")
Back to Journals » Nutrition and Dietary Supplements » Volume 12
Level and Predictors of Mothers’ Knowledge and Attitude on Optimal Complementary Feeding in West Gojjam Zone, Northwest Ethiopia
Authors Abiyu C, Belachew T
Received 7 April 2020
Accepted for publication 24 June 2020
Published 27 July 2020 Volume 2020:12 Pages 113—121
DOI https://doi.org/10.2147/NDS.S257206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chandrika J Piyathilake
Chalachew Abiyu, Tefera Belachew
Faculty of Public Health, Department of Nutrition and Dietetics, Jimma University, Jimma, Ethiopia
Correspondence: Chalachew Abiyu Tel +251-913 52 6578
Email [email protected]
Introduction: Attaining the recommended level of complementary feeding practice remains a major public health concern in developing countries including Ethiopia. The ability of the mothers to apply the recommended feeding practice is associated with their knowledge and attitude on optimal complementary feeding. It is essential to examine the level and predictors of mothers’ knowledge and attitude on optimal complementary feeding to design evidenced-based effective intervention strategies.
Methods: A community-based cross-sectional study was carried out in West Gojjam Zone, Northwest Ethiopia from February to March 2017. A two-stage cluster sampling technique was applied to select the study subjects. Data were collected using a pre-tested, structured interviewer-administered questionnaire, and processed and analyzed using SPSS version 21. Binary and multivariable logistic regressions were used to identify predictors of mothers’ knowledge and attitude on complementary feeding.
Results: Overall, 60% and 51% of mothers had good knowledge and favorable attitude towards optimal complementary feeding, respectively. Predictors of mothers’ knowledge on optimal complementary feeding were maternal educational status [AOR=2; 95% CI: 1.15– 3.43], paternal educational status [AOR=2.2; 95% CI: 1.26– 5.13], ANC status [AOR=3.5; 95% CI: 1.9– 7.47], place of delivery [AOR=1.8; 95% CI: 1.13– 2.83], PNC status [AOR=2.2; 95% CI: 1.32– 3.73], and IYCF counseling [AOR= 2.5; 95% CI: 1.46– 7.52]. Likewise, maternal educational status [AOR=2.5; 95% CI: 1.49– 4.02], ANC status [AOR=2.7; 95% CI: 1.54– 4.57], IYCF counseling [AOR= 2.2; 95% CI: 1.47– 4.89], and possession of radio [AOR= 1.8; 95% CI: 1.35– 3.82] were significantly associated with mothers’ attitude towards optimal complementary feeding.
Conclusion: The overall level of mothers’ knowledge and attitude on optimal complementary feeding was not appreciable. Hence, behavior change interventions on optimal complementary feeding focusing on age-specific meal frequency and diversification; feeding during and after illness and the negative impact of bottle feeding should be strengthened in the community.
Keywords: knowledge, attitude, complementary feeding
Introduction
The first 2 years of life are a critical period for optimal growth and development of children. Most events of malnutrition happen in this period since there is a high demand for adequate diets. Malnutrition during the first 2 years of life will result in an irreversible impairment in physical growth, and brain development. Hence, enhancing feeding practice during this period is an important aspect to improve health and nutrition in children.1,2
From all established health and nutrition intervention approaches, appropriate infant and young child feeding (IYCF) has the highest degree of impact on the growth and survival of children.3 Suboptimal feeding practices account for more than half of the deaths of under five children worldwide. Greater than two-thirds of the deaths are related to inappropriate feeding practices during the first 2 years of life.2,4 On the opposite hand, studies indicate that the application of the optimum complementary feeding practices might stop 6% of deaths in under five children.5
Child undernutrition remains a serious public health challenge in Ethiopia. The prevalence of stunting, underweight and wasting were 38%, 24%, and 10%, respectively, in children under five years of age. The study area particularly has a high rate of malnutrition regardless of the area being a surplus crop producer. This could be caused by suboptimal child feeding practice which is in turn influenced by knowledge and attitude of mothers on child feeding practice.6
The complementary feeding period is a critical time of transition in infants characterized by a gradual shift from breast milk to family food. The incidence of growth faltering increases significantly at 6 months of age when complementary foods are being introduced particularly in most low and middle-income countries including Ethiopia.7 Suboptimal complementary feeding practices are associated with a high burden of malnutrition and mortality in children.8
Children need adequate quantities and quality of complementary foods to support their optimal growth and development, as breast milk alone is nutritionally insufficient after the age of 6 months. WHO recommends that mothers should introduce nutritionally sufficient, safe, age-specific complementary foods at the age of sixth month, keeping breastfeeding until the age of two years and beyond.8
Attaining the optimal level of complementary feeding remains a major public health concern in many developing countries. Complementary foods are initiated untimely, prepared in an unhygienic way; and lack the desired quality, amount, and nutrient density for optimal child growth and development of children.9 In Ethiopia, the optimal complementary feeding practice is only 7%. About 56% of children aged 6–8 months consumed complementary foods, only 45% of children were fed the minimum meal frequency and 14% of children achieved the minimum dietary diversity.6
Mothers’ knowledge and attitude on complementary feeding have a significant effect on their feeding behaviors. The ability of the mothers to apply the recommended complementary feeding practices is associated with their knowledge and attitude on optimal complementary feeding. Several factors could, in turn, affect mothers’ knowledge and attitude towards complementary feeding.10–12 The majority of the rural communities in Ethiopia are illiterate, have low socioeconomic status, and have restricted access to the fundamental health-care facilities which might have a negative influence on knowledge and attitude of mothers on complementary feeding.13
Promoting optimal complementary feeding practices is a global health priority to improve child feeding practices particularly in developing countries.14 The Ethiopian government carried out several efforts to enhance complementary feeding practices at different times through the implementation of IYCF guideline across the country.13 However, these efforts failed to improve feeding practices at the expected level. As a result, the problem of stunting has remained pervasively high in the country. This may be due to barriers of translating feeding recommendations into practice that is related to knowledge, attitude and cultural norms existing in the community. Hence, it is essential to examine the level and predictors mothers’ knowledge and attitude of mothers on optimal complementary feeding prevailing in the community to design evidenced-based effective intervention strategies focused on the specific determinants. This study aimed to examine the level and predictors of mothers’ knowledge and attitude on optimal complementary feeding.
Methods
Study Setting
This study was conducted in rural communities of West Gojjam Zone, Ethiopia from February to March 2017. West Gojjam Zone is one of the 13 administrative zones of the Amhara regional state. It has 13 rural districts, and each district is divided into kebeles (the lowest administrative units in Ethiopia). According to the population projection of Ethiopia for all regions at the district level from 2014 to 2017, which is based on the 2007 national census, the zone has a total population of 2,560,131 in 2016; of whom 1,262,144 (49.3%) were male and 1,297,987 (50.7%) were female. The rural part accounts for 92% of the total population. A total of 480,255 households were counted in this Zone, which results in an average of 4.39 persons to a household, and 466,491 housing units. From the total population mentioned, 315,228 were children of under five years of age of whom 160,214 were under two years of age.15
Study Design and Population
A community-based cross-sectional study was conducted among mothers of children under 2 years of age. Consented mothers who were residents in the study area were recruited for the study. Mothers who were ill and unable to communicate during the study were excluded from the study.
Sample Size Determination
This study was part of a larger study entitled
effectiveness of complementary feeding behavior change communication through community-level actors in improving feeding practices, nutritional and health status of infants
Registered at ClinicalTrials.gov as NCT03488680. The sample size was calculated using G-power based on the following assumptions. Tail (s): One; Effect size d: 0.3; α error probability= 0.05; and power (1- β error probability) = 0.8. This gave a sample size of 278. Then, it was multiplied by the design effect of 2 and allowing for a 10% loss to follow up, the total sample size was 612. The effect size of intervention on child linear growth was considered; the variable which gives the maximum sample size.16
Sampling Technique
A two-stage cluster sampling technique was applied. First, 2 out of the 13 districts in West Gojjam zone were selected by simple random sampling. Second, lists of all kebeles (clusters) in the selected districts were compiled from each district administrative office, and 16 kebeles were selected by simple random sampling. Each kebele in the selected districts forms the sampling frame, while the mother–child pairs within the kebeles formed the units of observation. The number of study subjects in the selected clusters was obtained from the records of prepared by health extension workers.
Data Collection Technique and Measurements
Data were collected using a pre-tested, structured interviewer-administered questionnaire adapted from WHO.2 The knowledge of mothers on complementary feeding was computed based on six knowledge questions with “yes” or “no” responses and for assessment of attitude, based on six attitude questions with “agree”, “disagree” and “don’t know” responses. A score of “1” was given for each correct response and “0” for the wrong response. The scores summed and a mean score for knowledge questions was computed and respondents who scored less than the mean were labeled as having “poor” knowledge and those scored equal to or above the mean were considered as having “good” knowledge. Likewise, the scores summed and a mean score for attitude questions was computed and respondents who scored below the mean were considered as having an “unfavorable” attitude and those scored equal to or above the mean were considered as having a “favorable” attitude.12 Data collectors arranged a comfortable environment by keeping mothers apart and making them free during the interview to minimize social desirability bias.
Data Quality Control
The questionnaire was prepared in English, and translated to the local language Amharic and then back to English by experts of the language to keep its consistency. Training on data collection tools was given to data collectors and supervisors. A pre-test was done on 5% of the sample to assess the clarity of the questions and applicability of the instrument. Cronbach’s alpha was determined (it was 0.86; the acceptable range is >0.7) to assess the reliability of the questionnaire before the actual data collection. Daily supervision was conducted by the supervisors and researcher.
Data Processing and Analyses
Data were double entered into the EPI-Info, exported to SPSS version 21 for cleaning and statistical analysis. Descriptive statistics were used to summarize the variables. Bivariable logistic analysis was done to show the crude effect of each variable on knowledge and attitude. Variables with a P-value of <0.2 in the bivariable analyses were entered into multivariable logistic regression analyses. Odds ratio (OR) with a 95% confidence interval (CI) was computed to assess the strength of association. A P-value of <0.05 was considered statistically significant in the multivariable analyses.
Ethical Approval and Consent to Participate
All procedures involving the research were approved by Jimma University College of Health sciences institutional and review board (IRB). Permission to undertake the study was obtained from the regional, zonal and district administration and health offices of the study area. After the identification of eligible mothers, the nature, and purpose of the study was explained along with their right to refuse. Written informed consent was obtained from all study participants. The right of the participant to withdraw from the study at any time was respected. The study was conducted in accordance with the Declaration of Helsinki. The data were not accessed by a third person, except investigators, and were kept confidential.
Results
Maternal Sociodemographic, Obstetric and Health-Care Characteristics
A total of 612 mothers were recruited in the study yielding a response rate of 100%. The mean (±SD) age of the mothers was of 28 (±5) years. Majority of the mothers were married (93.6%) and had no formal education (77.3%). Majority of the mothers were housewives (85%) and all of their husbands (100%) were farmers. All of the study participants (100%) were from the Amhara ethnic group and Orthodox Christian in religion. The mean (±SD) family size of the respondents was 5.4±1.8.
Respondent’s index children were almost in equal proportion for sex. The majority (82.5%) of mothers were multiparous and nearly half (47.0%) of them perceived their babies’ birth weight as a medium. Nearly three-fourths (71.7%) of mothers had antenatal care (ANC) visits for the index child and 86% of them had less than four ANC visits. Two-thirds (59.2%) of respondents delivered their index child in their home and nearly three-fourths (74.5%) of them had no postnatal care (PNC). Almost one-third (32.2%) of mothers were counseled about child feeding during their pregnancy of the index child. Respondents (79.6%) had no functioning radio at their home. Among respondents who had a functioning radio nearly a quarter (22.4%) of them did listen to seven solutions (a radio drama focused on IYCF) [Table 1].
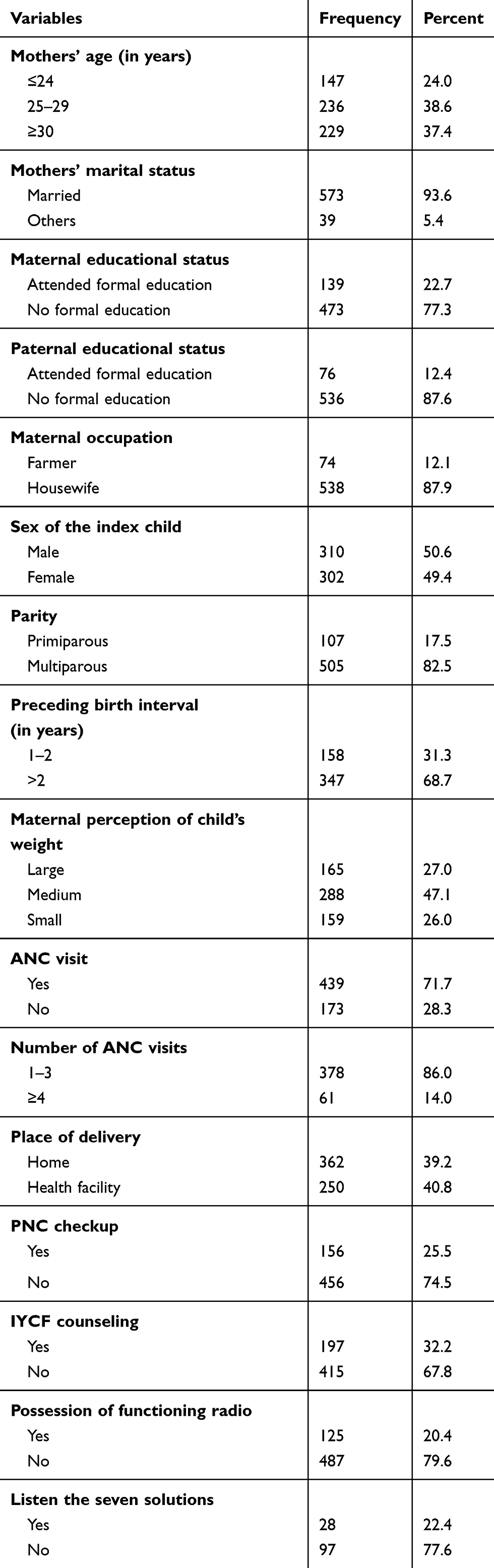 |
Table 1 Maternal Sociodemographic, Obstetric and Health-Care Characteristics, West Gojjam Zone, Northwest Ethiopia, 2017 |
Mothers’ Knowledge on Optimal Complementary Feeding
Overall, 60.0% of mothers had good knowledge of complementary feeding. Regarding the particular knowledge proportions, the majority of the respondents (82.0%) knew the duration of exclusive breastfeeding, and the right age to introduce complementary food (79.0%). Only 32.0% and 22.6% of mothers had known the recommended complementary feeding frequency for 6–8 and 9–23 months of age baby, respectively. Small proportions of the mothers (11.5%) knew the minimum number of food groups a 6–23-month baby should consume. Only 56.0% of mothers knew a non-breastfed baby needs extra meals [Table 2].
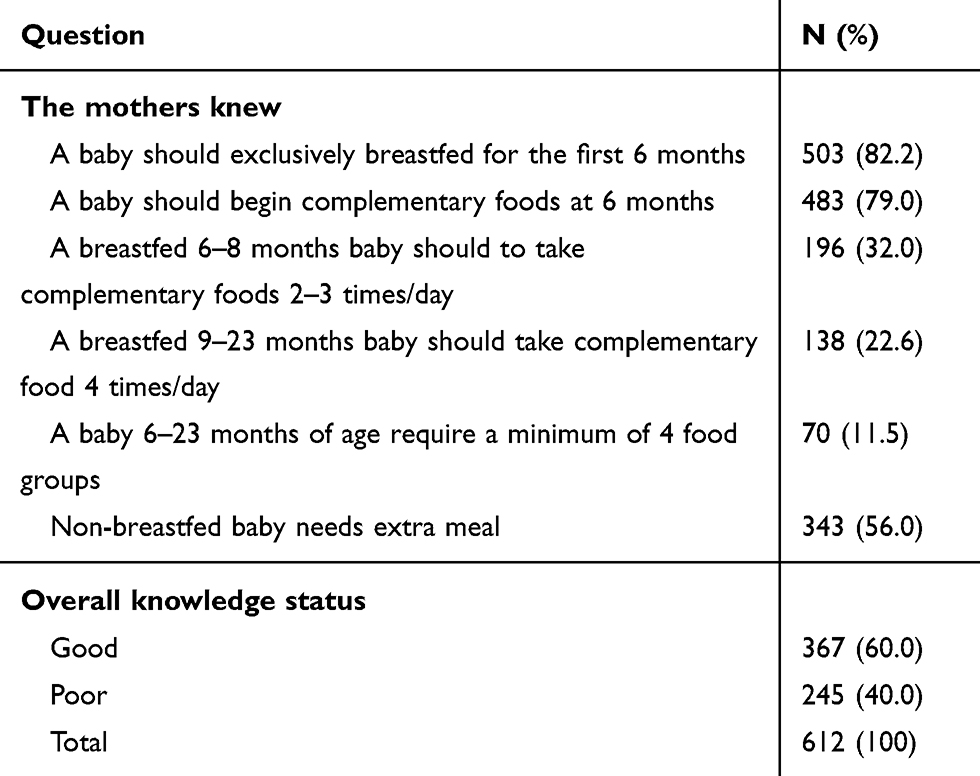 |
Table 2 Mothers’ Knowledge on Optimal Complementary Feeding, West Gojjam Zone, Northwest Ethiopia, 2017 |
Mothers’ Attitude Towards Complementary Feeding
Overall, only 51.0% of mothers had a favorable attitude towards complementary feeding. Regarding the specific attitude proportions, majority of the mothers (72.0%) believe breastfeeding alone is not sufficient for a child after 6 months, and giving complementary foods after 6 months makes a baby healthy (75.0%). Only 45.1% and 42.0% of mothers feel giving fruits and vegetables; and animal-source foods is good for a baby, respectively. Few numbers of respondents (12.6%) believe bottle feeding is not good for child’s health, and giving extra meal is important before and after an illness, 15.0% [Table 3].
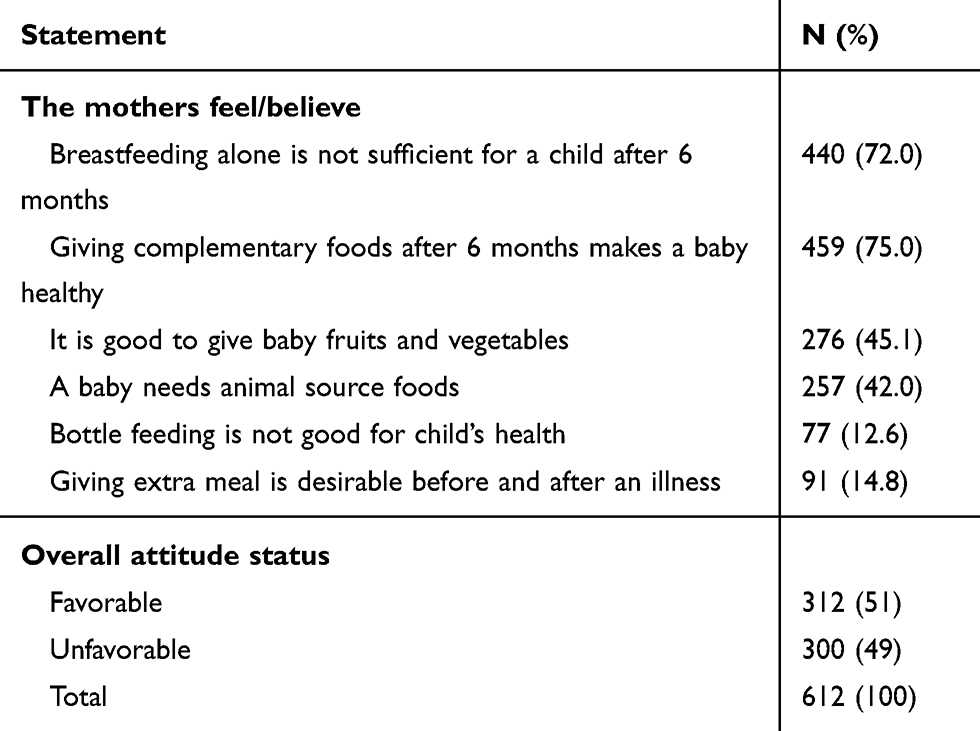 |
Table 3 Mothers’ Attitude Towards Optimal Complementary Feeding, West Gojjam Zone, Northwest Ethiopia, 2017 |
Predictors of Mothers’ Knowledge and Attitude Towards Optimal Complementary Feeding
On multivariable logistic regression analysis, maternal educational status [AOR=2; 95% CI: 1.15–3.43], paternal educational status [AOR=2.2; 95% CI: 1.26–5.13], ANC status [AOR=3.5; 95% CI: 1.9–7.47], place of delivery [AOR=1.8; 95% CI: 1.13–2.83], PNC status [AOR=2.2; 95% CI: 1.32–3.73], and IYCF counseling [AOR= 2.5; 95% CI: 1.46–7.52] were significantly associated with mothers’ knowledge on optimal complementary feeding. Likewise, maternal educational status [AOR=2.5; 95% CI: 1.49–4.02], ANC status [AOR=2.7; 95% CI: 1.54–4.57], IYCF counseling [AOR= 2.2; 95% CI: 1.47–4.89], and possession of radio [AOR= 1.8; 95% CI: 1.35–3.82] were positively associated to attitude of mothers towards optimal complementary feeding [Table 4].
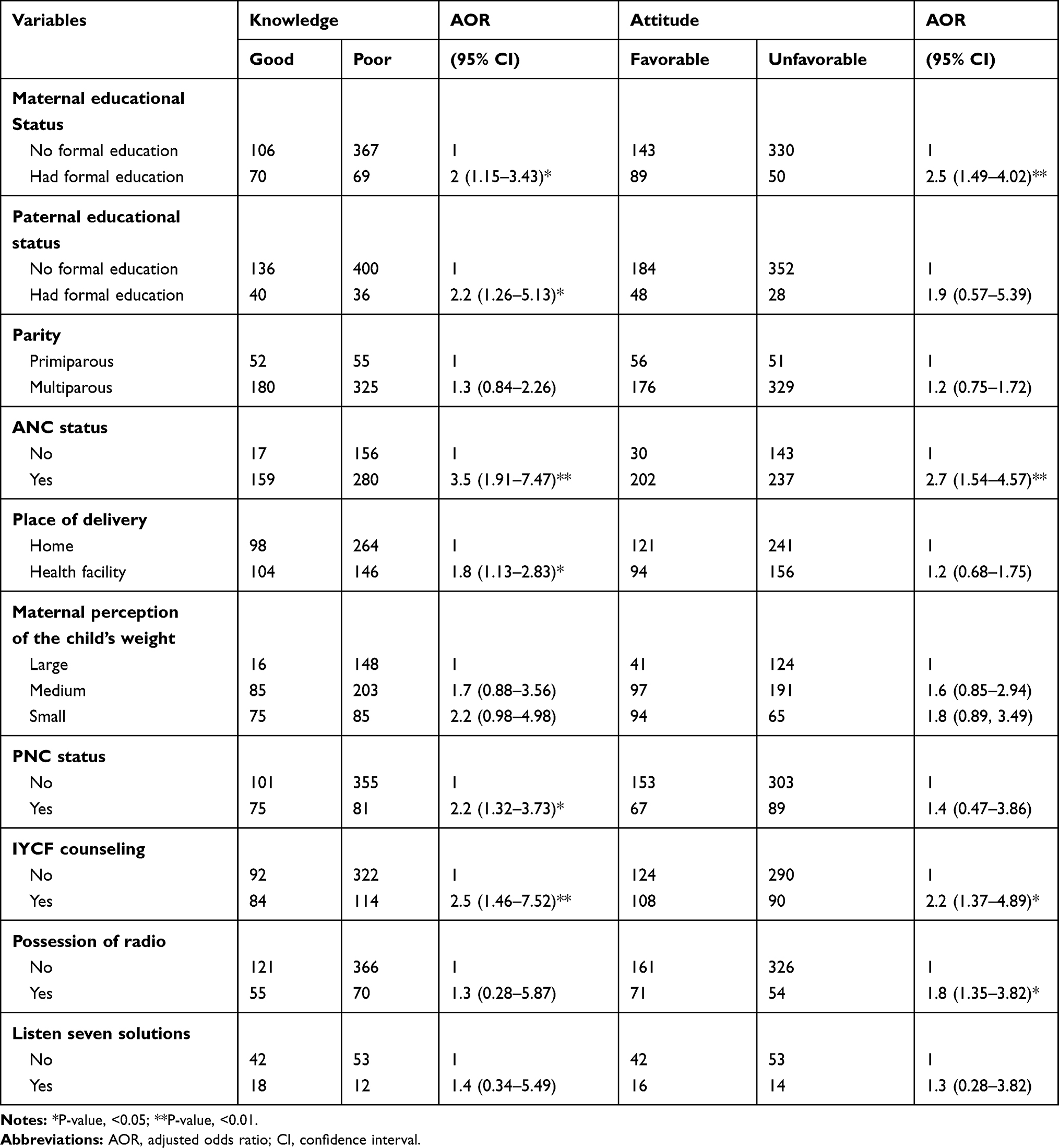 |
Table 4 Multivariable Logistic Regression Model Predicting Mother’s Knowledge and Attitude on Optimal Complementary Feeding, West Gojjam Zone, Northwest Ethiopia, 2017 |
Discussion
Mothers who have good knowledge and favorable attitude on optimal complementary feeding practice are more likely to have better feeding practice than those who have poor knowledge and unfavorable attitude.10 This study examined the level and predictors of knowledge and attitude of mothers on optimal complementary feeding. The information generated could be useful for health and nutrition policymakers to design evidenced-based and effective intervention strategies to improve child feeding practices thereby child’s growth, development and survival.
In this study, overall 60.0% of the mothers had good knowledge of complementary feeding. This result was higher than the study done in Nigeria (15.0%)17 but lower than the result found in Kosova (88.4%).18 This may be due to differences in sociodemographic characteristics of the study subjects.
Regarding the specific knowledge levels, 71.6% of mothers knew the recommended duration of exclusive breastfeeding, which was consistent with the findings done in Bahir Dar (84.3%),19 and Fiche Town (80.0%).20 It was higher than the study finding in Mizan Aman (34.7%),21 and lower than the result found in Ghana (97.5%).22 Exclusive breastfeeding in the first 6 months of life saves lives. During this period, an infant who is not breastfed is more than 14 times more likely to die from all causes of mortality than an exclusively breastfed infants.23
WHO recommends that babies should begin complementary foods at the sixth month of age. Locally accessible and affordable foods that enrich the baby’s diet with additional calories and micronutrients should be offered.23 In this study, 79.0% of the mothers knew the right age to introduce complementary food which was lower than the study done in Bahir Dar (88.0%),19 but higher than the result found in Fiche Town (80.0%).20
Only 32.0% of mothers in this study knew the recommended complementary feeding frequency per day which was consistent with the findings in Bahir Dar (31.0%)19 and Nigeria (29.6%).17 However, it was much lower than the study done in Ghana (86%).11 This could be differences in the study settings. In this study, 56.0% of respondents knew that non-breast feed infants needs extra meals which was slightly lower than the study done in Bahir Dar (67.0%).19
Regarding mothers’ attitude towards complementary feeding, overall 51.0% of the mothers in this study had a favorable attitude towards complementary feeding which was consistent with the study done in India (50.0%),24 but higher than the finding in Yemen (13.0%).25
Several determinants can affect mothers’ knowledge and attitude towards complementary feeding. These determinants include maternal age, educational, marital, and work status of the mother, residence, exposure to mass media, family size, wealth status, antenatal care visits, place of delivery, age and sex of the child.26
In Ethiopia, each woman who comes to the health facilities for different services is being counseled on child nutrition including IYCF practices. Moreover, education on IYCF is being given by health extension workers to all pregnant and lactating women at health posts and home. All these have a direct contribution to maternal knowledge and attitude on complementary feeding. However, women’s health-care utilization habits and implementation of the recommendations are poor.6
In this study, mothers who had formal education were more likely to have good knowledge and a favorable attitude about optimal complementary feeding than those who had no formal education. This might be due to the fact that literate mothers can understand nutrition information which empowers them to resist external interferences and pressures. Similarly, mothers who had ANC follow-up were more knowledgeable and had a favorable attitude towards optimal complementary feeding than those who had no ANC follow-up. The possible reason is that mothers who have ANC follow-up are more likely to be counseled by health professionals about optimal complementary feeding practices.
The odds of having good knowledge and favorable attitude about optimal complementary feeding were higher among mothers who had IYCF counseling as compared to those who had no IYCF counseling. This significant association can be explained by the fact that IYCF counseling has a direct contribution and a pivotal role in enhancing mothers’ complementary feeding knowledge and attitude.
The odds of having good knowledge about optimal complementary feeding were higher among mothers who had PNC follow-up as compared to those who had no PNC follow-up. Likewise, mothers who delivered at health facilities were more likely to have good knowledge about optimal complementary feeding than those who gave birth at home. The likely explanation could be mothers who gave birth at health institutions have a better opportunity to access the appropriate child feeding information that can improve their knowledge about complementary feeding.
Mothers who had a functioning radio were more likely to have a favorable attitude on optimal complementary feeding than those who had no radio. The likely reason could be respondents who had radio have a better opportunity to get child feeding education broadcasted by radio.
Strength and Limitation of the Study
Strength of this study includes pre-test before the actual study and implementation of frequent supervision during data collection. There are also limitations to be mentioned. First, this study might have information bias for the knowledge and attitude questions which might have led to the over-reporting of the desirable answers due to fear of being judged. Second, since it was a cross-sectional study, causal inferences between variables cannot be investigated.
Conclusion and Recommendations
This study showed that the overall level knowledge and attitude of mothers on complementary feeding were low. Hence, behavior change intervention on optimal complementary feeding focusing on age-specific meal frequency and diversification (the significance of fruits, vegetables and animal-source foods); feeding during and after illness and the negative impact of bottle feeding should be strengthened in the community. Moreover, interventions that can improve the health-care utilization of mothers have to be applied to use health facilities as an opportunity to deliver counseling and support on optimal complementary feeding practices.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All procedures involving the research were approved by Jimma University College of Health sciences institutional and review board (IRB). Permission to undertake the study was obtained from the regional, zonal and district administration and health offices of the study area. Written informed consent was obtained from all study participants. The data were not accessed by a third person, except investigators, and were kept confidential.
Acknowledgments
We would like to thank the study participants for providing valuable information. We are also grateful to express our gratitude to data collectors and supervisors for their commitment.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no competing interests.
References
1. Indicators for assessing infant and young child feeding practices. Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington DC. 2007:1–19.
2. World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices. World Health Organization; 2010. Available from: https://apps.who.int/iris/bitstream/10665/42590/1/9241562218.pdf.
3. Ruel M, Hoddinott J Early childhood nutrition. 2008. Available from: https://www.researchgate.net/publication/23778956.
4. de Souza S, Caetano C, Ortiz T, et al. Complementary feeding of infants in their first year of life: focus on the main pureed baby foods. Rev Assoc Med Bras. 2014;60(3):231–235.
5. WHO. Global Strategy for Infant and Young Child Feeding. Fifty-Fourth World Heal Assem. Vol. 1; 2001:5.
6. Chung SS, Yeh CH, Feng SJ, et al. The impact of STI induced reliabilities for scaled p-MOSFET in an advanced multiple oxide CMOS technology.
7. Al-mekhlafi MSH, Surin J, Atiya AS, Ariffin WA, Mahdy AKM. Current prevalence and predictors of protein-energy malnutrition among schoolchildren in rural Peninsular Malaysia. Southeast Asian J Med Public Health. 2008;39(5):922–931.
8. WHO Guideline. Improving childhood development-summary. 2019. Available from: www.who.int/maternal_child_adolescent/child/summary_guideline_improving_early_childhood_development.pdf.
9. Pelletier DL, Frongillo EA, Habicht JP. Epidemiologic evidence for a potentiating effect of malnutrition on child mortality. Am J Public Health. 1993;83(8):1130–1133. doi:10.2105/AJPH.83.8.1130
10. Egata G, Berhane Y, Worku A. Predictors of non-exclusive breastfeeding at 6 months among rural mothers in east Ethiopia: a community-based analytical cross-sectional study. Int Breastfeed J. 2013;8:8.
11. Gyampoh S, Otoo GE, Aryeetey RN. Child feeding knowledge and practices among women participating in growth monitoring and promotion in Accra, Ghana. BMC Pregnancy Childbirth. 2014;14(1):180. doi:10.1186/1471-2393-14-180
12. Fadare O, Id MA, Mavrotas G, Akerele D, Ogunniyi A. Mother ’ s nutrition-related knowledge and child nutrition outcomes: empirical evidence from Nigeria. PloS One. 2019;14:e0212775.
13. FMOH. National strategy for infant and young child feeding. 2004 April 1–23. Available from: https://motherchildnutrition.org/nutrition-protection-promotion/pdf/mcn-national-startegy-for-inafnt-and-young-child-feedign-ethiopia.pdf.
14. Caulfield LE, Huffman SL, Piwoz EG. Interventions to improve intake of complementary foods by infants 6 to 12 months of age in developing countries: impact on growth and on trie prevalence of malnutrition and potential contribution to child survival. Food Nutr Bull. 1999;20(2):183–200. doi:10.1177/156482659902000203
15. Amhara Regional State. Budget brief amhara regional state 2007/08 – 2015/16. Unicef. 2016.
16. Arikpo D, Edet ES, Chibuzor MT, Odey F, Caldwell DM. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst Rev. 2018;5:1–147. doi:10.1002/14651858.CD011768.pub2.www.cochranelibrary.com
17. Olatona FA, Adenihun JO. Complementary feeding knowledge, practices, and dietary diversity among mothers of under-five children in an urban community in Lagos state, Nigeria. Int J MCH AIDS. 2017;6(1):46. doi:10.21106/ijma.203
18. Berisha M, Ramadani N, Hoxha R. Knowledge, attitudes and practices of mothers in Kosova about complementary feeding for infant and children 6–24 months. Med Arch. 2017;71(1):37–41. doi:10.5455/medarh.2017.71.37-41
19. Demilew YM. Factors associated with mothers ’ knowledge on infant and young child feeding recommendation in slum areas of Bahir Dar City, Ethiopia: cross sectional study. BMC Res Notes. 2017;10:191. doi:10.1186/s13104-017-2510-3
20. Shukure R. Assessment of knowledge, attitude and practice on initiation of complementary feeding among under two years children in Fiche Town, North Showa Zone, Ethiopia. Int J Biomed Eng Clin Sci. 2017;3(6):103–109. doi:10.11648/j.ijbecs.20170306.16
21. Tadele N, Habta F, Akmel D, Deges E. Knowledge, attitude and practice towards exclusive breastfeeding among lactating mothers in Mizan Aman town, Southwestern Ethiopia: descriptive cross- sectional study. Int Breastfeed J. 2016;11:3. doi:10.1186/s13006-016-0062-0
22. Nukpezah RN, Nuvor SV, Ninnoni J. Knowledge and practice of exclusive breastfeeding among mothers in the tamale metropolis of Ghana. Reprod Health. 2018;15:140.
23. Black RE, Allen LH, Bhutta ZA, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371:243–260.
24. Karnawat D, Karnawat BS, Joshi A, Kohli GK. Knowledge, attitude & practices about infant feeding among mothers of urban & rural areas of Ajmer district. J Med Res. 2015;1(3):90–94.
25. Dallak AM, Al-rabeei NA, Aljahmi YA. Breastfeeding knowledge, attitude, and practices among mothers attending health centers in Sana ’ a City. ARC J Public Health Community Med. 2016;1(2):9–17.
26. Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International; 2012.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.