")
Back to Journals » International Journal of General Medicine » Volume 15
Length of Hospital Stay and Its Predictors Among Neonatal Sepsis Patients: A Retrospective Follow-Up Study
Authors Sisay EA , Mengistu BL, Taye WA, Fentie AM , Yabeyu AB
Received 12 August 2022
Accepted for publication 25 October 2022
Published 9 November 2022 Volume 2022:15 Pages 8133—8142
DOI https://doi.org/10.2147/IJGM.S385829
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Eskinder Ayalew Sisay,1 Bethlehem Lemma Mengistu,1 Workeabeba Abebe Taye,2 Atalay Mulu Fentie,1 Abdella Birhan Yabeyu3
1Department of Pharmacology and Clinical Pharmacy, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pediatrics and Child Health, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Pharmacy, Ambo University, Ambo, Ethiopia
Correspondence: Eskinder Ayalew Sisay, Email [email protected]
Introduction: Sepsis is common among neonates, and is often fatal. Hospitalization results in severe nosocomial infections which could be resistant to antibiotics. It also incurs higher fees for medical care.
Methods: A retrospective follow-up study, which includes 206 neonates, was conducted to assess the length of hospital stay among neonatal sepsis patients from September 2018 to September 2020 at TASH Hospital, Addis Ababa, Ethiopia. Data were collected from medical charts. Mean length of hospital stay was compared using independent sample t-tests. Risk factors for length of stay were identified using binary logistic regression analysis.
Results: All neonates stayed a total of 325 days, which gives 75,512 neonate-days. Neonates who stayed more than 7 days had low mean birth weight and higher mean age at admission. Mean length of stay was higher among neonates with comorbid illness, neonates with drug therapy problems and male neonates. Even though the mean length of stay is shorter among neonates with maternal PROM and CS delivery, these maternal factors were found to be insignificant in the multivariate logistic regression.
Discussion: Similar to other studies, neonates with low birth weight and comorbidity had a longer hospital stay. Neonates with maternal PROM and CS delivery had a shorter stay. But these maternal factors, identified by prior studies as risk factors for neonatal sepsis and its mortality, are not found to be predictors of prolonged hospitalization. Having neurologic features and drug therapy problems among neonates with sepsis prolonged hospital stay.
Conclusion: The mean length of stay varies with respect to maternal and neonatal factors. Lower birth weight, presence of neurologic features, presence of comorbidity, presence of drug therapy problems and being male are found to be predictors of a longer hospital stay among neonates with sepsis.
Keywords: neonatal sepsis, Ethiopia, hospital stay
Introduction
Newborn babies less than 28 days can encounter a bloodstream infection known as neonatal sepsis (NS).1,2 Epidemiology indicates that up to 3 million sepsis cases occur per year among neonates, with a global mortality of 400,000–700,000 every year.3
Sepsis among neonates can be classified into early onset and late onset. Early onset neonatal sepsis (EONS) is diagnosed among neonates with age less than seven days and it is caused by infection developed in the mother earlier and in the course of delivery and transmitted by way of bloodstream or placenta. Late onset neonatal sepsis (LONS) is diagnosed among neonates with age above seven days and neonates acquire this infection once delivered.4,5 According to the global estimates of neonatal sepsis, EONS is 2.6-fold more prevalent compared to LONS.6 This estimate comprises data from 2 low-income, 20 middle-income and 4 high-income countries which do not show the actual incidence in developing nations where LONS is more common than EONS.
Causative organisms for sepsis among neonates vary between low-income and high-income countries.7 Prevalent pathogens causing sepsis among neonates in low-income countries include: Staphylococcus aureus, Escherichia Coli and Klebsiella species.8
Treatment guidelines for neonatal sepsis suggest hospital admission as well as parenteral treatment containing gentamicin with benzyl penicillin or ampicillin for a minimum of seven to ten days.3,7 Clinicians may also consider the use of second-generation cephalosporins and vancomycin. Duration of hospital stay is determined depending on patient wellbeing and the pathogen identified by the culture and sensitivity tests.
Multiple births, not attending antenatal care (ANC), cesarean section (CS) delivery, absence of breastfeeding immediately after delivery, premature birth, low birth weight, EONS and duration of hospitalization are found to be predictors of neonatal sepsis morbidity.9–13
Prolonged hospitalization among neonates increases the chance of acquiring a new infection, which increases cost of treatment. It also complicates the selection of antibiotics. Hence, assessing length of hospital stay and its contributing factors among neonatal sepsis patients helps to design plans which can solve problems and thus improves patient outcomes.
This study aimed to assess the mean length of hospital stay as well as to identify its predictors among neonates treated at a resource limited set up.
Methodology
Study Area and Study Design
The study was undertaken at a university hospital (Tikur Anbessa Specialized Hospital [TASH]) in Addis Ababa, Ethiopia. It is a tertiary hospital with multiple specialty departments. Study participants were recruited from neonatal intensive care unit (NICU) which is under the pediatrics department.31
A retrospective follow-up study among neonates admitted at NICU was conducted from September, 2018 to September, 2020.31
Eligibility Criteria
Neonates with age ≤28 days admitted at NICU and who had sepsis diagnosis clinically or with culture were included in the study. Neonates who were treated for less than 2 days as well as who left against medical advice or referred to another healthcare facility were excluded from the study.
Sampling Technique and Sample Size
The sample size for this cohort study was determined considering a 95% level of confidence interval, 80% power and adjusted hazard ratio of 0.34, as depicted in an earlier Ethiopian study.10 A total of 206 neonates who were admitted to the NICU from September, 2018 to September, 2020 were enrolled in the study by systematic random sampling method. The first medical chart was selected using simple random sampling and consecutive medical charts were selected every 5 for SVD-delivered and every 10 for CS-delivered neonates till we achieved the total number of study participants, which is 137 neonates with SVD-delivery and 69 neonates with CS-delivery.
Data Collection and Analysis
Data were collected using a structured questionnaire prepared in English which was adapted from previous studies5,10,14 and includes sociodemographic characteristics, mode of delivery, maternal predictors, signs and symptoms and sepsis type, treatment modality and length of hospital stay. Two nurses working at NICU ward were enrolled as data collectors after training.
Data was entered and analyzed using SPSS version 25. Frequency, mean and percentage were calculated to describe the findings. The mean length of hospital stay was compared between different categorical variables using the independent samples t-test. Regression analysis was employed for assessing risk factors of length of hospitalization. Statistical significance was determined at p-value <0.05.
Ethical Considerations
The study has got ethical clearance from Pharmacy School at Addis Ababa University, with a reference number ERB/SOP/201/02/2020. Being a retrospective follow-up study, we have used secondary data abstracted from medical charts. Consent was obtained from NICU; thus informed consent from the parents of the study participants was not required for the study and was exempted by the ethics committee. Patient identifiers were not recorded during data collection to keep confidentiality. This study complies with the Declaration of Helsinki.
Operational Definition
- Neonatal sepsis: defined as blood-stream infection among neonates aged ≤28 days,5,15 diagnosed by the attending physician either clinically or by blood culture. For clinical diagnosis of sepsis, physicians in our set-up used fever, complete blood count findings, inflammatory markers and respiratory, gastrointestinal, neurologic and metabolic features.
- Length of hospital stay: classified as early if it is less than or equal to seven days and late or prolonged if it is for longer than seven days.
Results
Participants’ Sociodemographic Characteristics
This study recruited 206 neonates. Male neonates accounted for 56.8%. Neonates had a mean age of 2.63 days. Low birth weight (weight less than 2.5 kg) was recorded among 44% of study participants. We had 5 overweight neonates (>4 kg), 91 low birth weight neonates (<2.5 kg) and 110 normal birth weight neonates (2.5–4 kg). ANC attendance was recorded among majority of participants. Term delivery accounted for 58.3% (Table 1).
 |
Table 1 Sociodemographic Features of Participants Admitted at NICU, TASH, Addis Ababa, Ethiopia |
Clinical Data
Considering maternal risk factors for neonatal sepsis, 78 mothers (37.9%) had experienced premature rupture of membrane (PROM). Chorioamnionitis was seen among 17 (8.3%) mothers. Maternal labor lasting <18 hours was recorded for 84.4% of the neonates. Maternal UTI and febrile history was absent among majority of the neonates (Table 2).
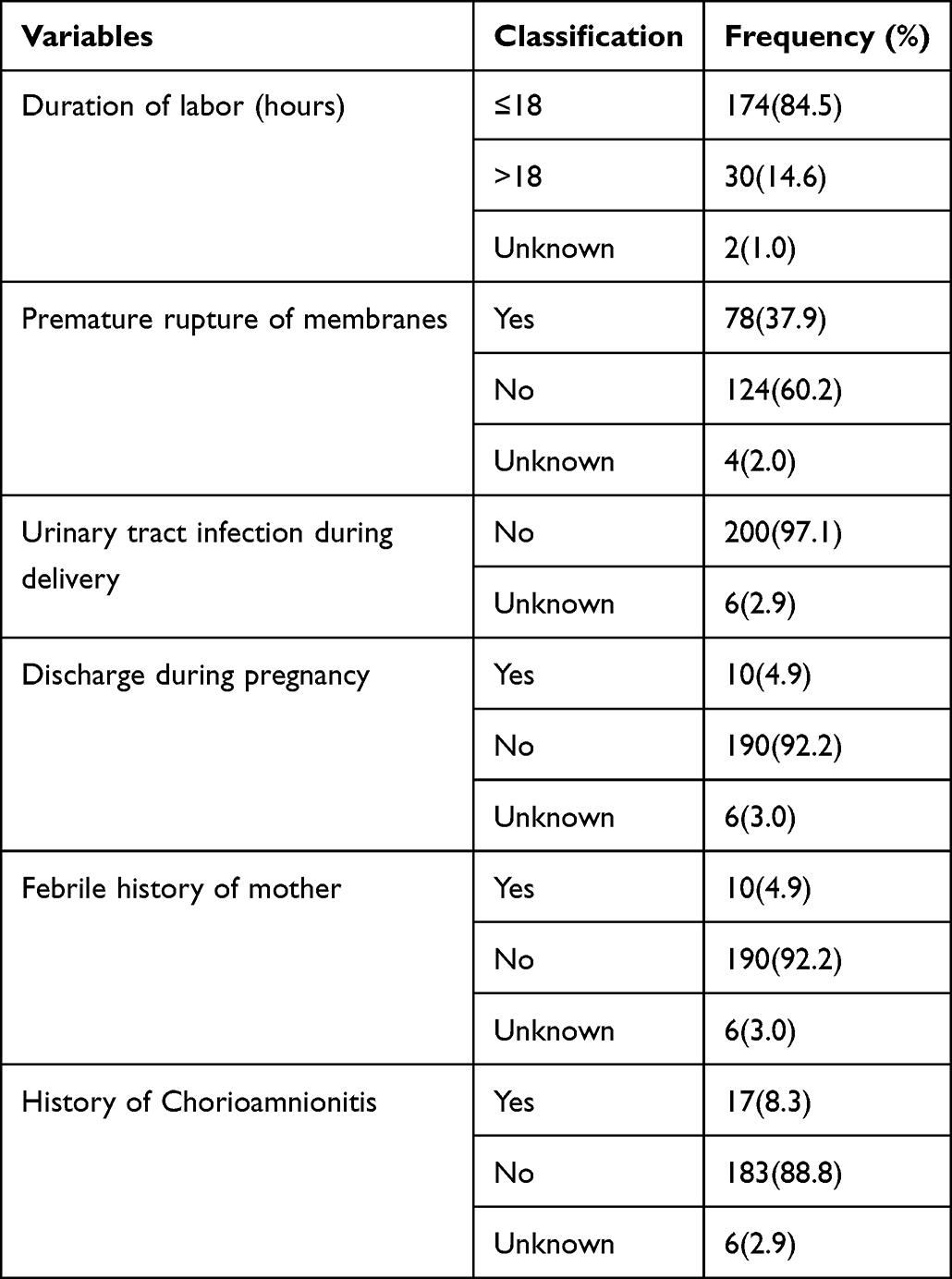 |
Table 2 Maternal Predictors of Sepsis for Neonates Admitted at NICU, TASH, Addis Ababa, Ethiopia |
With respect to the medical history, more than 80% of neonates did not have prior hospitalization: 71.4% of neonates had EONS and 52 neonates had comorbidity. Neonatal jaundice accounted for the highest comorbidity. More frequent focus of sepsis infection was CNS and chest (Table 3).
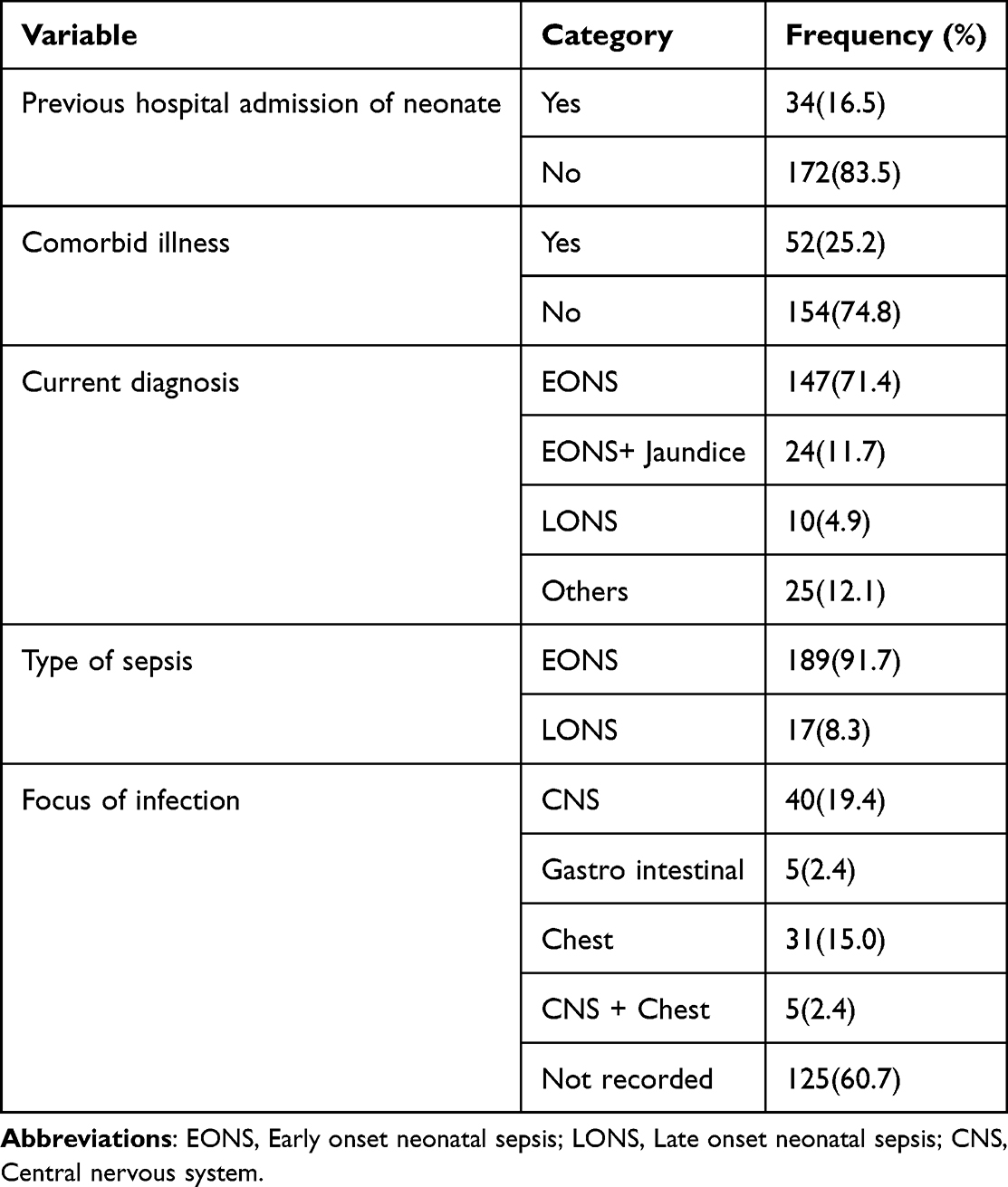 |
Table 3 Medical History of Neonatal Sepsis at TASH, NICU, Addis Ababa, Ethiopia (n = 206) |
During the study period, a total of 76 samples were sent for culture, of which nearly 41 samples were sent after empiric treatment with antibiotics. Culture and gram stain results were received only for 12 neonates and the specific pathogens identified were K.pneumonia (ie predominant pathogen that is identified in 7 neonates), E.coli, Acitinobacteracia, Enterobacteracia and MRSA. Culture and sensitivity data showed bacterial growth among 12 neonatal sepsis patients and gram-negative pathogens were common.
The most common symptom among the study participants was GI symptom followed by respiratory symptom, which existed in184 (89.3%) and 100 (48.5%) neonates, respectively (Table 4). The reported GI symptoms were poor feeding, vomiting and abdominal distension. The respiratory symptoms were irregular respiration/tachypnea, flaring and granting and chest retraction. Reported neurologic features were tremor/seizure, decreased activity/lethargy and irritability (Table 4).
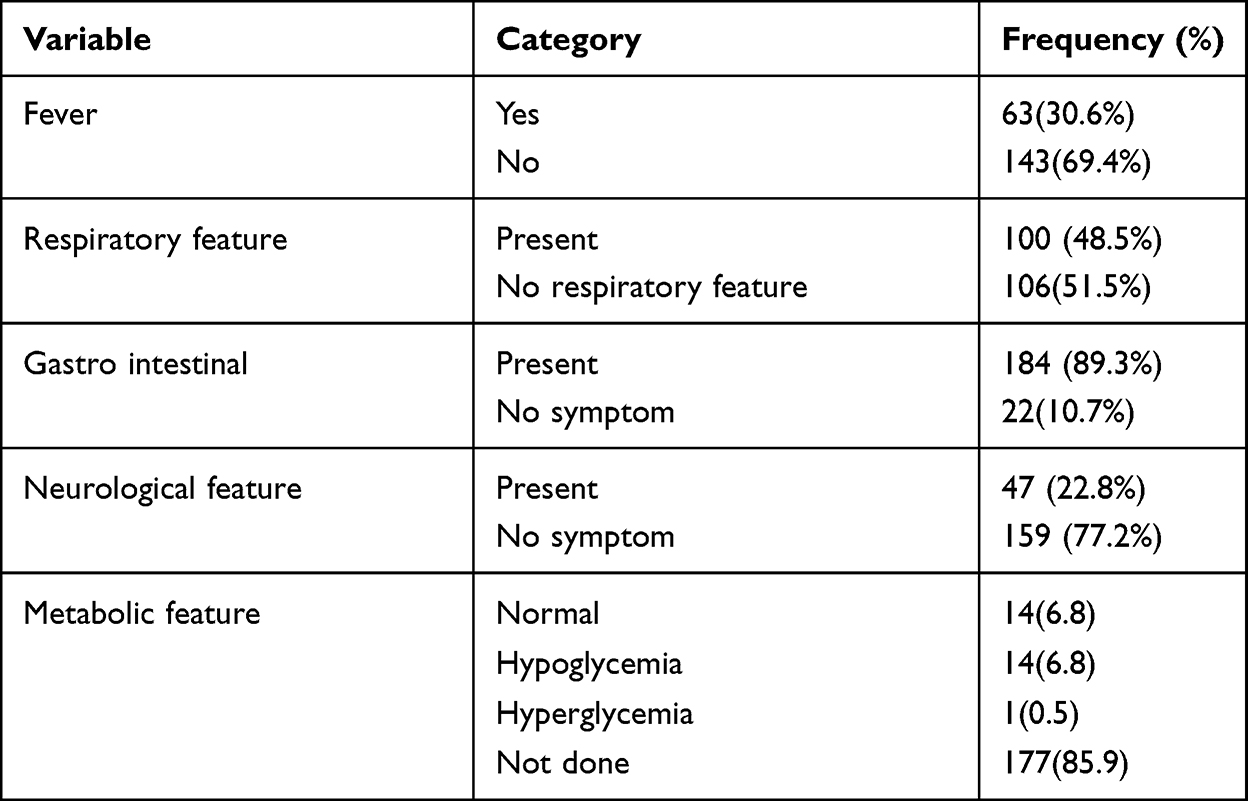 |
Table 4 Clinical Symptoms of Neonatal Sepsis Among Neonates Admitted at TASH, Addis Ababa, Ethiopia (n = 206) |
Antibiotics were prescribed empirically for 195 (94.7%) neonates; 81.6% of the prescriptions consisted of Ampicillin with Gentamicin, while 13.1% of the prescriptions were for Ampicillin with ceftriaxone (Figure 1).
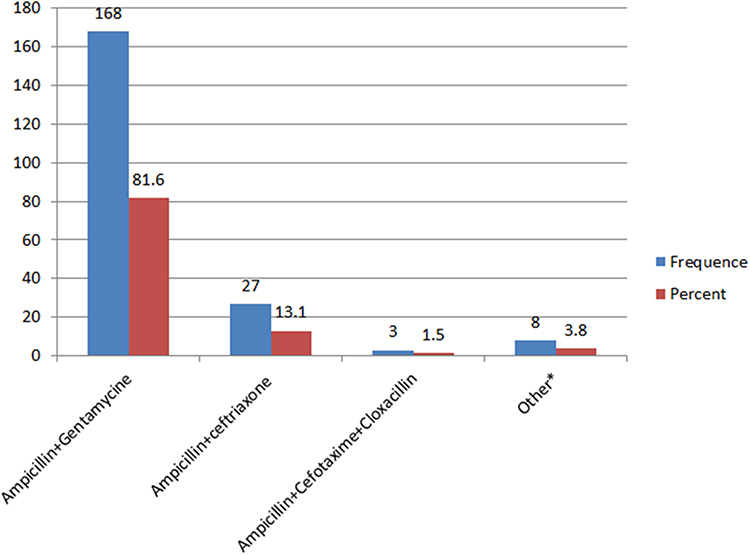 |
Figure 1 Antibiotic regimen percentages prescribed for neonates with sepsis admitted at NICU, TASH, Addis Ababa, Ethiopia (Other* Ampicillin + Gentamicin + Metronidazole; Ampicillin + Ceftriaxone; Cefepime + Vancomycin; Cefepime + Vancomycin + Metronidazole; Ceftriaxone + Azithromycin; Ceftriaxone + Gentamicin). |
Length of Hospital Stay
All 206 neonates stayed a total of 325 days, which gives 75,512 neonate-days. The mean length of hospital stay is 8.92 days (± 6.18 SD) (min 3 days, max 30 days). Based on the category of length of hospital stay used in our study, 129 (62.6%) neonates stayed for ≤7 days while 77 (37.4%) neonates stayed for longer than 7 days.
Comparison of the Mean Length of Hospital Stay
We compared the mean length of hospital stay for different categorical variables using the independent samples t-test. The mean length of hospital stay was found to be statistically different with respect to mode of delivery, presence of comorbid illness, gender and presence of premature rupture of membranes (PROM). The current study showed that neonates with comorbid illness and drug-related problems, neonates delivered by SVD, male neonates and neonates without PROM had higher mean length of hospital stay (Table 5).
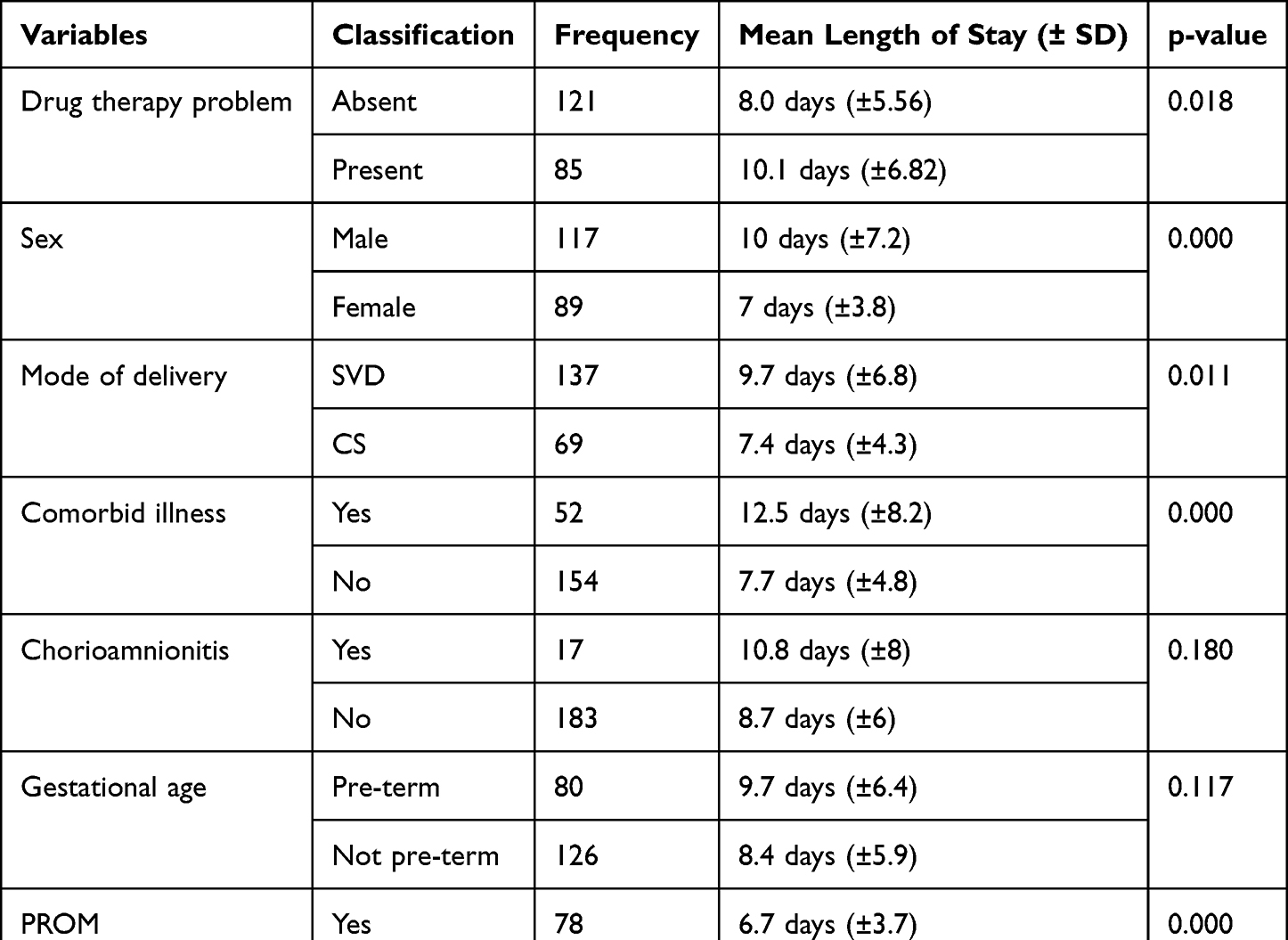 |
Table 5 Mean Difference for Length of Hospital Stay for Sepsis Amongst Neonates Admitted at NICU, TASH, Addis Ababa, Ethiopia |
We also compared the length of hospital stay with respect to the mean birth weight and mean age at admission using the independent samples t-test by assuming equal variances and at a 2-tailed significance level. Results showed that there is statistical significant difference in the mean of birth weight and mean age between neonates admitted for ≤7 days and >7 days (Table 6).
 |
Table 6 Independent Samples t-Test for Mean Birth Weight and Age at Admission with Respect to Length of Hospital Stay |
Predictors of Length of Hospital Stay
We did statistical analysis to identify predictors of length of hospital stay using variables including: socio demographic variables, method of delivery (SVD and CS), clinical presentations, drug-related problems and maternal factors.
Logistic regression analysis was employed to test predictors for length of hospital stay. Univariate logistic regression analysis was done for the independent variables and we included variables with p-value >0.2 in the multivariate logistic regression analysis. Multivariate logistic regression analysis showed that birth weight, presence of chorioamnionitis, presence of neurological features, presence of comorbidities, presence of drug therapy problems and being male were significantly associated with length of hospital stay (Table 7).
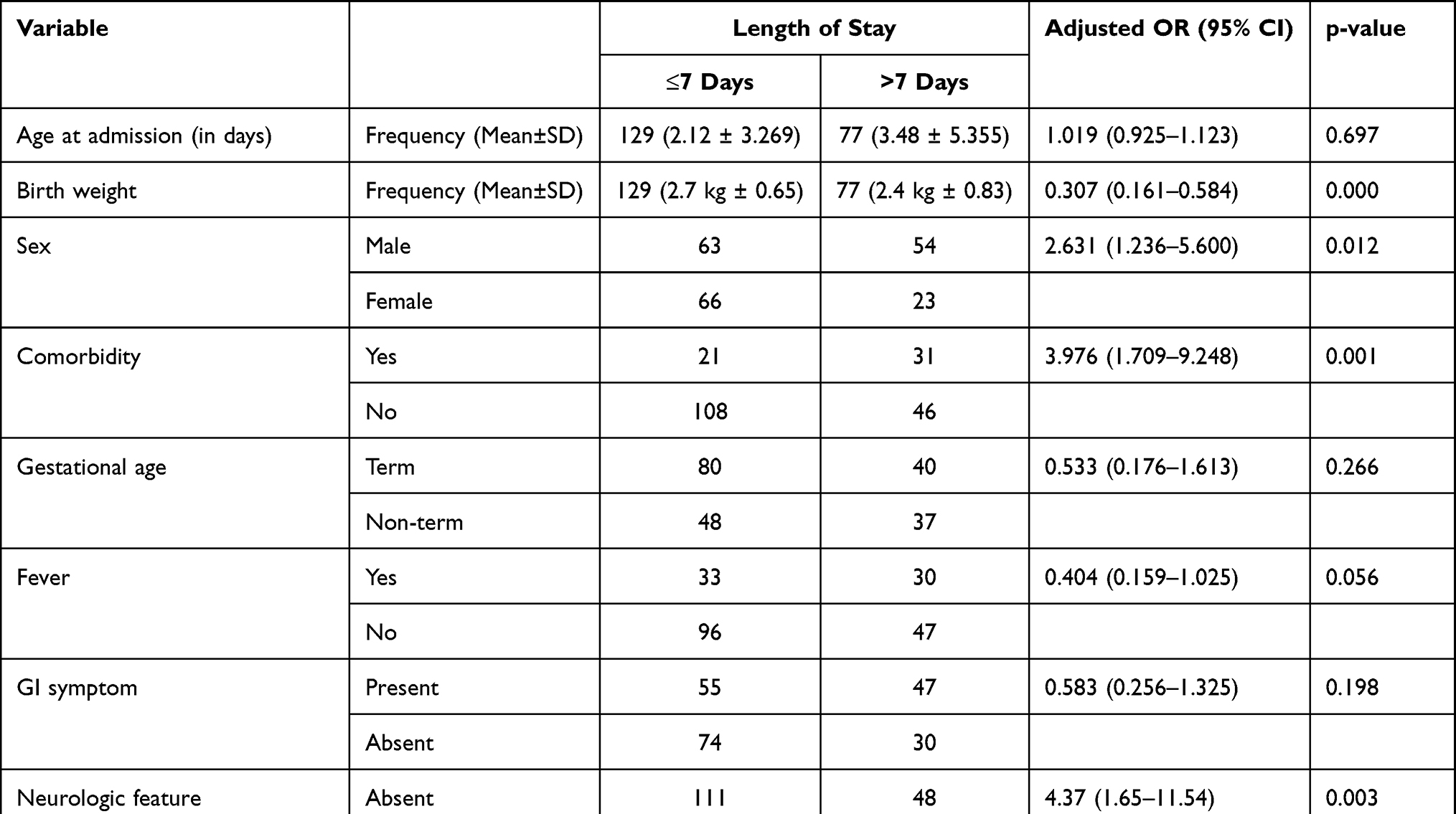 |
Table 7 Length of Hospital Stay Predictors for Neonatal Sepsis Patients Admitted at NICU, TASH, Addis Ababa, Ethiopia (Multivariate Logistic Regression Analysis Result) |
Discussion
In the current study, 137 neonates with SVD-delivery and 69 neonates with CS-delivery were included. All neonates were diagnosed with sepsis but only 5.82% (n = 12) of cases were culture proven. However, Philippine and Ethiopian studies indicated greater cases of sepsis proved by blood culture, accounting for nearly half of the neonatal sepsis cases.2,5,7–10,16 Gram negatives were the predominant pathogens identified in our study, which is similar to other studies in developing countries in Asia, the Middle East and Africa.17–22 Contradictory result was obtained where gram positive were predominant over gram negative pathogens, as indicated in different studies.20,23–26 The possible explanation for this difference may relate to the difference in causative pathogens between the regions and the periods. It might be also associated with other aspects (sample handling, laboratory quality and timing in antibiotic initiation).
Most of the neonates were treated with empiric antibiotics, predominantly by the combination of “Ampicillin + Gentamicin”. According to WHO guidelines, parenteral Ampicillin with Gentamicin is a preferred treatment for a neonate having known risk factors of sepsis for no less than 2 days. Nevertheless, using unconventional practices to use cephalosporin (mostly Cefotaxime) or glycopeptides (mostly Vancomycin) is increasing as recommended therapy, particularly for LONS because of higher antibiotic resistance among prevalent pathogens like Coagulase negative staphylococci. For EONS, we can use Ampicillin with 3rd generation cephalosporins (mostly Cefotaxime) as alternative therapy.7,27 Previous Ethiopian studies also showed predominant use of Ampicillin with Gentamicin.15,28 In contrast, a Pakistani study showed that Amikacin with Cefotaxime was also given as initial therapy.13 The dissimilarity in the management approaches can be related to variation of the causative agent for sepsis as well as the antimicrobial susceptibility pattern among the different set ups.
The mean length of hospital stay was found to be statistically different with respect to mode of delivery, presence of comorbid illness, gender and presence of PROM. The current study showed that neonates with comorbid illness, neonates delivered by SVD, male neonates and neonates without PROM had higher mean length of hospital stay. Absence of PROM and SVD delivery were previously known to reduce the risk of neonatal sepsis9–13 but this did not necessarily associate with the length of hospital stay for the treatment of neonatal sepsis. This is shown by our study, where neonates delivered from mothers with these factors had a prolonged hospital stay. In our study it is observed that neonates who stayed more than 7 days had low mean birth weight and a higher mean age at admission.
Similar to other studies, the current study showed that lower birth weight is associated with longer hospital stay.29,30 This is shown by the logistic regression analysis where an increase in birth weight was found to be protective and thus is associated with a shorter hospital stay, ie ≤7 days (AOR = 0.3). Neonates with comorbid illness and neurologic features were more likely to stay longer (AOR = 3.9 and AOR = 4.37 respectively). Male neonates stay longer compared to female neonates, indicating gender as a predictor of length of hospital stay. Maternal history of Chorioamnionitis is associated with shorter hospital stay of neonates; this may be due to health professionals’ curiosity and better follow-up care for those neonates delivered from mothers with Chorioamnionitis as it is a well-known risk factor for neonatal sepsis.
We also found statistical significant difference in the mean length of hospital stay between neonates with and without drug-related problems (10 days vs 8 days). Absence of drug therapy problem was found to be protective and thus is associated with a shorter hospital stay, ie ≤7 days (AOR = 0.4). Neonates with drug therapy problems were 2.5 times more likely to stay more than 7 days as compared to neonates without drug therapy problems. The drug-related problems were retrospectively identified by clinical pharmacist and include: sub-therapeutic dosage of antibiotics, use of ineffective antibiotics, unnecessary use of antibiotics and a need for additional antibiotics among neonates with sepsis. This finding indicates the importance of solving drug-related problems to shorten the length of hospitalization and is a call for clinical pharmacists’ involvement in the neonatal ICU of the study set up.
The current study recommends the OBY/GYN department as well as the health professionals to carefully manage sepsis among neonates as well as contemplate the predictors for length of stay.
Conclusion
The mean length of hospital stay is higher among neonates with comorbid illness, neonates delivered by SVD, neonates without PROM, neonates with drug therapy problems and male neonates. Neonates who stayed more than 7 days had low mean birth weight and a higher mean age at admission. But only lower birth weight, presence of neurologic features, presence of comorbidity, presence of drug therapy problems and being male were found to be significant predictors of longer hospital stay among neonates with sepsis.
Acknowledgments
We would like to acknowledge Mrs Bethlehem L. Mengistu as this paper emanates from her thesis. We also would like to thank Addis Ababa University and Tikur Anbessa Specialized Hospital for funding this research project and for providing access to patient data, respectively.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aggarwal R, Sarkar N, Deorari AK., et al. Sepsis in the newborn. Indian J Pediatr. 2001;68(12):1143–1147. doi:10.1007/BF02722932
2. Hanumantha S, Tabaseera N. Bacteriological Profile and Antimicrobial Susceptibility Pattern of Blood Culture Isolates among Septicemia Suspected Children in a Rural Tertiary Care Hospital. Int J Curr Microbiol App Sci. 2017;6(11):1167–1171. doi:10.20546/ijcmas.2017.611.139
3. World Health Organization. (2020). Global report on the epidemiology and burden of sepsis: current evidence, identifying gaps and future directions. World Health Organization. Available from: https://apps.who.int/iris/handle/10665/334216.
4. Vergnano S, Sharland M, Kazembe P, Mwansambo C, Heath PT. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2005;90(3):F220–4. doi:10.1136/adc.2002.022863
5. Tewabe T, Mohammed S, Tilahun Y, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia: a retrospective chart review. BMC Res Notes. 2016;10:265. doi:10.1186/s13104-017-2573-1
6. Fleischmann C, Reichert F, Cassini A, et al. Global incidence and mortality of neonatal sepsis: a systematic review and meta-analysis. Arch Dis Child. 2021;106(8):745–752. doi:10.1136/archdischild-2020-320217
7. Fuchs A, Bielicki J, Mathur S, Mike Sharland JN, Van DA. Antibiotic use for sepsis in neonates and children: evidence update. WHO Reviews; 2016. Available from: https://pdf4pro.com/amp/view/antibiotic-use-for-sepsis-in-neonates-and-children-2016-47c88e.html.
8. Shitaye D Neonatal sepsis: bacterial etiologic agents and their antibiotic susceptiability pattern in Tikur Anbessa Hospital, Addis Ababa, Ethiopia. M.Sc. Thesis, Addis Ababa University; 2008. Available from: http://213.55.95.56/handle/123456789/5116.
9. Worku B, Kassie A, Mekasha A, Tilahun B, Worku A. Predictors of early neonatal mortality at a neonatal intensive care unit of a specialized referral teaching hospital in Ethiopia. Ethiop J Heal Dev. 2012;26(3):200–207.
10. Orsido TT, Asseffa NA, Berheto TM. Predictors of Neonatal mortality in Neonatal intensive care unit at referral Hospital in Southern Ethiopia: a retrospective cohort study. BMC Pregnancy Childbirth. 2019;19(1):83. doi:10.1186/s12884-019-2227-5
11. Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr. 2020;1:10. doi:10.1155/2020/8327028
12. Leal YA, Álvarez-Nemegyei J, Velázquez JR, et al. Risk factors and prognosis for neonatal sepsis in southeastern Mexico: analysis of a four-year historic cohort follow-up. BMC Pregnancy Childbirth. 2012;12(1):48. doi:10.1186/1471-2393-12-48
13. Atif M, Zia R, Malik I, Ahmad N, Sarwar S. Treatment outcomes, antibiotic use and its resistance pattern among neonatal sepsis patients attending Bahawal Victoria Hospital, Pakistan. PLoS One. 2021;16(1):e0244866. doi:10.1371/journal.pone.0244866
14. Freitas FTM, Araujo AFOL, Melo MIS, Romero GAS. Late-onset sepsis and mortality among neonates in a Brazilian Intensive Care Unit: a cohort study and survival analysis. Epidemiol Infect. 2019;147:e208. doi:10.1017/S095026881900092X.
15. Fekadu G, Abera T, Tekle T. Clinical Treatment Outcomes of Neonatal Sepsis in Neonatal Intensive Care Unit of Wollega University Teaching and Referral Hospital, Nekemte Town, Western Ethiopia. Pediatr Ther. 2019;9(1):845.
16. Wale A, Chelkeba L, Wobie Y, Abebe A. Treatment Outcome and Associated Factors of Neonatal Sepsis at Mizan Tepi University Teaching Hospital, South West Ethiopia: a Prospective Observational Study. Pediatric Health Med Ther. 2021;12:467–479. doi:10.2147/PHMT.S322069
17. de Souza Rugolo LMS, Bentlin MR, Mussi-Pinhata M. Late-Onset Sepsis in very Low Birth Weight Infants: a Brazilian Neonatal Research Network Study. J Trop Pediatr. 2014;60(6):415–421. doi:10.1093/tropej/fmu038
18. Islam QR, Shahidullah M, Islam MZ, Mridha MAA, Akter S. Bacterial Profile of Neonatal Septicemia and Antibiotic Susceptibility Pattern of the Isolates in Tertiary Care Hospital, Dhaka, Bangladesh. Bangladesh J Child Health. 2019;43(1):35–40. doi:10.3329/bjch.v43i1.41216
19. Pokhrel B, Koirala T, Shah G, et al. Bacteriological profile and antibiotic susceptibility of neonatal sepsis in neonatal intensive care unit of a tertiary hospital in Nepal. BMC Pediatr. 2018;18(1):208. doi:10.1186/s12887-018-1176-x
20. El-din EMRS, El-sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of Neonatal Sepsis and Implicated Pathogens: a Study from Egypt. Biomed Res Int. 2015;2;11. doi:10.1155/2015/509484
21. Yadav NS, Sharma S, Chaudhary DK, et al. Bacteriological profile of neonatal sepsis and antibiotic susceptibility pattern of isolates admitted at Kanti Children’s Hospital, Kathmandu, Nepal. BMC Res Notes. 2018;11(1):301. doi:10.1186/s13104-018-3394-6
22. Tapa S, Sapkota LB. Changing Trend of Neonatal Septicemia and Antibiotic Susceptibility Pattern of Isolates in Nepal. Int J Pediatr. 2019;7. doi:10.1155/2019/3784529
23. Peterside O, Pondei K, Akinbami FO. Bacteriological Profile and Antibiotic Susceptibility Pattern of Neonatal Sepsis at a Teaching Hospital in Bayelsa State, Nigeria. Trop Med Health. 2015;43(3):183–190. doi:10.2149/tmh.2015-03.
24. Gupta S, Sakhuja A, Kumar G, et al. Culture-Negative Severe Sepsis: nationwide Trends and Outcomes. Chest. 2016;150(6):1251–1259. doi:10.1016/j.chest.2016.08.1460
25. Aku FY, Akweongo P, Nyarko K, et al. Bacteriological profile and antibiotic susceptibility pattern of common isolates of neonatal sepsis, Ho Municipality, Ghana-2016. Neonatol Perinatol. 2018;4:25. doi:10.1186/s40748-017-0071-z
26. Geyesus T, Moges F, Eshetie S, et al. Bacterial etiologic agents causing neonatal sepsis and associated risk factors in Gondar, Northwest Ethiopia. BMC Pediatr. 2017;17(1):137. doi:10.1186/s12887-017-0892-y
27. Korang SK, Safi S, Gluud C, Lausten-Thomsen U, Jakobsen JC. Antibiotic regimens for neonatal sepsis - a protocol for a systematic review with meta-analysis. Syst Rev. 2019;8(1):306. doi:10.1186/s13643-019-1207-1
28. Woldu MA, Guta MB, Lenjisa JL. Assessment of the incidence of neonatal sepsis, its risk factors, antimicrobials use and clinical outcomes in Bishoftu General Hospital, neonatal intensive care unit, Debrezeit-Ethiopia. Int J Contemp Pediatr. 2014;1(3):135–141.
29. Sahiledengle B, Tekalegn Y, Zenbaba D, Woldeyohannes D, Teferu Z. Which Factors Predict Hospital Length-of-Stay for Children Admitted to the Neonatal Intensive Care Unit and Pediatric Ward? A Hospital-Based Prospective Study. Glob Pediatr Health. 2020;7:2333794X20968715. doi:10.1177/2333794X20968715
30. Seaton SE, Barker L. Modelling neonatal care pathways: investigating length of stay for preterm infants. Infant. 2016;12(3):87–90.
31. Mengistu BL. Treatment Outcome of Neonatal Sepsis and Associated Factors among Neonates Admitted to Neonatal Intensive Care Unit of Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: a Retrospective Cohort Study [Thesis]. Addis Ababa: Addis Ababa University; 2022. Available from: http://etd.aau.edu.et/bitstream/handle/123456789/31232/Bethlehem%20Lemma.pdf?isAllowed=y&sequence=1.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.