")
Back to Journals » Clinical Optometry » Volume 12
Level of Glaucoma Drug Adherence and Its Associated Factors Among Adult Glaucoma Patients Attending Felege Hiwot Specialized Hospital, Bahir Dar City, Northwest Ethiopia
Authors Assem AS , Fekadu SA , Yigzaw AA, Nigussie ZM , Achamyeleh AA
Received 1 August 2020
Accepted for publication 10 October 2020
Published 27 October 2020 Volume 2020:12 Pages 189—197
DOI https://doi.org/10.2147/OPTO.S274850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Abel Sinshaw Assem,1 Sofonias Addis Fekadu,1 Amsal Ambaw Yigzaw,2 Zelalem Mehari Nigussie,3 Anemaw Asrat Achamyeleh3
1Department of Optometry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Ophthalmology, Felege Hiwot Specialized Hospital, Bahir Dar, Ethiopia; 3Department of Epidemiology and Biostatics, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Abel Sinshaw Assem Tel +251912857435
Email [email protected]
Background: Glaucoma is a chronic optic nerve disease, often asymptomatic in an early stage, which is usually associated with elevated intraocular pressure. Good adherence to ocular hypotensive agents is essential to control the intraocular pressure and optic nerve damage. There is limited information on glaucoma drug adherence and associated factors in Ethiopia, particularly in the study area.
Objective: To determine the level of glaucoma drug adherence and associated factors among adult glaucoma patients attending Felege Hiwot Specialized Hospital, Northwest Ethiopia, 2019.
Materials and Methods: A hospital-based cross-sectional study was conducted at Felege Hiwot specialized Hospital from March 2019 to May 2019. A systematic random sampling method was used to select 402 study participants. A structured questionnaire was prepared, and adherence was assessed by using self-report questions. The collected data were entered into Epi data version 4.2.2.1 and exported into Statistical Package for Social Science version 23 for analysis. Tables, graphs, frequency, mean, and standard deviation were used for descriptive statistics. Variables with a p-value of < 0.2 in the bivariable logistic regression were entered in the multivariable logistic regression, and variables with a p-value of < 0.05 under multivariable analysis were taken as statistically significant factors for glaucoma drug adherence.
Results: Among a total of 390 study participants, 212 (56.2%) were adherent to their topical medication. Early glaucoma (AOR=2.8: 95% CI =1.29– 5.91), normal vision (AOR=1.9: 95% CI=1.15– 3.09), urban residence (AOR=1.6: 95% CI=1.03– 2.51), family support (AOR=1.7: 95% CI=1.06– 2.76) and information from pharmacist (AOR=1.8: 95% CI=1.11– 2.99) were significantly associated with adherence.
Conclusion: The level of glaucoma drug adherence was 56.2% among patients attending Felege Hiwot Specialized Hospital. Early glaucoma, normal visual acuity, family support, information on medication from the pharmacist, and urban residence were positively associated with adherence.
Keywords: glaucoma, adherence level, Bahir Dar, Ethiopia
Introduction
Glaucoma is a progressive optic nerve damage that leads to irreversible visual loss and it is the second leading cause of blindness worldwide.1 It is characterized by changes in the optic disc and visual field defect with a progressive loss of retinal ganglion cells. The common risk factors for glaucoma include raised intraocular pressure (IOP), age, family history, and ethnicity.2
According to the reports of World Health Organization (WHO), 285 million people were visually impaired and 39 million people were blind in 2010. Glaucoma accounts for 8% of blindness and 2% of visual impairment globally.3 In Ethiopia, glaucoma is the most common cause of irreversible blindness which was estimated as 62,000 people were blind.4
Adherence is generally defined as the extent to which patients take medications as prescribed by their eye care providers.5 Generally, glaucoma drug adherence and associated factors were classified into four general groups. These are; patient-related, medication-related, provider-related, and situational/environmental-related factors.6 Adherence to long-term therapy for chronic diseases in developed countries averages 50% and is much lower in developing countries. A systematic review conducted in Latin American on adherence to glaucoma medication rate varies from 4.6% to 59%7 and in the United States of America it ranges from 51% to 56%.8 Poor adherence is a worldwide problem that compromises the effectiveness of treatment, quality of life, and health economics.9
Even though WHO plans to avoid preventable blindness, but still there is a problem with glaucoma drug adherence in developing countries including Ethiopia10–12 that brought them to be visually impaired. Adherence is one of the major problems in glaucoma management due to the asymptomatic nature of the disease condition at an earlier stage. Medication nonadherence is a growing concern to health-care systems, physicians, and other stakeholders due to increasing prevalence associated with adverse outcomes and higher costs of eye care service.13
If appropriate, effective, and successful treatment is provided; blindness secondary to Glaucoma is preventable. Patient adherence to the medication is a major challenge that is now recognized as an essential component of treatment.14 The primary objective of glaucoma therapy is to prevent progressive vision loss and blindness by lowering intraocular pressure.15 Intraocular pressure lowering can be achieved by eye medication, laser treatment, surgery, or any combination of modalities. Topical medication is the first management of choice to reduce IOP by enhancing aqueous outflow and/or reducing aqueous production. Long-term adherence to ocular hypotensive medication is crucial to limit glaucoma disease progression.16,17
Nonadherence among glaucoma patients has been reported to be from 5% to 80% in different studies. Patients with poor adherence to topical glaucoma medication have worse outcomes with a higher rate of visual loss and increased health-care costs.14 Nonadherence to ocular hypotensive medication in Ethiopia ranges from 39.60%18 to 67.5%.10 Although numerous socioeconomic factors are associated with poor adherence, those factors must be addressed at the societal level. Maximizing patient adherence to medication has the potential to reduce the number of surgical interventions required to treat glaucoma, prevent unnecessary vision loss, and save the overall healthcare system cost in the long run.14,19 Therefore, this study aimed to assess the level of glaucoma drug adherence and factors associated with it among adult glaucoma patients attending Felege Hiwot Specialized Hospital. The finding of this study will provide baseline evidence to eye care professionals for their clinical practice and knowledge of the factors for poor adherence serve as an entry point for future interventions to increase adherence level to glaucoma medication.
Materials and Methods
Study Design, Setting, and Period
Institutional-based cross-sectional study was conducted at Felege Hiwot Specialized Hospital, Bahir Dar city, from March to May 2019. Bahir Dar is the capital city of the Amhara National Regional State, which is located 556 kilometers Northwest from Addis Ababa, the capital city of Ethiopia. Felege Hiwot Specialized Hospital is one of the largest referral hospitals in the Amhara National Regional State. The hospital provides comprehensive eye care services including; major surgeries, minor surgeries, glaucoma follow-up, general outpatient, and inpatient eye care services for those patients coming from different areas of the country. The eye care professionals involved in the service provision in the hospital include 2 senior ophthalmologists, 1 cataract surgeon, 4 optometrists, 5 ophthalmic officers, 2 BSc (Bachelor of Science), and 5 diploma ophthalmic nurses.
Source and Study Population
All adult glaucoma patients attending Felege Hiwot Specialized Hospital glaucoma clinic were the source population and those adult glaucoma patients attending the glaucoma clinic during the study period were the study population.
Inclusion and Exclusion Criteria
All adult patients aged ≥18 years, with the diagnosis of glaucoma by a senior ophthalmologist, and who had followed up for treatment with one or more topical hypotensive medications in one or both eyes at least for the past 6 months were included in the study. Those who had undergone laser or surgical glaucoma therapy and post-operation follow-up on topical medication like anti-inflammatory drugs other than glaucoma medication were excluded from the study.
Sample Size Determination
A total sample size of 402 was determined with a single population proportion formula by taking a similar study done in Gondar University Referral Hospital (61%)18 and by considering 95% confidence interval, 5% margin of error, and 10% nonresponse rate.
Sampling Technique
A systematic random sampling method was used to select the sample from the study participants with a sampling fraction of six. A total of 2389 glaucoma patients were seen and their medical cards were reviewed between March and May 2019. The sampling interval was calculated to be 2389/402 = 6. A starting point was chosen randomly from numbers 1 to 6 and hence eligible individuals were chosen every six patients at regular intervals from the sampling frame that had to followup at the glaucoma clinic during the data collection period.
Operational Definitions
Adherent to medication: The study participants who scored ≥60% with self-report questions were categorized as adherent and those who scored <60% were categorized as nonadherent to their ocular hypotensive medication.18
Knowledgeable about glaucoma and drug adherence: Those participants who answered ≥ mean of knowledge questions were classified as knowledgeable.
Early glaucoma: the presence of glaucomatous optic nerve head damage but no visual field abnormalities within the central 10° and cup-to-disc ratio (CDR) ≤0.65.1
Moderate glaucoma: optic nerve abnormalities consistent with glaucoma and glaucomatous visual field abnormalities in one hemifield and not within 5° of fixation with moderate glaucomatous disc features of vertical CDR = 0.7–0.85.1
Advanced glaucoma: patients who have CDR of 0.85–0.95 and glaucomatous visual field abnormalities in both hemifields and/or loss within 5° of fixation in at least one hemifield, with the ability of light perception.1
Data Collection Procedures
A structured form of a questionnaire was constructed after thorough literature was searched (Annex 1). The data were collected through face-to-face interview after written informed consent was obtained from each study participant by three experienced ophthalmic nurses. Additionally, a data extraction format was developed to review the chart of each eligible patient to assess the type and stage of glaucoma, IOP, and visual acuity (VA) of study participants. The diagnosis of glaucoma was made by a senior ophthalmologist.
Data Collection Tool
A structured form of self-report questionnaire and data extraction format were used to collect data from the study participants. The questionnaire was used for face-to-face interviews of study participants and the data extraction format was used to collect data from medical cards of study participants to identify the type and severity of glaucoma, IOP level, and visual acuity (Annex 1).
Six questions were developed and consulted by experts of glaucoma managements and researcher to identify adherence of anti-glaucoma medications. Physicians’ comments were also incorporated to approve the questions. Answers “no” was coded as 1, while “yes” was as 0 except for question number 1 in which “yes” was coded as 1 and “no” was 0. The items were then summed to give a range of score from 0 to a maximum score of six. Participants who scored ≥60% with self-report questions were categorized as adherent to their glaucoma medication.
Data Quality Control
The questionnaire was initially prepared in English and translated into local (Amharic) Language. It was then checked for consistency by back-translation to English. To ensure the quality of data, pretest was carried out on 5% of the sample size in Gondar University Referral Hospital. Training had been given for data collectors and the supervisor for one day before data collection and the collected data were checked for completeness, accuracy, and clarity by the principal investigator daily during the data collection period. Then, the necessary correction has been given to the data collectors accordingly to the aim of the study.
Data Processing and Analysis
The collected data were checked, coded, and entered into Epi data version 4.2.2.1 and exported to Statistical Package for Social Science (SPSS) version 23 software for analysis. The descriptive statics were presented via tables, percentages, mean, and standard deviations. Hosmer-Lemeshow goodness of fit was done to check the model assumption of logistic regression (P =0.16). The bivariable analysis was implemented to identify each candidate variables that were associated with adherence level with p-value <0.2. The adjusted odds ratio (AOR) with 95% confidence interval (CI) were used in the multivariable analysis to determine factors associated with glaucoma medication adherence and a p-value <0.05 was considered statistically significant.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 390 study participants were included in the study with a response rate of 97% and a mean age of 59.9 years (±SD of 11). Out of the total study participants, 263 (67.4%) were males. The majority of the respondents 245 (62.6%) were not educated (had no formal education). More than three-fourth 329 (84.4%) of the participants were married and almost all 364 (93.3%) and 377 (96.7%) of the participants were Orthodox Christians and Amhara in ethnicity, respectively. Nearly two-thirds of 253 (64.9%) of the participants had poor knowledge regarding glaucoma and medication adherence (Table 1).
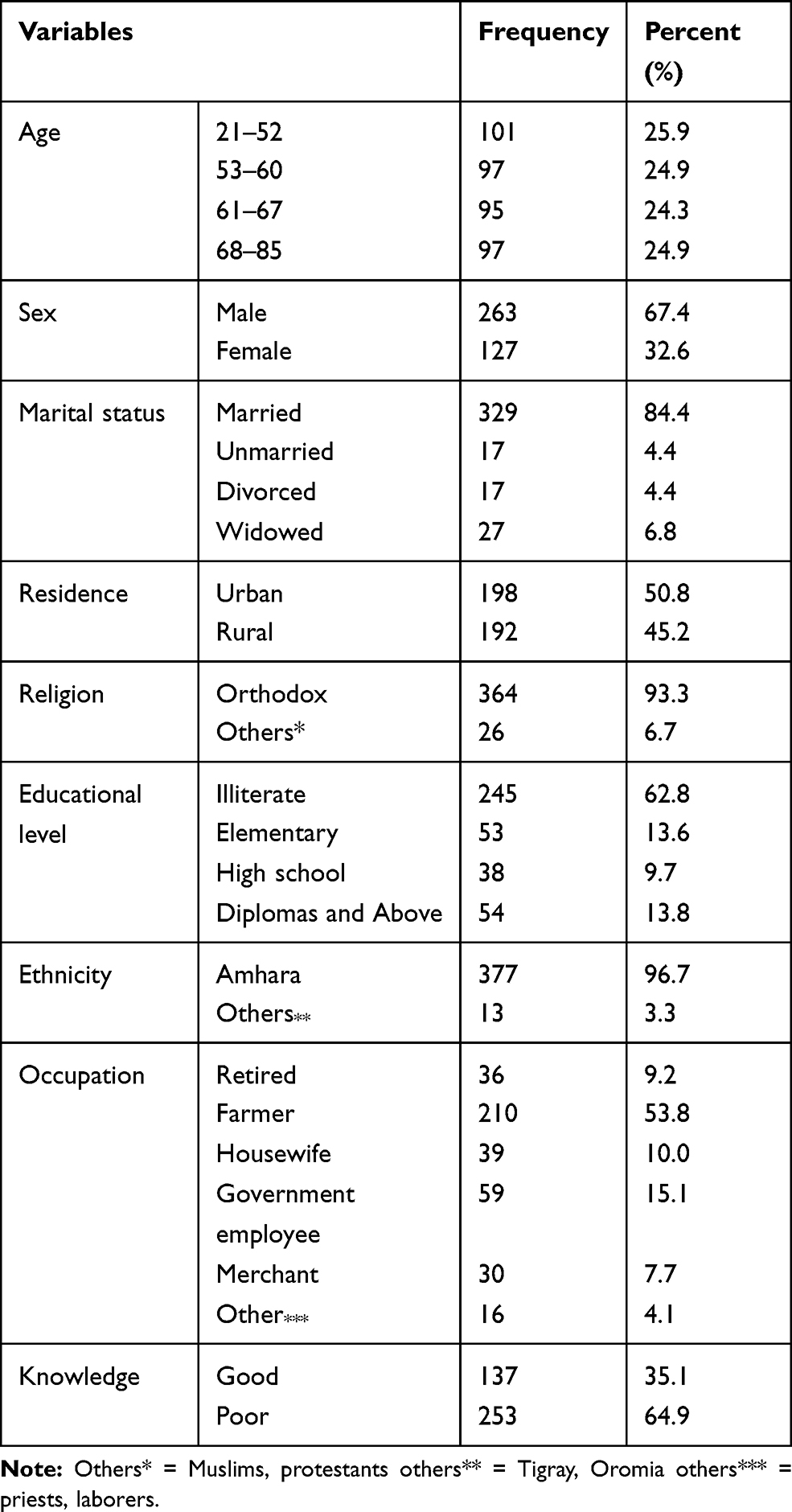 |
Table 1 Socio-Demographic Characteristics of the Study Participants Attending Felege Hiwot Specialized Hospital, Bahir Dar, Northwest Ethiopia, 2019 |
Medication and Situational Related Factors
Three-fourth of the study participants 290 (74.4%) used two types of medications and more than half 225 (57.7%) of the participants obtained their medication free of charge, as well as 262 (67.3%) of the participants, did not get the medication in the hospital at each follow-up time. Almost all 370 (94.9%) of the respondents had not used eye drops other than glaucoma medication and only 75 (19.2%) of participants had major co-morbidity (Table 2).
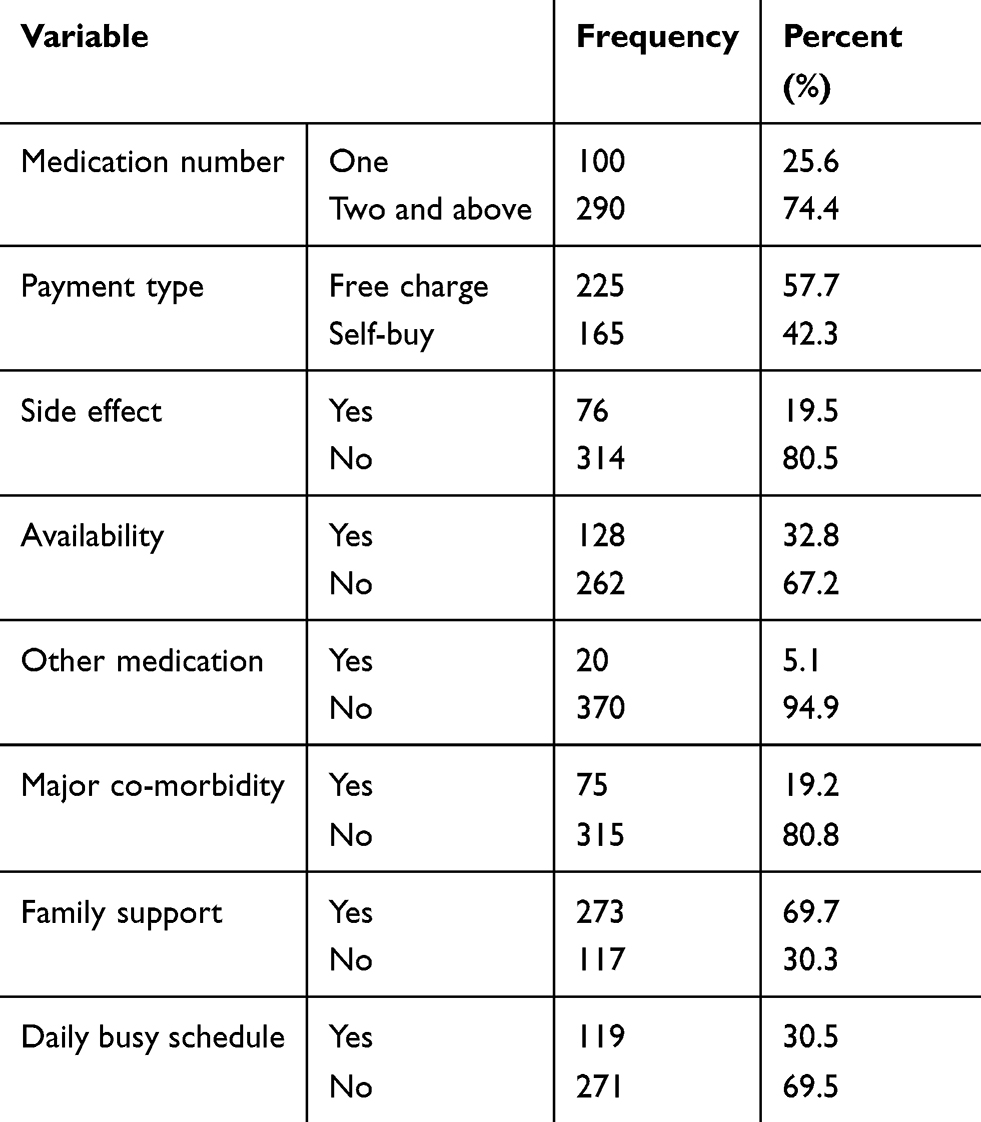 |
Table 2 Medication-Related Factors Among Glaucoma Patients Attending Felege Hiwot Specialized Hospital, Bahir Dar, Northwest Ethiopia, 2019 |
Provider-Related Factors
The majority of the study participants 271 (69.5%) and 287 (73.6%) had got information about medication adherence and how to use their medication from health service providers, respectively (Table 3).
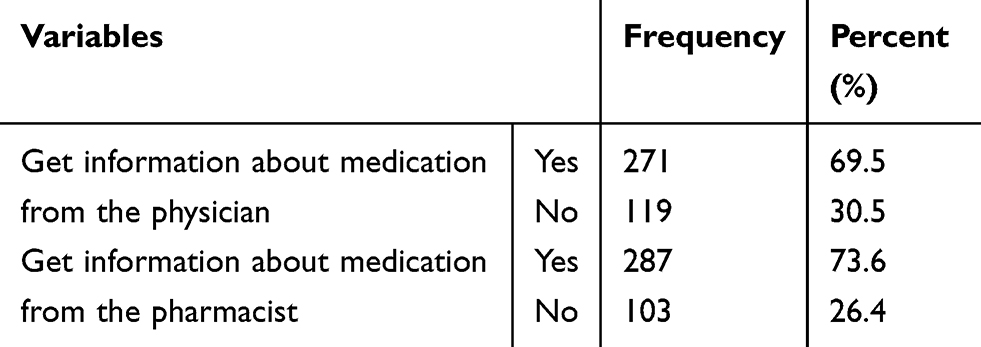 |
Table 3 Provider-Related Factors Among Glaucoma Patients Attending Felege Hiwot Specialized Hospital, Bahir Dar, Northwest, Ethiopia, 2019 |
Glaucoma Related Factors
Most of the participants 327 (83.8%) had primary open-angle glaucoma (POAG) followed by Pseudo-exfoliation glaucoma (PXG) which accounts 39 (10%) based on the type of glaucoma classification. Based on the international council of ophthalmology’s classification of visual acuity, 186 (47.7%) of participants had normal vision, 72 (18.5%) low vision, and 132 (33.8%) were blind (Table 4).
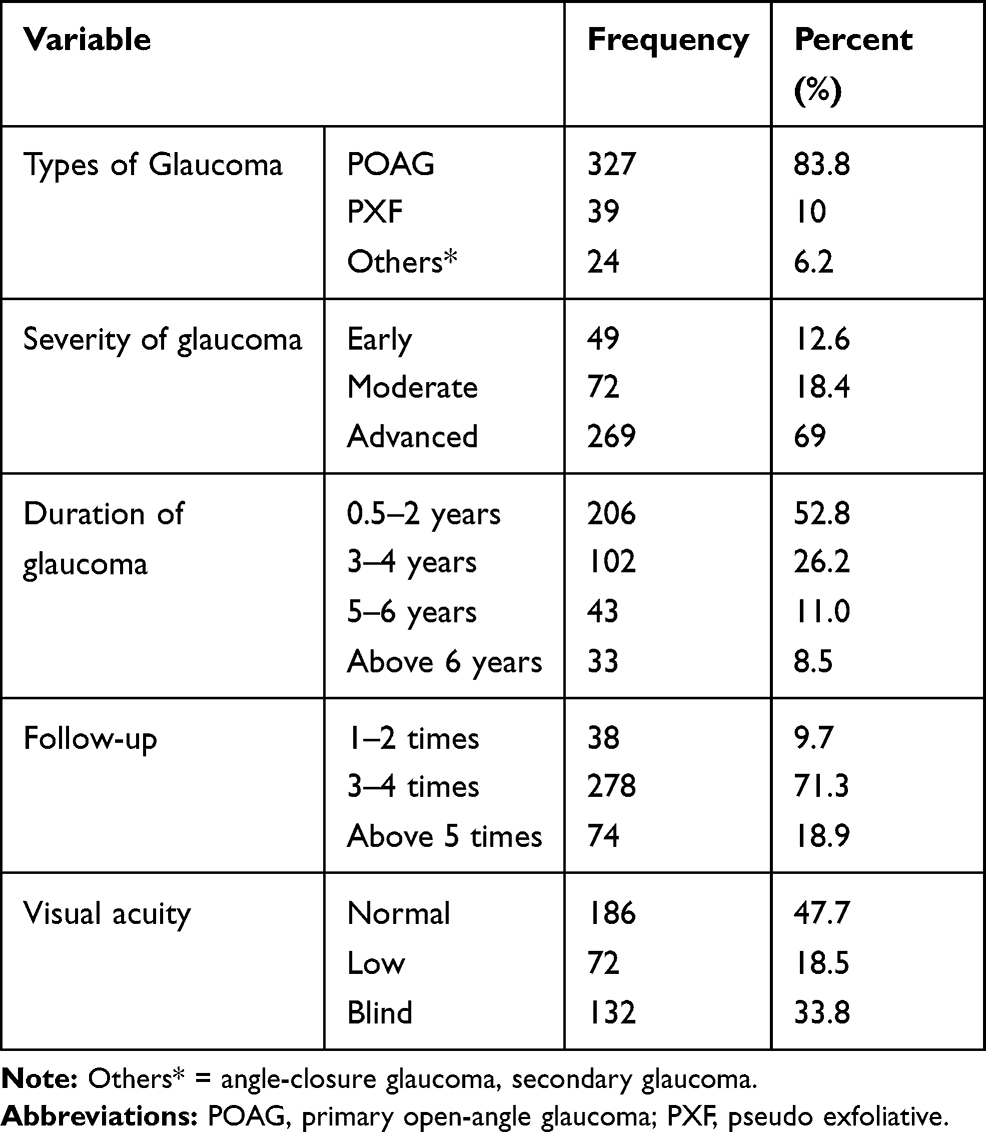 |
Table 4 Glaucoma Related Factors Among Glaucoma Patients Attending Felege Hiwot Specialized Hospital, Bahir Dar, Northwest, Ethiopia, 2019 |
Level of Glaucoma Medication Adherence
Assessment of participants' response to self-report questions revealed that among a total of 390 glaucoma patients, 219 (56.2%) (95% CI: 51–62) participants were adherent to their glaucoma medication.
Factors Associated with Glaucoma Medication Adherence
All independent variables were tested for crude association with level of glaucoma drug adherence using bivariable logistic regression. In multiple logistic analysis, variables including glaucoma severity, visual acuity, family support, residence, and information from pharmacist were significantly associated with glaucoma drug adherence.
The odds of being adherent among urban residences were 1.6 times more as compared to those who were rural residences (AOR=1.6: 95% CI=1.03–2.510). The odds of being adherent among participants who had early glaucoma was 2.8 times more as compared to participants who had advanced glaucoma (AOR=2.8: 95% CI=1.29–5.91). Participants who had normal vision were 1.9 times more adherent to their glaucoma drugs than participants who were blind (AOR= 1.9: 95% CI=1.15–3.09). Besides, the odds of being adherent among participants who had family support were 1.7 times more than those participants who did not have family support (AOR=1.7: 95% CI=1.06–2.76). Glaucoma patients who had got information on medication from the pharmacist were 1.82 times more adherent to their medication than those who had not got information (AOR =1.8: 95% CI=1.11–2.99) (Table 5).
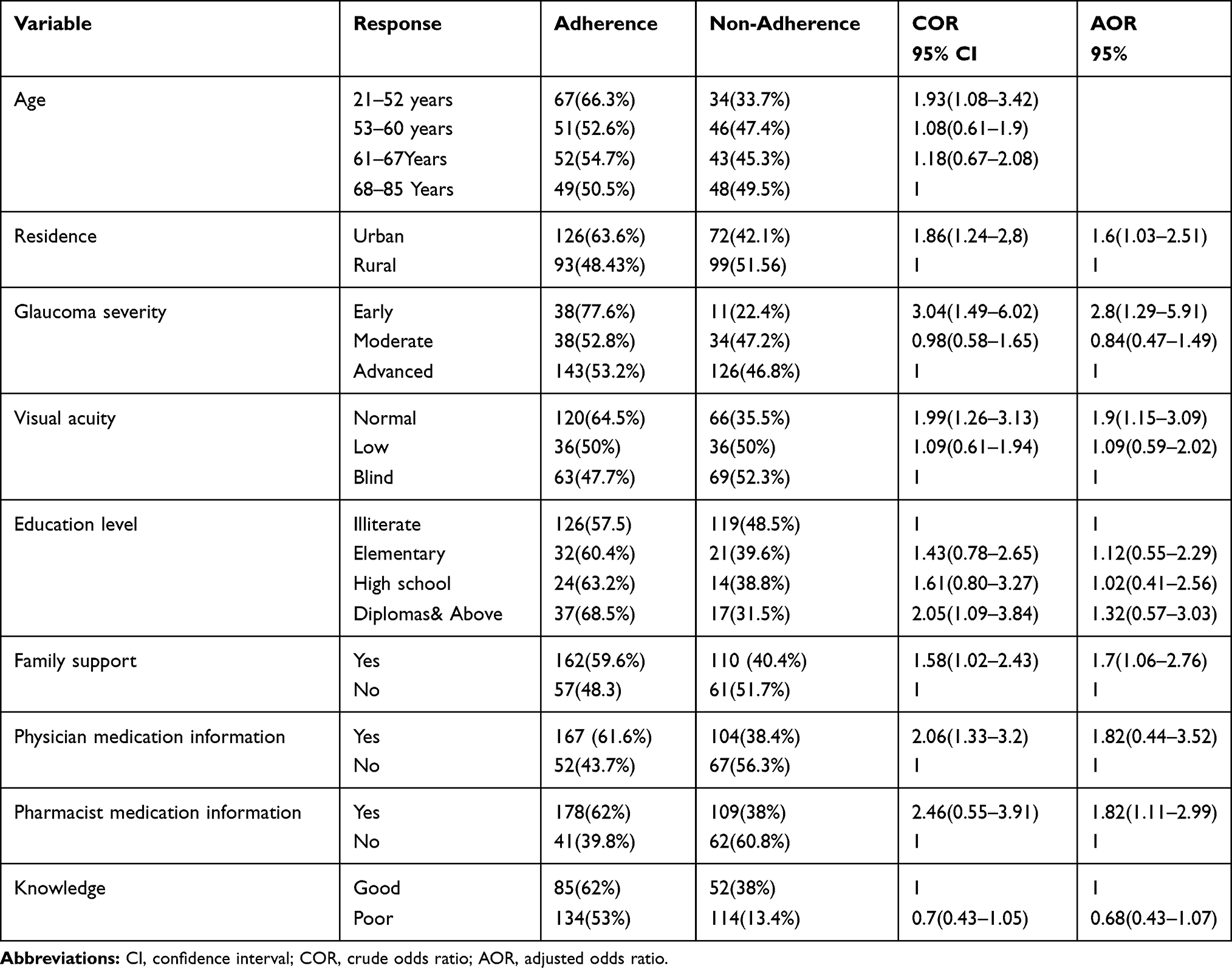 |
Table 5 Factors Associated with Glaucoma Drug Adherence Among Adult Glaucoma Patients Attending Felege Hiwot Specialized Hospital, Bahir Dar, Northwest Ethiopia, 2019 |
Discussion
This study attempted to assess the level of glaucoma drug adherence and its associated factors on patients attending Felege Hiwot Specialized Hospital. The study showed that 219 (56.2%) of the participants were adherent to their ocular hypotensive medication. This result is consistent with a study conducted in Gondar University Hospital, Ethiopia.18 This similarity might be evident owing to the use of a questionnaire for interviewing the patients.
The result of the present study is higher than studies done in Jimma Hospital (32.5%)10 and Menelik Hospital (42.6%).20 This variation might be due to inconsistency of definition given to the level of drug adherence and a study done in Jimma used a small sample size which had only 200 glaucoma patients. This result is also higher than studies done in India (50%),11 Iran (34%),21 Ghana (9.9%),22 Egypt (46.6%),23 and Arab (50%).24 This variation might be due to inconsistency of the definition given for the level of adherence and differences in patients group.
On the other hand, the level of glaucoma drug adherence is lower than studies done in South Korea (72.6%)25 and America (72.5%).26 The possible justification could be due to differences in socioeconomic status and educational level of the participants. Both above studies also assessed the level of adherence by using medication possession ratio and patient data from pharmacy claims to define adherence ratio unlike in our study.
The odds of being adherent to glaucoma medication among urban residences were 1.6 times more as compared to those who were rural residences. This is similar with the study done at Gondar University Hospital, Ethiopia.18 This might be explained by patients who were urban residents have better awareness and knowledge on glaucoma and medication adherence as compared to rural residents. Different mass media agencies that give additional information and promotion of different mechanisms of disease control are functional at urban areas that might in turn increase the adherence level of patients in urban.
The odds of being adherent among participants who had early glaucoma was 2.8 times more as compared to participants who had advanced glaucoma. This is supported by a study conducted in Jimma University Hospital, Southwest Ethiopia.10 This might be because of those patients who had early glaucoma had good vision and are not dependent on others like for medication application and for transportation to a health facilities for follow-up. But, in a study conducted in California, patients who had early glaucoma were less likely to adhere to their medication than those who had advanced disease.27 This variation might be due to the difference in the distribution of disease severity and adherence status. In California, 44% of study participants had mild or moderate glaucoma,27 whereas in this study 12.6% and 18.5% had mild and moderate glaucoma, respectively.
In addition, this study confirmed that glaucoma patients who had normal vision were 1.9 times more adherent to their glaucoma drugs than patients who were blind. This is supported by a study done at Gondar University Hospital, Northwest Ethiopia18 and Brazil, where quality of vision was significantly associated with adherence.28 This might be due to the fact that patients with poor vision are dependent on their activities like for the application of drops and transportation to health institutions for follow-up. Another possible reason could be that patients who had poor vision may perceive no change with topical medication instead needs other options like surgery. Furthermore, those patients who had poor vision might feel hopelessness that might also reduce the adherence level of glaucoma medication. In contrast to this study, a systematic review found that there was no association between visual acuity and adherence to topical medication.29
Participants who had family support were 1.7 times more adherent to their medication than those who had no family support. This result is similar with a study done in Kashan, Iran,21 where lack of family support was associated with poor adherence. This is might be due to family support for patients’ increases the motivation to remember and to take the medication properly that might contribute to increased adherence level of glaucoma medication.
In this study, glaucoma patients who had got information on medication from the pharmacist were 1.8 times more adherent to their medication than those who had not got information. Studies conducted in Iran21 and Saudi Arabia24 also supported this result. This is because patients who had got information on glaucoma and medication from health-care providers may have a better knowledge of disease condition and medication effect, and most patients positively accept what their care providers said to them. Cost of medication, side effects of drops and nonavailability of drops were not associated with adherence. This finding is supported by studies done in Jimma, Southwest Ethiopia10 and Iran.21
Forgetfulness was the most common reason for nonadherence. This is in line with other studies done in different countries.11,23,30,31 The disease condition is painless, progressive, and no immediate disability unless the disease reaches the end stage, due to these reason patients may not consider becoming blind and may not give attention. The other reason might be due to patient's perception of glaucoma as a curable disease after they gain a good vision secondary to mature cataract surgery was done for them.23
Limitation
Difficulty to test the association between intraocular pressure decrement and adherence level due to unavailability of standardized tonometer.
Conclusion
The level of glaucoma drug adherence was 56.2% among patients attending Felege Hiwot Specialized Hospital. Glaucoma severity, normal visual acuity, family support, residence, and information on medication from pharmacist were associated with adherence level. Therefore, awareness creation, health education, and information about medication adherence and disease condition are important. Health-care providers should give due attention and prioritize those identified factors and give frequent counseling regarding the importance of glaucoma drug adherence.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; CDR, cup to disc ratio; IOP, intraocular pressure; WHO, World Health Organization.
Data Sharing Statement
The data will be available upon request from the corresponding author.
Ethical Consideration
Bahir Dar University Ethical Review Board approved the study as per the Declaration of Helsinki. Ethical clearance was obtained from Bahir Dar University, College of Medicine and Health Science, Ethical Review Committee. Written informed consent was obtained from the study participants after a brief explanation of the objective of the study. Any involvement in the study was after their complete consent was obtained. Any participant who was not willing to participate in the study would not be forced to do so. The individual patients not subject to any harm as far as confidentiality was kept.
Consent for Publication
Not applicable.
Acknowledgment
We would like to thank Bahir Dar University College of Medicine and Health Sciences and Felege Hiwot Specialized Hospital for their technical support to perform this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
We, the authors, declare that we have no competing interests.
References
1. Gupta N, Aung T, Congdon N. International council of ophthalmology guidelines for glaucoma eye care. Int Council Ophthalmol. 2016;2–20.
2. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi:10.1001/jama.2014.3192
3. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
4. Giorgis AT. Raising public awareness of glaucoma in Ethiopia. Commun Eye Health J. 2012;25:46.
5. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
6. Stryker JE, Beck AD, Primo SA, et al. An exploratory study of factors influencing glaucoma treatment adherence. J Glaucoma. 2010;19(1):66–72. doi:10.1097/IJG.0b013e31819c4679
7. DeCastro ANBV, Mesquita WA. Noncompliance with drug therapy of glaucoma: a review about intervening factors TT - Abandono do tratamento medicamentoso do glaucoma: uma revisão sobre os fatores intervenientes. Braz J Pharm Sci. 2009;45(3):453–459. doi:10.1590/S1984-82502009000300010
8. Sheer R, Bunniran S, Uribe C, Fiscella RG, Patel VD, Chandwani HS. Predictors of nonadherence to topical intraocular pressure reduction medications among medicare members: a claims-based retrospective cohort study. J Manage Care Spec Pharm. 2016;22(7):808–817a. doi:10.18553/jmcp.2016.22.7.808
9. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
10. Tamrat L, Gessesse GW, Gelaw Y. Adherence to topical glaucoma medications in Ethiopian patients. Middle East Afr J Ophthalmol. 2015;22(1):59–63. doi:10.4103/0974-9233.148350
11. Rajurkar K, Dubey S, Gupta PP, John D, Chauhan L. Compliance to topical anti-glaucoma medications among patients at a tertiary hospital in North India. J Curr Ophthalmol. 2018;30(2):125–129. doi:10.1016/j.joco.2017.09.002
12. Abdull MM, Chandler C, Gilbert C. Glaucoma, “the silent thief of sight”: patients’ perspectives and health seeking behaviour in Bauchi, northern Nigeria. BMC Ophthalmol. 2016;16(1):1–9. doi:10.1186/s12886-016-0220-6
13. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
14. Robin A, Grover DS. Compliance and adherence in glaucoma management. Indian J Ophthalmol. 2011;59(1):93. doi:10.4103/0301-4738.73693
15. Yip JLY, Foster PJ. Ethnic differences in primary angle-closure glaucoma. Curr Opin Ophthalmol. 2006;17(2):175–180. doi:10.1097/01.icu.0000193078.47616.aa
16. McVeigh KA, Vakros G. The eye drop chart: A pilot study for improving administration of and compliance with topical treatments in glaucoma patients. Clin Ophthalmol. 2015;9:813–819.
17. Netland PA. Glaucoma Medical Therapy: Principles and Management. Oxford University Press, USA; 2008.
18. Anbesse DH, Yibekal BT, Assefa NL. Adherence to topical glaucoma medications and associated factors in Gondar University Hospital Tertiary Eye Care Center, northwest Ethiopia. Eur J Ophthalmol. 2019;29(2):189–195. doi:10.1177/1120672118772517
19. Djafari F, Lesk MR, Harasymowycz PJ, Desjardins D, Lachaine J. Determinants of adherence to glaucoma medical therapy in a long-term patient population. J Glaucoma. 2009;18(3):238–242. doi:10.1097/IJG.0b013e3181815421
20. Mehari T, Giorgis AT, Shibeshi W. Level of adherence to ocular hypotensive agents and its determinant factors among glaucoma patients in Menelik II Referral Hospital, Ethiopia. BMC Ophthalmol. 2016;16(1):1–8. doi:10.1186/s12886-016-0316-z
21. Movahedinejad T, Adib-Hajbaghery M. Adherence to treatment in patients with open-angle glaucoma and its related factors. Electron Physician. 2016;8(9):2954–2961. doi:10.19082/2954
22. Ocansey S, Kyei S, Diafo A, Darfor KN, Boadi-Kusi SB, Aglobitse PB. Cost of the medical management and prescription pattern for primary open angle glaucoma (POAG) in Ghana-a retrospective cross-sectional study from three referral facilities. BMC Health Serv Res. 2016;16(1):1–8. doi:10.1186/s12913-016-1528-x
23. Abu Hussein NB, Eissa IM, Abdel-Kader AA. Analysis of factors affecting patients’ compliance to topical antiglaucoma medications in egypt as a developing country model. J Ophthalmol. 2015;2015.
24. Masoud M, Sharabi-Nov A, Pikkel J. Noncompliance with ocular hypertensive treatment in patients with primary open angle glaucoma among the Arab population in Israel: a cross-sectional descriptive study. J Ophthalmol. 2013;2013.
25. Kim CY, Park KH, Ahn J, et al. Treatment patterns and medication adherence of patients with glaucoma in South Korea. Br J Ophthalmol. 2017;101(6):801–807. doi:10.1136/bjophthalmol-2016-308505
26. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122(7):1308–1316. doi:10.1016/j.ophtha.2015.03.026
27. Ung C, Zhang E, Alfaro T, et al. Glaucoma severity and medication adherence in a county hospital population. Ophthalmology. 2013;120(6):1150–1157. doi:10.1016/j.ophtha.2012.11.026
28. Ribeiro MVMR, Ribeiro LEF, Ribeiro ÊAN, Ferreira CV, Barbosa FT. Adherence assessment of eye drops in patients with glaucoma using 8 item Morisky Score: a cross sectional study. Rev Bras Oftalmol. 2016;75(6):432–437. doi:10.5935/0034-7280.20160087
29. Olthoff CMG, Schouten JSAG, Van De Borne BW, Webers CAB. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension: an evidence-based review. Ophthalmology. 2005;112(6):953–961.e7. doi:10.1016/j.ophtha.2004.12.035
30. Tsai T, Robin AL, Smith JP. An evaluation of how glaucoma patients use topical medications: a pilot study. Trans Am Ophthalmol Soc. 2007;105:29–33.
31. Mansberger SL, Sheppler CR, McClure TM, et al. Psychometrics of a new questionnaire to assess Glaucoma adherence: the Glaucoma treatment compliance assessment tool. Trans Am Ophthalmol Soc. 2013;111:1–16.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.