichowitz C, Ngocho JS, et al. Retention in HIV care during pregnancy and the postpartum period in the Option B+ era: a systematic review and meta-analysis of studies in Africa. J Acquir Immune Defic Syndr. 2018;77(5):427. doi:10.1097/QAI.0000000000001616
12. Krebs LD Ethiopia’s prevention of mother-to-child transmission (pmtct) programs: addressing attrition and loss to follow-up. 2012.
13. Tarekegn M, Baru A, Seme A. Levels of option B+ ART drugs adherence and associated factors among pregnant women following ART services at public health facilities of East Shawa Zone, Oromia, Ethiopia. Sex Reprod Healthc. 2019;22:100459. doi:10.1016/j.srhc.2019.100459
14. Lodebo TM, Suloro JA. Level of adherence and associated factors to option B+ PMTCT among HIV positive pregnant women in Hadiya Zone, Southern Ethiopia. Glob J Health Sci. 2017;2(1):39–58.
15. Tolossa T, Mulisa D, Fetensa G, Fekadu G. Magnitude and factors associated with lost to follow-up among women under option B+ PMTCT program at East Wollega public health facilities, Western Ethiopia. Int J Africa Nurs Sci. 2020;13:100212. doi:10.1016/j.ijans.2020.100212
16. Mitiku I, Arefayne M, Mesfin Y, Gizaw M. Factors associated with loss to follow-up among women in Option B+ PMTCT programme in northeast Ethiopia: a retrospective cohort study. J Int AIDS Soc. 2016;19(1):20662. doi:10.7448/IAS.19.1.20662
17. Tsegaye D, Deribe L, Wodajo S. Levels of adherence and factors associated with adherence to option B+ prevention of mother-to-child transmission among pregnant and lactating mothers in selected government health facilities of South Wollo Zone, Amhara Region, northeast Ethiopia, 2016. Epidemiol Health. 2016;38:e2016043. doi:10.4178/epih.e2016043
18. Ebuy H, Yebyo H, Alemayehu M. Level of adherence and predictors of adherence to the option B+ PMTCT programme in Tigray, northern Ethiopia. Int J Infect Dis. 2015;33:123–129. doi:10.1016/j.ijid.2014.12.026
19. Nachega JB, Uthman OA, Anderson J, et al. Adherence to antiretroviral therapy during and after pregnancy in low-, middle and high income countries: a systematic review and meta-analysis. AIDS. 2012;26(16):2039. doi:10.1097/QAD.0b013e328359590f
20. Zacharius KM, Basinda N, Marwa K, Mtui EH, Kalolo A, Kapesa A. Low adherence to Option B+ antiretroviral therapy among pregnant women and lactating mothers in eastern Tanzania. PLoS One. 2019;14(2):e0212587. doi:10.1371/journal.pone.0212587
21. Demelash Y, Abebe N, Sharew Y, Mehare T. Adherence of Option B+ prevention of mother-to-child transmission program and its associated factors among pregnant and lactating mothers in public health facilities of East Gojjam zone, Amhara region, Ethiopia, 2017. Int J. 2019;5(10):301.
22. Decker S, Rempis E, Schnack A, et al. Prevention of mother-to-child transmission of HIV: postpartum adherence to Option B+ until 18 months in Western Uganda. PLoS One. 2017;12(6):e0179448. doi:10.1371/journal.pone.0179448
23. Ekama S, Herbertson E, Addeh E, et al. Pattern and determinants of antiretroviral drug adherence among Nigerian pregnant women. J Pregnancy. 2012;2012.
24. Schnack A, Rempis E, Decker S, et al. Prevention of mother-to-child transmission of HIV in option B+ era: uptake and adherence during pregnancy in Western Uganda. AIDS Patient Care STDS. 2016;30(3):110–118. doi:10.1089/apc.2015.0318
25. Lumbantoruan C, Kermode M, Giyai A, Ang A, Kelaher M. Understanding women’s uptake and adherence in option B+ for prevention of mother-to-child HIV transmission in Papua, Indonesia: a qualitative study. PLoS One. 2018;13(6):e0198329. doi:10.1371/journal.pone.0198329
26. Organization WH. Towards the Elimination of Mother-To-Child Transmission of HIV: Report of a WHO Technical Consultation. Vol. 2011. November 9–11, 2010. Geneva, Switzerland.
27. King R, Matovu JN, Rujumba J, et al. PMTCT option B+ 2012 to 2018—taking stock: barriers and strategies to improve adherence to option B+ in urban and rural Uganda. Afr J AIDS Res. 2020;19(2):135–146. doi:10.2989/16085906.2020.1760325
28. Elwell K. Facilitators and barriers to treatment adherence within PMTCT programs in Malawi. AIDS Care. 2016;28(8):971–975. doi:10.1080/09540121.2016.1153586
29. Moth IA, Ayayo A, Kaseje D. Assessment of utilisation of PMTCT services at Nyanza Provincial Hospital, Kenya. SAHARA J. 2005;2(2):244–250. doi:10.1080/17290376.2005.9724847
30. Kassaw M, Matula S, Mamo A, Kassie A, Abate B. The perceived determinants and recommendations by mothers and healthcare professionals on the loss-to-follow-up in option B+ program and child mortality in the Amhara Region, Ethiopia. BMC Infect Dis. 2020.
31. Tolossa T, Kassa GM, Chanie H, Abajobir A, Mulisa D. Incidence and predictors of lost to follow-up among women under option B+ PMTCT program in western Ethiopia: a retrospective follow-up study. BMC Res Notes. 2020;13(1):18. doi:10.1186/s13104-019-4882-z
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.