")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Lessons from China’s Experience: Legal Analysis of Health Risks and Medical Obstacles of Personnel in COVID-19 Control Areas
Authors Zheng L , Li T , Chen Q
Received 5 February 2023
Accepted for publication 12 April 2023
Published 20 April 2023 Volume 2023:16 Pages 735—745
DOI https://doi.org/10.2147/RMHP.S407362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Long Zheng,1 Taoying Li,2 Qiang Chen3
1Graduate School and Open Learning College, Cavite State University, Indang, Philippines; 2Department of Law, Jiangxi Police College, Nanchang, People’s Republic of China; 3Urban and Rural Cultural Development Research Center, Guangzhou College of Applied Science and Technology, Guangzhou, People’s Republic of China
Correspondence: Taoying Li, Department of Law, Jiangxi Police College, No. 1666 Xingwan Avenue, Xinjian District, Nanchang, Jiangxi Province, People’s Republic of China, Tel +8618279129536, Email [email protected]
Purpose: Individuals in controlled areas often face restrictions on their personal freedom, and if they are unable to receive medical treatment when needed, it can significantly increase their health risks. However, current epidemic prevention and control policies do not provide clear guidelines on how to ensure individuals in controlled areas to seek medical attention when faced with health problems. By implementing specific measures that local governments must take in order to protect the health of those in controlled areas, the risks to their health can be greatly reduced.
Patients and Methods: Our research utilizes a comparative approach to analyze the measures adopted by various regions for safeguarding the health of individuals in control areas, and the diverse outcomes they produce. We conduct empirical analysis and present examples of severe health risks that individuals in control areas face due to inadequate health protection measures. Furthermore, we conduct a critical evaluation of China’s legal management of control areas, identifying both its principles and shortcomings.
Results: The lack of unified legal regulations has led some local governments to make some shortcomings in making decisions on epidemic prevention and control. Specifically, some governments have neglected to provide adequate medical protection for individuals in controlled areas, limited the authority of specific implementers of prevention policies, and failed to establish fair punishment mechanisms. These shortcomings have a direct impact on the health of those in controlled areas and can even lead to tragic outcomes.
Conclusion: Effective management of individuals in control areas during public health emergencies is crucial in reducing health risks. To achieve this, China needs to establish unified regulations and requirements, particularly with regards to medical protection, for individuals in control areas. Such measures can be achieved through the improvement of legislation, which can significantly reduce health risks faced by individuals in control areas during public health emergencies.
Keywords: COVID-19, people in control areas, health risks, healthcare, Chinese law
Introduction
On January 4th 2022, a netizen’s microblog caused outrage among Chinese netizens. The blog was released by a family member of a pregnant woman in Xi ‘an, in which she said: On January 1, a pregnant woman could not reach the 120 emergency hotline for her stomach pain, and then called the 110 police to send her to the hospital. She arrived at the Xi’an High-Tech Hospital at 8:00 p.m. but was unable to be admitted at the entrance due to the lack of a negative nucleic acid certificate within the prescribed time required by the hospital, so she waited until 10:00 p.m. During the waiting time at the entrance, the pregnant woman had a hemorrhage and her 8-month-old baby was miscarried. According to her description, someone else experienced the same thing in Xi’an at that time: she was pregnant too, and could not reach 120, so she could not seek medical treatment in time at the hospital, which finally led to abortion.1,2 At that time, Xi’an was under a city-wide lockdown due to COVID-19 prevention and control.3 The incident quickly went viral on the Internet and attracted tremendous attention and discussion. On January 5th 2022, an investigation organized by the Health Commission of Shaanxi Province and Xi’an City was conducted and the incident was considered as a liability accident. The Health Commission of Xi’an City instructed Xi’an Gaoxin Hospital to take the initiative to communicate with the patient, prepare for the postoperative rehabilitation treatment and reassurance compensation, and apologize to the public.4,5 However, the handling of relevant responsible people has not stopped public reflection on this incident, and the incident was continuously spread on various platforms, forcing people to pay more attention to and think about the health risks caused by medical obstacles of people in COVID-19 control zones.
Of course, such a situation is not that common in China, and China’s government has made great efforts to safeguard the health of people in control zones. China’s government has provided various preventive interventions at all costs to protect individual and public health.6 Since the outbreak of COVID-19 epidemic in China in 2020, the National Health Commission of People’s Republic of the China has repeatedly emphasized the need to give priority to ensuring the medical needs of groups such as acute and critical patients by means of documents or holding press conferences7 and has provided free treatment for these individuals.8 On July 18th 2020, the National Health Commission of People’s Republic of China made the Notice on the Normalization of Epidemic Prevention and Control under Notice on Standardizing the Diagnostic and Treatment Process in Medical Institutions (Joint Prevention and Control Mechanism Medical Hair [2020] 272). It has clearly stated that medical institutions shall establish green channels for the treatment of patients with acute and critical illnesses, and perform nucleic acid testing while actively resuscitating patients who cannot be excluded from COVID-19. Epidemic prevention and control shall not be used as an excuse to delay treatment or put off patients with acute and critical illnesses.” Since 2022, National Health Commission of People’s Republic of China has again given guidance on medical protection and health of people in the control zones, including the establishment of a ledger for health-sensitive people in the control zones, for the aim of responding to their needs immediately. Specifically, green channels should be constructed for medical treatment and patients with chronic diseases like diabetes and hypertension should be assured of their daily medication needs, etc.9 Many local governments have also formulated their own local policies on medical care for people in the control zones according to the guidelines of the National Health Commission of China, and have achieved good results. Take Beijing as an example, has taken a number of measures to satisfy the medical needs of people in the control zones, including the establishment of a Service Hotline and an emergency fleet. In April 2022, Ms. Yang’s father had a heart attack in Beijing, yet the ambulances could not enter the control zone. She dialed the hotline and the community workers quickly came to her home and issued a request for medical treatment, arranging for her father to go out for medical treatment.10,11
Through the introduction of the above two incidents, it is not difficult to find that different local epidemic prevention policies have a significant impact on the health of people in the control zones.
It is undeniable that the COVID-19 pandemic has wreaked havoc on global healthcare systems,12 the response to the pandemic has violated the health framework, including the right to health,13,14 reinforcing the need for better public policy making by states to protect the health of their citizens.15 In his regular press conference, WHO Director-General Tedros stated that despite the crisis, basic health services must continue. Babies are still being born, and vaccines must still be delivered. People with other diseases still need treatment to save their lives”.16 We cannot neglect the treatment of other diseases because of the COVID-19 pandemic. This is especially important for those in control zones, who are not only at high risk of COVID-19 infection, but also face other health risks,17 since their personal freedom is restricted for public interest.18 They are more dependent on government policies for their health and medical care. Therefore, we must pay attention to the health rights of this group of people in order to build a way forward with these rights at the core.19
These issues have also clearly drawn attention.Especially the impact of COVID-19 isolation measures on mental health.20,21 Recent studies have suggested that individuals subjected to pandemic-related isolation are at an increased risk of mental health problems, particularly adolescents.22,23 Additionally, elderly and pregnant individuals require special care during isolation.24–26 While much research has focused on community and individual self-regulation during isolation, it is important to recognize that laws also serve as a social determinant of health.27
While China has adjusted its COVID-19 control measures and management program,28 it is important to recognize that this pandemic may not be the last. As WHO Director-General Tedros has pointed out, “outbreaks and pandemics are inevitable, and we must be better prepared to handle the next one”.29 By learning from the lessons of COVID-19 and establishing a more robust legal system, we can respond more rationally to future public health emergencies and minimize the harm to individual citizens.This is not only for China, but also for other countries.
Delineation and Management of Control Zones
In order to prevent the spread of COVID-19, China has achieved good results in preventing and controlling COVID-19 pandemic by controlling the zones with the risk of COVID-19 spread and limiting the free movement of people in this area.30 In China, hierarchical management is implemented according to the high risk of virus infection in the zones. In China, according to the regional risk of virus infection, it is managed at different levels. There are lockdown zones, control zones, precaution zones.31
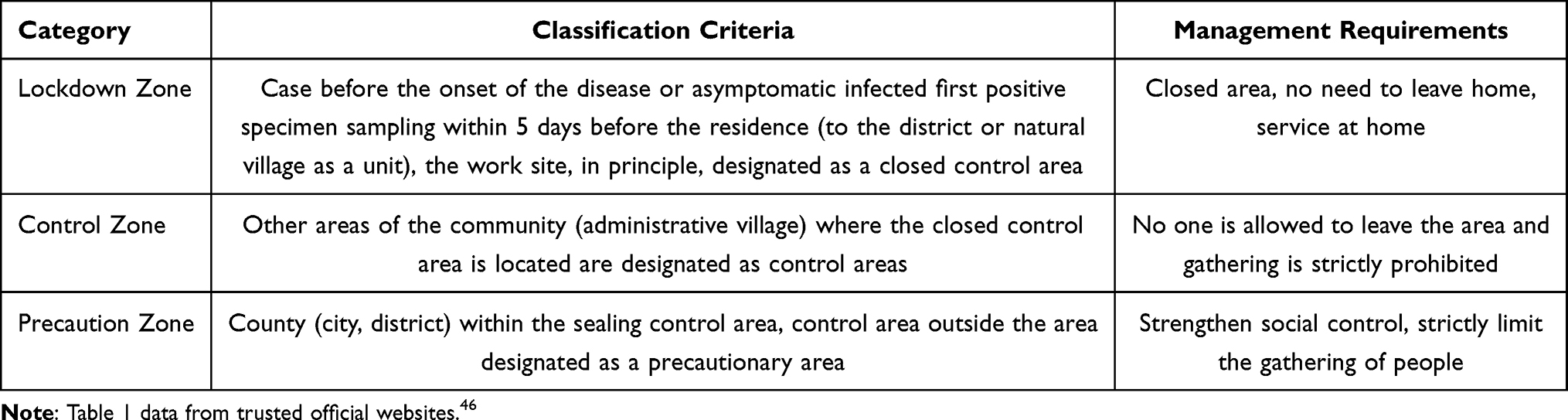 |
Table 1 The Classification Criteria and Management Requirements of China’s Lockdown, Control an Precaution Zones |
In the management of the lockdown zones, control zones and the precaution zones, the management of the lockdown zones is the strictest, which follows the principle of “area closed, without leaving home, service door-to-door”. Firstly, compulsory regional isolation measures should be implemented in the lockdown zones. The entire lockdown zone only retains an entrance and exit, and the establishment of posts, for 24-hour guard duty. Secondly, the flow of people in the zone was strictly restricted. All the residents in the lockdown zone were not allowed to go out of their homes; vehicles were prohibited to pass; the buildings (units) were sealed and controlled; and the community arranged for 24-hour patrol duty to strictly prevent people from going out. Thirdly, residents are not allowed to gather, business service in the region were stopped, and all entertainment places, restaurants, shops, fitness club and cultural activities, etc. are closed.
The management of the control zones is relatively lenient compared to the lockdown zones, which should follow the principle of “no people leaving the area, no gathering”. First, the compulsory regional isolation measures are implemented. Only one entrance and exit in the control zones are reserved, and people are assigned to guard the area 24 hours a day to ensure that only people can get in and out. Second, the movement of people in the area is restricted. Each household living in the control zone can arrange for one person to buy living materials in designated place on the premise of strict personal protection every two days, and vehicles are forbidden to pass in the control area. Third, it is strictly forbidden to gather people. Basketball courts, badminton courts, fitness clubs and other facilities in the control zones are closed. All kinds of group gathering activities are suspended.
Compared with the former two, the management of the precaution zone is the most relaxed. The precaution zone follows the principle of “strengthening social control, strictly limiting the gathering of people”. First, traffic restrictions are implemented. Vehicles entering and leaving the zone are carefully ordered. Residents’ safety is guaranteed. Second, residents’ gathering is moderately restricted moderate restrictions on the gathering of people. Gathering activities such as family gatherings and dinners are strictly restricted. Activities of chess rooms, theaters, Internet cafes and other indoor public places in the zone are suspended. Third, public places are strictly controlled. For shopping malls, supermarkets, farmers’ markets and other basic living materials supply places in the region, people entering the market are reasonably controlled. Working from home are advocated.
The expression of the control areas in this article refers to the lockdown zones and control zones.
China’s Legal System and the Basis for Developing Health Policies for People in Control Areas
In China, laws can be roughly divided into four levels according to their validity (Figure 1), namely the Constitution, laws, administrative regulations and local regulations. The Constitution is the fundamental law of the country and the basis for all other laws and regulations, which applies to all citizens of the country and has the highest authority, and no law, administrative regulation, or local regulation can contradict the Constitution. Laws are normative legal documents formulated by the National People’s Congress and its Standing Committee, which are the most authoritative norms other than the Constitution. Administrative regulations are the laws and regulations formulated by the State Council to lead and they are made by the State Council in accordance with the Constitution and laws to lead and manage the administrative work of the country, and are the general term for all kinds of regulations on politics, economy, education, science and technology, culture, foreign affairs, etc. Administrative regulations cannot contradict the Constitution and laws, and are less authoritative than laws. Local regulations are made by the people’s congresses and their standing committees at the provincial level and by local governments in accordance with the specific conditions and practical needs of their administrative regions, and are not in conflict with the Constitution, laws and administrative regulations. Local laws and regulations are formulated on the premise that they do not contradict the Constitution, laws and administrative regulations.
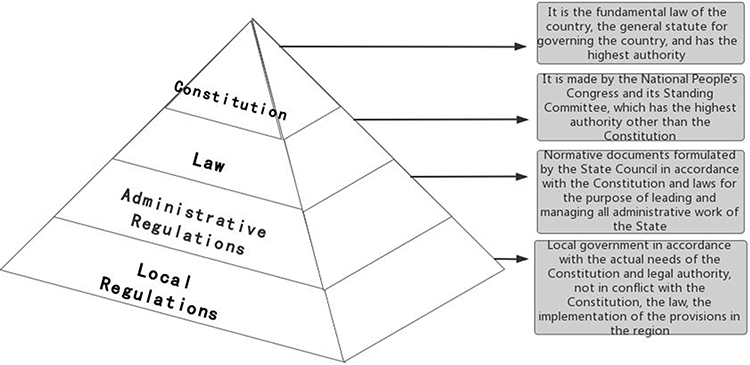 |
Figure 1 China’s Law Framework. (This picture shows the composition of China’s legal system, with the Constitution having the highest authority, followed by laws, administrative regulations at the third level of effectiveness, and local regulations at the lowest level). |
The provisions on the delineation of control zones and the medical protection of people in the control zones are covered in the Constitution, laws and administrative regulations, but none of them make clear provisions on the specific measures of protection. For example, Article 21 of the Constitution of the People’s Republic of China stipulates that the state develops medical and healthcare, develops modern and traditional medicine, encourages and supports rural collective economic organizations, state enterprises and institutions, and street organizations in organizing various medical and health facilities, carrying out mass health activities, and protecting the health of the people. This stipulates that the state has the obligation to protect people’s health, but it does not mention how to regulate the health and medical security of people in the control area in case of public health emergencies. For example, Article 41 of the Prevention and Control of Infectious Diseases Law of the People’s Republic of China (PCIDL) provides that the government at or above the county level that implements isolation measures shall provide living security for the isolated personnel; local governments should provide various livelihood protection measures for the personnel in the quarantine area while delineating the quarantine area. It is not clearly stipulated how and to what extent the security should be provided, and it is not specifically stipulated on the health and medical treatment of the people in the isolated area.
Article 17 of the People’s Republic of China Emergency Response Law (ERL) stipulates that local governments can formulate corresponding emergency plans according to relevant laws and regulations, the emergency plans of the people’s governments at higher levels and their relevant departments, and the actual situation in the region. This is an authorization for local governments to formulate local policies in response to emergencies. In the administrative regulations, there are also no detailed provisions on the medical security of people in the control zone. The Regulations on the Administration of Medical Institutions formulated by the State Council only stipulate that medical institutions are to save lives, prevent and treat diseases, and serve the health of citizens, which are the principles on the duties of medical institutions. In the absence of clear and specific provisions in the superordinate law, local governments have formulated local policies in response to the COVID-19 pandemic based on the authority of the law in conjunction with the actual situation in the region. However, due to the lack of clear provisions of the higher law, local policies lacked formulation standards, leading to some unreasonable local policies that created medical barriers and health risks for people in the control zones.
Types of Medical Barriers for People in Control Areas in Some Regions
Negligence of Local Policies on Medical Coverage for People in Control Areas
In order to prevent and control the epidemic, some local governments have taken measures, including suspending medical services in some hospitals, which have caused great health risks to people in the controlled areas. On March 25th, 2022, a nurse in Shanghai had an asthma attack at home, yet the medication could not be relieved on time. Her family took her to the nearest Eastern Hospital where she worked for medical treatment. However, when she arrived at the entrance, the hospital closed the emergency room for epidemic prevention and control and thus refused to admit her for treatment. She and her family had no choice but to go to the East Hospital of Renji Hospital, which was the only hospital that accepted emergency cases at that time. However, it took several hours of tossing and turning, delaying the best time for treatment, and the nurse died at around 11:00 pm that night.32 At that time, Shanghai was under high pressure control of the epidemic, and most of the areas adopted measures of containment and control. According to statistics, a total of 41 medical institutions in Shanghai suspended some of their medical services, including emergency medical services, to cooperate with the epidemic coordination work.33 Providing medical care to such a large number of people in control zones requires more personnel, material, and financial resources, and should preserve the ability to provide medical care for all in an emergency.34 However, at this time, so many medical institutions in Shanghai have stopped providing medical services, which not only aggravates the shortage of medical resources, but also neglects the medical security of people in the controlled areas.
Limited Decision-Making Power of the Specific Implementers of the Epidemic Prevention Policy
In China, a total of 5 departments are involved in the management of the control zones (Figure 2). Among these departments, the COVID-19 Epidemic Prevention and Control Command has the highest authority and systematically coordinates the prevention and control of COVID-19, including the delineation of control areas. The local health councils follow and are the formulators of regional management measures. Hospitals, communities, and police are the specific implementers of COVID-19 prevention and control policies, with much less authority than the COVID-19 Epidemic Prevention and Control Command and health councils, and often need to seek authorization for the implementation of specific epidemic prevention measures.35
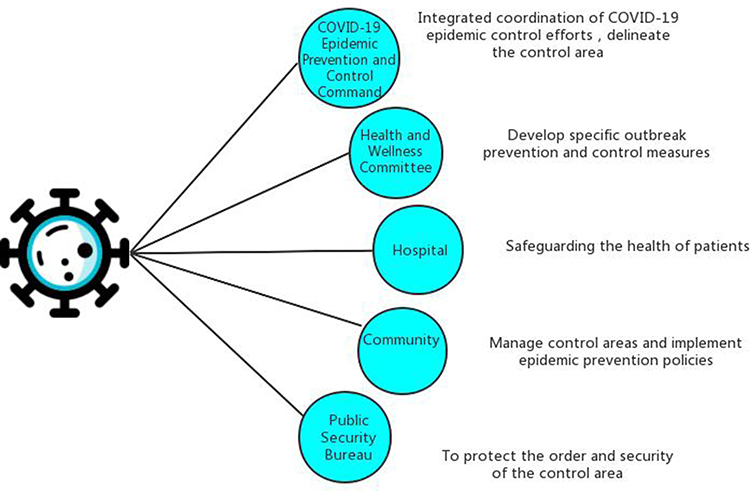 |
Figure 2 Chinese departments involved in COVID-19 epidemic prevention and control. (This image shows a total of five departments in China that are primarily responsible for and involved in the control of COVID-19 and their specific responsibilities in the control of the COVID-19 epidemic). |
On November 1st, 2022, a 3-year-old boy died of carbon monoxide poisoning in Xiyuan Street, Qilihe District, Lanzhou, Gansu Province.36 In this incident, netizens questioned why it took nearly 2 hours for an ambulance to arrive in 10 minutes. Why did not the community staff provide help to the patient in the first place? The reason lies in the fact that hospitals and communities are controlled as the specific authority of the epidemic prevention policy, but hospitals in this case do not have the authority to open special emergency hotlines and send special rescue vehicles for people in the control area. Community workers need to report the situation through layers of instructions to get the final authorization to implement rescue measures. As Table 2 shows, the 3-year-old boy’s life was consumed minute by minute in the interconnection of different agencies. Obviously, the direct manager of the control zone and the specific implementer of the epidemic prevention policy should be given discretionary power in emergency situations in order to save valuable time for the medical activities of the people in the control zone. Although the responsible personnel were held accountable afterwards, today, with the normalization of epidemic prevention and control, the protection of the health rights of those who are restricted from traveling due to epidemic prevention and control cannot be promoted by tragedy, but should be guaranteed by a comprehensive mechanism.
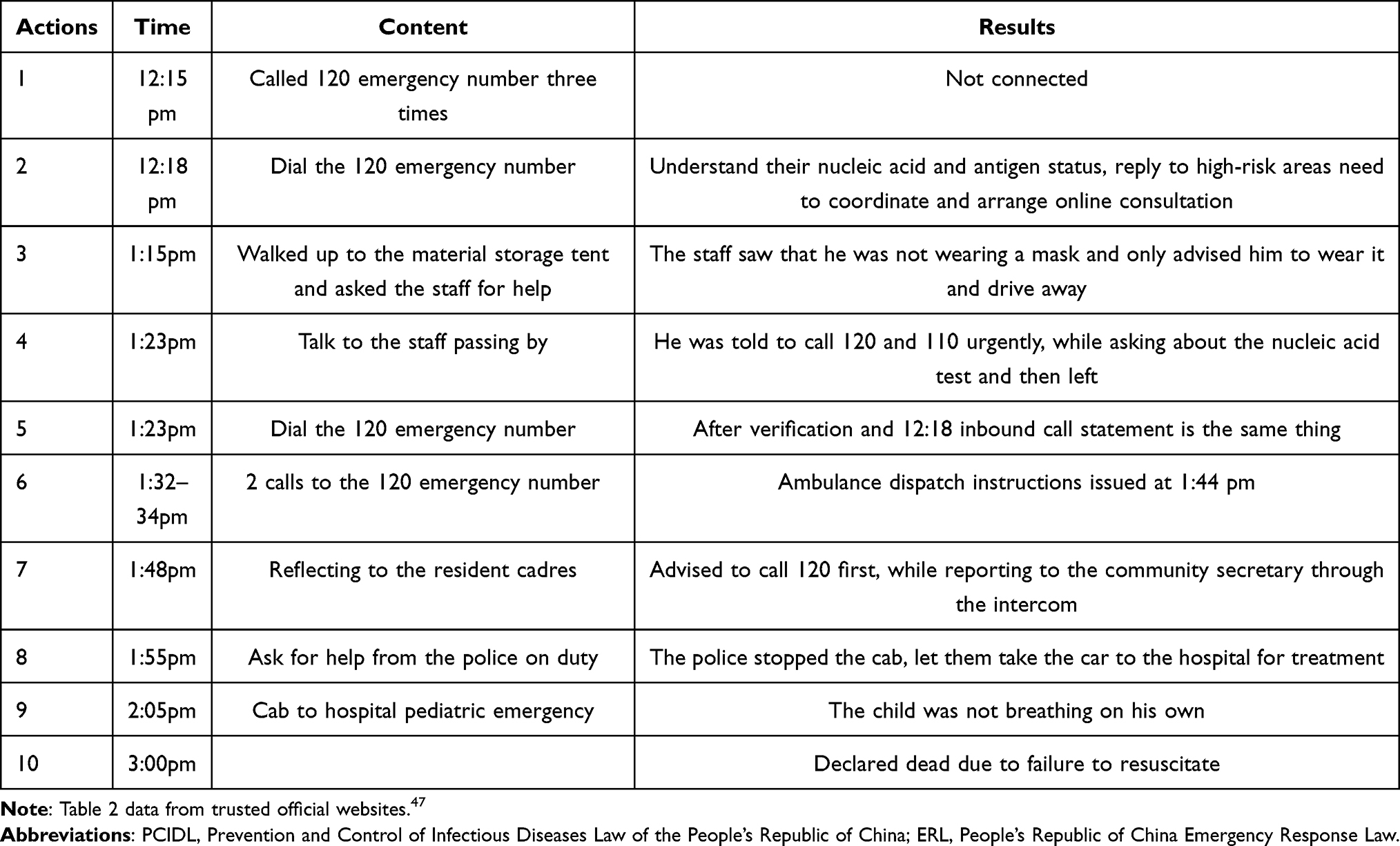 |
Table 2 Official Notification of Lanzhou 2-Year-Old Boy’s Gas Poisoning Death Investigation Details |
Lack of Fair Punishment Mechanism
Although Article 1218 of the Civil Code of the People’s Republic of China stipulates the liability of medical institutions for medical treatment: “If a patient suffers damage during medical treatment activities and the medical institution or its medical personnel are at fault, the medical institution shall bear the liability for compensation”. This is a punitive damages provision in the case of medical institutions’ faults. Strictly speaking, it is the division of civil tort liability, and it is not a special punishment for the ineffective health protection of people in the control area in public health emergencies. Article 335 of the Criminal Law of the People’s Republic of China stipulates that medical personnel who are seriously irresponsible and cause death or serious damage to the health of the patients shall be sentenced to fixed-term imprisonment of not more than three years or criminal detention. This is a punishment for medical personnel who are seriously negligent and cause serious consequences, in order to warn medical personnel to perform their duties seriously. It is a general regulation, and it is not specifically for the punishment of ineffective medical protection of people in the control area during public health emergencies. Moreover, in epidemic prevention and control, medical institutions often use the execution of epidemic prevention and control as an excuse to deny responsibility for fault in specific incidents. It is difficult to punish medical institutions on the basis of the punitive provisions of the Civil Code of the People’s Republic of China and the Criminal Law of the People’s Republic of China. Taking the miscarriage of the pregnant woman in Xi’an as an example, the punishment for the hospital involved is as follows: 1. Shut down for rectification for 3 months, and reopen after the rectification is qualified; 2. Give a warning; 3. Instruct Xi an Gaoxin Hospital to investigate the responsibility of the head of the hospital, suspend the general manager, and remove the post of outpatient department director, obstetric department director and deputy director of medical department; 4. Inform criticism with the public, interview the hospitals main responsible person, and instruct the hospital to reassure patients and families.37 The nature of the punishment is neither civil nor criminal, but a relatively light administrative punishment. In contrast, the punishment for operators who fail to implement various preventive and control measures, such as “scanning the premises code, taking body temperature, and reminding to wear masks”, is also suspension,38 and the staff who fail to implement the epidemic prevention and control work are punished, accountable, dismissed, or even further processed after filing a case.39,40 A comparison of the two shows that the punishment for medical institutions that cause serious consequences is not heavier than that for operators that do not cause serious consequences. This is because the lack of specific penalty provisions leads to a lack of clear criteria for the punishment of specific implementing agencies and executors of the policy, which leads to an imbalance between the severity of the punishment and the serious consequences of ineffective medical care for those in the control zone, and thus making it difficult to create a deterrent.
German Policy on the Management of COVID-19 Segregated Personnel
Although China’s outbreak prevention and control measures have been highly praised by WHO,41 other countries’ outbreak prevention and control measures are also worth learning and absorbing from China, especially the health protection measures for those under control. Germany, for instance, had a relatively low excess mortality rate during the COVID-19 crisis, one of the lowest among European countries.42 This success can be attributed to the amendment to the German Act on the Prevention and Control of Infectious Diseases, which clarified the authorities’ responsibilities in outbreak prevention and control.43 Health commissioners contacted quarantined persons daily and recorded their physical status,44 while a hierarchical model of treatment ensured that those who were unwell received initial consultation from the nearest family doctor, and if necessary, were referred to a specialist or hospital.45 These measures significantly protected the health of those under quarantine.
Discussion
Clarifying the Criteria for Medical Coverage of People in Control Areas in Sectoral Laws
In China, the designation and management system of controlled areas is based on the constitution and supported by a series of laws, administrative regulations, and government rules. PCIDL designates controlled areas, while the ERL authorizes local governments to formulate specific safeguards. However, these laws and regulations provide only general and principled provisions for the livelihood protection of individuals in controlled areas and do not specifically address medical protection for those individuals.
The basic medical security standards for people in the control zones should be set in legislation from the following three aspects to ensure the health of people in the control zones. First, the legislation should strengthen the health protection of the personnel in the control zone, and it can be stipulated in Article 43 of the PCIDL that it should be clear that the local government should assign additional medical personnel to be stationed in the control zone when delineating the control area, so that the health condition of the personnel in the control area can be mapped, and the emergency situation can be answered at any time. Second, the vehicles and materials in the control zone should be well protected.Local governments should be required in ERL to provide special vehicles for the control zone, or coordinate the opening of 120 emergency line for people in the control area, to ensure that people in the control zone can seek medical treatment in a timely manner. Finally, the process of medical treatment should be simplified, and hospitals are required to set up special wards for patients in controlled areas, and all nucleic acid testing and medical treatment are carried out at the same time, so as to avoid delaying patients’ condition.
Giving Discretion to the Implementers of Epidemic Prevention and Control Policies
Considering China’s large population, it may not be realistic to have enough family doctors for quarantines as in Germany. However, this can be compensated for by providing sufficient discretion to the implementers of the epidemic prevention and control policy. Hospitals, communities, and police are the executors of the epidemic control policy, and they are the departments or subjects to which individuals in controlled areas have direct access when they need to seek medical treatment. Granting discretionary power to these entities in policy implementation can enable them to assist individuals in controlled areas in accessing medical treatment as quickly as possible.
Firstly, the specific responsibilities of hospitals, communities and police in epidemic prevention and control should be clarified in the legislation, so as to lay a legalized foundation for hospitals, communities and police to participate in epidemic prevention and control. Secondly, hospitals, communities and police should be granted discretionary power in implementing epidemic prevention and control measures, so that they can decide the relief measures they need to take on their own according to the emergency situation of the matter, and even break the epidemic prevention and control policy under special circumstances. Finally, the exemption clause is added to exempt hospitals, communities and police from punishment for failing to comply with the epidemic prevention and control regulations in order to protect the health of people in the control zones.
Establishing a Fair Punishment System
An unfair punishment system can lead to selective implementation of epidemic prevention and control policies by staff, resulting in disregard for the health of people in the control area. To address this issue, The law should make special provisions on how to protect the health of people in the controlled area. Firstly, the law should clarify the responsibility of communities and hospitals to provide assistance to people in the control zone. Should be clearly defined in PCIDL, managers of the control area and hospitals have an obligation to provide assistance to people in the control zone and cannot avoid or refuse to do so. Secondly, hospitals and individuals who fail to or improperly implement the relevant regulations should face punishment, including compensation, fines, demotion, dismissal, etc. Additionally, The CL should also stipulate that those who cause serious consequences such as injuries or deaths of people in the control zones will be investigated for criminal responsibility.
Conclusion
Through the analysis of the medical obstacles faced by the people in the control zone, it can be found that the ambiguity of the law is an important reason for the medical obstacles of the people in the control zone. Although the ERL authorizes local governments to formulate local policies in response to emergencies, there is still a lack of detailed legal provisions on what the emergency response plan should contain and what aspects the local government must safeguard. In light of the medical obstacles faced by individuals in controlled areas, it is necessary to improve Chinese legislation regarding specific relief measures, the authority of control area managers and policy implementers, and punishment for poor implementation of control policies. Doing so can help establish a legal system for medical protection of individuals in controlled areas.
Limitations of the Study
Our study has three limitations. First, we searched for typical incidents of medical disorders faced by the individuals in the COVID-19 control zone managed by the Chinese government, but the cases we were able to collect were officially confirmed incidents, and we could not collect accurate data on all controlled individuals who faced medical disorders. We have no way to guarantee the authenticity of the disclosed cases because they have not been officially confirmed. Therefore, we can only analyze and corroborate these officially published cases. Second, the control of COVID-19 is a dynamic process, so the policies of local governments in the control zones are always changing, so the subsequent adjustments and changes in management policies for control areas are not included in this study. Third, we focused more on the normative function of the law than on the social function, and the effect of the study was limited. In the future, we should expand the research scope to achieve a more comprehensive and systematic protection of the health of people in the control area in case of health emergencies. Despite the above limitations, it is undeniable that this paper has helped us to recognize the shortcomings in the management of COVID-19 control zones in China, and more research is needed to further improve the management of control zones in China in response to public health emergencies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pregnant women in Xi’an forced to miscarry by “deadly rules”; 2022. Available from:http://k.sina.com.cn/article_6443535879_v180108e07019015pvt.html.
2. Xi’an miscarriage: don’t let such a tragedy happen a second time; 2022. Available from: https://view.inews.qq.com/k/20220110A0CVJT00?web_channel=wap&openApp=false.
3. A pregnant woman in Xi’an had a miscarriage after waiting 2 hours in front of the hospital, what about maternal visits and deliveries during the epidemic?; 2022. Available from: https://view.inews.qq.com/a/20220105A09B3X00.
4. Xi’an, Shaanxi province: “pregnant women miscarriage” incident related to the responsible person was dealt with; 2022. Available from: http://tv.cctv.com/2022/01/06/VIDE0JVw1YK1J3REL45naoyj220106.shtml.
5. National Health Commission responds to miscarriage of pregnant woman in Xi’an; 2022. Available from: https://cj.sina.com.cn/articles/view/5069478980/12e2a1c44019015bjz.
6. Zhang S, Wang Z, Chang R, et al. COVID-19 containment: china provides important lessons for global response. Front Med. 2020;14(2):215–219. doi:10.1007/s11684-020-0766-9
7. The state council information office of the People’s Republic of China. Fighting COVID-19: China in action; 2021. Available from: http://english.www.gov.cn/atts/stream/files/5edc549dc6d0cc300eea778c.
8. National Health Commission: priority protection of acute and critical patients and other groups of medical needs; 2020. Available from: https://www.sohu.com/a/381881843_162522.
9. How to protect the normal access to medical care for isolation and containment personnel? National Health Care Commission response; 2022. Available from: http://www.bjnews.com.cn/detail/166824307114634.html.
10. How to protect the residents of the closed control area to quickly access medical care? Beijing districts do so; 2022. Available from: https://view.inews.qq.com/k/20220524A02NY10Z?web_channel=wap&openApp=false.
11. 2400 people have been guaranteed medical treatment! This district of Beijing’s control area has an emergency fleet played a big role; 2022. Available from: https://cj.sina.com.cn/articles/view/1750344480/68542320019019eb9?finpagefr=p_104.
12. Cecília T, Bhavana P, Rebecca R. Centering the right to health of childbearing people in the US during the COVID-19 pandemic. Front Public Health. 2022;10:1–5.
13. Burroughs E, Hill I, Taylor KJ, et al. Maternal health inequities during the COVID-19 pandemic. UrbanInstitute; 2021. Available from: https://www.rwjf.org/en/library/research/.2021/05/maternal-health-inequities-during-The-covid-19-pandemic.html.
14. Almuslim H, AlDossary S. Models of incorporating telehealth into obstetric care during the COVID-19 pandemic, its benefits and barriers: a scoping review. Telemed e-Health. 2021;28:24–38.
15. José L, Paulo A, Fernando A, Italla M, Paula C, Luiz C. Collision of fundamental human rights and the right to health access during the novel coronavirus pandemic. Front Public Health. 2021;08:1–14.
16. WHO: basic health services should continue to be provided while responding to the outbreak; 2022. Available from: https://www.ytcutv.com/folder355/folder356/folder383/folder391/2020-03-31/1320545.html.
17. Penelope F, Edwina D, Shannon M, Greg JF, Sarah B. Protecting mental health in quarantine: exploring lived experiences of healthcare in mandatory COVID-19 quarantine, New South Wales, Australia. SSM Popul Health. 2023;21:1–11.
18. Boudon R, Rawls J. A Theory of Justice. Contemp Sociol. 1976;5(05):102. doi:10.2307/2062920
19. Fei Q, Qi W. Guaranteeing the health rights of people with disabilities in the COVID-19 pandemic: perspectives from China. Risk Manag Healthc Policy. 2020;13(13):2357–2363. doi:10.2147/RMHP.S273685
20. Xue SP, Gu Q, Zhu KX, Jiang JH. Self-compassion buffers the impact of learned helplessness on adverse mental health during COVID-19 lockdown. J Affect Disord. 2023;327(372):285–291. doi:10.1016/j.jad.2023.01.099
21. Adhikari B, Poudel L, Thapa TB, Neupane D. Prevalence and factors associated with depression, anxiety, and stress symptoms among home isolated COVID-19 patients in Western Nepal. Dialogues Health. 2023;2:1–6.
22. Shawcroft J, Gale M, Sarah MC, Jean MT. screens and quarantine; the relationship between adolescent media use and mental health prior to and during COVID-19. Heliyon. 2022;8:1–9.
23. Kellie B. Emerging mental health issues in children and adolescents secondary to the COVID-19 pandemic. Adv Family Pract Nurs. 2022;11:1–21.
24. David R, Julia GB, Karla TW. “Second set of eyes”: family caregivers and post-acute home health care during the COVID-19 pandemic. Patient Educ Couns. 2023;106(109):1–6. doi:10.1016/j.pec.2022.10.352
25. Dowse G, Stein EJ. Born into an isolating world: family-centred care for babies born to mothers with COVID-19. EClinicalMedicine. 2023;56:1–12.
26. Pairin Y, Supa P, Ruangurai A, Siripoon P, Kasemsuk W, Buasai N. The roles of community health nurses for older adults during the COVID-19 pandemic in Northeastern Thailand: a qualitative study. Int J Nurs Sci. 2023;10(10):53–63. doi:10.1016/j.ijnss.2022.12.014
27. Parmet WE, Erwin PC. The challenges to public health law in the aftermath of COVID-19. Am J Public Health. 2023;113(3):267–268. doi:10.2105/AJPH.2022.307208
28. National Health Commission: the new crown pneumonia name change, the implementation of “B class B management”. Available from: http://swj.wuhan.gov.cn/tzdt/jcss/202212/t20221229_2121629.html.
29. WHO: the world needs to be better prepared for the next pandemic. Available from: https://oversea.huanqiu.com/article/3zngTBbGlTD.
30. Cecília T, Bhavana P, RC R. the right to health of childbearing People in the US during the COVID-19 pandemic. Front Public Health. 2022;10:1–5.
31. What are the criteria for dividing the closed area, control area and prevention area?; 2022. Available from: http://www.jl.gov.cn/szfzt/jlzxd/fkzs/202203/t20220331_8423281.html.
32. Nanjing Qixia District Hospital launched an emergency plan for the timely treatment of patients in the closed control area; 2022. Available from: https://cj.sina.com.cn/articles/view/1653603955/628ffe7302001efjy.
33. The suspension and resumption of medical services in major medical institutions in Shanghai on March 25, summarized in one article; 2022. Available from: https://baijiahao.baidu.com/s?id=1728246851606719296&wfr=spider&for=pc.
34. Hargreaves S, Kumar B, McKee M, Jones L, Veizis A. Europe’s migrant containment policies threaten the response to covid-19. BMJ. 2020;368:m1213. doi:10.1136/bmj.m1213
35. Feng Y. Research on the legality of community-imposed health coercive isolation measures in major epidemic prevention and control. J Tangshan Normal Coll. 2020;9:127–139.
36. Lanzhou G: a 3-year-old boy died of carbon monoxide poisoning, the police briefing came; 2022. Available from: https://page.om.qq.com/page/OJpV-Vl_f_rlvuHE7mt3fKlA0?source=cp_1009.
37. Delayed diagnosis and treatment, bad influence! Xi’an “maternal miscarriage incident” hospital involved in the results came; 2022. Available from: https://baijiahao.baidu.com/s?id=1721892822165034978&wfr=spider&for=pc.
38. Prevention and control measures are not in place in the Daoli District, four market entities were ordered to suspend business rectification; 2022. Available from: https://app.myzaker.com/news/article.php?f=weixin_mp&pk=637050e21bc8e05645000003.
39. Epidemic prevention and control is not effective! Fujian 428 people were dealt with; 2022. Available from: https://baijiahao.baidu.com/s?id=1658055955051325794&wfr=spider&for=pc.
40. Inadequate prevention and control, 8 cadres were filed and handled; 2022. Available from: https://view.inews.qq.com/a/20220427A0CTUE00.
41. WHO praises China: very strong measures taken; 2022. Available from: https://baijiahao.baidu.com/s?id=1728771034740743065&wfr=spider&for=pc.
42. Scott L, Kenneth AD, Michelle F, Jarman H, Trump BD. Alignment and authority: federalism, social policy, and COVID-19 response. Health Policy. 2023;127:12–18. doi:10.1016/j.healthpol.2022.11.007
43. Desson Z, Lambertz, L, Peters, JW, Falkenbach, M, Kauer, L. Europe's Covid-19 outliers: German, Austrian and Swiss policy responses during the early stages of the 2020 pandemic Health Policy and Technology; 2020;9(4);405–418. doi:10.1016/j.hlpt.2020.09.003
44. How does “home isolation” work in Germany? Including these details; 2020. Available from: https://www.163.com/dy/article/F7K4PPLI0514DTKM.html.
45. Wu Y. Analysis of the situation of novel coronavirus pneumonia epidemic in Germany and prevention and control measures. Country Reg Stud. 2020;2:142–172.
46. What is the difference between the closed area, the control area and the prevention area? Read it in one article!; 2022. Available from: https://baijiahao.baidu.com/s?id=1727809153477871453&wfr=spider&for=pc.
47. Lanzhou informed 3-year-old child died of gas poisoning investigation details, his father called 120 time line announced; 2022. Available from: https://baijiahao.baidu.com/s?id=1748454368024489030.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.