")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Level of Community Readiness for the Prevention of COVID-19 Pandemic and Associated Factors Among Residents of Awi Zone, Ethiopia: A Community-Based Cross-Sectional Study
Authors Adane D, Yeshaneh A , Wassihun B , Gasheneit A
Received 20 January 2021
Accepted for publication 20 March 2021
Published 13 April 2021 Volume 2021:14 Pages 1509—1524
DOI https://doi.org/10.2147/RMHP.S302974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Daniel Adane,1 Alex Yeshaneh,1 Biresaw Wassihun,2 Addisu Gasheneit3
1Department of Midwifery, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2Department of Midwifery, College of Medicine and Health Sciences, Arbaminch University, Arbaminch, Ethiopia; 3Awi Zone Health Office, Amhara Regional State Health Bureau, Bahir Dar, Ethiopia
Correspondence: Alex Yeshaneh Email [email protected]
Background: Novel coronavirus 19 is a contagious disease that affects all most all countries of the world and puts the world in great challenge. Even though, there is a limited testing capacity in Africa the number of cases and deaths is progressively increased. This catastrophic case has a great impact in Africa unless preventive measures are effectively undertaken. In Ethiopia, the number of COVID-19 cases and death are increasing over time. Therefore, this study was aimed to assess the level of community readiness for COVID-19 pandemic prevention and its associated factors in residents of Awi Zone, Northwest Ethiopia.
Methods: A community-based cross-sectional study design was conducted among 1524 study participants from July 28 to August 27, 2020. Data were collected using structured and pre-tested interviewer-administered questionnaires. The collected data were entered into EPI data 4.6 versions and analyzed using Statistical Package for Social Science (SPSS) version 24.0. Those variables with P-value< 0.25 were entered into multivariable analyses and those variables with P-value < 0.05 were considered statistically significant. Finally, the findings of the result were explained using texts, figures, and tables.
Results: A total of 1423 participants have participated in the study. The finding revealed that the prevalence of knowledge, attitude, perception, and practice towards COVID-19 were found to be 76.6%, 68.4%, 68.5%, and 29% respectively. In final model, being a female [AOR=1.388 (95% CI: 1.050– 1.834) P= 0.021], married respondents [AOR=3.116 (95% CI: 1.592– 6.099) P= 0.001], Muslim religion followers [AOR=2.392 (95% CI:1.503– 3.806) P=0.002], and able to read and write [AOR=1.986 (95% CI:1.311– 3.006) P=0.002] were some of the variables significantly associated with the level of community readiness towards COVID-19 preventive measures.
Conclusion: The study findings indicate that respondent’s level of community readiness for COVID-19 prevention was mainly affected by sex, marital status, religion, and educational status. The Health education programs aimed at mobilizing and improving COVID-19 related level of community readiness especially practice are urgently needed. Awareness creation programs on more targeted groups such as men, unmarried and those with low educational level and religious leaders should be teaching the believers by interacting with faith and science on the means of preventing the pandemic.
Keywords: COVID-19, knowledge, attitude, readiness, practice, perception, Ethiopia
Introduction
Mankind has observed and fighting an invisible enemy of several pandemics through history where some of which were more disastrous to humans.1 In Wuhan, Hubei Province, China, a cluster of pneumonia cases of unknown etiology was reported in December 2019, and China’s center of disease control (CDC) reported a novel coronavirus as the causative agent of coronavirus disease 2019 (COVID-19) outbreak on January 2020.2 World health organization (WHO) also declared COVID-19 as a Public Health Emergency of International Concern (PHEIC) on 31st of January 2020 and declared as a pandemic on 11th March 2020.3
The virus has no proven therapeutic drugs and or vaccines, but the only key transmission preventing strategies depends on; educating the public about the nature of the disease and the transmission route, restricting mobility within and across borders, physical distancing, hand washing, environmental cleaning, and the rational use of personnel protective equipment (PPE) like masks.4,5 However, strict mass social distancing and lockdown may be difficult in countries of low-and-middle-income countries (LMIC) with foregoing unstable economic ground level, where most of the population leads their life from daily based income.6,7 In the context of developing countries unless the concerned bodies like governments, institutions, or wealthy individuals address the impacts of strict lockdown and travel ban for the most vulnerable communities, household food insecurity and related morbidity and mortality might be much higher than COVID-19.8,9
COVID-19 pandemic affects almost all continents of the world; America and Asian countries were highly affected. In Africa, because of low testing capacity, week contact tracing, and poor reporting system, the number of cases and deaths are low as compared to developed nations.10 The case-fatality rate (CFR) of the diseases depends on patients’ age, substance abuse, and any comorbidity. Even if most COVID-19 cases are mild, ~25% of COVID-19 patients require intensive care and ~10% need mechanical ventilation. Now, the COVID-19 pandemic is the most challenging event for the whole world’s features such as the socio-economic, healthcare system, and psychological wellbeing of humanity.11
Even though many countries in Africa scale-up their preparation and readiness to tackle the COVID-19 pandemic, shortage of testing kits, poor tracing system, poor health care system, shortage of PPE, shortage of laboratories, and negligence of the public to the preventive measures are the big challenge for the continent.4,10,12 Continuous increment of the infection, morbidity, lack of therapeutic measures, increased costs of the PPE, and medications are also major constraints in less developed nations.13
Community readiness is crucial to decrease the burden of COVID-19 on socio-economic activities and the healthcare system.14 Knowledge, attitude, perception, and practice for COVID-19 prevention strategies vary from the country.15–25 WHO recommends that different approaches to the countries to prepare themselves to respond to COVID-19pandemic. To reduce transmission of COVID-19 and its economic, public, and social impacts; assessing the risk and immediate implementation of appropriate measures are essential.16
In Ethiopia, especially in rural communities, residents may notice themselves as low risk of acquiring COVID-19, and compliance with the preventive measures is very poor. During a weekend the communities are mainly gathered for a traditional organization like mahber/senbetie, teskar, ekub, edir, wedding, and religious purpose. Unless immediate measures are taken nationwide, we will cost a lot. Publics’ knowledge, perception, attitudes, and practices towards COVID-19 preventive measures are pillars for the overall preparedness, readiness, and response. Therefore, this study was aimed to assess the level of community preparedness and associated factors for COVID-19 preventive measures among communities of the Awi zone.
Methods and Materials
Study Setting and Design
A community-based cross-sectional study design was conducted in the Awi zone from July 28 to August 27, 2020. This zone is one of 11 zones of the Amhara Regional State, Northwest Ethiopia. Injibara is the administrative center of the Awi zone and is located 452 km north of Addis Ababa and 129 km South of BahirDar (City of Amhara Region). The zone has 9 districts and three administrative towns. The zone is bordered in the west by Benishangul-Gumuz Region, on the North by West Gondar Zone, and the East by West Gojjam Zone. According to 2007 census data conducted by Central Statistical Agency, this zone had a total population of 1,322,693, of whom 64, 8295 were men and 674,397 were females.26
Populations
All residents in the Awi zone, Northwest Ethiopia were the source population whereas all selected study participants during the study period were the study populations.
Inclusion and Exclusion Criteria
The head of households whose age is greater than 18 years old and those who reside at least for the last six months in the study area was included in the study whereas, those who were unable to communicate due to critical illness were excluded from the study.
Sample Size Determination
The separate sample size estimate for each objective was determined using Epi info 7 StatCalc. The largest sample size; which is 1057 was taken.23 By adding a 1.5 design effect and non-response rate of 10% to the largest sample, the calculated final sample size for the study was 1744. However, one of the study areas which had a sample size of 220 was excluded from the final analysis due to its false report; hence the total last sample size was reduced to 1524.
Sampling Procedures
All districts and administrative towns of the zone were included in the study. Initially, the calculated sample size was proportionally allocated to each Kebele based on the number of households. Then, each household was selected by using a simple random sampling method based on the allocated proportion.
Data Collection Tools
A structured interviewer-administered questionnaire was used to collect data. The survey tool and interview guides were developed by reviewing different works of literature, current national and international guidelines on COVID-19 prevention. The tool contains; socio-demographic characteristics, knowledge of residents, and the community perception, attitude of the individuals, and COVID-19 prevention practice-related questions. Twenty-two data collectors and six supervisors were involved in the data collection process.
Data Collection Techniques
The data were collected from the head of households or from those family members whose age is 18 years old and above in selected households of each kebeles. Before starting data collection, three-day training was given for both the data collectors and supervisors on data collection ways and overall procedures. The data collectors have collected the information by following the current public health and social measures of the COVID-19 pandemic. Before interviewing the study participants, information was given to data collectors about the aim of the study, purposes, risks and possible benefits, and the right to refuse to participate in the study. Then those participants who sign in the voluntary consent were interviewed.
Operational Definitions
Level of Community Readiness for COVID-19 Pandemic Prevention
Communities’ level of readiness for COVID-19 pandemic was indicated as ready if the respondents have good knowledge, increase vulnerability perception, positive attitude, and good practice towards prevention measures, and not ready if either one or more of the above-stated sub-categories were reversely responded.
Knowledge About COVID-19
The respondents’ level of knowledge about COVID-19 was reported as good knowledge if the study participant correctly responded to more than or equal to 75% of knowledge assessment tools, and poor for <75%.19
Perception of COVID-19
The respondents’ perception about COVID-19 was assessed by 5 points Likert scale, and the highest score above the mean was indicated as increase vulnerability perception and low as poor perception.21
Attitudes Towards COVID-19
The attitude of the participant was categorized as positive or favorable if responded above the mean score of the responses and negative if below the mean score.20,22
The Practice of COVID-19 Prevention Measures
The respondents’ level of practice of COVID-19 prevention measures was reported as good practice if the study participant correctly responded to more than or equal to 75% of practice assessment tools, and poor for <75%.19
Data Quality Control
To make sure the quality, the questionnaire was translated into the local language (to Amharic) by experts. Finally, before data collection, it was re-translated back to English to verify consistency. A pre-test was conducted among 3% of the study sample in kebeles out of study setting to verify the appropriateness and feasibility of the tool (for validity and reliability test) and modifications were taken accordingly before actual data collection. Extensive training was given for both data collectors and supervisors. The tool was used with a reliability test or Cronbach’s alpha correlation coefficient of greater than or equal to 0.7 for inter-item consistency. The data collection team was communicated and discussed with principal investigators if they face any challenges during the daily basis data collection period.
Data Analysis
Descriptive analysis was done by computing proportions and summary statistics. The bivariate analysis was used to see the association between each independent variable and the outcome variables by using binary logistic regressions. The assumption for binary logistic regression was checked. The goodness of fit was tested by the log-likelihood ratio (LR). All variables with P<0.25 in the bivariate analysis were included in the final model of multivariable analysis to control all possible confounders. A Multi-collinearity test was carried out to see the correlation between independent variables by using collinearity statistics (Variance inflation factor (VIF) >10 and standard error >2 was considered as suggestive of the existence of multi co-linearity). The adjusted odds ratio along with 95% CI was estimated to identify factors in the multivariable model. In this study P-value < 0.05 was deemed to declare statistical significance. Then, the finding was presented by using simple frequencies, summary measures, tables, texts, and figures.
Results
Socio-Demographic Characteristics
In this study, a total of 1423 respondents have participated with a response rate of 93.4%. The age of respondents ranges from 18–81 years with a mean and standard deviation (SD) of 33.83 ± 11.84 years respectively. More than half (54.7%) of the study participants were males and 643 (45.2%) were in the age group of 18–29 years. Nine hundred eighty-three (69.1%) were from the Agew ethnic group and 1278 (89.8%) of respondents were orthodox Christian religion followers. Eight hundred six of the study participants (56.6%) were married in marital status. Four hundred forty-five (31.3%) of the study participants had an educational level of college and above and 343 (24.1%) of the participants have been working as government employees (Table 1).
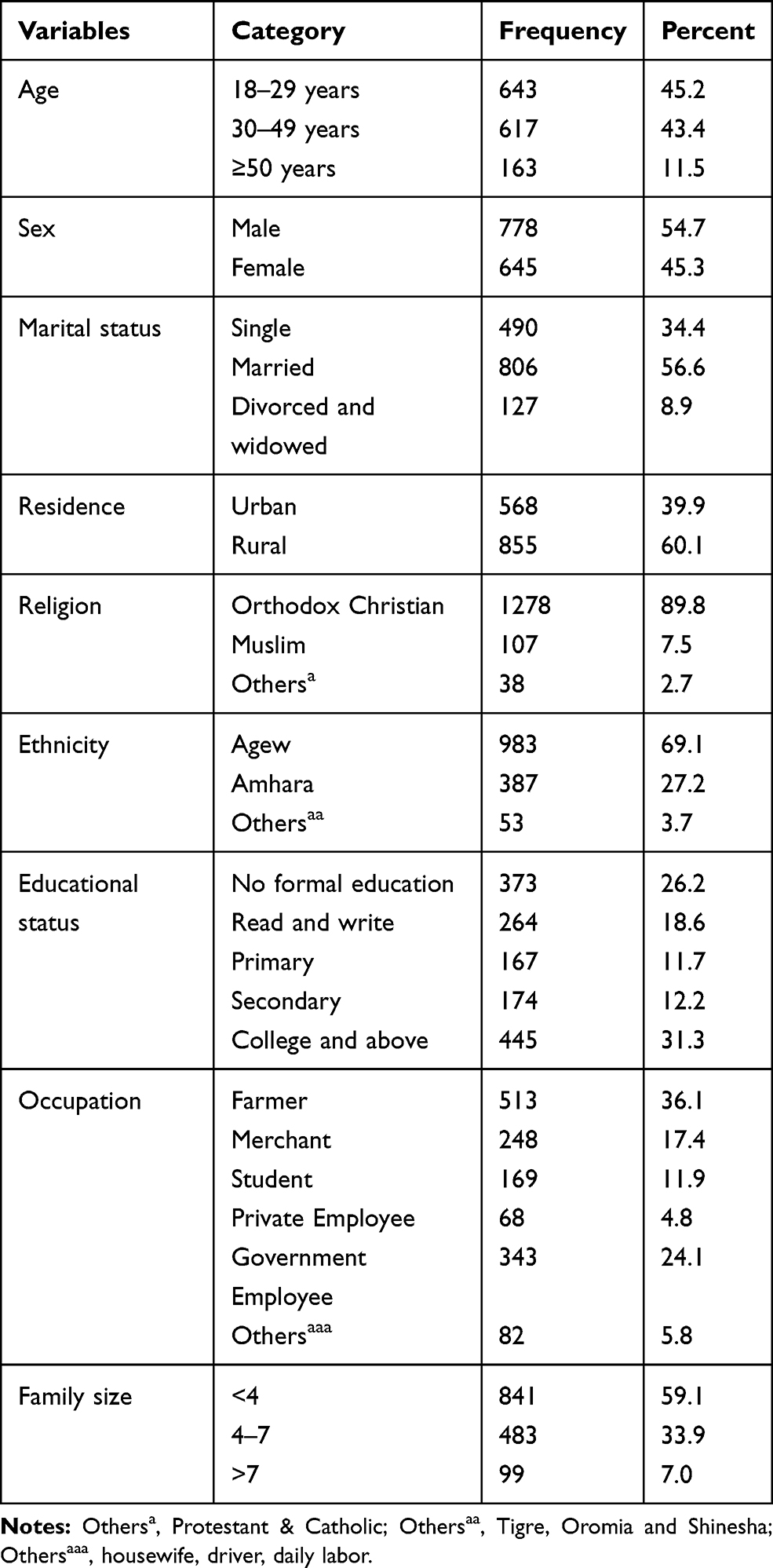 |
Table 1 Socio-Demographic Characteristics of Participants Towards COVID-19 Pandemic in Awi Zone, Amhara Region, Ethiopia, 2020 (n=1423) |
Source of Information for COVID-19
All (100%) of the study participants had heard about the COVID-19 pandemic. The main source of information for about 54.7% of the study participants were mass media, whereas the remaining were obtained from community/friends and family (41%), 36.4% from health care providers, 5.4% from print media, and 3.4% from others like; phone text, from religious places, and prisons.
Respondents’ Knowledge of COVID-19 Pandemic
This study revealed that the prevalence of good knowledge was found to be 76.6% (95% CI, 74.3–78.7). Nine hundred forty-one (89.4%) of study participants were correctly answered COVID-19 as a viral infection and 66.4% respond to the incubation period of COVID-19 infection is from 2–14 days. Five hundred seventy-two (40.2%) of the study participants mentioned all (fever, cough, sore throat, fatigue, and headache) signs and symptoms of the COVID-19 pandemic. About 27.5% of the study participants did not know that asymptomatic patients can transmit the infection to healthy individuals. Whereas 83.2% of study participants knew elderly patients are at higher risk of being infected with COVID-19. The majority (88.8%) of study participants knew that COVID-19 is transmitted by close contact and respiratory droplets and 87% of study participants knew that wearing masks can prevent infection of COVID-19 (Table 2).
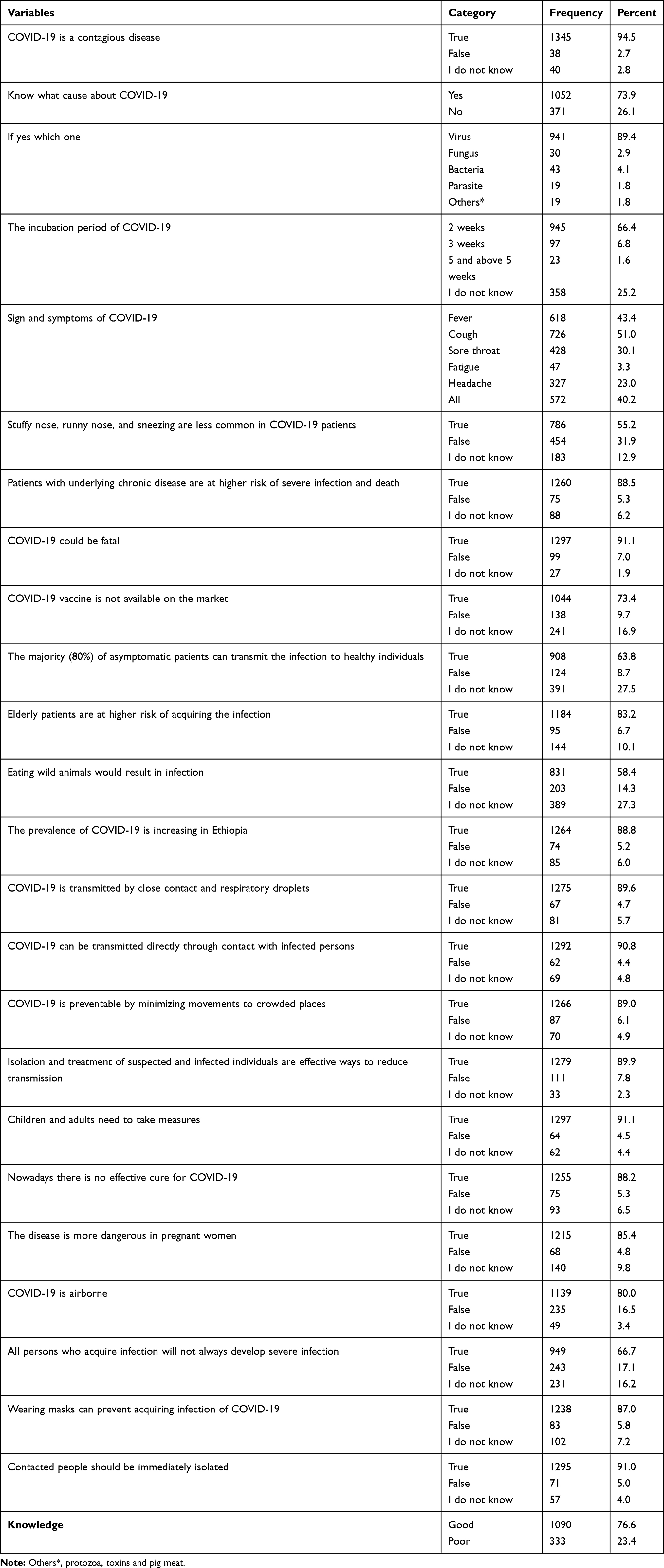 |
Table 2 Knowledge of Study Participants on COVID-19 in Awi Zone, Amhara Region, Ethiopia, 2020 |
Respondents’ Attitude on COVID-19 Pandemic
The finding of this study showed that about 68.4% (95% CI, 65.9–70.8) of the participants had a positive attitude towards COVID-19 preventive measures. The mean and standard deviation of participants attitude towards COVID-19 was 37.52 and 8.968 respectively. The majority (86.2%) of study participants agreed that early recognition of signs and symptoms of COVID-19 can improve treatment and recovery from COVID-19. More than three-fourth (78.2%) of the study participants believes that asymptomatic patients may infect healthy individuals. Nine hundred seventeen (64.4%) of study participants agreed that COVID-19 will finally be controlled successfully and 85.6% believe that compliance with the ministry of health (MOH) precaution will prevent the spread of disease. Almost all of the study participants believed in the value of handwashing and limited personal contact. Likewise, ~78.6% of the participants believed that having no face mask can increase transmission (Table 3).
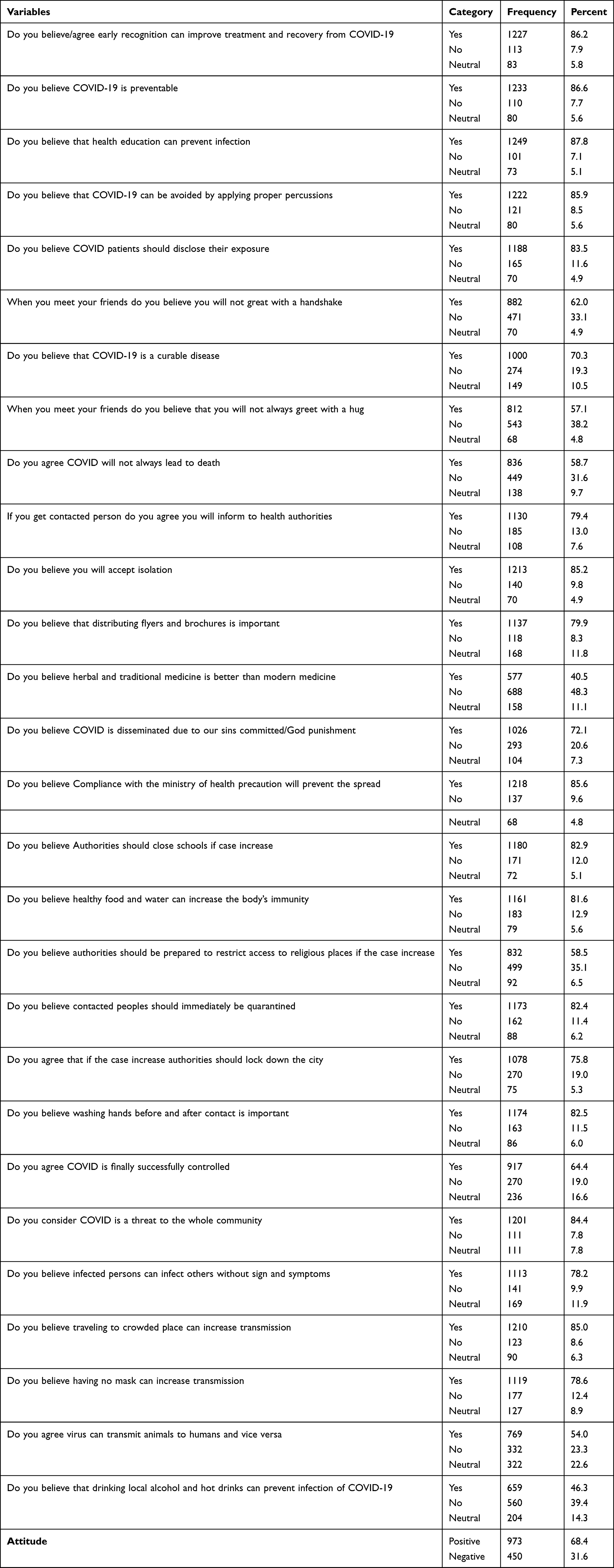 |
Table 3 Respondents Attitude Towards COVID-19 in Awi Zone, Amhara Region, Ethiopia, 2020 |
Respondents Perception of COVID-19
The mean and standard deviation of the study participant’s perception of COVID-19 was 7.73 and 2.229 respectively. According to this study, 68.5% (95% CI, 66–71) of study participants had a good perception of COVID-19. About 85.2% and 33.1% of study participants perceived that corona is scary and was designed as a biological weapon respectively (Table 4).
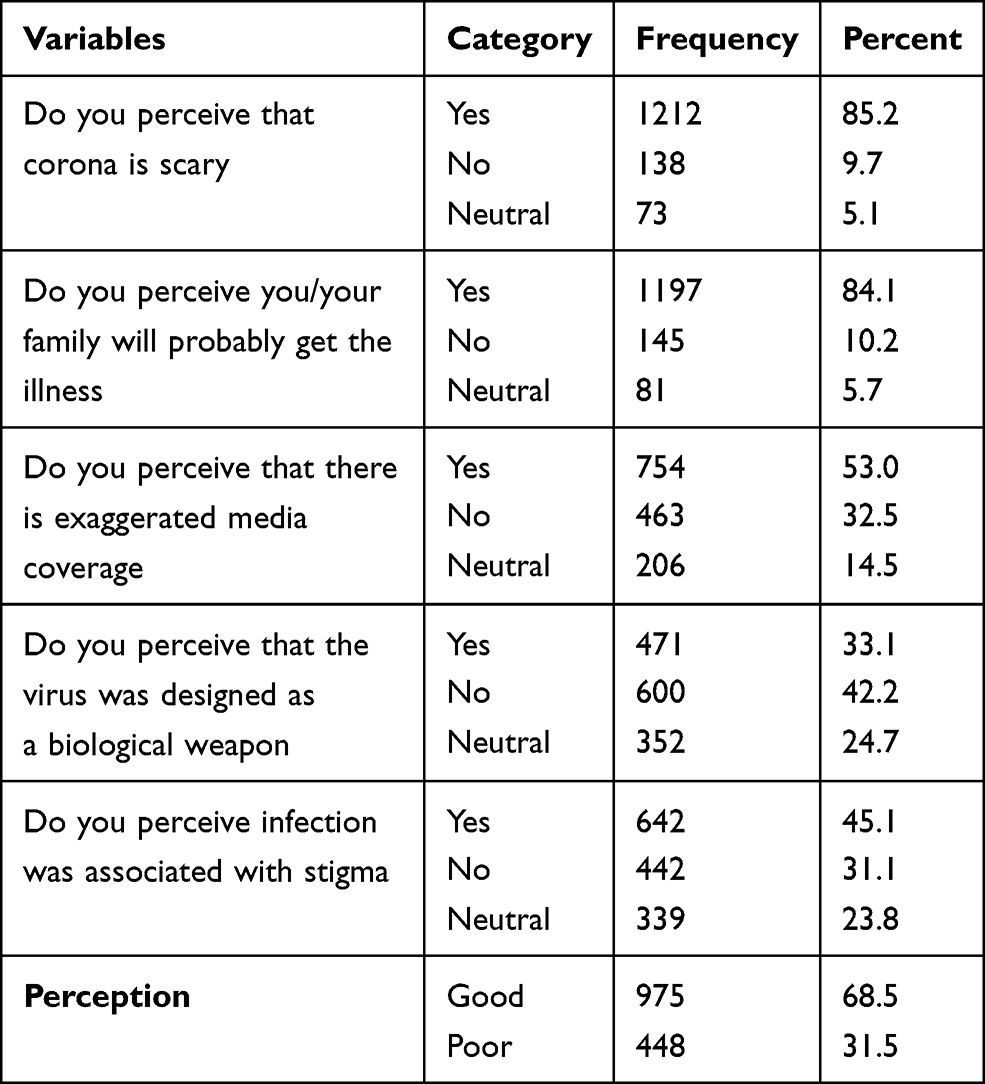 |
Table 4 Study Participant’s Perception of COVID-19 in Awi Zone, Amhara Region, Ethiopia, 2020 |
The Practice of Study Participants Towards COVID-19
About 29% (95% CI; 26.8–31.5) of study participants had a good practice. The majority of study participants have complied with COVID-19 preventive measures; 37.0% did not wash their hands, 43% did not apply physical distancing, only 35.6% avoid public transport, and 62.8% did not use any disinfectant and solutions to prevent infection. Surprisingly nearly three-fourth of the study participants did not use masks. More than three-fourths of the study participants stop shaking hands, hugging, and kissing while they greet others (Table 5).
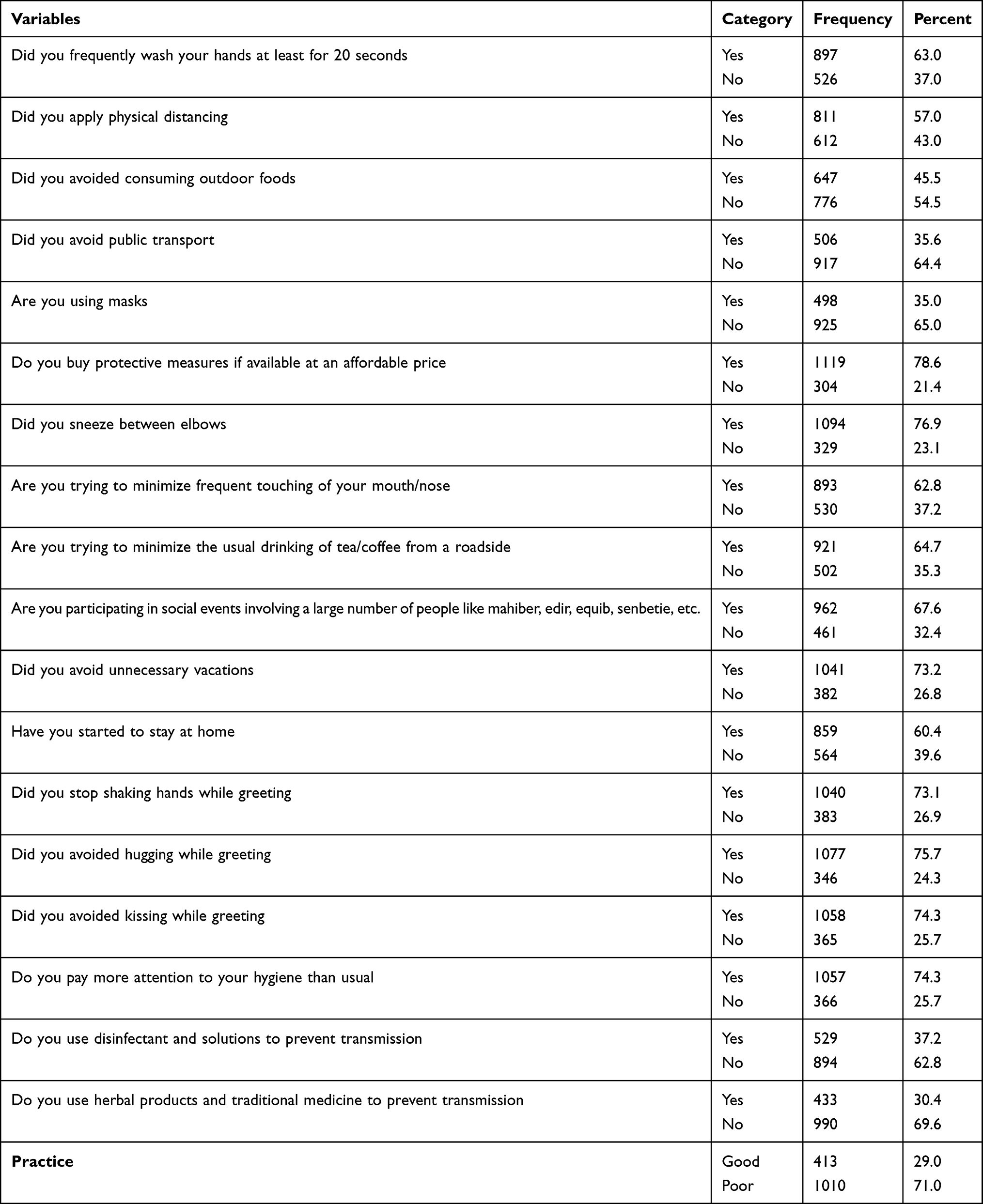 |
Table 5 Participants Practice on COVID-19 in Awi Zone, Amhara Region, Ethiopia, 2020 |
About 67.6% of participants were involved in large social events like mahiber, edir, equib, tesker, senbetie and religious ceremonies and only 10.4% utilize the mask in the study area (Figures 1 and 2).
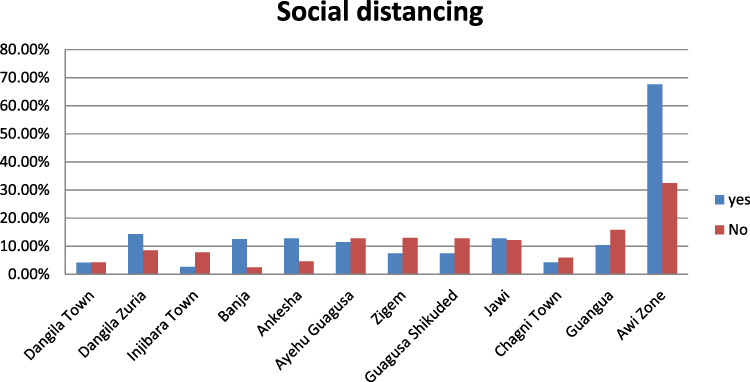 |
Figure 1 Participation of Awi zone communities in social events involving a large number of people like mahiber, edir, equib, senbetie, and religious ceremonies. |
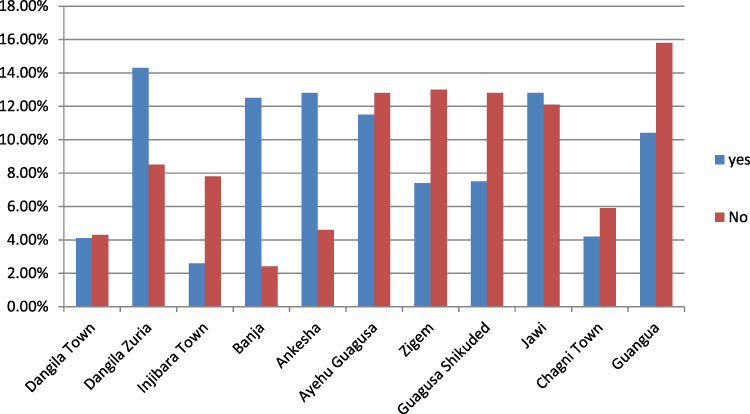 |
Figure 2 Distribution of mask utilization to prevent COVID-19 in Awi zone, Northwest Ethiopia, 2020. |
Level of Community Readiness Towards COVID-19 Prevention
About 20.2% (95% CI, 18.1–22.3) of the study participants were well ready on COVID-19 preventive measures (Figure 3).
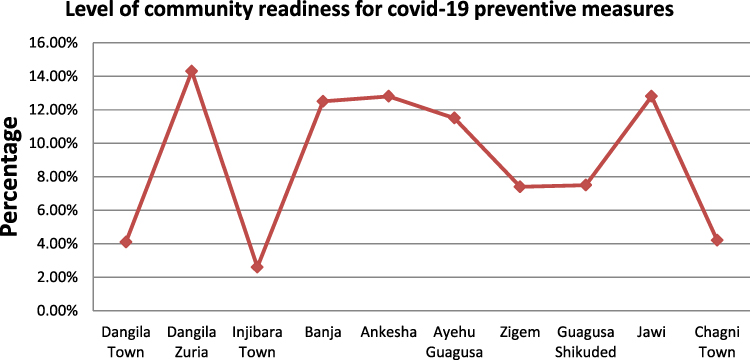 |
Figure 3 Study participants level of community readiness for COVID-19 prevention in Awi zone, Amhara region, Ethiopia, 2020. |
Factors Affecting the Level of Community Readiness Towards COVID-19
Binary Logistic regression was performed to assess the association of each independent variable with a level of community readiness for COVID-19 preventions. The factors that showed a p-value of less than 0.25 were added to the multivariable regression model. The result revealed that on the binary logistic regression: age, sex, marital status, residence, religion, educational status, occupation, and family size were significantly associated with the level of community readiness for COVID-19 prevention.
In multivariable logistic regression, all significant variables in binary logistic regression were adjusted. The result showed that the odd of readiness for COVID-19 prevention was 1.4 times more likely on females (AOR: 1.388, 95% CI: 1.050–1.834) as compared to males. Marital status was also significantly associated with the level of community readiness for COVID-19 prevention measures. Those married mothers were 3.12 times higher odds of ready for COVID-19 preventions (AOR: 3.116: 95% CI: 1.592–6.099) compared to their counterparts. The likelihood of the level of community readiness for COVID-19 prevention was 2.4 higher among Muslims (AOR: 2.392: 95% CI: 1.503–3.806) than Orthodox Christianity followers. The odds of readiness for COVID-19 prevention in study participants who can read and write were 2 more likely compared to their counterparts (Table 6).
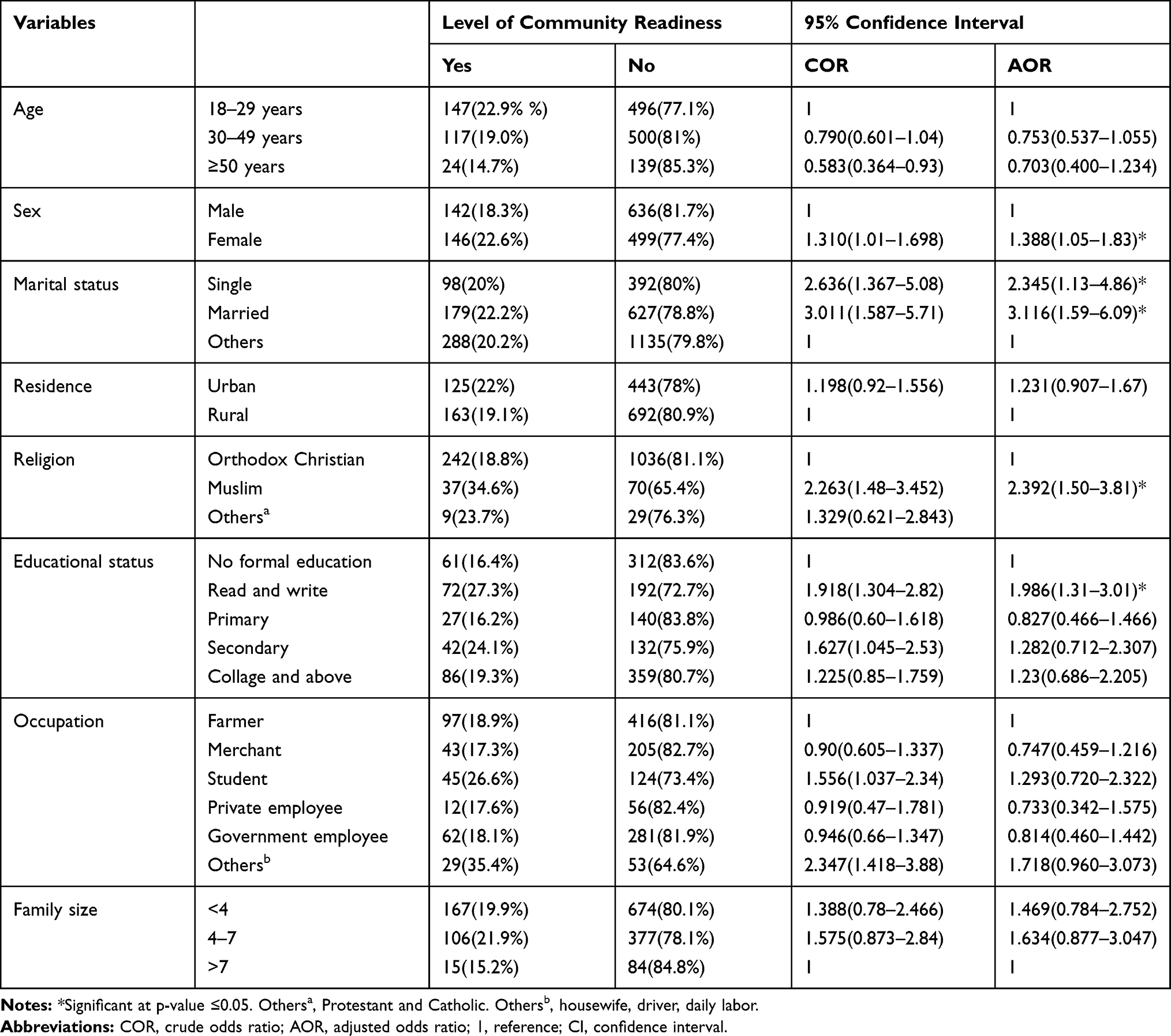 |
Table 6 Factors Affecting the Level of Community Readiness Towards COVID-19 in Awi Zone, Amhara Region, Ethiopia, 2020 |
Discussion
This is the first community-based cross-sectional study aimed at assessing the level of community readiness for COVID-19 pandemic prevention and associated factors among residents of Awi Zone, Northwest Ethiopia.
Communities’ negligence in preventive measures is the major obstacle to break the spread of the virus. This finding revealed that 20.2% (95% CI, 18.1–22.3) of the study participants were ready on COVID-19 preventive measures. The study found that the prevalence of good knowledge for COVID-19 prevention measures was found to be 76.6% (95% CI, 74.3–78.7), which implies that a majority of the communities had adequate knowledge towards COVID-19. This finding is consistent with other studies that have demonstrated satisfactory levels of knowledge for the pandemic.27 Nevertheless, in another study conducted among the Addis Zemen Ethiopia,28 Southwest Ethiopia,29 Debrebirhan Ethiopia,30 Bangladesh,31 Rural China,21 Paraguayans,22 Egypt,15 Yemen,32 Syrian33 population, a lower proportion of the study population had sufficient knowledge towards COVID-19 prevention measures when compared with the current study. The difference might be due to the time of the study and the population participated in the study. The majority of the study population in this study found in rural areas and had no access to electricity and the internet. As a result, they had limited information on COVID-19-related updates and preventive measures posted online by the official government, health authorities, and different media that are shown to have a positive effect on improving knowledge.
This finding is also very low compared to the study in Jimma Ethiopia and china.18,34 The reason for this discrepancy might be due to a difference in the socioeconomic status of study participants. Moreover, it may also be due to the differences in a tool used for the assessment of knowledge and time of data collection. In these studies, the data were collected during the main phase of the outbreak when most populations were exposed to a lot of information about COVID-19.
This finding also showed that about 68.4% (95% CI, 65.9–70.8) of the participants have a positive attitude toward COVID-19 preventive measures, which aligns with a study done in Southwest Ethiopia and Paraguay. However, our study has found a better attitude on the prevention of COVID-19 than a study conducted in Addis Zemen Ethiopia which showed that 36.1% of participants had a good attitude towards prevention and control of COVID-19.35 Moreover, our study was also found to be lower than studies done in Bangladesh,31 Nepal,19 and rural China.21 This variation might be caused by differences in the study area and population, geographic coverage, and number and type of questions used. The current study used large area coverage where most participants were from rural areas that had limited access to information sources than the situation abroad that included urban health facilities with better access to information sources.
The level of practices for the prevention of COVID-19 in Awi Zone, Northwest Ethiopia was 29% (95% CI; 26.8–31.5), which was lower than the study conducted in Iran, 71%,35 Southwest Ethiopia (59.4%), Addis Zemen Ethiopia,28 Bangladesh,31 China,21 Nepal,19 but much higher than the study conducted in Thailand, 17%.36 This inconsistency might be related to variations in the geographic area, the incidence of COVID-19, availability of PPE, training access, and information sources and awareness levels of the community. Our study also found out that 68.5% (95% CI, 66–71) of the study participants had a good perception of COVID-19 preventive measures. In this study, about 85.2% of study participants perceived that corona is scary. This is supported by Chen et al which showed that out of 4016 Anhui Province residents 92.6% think that this pandemic is scary.17
One of the important findings in this study is that surprisingly nearly three-fourth of the study participants did not use masks and about 67.6% of participants were involved in large social events like mahiber, edir, equib, tesker, senbetie, etc. This is very high compared to the finding from China,18 and it is also contrary to the WHO recommendations.37 This figure is very frustrating in the case of Ethiopia, where the community transmission of COVID-1 9 is more likely.38,39
This study also explores the association between socio-demographic variables with the level of community readiness towards COVID-19 preventive measures. Therefore, this finding revealed that sex, marital status, religion, and educational status were significantly associated with the level of community readiness towards COVID-19 preventive measures. This finding revealed that education is significantly associated with the level of community readiness towards COVID-19 preventive measures. Even though there is no similar study done anywhere about the level of community readiness toward COVID-19 prevention measures, there are studies that support the association of educational level with perception and knowledge toward COVID-19 prevention measures. For instance, the study was done in China,18 Paraguayans23 Egyptians,15 Mizan Aman,40 Arbaminch town,27 and Northwest Ethiopia41 showed the association of educational status with perception, attitude and knowledge of study participants toward COVID-19 prevention measures. This might be because education is the main driving force for everything which may make respondents internalize the risk analysis of the disease. The other possibilities might be due to participants who have higher educational levels could have better chances to access different COVID-19 related information and better to avoid a misconception and poor interpretations about the severity of the disease.
The likelihood of the level of community readiness for COVID-19 prevention was also higher among Muslims than Orthodox Christianity followers. This could be explained by Muslim participants had religious wearing nature and frequent hand washing practice particularly in females which might make themselves more protective than Christian religion followers. Lastly, being female and married women were also significantly associated with the level of community readiness toward COVID-19 prevention measures.
Conclusion and Recommendation
This study depicted that Awi zone communities were good in knowledge, positive attitude, and good perception of COVID-19 preventive measures. However, most participants had poor practices for COVID-19 preventive measures. Some of the major preventive actions like physical distancing, using a mask, and avoiding attending crowded populations were perceived as very difficult by a large proportion of the population. In this study, sex, marital status, religion, and educational status were significantly associated with the level of community readiness towards COVID-19 preventive measures. Even though, there is good knowledge, positive attitude, and good perception; a practice on the COVID-19 preventive measure was poor. Health education programs aimed at mobilizing and improving COVID-19 related level of community readiness especially practice are urgently needed.
Awareness creation programs on more targeted groups, such as men, unmarried, and those with low educational levels are required to improve the level of community readiness on the prevention of the COVID-19 pandemic. Advocacy of hand hygiene, physical distancing, use of mask, and other strategies should be more accomplished with respective bodies. As per finding increasing health education programs regarding the pandemic via different mass and Social Media, coordinated and combined efforts of Ethiopian authorities and all individuals will be needed to battle the multidimensional consequences of the pandemic.
Religious leaders should teach believers by interacting with faith and science on the means of preventing the pandemic. Every individual should apply and follow the government’s (Federal Ministry of Health) directions to control the distribution of the pandemic. It is also recommended that mixed methods research, program evaluations, and longitudinal research efforts should be undertaken to explore and address the effect of COVID-1 9 on Awi zone communities.
Strength and Limitation of the Study
Our study was a large community-based study design and had a broad scope with several strengths. It was based on a large sample size with population size to proportion allocation and focused on participants from rural areas; therefore, the findings can be generalized across the Awi zone (district) populations. Unlike other studies, we undertook face-to-face interviews and strict supervision with the Awi zone health bureau in this challenging situation, which is a strength. However, it has also the limitations of this study. There was no previously standardized and validated tool to assess the level of community readiness and associated factors towards COVID-19 prevention. We also did not find sufficient data to compare and contrast the level of community readiness with others, and it makes our discussion shallow. Our study also shares the limitation of the study design.
Abbreviations
APHI, Amhara region Public Health Institution; CFR, Case-Fatality Rate; CDC, Center for Disease Control; LMIC, Low-and-middle-income countries; MERS, Middle East Respiratory Syndrome; PPE, Personal Protective Equipment’s; PHEIC, Public Health Emergency of International Concern; SARS, Severe Acute Respiratory Syndrome; SARS-CoV2, Severe Acute Respiratory Syndrome Coronavirus 2; WHO, World Health Organization.
Data Sharing Statement
All related data has been presented within the manuscript. The data set supporting the conclusions of this article is available from the corresponding author on request.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Before conducting the study, ethical clearance was obtained from the Amhara Public Health Institute Research Ethics Review Committee (Ref No. RTTD/811). Explanation about the purpose of the study and a letter of support was given to administrative bodies of the Awi zone. Written informed consent was obtained from each participant after clearly describing the purpose, benefit, and risk of the study. Study participants were informed of their full right to withdraw their participation at any stage of the interviewee. Confidentiality was maintained by using anonymous questionnaires.
Acknowledgments
The authors thank the Amhara regional health bureau for approval of ethical clearance and Awi Zone Health Office for technical and financial support of this study. Then, we would like to thank all committed study participants who were participated in the study during interviews. Lastly, we are indebted to each department’s health offices for their assistance and permission to undertake the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Awi Zone Health Office, but the funder has no role in the design of the study, collection, analysis, and interpretation of the data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Nadeem S. Coronavirus COVID-19: available free literature provided by various companies, journals, and organizations around the world. J Ongoing Chem Res. 2020;5(1):7–13.
2. Rapid Risk Assessment. Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK – Seventh Update, 25 March 2020. Stockholm: ECDC; 2020.
3. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Bio-Medica. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
4. Chiang C, El Sony A. Tackling the threat of COVID-19 in Africa: an urgent need for practical planning. Int J Tuberc Lung Dis. 2020;24:541–542. doi:10.5588/ijtld.20.0192
5. Balachandar V, Mahalaxmi I, Kaavya J, et al. COVID-19: emerging protective measures. Eur Rev Med Pharmacol Sci. 2020;24(6):3422–3425. doi:10.26355/eurrev_202003_20713
6. Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of COVID-19 in China and associated psychological problems. Asian J Psychiatr. 2020;51:102092. doi:10.1016/j.ajp.2020.102092
7. Banerjee D. The COVID-19 outbreak: crucial role the psychiatrists can play. Asian J Psychiatr. 2020;50:102014. doi:10.1016/j.ajp.2020.102014
8. Berger ZD, Evans NG, Phelan AL, Silverman RD. Covid-19: control measures must be equitable and inclusive. BMJ. 2020;368:m1141. doi:10.1136/bmj.m1141
9. Bhutta ZA, Basnyat B, Saha S, Laxminarayan R. Covid-19 risks and response in South Asia. BMJ. 2020;368:m1190. doi:10.1136/bmj.m1190
10. Gilbert M, Pullano G, Pinotti F, et al. Preparedness and vulnerability of African countries against importations of COVID-19: a modeling study. Lancet. 2020;395(10227):871–877. doi:10.1016/S0140-6736(20)30411-6
11. Bong CL, Brasher C, Chikumba E, McDougall R, Mellin-Olsen J, Enright A. The COVID- 19 pandemic: effects on low and middle-income countries. Anesth Analg. 2020;131:86–92. doi:10.1213/ANE.0000000000004846
12. Ahmed F, Ahmed N, Pissarides C, Stiglitz J. Why inequality could spread COVID-19. Lancet Public Health. 2020;5:e240. doi:10.1016/S2468-2667(20)30085-2
13. Abrams EM, Greenhawt M. Special article: risk communication during COVID-19. J Allergy Clin Immunol Pract. 2020;8:1791–1794. doi:10.1016/j.jaip.2020.04.012
14. Budd J, Miller BS, Manning EM, et al. Communication, collaboration, and cooperation can stop the 2019 coronavirus. Nat Med. 2020;26(2):151. doi:10.1038/s41591-020-0775-x
15. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the Novel Coronavirus Disease (COVID-19). J Community Health. 2020;45:881–890. doi:10.1007/s10900-020-00827-7
16. World Health Organization. Critical Preparedness, Readiness, and Response Actions for COVID-19: Interim Guidance, 22 March 2020. World Health Organization; 2020.
17. Chen Y, Jin YL, Zhu LJ, et al. [The network investigation on knowledge, attitude, and practice about COVID-19 of the residents in Anhui Province]. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(4):367–373. Chinese. doi:10.3760/cma.j.cn112150-20200205-00069
18. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
19. Hussain A, Garima T, Singh BM, Ram R, Tripti RP. Knowledge, attitudes, and practices towards COVID-19 among Nepalese Residents: a quick online cross-sectional survey. Asian J Med Sci. 2020;11(3):6–11. doi:10.3126/ajms.v11i3.28485
20. Zegarra-Valdivia J, Vilca BNC, Guerrero RJA. Knowledge, perception, and attitudes in Regard to COVID-19 Pandemic in Peruvian Population. 2020.
21. Lihua M, Ma L, Liu H, Jiang N, Wang S, Jiang X. Knowledge, beliefs/attitudes and practices of rural residents in the prevention and control of COVID-19: an online questionnaire survey. 2020.
22. Rios-González CM. Knowledge, attitudes, and practices towards COVID-19 in Paraguayans during outbreaks: a quick online survey. 2020.
23. Haque T, Hossain K, Bhuiyan M, et al. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: an online cross-sectional survey. 2020.
24. Olapegba PO, Ayandele O, Kolawole SO, et al. COVID-19 Knowledge and Perceptions in Nigeria. 2020.
25. Austrian K, Pinchoff J, Tidwell JB, et al. COVID-19 related knowledge, attitudes, practices, and needs of households in informal settlements in Nairobi, Kenya. 2020.
26. CSA. 2007 population and housing census of Ethiopia: administrative report; 2020:1–117. Available from: http://unstats.un.org/unsd/censuskb20/Attachment489.aspx.
27. Nigussie TF, Azmach NN. Knowledge, attitude and practice towards Covid-19 among Arbaminch Town, Southern Ethiopia: cross-sectional survey, 2020. GSJ. 2020;8(6).
28. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13.
29. Wondimu W, Ag E, Mekonen MA. Practice of Coronavirus Disease-1 9 prevention methods and associated factors in three zones of Southwest Ethiopia: community-based cross-sectional study. 2020.
30. Aynalem YA, Akalu TY, Gebresellassie B, Sharew NT, Shiferaw WS. Assessment of undergraduate student knowledge, practices, and attitude towards COVID-19 in Debre Berhan University, Ethiopia. 2020.
31. Islam S, Emran GI, Rahman E, et al. Knowledge, attitudes, and practices associated with the COVID-19 among slum dwellers resided in Dhaka City: a Bangladeshi interview-based survey. medRxiv. 2020. doi:10.1101/2020.09.15.20195255
32. Al Ahdab S. Knowledge, Attitudes, and Practices (KAP) towards pandemic COVID-1 9 among Syrians. 2020.
33. Alrubaiee GG, Al-Qalah TA, Al-Aawar MS. Knowledge, attitudes, anxiety, and preventive behaviors towards COVID-1 9 among health care providers in Yemen: an online cross-sectional survey. BMC Public Health. 2020;20(1):1. doi:10.1186/s12889-020-09644-y
34. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
35. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the Novel Coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Heal Organ. 2020.
36. Srichan P, Apidechkul T, Tamornpark R, et al. Knowledge, attitude and preparedness to respond to the 2019 novel coronavirus (COVID-19) among the bordered population of northern Thailand in the early period of the outbreak: a cross sectional study; 2020. Available from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3546046.
37. World Health Organization (WHO). Risk Communication and Community Engagement (RCCE) action plan guidance COVID-19 preparedness and response. 2020. Available from: https://www.who.int/publications/i/item/risk-communication-and-community-engagement-(rcce)-action-plan-guidance. Accessed March 16, 2020
38. Shigute Z, Mebratie AD, Alemu G, Bedi A. Containing the spread of COVID-1 9 in Ethiopia. J Glob Health. 2020;10(1):1–4.
39. Biadgilign S, Yigzaw M. COVID-1 9 in Ethiopia: current situation, missed opportunities, and the risk of health system disruptions. Pan Afr Med J. 2020;35(2):66. doi:10.11604/pamj.supp.2020.35.2.23906
40. Mechessa DF, Ejeta F, Abebe L, et al. Knowledge of COVID-19 and its associated factors in Mizan-Aman Town, Southwest Ethiopia, 2020. Int J Gen Med. 2020;13:507. doi:10.2147/IJGM.S263665
41. Kassie BA, Adane A, Tilahun YT, Kassahun EA, Ayele AS, Belew AK. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS One. 2020;15(8):e0238. doi:10.1371/journal.pone.0238415
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.